
Abstract
Infections represent a common health problem in people of all ages. Usually, the response given to them is appropriate and so little treatment is needed. Sometimes, however, the response to the infection is inadequate and may lead to organ dysfunction; this is the condition known as sepsis. Sepsis can be caused by bacteria, fungi or viruses and at present there is no specific treatment; its management basically focuses on containing the infection through source control and antibiotics plus organ function support. This article reviews key elements of sepsis management, focusing on diagnosis, biomarkers and therapy. The main recent advance in therapy is the strategy of personalized medicine, based on a precise approach using biomarkers to identify specific individuals who are likely to benefit from more personalized attention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sepsis is one of the most common causes of death among hospitalized patients in the intensive care unit (ICU). It is particularly difficult to diagnose in this setting because of the multiple comorbidities and underlying diseases that these patients present [1, 2].
The definitions of sepsis and septic shock focusing on the host’s inflammatory response have remained unchanged since the first consensus conference held in 1991. Advances in the understanding of the pathophysiology of sepsis, which is characterized today as a host reaction to infection involving not only the activation of pro- and anti-inflammatory responses but also modifications in non-immunological pathways (cardiovascular, autonomic, neurological, hormonal, metabolic and clotting), have led experts to revise the definitions. In 2016, the Sepsis-3 conference defined sepsis as a “life-threatening organ dysfunction caused by a deregulated host response to infection”, and septic shock as a “subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality” [3]. This is a narrative review with the objective to update the advances in sepsis management. The first part focuses on diagnosis, with a review of potential contribution of biomarkers, and the second part focuseson advances in therapy.
Compliance with Ethics Guidelines
This article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors.
Diagnosis of Sepsis
Clinical Diagnosis
The Sepsis-3 definitions call for a new clinical tool to replace the criteria for systemic inflammatory response syndrome (SIRS) in identifying patients with sepsis. These criteria are non-specific, as they are not present in all patients with infection, and they do not necessarily reflect an abnormal host response. This is, for example, the case of fever: immunosuppressed patients do not always develop fever, so the infection is hard to detect. In contrast, critically ill patients have a certain degree of hyperthermia but may not present infection [4].
The current recommendation for identifying both sepsis and septic shock is the use of the SOFA score [Sequential (Sepsis-Related) Organ Failure Assessment]. SOFA is a simple system, which uses accessible parameters in daily clinical practice to identify dysfunction or failure of the key organs as a result of sepsis. It was developed at an expert meeting and the assessment of physiological changes in response to septic attack was scored by consensus. Despite this initial subjectivity, the SOFA calibration is correct and properly adjusted to the subsequent evolution of the patient. Regardless of the initial SOFA score, an increase during the first 48 h in the ICU predicts a mortality rate of at least 50% [5, 6].
In 2016, qSOFA (quick SOFA) was developed. This new score includes only clinical criteria that are easily and quickly measurable at the bedside:
-
Altered level of consciousness, defined as a Glasgow Coma Scale score ≤ 13.
-
Systolic blood pressure ≤ 100 mmHg.
-
Respiratory rate ≥ 22 rpm.
When at least two of these criteria are present, it has been suggested that qSOFA has a similar predictive validity to the original score for the detection of patients with sepsis and likely to have a poor outcome [3]. Further validation is required, and it has received initial criticism on the grounds that it may be difficult to use in low- and middle-income countries. Moreover, sensitivity may be only 50% in patients with pneumonia in the Emergency Department, and poor specificity in subsets like hematological patients is to be expected.
It should be noted that recognition of septic shock has usually been associated with the presence of hypotension. However, this criterion is insufficient, since in most patients the onset of hypotension is preceded by tissue hypoperfusion. Tissue hypoperfusion is detected by measuring the levels of lactate in blood. Hypotension often does not appear, or appears late, whereas tissue perfusion may be severely compromised on a global or regional level without necessarily being associated with hypotension. For these reasons, the recognition of septic shock must be based on identifying tissue hypoperfusion. As there is no single and specific criterion for its identification, several parameters need to be evaluated [7, 8].
Laboratory Diagnosis
Laboratory tests are required to help diagnose sepsis, distinguish it from other conditions, and evaluate and monitor organ function, blood oxygenation and the acid–base balance.
In the diagnosis of sepsis, the contribution of laboratory hematological, biochemical and microbiological test is essential. However, culture-based diagnosis is slow, and so, in recent years, major efforts have been made to find biomarkers that allow early diagnosis of this disease. In general, the markers that are studied are related to inflammatory mechanisms, in the hope that they could complement or replace others already in use, such as C-reactive protein (CRP) and procalcitonin (PCT). These tools cannot be used alone, and should complement careful clinical assessment and other laboratory data. Many studies looking for the ideal biomarker are underway, although progress is slow [9, 10].
Other imaging tests are needed to evaluate the state of various organs, detect complications and identify the location of the infection. These tests are usually X-rays, CT scans or ultrasounds.
Biomarkers of sepsis
What They Are and What They Are For
A biomarker is defined by the National Institutes of Health as “a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention” [11]. In various types of laboratory test, physicians use biomarkers for patient diagnosis and treatment. In clinical practice, biomarkers may also be used for diagnostic or prognostic purposes, or as an associate to treatment, to identify those who may benefit most from a specific therapy or to predict its efficacy or toxicity [12]. The use of biomarkers is on the rise and there is a high demand for new molecules able to identify sepsis and septic shock.
Sepsis can be divided into two sequential phases: first, an initial hyper-inflammatory phase characterized by SIRS, which may resolve; second, a subsequent immunosuppressive phase, usually characterized by organ dysfunction and commonly referred to as CARS (compensatory anti-inflammatory response syndrome). There are markers of both phases, although the markers of the hyper-inflammatory phase are more numerous.
Proinflammatory Biomarkers
C-Reactive Protein (CRP)
CRP is an acute-phase protein produced by the liver, although it can also be synthesized by other cells like alveolar macrophages. Its plasma concentration remains stable in healthy patients, but its levels increase after trauma, inflammation, and other stimuli related to tissue damage. Bacterial infections are powerful stimuli that produce a rapid rise in CRP levels in a few hours. Interleukin-6 (IL-6) is thought to be the main mediator stimulating the production of CRP, but other cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor alpha (TNF-α), also produce it. Changes in plasma levels of CRP may be useful in the diagnosis and prognosis of infection; a fall in plasma levels indicates infection resolution. Its short half-life of about 19 h makes CRP a useful tool in the monitoring of the inflammatory response, infection, and antibiotic therapy. In addition, CRP laboratory tests are less expensive than cytokine measurements [13].
In contrast to most acute-phase proteins which undergo large variations in plasma levels (depending on rates of synthesis, consumption and catabolism), CRP plasma levels remain almost constant. This means that they are determined solely by the rate of synthesis, and their values reflect the presence and scale of the disease. Certain studies have linked the number of organ failures in septic patients with the severity of the clinical condition and with the intensity of the inflammatory stimulus, finding a moderate relationship between CRP levels and the number of organ failures. The CRP plasma concentration appears to reflect the magnitude of the inflammatory stimulus and sepsis severity [14].
Isolated CRP values can be helpful in diagnosing sepsis. However, in clinical practice, serial measurements are more useful to monitor the patient’s response. CRP is quite unspecific and it does not differentiate sepsis from other diseases, but it is commonly used to screen for early onset neonatal sepsis (within the first 24 h of life) because its sensitivity has been shown to be very high [15]. This sensitivity is also high after surgery, and so it is also used to monitor patients in the post-operative process [16].
Procalcitonin (PCT)
Procalcitonin (PCT) is widely considered to be the most useful marker of severe systemic inflammation [17]. Procalcitonin is normally present in the blood at very low levels; however, its production can be stimulated by inflammatory cytokines and bacterial endotoxins, causing its release in greater quantities in response to infection, and, in particular, to systemic bacterial infections. Compared to all other currently available sepsis markers, PCT seems to also have potential for discriminating between infectious and non-infectious systemic inflammation in low-acuity patients [18]. It may also be able to differentiate between viral and bacterial infections and may indicate the presence of bacterial superinfection in patients with viral diseases [19].
Procalcitonin levels serve as a biomarker of inflammatory response, providing an indicator of risk of sepsis: the higher the level of PCT, the greater the likelihood of systemic infection and sepsis. Given its high sensitivity to most types of infections, procalcitonin is widely regarded as the most sensitive biomarker to help diagnose (or rule out) bacterial sepsis. Global guidelines also recommend its use as a tool to optimize antibiotic treatment.
Procalcitonin has a shorter half-life than CRP, and PCT levels rise sooner in cases of bacterial infection. These favorable kinetics may allow earlier diagnosis of sepsis and better monitoring of its progression.
Biomarkers of the Immunosuppressive Phase
The importance of CARS after the hyper-inflammatory phase of sepsis was recognized a long time ago, but it is only recently that several biomarkers of this phase have started to receive attention. Within this phase, assessment of human leukocyte antigen-D related (HLA-DR) expression in monocytes is producing good results.
The role of HLA class 2 molecules is to process and present antigenic peptide fragments to CD4 T lymphocytes at the onset of the immune response. The expression of HLA-DR on the cell surface is a significant indicator of the immune response due to its important role in antigen presentation. Several researchers have reported an association between decreased expression of HLA-DR and functional inactivation of monocytes, and have established that the decreased expression of HLA-DR may be a sign of severe immunosuppression (considering sepsis not as a proinflammatory disorder but as an immune disorder including inflammation and immunosuppression) [20,21,22]. Monocytes with low expression of HLA-DR have reduced ability to secrete cytokines and present antigens; therefore, maintaining HLA-DR expression may be essential for an appropriate antibacterial response and for the prevention of infectious complications. The monocyte rate decreases in septic patients and, therefore, HLA-DR expression is also lower in septic patients. However, this also happens when the immune system is weakened [23].
Biomarkers of Organ Dysfunction
Lactate
Lactate is the marker of hypoperfusion par excellence. Increases in serum lactate levels imply progression to organ dysfunction and are associated with an increased mortality rate from 35% to 70%. Hyperlactatemia is considered a severe sepsis marker, as it reflects poor tissue perfusion. Numerous studies have established the use of lactate as a marker for diagnosis, prognosis, and treatment of tissue hypoxia in shock. In general, the determination of lactate is an indisputable criterion in the risk stratification of septic patients and provides guidance on the use of vasoactive drugs. The magnitude of the lactatemia reflects the severity of hypoperfusion and is directly related to mortality. A patient with severe sepsis with significant hypoperfusion (lactate > 4 mmol/l) is considered to be in shock even without the necessary hypotension criteria. Therefore, there is enough evidence to state that normotensive patients with severe sepsis and significant lactic acidosis should receive early antibiotics, hemodynamic monitoring and adequate resuscitation [24, 25].
Lactate biokineticsare also used as a prognostic marker in sepsis. The absence of blood lactate clearance is an independent predictor of death. In septic processes, an elevated level of serum lactate may be due to altered clearance, overproduction or a combination of both, and so a high level of lactate may be a manifestation of organ dysfunction since this clearance depends on the liver and kidney function. Numerous studies have demonstrated the usefulness of lactate as a prognostic indicator of states of shock, and it has established itself in ICUs as a useful indicator of tissue hypoperfusion [26,27,28].
Venous to Arterial Carbon Dioxide Pressure Difference (ΔpCO2)
Anaerobic metabolism is crucial in the pathophysiology of septic shock, and lactate and ΔpCO2 are the tools used to monitor these patients. Carbon dioxide (CO2) is produced in tissues during aerobic and anaerobic metabolism. During aerobic metabolism, the amount of CO2 produced is determined by the basal metabolism and respiratory quotient. During anaerobic metabolism, CO2 is produced from the bicarbonate that buffers acidic metabolites.
Because CO2 is about 20 times more soluble than oxygen, it is likely to be available outside ischemic tissues to the venous stream, and so it is a very sensitive marker of hypoperfusion. Therefore, the measurement of ΔpCO2 seems to be a good marker for correct microcirculation and a good prognostic indicator in septic shock, as it provides an index of tissue oxygenation [28]. The ΔpCO2, whether from mixed or central venous blood, has been considered as a predictor of the capacity of the cardiovascular system to eliminate the CO2 produced in peripheral tissues [29]. Levels above 6 mmHg within the first 24 h in critically ill patients are associated with poor outcomes. However, the usefulness of this parameter remains to be explored [30].
MR-proADM
Adrenomedullin (ADM) is a 52-amino acid peptide that belongs to the same family as PCT. Quantification of ADM would be particularly useful for prognosis, but unfortunately it is impossible due to its rapid clearance from the blood (through the kidneys and lungs). Furthermore, it circulates bound to proteins, making it inaccessible to immunometric analysis. [31].The middle region of proadrenomedullin (MR-proADM), comprising amino acids 45–92, reflects the levels of active ADM (which is rapidly degraded), and can be identified in septic patients, as septic patients who die have higher concentrations of this molecule than those who survive. The prognostic value of MR-proADM tends to be superior to other biomarkers such as CRP and PCT, discriminating between sepsis and SIRS [32]. It has mainly been evaluated in community-acquired pneumonia (CAP) [33]. The level of MR-proADM at the time of admission to the ICU/ER is an early predictor of severity and poor outcome in severe sepsis and septic shock by CAP/respiratory tract infections, with an accuracy comparable to PSI and CURB-65 scores, and higher than other laboratory measurements such as PCT or CRP. During admission, it is also a predictor of evolution comparable to PCT and CRP and superior to other laboratory measurements. In combination with forecast scores, it would improve their ability to predict mortality in the short, medium and long term.
Other Biomarkers
Research has recently begun into other biomarkers like cell-free DNA (cf-DNA), but a great deal of work in this area remains to be done. cf-DNA basically comprises short fragments of DNA found in plasma and released from the cells due to necrosis or apoptosis. The interest in cf-DNA has recently increased and it is currently being investigated as a biomarker in critical patients. cf-DNA levels are higher in sepsis patients than in healthy controls and also in non-survivors. Cell death is a common event in sepsis but it is not sepsis-specific, so cf-DNA has been investigated as a prognostic biomarker.
In brief, the definition of sepsis is quite imprecise. It includes many signs and symptoms, which makes its determination difficult. A better understanding of the disease and the complex cellular processes that it involves is necessary in order to find the definitive marker or markers.
Studies of single biomarkers have shown that there is no ideal biomarker for sepsis. Due to the condition’s complex pathophysiology, efforts should be focused on investigating combinations of multiple biomarkers to obtain more reliable and specific results [34, 35].
Therapy
Septic shock is a serious state of tissue hypoperfusion triggered by a systemic inflammatory response of infectious origin with impaired microcirculation and cytopathic hypoxia, which involves intense hypovolemia, vasodilation and cardiac dysfunction [36, 37]. Despite therapeutic innovations, the mortality rate in septic shock remains high [38, 39]. The main causes of death in these patients are refractory multi-organ failure and hypotension. In septic shock, early initiation of treatment is crucial, since a delay may result in multiple organ dysfunction [40].
Given the high incidence, mortality rate and social impact of the condition, in 2002, the Surviving Sepsis Campaign (SSC) was set up to reduce sepsis-related mortality. The SSC proposed a series of care bundles organized in a protocol of early and simple goals [41, 42].
The first, named “the 3-h severe sepsis resuscitation bundle”, contains all the therapeutic steps to be performed within 3 h of the presentation of septic shock: measurement of lactate level, obtaining blood cultures before antibiotics, and administration of broad spectrum antibiotics and of crystalloid 30 ml/kg for hypotension or lactate ≥ 4 mmol/L. The second part, “the 6-h septic shock bundle”, contains all therapeutic steps to be performed within 6 h of the presentation with septic shock: application of vasopressors (for hypotension not responding to initial fluid replacement) in order to maintain a mean arterial pressure (MAP) ≥ 65 mmHg, measurement of central venous pressure (CVP) and venous oxyhemoglobin saturation (ScvO2) when hypotension persists despite volume replacement or initial lactate ≥ 4 mmol/L, and re-measurement of lactate if the initial level was high [42].
As for “the 24-h management bundle”, some substantial changes have been introduced in response to the proposals put forward in subsequent studies, such as raising the level of glucose to establish insulin infusion to 180 mg/dl, and the withdrawal of the administration of recombinant-activated protein C (APCr). Only the controversy of adjuvant steroid therapy persists, remaining an indication for refractory shock in addition to adequate fluid resuscitation and vasopressor administration [42].
Initial Treatment of Septic Patient: “Time is Life”
Early administration of broad-spectrum antibiotics and early, intense fluid intake are the basis for effective treatment of septic shock. Vasopressors, although generally necessary, should initially be regarded as a second-line treatment with clear criteria for their use, administration of inotropic drugs and transfusion of packed red blood cells.
Oxygen and Mechanical Ventilation
The administration of oxygen via a mask or early endotracheal intubation is recommended in order to optimize and reduce oxygen consumption, by the increased work of breathing. It is also recommended for the protection of the airway in the case of impaired consciousness [42].
Early Antibiotic Treatment
Distinguishing the infection origin is a priority, because it favors early antibiotic treatment and/or surgical control of the focus. Kumar et al. reported that every hour of delay in antibiotic administration was associated with a reduced survival of 7.6% [43]. A large retrospective study of 17,990 patients with sepsis and septic shock found that delay in first antibiotic administration was associated with increase in the risk of mortality for each hour delay in antibiotic administration [44]. One recent retrospective cohort study found that each hour until initial antimicrobial administration was associated with a 8.0% increase in progression to septic shock, and time to initial antimicrobial was also associated with in-hospital mortality [45]. Moreover, a recent systematic review and meta-analysis concluded that the association between timing of antibiotic administration and mortality in severe sepsis and septic shock found no significant mortality benefit of administering antibiotics within 3 h of emergency department triage or within 1 h of shock recognition in severe sepsis and septic shock [46].
Current standard of care is that antibiotics are recommended within the first 3 h if the patient comes from the emergency unit and 1 h if admitted to the ICU from another service. The antibiotic choice is essential in the patient’s prognosis, since inappropriate antibiotic therapy has been associated with increased mortality [47, 48].
The initial antibiotic administered should be broad spectrum, and it must be reevaluated when microbiological culture results become available in order to adjust the treatment and target it specifically against the microorganism isolated. The rational use of antibiotics minimizes side effects, the emergence of bacterial resistance [49,50,51], toxicity, and the risk of superinfection, and it also reduces treatment costs (Table 1).
Initial Treatment of Hypoperfusion
Hypotension is the first clinical sign of impaired perfusion, but it may coexist with normal levels of arterial pressure (AP) [52,53,54]. The plasma level of lactate, though non-specific, is the best indicator of tissue perfusion and persistence of high levels is an important predictor of severity and mortality [55]. Other clinical signs such as capillary refill in skin and nails, persistent skin mottling, oliguria or disorders of consciousness may also indicate perfusion disorder [56]. The mottling score is reproducible and easy to evaluate at the bedside. The mottling score as well as its variation during resuscitation is a strong predictor of 14-day survival in patients with septic shock. [57].
Lactate values, CVP, urine output and SvcO2 should be measured systematically in the early hours of hospital treatment of patients in septic shock, regardless of their location. CVP is the most common measurement, despite its limitations [58]. In a practical sense, in addition to providing a reference for preload and effective blood volume, measurements of CVP provide a “safety threshold pressure” in fluid intake in resuscitation, as excessive fluid intake may be associated with subsequent oxygenation problems [59], though not comparable to the problem of establishing high doses of vasopressors without completing the proper administration of fluids.
The amount of fluids and the time to improve perfusion in septic shock are not well established; the time may exceed 24 h since the onset of symptoms, and is independent of hemodynamic and metabolic components [60].
An arterial catheter must be inserted invasively to monitor the AP, because it is generally underestimated when it is assessed with an oscilloscope system [61]. But it is important to check frequently for system failures that can lead to errors in the AP and in parameters derived from pressure waves [62]. We should also stress that the channeling of the central and arterial lines should in no way delay the intake of fluids, blood cultures, analysis and antibiotic therapy.
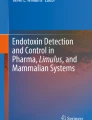
Several methods of continuous monitoring can be used which, together with echocardiography at bedside, help us to target treatment more precisely at late stages or when hypotension and respiratory failure id associated with normal lactate plasma levels [63, 64]. The pulmonary artery catheter should not be systematically used in septic shock patients because of the risk of increasing complications [65]. Figure 1 shows alternatives of hemodynamic monitoring according to the clinical situation of the patient in septic shock, based on personal experience of the authors.

Hemodynamic monitoring alternatives depending on the evolution and septic patient’s clinical status (in the authors’ practical experience). MAP mean arterial pressure, CVP central venous pressure, SvcO 2 central venous oxyhemoglobin saturation, ΔpCO 2 venous to arterial pCO2 difference, TT transthoracic, PiCOO pulse contour cardiac output
The rapid restoration of perfusion is achieved with the initial energetic fluid intake. Targets in hemodynamic patients are: MAP > 65 mmHg, CVP between 8 and 12, SvcO2 > 70%, lactate < 4 mmol/L and urine output > 0.5 mL/kg/h [42, 66, 67] (Fig. 2). The volume must be administered with crystalloid, although there is some debate about whether it should be saline solution 0.9% or Ringer-lactate solution because high amounts of saline can produce chloride overload. The total volume is variable, depending on the situation of each patient, but studies proposing 3–5 L in the first 3–6 h have produced good results [58].

Scheme of initial treatment of patients in septic shock. MAP mean arterial pressure, CVP central venous pressure, SvcO 2 central venous oxyhemoglobin saturation, VM mechanical ventilation, IAP intra-abdominal pressure, PiCOO pulse contour cardiac output, IC Immunocompromissed, CO cardiac output, CI cardiac index, PPV pulse pressure variation, SVV systolic volume variation, Ao aorta, Δ dynamics variables (systolic volume or pulse pressure variation)
Transfusion of Blood Products
Oxygen supply to the tissues depends on the level of hemoglobin. Transfusion is recommended in patients with severe sepsis when hemoglobin levels descend below 7 g/dL [42]. Critically ill patients generally have a better prognosis when blood transfusion is managed conservatively [66]. It is recommended that levels be kept between 7 and 9 g/dL, although this threshold rises in certain conditions such as myocardial ischemia, acute hemorrhage, refractory hypoxemia and lactic acidosis [42].
Treatment of Septic Patients in the Late Phase: Organ Dysfunction Support
After the first hours of septic shock, a late stage starts with a predominant presence of multi-organ dysfunction. AP is generally maintained with progressively higher doses of noradrenaline; less frequently, patients may present refractory hypotension, evolving to poor outcome [37, 67]. The addition of other vasoactive drugs to noradrenaline may be required (adrenaline, dobutamine or vasopressin). Indeed, adrenaline could be administered as rescue therapy in patients with refractory shock associated with low cardiac output as an alternative or in addition to noradrenaline [68].
This phase is characterized by a combination of cardiac dysfunction and respiratory and renal failures. In this respect, better control of hemodynamic parameters and more complex objectives are necessary; and close dynamic monitoring is required [63, 64, 69] (Figs. 1, 2).
Treatment during this phase involves specific organic support, mechanical ventilation, continuous hemofiltration, supply of blood products, and nutritional support. This means that a personalized therapeutic approach is necessary.
Adjunctive Measures
Corticosteroids
There is no evidence to support treatment with corticosteroids from the beginning of resuscitation or in patients with hemodynamically stable sepsis [70,71,72]. An ACTH test is not recommended. In patients with persistent shock after fluid challenge, who require high doses of vasoactive drugs and have not improved lactate levels in the first 6 h, the use of steroids may allow the withdrawal of vasoactive drugs. Although the evidence is limited, a combination of 200 mg of hydrocortisone followed by fludrocortisone seems to be the preferred option [42].
Control of Blood Glycemia
Hyperglycemia is toxic at the cellular level and may promote the development of organ failure in critically ill patients. There are many factors that cause the high incidence of hyperglycemia in these patients, especially in the most severe cases [73]. Hyperglycemia should be prevented by control of nutrition and triggers, and, if necessary, blood glucose can be contained using insulin infusion therapy [74]; it should be moderately demanding (< 180 mg/dL) to avoid hypoglycemia while maintaining levels around 140 mg/dL [42, 75]. Hypoglycemia is very detrimental in critically ill patients, is accompanied by increased mortality, and may counteract the favorable effect of glycemic control [76]. Glycemic variability is harmful and is associated with mortality, especially in patients with higher mean levels of blood sugar and even in non-diabetic patients, in whom cell damage is increased by hypoglycemia [77]. Fluctuating blood sugar levels are worse than stable, moderate hyperglycemia.
Other Measures
Like other critical patients, septic patients must undergo supportive measures such as mechanical ventilation, using ketamine rather than etomidate for intubation [78]. Mechanical ventilation with volumes of 6 ml per kg of ideal weight has been shown to decrease mortality in patients who develop acute respiratory distress syndrome (ARDS) [79]. It is recommended to maintain a plateau pressure below 30 cmH2O, and to use moderate positive end-expiratory pressure and the prone position in the case of ARDS [80]; recruitment maneuvers should only be used in patients with refractory hypoxemia and normalized preload [81, 82]. Other measures that should be mentioned are enteral nutrition, deep venous thrombosis prophylaxis and renal replacement therapy [42]. Continuous renal replacement therapies and intermittent hemodialysis are equivalent in patients with severe sepsis and acute renal failure.
Emerging Research Treatments: From the Visible to the Invisible
Mortality rates remain high despite the great efforts invested in implementing protocols. New emerging drugs focused on modifying the inflammatory response are currently being investigated for the treatment of septic shock [83, 84]. Immunomodulatory therapy for sepsis includes inflammatory cytokines, cellular receptors, nuclear transcription factors, coagulation activators and apoptosis regulators [85]. There are various therapies based on monoclonal antibodies that block inflammatory mediators and receptors, agents that block or eliminate bacterial products, modulators of immune function and immunostimulatory molecules. They have shown promising results in animal tests and are currently at various stages of clinical evaluation [86]. This is an approach based on the more modern concept of “precision” or “personalized” medicine [87, 88]. An example of “personalized medicine in sepsis management” is the potential benefit of beta blockers infusion in the subset of patients with tachycardia. Table 2 summarizes the main molecules studied.
Conclusion
In summary, sepsis remains a major health problem because of its high mortality and morbidity. Identification and early treatment is crucial in order to deliver prompt, correct treatment and increase the chances of survival. Currently, the diagnosis of sepsis focuses on the use of biomarkers. Progress in this field has been slow; most efforts have been centered on single markers, but, given the complexity of the sepsis response, the main focus should be on combinations of markers. The use of biomarkers in the future, using “omics” to individualize different subsets, will help improve the outcomes by improving diagnostic accuracy, reducing the time needed to identify the best treatment, and limiting unnecessary tests and treatments. Therapy remains based on source control, correct antibiotic prescription and supportive management. It is expected that the concept of precision medicine will establish itself as a way to identify subsets of patients able to benefit from individualized adjunctive therapy.
References
Novosad SA, Sapiano MRP, Grigg C, et al. Vital signs: epidemiology of sepsis: prevalence of health care factors and opportunities for prevention. Morb Mortal Wkly Rep. 2016;65(33):864–9.
Vincent J-L, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):1303–10.
Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801.
Kushimoto S, Gando S, Saitoh D, et al. The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis. Crit Care. 2013;17(6):R271.
Doerr F, Badreldin AM, Heldwein MB, et al. A comparative study of four intensive care outcome prediction models in cardiac surgery patients. J Cardiothorac Surg. 2011;6:21.
Minne L, Abu-Hanna A, deJonge E. Evaluation of SOFA-based models for predicting mortality in the ICU: A systematic review. Crit Care. 2008;12(6):R161.
Lee YI, Smith RL, Gartshteyn Y, Kwon S, Caraher EJ, Nolan A. Predictors of acute hemodynamic decompensation in early sepsis: an observational study. J Clin Med Res. 2016;8(8):575–81.
Lokhandwala S, Moskowitz A, Lawniczak R, Giberson T, Cocchi MN, Donnino MW. Disease heterogeneity and risk stratification in sepsis-related occult hypoperfusion: a retrospective cohort study. J Crit Care. 2015;30(3):531–6.
Faix JD. Biomarkers of sepsis. Crit Rev Clin Lab Sci. 2013;50(1):23–36.
Vincent J-L. The clinical challenge of sepsis identification and monitoring. PLoS Med. 2016;13(5):e1002022.
Atkinson AJ, Colburn WA, DeGruttola VG, et al. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;69(3):89–95.
Dupuy A-M, Philippart F, Péan Y, et al. Role of biomarkers in the management of antibiotic therapy: an expert panel review: I—currently available biomarkers for clinical use in acute infections. Ann Intensive Care. 2013;3(1):22.
Póvoa P, Coelho L, Almeida E, Fernandes A, Mealha R, Moreira P, et al. C-reactive protein as a marker of infection in critically ill patients. Clin Microbiol Infect. 2005;11:101–8.
Miglietta F, Faneschi ML, Lobreglio G, Palumbo CRA. Procalcitonin, C-reactive protein and serum lactate dehydrogenase in the diagnosis of bacterial sepsis, SIRS and systemic candidiasis. Le Infez Med. 2015;3:230–7.
Hofer N, Zacharias E, Müller W, Resch B. An update on the use of C-reactive protein in early-onset neonatal sepsis: current insights and new tasks. Neonatology. 2012;102:25–36.
Watt DG, Horgan PG, McMillan DC. Routine clinical markers of the magnitude of the systemic inflammatory response after elective operation: a systematic review. Surgery. 2015;157:362–80.
Riedel S, Melendez JH, An AT, Rosenbaum JE, Zenilman JM. Procalcitonin as a marker for the detection of bacteremia and sepsis in the emergency department. Am J Clin Pathol. 2011;135(2).
Harbarth S, Holeckova K, Froidevaux C, et al. Diagnostic value of procalcitonin, interleukin-6, and interleukin-8 in critically Ill patients admitted with suspected sepsis. Am J Respir Crit Care Med. 2001;164(3):396–402.
Ahn S, Kim WY, Kim S-H, et al. Role of procalcitonin and C-reactive protein in differentiation of mixed bacterial infection from 2009 H1N1 viral pneumonia. Influenza Other Respir Viruses. 2011;5(6):398–403.
Juskewitch JE, Abraham RS, League SC, et al. Monocyte HLA-DR expression and neutrophil CD64 expression as biomarkers of infection in critically ill neonates and infants. Pediatr Res. 2015;78(6):683–90.
Cazalis M-A, Friggeri A, Cavé L, et al. Decreased HLA-DR antigen-associated invariant chain (CD74) mRNA expression predicts mortality after septic shock. Crit Care. 2013;17(6):R287.
Vester H, Dargatz P, Huber-Wagner S, Biberthaler P, van Griensven M. HLA-DR expression on monocytes is decreased in polytraumatized patients. Eur J Med Res. 2015;20:84.
Das U. HLA-DR expression, cytokines and bioactive lipids in sepsis. Arch Med Sci. 2014;10(2):325–35.
Rhee C, Murphy MV, Li L, Platt R, Klompas M. Centers for disease control and prevention PreventionEpicenters Program. Lactate testing in suspected sepsis: trends and predictors of failure to measure levels. Crit Care Med. 2015;43(8):1669–76.
Holder AL, Gupta N, Lulaj E, et al. Predictors of early progression to severe sepsis or shock among emergency department patients with nonsevere sepsis. Int J Emerg Med. 2016;9(1):10.
Vincent J-L, Quintairos E, Silva A, Couto L, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20(1):257.
Bhat SR, Swenson KE, Francis MW, Wira CR. Lactate clearance predicts survival among patients in the emergency department with severe sepsis. West J Emerg Med. 2015;16(7):1118–26.
Bolvardi E, Malmir J, Reihani H, et al. The role of lactate clearance as a predictor of organ dysfunction and mortality in patients with severe sepsis. Mater Sociomed. 2016;28(1):57–60.
He H, Liu D, Long Y, et al. High central venous-to-arterial CO2 difference/arterial-central venous O2 difference ratio is associated with poor lactate clearance in septic patients after resuscitation. J Crit Care. 2016;31(1):76–81.
Naumann DN, Midwinter MJ, Hutchings S. Venous-to-arterial CO2 differences and the quest for bedside point-of-care monitoring to assess the microcirculation during shock. Ann Transl Med. 2016;4(2):37.
Henriquez-Camacho C, Losa J. Biomarkersfor sepsis. Biomed Res Int 2014:547818.
Christ-Crain M, Morgenthaler NG, Struck J, Harbarth S, Bergmann A, Müller B. Mid-regional pro-adrenomedullin as a prognostic marker in sepsis: an observational study. Crit Care. 2005;9(6):R816–24.
Liu D, Xie L, Zhao H, Liu X, Cao J. Prognostic value of mid-regional pro-adrenomedullin (MR-proADM) in patients with community-acquired pneumonia: a systematic review and meta-analysis. BMC Infect Dis. 2016;16:232.
Saukkonen K, Lakkisto P, Pettilä V, et al. Cell-free plasma DNA as a predictor of outcome in severe sepsis and septic shock. Clin Chem. 2008;54(6):1000–7.
Rhodes A, Wort SJ, Thomas H, Collinson P, Bennett ED. Plasma DNA concentration as a predictor of mortality and sepsis in critically ill patients. Crit Care. 2006;10(2):R60.
Harrois A, Huet O, Duranteau J. Alterations of mitochondrial function in sepsis and critical illness. Curr Opin Anaesthesiol. 2009;22:143.
Valenzuela Sánchez F, Bohollo de Austria R, Monge García I, Gil A. Shock séptico. Med Intensiva. 2005;29(3):192–200.
Kaukonen KM, Bailey M, Suzuki S, et al. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA. 2014;311:1308.
McPherson D, Griffiths C, Williams M et al. Sepsis-associated mortality in England: an analysis of multiple cause of death data from 2001 to 2010. BMJ Open 2013;3.
Blanco J, Muriel-Bombín A, Sagredo V, et al. Incidence, organ dysfunction and mortality in severe sepsis: a Spanish multicentre study. Crit Care. 2008;12:R158.
Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296.
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580.
Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–96.
Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42:1749.
Whiles BB, Deis AS, Simpson SQ. Increased time to initial antimicrobial administration is associated with progression to septic shock in severe sepsis patients. Crit Care Med. 2017;45:623–9.
Sterling SA, Miller WR, Pryor J, Puskarich MA, Jones AE. The impact of timing of antibiotics on outcomes in severe sepsis and septic shock: a systematic review and meta-analysis. Crit Care Med. 2015;43:1907–15.
Stephan Harbarth, Jorge Garbino, JéromePugin, Jacques A Romand, Daniel Lew, Didier Pittet Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003;115(7):529–535.
Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A, Jimenez-Jimenez FJ, Perez-Paredes C, Ortiz-Leyba C. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit Care Med. 2003;31(12):2742–51.
Mc Growan JE. Antimicrobial resistance in hospital organisms and its relation to antibiotic use. Rev Infect Dis. 1983;5:1033–48.
Kollef MH, Fraser VJ. Antibiotic resistance in the intensive care unit. Ann Intern Med. 2001;134:298–314.
Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med. 2010;38:1045.
Donnino MW, Nguyen B, Jacobsen G, Tomianovich M, Rivers E. Cryptic septic shock: a subanalysis of early, goal-directed therapy. Chest. 2003;124:90S-b.
Howell MD, Donnino M, Clardy P, Talmor D, Shapiro NI. Occult hypoperfusion and mortality in patients with suspected infection. Intensive Care Med. 2007;33:1892–9.
Puskarich MA, Trzeciak S, Shapiro NI, Heffner AC, Kline JA, Jones AE, Emergency Medicine Shock Research Network (EMSHOCKNET). Outcomes of patients undergoing early sepsis resuscitation for cryptic shock compared with overt shock. Resuscitation. 2011;82(10):1289–93.
Gu WJ, Zhang Z, Bakker J. Early lactate clearance-guided therapy in patients with sepsis: a meta-analysis with trial sequential analysis of randomized controlled trials. Intensive Care Med. 2015;41:1862–3.
Postelnicu R, Evans L. Monitoring of the physical exam in sepsis. Curr Opin Crit Care. 2017;23:232–6.
Ait-Oufella H, Lemoinne S, Boelle PY, et al. Mottling score predicts survival in septic shock. Intensive Care Med. 2011;37:801–7.
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzi A, Knoblich B, et al. Early goal-directed therapy in thetreatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–77.
Smith T, Grounds RM, Rhodes A. Central venous pressure: uses and limitations. In: Pinsky MR, Payen D, editors. Functional hemodynamic monitoring. Berlin: Springer; 2006. p. 99–110.
Ospina-Tascon G, Neves AP, Occhipinti G, Donadello K, Büchele G, Simion D, Chierego ML, Silva TO, Fonseca A, Vincent JL, De Backer D. Effects of fluids on microvascular perfusion in patients with severe sepsis. Intensive Care Med. 2010;36(6):949–55.
Farquhar IK. Continuous direct and indirect blood pressure measurement (Finapres) in the critically ill. Anaesthesia. 1991;46:1050.
Veremakis C, Holloran TH. The technique of monitoring arterial blood pressure. J CritIlln. 1989;4:82.
Richard JC, Bayle F, Bourdin G, Leray V, Debord S, Delannoy B, Stoian AC, Wallet F, Yonis H, Guerin C. Preload dependence indices to titrate volume expansion during septic shock: a randomized controlled trial. Crit Care. 2015;8(19):5. doi:10.1186/s13054-014-0734-3.
Monnet X, Rienzo M, Osman D, et al. Esophageal Doppler monitoring predicts fluid responsiveness in critically ill ventilated patients. Intensive Care Med. 2005;31:1195.
National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wheeler AP, Bernard GR, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med. 2006;354:2213.
Herbert P, Wells G, Blajchman M, Marshall J, Martin C, Pagliarello G, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Eng J Med. 1999;340:409–17.
Duraraj L, Schmidt G. Fluid therapy in resuscitated sepsis. Less is more. Chest. 2008;133:252–63.
Annane D, Vignon P, Renault A, Bollaert PE, Charpentier C, Martin C, et al. Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: a randomised trial. Lancet. 2007;370:676–84.
Pinsky MR, Payen D. Functional hemodynamic monitoring. Crit Care. 2005;9(6):566–72.
Boonen E, Vervenne H, Meersseman P, Andrew R, Mortier L, Declercq PE, Vanwijngaerden YM, Spriet I, Wouters PJ, Vander Perre S, Langouche L, Vanhorebeek I, Walker BR, Van den Berghe G. Reduced cortisol metabolism during critical illness. N Engl J Med. 2013;368:1477–88.
Casserly B, Gerlach H, Phillips GS, Lemeshow S, Marshall JC, Osborn TM, Levy MM. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38(12):1946–54.
Keh D, Trips E, Marx G, Wirtz SP, Abduljawwad E, Bercker S, et al. Effect of hydrocortisone on development of shock among patients with Severe sepsis: the HYPRESS randomized clinical trial. JAMA. 2016;. doi:10.1001/jama.2016.14799.
Nasraway SA. Hyperglycemia during critical illness. JPEN. 2006;30:254–8.
Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–67.
NICE-SUGAR Study Investigators for the Australian and New Zealand Intensive Care Society Clinical Trials Group and the Canadian Critical Care Trials Group, Finfer S, Chittock D, Li Y, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Hebert P, Henderson W, Heyland D, Higgins A, McArthur C, Mitchell I, Myburgh J, Robinson B, Ronco J. Intensive versus conventional glucose control in critically ill patients with traumatic brain injury: long-term follow-up of a subgroup of patients from the NICE-SUGAR study. Intensive Care Med. 2015;41(6):1037–47.
Vriesendorp TM, DeVries JH, van Santen S, et al. Evaluation of short-term consequences of hypoglycemia in an intensive care unit. Crit Care Med. 2006;34:2714–8.
Ali NA, O’Brien JM, Dungan K, et al. Glucose variability and mortality in patients with sepsis. Crit Care Med. 2008;36:2316–21.
Payen JF, Dupuis C, Trouve-Buisson T, et al. Corticosteroid after etomidate in critically ill patients: a randomized controlled trial. Crit Care Med. 2012;40:29.
The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–8.
Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159.
Fan E, Wilcox ME, Brower RG, et al. Recruitment maneuvers for acute lung injury: a systematic review. Am J Respir Crit Care Med. 2008;178:1156.
Hodgson C, Keating JL, Holland AE et al. Recruitment manoeuvres for adults with acute lung injury receiving mechanical ventilation. Cochrane Database Syst Rev 2009;CD006667.
Heming N, Lamothe L, Ambrosi X, Annane D. Emerging drugs for the treatment of sepsis. Expert Opin Emerg Drugs. 2016;21(1):27–37.
Annane D. Adjunctive treatment in septic shock: what’s next? Presse Med. 2016;45:105–9.
Christaki E, Anyfanti P, Opal SM. Immunomodulatory therapy for sepsis: an update. Expert Rev Anti Infect Ther. 2011;9(11):1013–33. doi:10.1586/eri.11.122.
Kotsaki A, Giamarellos-Bourboulis EJ. Emerging drugs for the treatment of sepsis. Expert OpinEmerg Drugs. 2012;17(3):379–91.
Rello J, Perez A. Precision medicine for the treatment of severe pneumonia in intensive care. Expert Rev Respir Med. 2016;10:297–316.
Rello J, Valenzuela-Sánchez F. Septic shock in the era of precision medicine. J Thorac Dis. 2016;. doi:10.21037/jtd.2016.03.83.
Opal SM, Laterre PF, Francois B, et al. Effect of eritoran, an antagonist of MD2TLR4, on mortality in patients with severe sepsis: the ACCESS randomized trial. JAMA. 2013;309:1154.
Rice TW, Wheeler AP, Bernard GR, et al. A randomized, doubleblind, placebocontrolled trial of TAK242 for the treatment of severe sepsis. Crit Care Med. 2010;38:1685.
Cruz DN, Antonelli M, Fumagalli R, et al. Early use of polymyxin B hemoperfusion in abdominal septic shock: the EUPHAS randomized controlled trial. JAMA. 2009;301:2445.
Schadler D, Brederlau J, Jorres A, Marx G, Meier Hellmann A, Putensen C, Quintel M, Spies C, Porzelius C, Engel C, Weiler N, Kuhlmann M. Extracorporeal cytokine hemoadsorption in patients with severe sepsis and acute lung injury. Am J Respir Crit Care Med, 2013;A5241.
Honore PM, Jacobs R, JoannesBoyau O, et al. Newly designed CRRT membranes for sepsis and SIRS a pragmatic approach for bedside intensivists summarizing the more recent advances: a systematic structured review. ASAIO J. 2013;59:99.
van Deuren M, Santman FW, van Dalen R, et al. Plasma and whole blood exchange in meningococcal sepsis. Clin Infect Dis. 1992;15:424.
Stegmayr BG. Plasmapheresis in severe sepsis or septic shock. Blood Purif. 1996;14:94.
Livigni S, Bertolini G, Rossi C, et al. Efficacy of coupled plasma filtration adsorption (CPFA) in patients with septic shock: a multicenter randomised controlled clinical trial. BMJ Open. 2014;4:e003536.
JoannesBoyau O, Honoré PM, Perez P, et al. Highvolumeversusstandardvolumehaemofiltration for septic shock patients with acute kidney injury (IVOIRE study): a multicentre randomized controlled trial. Intensive Care Med. 2013;39:1535.
Payen D, Mateo J, Cavaillon JM, et al. Impact of continuous venovenous hemofiltration on organ failure during the early phase of severe sepsis: a randomized controlled trial. Crit Care Med. 2009;37:803.
Desaki M, Takizawa H, Ohtoshi T, Kasama T, Kobayashi K, Sunazuka T. Ery- thromycin suppresses nuclear factor-kappaB and activator protein-1 activation in human bronchialepithelial cells. Biochem Biophys Res Commun. 2000;267:124–8. doi:10.1006/bbrc.1999.1917.
Kikuchi T, Hagiwara K, Honda Y, et al. Clarithromycin suppresses lipopolysaccharide-induced interleukin—8 production by human monocytes through AP-1 and NF-kappaB transcription factors. J Antimicrob Chemother. 2002;49:745–55. doi:10.1093/jac/dkf008.
Kanoh S, Rubin BK. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin Microbiol Rev. 2010;23:590–615.
Hsu BG, Lee RP, Yang FL, Harn HJ. ChenHI. Post-treatment with N- acetylcysteine ameliorates endotoxin shock-induced organ damage in conscious rats. Life Sci. 2006;79:2010–6. doi:10.1016/j.lfs.2006.06.040.
Döcke WD, Randow F, Syrbe U, et al. Monocyte deactivation in septic patients: restoration by IFN gamma treatment. Nat Med. 1997;3:678.
Laupland KB, Kirkpatrick AW, Delaney A. Polyclonal intravenous immunoglobulin for the treatment of severe sepsis and septic shock in critically ill adults: a systematic review and metaanalysis. Crit Care Med. 2007;35:2686.
Presneill JJ, Harris T, Stewart AG, et al. A randomized phase II trial of granulocyte macrophage colony stimulating factor therapy in severe sepsis with respiratory dysfunction. Am J Respir Crit Care Med. 2002;166:138.
Meisel C, Schefold JC, Pschowski R, et al. Granulocyte macrophage colony stimulating factor to reverse sepsis associated immunosuppression: a double blind, randomized, placebo controlled multicenter trial. Am J Respir Crit Care Med. 2009;180:640.
Bozza FA, Gomes RN, Japiassú AM, et al. Macrophage migration inhibitory factor levels correlate with fatal outcome in sepsis. Shock. 2004;22:309.
Arad G, Levy R, Hillman D, Kaempfer R. Superantigen antagonist protects against lethal shock and defines a new domain for T cell activation. Nat Med. 2000;6:414.
Zarychanski R, Doucette S, Fergusson D, et al. Early intravenous unfractionated heparin and mortality in septic shock. Crit Care Med. 2008;36:2973.
Yamakawa K, Aihara M, Ogura H, et al. Recombinant human soluble thrombomodulin in severe sepsis:a systematic review and metaanalysis. J Thromb Haemost. 2015;13:508.
Boeuf B, Gauvin F, Guerguerian AM, et al. Therapy of shock with naloxone: a metaanalysis. Crit Care Med. 1998;26:1910.
Staubach KH, Schröder J, Stüber F, et al. Effect of pentoxifylline in severe sepsis: results of a randomized, double blind, placebo controlled study. Arch Surg. 1998;133:94.
Tousoulis D, Psarros C, Demosthenous M, Patel R, Antoniades C, Stefanadis C. Innate and adaptive inflammation as a therapeutic target invascular disease: the emergingrole of statins. J Am Coll Cardiol. 2014;63:2491–502.
Vandermeer ML, Thomas AR, Kamimoto L, Reingold A, GershmanK Meek J, et al. Association between use of statins and mortality among patients hospitalized with laboratory-confirmed influenza virus infections: a multistate study. J Infect Dis. 2012;205:13–9. doi:10.1093/infdis/jir695.
Morelli A, Ertmer C, Westphal M, et al. Effect of heart rate control with esmolol on hemodynamic and clinical outcomes in patients with septic shock: a randomized clinical trial. JAMA. 2013;310:1683.
Morelli A, Singer M, Raieri VM, D’Egidio A, Mascia L, Orecchioni A, et al. Heart rate reduction with esmolol is associated with improved arterial elastance in patients with septic shock: a prospective observational study. Intensive Care Med. 2016;. doi:10.1007/s00134-016-4351-2.
Polito A, Parisini E, Ricci Z, Picardo S, Annane D. Vasopressin for treatment of vasodilatory shock: an ESICM systematic review and meta-analysis. Intensive Care Med. 2012;38:9–19.
Maybauer MO, Maybauer DM, Enkhbaatar P, Laporte R, Wiśniewska H, Traber LD, et al. The selective vasopressin type 1a receptor agonist selepressin (FE 202158) blocks vascular leak in ovine severe sepsis. Crit Care Med. 2014;42:e525–33.
Pavlov VA, Ochani M, Yang LH, Gallowitsch-Puerta M, Ochani K, Lin X, et al. Selective alpha7-nicotinic acetylcholine receptor ago- nist GTS-21 improves survival in murine endo- toxemia and severe sepsis. Crit Care Med. 2007;35:1139–44.
Venet F, Foray AP, Villars-Méchin A, Malcus C, Poitevin-Later F, et al. IL-7 restores lymphocyte functions in septic patients. J Immunol. 2012;189:5073–81.
Ostatin A, Paltsev A, Leplina O, Shevela Y, Chernykh H. The experience of surgical infec- tions treatment with extracorporalimmu-notherapy. Medicinskaya Immunol. 2000;2:43–51.
Li C, Bo L, Liu Q, Jin F. Thymosin alpha1 based immunomodulatory therapy for sepsis: a systematic review and meta-analysis. Int J Infect Dis. 2015;33:90–6.
Chang K, Svabek C, Vazquez-Guillamet C, Sato B, Rasche D, Wilson S, et al. Targeting the programmed cell death 1: programmed cell death ligand 1 pathway reverses T cell exhaustion in patients with sepsis. Crit Care. 2014;18:R3.
Cavaillon JM, Eisen D, Annane D. Is boosting the immune system in sepsis appropriate? Crit Care. 2014;18:216.
Kwak S, Ku SK, Kang H, Baek MC, Bae JS. Methylthiouracil, a new treatment option for sepsis. Vascul Pharmacol. 2015;. doi:10.1016/j.vph.2015.07.013.
Acknowledgments
Funding for the production of this manuscript was provided by CIBERES and FISS 14/01296, Instituto de Salud Carloos III, Madrid, Spain. No funding or sponsorship was received for the publication of this article. The authors would like to thank Mike Maudsley for the English language review. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole and have given final approval to the version to be published.
Disclosures
Jordi Rello has received grant support from ThermoFisher. Francisco Valenzuela has received grant support from ThermoFisher. Maria Ruiz and Silvia Moyano have nothing to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/51CCF06006068305.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Rello, J., Valenzuela-Sánchez, F., Ruiz-Rodriguez, M. et al. Sepsis: A Review of Advances in Management. Adv Ther 34, 2393–2411 (2017). https://doi.org/10.1007/s12325-017-0622-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-017-0622-8