
Abstract
Conventional radiography is regularly used to evaluate complications after total hip arthroplasty. In various recent consensus meetings, however, plain radiographs of a potentially infected hip joint have been judged as being only relevant to exclude diagnoses other than infection. Solid data on radiographic presentations of periprosthetic joint infection (PJI) are scarce. As a result, the prognostic value of radiological features in low-grade PJI remains uncertain. The present review article aims to present an overview of the available literature and to develop ideas on future perspectives to define the diagnostic possibilities of radiography in PJIs of the hip. The primary outcome of interest of this systematic review was the radiologic presentation of periprosthetic joint infections of the hip. As secondary outcome of interest served the sensitivity and specificity of the radiologic presentation of periprosthetic joint infections. Of the included articles, 26 were reviews, essays, or case reports and only 18 were clinical studies. Typical radiologic abnormalities of PJI were a periosteal reaction, a wide band of radiolucency at the cement–bone or metal–bone interface, patchy osteolysis, implant loosening, bone resorption around the implant, and transcortical sinus tracts. The frequency of their occurrence is still inadequately defined. A deeper understanding of the underlying causes and the relation between microorganisms to radiologic abnormalities can probably help clinicians in the future to diagnose a PJI. This is why further research shall focus on the radiographic features of PJI.
Similar content being viewed by others


Introduction
Conventional radiography is regularly used to evaluate joint prostheses after implantation and during follow-up, as X-rays can detect potential abnormalities involving both the implant and the surrounding bone. Such abnormalities could be for example periprosthetic fracture, dislocation, osteolysis due to third body wear, or sinking of the shaft. One of the major complications after arthroplasty is periprosthetic joint infection (PJI). In various recent consensus meetings, however, plain radiographs of a potentially infected hip joint have been judged as being only relevant to exclude diagnoses other than infection [1,2,3]. In the consensus statement published by Romano and colleagues in 2020, for example, the diagnostic performance of conventional radiography in detecting PJI would be very low.
Furthermore, conventional radiography would show demineralization only when more than 30–50% of bone mass has been lost. Abnormalities of bone around the implant would usually be non-specific for infection. In addition, up to 50% of conventional X-ray exams would give negative results [1]. In another recent consensus statement published by Signore et al. [2, 3], the authors state that “Regarding PJI, conventional radiography often yields normal results or may detect non-specific signs of soft-tissue swelling. Serial plain radiography has been reported to have a sensitivity of 14% and specificity of 70% in detecting implant-associated infections [4]. Radiographic signs that may reveal PJI with high specificity are gas formation and active, immature periostitis. Radiographic signs with low specificity include soft-tissue swelling, periprosthetic lucency, and component loosening. However, differentiation between septic and aseptic periprosthetic lucency and component loosening is almost impossible in conventional radiography. Also, these signs are visible only when almost 30% of the bone mass has been lost; thus, 50% of radiographs remain normal despite the presence of infection”. These consensus statements are, however, only based on three references [5,6,7].
Most of the studies to which these statements relate date to the late 80 s and early 90 s [5, 7, 8]. The foundations of the data referenced here are also quite weak, such as in the study from Tigges et al., [7] with 20 confirmed infected hip arthroplasties, or Lyons et al. [5] 50 painful hip arthroplasties. The largest series presented was from Thoren and Hallin in 1989 [8], where the authors analysed 102 hip revisions. Of these, however, only 47 were infected and the prostheses analysed were original Charnley prostheses which possessed a 22.225-mm head in ultra-high molecular weight polyethylene (UHMW PE) in an all-cemented technique and a metal-on PE bearing. The arthroplasty landscape has, however, largely changed since then. Today's arthroplasties often contain an uncemented cup and a ceramic head. Depending on the country the stem is often uncemented ranging from 37% in the National Joint Registry in Great Britain to 78% in the German Arthroplasty Registry in Germany [9]. Uncemented stems usually consist of titanium which altogether changes the immunogenicity of the wear particles generated. Moreover, the annual number of patients treated with arthroplasties has multiplied and as such the surgical technique and postoperative rehabilitation protocols have been optimized and largely standardized. In addition, life expectancy has increased with people in old age having multiple comorbidities in addition to joint replacement. This supposedly changes the spectrum of bacteria responsible for infections. While we are quite effective in treating acute PJIs, the successful management of low-grade infections is still a challenge. This includes reliable, sensitive and specific diagnostics of such low-grade PJIs. Nevertheless, substantial progress has been made in the diagnosis of such an event with improvements in the histopathological analysis of the periprosthetic membrane [10, 11], the advent of PCR analyses [12], and synovial fluid analysis including the analysis of PMNs, alpha-defensin or leukocyte esterase-levels [13,14,15,16]. Other newer markers are presently under investigation, such as pentraxin-3 [17], calprotectin [18], or myeloperoxidase [19]. Of note, thresholds for leukocytes in low-grade PJIs have been constantly lowered over the past decades ranging now—depending on the joint—between 1000 and 2000 leukocytes/µl only [20]. Cultivation techniques for bacteria have also been more and more standardized. We can assume that the overall sensitivity and specificity have increased over the past 30 years. Similarly, the technique of acquiring radiographs has also improved with the widespread introduction of digital radiography. The digital data set allows for post-imaging optimization of each X-ray to visualize structures that were difficult to discern in traditional images intended for a good bone contrast only. Nevertheless, solid data on radiographic presentations of PJI are scarce. As a result, the prognostic value of radiological features in low-grade PJI remains uncertain. The present review article aims to present an overview of the available literature and to develop ideas on future perspectives to define the diagnostic possibilities of radiography in PJIs of the hip.
Materials and methods
Eligibility criteria
All published articles related to the radiographic presentation of PJI of the hip were accessed. Only articles available in English, French, Spanish or German were eligible. Original studies with a level of evidence of I to IV according to the Oxford Centre of Evidence-Based Medicine [21] plus review articles and essays were considered.
Search strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the 2020 PRISMA statement [22]. On July 24, 2023, PubMed and Web of Science were accessed. The following keywords were used: "periprosthetic joint infection hip radiograph"; "Prosthesis-Related Infections"[Mesh] AND "Radiography"[Mesh]) AND "Hip"[Mesh]; "Radiography"[Mesh]) AND "Hip"[Mesh]) AND "Infections"[Mesh]; "radiography" "hip arthroplasty" "infection"; "x-ray" "hip arthroplasty" "infection"; "x-ray" "periprosthetic joint infection" "hip"; "periprosthetic joint infection" "hip" "radiograph"; "heterotopic ossification" "hip arthroplasty" "infection"; "heterotopic ossification" "hip" "periprosthetic joint infection". No filters were applied.
Selection and data collection
Three authors (UKH; MM; GE) independently performed the database search. All the resulting titles were screened and, if suitable, the abstract was accessed. The full text of the abstracts, which matched the topic, was accessed. A cross-reference of the bibliography of the full-text articles was also screened for inclusion. If the full text was not accessible or available, the article was not considered for inclusion. Disagreements were debated before final inclusion into the study.
Data items and outcome of interest
The following data at baseline were extracted: author, year of publication and journal, PMID/PCMID/DOI, type of analysis performed, country of origin, main study outline, number of patients used for the relevant statements, and statements made regarding radiography and PJI of the hip. A suitable level of evidence was attributed to each study. The primary outcome of interest was the radiologic presentation of PJI of the hip. As secondary outcome of interest served the sensitivity and specificity of the described image characteristics.
Results
Study selection
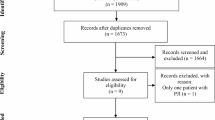
The literature search resulted in 1248 articles (Fig. 1). After the removal of duplicates, 1121 articles were screened. Having screened titles and abstracts, the original manuscript was accessed for 71 studies. Of these 44 finally met the inclusion criteria, the other publications were either in Chinese (n = 3), not retrievable (n = 10), retracted (n = 1), were not related to the research question (n = 6), or did not directly report radiographic parameters (n = 7). Of the finally included articles, 26 were reviews, essays, or case reports. Only 18 publications were clinical studies with a level of evidence between IV and II.

Flowchart of the literature search
Review summary
Summarizing the statements provided in the review articles, essays, and case reports (Table 1), a few commonly reported traits can be made out: claimed radiographic signs of infection are periosteal reaction [23,24,25,26,27,28,29,30,31,32,33], formation of lamellae [23], focal osteolysis or bone destruction [7, 23, 24, 26, 28, 31, 33,34,35,36,37,38], a wide radiolucent zone [23, 32, 36, 39], signs of loosening in a previously well-fixed implant [24, 27, 28, 32, 34], heterotopic bone formation [28, 40], mottling [31], an intracortical sinus tract [24, 28], periprosthetic fractures [27], adjacent soft-tissue collection [29, 30, 32], and rapid disease progression [25]. Aseptic loosening tends to produce uniform radiolucency, whereas particle disease produces multifocal radiolucencies related to localized osteolysis. Infection can produce either of these patterns [41, 42] with an osteolysis of > 2 mm being indicative of infection [41]. The radiographic presentation thereby seems to be a function of time, with early infections presenting without radiological features and late infections presenting with inflammatory and reactive osteoproliferative changes of the bone [34, 43]. These signs are only present in a subpopulation of all PJI and thus have a low sensitivity while having a reasonable specificity.
Original data
Looking at the original data (Table 2), the numbers on which statements are based are generally low ranging from 2 to 50 with a median of 15. The discrepancies in the reported data are, however, extreme: radiographic abnormalities are visible in all cases of PJI of the hip [44,45,46,47]. Other authors only report very low incidences of such findings [48,49,50]. Related features are periosteal reaction [5, 45], a radiolucent zone [7, 45], sinking of the prosthesis or loosening [45, 49,50,51], periprosthetic osteolysis or scalloped endosteal bone resorption [5, 7, 38, 50, 52], scalloping [45], and in cemented shafts cement mantle irregularities [51]. The first changes appear to be visible 3 months after the onset of symptoms [45]. The absence of periprosthetic osteolysis was reported to be predictive of aseptic loosening [52]. Lyons et al., reported a sensitivity of 47% and a specificity of 96% for scalloped bone resorption whereas laminated periosteal new bone had only a 25% sensitivity with, however, also a 92% specificity (n = 16) [5].
Heterotopic bone formation can occur in PJIs [53], but it can also be present in cases of aseptic loosening or just idiopathic [52]. In a retrospective study including 168 patients, Manrique et al. [54], reported an incidence of heterotopic ossifications following surgical treatment of PJI of the hip 84% and in aseptic revision cases of only 11%. Cases after periprosthetic joint infection in that study also had significantly higher Brooker grades [54]. In a CT-based study, Isern-Kebschull et al., reported a sensitivity for periarticular ossifications of 20% (8.4–36.9), a specificity of 79% (66.3–88.1), a positive predictive value of 35 (15.4–59.2), and a negative predictive value of 63 (51.3–73.9) [55].
Regarding risk factors for infection, an interesting observation was made by Rey Fernandez et al. who described that patients with more than 60 mm soft-tissue thickness over the greater trochanter had a sevenfold higher risk of infection [56].
Only one study explicitly elaborated on the detected bacteria and described the associated radiologic findings: Barrack et al. [44], reported 5 cases infected with S. epidermidis and found periostitis (3×), focal lysis (1×), diffuse lysis with endosteal scalloping (1×) and heterotopic ossification (2×). One case with Strept. sanguis had focal lyses around the implant.
Discussion
PJI is one of the most serious complications after total hip arthroplasty and poses major diagnostic challenges for clinicians. Radiological imaging, especially plain radiographs, is part of every diagnostic workup in case of suspected complications after total hip arthroplasty. There are plenty of reviews and original works dealing with the diagnostic algorithm of PJI. This review aimed to summarize and analyse the available information about the radiologic presentation of PJI and the frequency of appearance. Furthermore, we raised the question of whether the causative microorganisms differ regarding the radiologic presentation.
The first observation of this review is the lack of original data evaluating the radiologic characteristics of PJI of the hip. There are more reviews (n = 26) repeating findings of other studies than original works (n = 18). These reviews mainly concentrate on the diagnosis of PJI, however, they do not focus on the radiographic presentation of PJIs. As described in the section "results", the main statements regarding the radiologic presentation in the reviews are the above-mentioned radiologic pathologies. They do not report on the frequency of the radiologic findings and no correlation to causative microorganisms was analysed. Furthermore, the findings regarding the radiologic presentation of PJI of original works are often coproducts of other primary endpoints [5, 44, 46, 48, 50, 51, 53].
The next interesting finding of this review is the frequency of radiologic abnormalities in the case of a proven PJI of the hip. While some authors report radiographic changes in all of their PJI cases (100%) [44, 45, 47], other authors only presented abnormalities in 14–63% [48,49,50, 57]. Multiple reasons could explain this wide range. Therefore, having a closer look at the original works reporting the frequencies is necessary. The first possible explanation is the lack of a standardized follow-up to classify radiologic changes in the case of PJI. Some authors present radiographs already 6 months after surgery while other authors describe X-rays taken nine years postoperatively. The given collectives are mostly very small with numbers of patients between 6 and 20. Such collectives are not big enough to give sufficient information about the frequency of the appearance of radiological abnormalities.
Furthermore, the oldest and latest works reporting frequencies are separated by more than 40 years of medical evolution [45, 47]. The definition and the diagnostic algorithm have, however, relevantly changed since then and therefore these studies lack comparability [58, 59]. Similarly, the technique of acquiring radiographs has also improved with the advent of digital radiography. This allows post-imaging optimization of each X-ray to visualize also structures such as soft tissues that were difficult to discern in traditional images intended for a good bone contrast only.
When using radiographs not only to exclude differential diagnoses, but also to diagnose a PJI, sensitivity and specificity are crucial. Two original works are reporting about the diagnostic value with similar results. The sensitivity could be classified as low at 20–25% while the specificity of periosteal reactions and periarticular calcifications is moderate to good (79–92%) [5, 52]. Consequently, plain radiographs could be used to confirm PJI in the presence of characteristic radiologic abnormalities. Especially in the case of early PJI, the majority of cases of early PJI radiographs are still usually normal [43]. As a consequence, the question of how to interpret and use radiographs to diagnose late PJIs and the diagnostic value of this technique remains equivocal with the analysed literature.
Having a look at radiographs taken after septic revisions of hip arthroplasties, three original works report heterotopic ossifications. Incidences range depending on the collective analysis between 12 and 84%. Brooker grades presented were mainly between one and three [53, 54, 60]. Interestingly, when comparing aseptic and septic revisions, heterotopic ossifications are significantly more likely in septic cases (11 vs. 84%) and present with significantly higher Brooker grades [54]. Consequently, some kind of interaction between soft tissue and the causing microorganisms can be assumed. This assumption is highlighted by the observation of Rey Fernández et al., that there is an association between higher soft-tissue thickness and risk for PJI after primary total hip replacements. Furthermore, patients with more than 60 mm soft-tissue thickness around the major trochanter had a sevenfold higher risk of PJI [56]. Unfortunately, there are no data available considering the association between the causing microorganisms and soft-tissue changes.
Historically and as presented in the analysed reviews, characteristics that are described to recognize a PJI of the hip on a plain radiograph are periosteal reaction, a wide band of radiolucency at the cement–bone or metal–bone interface, patchy osteolysis, implant loosening, bone resorption around the implant, and transcortical sinus tracts. In cases of aseptic loosening, there is slow and progressive evolution, while in cases of infectious loosening, this loosening occurs rapidly, in a more aggressive manner and with greater bone destruction [7, 61]. Data regarding the frequency of occurrence of the named radiologic abnormalities in cases of PJI are insufficient. Prospective or at least retrospective analyses with larger collectives are necessary to evaluate the frequency and to define the diagnostic value of the radiologic presentation for the diagnosis of PJI. Furthermore, there is a lack of data analysing the association between the causative microorganisms and the radiologic appearance. Although imaging techniques like computer tomography [52, 55, 62] or magnetic resonance imaging [63] have been reported to also provide additional and helpful clues concerning the presence of a PJI such as periosteal reaction, capsule oedema, and intramuscular oedema, the mainstay in diagnosing PJI to date remains plain radiographs.
Conclusion
Typical radiologic abnormalities of PJI are periosteal reaction, a wide band of radiolucency at the cement–bone or metal–bone interface, patchy osteolysis, implant loosening, bone resorption around the implant, and transcortical sinus tracts. The frequency of their occurrence is still inadequately defined. A deeper understanding of the underlying causes and the relation to microorganisms can probably help clinicians in the future to diagnose a PJI. This is why further research should still further evaluate the radiographic features and value in the context of PJI.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available throughout the manuscript.
References
Romano CL, Petrosillo N, Argento G, Sconfienza LM, Treglia G, Alavi A, Glaudemans A, Gheysens O, Maes A, Lauri C, et al. The role of imaging techniques to define a peri-prosthetic hip and knee joint infection: multidisciplinary consensus statements. J Clin Med. 2020;9(8):2548.
Signore A, Sconfienza LM, Borens O, Glaudemans A, Cassar-Pullicino V, Trampuz A, Winkler H, Gheysens O, Vanhoenacker F, Petrosillo N, et al. Consensus document for the diagnosis of prosthetic joint infections: a joint paper by the EANM, EBJIS, and ESR (with ESCMID endorsement). Eur J Nucl Med Mol Imaging. 2019;46(4):971–88.
Signore A, Sconfienza LM, Borens O, Glaudemans A, Cassar-Pullicino VN, Trampuz A, Winkler H, Gheysens O, Vanhoenacker F, Petrosillo N, et al. Correction to: consensus document for the diagnosis of prosthetic joint infections: a joint paper by the EANM, EBJIS, and ESR (with ESCMID endorsement). Eur J Nucl Med Mol Imaging. 2019;46(5):1203.
Rabin DN, Smith C, Kubicka RA, Rabin S, Ali A, Charters JR, Rabin H. Problem prostheses: the radiologic evaluation of total joint replacement. Radiographics. 1987;7(6):1107–27.
Lyons CW, Berquist TH, Lyons JC, Rand JA, Brown ML. Evaluation of radiographic findings in painful hip arthroplasties. Clin Orthop Relat Res. 1985;195:239–51.
Math KR, Zaidi SF, Petchprapa C, Harwin SF. Imaging of total knee arthroplasty. Semin Musculoskelet Radiol. 2006;10(1):47–63.
Tigges S, Stiles RG, Roberson JR. Appearance of septic hip prostheses on plain radiographs. AJR Am J Roentgenol. 1994;163(2):377–80.
Thoren B, Hallin G. Loosening of the Charnley hip. Radiographic analysis of 102 revisions. Acta Orthop Scand. 1989;60(5):533–9.
Humez M, Kotter K, Skripitz R, Kuhn KD. Register data on cemented arthroplasty: a proof for cementless fixation? Orthopadie (Heidelb). 2023;53:163.
Morawietz L, Classen RA, Schroder JH, Dynybil C, Perka C, Skwara A, Neidel J, Gehrke T, Frommelt L, Hansen T, et al. Proposal for a histopathological consensus classification of the periprosthetic interface membrane. J Clin Pathol. 2006;59(6):591–7.
Krenn V, Morawietz L, Perino G, Kienapfel H, Ascherl R, Hassenpflug GJ, Thomsen M, Thomas P, Huber M, Kendoff D, et al. Revised histopathological consensus classification of joint implant related pathology. Pathol Res Pract. 2014;210(12):779–86.
Qu X, Zhai Z, Li H, Li H, Liu X, Zhu Z, Wang Y, Liu G, Dai K. PCR-based diagnosis of prosthetic joint infection. J Clin Microbiol. 2013;51(8):2742–6.
Barrack RL, Jennings RW, Wolfe MW, Bertot AJ. The Coventry Award. The value of preoperative aspiration before total knee revision. Clin Orthop Relat Res. 1997;345:8–16.
Duff GP, Lachiewicz PF, Kelley SS. Aspiration of the knee joint before revision arthroplasty. Clin Orthop Relat Res. 1996;331:132–9.
Deirmengian C, Kardos K, Kilmartin P, Gulati S, Citrano P, Booth RE Jr. The alpha-defensin test for periprosthetic joint infection responds to a wide spectrum of organisms. Clin Orthop Relat Res. 2015;473(7):2229–35.
Unter Ecker N, Koniker A, Gehrke T, Salber J, Zahar A, Hentschke M, Citak M. What is the diagnostic accuracy of alpha-defensin and leukocyte esterase test in periprosthetic shoulder infection? Clin Orthop Relat Res. 2019;477(7):1712–8.
Logroscino G, Fidanza A, Giusti I, Poppa G, Troianello L, Calafiore F, Saracco M, Avigni R, Leone R, Mantovani A, et al. Pentraxin 3, a new biomarker for the diagnosis and management of PJI in primary and revision hip arthroplasty. Acta Biomed. 2023;94(S2): e2023100.
Xing J, Li J, Yan Z, Li Y, Liu X, He L, Xu T, Wang C, Zhao L, Jie K. Diagnostic accuracy of calprotectin in periprosthetic joint infection: a diagnostic meta-analysis. J Orthop Surg Res. 2022;17(1):11.
Ikeda S, Uchiyama K, Minegishi Y, Nakamura M, Takaso M. Evaluation of myeloperoxidase in synovial fluid as a biomarker for chronic periprosthetic joint infection. Int Orthop. 2020;44(10):1915–20.
Sendi P, Muller AM, Berbari E. Are all joints equal? Synovial fluid analysis in periprosthetic joint infection. J Bone Jt Infect. 2018;3(5):258–9.
Howick J CI, Glasziou P, Greenhalgh T, Carl Heneghan, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M. The 2011 Oxford CEBM levels of evidence. Oxford centre for evidence-based medicine. https://cir.nii.ac.jp/all?q=http://www.cebm.net/index.aspx?o%3D5653. 2011. Accessed Mar 2022
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Breitenseher MJ, Mayerhöfer M, Gottsauner-Wolf F, Krestan C, Toma CD, Imhof H. Diagnostic imaging in hip prostheses. Radiologe. 2002;42(6):474–9.
Enayatollahi MA, Parvizi J. Diagnosis of infected total hip arthroplasty. Hip Int. 2015;25(4):294–300.
Enge Júnior DJ, Castro A, Fonseca E, Baptista E, Padial MB, Rosemberg LA. Main complications of hip arthroplasty: pictorial essay. Radiol Bras. 2020;53(1):56–62.
Fritz J, Lurie B, Miller TT. Imaging of hip arthroplasty. Semin Musculoskelet Radiol. 2013;17(3):316–27.
Lee KJ, Goodman SB. Identification of periprosthetic joint infection after total hip arthroplasty. J Orthop Translat. 2015;3(1):21–5.
Lüdemann CM, Schütze N, Rudert M. Diagnosis of periprosthetic hip infections. Oper Orthop Traumatol. 2015;27(3):237–50 (quiz 251).
Miller TT. Imaging of hip arthroplasty. Eur J Radiol. 2012;81(12):3802–12.
Mulcahy H, Chew FS. Current concepts of hip arthroplasty for radiologists: part 2, revisions and complications. AJR Am J Roentgenol. 2012;199(3):570–80.
Mullins MF, Sutton RN, Lodwick GS. Complications of total hip replacement. A roentgen evaluation. Am J Roentgenol Radium Ther Nucl Med. 1974;121(1):55–60.
Parvizi J, Fassihi SC, Enayatollahi MA. Diagnosis of periprosthetic joint infection following hip and knee arthroplasty. Orthop Clin North Am. 2016;47(3):505–15.
Thejeel B, Endo Y. Imaging of total hip arthroplasty: part II–imaging of component dislocation, loosening, infection, and soft tissue injury. Clin Imag. 2022. https://doi.org/10.1016/j.clinimag.2022.09.011.
Hargunani R, Madani H, Khoo M, Fotiadou A, Pressney I, Calleja M, O’Donnell P. Imaging of the painful hip arthroplasty. Can Assoc Radiol J. 2016;67(4):345–55.
Lohmann CH, Rampal S, Lohrengel M, Singh G. Imaging in peri-prosthetic assessment: an orthopaedic perspective. EFORT Open Rev. 2017;2(5):117–25.
Mushtaq N, To K, Gooding C, Khan W. Radiological imaging evaluation of the failing total hip replacement. Front Surg. 2019;6:35.
Song Y, Shao HY, Cheng X, Guo Y. First case of periprosthetic joint infection due to Clostridioides difficile in China. BMC Infect Dis. 2021;21(1):1–5.
Van Odijk J, Marchal G, Baert A, Mulier J, Verhelst M. The radiological images of complications of the total hip arthroplasty. J Belge Radiol. 1974;57(6):429–36.
Segal A, Krauss ES. Infected total hip arthroplasty after intravesical bacillus Calmette-Guerin therapy. J Arthroplasty. 2007;22(5):759–62.
Kinoshita Y, Nakano S, Yoshioka S, Nakamura M, Goto T, Hamada D, Sairyo K. A rare case of extremely severe heterotopic ossification after primary total hip arthroplasty due to persistent mild periprosthetic joint infection. Case Rep Orthop. 2021;2021:8849929.
Awan O, Chen L, Resnik CS. Imaging evaluation of complications of hip arthroplasty: review of current concepts and imaging findings. Can Assoc Radiol J. 2013;64(4):306–13.
Chang CY, Huang AJ, Palmer WE. Radiographic evaluation of hip implants. Semin Musculoskelet Radiol. 2015;19(1):12–20.
Bültmann FJ, Dihlmann W. Radiologically recognisable local complications of alloplastic hip replacement (total prosthesis). Fortschr Geb Rontgenstr Nuklearmed. 1973;119(1):101–7.
Barrack RL, Harris WH. The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am. 1993;75(1):66–76.
Bergström B, Lidgren L, Lindberg L. Radiographic abnormalities caused by postoperative infection following total hip arthroplasty. Clin Orthop Relat Res. 1974;99:95–102.
Rajkumar N, Soundarrajan D, Kumar PC, Dhanasekararaja P, Rajasekaran S. Clinical and radiological outcome of acetabular reconstruction rings in complex primary and revision total hip arthroplasty. Indian J Orthop. 2021;55(5):1267–76.
Ure KJ, Amstutz HC, Nasser S, Schmalzried TP. Direct-exchange arthroplasty for the treatment of infection after total hip replacement. An average ten-year follow-up. JBJS. 1998;80(7):961–8.
Ring PA. Total replacement of the hip joint. A review of a thousand operations. J Bone Joint Surg Br. 1974;56(1):44–58.
Schuldt A, Lehnick D, Agten CA, Beck M, Kist M, Bhure U, del Pérez Sol Lago M, Strobel K. Performance of radiography and single-photon emission computed tomography/computed tomography in painful total hip arthroplasty and impact on arthroplasty survival. Nucl Med Commun. 2020;41(9):875–82.
Sirka A, Clauss M, Tarasevicius S, Wingstrand H, Stucinskas J, Robertsson O, Emil Ochsner P, Ilchmann T. Excellent long-term results of the Müller acetabular reinforcement ring in primary total hip arthroplasty: a prospective study on radiology and survival of 321 hips with a mean follow-up of 11 years. Acta Orthop. 2016;87(2):100–5.
Tapadiya D, Walker RH, Schurman DJ. Prediction of outcome of total hip arthroplasty based on initial postoperative radiographic analysis. Matched, paired comparisons of failed versus successful femoral components. Clin Orthop Relat Res. 1984;186:5–15.
Isern-Kebschull J, Tomas X, García-Díez AI, Morata L, Moya I, Ríos J, Soriano A. Value of multidetector computed tomography for the differentiation of delayed aseptic and septic complications after total hip arthroplasty. Skelet Radiol. 2020;49(6):893–902.
Burastero G, Alessio-Mazzola M, Cavagnaro L, Chiarlone F, Carrega G, Capello AG, Lovisolo S, Felli L. Conservative two-stage revision with primary components of infected total hip arthroplasty: an analysis of survival, clinical and radiographic outcomes. PLoS ONE. 2020;15(10): e0239981.
Manrique J, Alijanipour P, Heller S, Dove M, Parvizi J. Increased risk of heterotopic ossification following revision hip arthroplasty for periprosthetic joint infection. Arch Bone Jt Surg. 2018;6(6):486–91.
Isern-Kebschull J, Tomas X, García-Díez AI, Morata L, Ríos J, Soriano A. Accuracy of computed tomography-guided joint aspiration and computed tomography findings for prediction of infected hip prosthesis. J Arthroplasty. 2019;34(8):1776–82.
Rey Fernández L, Angles Crespo F, Miguela Álvarez SM, Bernaus-Johnson MC, Bartra Ylla A, Font-Vizcarra L. Soft-tissue thickness radiographic measurement: a marker to evaluate acute periprosthetic joint infection risk in total hip replacement. J Bone Jt Infect. 2021;6(6):211–7.
Tigges S, Stiles R, Roberson J. Complications of hip arthroplasty causing periprosthetic radiolucency on plain radiographs. AJR Am J Roentgenol. 1994;162(6):1387–91.
Parvizi J, Tan TL, Goswami K, Higuera C, Della Valle C, Chen AF, Shohat N. The 2018 definition of periprosthetic hip and knee infection: an evidence-based and validated criteria. J Arthroplasty. 2018;33(5):1309-1314 e1302.
Villa JM, Pannu TS, Piuzzi N, Riesgo AM, Higuera CA. Evolution of diagnostic definitions for periprosthetic joint infection in total hip and knee arthroplasty. J Arthroplasty. 2020;35(3S):S9–13.
Rosteius T, Rausch V, Pätzholz S, Lotzien S, Baecker H, Schildhauer TA, Geßmann J. Incidence and risk factors for heterotopic ossification following periprosthetic joint infection of the hip. Arch Orthop Trauma Surg. 2019;139:1307–14.
Temmerman OP, Raijmakers PG, Berkhof J, Hoekstra OS, Teule GJ, Heyligers IC. Accuracy of diagnostic imaging techniques in the diagnosis of aseptic loosening of the femoral component of a hip prosthesis: a meta-analysis. J Bone Joint Surg Br. 2005;87(6):781–5.
Cyteval C, Hamm V, Sarrabere MP, Lopez FM, Maury P, Taourel P. Painful infection at the site of hip prosthesis: CT imaging. Radiology. 2002;224(2):477–83.
Galley J, Sutter R, Stern C, Filli L, Rahm S, Pfirrmann CWA. Diagnosis of periprosthetic hip joint infection using MRI with metal artifact reduction at 1.5 T. Radiology. 2020;296(1):98–108.
Khodarahmi I, Fritz J. Advanced MR imaging after total hip arthroplasty: the clinical impact. Semin Musculoskelet Radiol. 2017;21(5):616–29.
Koutserimpas C, Naoum S, Giovanoulis V, Raptis K, Alpantaki K, Dretakis K, Vrioni G, Samonis G. Fungal periprosthetic hip joint infections. Diagnostics (Basel). 2022;12(10):2341.
Love C, Marwin SE, Palestro CJ. Nuclear medicine and the infected joint replacement. Semin Nucl Med. 2009;39(1):66–78.
Roth TD, Maertz NA, Parr JA, Buckwalter KA, Choplin RH. CT of the hip prosthesis: appearance of components, fixation, and complications. Radiographics. 2012;32(4):1089–107.
Itasaka T, Kawai A, Sato T, Mitani S, Inoue H. Diagnosis of infection after total hip arthroplasty. J Orthop Sci. 2001;6(4):320–6.
Gustilo RB, Pasternak HS. Revision total hip arthroplasty with titanium ingrowth prosthesis and bone grafting for failed cemented femoral component loosening. Clin Orthop Relat Res. 1988;235:111–9.
Riegler HF, Harris CM. Heterotopic bone formation after total hip arthroplasty. Clin Orthop Relat Res. 1976;117:209–16.
Acknowledgements
None.
Registration and protocol
The present review was not registered.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
UH: conception and design, drafting (original and revision); FM: supervision, drafting (revision); GF: literature search, study selection and data extraction, risk of bias assessment; MM: literature search, study selection and data extraction; BF: supervision, drafting (revision). All authors have agreed to the final version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study complies with ethical standards.
Consent to publication
Not applicable.
Competing interests
The authors declare that they have any competing interests for this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hofmann, U.K., Eleftherakis, G., Migliorini, F. et al. Diagnostic and prognostic relevance of plain radiographs for periprosthetic joint infections of the hip: a literature review. Eur J Med Res 29, 314 (2024). https://doi.org/10.1186/s40001-024-01891-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-024-01891-8