
Abstract
Background
Poor glycemic control is associated with left ventricular (LV) dysfunction in patients with type 2 diabetes mellitus (T2DM). Nonetheless, the association between glycemic control and right ventricular (RV) function in T2DM has not been studied. This study aimed to evaluate the correlation between glycemic control and biventricular function and assess whether one ventricular function was mediated by the other ventricular changes using cardiac magnetic resonance.
Materials and methods
A total of 91 T2DM patients with normal ejection fraction were enrolled and divided into two groups according to glycated hemoglobin (HbA1c) with a cut off 7%. Twenty controls were included. Biventricular ventricular strain parameters, including global peak systolic radial strain, global peak systolic circumferential strain (GCS), global peak systolic longitudinal strain (GLS), peak diastolic radial strain rate (RSR), peak diastolic circumferential strain rate (CSR) and peak diastolic longitudinal strain rate (LSR) were measured.
Results
Compared with controls, patients with both HbA1c < 7% and HbA1c ≥ 7% showed significantly lower LVGCS, LVGLS, LVCSR, LVLSR, RVGLS, RVRSR, RVCSR and RVLSR. Patients with HbA1c ≥ 7% elicited significantly higher RVGCS than controls and lower LVGLS, LVCSR, LVLSR, RVGLS and RVLSR. Multivariable linear regression demonstrated that HbA1c was independently associated with LVGLS, LVLSR, RVGLS and RVLSR after adjustment for traditional risk factors. LV (RV) was not statistically mediated by the other ventricular alterations.
Conclusion
In T2DM patients, glycemic control was independently associated with impaired LV and RV systolic and diastolic function and these associations were not mediated by the other ventricular changes.
Key points
-
Biventricular strain decreased in T2DM patients with preserved EF.
-
Suboptimal glycemic control aggravated the deterioration of biventricular strain in T2DM patients.
-
HbA1c was independently associated with biventricular strain after adjustment for risk factors.
-
Relationship of HbA1c with LV or RV strain wasn’t mediated by the other ventricular.
Similar content being viewed by others


Introduction
It is estimated that there are currently 451 million people worldwide living with diabetes mellitus (DM), and it is expected to reach 650 million by 2045 [1]. Among people with DM, cardiovascular disease (CVD) is the leading cause of death, with a risk of death twice that of those without DM [2, 3]. Typically, left ventricular (LV) diastolic dysfunction is an early manifestation of DM-induced heart disease, followed by LV remodeling and systolic dysfunction, which could even lead to heart failure with the progression of DM [4,5,6]. Apart from the LV, several studies have proposed and confirmed that right ventricular (RV) morphology and function were also affected in DM [7, 8]. Besides, impaired RV structure and function was associated with increased risks of heart failure; RV function was shown to be a stronger predictor of mortality than LV function in heart failure with preserved ejection fraction (EF) [9]. Thus, early identification of biventricular subclinical dysfunction could facilitate earlier intervention and improves prognosis.
Cardiac magnetic resonance (CMR) imaging has emerged as the gold standard for non-invasive evaluation of biventricular structure and function in recent years [10]. The conventional measurement of ejection fraction (EF) could not evaluate myocardial regional function and is not sensitive for early myocardial systolic function impairment [10]. CMR-derived strain analysis using routinely cine sequence is an emerging modality which allows for early evaluation of global and regional subclinical myocardial dysfunction in longitudinal, circumferential, and radial directions. Myocardium consists of three layers: the inner oblique, the middle circular, and the outer oblique myocardial layers [11]. Longitudinal strain represents the longitudinal shortening of the cardiomyocytes from the base to the apex, and it is mostly determined by the longitudinally oriented myocardial fibers in the subendocardial layer [11]. Circumferential strain represents cardiomyocytes shortening along the LV circular perimeter in the shortaxis, and it is mostly influenced by circumferentially oriented muscle fibers in the midwall [11]. Radial strain represents myocardial thickening during systole toward the center of the ventricular cavity and it is influenced by full myocardial layers [11].
Factors contributing to myocardial impairment remain to be fully investigated and identifying the underlying mechanisms could help guide decision-making. It is recognized that chronic hyperglycemia could impair mitochondrial energy signaling and cause endothelial dysfunction, resulting in intra-endothelial accumulation of advanced glycated end products and increased myocardial oxidative stress, as well as cardiomyocyte hypertrophy, collagen deposition and cross-linking, all of which may lead to myocardial remodeling and dysfunction [12,13,14,15,16,17]. Additionally, several concepts suggest that ventricular interdependence may be an additional important determinant [18,19,20]. Previous studies have reported that poor glycemic control is associated with subclinical LV myocardial dysfunction and remodeling in patients with type 2 DM (T2DM) [21, 22]. However, the impact of glycemic control on the RV function has not been systematically investigated. Besides, it is not clear whether the influence of glycemic control on the LV (RV) is independent of the other ventricle.
Therefore, the present study aimed to evaluate the impact of glycemic control on biventricular myocardial function in T2DM patients with preserved ejection fraction (EF) using CMR imaging strain analysis. Moreover, we explored whether the association between glycemic control and LV (RV) variations was influenced by other ventricular changes.
Methods
Study population
Patients with T2DM who were submitted to CMR in the First Affiliated Hospital of Chengdu Medical College from January 2019 to July 2022 (as defined by the American Diabetes Association criteria [23]) were included in the study. Patients with myocardial infarction, known coronary artery disease, clinical symptoms of heart failure or angina, significant valvular disease (moderate to severe valvular stenosis or regurgitation), Corona Virus Disease (COVID) myocarditis, bundle branch block, atrial fibrillation, chronic lung disease, pulmonary hypertension, with LV ejection fraction (LVEF) < 50% on CMR, severe hepatic (Child-Turcotte-Pugh score ≥ 10) and renal dysfunction (estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73 m2) were excluded. Finally, a total of 91patients were enrolled. In the control group, 20 healthy individuals, age and sex-matched, with normal HbA1c and without diabetes or pre-diabetes diagnosis were enrolled. This retrospective study was in accordance with the principles of the Declaration of Helsinki and approved by the ethical committee of our institution.
Clinical measurements
Data on demographic and clinical information were obtained based on patient reports and medical records at the time of CMR. Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m). Body surface area (BSA) was computed as 0.0057 × height (cm) + 0.0121 × weight (kg) + 0.0882 for men and 0.0073 × height (cm) + 0.0127 × weight (kg)—0.2106 for women. Smoking history was defined as previous or current tobacco use. Family history of coronary artery disease (CAD) was collected. Hypertension was defined as a systolic and/or diastolic blood pressure ≥ 140 and/or 90 mmHg or the use of anti-hypertensive medication. Dyslipidemia was determined as total cholesterol (TC) > 200 mg/dl, low-density lipoprotein (LDL) ≥ 130 mg/dl and high-density lipoprotein (HDL) < 40 mg/dl for males or HDL < 50 mg/dl for females or the use of lipid-lowering medications. Fasting blood samples were acquired to measure biochemical indices such as fasting plasma glucose, glycated hemoglobin (HbA1c), TC, triglycerides, HDL and LDL. Estimated glomerular filtration rate (eGFR) was calculated based on the Modification of Diet in Renal Disease (MDRD) study equations [24]. Additionally, information regarding medications was also recorded.
Cardiac magnetic resonance protocol
CMR examinations were performed with a 1.5 T whole-body scanner (Siemens Avanto, Erlangen, Germany) in the supine position. Electrocardiography gating (ECG) and respiratory gating technique were applied to monitor dynamic changes during the entire scanning process. Data were recorded during the breath-holding period following the end of expiration. A standard balanced steady-state free precession (bSSFP) sequence was used to obtain two-, three- and four-chamber cine images in the long-axis view, as well as a stack of continuous cine images from the apex to the base in the short-axis view. Acquisition parameters were as follows: Repetition time (TR) = 3.2 ms, echo time (TE) = 1.6 ms, flip angle = 60°, pixel size = 2.4 × 1.4 mm. To exclude perfusion defection, rest first-pass perfusion images were acquired in three standard short-axis slices (basal, middle, and apical) with dynamic inversion recovery prepared echo-planar image sequencing. The acquisition parameters were: TR/TE: 187/1.0 ms, flip angle: 50°, slice thickness: 8 mm, and matrix size: 270 × 210. To rule out myocardial infarction, late gadolinium enhancement (LGE) images were acquired with segmented-turbo-FLASH–phase-sensitive inversion recovery (PSIR) sequence 10–15 min after contrast administration. The acquisition parameters were: TR/TE: 187/1.0 ms, flip angle: 50°, slice thickness: 8 mm, and matrix size: 270 × 210. T1 mapping and T2 mapping sequence examinations were not performed in this population.
Image analysis
CMR data were analyzed using commercial software (cvi42; Circle Cardiovascular Imaging Inc., Calgary, Alberta, Canada) by an experienced radiologist with more than three years of CMR experience. The endocardial and epicardial borders of the LV and RV myocardium on the short-axis cine images were manually traced at the end-diastolic and end-systolic phases; meanwhile, the papillary muscles and trabeculae were excluded in all series in the short-3D module. The biventricular structural and functional parameters were automatically computed, including mass, end-systolic volume (ESV), end-diastolic volume (EDV), stroke volume (SV) and EF. Mass, EDV, ESV indexed for BSA (MI, EDVI and ESVI) were calculated using the Mosteller formula [25]. Global LV and RV strain parameters analysis were performed by manually defining the endocardium and epicardium at the end-diastolic phase and automatically tracking myocardial voxel points on the short-axis, two- and four-chamber long-axis cine images. Both LV and RV strain indices included the global peak systolic radial strain (GRS), global peak systolic circumferential strain (GCS), global peak systolic longitudinal strain (GLS), peak diastolic radial strain rate (RSR), peak diastolic circumferential strain rate (CSR) and peak diastolic longitudinal strain rate (LSR).
Reproducibility
Intra- and inter-observer reproducibility for LV and RV strain variables was measured in 30 randomly selected patients. One investigator analyzed these patients on two separate measurements with 1-month interval to evaluate for intra-observer reproducibility. For inter-observer reproducibility, a second observer blinded to the clinical and CMR results independently measured LV and RV strain parameters.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation and median (25–75% interquartile range (IQR)) for normal distribution and non-normal distribution, respectively. Categorical data are expressed as numbers (percentages). Comparisons of baseline characteristics and biventricular structure and function parameters among groups were performed using one-way analysis of variance with the Bonferroni post-hoc correction, Kruskal–Wallis rank test or Chi squared test as appropriate. Univariable and multivariable linear regression analysis was performed to assess the association of HbA1c with LV and RV function. Model 1: unadjusted regression analysis. Model 2: adjusted for age, sex, BMI, diabetic duration, smoking, hypertension, dyslipidemia, hypoglycemic mediation, FBG, eGFR and LVMI/RVMI. Mediation analyses were performed to assess whether the changes in the structure and function of one ventricle statistically mediated the association between HbA1c and the function of the other ventricle after adjustment for traditional risk factors. Thus, we added these factors (RVEF, RVMI, RVGLS, RVLSR, LVEF, LVMI, LVGLS, LVLSR) to the aforementioned linear regression models. Both independent and joint mediation effects were presented as the relative change of the regression coefficient. The corresponding 95% confidence intervals were assessed according to Preacher and Hayes (10,000 bootstrap iterations) [26]. Multicollinearity was assessed by collinearity diagnostics (i.e., tolerance < 0.1 and/or variance inflation factor > 10). Intra-class correlation coefficients (ICC) were calculated to evaluate inter-observer and intra-observer reproducibility. All analyses were performed with the statistical software package SPSS version 22.0 (SPSS IBM Corporation, Armonk, NY, USA). A two-sided p value < 0.05 was considered statistically significant.
Results
Baseline characteristics
In total, 111 individuals (20 controls and 91 patients) were included in this study. These T2DM patients were divided into two subgroups according to HbA1c levels (< 7.0% and ≥ 7.0%) based on previous studies [22]. Table 1 demonstrates the demographic characteristics and clinical data of the total study population. Participants in the three groups were comparable in age, gender distribution and BMI. Compared with controls, patients with HbA1c < 7.0% had lower eGFR values (86.96 ± 20.95 ml/min/1.732 m2 vs. 100.61 ± 15.45 ml/min/1.732 m2, p < 0.05) but higher FBG (6.76 ± 1.40 mmol/L vs. 5.07 ± 0.61 mmol/L, p < 0.05) and HbA1c (5.99 ± 0.53% vs. 5.35 ± 0.63%, p < 0.05), whereas patients with HbA1c ≥ 7.0% had lower eGFR (78.41 ± 24.78 ml/min/1.732 m2 vs. 100.61 ± 15.45 ml/min/1.732 m2, p < 0.05) but higher FBG (8.73 ± 3.31 mmol/L vs. 5.07 ± 0.61 mmol/L, p < 0.05) and HbA1c (7.80 ± 1.22% vs. 5.35 ± 0.63%, p < 0.05). As compared with T2DM patients with HbA1c < 7.0%, patients with HbA1c ≥ 7.0% exhibited significantly higher FBG (8.73 ± 3.31 mmol/L vs. 6.76 ± 1.40 mmol/L, p < 0.05) and HbA1c (7.80 ± 1.22% vs. 5.99 ± 0.53%, p < 0.05). Out of the patients with HbA1c < 7.0%, a total of 16 (29%) patients reported a smoking history, 33 (60%) patients had hypertension, and 30 (55%) patients had dyslipidemia. Meanwhile out of the patients with HbA1c ≥ 7.0%, 11 (31%) patients described a smoking history, 20 (56%) patients had hypertension and 23 (64%) patients had dyslipidemia. With regard to cardiovascular complications, 4 (7%), 5 (9%), 5 (9%) and 9 (16%) patients with HbA1c < 7.0% had retinopathy, neuropathy, nephropathy and peripheral vascular disease, respectively. Furthermore, 3 (8%) patients had retinopathy and 4 (11%) patients had neuropathy and 4 (11%) patients had nephropathy and 7 (19%) had peripheral vascular disease in the group with HbA1c ≥ 7.0%. Medications for all patients are presented in Table 1.
CMR findings
Left ventricular mass index (LVMI) was higher in T2DM patients with HbA1c ≥ 7.0% than controls (61.72 ± 14.48 g/m2 vs. 52.30 ± 14.25 g/m2, p < 0.05). Regarding other LV functional and structural parameters, there were no significant difference among the three groups. By comparing LV strain parameters, regarding systolic function, patients with HbA1c < 7.0% had significantly lower LVGCS (− 19.05 ± 3.27% vs. − 22.87 ± 4.11%, p < 0.05) and LVGLS (− 18.41 ± 3.04% vs. − 22.89 ± 3.05%, p < 0.05) than controls. There were no significant differences in the LVEF and LVGRS between the patients with HbA1c < 7.0% and controls. Patients with HbA1c ≥ 7.0% had significantly lower LVGCS (− 18.27 ± 2.14% vs. − 18.84 ± 3.29%, p < 0.05) and LVGLS (− 16.72 ± 3.87% vs. 18.67 ± 2.97%, p < 0.05) compared with controls. LVEF and LVGRS were not significantly different between the patients with HbA1c ≥ 7.0% and controls. LVGLS (− 16.72 ± 3.87% vs. − 18.41 ± 3.04%, p < 0.05) was significantly lower in patients with HbA1c ≥ 7.0% than in patients with HbA1c < 7.0%. Patients in the two groups were similar in terms of LVEF, LVGRS and LVGCS. Concerning diastolic function, patients with HbA1c < 7.0% had significantly lower LVCSR (0.99 ± 0.26% vs. 1.36 ± 0.27%, p < 0.05) and LVLSR (1.10 ± 0.21% vs. 1.28 ± 0.26%, p < 0.05) than controls. No significant differences were observed in the LVRSR between the patients with HbA1c < 7.0% and controls. Patients with HbA1c ≥ 7.0% had significantly lower LVCSR (0.81 ± 0.24% vs. 1.36 ± 0.27%, p < 0.05) and LVLSR (0.94 ± 0.20% vs. 1.02 ± 0.22%, p < 0.05) compared with controls. Moreover, LVRSR values were not significantly different between patients with HbA1c ≥ 7.0% and controls. Whilst LVCSR (0.81 ± 0.24% vs. 0.99 ± 0.26%, p < 0.05) and LVLSR (0.94 ± 0.20% vs. 1.10 ± 0.21%, p < 0.05) were significantly lower in patients with HbA1c ≥ 7.0% than those with HbA1c < 7.0%. Patients in the two groups were comparable in terms of LVRSR.
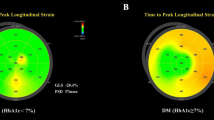
RVEDVI, RVESVI, RVSVI and RVEF were comparable among the three groups. By comparing RV strain parameters, regarding systolic function, patients with HbA1c < 7.0% had significantly lower RVGLS (− 18.50 ± 2.32% vs. − 21.46 ± 2.74%, p < 0.05) than controls. There were no significant differences in the RVEF, RVGRS and RVGCS between the patients with HbA1c < 7.0% and controls. Patients with HbA1c ≥ 7.0% had significantly lower RVGCS (− 18.60 ± 3.00% vs. − 20.03 ± 2.79%, p < 0.05) and RVGLS (− 17.09 ± 3.11% vs. − 21.46 ± 2.74%, p < 0.05) compared with controls. RVEF and RVGRS values were not significantly different between the patients with HbA1c ≥ 7.0% and controls. RVGLS (− 17.09 ± 3.11% vs. − 18.50 ± 2.32%, p < 0.05) was significantly lower in patients with HbA1c ≥ 7.0% than patients with HbA1c < 7.0%. Patients in the two groups were similar in terms of RVEF, RVGRS and RVGCS. Regarding diastolic function, patients with HbA1c < 7.0% had significantly lower RVRSR (− 1.81 ± 0.45% vs. − 2.65 ± 0.87%, p < 0.05), RVCSR (0.85 ± 0.23% vs. 1.19 ± 0.18%, p< 0.05) and RVLSR (0.87 ± 0.13% vs. 1.14 ± 0.18%, p < 0.05) than controls. Patients with HbA1c ≥ 7.0% had significantly lower RVRSR (− 1.44 ± 0.68% vs. − 2.65 ± 0.87%, p < 0.05), RVCSR (0.76 ± 0.26% vs. 1.19 ± 0.18%, p < 0.05) and RVLSR (0.75 ± 0.14% vs. 1.14 ± 0.18%, p < 0.05) compared with controls. RVLSR (0.75 ± 0.14% vs. 0.87 ± 0.13%, p < 0.05) was significantly lower in patients with HbA1c ≥ 7.0% than patients with HbA1c < 7.0%, but RVRSR and RVCSR were not significantly different between the two groups (Table 2). Figure 1 presented representative CMR cine images and CMR-derived peak strain curves in T2DM patients.

Representative CMR pseudocolor images and CMR-derived peak strain curves in T2DM patients. A, C: LV, RV pseudocolor images in short-axis; B, D: LV, RV global peak strain curve in circumferential direction; E, G: LV, RV pseudocolor images in horizontal 4-chamber long-axis; F, H: LV, RV global peak strain curves in longitudinal direction
Associations between HbA1c and LV and RV strain in patients with T2DM
Table 3 reported the relationship between LV strain and HbA1c in T2DM patients. Unadjusted univariable linear regression analysis demonstrated a statistically significant association between HbA1c and LVGCS [β (95%CI) = 0.32 (0.12,0.52), p = 0.002], LVGLS [β (95%CI) = 0.374 (0.18, 0.57), p < 0.001], LVRSR [β (95%CI) = 0.26 (− 0.05, 0.46), p = 0.014], LVCSR [β (95%CI) = − 0.23 (− 0.43, 0.02), p = 0.029] and LVLSR [β (95%CI) = − 0.40 (− 0.59, − 0.20), p < 0.001]. Multivariable linear regression analysis depicted an independent correlation between HbA1c and LVGLS [β (95%CI) = 0.27 (0.03, 0.51, p = 0.030)] and LVLSR [β (95%CI) = − 0.39 (− 0.67, − 0.11), p = 0.007] after adjustment for age, sex, BMI, diabetic duration, smoking, family history of CAD, hypertension, dyslipidemia, hypoglycemic mediation, FBG, eGFR and LVMI. Table 4 reported the relationship between RV strain and HbA1c in T2DM patients. Univariable linear regression analysis demonstrated that HbA1c was significantly associated with RVGLS [β (95%CI) = 0.59 (0.42, 0.76), p < 0.001], RVRSR [β (95%CI) = 0.29 (0.09, 0.49), p = 0.005], RVCSR [β (95%CI) = − 0.37 (− 0.56, − 0.17), p < 0.001] and RVLSR [β (95%CI) = − 0.45 (− 0.64, − 0.27), p < 0.001]. Multivariable linear regression analysis revealed that HbA1c was independently correlated with RVGLS [β (95%CI) = 0.56 (0.33, 0.80), p < 0.001] and RVLSR [β (95%CI) = − 0.39 (− 0.65, − 0.14), p = 0.003].
Mediation analysis
All mediation analyses were performed after adjustment for age, sex, BMI, diabetes duration, smoking, family history of CAD, hypertension, dyslipidemia, FBG, triglycerides, total cholesterol, high-density lipoprotein, low-density lipoprotein, eGFR and hypoglycemic therapy. The difference in LVGLS among patients with different levels of HbA1c was not mediated by RVMI, RVEF and RVGLS. The difference in LVLSR among patients with different levels of HbA1c was not mediated by RVMI, RVEF and RVLSR. Additionally, LVMI, LVEF and LVGLS had no significant mediating effects on RVGLS, and LVMI, LVEF and LVGLS showed no significant mediating effects on RVLSR (Additional file 1: Table S1).
Intra-observer and inter-observer reproducibility of LV and RV strain parameters
The intra-observer and inter-observer reproducibility of LV and RV strain and strain rate were considered good (all ICCs > 0.75). The intra-observer and inter-observer correlation coefficients are represented in Table 5. The reproducibility of LV strain parameters was excellent. The ICC values in the intra-observer analysis were 0.892 (95% CI 0.798–0.931), 0.923 (95% CI 0.831–0.964), 0.919 (95% CI 0.825–0.960), 0.907 (95% CI 0.793–0.946), 0.931 (95% CI 0.867–0.972) and 0.925 (95% CI 0.0.866–0.981) for LVGRS, LVGCS, LVGLS, LVRSR, LVCSR and LVLSR, respectively. The ICC values in the inter-observer analysis were 0.854 (95% CI 0.786–0.879), 0.901 (95% CI 0.807–0.952), 0.896 (95% CI 0.814–0.943), 0.864 (0.761–0.927), 0.907 (95% CI 0.802–0.952) and 0.899 (95% CI 0.796–0.956) for LVGRS, LVGCS, LVGLS, LVRSR, LVCSR and LVLSR, respectively. The reproducibility of RV strain parameters was good to excellent. The ICC values in the intra-observer analysis were 0.783 (95% CI 0.707–0.852), 0.875 (95% CI 0.757–0.936), 0.894 (95% CI 0.797–0.941), 0.797 (95% CI 0.713–0.874), 0.881 (95% CI 0.758–0.943), 0.903 (95% CI 0.804–0.951) for RVGRS, RVGCS, RVGLS, RVRSR, RVCSR and RVLSR, respectively. The ICC values in the inter-observer analysis were 0.751 (95% CI 0.691–0.836), 0.838 (95% CI 0.755–0.873), 0.865 (95% CI 0.759–0.916), 0.762 (95% CI 0.706–0.855), 0.869 (95% CI 0.773–0.919) and 0.886 (95% CI 0.779–0.937) for RVGRS, RVGCS, RVGLS, RVRSR, RVCSR and RVLSR, respectively.
Discussion
This study showed that the occurrence of decreased biventricular strain in T2DM patients with preserved EF compared with controls, and suboptimal glycemic control (HbA1c ≥ 7%) aggravated the deterioration of biventricular strain in T2DM patients. HbA1c was independently associated with LVGLS, LVLSR, RVGLS and RVLSR after adjustment for risk factors in T2DM patients. Additionally, the relationships between HbA1c and LV (RV) strain were not statistically mediated by parameters of the other ventricular structure, function and strain in this diabetic cohort.
The prevalence of heart failure in T2DM patients is 22% [27] and LV diastolic dysfunction is the initial manifestation of diabetic cardiac pathology [4, 28, 29]. Increasing investigations found the occurrence of subclinical LV systolic and diastolic dysfunction in T2DM patients and considered that the EF is not a good indicator of early LV functional impairment [7, 22]. CMR tissue tracking could sensitively and reliably detect the abnormalities of both systolic and diastolic function in T2DM [22, 30]. The underlying mechanism of myocardial dysfunction in T2DM is complicated and multicomponent. Recently, some studies considered that a chronic increase in blood glucose levels could impair LV function via various mechanisms, such as modification in mitochondrial energy metabolism, elevation in myocardial oxidative stress, activation of the endothelin system and the renin–angiotensin–aldosterone system (RAAS), and the production of advanced glycosylation end products (AGEs) resulting in the damage of cardiomyocytes and imbalances of calcium homeostasis [15, 16, 31, 32]. Previous studies revealed the adverse effects of hyperglycemia on LV systolic longitudinal and circumferential strain in asymptomatic T2DM and detrimental subclinical decline in LV circumferential strain in obese adolescents with dysglycemia, indicating the importance of blood glucose control [33, 34]. Thus, reasonable and standard glycemic control may help alleviate myocardial injury and subsequent potential cardiovascular events. The formation of HbA1c is slow, continuous and irreversible, depending on the ambient glucose concentration. HbA1c could reflect glycemic status in the past 8–12 weeks and has been proven to superiorly estimate mean glycemia than conventional measurements of blood glucose concentration [35,36,37,38,39]. Studies showed that an approximate 1% decline in HbA1c is coupled with a 16% decreased exposure to heart failure, and poor glycemic control at admission was associated with all-cause mortality and major adverse cardiovascular and cerebrovascular events [40, 41]. However, results from large randomized trials disputed the merits of intensive glycemic control and the concept that strengthening blood glucose control with uniformity should be substituted by individualized HbA1c goals as an ideal target is increasingly recognized [42, 43].
The present study found that T2DM patients with suboptimal glycemic control (HbA1c ≥ 7.0%) had significantly lower systolic and diastolic longitudinal strain than those with HbA1c < 7.0%. These results indicated that improvements in glycemic control were likely accompanied by significant amelioration in LV function, consistent with previous studies [22, 44]. Longitudinal myocardial fibers were predominantly positioned in the sub-endocardium, and the wall layer was most vulnerable to microvascular ischemia. LV longitudinal strain and strain rate decrease were considered as the major and earliest markers of preclinical DM-related cardiac dysfunction [30, 45]. Although it is not clear whether the duration and degree of glycemic control impairment induce cardiac dysfunction, it supports the conception that HbA1c < 7% may be important for cardiac health [46]. A recent study demonstrated that poor blood glucose control was an independent predictor of all directions of peak systolic strain and peak diastolic strain rate in Chinese T2DM patients with normal LVEF [22]. However, our study only revealed a significant association between glycemic control and LV subclinical systolic and diastolic dysfunction in the longitudinal direction instead of all directions, which is independent of risk factors in T2DM patients with preserved EF. One of the possible explanations for this discrepancy was the duration of diabetes in the study population, considering that the duration of diabetes in the present study was less than in Zhou et al.’ study, and the HbA1c level was lower in the present study, indicating that our study population was at an earlier stage of diabetes and strain analysis could sensitively detect early myocardial damage relative conventional parameters. Therefore, focusing on alterations in LV strain may facilitate the clinical management of T2DM patients with poor glycemic control to reduce cardiovascular disease risk and improve outcomes.
Recently, the emphasis on RV functional evaluation has attracted substantial attention and RV dysfunction was considered to be associated with adverse outcomes [27, 47]. Although some studies reported the association between RV dysfunction and diabetes [8], information on the role of HbA1c in RV function was scarce, and the topic remained largely unexplored, probably due to certain technical limitations. RV functional evaluation was generally challenging due to sophisticated geometry and motion. CMR is the gold standard for assessment of RV structure and function and CMR tissue tracking strain analysis could provide a more comprehensive and accurate assessment of RV global and regional function. Therefore, the present study further extended previous research and applied CMR tissue tracking to explore the effects of glycemic control on RV function in T2DM patients. Parallel to the findings in the LV, the results demonstrated that RV longitudinal strain and strain rate were significantly lower in patients with suboptimal glycemic control than optimal glycemic control although RVEF and structure were unaffected. Furthermore, glycemic control was significantly associated with RV longitudinal systolic and diastolic dysfunction in T2DM patients. A recent study also delineated the significant relationship between RV longitudinal strain and HbA1c [48]. One of the possible underlying mechanisms for this finding may be poor glycemic control and subsequent hyperglycemia and the formation of advanced glycation, which could exert detrimental effects on myocardial calcium handling, leading to RV contractile and relaxed impairment [49]. These findings probably emphasized the underlying mechanistic role of glycemic control in RV dysfunction, as well as the fact that poor glycemic control may indicate subclinical myocardial dysfunction in patients with T2DM.
The present study showed that the associations of HbA1c with LV and RV strain were not statistically mediated by other ventricular structure and function changes after adjustment for risk factors, suggesting that blood glucose control may produce direct effects on the myocardium that interacted independently with each other in both ventricles. Even though a parallel impact may exist on LV and RV function in diabetes, some comparable pathophysiological pathways may have divergent influences on RV and LV structure and function in diabetes, possibly in part due to the differences in LV and RV anatomy, compliance, and pressure [19, 20]. Further investigation is necessary to determine whether improving blood glucose control can ameliorate biventricular dysfunction.
Limitation
This research has several limitations. First, this is a retrospective single-center study with a relatively small sample size. Thus, our findings need to be further validated in multicenter studies with a larger population. Second, the cross-sectional design of the study cannot elucidate strong cause-and-effect associations. Third, the patients included in this study have a short diabetic duration, meaning that our findings may not necessarily be applicable to a wide range of diabetic patients, especially those with long-term diabetes. Fourth, clinical outcomes such as heart failure were not considered and evaluated in this study.
Conclusion
The present study revealed that plasma glucose control was associated with the LV and RV systolic and diastolic function in T2DM patients with normal LVEF, independently of other traditional cardiovascular risk factors. This correlation was not statistically mediated by other ventricular changes, suggesting that HbA1c affected both LV and RV function probably via direct myocardial involvement.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CSR:
-
Peak diastolic circumferential strain rate
- EDVI:
-
End-diastolic volume index
- EF:
-
Ejection fraction
- eGFR:
-
Estimated glomerular filtration rate
- ESVI:
-
End-systolic volume index
- FBG:
-
Fasting blood glucose
- GCS:
-
Global peak systolic circumferential strain
- GLS:
-
Global peak systolic longitudinal strain
- GRS:
-
Global peak systolic radial strain
- HbA1c:
-
Glycosylated hemoglobin
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- LSR:
-
Peak diastolic longitudinal strain rate
- LV:
-
Left ventricular
- MI:
-
Mass index
- RSR:
-
Peak diastolic radial strain rate
- RV:
-
Right ventricular
- SVI:
-
Stroke volume index
- T2DM:
-
Type 2 diabetes mellitus
References
Cho NH, Shaw JE, Karuranga S et al (2018) IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 138:271–281
Fox CS, Coady S, Sorlie PD et al (2007) Increasing cardiovascular disease burden due to diabetes mellitus: the Framingham heart study. Circulation 115(12):1544–1550
Preis SR, Hwang SJ, Coady S et al (2009) Trends in all-cause and cardiovascular disease mortality among women and men with and without diabetes mellitus in the Framingham heart study, 1950 to 2005. Circulation 119(13):1728–1735
von Bibra H, St John Sutton M (2010) Diastolic dysfunction in diabetes and the metabolic syndrome: promising potential for diagnosis and prognosis. Diabetologia 53(6):1033–1045
Stratmann B, Tschoepe D (2011) Heart in diabetes: not only a macrovascular disease. Diabetes Care 34(Suppl 2):S138-144
Sánchez-Barriga JJ, Rangel A, Castañeda R et al (2001) Left ventricular diastolic dysfunction secondary to hyperglycemia in patients with type II diabetes. Arch Med Res 32(1):44–47
Jensen MT, Fung K, Aung N et al (2019) Changes in cardiac morphology and function in individuals With diabetes mellitus: the UK biobank cardiovascular magnetic resonance substudy. Circ Cardiovasc Imaging 12(9):e009476
Hu BY, Wang J, Yang ZG et al (2019) Cardiac magnetic resonance feature tracking for quantifying right ventricular deformation in type 2 diabetes mellitus patients. Sci Rep 9(1):11148
Melenovsky V, Hwang SJ, Lin G et al (2014) Right heart dysfunction in heart failure with preserved ejection fraction. Eur Heart J 35(48):3452–3462
Seetharam K, Lerakis S (2019) Cardiac magnetic resonance imaging: the future is bright. F1000Res 8:1636
Muser D, Castro S, Santangeli P et al (2018) Clinical applications of feature-tracking cardiac magnetic resonance imaging. World J Cardiol 10(11):210–221
Feng B, Chen S, Chiu J et al (2008) Regulation of cardiomyocyte hypertrophy in diabetes at the transcriptional level. Am J Physiol Endocrinol Metab 294(6):E1119-1126
Monnier VM, Sell DR, Abdul-Karim FW et al (1988) Collagen browning and cross-linking are increased in chronic experimental hyperglycemia. Relev Diabetes Aging Diabetes 37(7):867–872
van Heerebeek L, Hamdani N, Handoko ML et al (2008) Diastolic stiffness of the failing diabetic heart: importance of fibrosis, advanced glycation end products, and myocyte resting tension. Circulation 117(1):43–51
Xie J, Cui K, Hao H et al (2016) Acute hyperglycemia suppresses left ventricular diastolic function and inhibits autophagic flux in mice under prohypertrophic stimulation. Cardiovasc Diabetol 15(1):136
Gao X, Xu Y, Xu B et al (2012) Allopurinol attenuates left ventricular dysfunction in rats with early stages of streptozotocin-induced diabetes. Diabetes Metab Res Rev 28(5):409–417
Domingueti CP, Dusse LM, Carvalho M et al (2016) Diabetes mellitus: the linkage between oxidative stress, inflammation, hypercoagulability and vascular complications. J Diabetes Complications 30(4):738–745
Haddad F, Doyle R, Murphy DJ et al (2008) Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation 117(13):1717–1731
Haddad F, Hunt SA, Rosenthal DN et al (2008) Right ventricular function in cardiovascular disease, part I: anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation 117(11):1436–1448
Sanz J, Sánchez-Quintana D, Bossone E et al (2019) Anatomy, function, and dysfunction of the right ventricle: JACC state-of-the-art review. J Am Coll Cardiol 73(12):1463–1482
Linssen PBC, Veugen MGJ, Henry RMA et al (2020) Associations of (pre)diabetes with right ventricular and atrial structure and function: the Maastricht Study. Cardiovasc Diabetol 19(1):88
Zhou FL, Deng MY, Deng LL et al (2021) Evaluation of the effects of glycated hemoglobin on cardiac function in patients with short-duration type 2 diabetes mellitus: a cardiovascular magnetic resonance study. Diabetes Res Clin Pract 178:108952
Classification and Diagnosis of Diabetes (2019) Standards of medical care in diabetes-2019. Diabetes Care 42(Suppl 1):S13-s28
Stevens LA, Coresh J, Greene T et al (2006) Assessing kidney function–measured and estimated glomerular filtration rate. N Engl J Med 354(23):2473–2483
Hundley WG, Bluemke DA, Finn JP et al (2010) ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American college of cardiology foundation task force on expert consensus documents. Circulation 121(22):2462–2508
Preacher KJ, Hayes AF (2008) Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods 40(3):879–891
Liu JH, Wu MZ, Li SM et al (2021) Association of serum uric acid with biventricular myocardial dysfunction in patients with type 2 diabetes mellitus. Nutr Metab Cardiovasc Dis 31(10):2912–2920
von Bibra H, Paulus WJ, St John Sutton M et al (2015) Quantification of diastolic dysfunction via the age dependence of diastolic function - impact of insulin resistance with and without type 2 diabetes. Int J Cardiol 182:368–374
Leung M, Wong VW, Hudson M et al (2016) Impact of Improved glycemic control on cardiac function in type 2 diabetes mellitus. Circ Cardiovasc Imaging 9(3):e003643
Chen Y, Zeng W, Chen W et al (2020) Evaluating the correlation of the impairment between skeletal muscle and heart using MRI in a spontaneous type 2 diabetes mellitus rhesus monkey model. Acta Diabetol 57(6):673–679
Oktay AA, Akturk HK, Esenboğa K et al (2018) Pathophysiology and prevention of heart disease in diabetes mellitus. Curr Probl Cardiol 43(3):68–110
Jia G, Hill MA, Sowers JR (2018) Diabetic cardiomyopathy: an update of mechanisms contributing to this clinical entity. Circ Res 122(4):624–638
Bogdanović J, Ašanin M, Krljanac G et al (2019) Impact of acute hyperglycemia on layer-specific left ventricular strain in asymptomatic diabetic patients: an analysis based on two-dimensional speckle tracking echocardiography. Cardiovasc Diabetol 18(1):68
Brar PC, Chun A, Fan X et al (2019) Impaired myocardial deformation and ventricular vascular coupling in obese adolescents with dysglycemia. Cardiovasc Diabetol 18(1):172
Ikeda M, Shimazawa R (2019) Challenges to hemoglobin A1c as a therapeutic target for type 2 diabetes mellitus. J Gen Fam Med 20(4):129–138
Sacks DB (2012) Measurement of hemoglobin A(1c): a new twist on the path to harmony. Diabetes Care 35(12):2674–2680
Cohen RM, Franco RS, Khera PK et al (2008) Red cell life span heterogeneity in hematologically normal people is sufficient to alter HbA1c. Blood 112(10):4284–4291
Singer DE, Coley CM, Samet JH et al (1989) Tests of glycemia in diabetes mellitus. Their use in establishing a diagnosis and in treatment. Ann Intern Med 110(2):125–137
Mortensen HB, Christophersen C (1983) Glucosylation of human haemoglobin a in red blood cells studied in vitro. Kinetics of the formation and dissociation of haemoglobin A1c. Clin Chim Acta 134(3):317–326
Iribarren C, Karter AJ, Go AS et al (2001) Glycemic control and heart failure among adult patients with diabetes. Circulation 103(22):2668–2673
Li Y, Li X, Zhang Y et al (2020) Impact of glycemic control status on patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention. BMC Cardiovasc Disord 20(1):36
Skyler JS, Bergenstal R, Bonow RO et al (2009) Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American diabetes association and a scientific statement of the American College of cardiology foundation and the American heart association. Diabetes Care 32(1):187–192
Seidu S, Achana FA, Gray LJ et al (2016) Effects of glucose-lowering and multifactorial interventions on cardiovascular and mortality outcomes: a meta-analysis of randomized control trials. Diabet Med 33(3):280–289
Kozakova M, Morizzo C, Fraser AG et al (2017) Impact of glycemic control on aortic stiffness, left ventricular mass and diastolic longitudinal function in type 2 diabetes mellitus. Cardiovasc Diabetol 16(1):78
Mochizuki Y, Tanaka H, Matsumoto K et al (2017) Impact of left ventricular longitudinal functional mechanics on the progression of diastolic function in diabetes mellitus. Int J Cardiovasc Imaging 33(12):1905–1914
Demmer RT, Allison MA, Cai J et al (2016) Association of impaired glucose regulation and insulin resistance with cardiac structure and function: results from ECHO-SOL (echocardiographic study of latinos). Circ Cardiovasc Imaging 9:10
Lejeune S, Roy C, Ciocea V et al (2020) Right ventricular global longitudinal strain and outcomes in heart failure with preserved ejection fraction. J Am Soc Echocardiogr 33(8):973-984.e972
Kosmala W, Przewlocka-Kosmala M, Mazurek W (2007) Subclinical right ventricular dysfunction in diabetes mellitus–an ultrasonic strain/strain rate study. Diabet Med 24(6):656–663
Kang Y, Wang S, Huang J et al (2019) Right ventricular dysfunction and remodeling in diabetic cardiomyopathy. Am J Physiol Heart Circ Physiol 316(1):H113-h122
Funding
None.
Author information
Authors and Affiliations
Contributions
JZ designed research, wrote the paper, reviewed the paper, gave input to improve the paper, read and approved the final manuscript. WL collected data, measured imaging parameters, performed research, wrote the paper. FC revised and improved the paper. ZX reviewed and analyzed data, performed the data interpretation. KZ measured imaging parameters. RH revised the paper, reviewed the paper, gave input to improve the paper and approved the final manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of our Hospital, Chengdu Medical College The First Affiliated Hospital (Chengdu, Sichuan, China) with a waiver of informed consent due to the retrospective nature of this investigation.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Mediation analyses: cardiac magnetic resonance biventricular strain analysis in diabetic patients. All analyses were adjusted for age, sex, BMI, diabetic duration, smoking, family history of CAD, hypertension, dyslipidemia, fasting blood glucose, triglycerides, total cholesterol, high-density lipoprotein, low-density lipoprotein, eGFR and hypoglycemic therapy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhu, J., Li, W., Chen, F. et al. Impact of glycemic control on biventricular function in patients with type 2 diabetes mellitus: a cardiac magnetic resonance tissue tracking study. Insights Imaging 14, 7 (2023). https://doi.org/10.1186/s13244-022-01357-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-022-01357-7