
Abstract
Backgrounds
The role of right ventricular (RV) and atrial (RA) structure and function, in the increased heart failure risk in (pre)diabetes is incompletely understood. The purpose of this study is to investigate the associations between (pre)diabetes and RV and RA structure and function, and whether these are mediated by left ventricular (LV) alterations or pulmonary pressure.
Methods
Participants of the Maastricht Study; a population-based cohort study (426 normal glucose metabolism (NGM), 142 prediabetes, 224 diabetes), underwent two-dimensional and tissue Doppler echocardiography. Multiple linear regression analyses with pairwise comparisons of (pre)diabetes versus NGM, adjusted for cardiovascular risk factors, and mediation analyses were used.
Results
In general, differences were small. Nevertheless, in individuals with prediabetes and diabetes compared to NGM; RA volume index was lower (both p < 0.01, ptrend < 0.01), RV diameter was lower (both p < 0.01, ptrend < 0.01) and RV length was significantly smaller in diabetes (p = 0.67 and p = 0.03 respectively, ptrend = 0.04), TDI S′RV was lower (p = 0.08 and p < 0.01 respectively, ptrend < 0.01), TDI E′RV was lower (p = 0.01 and p = 0.02 respectively, ptrend = 0.01) and TDI A′RV was lower (p < 0.01 and p = 0.07 respectively, ptrend = 0.04). Only the differences in RA volume index (7.8%) and RV diameter (6.2%) were mediated by the maximum tricuspid gradient, but no other LV structure and function measurements.
Conclusions
(Pre)diabetes is associated with structural RA and RV changes, and impaired RV systolic and diastolic function, independent of cardiovascular risk factors. These associations were largely not mediated by indices of LV structure, LV function or pulmonary pressure. This suggests that (pre)diabetes affects RA and RV structure and function due to direct myocardial involvement.
Similar content being viewed by others


Background
The role of right ventricular (RV) structure and function in the increased risk of heart failure in patients with type 2 diabetes (T2DM) [1] and prediabetes [2] is incompletely understood [3,4,5] but may be important. Indeed, in a population free of overt cardiovascular disease [6], Kawut et al. showed that RV (independent of left ventricular (LV)) mass was associated with increased risk of heart failure. In another study [7], in heart failure patients, RV function was a stronger predictor of mortality than LV function.
In (pre)diabetes, parallel effects on RV and LV structure and function may occur through direct myocardial effects (e.g. fibrosis, oxidative stress, altered calcium homeostasis and substrate metabolism) [8,9,10]; through indirect effects via alterations in vascular function (e.g. arterial stiffening and microvascular dysfunction) [11]; and (or) through ventricular interdependence (i.e. structure, compliance, and function of the one ventricle, through direct mechanical interaction via septal wall and pericardium, may affect structure and function of the other ventricle) [3,4,5].
Associations of (pre)diabetes with RV structure and function have not been systematically investigated [9, 11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27]. Previous studies in general have been performed in selected and small populations (with type 1 diabetes [12, 14, 17, 25], in outpatient clinics [9, 12,13,14,15,16,17, 21,22,23, 25,26,27], with heart failure [24], with pulmonary hypertension [11], and (or) with less than 150 participants [12, 14,15,16,17,18, 20, 22, 24,25,26,27]), have not been adjusted for potential confounders [12, 14,15,16,17, 20, 22, 23, 25, 26], and have not investigated the role of prediabetes [11, 12, 14,15,16,17,18, 20,21,22,23,24,25,26]. In the population-based MESA study [19], (pre)diabetes was associated with lower RV mass and smaller RV volume, but not with RV systolic function, while RV diastolic function was not assessed.
In view of these considerations, we assessed associations between (pre)diabetes and RV and LV structure and function in the population-based Maastricht Study. In addition, we tested the hypothesis that RV alterations in (pre)diabetes are mediated by LV alterations and (or) pulmonary pressure.
Methods
Study population
We used data from The Maastricht Study, an observational prospective population-based cohort study. The rationale and methodology have been described previously [28]. In brief, the study focuses on the etiology, pathophysiology, complications and comorbidities of T2DM and is characterized by an extensive phenotyping approach. Eligible for participation were all individuals aged between 40 and 75 years and living in the southern part of the Netherlands. Participants were recruited through mass media campaigns and from the municipal registries and the regional Diabetes Patient Registry via mailings. Recruitment was stratified according to known T2DM status, with an oversampling of individuals with T2DM, for reasons of efficiency. The present report includes cross-sectional data from the first 866 participants, who completed the baseline survey between November 2010 and March 2012. To augment statistical power, another random sample of 218 participants was added, who had completed the baseline survey between April 2012 and April 2013. The examinations of each participant were performed within a time window of three months. Patients with type 1 diabetes mellitus or a paced heart rhythm were excluded. The study has been approved by the institutional medical ethical committee (NL31329.068.10) and the Minister of Health, Welfare and Sports of the Netherlands (Permit 131088-105234-PG). All participants gave written informed consent.
Glucose metabolism status
To determine glucose metabolism status, all participants (except those who used insulin) underwent a standardized 2-h 75 g oral glucose tolerance test after an overnight fast. For safety reasons, participants with a fasting glucose level above 11.0 mmol/L, as determined by a finger prick, did not undergo the oral glucose tolerance test. For these individuals, fasting glucose level and information about diabetes medication were used to determine glucose metabolism status. Glucose metabolism status was defined according to the WHO 2006 criteria into normal glucose metabolism (NGM), impaired fasting glucose, impaired glucose tolerance (combined as prediabetes), and T2DM [29].
Echocardiography
Echocardiograms were obtained according to a standardized protocol consisting of two-dimensional, M-mode, color flow Doppler, pulsed and continuous wave Doppler and Tissue Doppler recordings (TDI) with use of echo equipment (Vivid E9 with 2.5-3.5 MHz and 4 V transducer, GE Vingmed). All recordings were digitally stored and analyzed off-line (EchoPAC PC, version 112) by four researchers blinded to (pre)diabetes status. Details on echocardiographical procedures are provided in Additional file 1.
Covariates
Office blood pressure (Omron 705IT, Omron, Japan) and ambulatory 24 h blood pressure (WatchBP O3, Microlife AG, Switzerland) were measured as described elsewhere [28]. Fasting serum concentrations of total cholesterol, high density lipoprotein (HDL) cholesterol, triglycerides and creatinine were measured (Beckman Synchron LX20, Beckman Coulter inc., Brea USA) [28]. Cystatin C was measured by a particle enhanced immunoturbidimetric assay (Roche Cobas 8000, Roche diagnostics, Basel, Switzerland). Estimated glomerular filtration rate (eGFR) was estimated according to the Chronic Kidney Disease Epidemiology Collaboration equation based on both serum creatinine and serum cystatin C [30]. Albuminuria, defined as an urinary albumin excretion ≥ 30 mg/24 h, was determined (twice) as described elsewhere [31]. Antihypertensive, lipid-modifying, and glucose-lowering medication use were assessed with a medication interview [28]. Renin-angiotensin system modifying agents were defined angiotensin converting enzyme inhibitors, angiotensin II inhibitors and (or) renin inhibitors use. Waist circumference was measured midway between the lower rib margin and the iliac crest end-expiratory. Alcohol consumption, smoking status (never, former, current), prevalent cardiovascular disease and physical activity were determined by questionnaire [28]. Alcohol consumption was categorized into non-consumers, low-consumers (≤ 7 and ≤ 14 glasses per week for females and males respectively) and high-consumers (> 7 and > 14 glasses per week for females and males respectively). Total and moderate to vigorous physical activity was assessed by a modified version of the Community Healthy Activities Model Program for Seniors (CHAMPS) questionnaire [32]. Prevalent cardiovascular disease was defined as a self-reported history of myocardial infarction, or cerebrovascular infarction or hemorrhage, or percutaneous artery angioplasty of, or vascular surgery of the coronary, abdominal, peripheral or carotid arteries. Other clinical characteristics (i.e. body mass index, waist-to-hip ratio, presence of hypertension, and HbA1c) were obtained from physical examination and laboratory assessment as described elsewhere [28].
Statistical analyses
All analyses were performed with the statistical software package SPSS version 21.0 (SPSS IBM Corporation, Armonk, NY, USA). Descriptive statistics are presented as mean (± standard deviation), or in case of a skewed distribution as median [interquartile range] or frequencies (percentages). Variables with a skewed distribution were natural-log-transformed in order to meet normality criteria. Comparisons of population characteristics between groups were made by use of independent T-test or Chi squared test as appropriate. Dependent variables were standardized into sex specific Z-scores (individual value-meansex)/(standard deviationsex). As sex had a skewed distribution in categories of glucose metabolism status, sex-specific means and standard deviations of the NGM group were used. Multiple linear regression analyses, both linear trend analyses and pairwise comparisons of prediabetes or T2DM versus NGM respectively (with dummy variables), were used to determine associations of (pre)diabetes with RA volume index, RV structure (i.e. RV diameter, RV length), and RV functions (i.e. TDI S’RV, TDI E’RV, TDI A’RV, TDI E′/A′ratio, RV myocardial performance index). Model 1 was adjusted for age; model 2 was additionally adjusted for cardiovascular risk factors associated with RV structure and functioning [19, 33] (i.e. systolic blood pressure, antihypertensive medication use, smoking status, prior cardiovascular disease, and waist circumference); and model 3 was additionally adjusted for albuminuria, eGFR, total to high density lipoprotein cholesterol ratio, triglycerides, and the use of lipid-modifying medication. Mediation analyses was performed to assess the extent to which ventricular interdependence and pulmonary hypertension statistically mediated the association between (pre)diabetes and RV structure and function. Hence, we added these factors (i.e. LV mass index, peak flow velocity E/longitudinal velocities E ratio, LV ejection fraction, maximum gradient of the tricuspid valve) to the aforementioned regression models. Both independent and joint mediation effects were expressed as the (relative) change of the regression coefficient. The corresponding 95% confidence intervals were assessed according to Preacher and Hayes (10,000 bootstrap iterations) [34]. Multicollinearity was assessed by collinearity diagnostics (i.e. tolerance < 0.1 and/or variance inflation factor > 10). A two-sided P-value < 0.05 was considered statistically significant, except for interaction analyses, where P < 0.10 was used.
Results
Study population
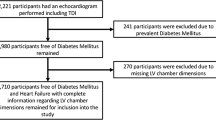
Of the 1084 participants, echocardiography was obtained in 933 individuals. Participants were excluded due to exclusion criteria (n = 7), missing covariates (n = 72), and missing two-dimensional (n = 57) or TDI (n = 101) echocardiographic analyses, resulting in 792 and 748 participants eligible for current analyses respectively (Fig. 1). Individuals with missing data more frequently had T2DM; however, within strata of (pre)diabetes, these individuals were largely comparable (Additional file 2: Table S1).

Selection of study population. HDL high density lipoprotein, RA right atrium, RV right ventricle, 2D two-dimensional, LV left ventricle, TDI tissue Doppler imaging
Characteristics
Characteristics of the total study population and stratified according to (pre)diabetes are given in Tables 1, 2 and Additional file 2: Table S2. Participants with (pre)diabetes had a worse cardiovascular risk profile; they were older and more often men, had a higher body mass index, greater waist circumference, higher blood pressure, lower HDL, higher triglycerides, lower eGFR, and less physical activity. They also more frequently had prior cardiovascular disease, hypertension and albuminuria, and more often used antihypertensive and lipid-modifying medication (Table 1, Additional file 2: Table S2).
Participants with (pre)diabetes had lower LV end diastolic volume index, higher LVMI, worse LV systolic function, and worse LV diastolic function (lower E/A ratio, higher E/E′-ratio averaged, more frequent abnormal diastolic function grade). In addition, they had lower RA volumes, worse RV systolic function, and worse RV diastolic function (lower E/A ratio of the tricuspid valve, lower E′RV). Participants with (pre)diabetes more often had wall motion abnormalities (Table 2).
Associations between (pre)diabetes and RA and RV structure and function
RA volume index was lower in individuals with prediabetes and T2DM compared to NGM (p < 0.01 and p < 0.01 respectively, p for trend < 0.01; Table 3). Adjustment for potential confounders of models 2 and 3 attenuated the difference in RA volume index, although the association remained statistically significant (p < 0.01 and p < 0.01 respectively, p for trend < 0.01).
RV diameter was lower in individuals with prediabetes and T2DM compared to NGM (p = 0.24 and p = 0.02 respectively, p for trend 0.02; Table 3). Adjustment for potential confounders of models 2 and 3 strengthened the difference in RV diameter (p < 0.01 and p < 0.01 respectively, p for trend < 0.01). RV length was not significantly different in individuals with prediabetes and T2DM compared to NGM (p = 0.12 and p = 0.07, p for trend 0.06); however, after adjustment for potential confounders, RV length was not different in prediabetes but significantly smaller in T2DM compared to NGM (p = 0.67 and p = 0.03 respectively, p for trend = 0.04).
TDI S′RV was lower in individuals with prediabetes and T2DM compared to NGM (p = 0.08 and p < 0.01 respectively, p for trend < 0.01; Table 3). Adjustment for potential confounders had no effect on this difference.
Both TDI E′RV and A′RV were lower in individuals with prediabetes and T2DM compared to NGM (for both measurements p < 0.01 and p < 0.01 respectively, p for trend < 0.01; Table 3). Adjustment for potential confounders attenuated these differences, although the association remained significant in TDI E′RV (p = 0.01 and p = 0.02 respectively, p for trend = 0.01) and (borderline) significant in A′RV (p < 0.01 and p = 0.07 respectively, p for trend = 0.04). TDI RV E′/A′ ratio was not significantly different in individuals with prediabetes and T2DM compared to NGM (p = 0.84 and p = 0.38 respectively, p for trend = 0.39), nor after full adjustment (p = 0.85 and p = 0.49 respectively, p for trend 0.50).
The RV myocardial performance index was not significantly different in individuals with prediabetes and T2DM compared to NGM (p = 0.71 and p = 0.65 respectively, p for trend = 0.63; Table 3), nor after full adjustment (p = 0.34 and p = 0.12 respectively, p for trend 0.12).
Mediation
The difference in RA volume index between individuals with T2DM and those with NGM was partly mediated by the maximum gradient of the tricuspid valve (statistical mediating effect 7.8%, bootstrapped 95% CI 0.1–20.1%; Fig. 2); E/E′, LVMI, or LVEF had no significant mediating effects. The difference in RV diameter between individuals with T2DM and those with NGM was partly mediated by the maximum gradient of the tricuspid valve (statistical mediating effect 6.2%, bootstrapped 95% CI 0.3–16.4%); E/E′, LVMI, or LVEF had no significant mediating effects. Differences in RV length, S′RV, E′RV, or A′RV between individuals with T2DM and those with NGM were not significantly mediated by the maximum gradient of the tricuspid valve, E/E′, LVMI, or LVEF (Additional file 2: Table S3a, b).

Mediating effects. Mediating effects are presented as indirect effects of T2DM on RV structure and function (absolute effect on left Y-axis, relative effect in percentages on right Y-axis) through potential mediators. All analyses are adjusted for age, office systolic blood pressure, antihypertensive medication, smoking status, prior cardiovascular disease, waist circumference albuminuria, eGFR, total to high density lipoprotein cholesterol ratio, triglycerides, the use of lipid-modifying medication. RV right ventricle, RA right atrium, LVMI left ventricular mass index, E/E′ peak flow velocity E/longitudinal velocities E ratio, LVEF left ventricular ejection fraction, TR max grad maximum gradient of the tricuspid valve
Additional analyses
In the associations of (pre)diates with RV and RA structure and function, no interaction between (pre)diabetes and sex was observed. Furthermore, in these associations no interaction between (pre)diabetes and age was observed except for the RV E′/A′ (p-interaction = 0.01); the difference between individuals with T2DM and NGM was greater in the youngest compared to the oldest; however, both differences were not statistically significant (data not shown). The results of statistical analyses did not materially change when these were repeated on those with full echocardiographic data (mediators included); when office systolic blood pressure was replaced by ambulatory 24-h systolic blood pressure; when analyses were additionally adjusted for renin-angiotensin system modifying agents or moderate to vigorous physical activity; or subjects were excluded with atrial fibrillation, wall motion abnormalities, significant valvular pathology, and prior cardiovascular disease (Additional file 2: Table S4a–e).
Discussion
This study shows that both prediabetes and T2DM are associated with structural RA and RV changes, and impaired RV systolic and diastolic function, and that these associations are independent of other traditional cardiovascular risk factors. The associations between (pre)diabetes and RA and RV structure and function were largely not statistically mediated by indices of LV structure, LV function or pulmonary pressure, except for the associations between (pre)diabetes and RA and RV structure, which were statistically mediated by pulmonary pressure to a very limited extent.
This study extends previous research because of the assessment of RA and RV structure and RV function (i.e. systolic and diastolic) in a relatively large population-based study, with special emphasis on prediabetes; the comprehensive clinical characterization, which enables extensive adjustment for potential confounders; and statistical mediation analyses to investigate the role of LV structure and function in these associations. With regard to the RV structure, and in agreement with earlier studies [9, 18, 19] we showed that pre(diabetes) was associated with a smaller RV (i.e. RV diameter and RV length) although some smaller and(or) unadjusted studies [12,13,14, 16, 17, 22, 24,25,26,27] did not find this association. With regard to RV systolic function, and in agreement with earlier study [24,25,26,27], we showed that (pre)diabetes is associated with RV impaired systolic function independent of traditional risk factors, in contrast to most smaller and(or) unadjusted studies [9, 11,12,13,14, 16,17,18, 20, 22], which found no association. The Mesa study [19], which used RV ejection fraction as measurement for systolic function, found no association either. This could be explained by the fact that TDI-derived measurements, which are used in our study, are more sensitive to alteration of RV systolic function [35]. With regard to diastolic function, in agreement with most earlier studies [9, 13, 14, 17, 18, 20, 22, 24,25,26,27] we showed that (pre)diabetes was associated with impaired RV diastolic function (lower E′RV, lower E/A ratio of the tricuspid valve). In contrast to other studies [14, 17, 22, 25,26,27] we observed a lower A′RV in (pre)diabetes, although the latter studies were unadjusted [14, 17, 22, 25,26,27] and(or) performed in a selected study population (i.e. normotensive, younger, and (or) with type 1 diabetes patients) [14, 17, 25].
Pathophysiology
Although in (pre)diabetes parallel effects on RV and LV structure and function may occur, our results show that the associations between (pre)diabetes and RA and RV structure and function were not mediated by indices of LV structure of function. Since there was no collinearity in mediation analyses, these results suggest a direct myocardial effect, which may apply to both ventricles independently of each other. For instance, as investigated in the RV of Zucker diabetic fatty rats versus controls, lower metabolic rates of glucose utilization and reduced insulin sensitivity were observed [36], which parallels the metabolic changes of the LV in these rats [37]. The subsequent hyperglycemia may alter calciumhomeostasis by inducing calcium/calmodulin-depent kinase II-delta activity as shown in RA and RV myocardium of patients with T2DM and Zucker diabetic fatty rats, which was associated with altered cardiac contractility and relaxation [10]. Nevertheless, Song et al. did show that the expression of cardiac metabolism (i.e. AKT activity and glucose transporter 4) differs among the RV, LV, and interventricular septum [38]. As the RV has, in comparison to the LV, lower mass (i.e. less oxygen consumption), a higher compliance, and lower pressures [4], it is possible that the similar pathophysiological pathways in (pre)diabetes may have differential effects on RA, RV and LA and LV structure and function [5]. Future research which improves the understanding of these differential effects, can therefore contribute to the development of RV targeted therapy.
Confouding
Despite extensive adjustment for potential confounders, residual confounding cannot be fully ruled out. For example subclinical respiratory disease may be important in the association of (pre)diabetes and RA and RV structure and function [39]. Moreover, the use of body surface area to index the RA and LV mass may lead to overcorrection in the more obese (e.g. T2DM) population (with a consequential underestimation of the observed associations) [40].
Limitations
The limitations of the present study may be its cross-sectional design which does not allow strong causal inferences. Reverse causality cannot be excluded, although, from a pathophysiological point of view it appears likely that (pre)diabetes can cause structural RA and RV changes and impaired RV function but not vice versa. Second, echocardiographic assessment of RA and RV structure and function could be hampered by several aspects; the crescent shape and anatomical position of the RV and RA adds complexity to measurement of structure and function (e.g. leading to increased random error of measurement); assessment of RA and RV pressures is less accurate than invasive testing and the use of a multiparameter approach to indicate RV diastolic function whereas a clear definition on RV diastolic function is absent [41, 42]. Other imaging modalities which are less hampered by anatomy (e.g. 3D echocardiography, cardiac MRI) or may be more sensitive to preclinical changes (e.g. deformation echocardiography using strain imaging or speckle tracking) or invasive testing were not available in this study. Third, the generalizability of our findings to other populations can be questioned; the study population primarily consisted of European Caucasians and within this cohort individuals with T2DM were well controlled for their diabetes (i.e. mean HbA1c 6.9%) and comorbid cardiovascular risk factors (i.e. use of antihypertensive and lipid-modifying medication in 68.8% and 74.1% respectively). Fourth, RV function was measured with use of TDI in the whole study population whereas only in a subset tricuspid inflow velocities and TAPSE were measured. Nevertheless, TDI measurements have been shown to be a reliable proxy measurement for RV function [35]. Fifth, clinical outcomes (e.g. incident heart failure, or cardiovascular death) were not available. However previous studies, in a general population, showed that RV structure and function were independent risk factors for incident heart failure and cardiovascular death [6, 43].
Conclusions
In conclusion, in this population-based study (pre)diabetes is associated with structural RA and RV changes, and impaired RV systolic and diastolic function, independent of traditional cardiovascular risk factors. These associations were largely not statistically mediated by indices of LV structure, LV function or pulmonary pressure. This suggests that (pre)diabetes affects the RA and RV structure and function due to direct myocardial involvement. Although the absolute differences are small, this should increase the awareness that in patients with (pre)diabetes preclinical structural and functional changes already have taken place. The accumulated changes may alter the course of overt cardiac disease [44]. Although RV-targeted therapy is not available at the moment, these results suggest that future research should focus on the pathophysiological pathways of RA and RV impairment in (pre)diabetes.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LV:
-
Left ventricular
- LVMI:
-
Left ventricular mass index
- LVEF:
-
Left ventricular ejection fraction
- NGM:
-
Normal glucose metabolism
- RA:
-
Right atrial
- RV:
-
Right ventricular
- T2DM:
-
Type 2 diabetes mellitus
- TAPSE:
-
Tricuspid annular plane systolic excursion
- TDI:
-
Tissue doppler imaging
- TRmax grad:
-
Maximum tricuspid gradient
References
Kannel WB, McGee DL. Diabetes and cardiovascular disease. The Framingham study. JAMA. 1979;241(19):2035–8.
Ford ES, Zhao G, Li C. Pre-diabetes and the risk for cardiovascular disease: a systematic review of the evidence. J Am Coll Cardiol. 2010;55(13):1310–7.
Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117(13):1717–31.
Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436–48.
Sanz J, Sanchez-Quintana D, Bossone E, Bogaard HJ, Naeije R. Anatomy, function, and dysfunction of the right ventricle: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(12):1463–82.
Kawut SM, Barr RG, Lima JA, Praestgaard A, Johnson WC, Chahal H, Ogunyankin KO, Bristow MR, Kizer JR, Tandri H, et al. Right ventricular structure is associated with the risk of heart failure and cardiovascular death: the multi-ethnic study of atherosclerosis (MESA)–right ventricle study. Circulation. 2012;126(14):1681–8.
Melenovsky V, Hwang SJ, Lin G, Redfield MM, Borlaug BA. Right heart dysfunction in heart failure with preserved ejection fraction. Eur Heart J. 2014;35(48):3452–62.
Boudina S, Abel ED. Diabetic cardiomyopathy revisited. Circulation. 2007;115(25):3213–23.
Tadic M, Celic V, Cuspidi C, Ilic S, Pencic B, Radojkovic J, Ivanovic B, Stanisavljevic D, Kocabay G, Marjanovic T. Right heart mechanics in untreated normotensive patients with prediabetes and type 2 diabetes mellitus: a two- and three-dimensional echocardiographic study. J Am Soc Echocardiogr. 2015;28(3):317–27.
Daniels LJ, Wallace RS, Nicholson OM, Wilson GA, McDonald FJ, Jones PP, Baldi JC, Lamberts RR, Erickson JR. Inhibition of calcium/calmodulin-dependent kinase II restores contraction and relaxation in isolated cardiac muscle from type 2 diabetic rats. Cardiovasc Diabetol. 2018;17(1):89.
Whitaker ME, Nair V, Sinari S, Dherange PA, Natarajan B, Trutter L, Brittain EL, Hemnes AR, Austin ED, Patel K, et al. Diabetes mellitus associates with increased right ventricular afterload and remodeling in pulmonary arterial hypertension. Am J Med. 2018;131(6):702.
Jedrzejewska I, Krol W, Swiatowiec A, Wilczewska A, Grzywanowska-Laniewska I, Dluzniewski M, Braksator W. Left and right ventricular systolic function impairment in type 1 diabetic young adults assessed by 2D speckle tracking echocardiography. Eur Heart J Cardiovasc Imaging. 2016;17(4):438–46.
Tadic M, Ilic S, Cuspidi C, Ivanovic B, Bukarica L, Kostic N, Marjanovic T, Kocijancic V, Celic V. Left and right atrial phasic function and deformation in untreated patients with prediabetes and type 2 diabetes mellitus. Int J Cardiovasc Imaging. 2015;31(1):65–76.
Karamitsos TD, Karvounis HI, Dalamanga EG, Papadopoulos CE, Didangellos TP, Karamitsos DT, Parharidis GE, Louridas GE. Early diastolic impairment of diabetic heart: the significance of right ventricle. Int J Cardiol. 2007;114(2):218–23.
Kosmala W, Przewlocka-Kosmala M, Mazurek W. Subclinical right ventricular dysfunction in diabetes mellitus–an ultrasonic strain/strain rate study. Diabetic Med. 2007;24(6):656–63.
Tadic M, Cuspidi C, Vukomanovic V, Ilic S, Celic V, Obert P, Kocijancic V. The influence of type 2 diabetes and arterial hypertension on right ventricular layer-specific mechanics. Acta Diabetol. 2016;53(5):791–7.
Suran D, Sinkovic A, Naji F. Tissue Doppler imaging is a sensitive echocardiographic technique to detect subclinical systolic and diastolic dysfunction of both ventricles in type 1 diabetes mellitus. BMC Cardiovasc Disord. 2016;16:72.
Widya RL, van der Meer RW, Smit JW, Rijzewijk LJ, Diamant M, Bax JJ, de Roos A, Lamb HJ. Right ventricular involvement in diabetic cardiomyopathy. Diabetes Care. 2013;36(2):457–62.
Chahal H, Johnson C, Tandri H, Jain A, Hundley WG, Barr RG, Kawut SM, Lima JA, Bluemke DA. Relation of cardiovascular risk factors to right ventricular structure and function as determined by magnetic resonance imaging (results from the multi-ethnic study of atherosclerosis). Am J Cardiol. 2010;106(1):110–6.
Kosmala W, Colonna P, Przewlocka-Kosmala M, Mazurek W. Right ventricular dysfunction in asymptomatic diabetic patients. Diabetes Care. 2004;27(11):2736–8.
Movahed MR, Milne N. Presence of biventricular dysfunction in patients with type II diabetes mellitus. Congest Heart Fail. 2007;13(2):78–80.
Tayyareci Y, Yurdakul S, Tayyareci G, Nisanci Y, Umman B, Bugra Z. Impact of myocardial acceleration during isovolumic contraction in evaluating subclinical right ventricular systolic dysfunction in type 2 diabetes mellitus patients. Echocardiography. 2010;27(10):1211–8.
Paneni F, Gregori M, Tocci G, Palano F, Ciavarella GM, Pignatelli G, Marra A, Sciarretta S, Ferrucci A, Volpe M. Do diabetes, metabolic syndrome or their association equally affect biventricular function? A tissue Doppler study. Hypertens Res. 2013;36(1):36–42.
Gorter TM, Streng KW, van Melle JP, Rienstra M, Dickinson MG, Lam CSP, Hummel YM, Voors AA, Hoendermis ES, van Veldhuisen DJ. Diabetes mellitus and right ventricular dysfunction in heart failure with preserved ejection fraction. Am J Cardiol. 2018;121(5):621–7.
Ahmed TA, Ahmed YA, Arafa AI, Salah RA. Detection of occult right ventricular dysfunction in young Egyptians with type 1 diabetes mellitus by two-dimensional speckle tracking echocardiography. Indian Heart J. 2018;70(5):665–71.
Parsaee M, Bahmanziari P, Ardeshiri M, Esmaeilzadeh M. Obvious or subclinical right ventricular dysfunction in diabetes mellitus (type II): an echocardiographic tissue deformation study. J Tehran Heart Center. 2012;7(4):177–81.
Kowsari AA, Hosseinsabet A. Evaluation of the right ventricular function in prediabetes: a 2-d speckle tracking echocardiographic study. Ultrasound Med Biol. 2016;42(6):1321–9.
Schram MT, Sep SJ, van der Kallen CJ, Dagnelie PC, Koster A, Schaper N, Henry RM, Stehouwer CD. The Maastricht Study: an extensive phenotyping study on determinants of type 2 diabetes, its complications and its comorbidities. Eur J Epidemiol. 2014;29(6):439–51.
World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia. Geneva: World Health Organization; 2006.
Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, Kusek JW, Manzi J, Van Lente F, Zhang YL, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. New Engl J Med. 2012;367(1):20–9.
Martens RJ, Kimenai DM, Kooman JP, Stehouwer CD, Tan FE, Bekers O, Dagnelie PC, van der Kallen CJ, Kroon AA, Leunissen KM, et al. Estimated glomerular filtration rate and albuminuria are associated with biomarkers of cardiac injury in a population-based cohort study: the maastricht study. Clin Chem. 2017;63(4):887–97.
Stewart AL, Mills KM, King AC, Haskell WL, Gillis D, Ritter PL. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med Sci Sports Exerc. 2001;33(7):1126–41.
Tadic M, Cuspidi C, Sljivic A, Andric A, Ivanovic B, Scepanovic R, Ilic I, Jozika L, Marjanovic T, Celic V. Effects of the metabolic syndrome on right heart mechanics and function. Canad J Cardiol. 2014;30(3):325–31.
Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–91.
Gondi S, Dokainish H. Right ventricular tissue Doppler and strain imaging: ready for clinical use? Echocardiography. 2007;24(5):522–32.
van den Brom CE, Bosmans JW, Vlasblom R, Handoko LM, Huisman MC, Lubberink M, Molthoff CF, Lammertsma AA, Ouwens MD, Diamant M, et al. Diabetic cardiomyopathy in Zucker diabetic fatty rats: the forgotten right ventricle. Cardiovasc Diabetol. 2010;9:25.
van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, Molthoff CF, Lammertsma AA, van der Velden J, Boer C, et al. Altered myocardial substrate metabolism is associated with myocardial dysfunction in early diabetic cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol. 2009;8:39.
Song J, Shen S, Zhang M, Wang K, Zhang Y, Li X, Wang N, Cao Y. Differences in Akt signaling and metabolism gene expression in the right heart, intraventricular septum and left heart of rodents. Int J Clin Exp Pathol. 2015;8(10):12915–21.
Takahashi T, Yoshihisa A, Sugimoto K, Yokokawa T, Misaka T, Kaneshiro T, Oikawa M, Kobayashi A, Nakazato K, Ishida T, et al. Associations between diabetes mellitus and pulmonary hypertension in chronic respiratory disease patients. PLoS ONE. 2018;13(10):e0205008.
Hoit BD. It’s time to index the right ventricle, but to what and how? J Am Soc Echocardiogr. 2012;25(12):1277–9.
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685–713.
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiogr. 2016;29(4):277–314.
Modin D, Mogelvang R, Andersen DM, Biering-Sorensen T. Right ventricular function evaluated by tricuspid annular plane systolic excursion predicts cardiovascular death in the general population. J Am Heart Assoc. 2019;8(10):e012197.
Roifman I, Ghugre N, Zia MI, Farkouh ME, Zavodni A, Wright GA, Connelly KA. Diabetes is an independent predictor of right ventricular dysfunction post ST-elevation myocardial infarction. Cardiovasc Diabetol. 2016;15:34.
Acknowledgements
Not applicable.
Funding
This study was supported by the European Regional Development Fund via OP-Zuid, the Province of Limburg, the Dutch Ministry of Economic Affairs (Grant 31O.041), Stichting De Weijerhorst (Maastricht, The Netherlands), the Pearl String Initiative Diabetes (Amsterdam, The Netherlands), CARIM School for Cardiovascular Diseases (Maastricht, The Netherlands), Stichting Annadal (Maastricht, The Netherlands), Health Foundation Limburg (Maastricht, The Netherlands) and by unrestricted Grants from Janssen-Cilag B.V. (Tilburg, The Netherlands), Novo Nordisk Farma B.V. (Alphen aan den Rijn, The Netherlands) and Sanofi-Aventis Netherlands B.V. (Gouda, The Netherlands).
Author information
Authors and Affiliations
Contributions
PL participated in acquisition of data, analyzed data, interpreted results, and wrote the manuscript. MV participated in acquisition of data, contributed to discussion, reviewed and edited the manuscript. RH, CK, and MS contributed to study conception, study design, and reviewed and edited the manuscript. AK contributed to discussion, reviewed and edited the manuscript. HPBLR contributed to study design, interpretation of data, revised the manuscript critically for important intellectual content. CS contributed to conception and design, contributed interpretation of data, revised the manuscript critically for important intellectual content. CS is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has been approved by the institutional medical ethical committee (Medisch Ethische Toetsingscommissie, Maastricht University) (NL31329.068.10) and the Minister of Health, Welfare and Sports of the Netherlands (Permit 131088-105234-PG). All participants gave written informed consent.
Consent for publication
Not applicable.
Competing interests
PL, MV, RH, CK, AK, MS, and CS have nothing to disclose. Dr. HPBLR reports unrestricted research grants from Roche Diagnostics, Vifor and Novartis and serves as member of the advisory board of Roche Diagnostics, Vifor and Novartis outside the submitted work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Supplemental methods.
Additional file 2.
Supplemental tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Linssen, P.B.C., Veugen, M.G.J., Henry, R.M.A. et al. Associations of (pre)diabetes with right ventricular and atrial structure and function: the Maastricht Study. Cardiovasc Diabetol 19, 88 (2020). https://doi.org/10.1186/s12933-020-01055-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-020-01055-y