
Abstract
Background
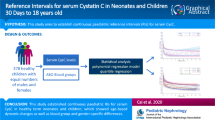
Cystatin C (Cys-C) is a more sensitive marker of renal function than creatinine (Cre) in pediatric and adult populations. However, the reference values of serum Cys-C for estimating glomerular filtration rates (eGFRs) in premature infants during the first year of life have not been sufficiently studied.
Methods
In this prospective study, 481 blood samples were collected from 261 preterm infants with uncomplicated clinical courses during their first year of life. Infants were divided into three groups according to gestational age at birth: 27–30 weeks, 31–33 weeks, and 34–36 weeks. Serum Cys-C and Cre levels were measured at 6–30 days, 3–5 months, 7–9 months, and 12–14 months after birth and the eGFR was calculated using two previously published equations.
Results
The median serum Cys-C levels were 1.776, 1.248, 1.037, and 0.960 mg/L at the first, second, third, and fourth measurement time-point, respectively, with the value significantly decreasing with age up to 12–14 months. Cys-C levels were independent of gestational age and gender. In contrast to Cys-C, serum Cre values declined rapidly up to 3–5 months, then remained constant up to 12–14 months. Using the Cys-C-based equation, the eGFR significantly increased with increasing age until approximately 1 year after birth; however, no such trend was noted using the equation based on Cys-C + Cre.
Conclusions
Reference ranges for Cys-C in premature infants decline gradually over the first year after birth. Cys-C appears to be a more reliable marker than Cre for estimating GFR in preterm infants.
Similar content being viewed by others


Introduction
Preterm birth is associated with interruption of the normal organogenesis of the kidney and the vascular tree, leading to low nephron endowment, hypertension, endothelial dysfunction, and proteinuria in some individuals [1]. Because nephrogenesis is ongoing until week 36 of gestation, preterm birth before this period may result in reduced nephron number, especially if there is superimposed acute kidney injury (AKI). Indeed, AKI is a common problem in preterm neonates [2]. In many cases, the AKI can be resolved and kidney function can return to normal, but some cases result in permanent kidney injury [3, 4]. Preterm neonates with AKI have a high incidence of low glomerular filtration rate (GFR) several years later [5]. Therefore, early detection of renal function impairment is of great importance for prevention of more severe renal damage.
Glomerular filtration rate is known to be one of the most sensitive markers of kidney function and kidney disease progression. Because of the technical difficulty in collecting urine from neonates and infants, serum creatinine (Cre) is widely used to determine GFR in these patient groups. However, Cre is a metabolic product of muscular tissue, and its production rate changes depending on muscle mass [6]. In addition, serum Cre concentration is often not affected unless the GFR falls below normal levels. Thus, Cre analysis is not considered an accurate method for measuring mild and moderate changes in GFR [2].
Cystatin C (Cys-C) is a 13,600-Da protein synthesized by a house-keeping gene and found in all nucleated cells, which means that its amount in the blood is constant [7]. It appears to be a more sensitive alternative to Cre for evaluation of GFR due to its constant production rate, ability to pass freely through the glomerulus [8], and the fact that its levels are not influenced by muscle mass or gender [9]. Accordingly, various studies have been performed to determine the reference values of Cys-C in infants and children [10, 11]. These have been found to vary with the age of the individual, being highest at birth and falling progressively until the age of 1 year, when they are similar to those of adults [12]. However, data on the reference levels of Cys-C in preterm infants during this period are limited.
The aim of this longitudinal study was to investigate trends in the reference values of serum Cys-C in preterm infants during the first year of life and to determine the reliability of serum Cys-C level for the estimation of the GFR.
Patients and methods
Subjects
A total of 475 neonates admitted to the neonatal intensive care unit of Kitakyushu Municipal Medical Center between 2009 and 2012 were considered for enrollment in this prospective study. Exclusion criteria included: (1) any renal pathology or signs of acute renal failure; (2) any congenital anomaly; (3) asphyxia at birth, defined as an Apgar score of <7 at 1 or 5 min; (4) any severe systemic illness which could affect renal function (e.g., patent ductus arteriosus, necrotizing enterocolitis, sepsis); (5) any use of medications that might interfere with renal function (e.g., indomethacin, aminoglycosides, glycopeptides); (6) use of steroids; (7) gestational age (GA) of >36 weeks. None of the infants or their mothers had hyperthyroidism or hypothyroidism. Infants who had respiratory distress syndrome or needed inotropic agents or mechanical ventilation support were included. Infants born at less than 27 gestational weeks were not included because they had at least one of the aforementioned exclusion criteria. The final study population consisted of 261 premature infants. Patients were divided into three groups according to GA, namely, GA of 27–30, 31–33, and 34–36 weeks, respectively (Fig. 1). Neonates were considered small for GA (SGA) if their weight at birth fell below the 10th percentile for their GA according to standards of birth size for Japanese neonates.

Flowchart of patient selection and classification into three groups according to gestational age (GA) at birth. A total of 261 infants were recruited after the exclusion of infants who developed complications or had to be given nephrotoxic drugs (see Subjects section). The three GA groups were 27–30, 31–33, and 34–36 weeks GA at birth. Numbers in chart Number of infants, PNA Postnatal age
Measurement
Blood samples for the measurement of Cre and Cyc-C were obtained from each infant’s peripheral arteries or veins at 6–30 days, 3–5 months, 7–9 months, and 12–14 months after birth. Samples were not collected immediately after delivery because infant Cre levels may be influenced by maternal ones up to the second day of life [13]. A total of 481 blood samples were collected from our 261 preterm infants during the first year of life, and serum levels of Cys-C and Cre were measured concurrently. Serum Cys-C was analyzed by SRL Inc. (Tokyo, Japan) using a colloidal gold immunoassay (Nescauto GC Cystatin C; Alfresa Pharma Corp., Osaka, Japan) in a BioMajesty JCA-BM8020 clinical chemistry analyzer (JEOL Ltd., Tokyo, Japan). The obtained Cys-C values were calibrated to international reference standard (ERM-DA471/IFCC) as previously reported [14]. Serum Cre was determined with an enzymatic method using the JCA-BM6070 automated clinical chemistry analyzer (JEOL Ltd.).
We also assessed renal function by using two equations that have been previously used for this purpose. Cys-C-based estimated GFR (eGFR) was calculated using Zappitelli’s formula [75.94 × (Cys-C) −1.170] [15, 16], while Cys-C + Cre-based eGFR was calculated using the Schwartz-combined formula {3.98 × [body length (cm)/serum Cre]0.456 × (1.8/Cys-C)0.418 × (30/blood nitrogen urea)0.079}. However, we did not use blood nitrogen urea in the calculation as it was not determined in our study, similar to the method of Treiber et al. [16, 17].
Statistical analysis
The chi-squared (χ2) test and Fisher’s exact test were used to compare categorical variables. Numerical data were expressed as median and minimum–maximum range. Reference intervals of Cys-C levels and eGFRs, including 90 % confidence intervals, were determined according to Clinical Laboratory Standards Institute guidelines [18]. Differences among the three GA groups were assessed using the non-parametric Kruskal–Wallis test. The Friedman rank-sum test was used for longitudinal data analysis. Post hoc tests, specifically Wilcoxon signed-rank tests with Bonferroni correction, were conducted to assess differences between time points. All p values were based on two-sided testing, and the significance level was set at 0.05. Statistical analyses were performed with MedCalc software version 15.8 (MedCalc, Mariakerke, Belgium) and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (R Foundation for Statistical Computing, Vienna, Austria) that modifies R by adding statistical functions frequently used in biostatistics [19].
Results
A total of 261 preterm infants were enrolled in this study, of whom 15 were born at 27–30 weeks, 93 (neonates) at 31–33 weeks, and 153 at 34–36 weeks. Some infants were lost to follow-up at 14 months after birth (Fig. 1). General characteristics of the infants in each group are shown in Table 1. There were no significant differences among the three GA groups in terms of gender ratio or Apgar scores at 1 and 5 min; however, there were significant differences in birth weight, the proportion of SGA infants, the pH of the umbilical artery, the proportion of patients who had respiratory distress syndrome and required inotropic agents and mechanical ventilation support, and the duration of oxygen supplementation and mechanical ventilation.
The longitudinal levels of serum Cys-C are presented in Table 2 and Fig. 2. Levels were highest in blood samples collected at 6–30 days of life and declined significantly with increasing age until about 1 year after birth (p < 0.01 for trend). There were no significant differences among the GA groups at any time during the first year of life. Median Cre levels were 0.5, 0.1, 0.1, and 0.2 mg/dL at 6–30 days, 3–5 months, 7–9 months, and 12–14 months of life, respectively. Like the Cys-C levels, Cre levels were also highest in the blood samples collected at 6–30 days; however, they decreased rapidly over the next 3–5 months of life, but then stabilized, with no significant change in Cre values at any measurement time point after 3–5 months of life (Fig. 2). Unlike the Cys-C levels, there were significant differences in the Cre levels among the GA groups, but only in neonates aged 6–30 days. The median Cre levels were 0.7 mg/dL among the infants born at 27–30 weeks, 0.6 mg/dL among the infants born at 31–33 weeks, 0.5 mg/dL among the infants born at 34–36 weeks (p < 0.01, Fig. 2). We did not find significant differences in the serum Cys-C and Cre levels between male and female infants (data not shown).

Median serum values of cystatin-C (Cys-C) and creatinine (Cre) during the study period. Box plot with the median (horizontal line in box), interquartile range (IQR, box), and minimum and maximum values that fall within 1.5-fold the IQR (whiskers). Cys-C was highest at 6–30 days after birth and gradually declined until about 1 year after birth. This decrease was statistically significant from each measurement time point to the next (*p < 0.01 for each PNA). There were no significant changes in Cre values between measurements after 3–5 months of life. There were significant differences in the Cre levels among the GA groups only at 6–30 days after birth (**p < 0.01), PNA, Postnatal age
Figure 3 and Table 3 show the longitudinal serum Cys-C levels for appropriate for GA (AGA) and SGA infants. There was a significant difference between AGA and SGA infants only at 3–5 months (p = 0.01), and no differences were noted at other measurement time points during the first year of life.

Median serum Cys-C levels in the appropriate for GA (AGA) and small for GA (SGA) preterm infants during the first year of life. Box plot with the median (horizontal line), IQR (box), and minimum and maximum values that fall within 1.5-fold the IQR (whiskers). There were significant differences between AGA and SGA infants only at 3–5 months after birth (*p = 0.01)
Estimations of GFRs using two methods in preterm infants are presented in Table 4 and Fig. 4. The eGFR appeared to be higher when calculated using the equation based on both Cys-C and Cre than when using the equation based on only Cys-C from 3 to 9 months of life (Fig. 4). The eGFR based on only Cys-C was the lowest at 6–30 days and increased significantly with increase in age until approximately 1 year after birth (p < 0.01 for trend). However, we did not find a significant difference in eGFRs based on Cys-C + Cre between 7–9 months and 12–14 months.

Estimated glomerular filtration rate (eGFR) values in the preterm infants calculated using the Cys-C-based equation and the Cys-C + Cre-based equation. Bar Median value, whiskers 95 % reference interval. *p < 0.01 vs. the value at 6–30 days; **p < 0.01 vs. the value at 3–5 months; ***p < 0.01 vs. the value at 7–9 months
Discussion
Although Cys-C is known to be a reliable marker of renal function, only a few studies have attempted to determine reference intervals for Cys-C levels in preterm infants, with most having focused on the first 30 postnatal days [10, 20–25]. To the best of our knowledge, this is the first longitudinal study to evaluate reference values of serum Cys-C in preterm infants over the entire first year of life.
In this study, the highest serum Cys-C concentration was found at 6–30 days after birth, followed by a gradual decrease over the following months. Cataldi et al. reported that Cys-C does not cross the placental barrier [26]; therefore, this decrease in level after birth probably reflects the maturation of glomerular filtration capacity. Although Cre values in the three GA groups were likewise highest at 6–30 days after birth, they decreased rapidly up to 3–5 months after birth and remained constant thereafter. Boer et al. also found that mean serum Cre values decreased rapidly from day 1 to the second month of life, after which they stabilized until the seventh month, followed by a slight increase [27]. Boer et al.’s reference values for Cre were also similar to ours. High Cre levels in newborns are believed to represent maternal Cre levels. We speculate that the rapidly decreasing trend in Cre levels after the first month of life and the stable trend until 12–14 months which we observed in our study reflect the small muscle mass of premature infants and insensitivity to their gradually maturing renal function. This explanation is supported by the observations of Cho et al., who reported that blood Cre level is influenced by muscle mass and is insensitive to slightly reduced renal function [28].
Among the GA groups, there were significant differences only in the Cre values at 6–30 days during the first year of life (Fig. 2). The median first sampling day of life was day 7, and there were no significant differences in the sampling day among all the GA groups (data not shown). Our results are consistent with those of previous reports which showed that serum Cre levels are higher in premature infants than in mature infants during the first few days of life [29]. One possible explanation of the transient increase in serum Cre levels in premature infants is Cre reabsorption across immature leaky tubules [30]. Therefore, there is a possibility of misdiagnosing AKI in the first few days of life in preterm infants. We speculate that Cys-C is not reabsorbed through renal tubules. In our premature infant population, the Cys-C levels during the first year of life were not affected by GA or gender. Therefore, it would appear that Cys-C is a more reliable marker than Cre for the early detection of mild renal dysfunction in preterm infants.
Previous studies have reported an association between intrauterine growth restriction and decreased renal volume [31] or renal dysfunction later in life [32]. Basioti et al. reported that glomerular function was similar between SGA children and AGA controls at preschool age; however, SGA children showed subtle alterations in tubular function [33]. The time point at which renal function is impaired in SGA populations is unknown. In our study, there were significant differences in Cys-C levels between SGA and AGA infants only at 3–5 months. Although the reason for such a difference is unknown, we speculate that the number of subjects might not have been sufficient to detect significant differences at other time points or, alternatively, that SGA might not be a risk factor for renal dysfunction until 1 year after birth. Larger studies are required to evaluate the longitudinal renal function of SGA infants from birth.
We estimated GFRs by using equations that have been previously reported [15–17]. We speculate that the eGFR based on the Cys-C formula but not on the Cys-C + Cre formula could reflect the true GFR during the first year of life for the following reasons: (1) the increasing trend and the values of the eGFR based on only Cys-C might be similar to those based on inulin clearance [34]; (2) the serum Cre levels might be influenced by maternal Cre levels, especially during the initial days of life [13]; (3) the serum Cre levels might be influenced by the small muscle mass of the infant in the first year after birth [6]. Further studies are required to assess which formula is better at estimating GFRs in preterm infants at this age.
The limitations of our study include the small number of infants in each GA group, which may have reduced the reliability of the calculated reference interval. In addition, our study did not include infants born at less than 27 gestational weeks. Such extremely premature infants often have asphyxia at birth, require prolonged use of a mechanical ventilator, or develop complications requiring nephrotoxic medication, making it difficult to determine a reference Cys-C interval. Further studies with a larger number of healthy infants are needed to determine reference interval more accurately.
In conclusion, serum Cys-C reference ranges in premature infants during the first year after birth are independent of GA and gender and show a decreasing trend. Cys-C appears to be a more reliable marker than Cre for estimating GFR in preterm infants.
References
Abitbol CL, Rodriguez MM (2012) The long-term renal and cardiovascular consequences of prematurity. Nat Rev Nephrol 8:265–274
Askenazi DJ, Ambalavanan N, Goldstein SL (2009) Acute kidney injury in critically ill newborns: what do we know? What do we need to learn? Pediatr Nephrol 24:265–274
Goldstein SL, Devarajan P (2011) Acute kidney injury in childhood: should we be worried about progression to CKD? Pediatr Nephrol 26:509–522
Durkan AM, Alexander RT (2011) Acute kidney injury post neonatal asphyxia. J Pediatr 158:e29–e33
Abitbol CL, Bauer CR, Montane B, Chandar J, Duara S, Zilleruelo G (2003) Long-term follow-up of extremely low birth weight infants with neonatal renal failure. Pediatr Nephrol 18:887–893
Perrone RD, Madias NE, Levey AS (1992) Serum creatinine as an index of renal function: new insights into old concepts. Clin Chem 38:1933–1953
Filler G, Priem F, Vollmer I, Gellermann J, Jung K (1999) Diagnostic sensitivity of serum cystatin for impaired glomerular filtration rate. Pediatr Nephrol 13:501–505
Grubb A (1992) Diagnostic value of analysis of cystatin C and protein HC in biological fluids. Clin Nephrol 38[Suppl 1]:S20–S27
Bokenkamp A, Domanetzki M, Zinck R, Schumann G, Byrd D, Brodehl J (1998) Cystatin C—a new marker of glomerular filtration rate in children independent of age and height. Pediatrics 101:875–881
Finney H, Newman DJ, Thakkar H, Fell JM, Price CP (2000) Reference ranges for plasma cystatin C and creatinine measurements in premature infants, neonates, and older children. Arch Dis Child 82:71–75
Randers E, Krue S, Erlandsen EJ, Danielsen H, Hansen LG (1999) Reference interval for serum cystatin C in children. Clin Chem 45:1856–1858
Yata N, Uemura O, Honda M, Matsuyama T, Ishikura K, Hataya H, Nagai T, Ikezumi Y, Fujita N, Ito S, Iijima K, Saito M, Keneko T, Kitagawa T (2013) Reference ranges for serum cystatin C measurements in Japanese children by using 4 automated assays. Clin Exp Nephrol 17:872–876
Falcao MC, Okay Y, Ramos JL (1999) Relationship between plasma creatinine concentration and glomerular filtration in preterm newborn infants. Rev Hosp Clin Fac Med Sao Paulo 54:121–126
Uemura O, Nagai T, Ishikura K, Ito S, Hataya H, Gotoh Y, Fujita N, Akioka Y, Kaneko T, Honda M (2014) Cystatin C-based equation for estimating glomerular filtration rate in Japanese children and adolescents. Clin Exp Nephrol 18:718–725
Zappitelli M, Parvex P, Joseph L, Paradis G, Grey V, Lau S, Bell L (2006) Derivation and validation of cystatin C-based prediction equations for GFR in children. Am J Kidney Dis 48:221–230
Treiber M, Pecovnik Balon B, Gorenjak M (2015) A new serum cystatin C formula for estimating glomerular filtration rate in newborns. Pediatr Nephrol 30:1297–1305
Schwartz GJ, Schneider MF, Maier PS, Moxey-Mims M, Dharnidharka VR, Warady BA, Furth SL, Munoz A (2012) Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int 82:445–453
CLSI (2008) Defining, establishing and verifying reference intervals in the clinical laboratory; Approved Guideline. CLSI document EP28-A3c, 3rd edn. Clinical and Laboratory Standards Institute, Wayne
Kanda Y (2013) Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 48:452–458
Armangil D, Yurdakok M, Canpolat FE, Korkmaz A, Yigit S, Tekinalp G (2008) Determination of reference values for plasma cystatin C and comparison with creatinine in premature infants. Pediatr Nephrol 23:2081–2083
Dorum S, Silfeler I, Dorum BA, Silfeler DB, Canbak Y, Say A (2012) Reference values of serum cystatin-C for full-term and preterm neonates in Istanbul. Indian J Pediatr 79:1037–1042
Demirel G, Celik IH, Canpolat FE, Erdeve O, Biyikli Z, Dilmen U (2013) Reference values of serum cystatin C in very low-birthweight premature infants. Acta Paediatr 102:e4–e7
Elmas AT, Tabel Y, Elmas ON (2013) Reference intervals of serum cystatin C for determining cystatin C-based glomerular filtration rates in preterm neonates. J Matern Fetal Neonatal Med 26:1474–1478
Filler G, Lepage N (2013) Cystatin C adaptation in the first month of life. Pediatr Nephrol 28:991–994
Lee JH, Hahn WH, Ahn J, Chang JY, Bae CW (2013) Serum cystatin C during 30 postnatal days is dependent on the postconceptional age in neonates. Pediatr Nephrol 28:1073–1078
Cataldi L, Mussap M, Bertelli L, Ruzzante N, Fanos V, Plebani M (1999) Cystatin C in healthy women at term pregnancy and in their infant newborns: relationship between maternal and neonatal serum levels and reference values. Am J Perinatol 16:287–295
Boer DP, de Rijke YB, Hop WC, Cransberg K, Dorresteijn EM (2010) Reference values for serum creatinine in children younger than 1 year of age. Pediatr Nephrol 25:2107–2113
Cho SY, Hahn WH, Lee HJ, Suh JT, Lee A, Cho BS, Suh JS (2012) The clinical significance of serum cystatin C in critically ill newborns with normal serum creatinine. J Clin Lab Anal 26:267–271
Thayyil S, Sheik S, Kempley ST, Sinha A (2008) A gestation- and postnatal age-based reference chart for assessing renal function in extremely premature infants. J Perinatol 28:226–229
Bueva A, Guignard JP (1994) Renal function in preterm neonates. Pediatr Res 36:572–577
Silver LE, Decamps PJ, Korst LM, Platt LD, Castro LC (2003) Intrauterine growth restriction is accompanied by decreased renal volume in the human fetus. Am J Obstet Gynecol 188:1320–1325
Chan PY, Morris JM, Leslie GI, Kelly PJ, Gallery ED (2010) The long-term effects of prematurity and intrauterine growth restriction on cardiovascular, renal, and metabolic function. Int J Pediatr 2010:280402
Basioti M, Giapros V, Kostoula A, Cholevas V, Andronikou S (2009) Growth restriction at birth and kidney function during childhood. Am J Kidney Dis 54:850–858
Schwartz GJ, Furth SL (2007) Glomerular filtration rate measurement and estimation in chronic kidney disease. Pediatr Nephrol 22:1839–1848
Acknowledgments
We thank J. Kishimoto (Data Management Center, Center for Clinical and Translational Research, Kyushu University Hospital) for helping with the statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The children’s parents provided written informed consent according to the Declaration of Helsinki, and ethics approval was obtained from the institutional review board.
Conflict of interest
The authors declare that no conflict of interest exists.
Rights and permissions
About this article

Cite this article
Nakashima, T., Inoue, H., Fujiyoshi, J. et al. Longitudinal analysis of serum cystatin C for estimating the glomerular filtration rate in preterm infants. Pediatr Nephrol 31, 983–989 (2016). https://doi.org/10.1007/s00467-015-3309-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-015-3309-x