
Abstract
Metabolic acidosis is a disorder frequently encountered in emergency medicine and intensive care medicine. As literature has been enriched with new data concerning the management of metabolic acidosis, the French Intensive Care Society (Société de Réanimation de Langue Française [SRLF]) and the French Emergency Medicine Society (Société Française de Médecine d’Urgence [SFMU]) have developed formalized recommendations from experts using the GRADE methodology. The fields of diagnostic strategy, patient assessment, and referral and therapeutic management were addressed and 29 recommendations were made: 4 recommendations were strong (Grade 1), 10 were weak (Grade 2), and 15 were experts’ opinions. A strong agreement from voting participants was obtained for all recommendations. The application of Henderson–Hasselbalch and Stewart methods for the diagnosis of the metabolic acidosis mechanism is discussed and a diagnostic algorithm is proposed. The use of ketosis and venous and capillary lactatemia is also treated. The value of pH, lactatemia, and its kinetics for the referral of patients in pre-hospital and emergency departments is considered. Finally, the modalities of insulin therapy during diabetic ketoacidosis, the indications for sodium bicarbonate infusion and extra-renal purification as well as the modalities of mechanical ventilation during severe metabolic acidosis are addressed in therapeutic management.
Similar content being viewed by others


Introduction
The Henderson–Hasselbalch method defines metabolic acidosis by the presence of an acid–base imbalance associated with a plasma bicarbonate concentration below 20 mmol/L. The association of this imbalance with decreased pH is called “acidemia,” which is often described as severe when the pH is equal to or below 7.20.
Metabolic acidosis is a frequent event in patients receiving emergency treatment or intensive care. Physicians have at their disposal numerous plasma and urine tests to characterize metabolic acidosis, determine its etiology, and refer patients. Acute metabolic acidosis may accompany various diseases and be associated with organ failure, in particular respiratory (increased ventilatory demand) and cardiovascular (arterial vasodilation, decreases in cardiac inotropism and cardiac output, ventricular arrythmia) [1,2,3]. The role of acute metabolic acidosis in these organ failures is mostly suggested by experimental studies in animals or in vitro, as few clinical studies in humans are available [1].
The last consensus conference on the “correction of metabolic acidosis in intensive care” was published in 1999 by the Société de Réanimation de Langue Française (SRLF), with the participation of the Société Française d’Anesthésie et de Réanimation (SFAR), the Société Francophone d’Urgences Médicales (SFUM), the Groupe Francophone de Réanimation et Urgences Pédiatriques (GFRUP), Samu de France, the Société Française de Nutrition Entérale et Parentérale, and the Société de Néphrologie. Point-of-care testing has since grown and enables clinicians to access blood gas measurements very quickly, including in pre-hospital settings. In addition, new data on diagnosis and prognostic tools and the treatment of metabolic acidosis have enriched literature. This is why the SRLF and the Société Française de Médecine d’Urgence (SFMU) propose these formal guidelines on the diagnosis and management of metabolic acidosis. Through analysis of the level of evidence in the literature, the purpose of these guidelines is to specify the diagnostic strategy, referral of patients, and therapeutic management in pre-hospital settings, in the emergency room, and in intensive care.
Method
The guidelines were drawn up by a group of twelve experts convened by the SRLF and the SFMU. The group’s agenda was defined beforehand. The organizing committee first defined the questions to be addressed with the coordinators and then designated the experts in charge of each question. The questions were formulated according to a Patient Intervention Comparison Outcome (PICO) format after a first meeting of the expert group. Literature was analyzed and the guidelines were formulated using Grade of Recommendation Assessment, Development and Evaluation (GRADE) methodology. A level of evidence was defined for each bibliographic reference cited as a function of the type of study and could be reassessed in light of the methodological quality of the study. An overall level of evidence was determined for each endpoint, taking into account the level of evidence of each bibliographic reference, the between-study consistency of the results, the direct or indirect nature of the results, and cost analysis. Three levels of proof were used (Table 1):
-
A high overall level of evidence enabled formulation of a “strong” recommendation (should be done… GRADE 1+, should not be done… GRADE 1−).
-
A moderate, low, or very low overall level of evidence led to the drawing up of an “optional” recommendation (should probably be done… GRADE 2+, should probably not be done… GRADE 2−).
-
When literature was inexistent or insufficient, the question could be the subject of a recommendation in the form of an expert opinion (the experts suggest…).
The proposed recommendations were presented and discussed one by one. The aim was not necessary to reach a single and convergent opinion of the experts on all the proposals, but to define the points of agreement and the points of disagreement or uncertainty. Each expert then reviewed and rated each recommendation using a scale of 1 (complete disagreement) to 9 (complete agreement). The collective rating was done using a GRADE grid. To approve a recommendation regarding a criterion, at least 50% of the experts had to be in agreement and less than 20% in disagreement. For an agreement to be strong, at least 70% of the experts had to be in agreement. In the absence of strong agreement, the recommendations were reformulated and rated again, with a view to reaching a consensus. Only expert opinions that elicited strong agreement were kept.
Areas of recommendations
Three areas were defined: diagnostic strategy, referral of patients, and therapeutic management. A bibliographic search was conducted using the MEDLINE database via PubMed and the Cochrane database. For inclusion in the analysis, the publications had to be written in English or French. The analysis focused on all literature data without imposing a date limit, according to an order of appraisal ranging from meta-analyses to randomized trials to observational studies. The size of the study populations and the relevance of the research were considered for each study.
Summary of results
The summary of the results by the experts according to the GRADE method led to the drawing up of 29 guidelines. Of these guidelines, 4 had a high level of evidence (GRADE 1±) and 10 a low level of evidence (GRADE 2±). The GRADE method was inapplicable to 15 guidelines, which resulted in expert opinions. After two rounds of scoring, a strong agreement was reached for all guidelines. Table 2 provides a summary of the recommendations.
First area: Diagnostic strategy
Should arterial blood gas measurements be performed in the patients with a decreased plasma bicarbonate level when diagnosing acid–base imbalance?
R1.1—The experts suggest that arterial blood gas measurements be performed in patients with a decreased plasma bicarbonate level so as to eliminate respiratory alkalosis, confirm the diagnosis of metabolic acidosis, and test for mixed acidosis (EXPERT OPINION).
Rationale Acidosis is a pathophysiological process that may account for a decrease in blood pH that defines acidemia. Two main mechanisms may be responsible: a decrease in plasma bicarbonate, defining metabolic acidosis, and an increase in PaCO2, defining respiratory acidosis. In the case of metabolic acidosis, the decrease in plasma bicarbonate either reflects the intervention of the buffer system related to an accumulation of non-respiratory acids, or excessive loss of bicarbonate.
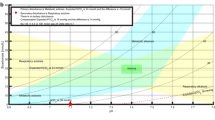
The pH can be kept normal through the decrease in PaCO2 obtained by compensating hyperventilation. Acidemia occurs when respiratory compensation is insufficient. The PaCO2 value that maintains a normal pH, called the expected PaCO2, can be calculated using the formula: expected PaCO2 = 1.5 × [HCO3−] + 8 ± 2 mmHg [4, 5]. Blood gas measurements can be used to assess respiratory compensation and so detect mixed acidemia: pH < 7.38, HCO3− < 20 mmol/L and measured PaCO2 > expected PaCO2.
As the decrease in plasma bicarbonate may also be related to a compensation mechanism of respiratory alkalosis [6], blood gas measurements would allow elimination of respiratory alkalemia: pH > 7.42 and PaCO2 < 38 mmHg.
Most studies that have measured the agreement and limits of agreement between venous and arterial blood gas measurements did not evaluate the clinical superiority of one method with respect to another for diagnosis of metabolic acidosis and were conducted on moderate-sized groups of selected patients. A meta-analysis of studies comparing arterial and venous blood gas measurements in patients in emergency rooms found excellent agreement between the arterial and venous pH (mean difference − 0.033 [95% CI − 0.039 to 0.027]) [7]. A single study of the management of ketoacidosis in the emergency room found that arterial blood gas measurements altered treatment in 3.7% of cases and changed disposition in 1% of cases [8]. These modifications were deemed negligible and the authors concluded that the techniques were equivalent. Very good agreement between arterial and venous measurements of base deficit was also found in trauma patients [9, 10]. Similar results, with a mean pH difference of 0.03 [95% CI − 0.02 to 0.08], were found in critically ill patients with metabolic acidosis of various causes, except ketoacidosis [11].
However, the agreement between venous and arterial blood gas measurements was much poorer for PaCO2. In a meta-analysis of studies comparing arterial and venous PaCO2 values in patients in the emergency room, the mean difference was 4.41 mmHg [95% CI 2.55–6.27], with limits of agreement ranging from − 20.4 to 25.8 mmHg [7].
Is base deficit a better measurement than plasma bicarbonate in diagnosing metabolic acidosis?
R1.2—Measurement of base deficit should probably not be preferred to that of plasma bicarbonate in identifying patients at risk of metabolic acidosis (GRADE 2−, STRONG AGREEMENT).
Rationale Clinical data are scarce and limited (observational, retrospective studies) [12,13,14]. The two largest studies show that if the control group is of patients with a base excess (BE) of −5 mmol/L, corresponding to a base deficit of 5 mmol/L, plasma bicarbonate below 20 mmol/L is a good diagnostic indicator of metabolic acidosis [13, 14]. BE corresponds to the quantity of strong acid (or of strong base in the case of a metabolic acidosis) that should be added in vitro to 1 L of plasma to normalize the pH to 7.40, with a PaCO2 of 40 mmHg and a temperature of 37 °C. There are several methods of calculating BE, but they all use plasma bicarbonate as the main component. Standard base excess (SBE) calculated using the van Slyke equation* takes into account a hemoglobin concentration of 5 g/dL which is the theoretical hemoglobin concentration in the extracellular space of bicarbonate distribution. The van Slyke equation for SBE is the most used clinically, but is not used in comparative studies with plasma bicarbonate. As BE is always calculated from plasma bicarbonate, the correlation between plasma bicarbonate and BE (and hence base deficit) is very strong.
* Van Slyke equation:
Base excess = (HCO3−–24.4) + (2.3 × Hb + 7.7) × (pH − 7.4) × (1 − 0.023 × Hb), with Hb in g/dL.
In case of metabolic acidosis, is the plasma anion gap corrected for albumin better than the uncorrected plasma anion gap in differentiating acid excess from base deficit?
R1.3—The anion gap corrected for albumin should probably be used rather than the uncorrected anion gap to differentiate acidosis related to acid load from acidosis related to base deficit (GRADE 2+, STRONG AGREEMENT).
Rationale Although most clinical data are prospective, they are scarce and observational. Comparisons between the corrected anion gap* (cAG) and the uncorrected anion gap** (AG) show either no difference [15, 16] or superiority of cAG [17,18,19]. Most authors consider that the pathological threshold is cAG or AG > 12 mmol/L. The physiological AG is mainly composed of phosphate and albuminate (weak anion from blood albumin). Consequently, hypoalbuminemia leads to a decrease in plasma albuminate and so to a decrease in AG. Hence, a normal AG associated with hypoalbuminemia corresponds to the presence of plasma acids, which replace albuminate to normalize AG. Taking the albumin level into account in the calculation of AG unmasks plasma acids when there is hypoalbuminemia. So, cAG is greater than AG, particularly in a population of patients with a high risk of hypoalbuminemia, as is the case for patients in intensive care or patients with malnutrition, hepatopathy, chronic inflammation, or urinary loss of albumin.
* cAG = AG + (40 − [albuminemia]) × 0.25, with albuminemia in g/L.
** AG = Na+ − (Cl− + HCO3−) = 12 ± 4 mmol/L (or AG = (Na+ + K+) − (Cl− + HCO3−) = 16 ± 4 mmol/L).
Is the Stewart method equivalent to the Henderson–Hasselbalch method using the anion gap corrected for albumin for the diagnosis of the mechanism of metabolic acidosis?
R1.4—The experts suggest first applying the Henderson–Hasselbalch method using the anion gap corrected for albumin for the diagnosis of the mechanism of metabolic acidosis. However, the Stewart method provides insight into situations unexplained by the Henderson–Hasselbalch method: acid–base imbalance secondary to blood sodium and chloride imbalance and complex disorders (EXPERT OPINION).
Rationale The Henderson–Hasselbalch approach using the anion gap corrected for albumin and the Stewart method was proposed for the identification of causes of acid–base imbalances [17, 20,21,22,23,24]. The anion gap (AG) (or unmeasured anions) requires just a simple and rapid calculation*. At equilibrium, AG does not account for low-level cations that are not measured routinely (Mg2+, Ca2+, H+) and is essentially explained by anions not determined by blood electrolyte measurements (essentially albuminate and phosphate). An increase in AG classically indicates the accumulation of an acid whose anion is not chloride and theoretically corresponds to the accumulation of one of the following compounds: lactate, acetoacetate, hydroxybutyrate, oxalate, glycolate, formate, salicylate, sulfate. However, this reasoning implies that the value of unmeasured anions, essentially albuminate, and more rarely phosphate (Pi), is normal. Indeed, hypoalbuminemia results in a decrease in unmeasured anions and will reduce the anion gap [25]. The accumulation of an anion like lactate or acetoacetate may therefore be missed, because AG is falsely normal. Albumin-correction AG (cAG)** identifies most situations where there is accumulation of an anion other than chloride and hypoalbuminemia [26].
The Stewart approach assumes that the acid–base balance is based on a dissociation of water molecules that depends on three independent variables: PaCO2, the strong ion difference which corresponds to the difference between strong cations and strong anions (apparent SID (appSID) = Na+ + K+ + Ca2+ + Mg2+ − Cl−) and the sum of non-volatile weak acids present in dissociated or undissociated form (Atot) defined by [albumin × (0.123 × pH − 0.631) + [Pi × (0.309 × pH − 0.469]. Use is made of the effective SID: eff SID = HCO3− + albuminate− + Pi− = HCO3− + Atot. Respiratory acid–base disturbances are exclusively defined by increased PaCO2. The approach to metabolic acid–base disturbances requires calculation of the strong ion gap (SIG), which is equal to appSID—eff SID. In the Stewart model, given that electrical neutrality must be respected, the variation in bicarbonate concentration is the consequence of the acid–base disturbance and not its cause unlike the hypothesis of Henderson–Hasselbalch model. A positive SIG indicates the presence of unmeasured anions and so of metabolic acidosis [27,28,29]. The Stewart approach appears at least equivalent to the Henderson–Hasselbalch approach in the case of accumulation of endogenous or exogenous acid or loss of bicarbonate [17, 20, 22, 25]. However, the Stewart approach sheds light on metabolic disorders secondary to blood sodium and chloride levels, such as hyperchloremic acidosis associated with saline fluid resuscitation, which the Henderson–Hasselbalch approach explains less easily [23, 26], and on complex disorders (hyperlactatemia at normal pH and BE) [30,31,32].
* AG = Na+ − (Cl− + HCO3−) = 12 ± 4 mmol/L (or AG = (Na+ + K+) − (Cl− + HCO3−) = 16 ± 4 mmol/L).
** cAG = AG + (40 − [blood albumin]) × 0.25, with blood albumin in g/L.
Does the use of a diagnostic algorithm improve etiological diagnosis of metabolic acidosis?
R1.5—The experts suggest using an algorithm to improve the etiological diagnosis of metabolic acidosis (EXPERT OPINION) (Fig. 1).

Algorithm recommended by the experts for etiological diagnosis of metabolic acidemia (EXPERT OPINION)
Rationale Few studies have evaluated the diagnostic impact of the use of an algorithm in metabolic acidosis, so it is difficult to provide a well-argued answer to the question. It is always essential to collect data by clinical history taking and physical examination [33]. Apart from the exceptions mentioned below, the use of an algorithm could subsequently be used to investigate simple settings of acidosis [28]. However, it is important to know if there are artifacts [34] or atypical [35], complex [33], or misleading clinical pictures [30, 36]. Acetylsalicylic acid poisoning associates initial respiratory alkalosis with metabolic acidosis responsible for an increase in the anion gap which is only partly explained by the accumulation of acetylsalicylic acid [33]. The increased anion gap acidosis seen in ethylene glycol poisoning is in part due to the accumulation of glycolic acid, which some laboratory analyzers misidentify as lactate [34, 37]. Diabetic ketoacidosis may be accompanied by hyperchloremic acidosis at hospital admission or a few hours after admission [35]. The association of lactate production with vomiting may lead to the clinical picture of metabolic alkalosis [30]. Abundant infusion of chloride-rich fluid during circulatory insufficiency associated with hyperlactatemia produces hyperchloremic acidosis [30, 38]. It is important to remember that the respiratory compensation observed in acute metabolic acidosis cannot correct the pH value beyond 7.40 (Fig. 1). Main causes of hyperlactatemia are listed in Table 3.
If no etiology is found, a hereditary metabolic disorder may be considered.
Should the urinary anion gap always be calculated in metabolic acidosis?
R1.6—The experts suggest that the urinary anion gap should only be calculated in metabolic acidosis without unmeasured anions or obvious etiology (EXPERT OPINION).
Rationale The urinary anion gap, calculated as the sum of measured anions and cations (Na+ + K+ + Cl−), was proposed for estimation of the urinary excretion of ammonium (NH4+) [39,40,41]. In acidosis with a normal anion gap, ammonium distinguishes between acidosis related to gastrointestinal loss of bicarbonate (negative urinary anion gap), acidosis linked to tubular acidosis, or hyporeninemic hypoaldosteronism (zero or increased anion gap) [39,40,41].
The diagnostic utility of the urinary anion gap, notably in the emergency room or in intensive care is, however, questionable. First, outside intensive care, the performance of this index is only validated by studies of very low level of evidence [6, 40, 41]. The urinary anion gap seems to be correlated with NH4+ excretion [28], but the correlation is weak, the reported variability is substantial, and none of the available studies adjust for confounding factors or report the diagnostic performance [6, 40, 41]. Second, the discriminating character and the contribution to diagnosis are not evaluated. Lastly, most studies conducted in the emergency room or in intensive care have not evaluated this parameter [22, 23, 27].
A single study suggests a high prevalence of tubular acidosis in intensive care. It is of low level of evidence, as the parameter used (urinary anion gap) is also a diagnostic criterion of the expected clinical picture (tubular acidosis) [42].
Should urinary pH always be measured in metabolic acidosis?
R1.7—The experts suggest that measurement of urinary pH should be restricted to patients with metabolic acidosis without unmeasured anions or obvious etiology, and with a strong clinical suspicion of tubular acidosis (EXPERT OPINION).
Rationale The measurement of urinary pH is less well validated than calculation of the urinary anion gap. Its diagnostic value is controversial and seems more restricted [28, 36, 39, 41].
Is measurement of venous lactate less effective than measurement of arterial lactate in diagnosing hyperlactatemia?
R1.8—The experts suggest that a normal value of venous lactate discounts hyperlactatemia (EXPERT OPINION).
R1.9—Arterial lactate should probably be measured to confirm hyperlactatemia in case of increased venous lactate (GRADE 2+, STRONG AGREEMENT).
Rationale Measurement of arterial lactate is the reference method for determining blood lactate. Venous blood is more easily sampled than arterial blood and less painful for the patient. Several studies have evaluated the agreement between measurements of venous and arterial blood lactate. A 2014 meta-analysis included three of these studies [7]. They were prospective or retrospective cohort studies involving patient selection bias (non-consecutive patients), blood lactate was rarely above 4 mmol/L, and the measurement equipment and sampling conditions differed from one study to another. The mean bias in the results ranged from − 0.016 to 1.06 mmol/L. The Bland–Altman limits of agreement ranged from − 1.51 to 2.65 mmol/L. These biases and limits, reported for the usual lactate values, show that measurement of venous lactate is inadequate for the diagnosis of hyperlactatemia.
Measurement of venous lactate has also been assessed in prognostic cohort studies of patients with severe trauma, suspected septic shock, or admitted to the emergency room [43,44,45,46]. The study populations were not all comparable and the results were not unequivocal, in particular for venous lactate values below 4 mmol/L. On the other hand, it seems that a venous lactate value above 4 mmol/L was strongly associated with an increased risk of death.
In conclusion, whereas the measurement of venous lactate can be useful in determining the prognosis, the literature data do not support its use in the diagnosis of hyperlactatemia.
Is the measurement of capillary blood lactate as effective as measurement of arterial lactate in diagnosing hyperlactatemia?
R1.10—Capillary blood lactate should not be measured to diagnose hyperlactatemia (GRADE 1−, STRONG AGREEMENT).
Rationale The measurement of capillary blood lactate is less invasive and faster than measurement of arterial lactate. Several cohort studies have compared these two methods of measurement. Mean bias ranged from − 0.99 to 2.4 mmol/L. The Bland–Altman limits of agreement ranged from − 5.6 to 5.4 mmol/L [47,48,49,50,51]. These results are difficult to analyze because different measuring equipment was used and there are inconsistencies between the results [52]. Measurement of capillary blood lactate is therefore insufficiently efficient and does not allow sufficiently accurate determination of arterial lactate.
Measurement of capillary blood lactate has been proposed as a prognostic tool. Most studies, conducted before hospital admission or upon admission to the emergency room, have combined several sampling techniques (venous and capillary). Few studies have analyzed measurement of capillary blood lactate as a prognostic tool for patients with severe trauma or suspected septic shock [44, 47, 53]. These studies were of low level of evidence and do not allow a conclusion to be drawn regarding the prognostic value of measurement of capillary blood lactate.
Hyperlactatemia occurs when there is an imbalance between lactate production and clearance [54]. Traditionally, the causes of hyperlactatemia have been divided into two groups: associated with tissue hypoxia (type A) and without tissue hypoxia (type B) [55, 56]. However, the mechanism can be mixed and the same etiology can be found in both groups [57].
Is measurement of capillary blood ketones more effective than measurement of urine ketones in diagnosing ketoacidosis?
R1.11—Capillary blood ketones rather than urine ketones should be measured when diagnosing ketoacidosis (GRADE 1+, STRONG AGREEMENT).
Rationale Studies comparing urine ketones and blood ketones are all observational. There is just one randomized controlled prospective study, but it evaluated the incidence of hospitalization/emergency assessment among patients with type 1 diabetes depending on self-measurement of blood ketones or urine ketones [58]. Most studies have included patients presenting to the emergency room because of a hyperglycemic episode (blood glucose generally > 2.5 g/L). The diagnostic criteria of diabetic ketoacidosis varied from one study to another, which makes comparison difficult. Whatever their quality, all the studies found greater specificity and a quicker diagnostic result with capillary blood ketones, for a comparable sensitivity. In addition, urine ketones may persist in the absence of significant blood ketones. Lastly, measurement of urine ketones determines only acetoacetate, whereas measurement of blood ketones determines solely beta-hydroxybutyrate, which is the predominant ketone body in the case of diabetic ketosis. Depending on the various cut-offs reported, blood ketones above 3 mmol/L associated with hyperglycemia constitute a good diagnostic criterion of diabetic ketoacidosis [59,60,61,62,63].
Second area: Patient assessment and referral
In case of metabolic acidosis, is the pH value useful to identify critically ill patients?
R2.1—The pH value should probably not be used alone to identify critically ill patients (GRADE 2−, STRONG AGREEMENT).
Rationale The blood pH is a fundamental laboratory parameter. Its value depends not only on metabolic or respiratory variations, but also on the site of arterial, venous, or capillary blood sampling. Clinical studies of the prognostic utility of blood pH in emergency medicine have used analysis of venous or arterial blood. The emergence of new tools for point-of-care measurement of pH has yielded recent published studies of its prognostic value before hospital admission. These observational studies essentially related to non-traumatic cardiac arrest and most failed to show a prognostic utility of the isolated measurement of pH [64, 65]. However, there is a need to assess pH combined with other clinical and biochemical parameters. Most in-hospital studies were observational, were limited by small numbers of patients, and assessed very different diseases (cardiac arrest, trauma, pneumonia, diabetic ketoacidosis). Most of them failed to show any prognostic value of pH measurement [8, 66, 67]. Only those studies of acute community-acquired pneumonia underscored the utility of the measurement of blood pH, but in the context of severity scores combined with other parameters [68, 69].
Is lactate measurement useful to identify critically ill patients?
R2.2—Hyperlactatemia, whatever its value, should be considered as a marker of severity in initial treatment. Diagnostic and therapeutic management should be rapid and multidisciplinary if needed (GRADE 1+, STRONG AGREEMENT).
R2.3—Increase in blood lactate should probably be monitored in the first hours of management so as to assess the response to treatment (GRADE 2+, STRONG AGREEMENT).
Rationale Numerous studies show an association between initial blood lactate and the prognosis of septic shock and trauma. They are mostly retrospective cohort studies or prospective observational studies. Their methodologies are often questionable and their levels of proof limited. Nonetheless, all the studies agree on the utility of early measurement of arterial or venous lactate in evaluating the severity of septic shock and the need for critical care [70]. Hyperlactatemia is an independent index of severity and an initial lactate level above 4 mmol/L in septic shock [71] and above 2 mmol/L in trauma patients [72,73,74] is always associated with a worse prognosis [71, 75].
Several studies report the additional prognostic usefulness of plasma lactate decrease (clearance). The best cut-off seems to be 30% lactate clearance at the sixth hour of treatment in septic shock [76]. Likewise, no lactate decrease or a decrease of less than 20% in the first 2- to 4-h is associated with a worse prognosis in trauma patients [77].
Initial hyperlactatemia is also associated with a greater treatment burden. Pre-admission measurement of lactate improves identification of patients needing intensive care [43].
Does intensive monitoring of patients with diabetic ketoacidosis improve prognosis?
R2.4—The experts suggest close monitoring of patients with diabetic ketoacidosis, ideally in intensive care unit (EXPERT OPINION).
Rationale The indication for admission to intensive care is clear in the case of organ failure associated with ketoacidosis. However, for several decades certain studies have suggested that patients with uncomplicated diabetic ketoacidosis can be managed by conventional hospital care [78,79,80]. One retrospective cohort study in over 15,000 patients in 159 American hospitals showed that the use of intensive care for diabetic ketoacidosis patients was not associated with differences in mortality or length of hospital stay [81]. However, the results are difficult to interpret and generalize as it was a retrospective study based on coding data in which no clinical or paraclinical finding concerning the severity of ketoacidosis was provided. Moreover, the criteria of admission to intensive care were not indicated. As continuous intravenous insulin therapy is generally necessary and potentially serious complications can appear during therapeutic management (hypokalemia, hypoglycemia, pulmonary edema, cerebral edema), close clinical and paraclinical monitoring is indispensable. Since this monitoring may be compromised in conventional hospital care because of organizational difficulties, patients with diabetic ketoacidosis should be admitted to intensive care so as to adapt the treatment and watch for potential side effects.
Third area: Therapeutic management
During diabetic ketoacidosis, what route of insulin delivery should be preferred?
R3.1—Insulin should probably be administered intravenously rather than subcutaneously in patients with diabetic ketoacidosis (GRADE 2+, STRONG AGREEMENT).
Rationale Two literature reviews have considered the optimal route for administration of insulin in diabetic ketoacidosis [82, 83]. Four controlled and randomized trials compared subcutaneous (SC) insulin with intravenous (IV) insulin in management of diabetic ketoacidosis in adults [84,85,86,87]. All evaluated the rate of correction of acidosis or the normalization of blood glucose. Three evaluated the length of hospital stay [85,86,87]. A lack of precision in the reported results meant that one of these studies [84] could not be included in the meta-analysis of the rate of correction of acidosis or normalization of blood glucose. This trial described a correction of ketosis and a significantly greater decrease in blood glucose at 2 h in the IV group, but non-significant results 4, 6, and 8 h after the start of therapeutic management. A meta-analysis of two trials comparing similar insulins [85, 87] found no significant difference in the rate of correction of acidosis or the normalization of blood glucose (difference = 0.2 h; 95% confidence interval [− 1.7–2.1]; p = 0.81). The last trial [86] reported similar results (d = − 1 h [− 3.2–1.2]; p = 0.36). The meta-analyses found no significant difference in the effect of the route of administration on the length of hospital stay. The literature data do not show that IV insulin therapy is preferable to SC insulin therapy, in terms of the rate of correction of acidosis, the normalization of blood glucose, or the length of hospital stay. However, few patients were included and they presented uncomplicated ketoacidosis. In addition, SC injections of insulin were performed regularly and the frequency of injections could be a source of discomfort or even pain.
As a venous route was often necessary, the continuous IV route seems preferable so as to facilitate restoration of water–electrolyte balance, avoid repeated SC injections, and reduce the risk of hypoglycemia, while ensuring better control of the insulin dose administered.
During diabetic ketoacidosis, should an insulin bolus be administered before starting continuous intravenous insulin therapy?
R3.2—An insulin bolus should probably not be administered before starting continuous intravenous insulin therapy in patients with diabetic ketoacidosis (GRADE 2−, STRONG AGREEMENT).
Rationale A literature review of the use of an initial insulin bolus before initiation of continuous intravenous insulin therapy identified just one randomized controlled trial [88] and one observational study [89]. In the latter, the normalization of blood glucose and the length of hospital stay did not differ significantly between the bolus and non-bolus groups (change in blood glucose 60.1 ± 38.2 vs 56.0 ± 45.4 mg/dL/h, respectively; p = 0.54; length of hospital stay 5.6 ± 5.3 vs 5.9 ± 6.9 days; p = 0.81). The authors noted more cases of hypoglycemia in the bolus group, but the difference was not statistically significant (6 vs 1%; p = 0.12). The randomized controlled trial compared three groups: a low-dose insulin bolus then a low insulin dose (0.07 IU/kg, then 0.07 IU/kg/h), a low insulin dose without an initial bolus (0.07 IU/kg/h), and double-dose insulin (0.14 IU/kg/h) without an initial bolus. The rate of correction of acidosis, the normalization of blood glucose, and the length of hospital stay did not differ between the three groups. It is important to note that this study did not evaluate the insulin dose commonly used in continuous intravenous administration, i.e., 0.1 IU/kg/h.
During diabetic ketoacidosis, should high or low continuous intravenous insulin doses be administered?
R3.3—Low continuous intravenous insulin doses should probably be administered in the treatment of diabetic ketoacidosis (GRADE 2+, STRONG AGREEMENT).
R3.4—The experts suggest using an initial dosage of 0.1 IU/kg/h without exceeding 10 IU/h, and to increase it in the absence of hypokalemia, if the targets for correction of blood ketones (0.5 mmol/L/h), bicarbonate (3 mmol/L/h), and capillary blood glucose (3 mmol/L/h) are not reached after the first hours of treatment (EXPERT OPINION).
Rationale The literature data, essentially from the 1970s, indicate that low continuous intravenous insulin doses are as effective as higher doses [90, 91]. A literature review found two trials (with no control group) reporting a decrease in blood glucose that was similar for low and high insulin doses. The risk of hypokalemia, hypoglycemia, or cerebral edema possibly associated with high doses and efficacy of low doses have justified their use in practice for several decades. However, if the targets for correction of blood ketones (0.5 mmol/L/h) or failing that of bicarbonate (3 mmol/L/h) and blood glucose (3 mmol/L/h) are not reached, it is possible to envisage increased doses, provided there is no hypokalemia.
Should sodium bicarbonate infusion be used in severe metabolic acidosis and, if so, in what situations?
R3.5—The experts suggest administering sodium bicarbonate to compensate for gastrointestinal or renal base loss in case of poor clinical tolerance (EXPERT OPINION).
Rationale The administration of sodium bicarbonate could limit the deleterious cardiovascular, respiratory, and cellular energy effects of loss of bicarbonate [2]. Sodium bicarbonate should be administered carefully as it is associated with a risk of hypokalemia, hypernatremia, hypocalcemia, rebound alkalemia, and water–sodium overload [2].
R3.6—Sodium bicarbonate should probably be administered to intensive care patients with severe metabolic acidemia (pH ≤ 7.20, PaCO2 < 45 mmHg) and moderate to severe acute renal insufficiency (GRADE 2+, STRONG AGREEMENT).
Rationale Metabolic acidosis accompanying states of shock is often multifactorial, with hyperlactatemia and renal insufficiency being involved first and foremost, plus potentially associated loss of bicarbonate. Several retrospective, observational, single-center [92,93,94] or prospective, multicenter studies [95] were insufficient to draw conclusions regarding the role of sodium bicarbonate. Two randomized, prospective, crossover, single-center physiological studies in 10 [96] and 14 patients [97] concluded that administration of sodium bicarbonate did not have a more favorable effect than saline solution on hemodynamic parameters measured by pulmonary arterial catheter in patients with metabolic lactic acidosis (blood bicarbonate ≤ 22 or 17 mmol/L and arterial blood lactate > 2.5 mmol/L).
A controlled, randomized, prospective multicenter study in 400 patients (pH ≤ 7.20, blood bicarbonate ≤ 20 mmol/L and PaCO2 ≤ 45 mmHg and blood lactate > 2 mmol/L or SOFA score > 4) compared the effect of sodium bicarbonate administration (4.2% q.s. pH ≥ 7.30) with the absence of such administration on a principal composite endpoint (day-28 mortality and/or presence of at least one organ failure at day 7, according to the SOFA score). The authors reported no effect of alkalinization (71% of patients in the control arm and 66% of patients in the bicarbonate arm reached the composite endpoint; the estimated absolute difference was − 5.5% ([95% CI − 15.2% to 4.2%], p = 0.24). The probability of day 28 survival was 46% [95% CI − 40% to 54%] in the control group and 55% [95% CI 49% to 63%]; p = 0.09 in the bicarbonate group.
In the a priori defined stratum “acute renal insufficiency—AKIN 2–3,” 74 (82%) of the 90 patients of the control group and 64 (70%) of the 92 patients of the bicarbonate group reached the composite endpoint (estimated absolute difference: − 12.3%, 95% CI − 26.0% to − 0.1%; p = 0.0462). The probability of survival at day 28 was 46% [95% CI 35% to 55%] in the control group and 63% [95% CI 52% to 72%] in the bicarbonate group (p = 0.0283).
These results were confirmed in multivariate analysis. In the general population and the “acute renal insufficiency” stratum, the patients randomized to the control arm received renal replacement therapy (RRT) more often and for longer than the patients of the bicarbonate arm (52% need for RRT in the control arm vs 35% in the bicarbonate arm, p < 0.001) [98].
R3.7—Sodium bicarbonate should not be administered routinely in the therapeutic management of circulatory arrest, apart from pre-existing hyperkalemia or poisoning by membrane stabilizers (GRADE 1−, STRONG AGREEMENT).
Rationale Since the 1999 French consensus conference, the role of sodium bicarbonate alkalinization in the therapeutic management of the cardiac arrest has been evaluated in 5 retrospective studies [99,100,101,102,103] and a prospective, randomized, double-blind, controlled multicenter study [104]. Four retrospective studies showed an increase in the frequency of resumption of spontaneous circulatory activity in patients treated with sodium bicarbonate [99, 101,102,103] and one reported decreased hospital survival in patients treated with sodium bicarbonate [100]. The randomized clinical trial (792 patients) found no difference in survival between the patients treated with sodium bicarbonate (7.4%) and those receiving a placebo (6.7%, p = 0.88). The use of sodium bicarbonate in patients could be reserved for pre-existing hyperkalemia or poisoning by membrane stabilizers [105].
R3.8—Sodium bicarbonate should probably not be administered to patients with diabetic ketoacidosis (GRADE 2−, STRONG AGREEMENT).
Rationale The administration of sodium bicarbonate transiently increases pH and may limit the deleterious cardiovascular and cellular energy effects of acidemia. However, the administration of sodium bicarbonate is associated with a risk of hypokalemia, hypernatremia, hypocalcemia, rebound alkalemia, and water–sodium overload [2]. A pathophysiological study in 39 patients has recently shown altered microvascular endothelial reactivity at the acute phase of diabetic ketoacidosis. This endothelial dysfunction was more marked when the arterial pH was below 7.20 and the vascular reactivity improved after 24 h of treatment. However, the administration of sodium bicarbonate was not tested in this observational study [106].
Since the 1999 French consensus conference, the role of sodium bicarbonate alkalinization in therapeutic management of ketoacidosis was reassessed in a retrospective single-center study [107] comparing 44 patients treated with bicarbonate and 42 untreated patients. The authors found no effect of sodium bicarbonate on the rate of correction of acidemia, as in previous studies, all of which were conducted in small populations [108].
R3.9—The experts suggest administering sodium bicarbonate in the therapeutic management of salicylate poisoning, whatever the pH value (EXPERT OPINION).
Rationale Salicylate poisoning is rare and potentially fatal. Toxicological expertise is needed to ensure optimal therapeutic management. The aim of bicarbonate administration is twofold: induce alkalemia to limit the passage of salicylate into the central nervous system and alkalinization of urine to promote renal excretion of salicylate [109, 110]. An old observational study in a small number of patients suggested that simple alkalinization leads to renal excretion of salicylate equal to or even greater than that of forced diuresis, alkaline diuresis, or not [111]. The administration of sodium bicarbonate should be subject to close monitoring as it is associated with a risk of hypokalemia, hypernatremia, hypocalcemia, alveolar hypoventilation, and fluid overload [2, 109]. In the case of severe poisoning, the experts suggest renal replacement therapy (cf. R3.13) and continued alkalinization between renal replacement therapy sessions until salicylate is completely eliminated.
Should renal replacement therapy be used in severe metabolic acidosis, and if so in what situations?
R3.10 In case of shock and/or acute renal insufficiency, the experts suggest initiation of renal replacement therapy if the pH is below or equal to 7.15 in the absence of severe respiratory acidosis and despite appropriate treatment (EXPERT OPINION).
Rationale There are no randomized controlled studies with mortality as the main endpoint that compare the initiation or not of renal replacement therapy in severe metabolic acidosis. The recommendations presented here come mostly from retrospective observational studies and case reports.
According to a questionnaire administered by the European Society of Intensive Care Medicine, 74% of intensivists consider metabolic acidosis (without indication of severity) to be a criterion for initiation of renal replacement therapy [112].
The plasma bicarbonate or pH cut-off authorizing renal replacement therapy could be deduced from the results of randomized studies comparing the effect on mortality of early or delayed initiation of renal replacement therapy in acute renal insufficiency. In 101 surgery patients, Wald et al. [113] found no difference in mortality as a function of the timing of renal replacement therapy, and plasma bicarbonate at its initiation was similar in the two groups: 20.7 ± 4.3 vs 20.1 ± 4.4 mmol/L. In 231 surgery patients with KDIGO stage-2 acute renal insufficiency, Zarbock et al. [114] found at initiation of renal replacement therapy similar plasma bicarbonate levels in the early and late arms: 20.9 ± 3.6 mmol/L vs 20.7 ± 3.7 mmol/L. Mortality was significantly lower in the early initiation group.
In the AKIKI study [115] in 619 patients with KDIGO stage-3 acute renal insufficiency, intention-to-treat analysis showed that pH and plasma bicarbonate were significantly lower in the late renal replacement therapy group (hard criteria for renal replacement therapy, including pH ≤ 7.15, rate of renal replacement therapy: 50%) than in the early renal replacement therapy group (6 h after inclusion, rate of renal replacement therapy: 100%): bicarbonate 16.6 ± 5.6 vs 18.9 ± 4.9 mmol/L (p < 0.001) and pH 7.25 ± 0.15 vs 7.30 ± 0.12 (p < 0.001). There was no difference in mortality between groups.
The IDEAL ICU study [116] included 488 septic shock patients with RIFLE stage F acute renal insufficiency randomized to 2 arms (renal replacement therapy started within 12 h following inclusion, rate of renal replacement therapy 97% versus renal replacement therapy started 48 h after inclusion in the absence of resolution of acute renal insufficiency, rate of renal replacement therapy: 62%). There was no difference in mortality (58 vs 54%) and the study was stopped as medical care was deemed futile. A pH ≤ 7.15 was a criterion for initiation of renal replacement therapy. Of the 41 patients in the late arm, 20 had a pH of 7.10.
The BICAR-ICU study [98] compared intravenous administration of 4.2% sodium bicarbonate (q.s. pH > 7.30) with a control arm without infusion of bicarbonate in patients with severe metabolic acidosis (pH ≤ 7.20, bicarbonate < 20 mmol/L and PaCO2 ≤ 45 mmHg) and a SOFA score ≥ 4 or arterial blood lactate ≥ 2 mmol/L. This randomized, controlled, intention-to-treat study was stratified according to age, AKIN stage 2 or 3 acute renal insufficiency, and septic shock. Renal replacement therapy was used if 2 of the 3 following criteria applied: pH < 7.20 after 24 h, hyperkalemia, or urine output < 0.3 mL/kg/h over 24 h. In the acute renal insufficiency sub-group of 182 patients, the probability of survival at day 28 was 46% [95% CI 35% to 55%] in the control group and 63% [95% CI 52% to 72%] in the bicarbonate group (p = 0.0283).
R3.11—In case of lactic acidosis suggestive of metformin poisoning, the experts suggest early initiation of renal replacement therapy when there is an organ dysfunction or in the absence of improvement in the first hours of therapeutic management (EXPERT OPINION).
Rationale Metformin-associated lactic acidosis is defined by arterial lactate above 5 mmol/L and pH below 7.35 during metformin treatment. Its incidence is low: from 10 to 12/100,000 [117, 118]. A 2015 literature review identified 175 publications (no randomized trial) reporting high mortality (30 to 50%) [119].
Yeh H-C et al. [117] collated case reports and studies from 1977 to 2014 (3 studies, 142 case reports) in 253 patients and found a mortality of 16.2%. Factors associated with mortality were mechanical ventilation and lactate level (17 vs 22 mmol/L, p < 0.01), but not pH, plasma bicarbonate, or level of metformin. A lactate level above 20 mmol/L was significantly associated with mortality.
A retrospective study conducted in Northern Italy from 2010 to 2015 collated 117 cases and reported 78.3% survival [118]. On average, at initiation of renal replacement therapy, the pH was below 7.04 and blood lactate above 12 mmol/L.
As the metformin dose is not always available and its prognostic value is subject to discussion [119], renal replacement therapy should be initiated without delay when there is an organ dysfunction or when there is no improvement in the first hours of therapeutic management. Renal replacement therapy is intended to correct water–electrolyte and acid–base disturbances and to ensure metformin clearance [119].
R3.12—In case of methanol or ethylene glycol poisoning, the experts suggest initiation of renal replacement therapy if the anion gap is above 20 mEq/L or if there is renal insufficiency or visual impairment (EXPERT OPINION).
Rationale Methanol poisoning and ethylene glycol poisoning are rare and potentially fatal. Expertise is needed to ensure optimal therapeutic management including, if necessary, specific intensive care procedures.
In alcohol poisoning (methanol and ethylene glycol), the pH at admission is correlated with the prognosis [120, 121]. A pH below 7.0 is predictive of death [122], whereas a pH above 7.22 is associated with survival [123]. The plasma anion gap (> 24 mEq/L or > 20 mEq/L in the case of hemodynamic instability) is correlated with the level of formate and with the prognosis [124].
Circulating methanol is removed by the kidney with a clearance of about 5 to 6 mL/min, which represents approximately 25 to 50% of its systemic elimination before its conversion to formic acid (responsible for the toxicity). This conversion is inhibited by intravenous administration of ethanol or fomepizole. The clearance of methanol achieved by intermittent hemodialysis ranges between 77 and 400 mL/min, and between 17 and 48 mL/min if renal replacement therapy is continuous [125, 126].
R3.13—In metabolic acidosis associated with salicylic acid poisoning, the experts suggest initiation of renal replacement therapy when there is neurological involvement and/or if the salicylic acid concentration is above 6.5 mmol/L (90 mg/dL) and/or if the pH is less than or equal to 7.20 (EXPERT OPINION).
Rationale Salicylate poisoning is rare and potentially fatal. Expertise is needed to ensure optimal therapeutic management comprising, if necessary, specific intensive care procedures.
A 2015 literature review by a group of experts [110] found 84 publications, 80 of which related to case reports or patient cohorts and to a randomized controlled trial, and collated 143 patients with salicylate poisoning. The authors concluded that salicylic acid is highly dialyzable and that intermittent hemodialysis is the preferred modality. They also concluded that development of acidemia should be considered as a warning sign because it indicates the onset of an organ dysfunction (lactic acidosis, ketoacidosis, renal, and/or respiratory insufficiency). In addition, the presence of acidemia increases the entry of salicylate into the central nervous system and the risk of cerebral edema.
A more recent retrospective study [127] in 56 mechanically ventilated patients with blood salicylate above 50 mg/dL reported 76% mortality. Failure to use renal replacement therapy was associated with increased mortality and survival was zero when blood salicylate was above 5.8 mmol/L, i.e., 80 mg/dL. However, no data were available on potential poisoning with other compounds or on the causes of death.
Given the limited volume and quality of the data, it is difficult to determine a toxic threshold accurately. However, it appears that above 6.5 mmol/L (90 mg/dL) the risk of death is high, even in the absence of clinical signs.
Should minute ventilation be increased in mechanically ventilated patients with metabolic acidosis?
R3.14—The experts suggest compensating for acidemia by increasing respiratory frequency without inducing intrinsic positive end-expiratory pressure, with a maximum of 35 cycles/min and/or a tidal volume up to 8 mL/kg of body mass, and by monitoring plateau pressure. The aim of ventilation is not to normalize pH. A target pH greater than or equal to 7.15 seems reasonable. Medical treatment of metabolic acidosis and of its cause should be envisaged concomitantly, as ventilatory compensation can only be symptomatic and temporary (EXPERT OPINION).
Rationale The control of breathing brings into play three types of interconnected structures: the control center commonly called the “respiratory centers” in the central nervous system at the level of the brainstem; the motor components of the respiratory system comprising the muscles of the upper airways, the thoracic cage, and the abdomen; and the receptors (chemoreceptors, muscle proprioceptors, airway and lung receptors) that transmit setpoints constantly to the respiratory centers (PCO2, pH, lung distension, respiratory muscle load…). Thus, the respiratory centers receive sensory and humoral information that enables homeostasis, while optimizing the energy cost of each respiratory cycle. The central chemoreceptors on the ventral side of the brainstem respond rapidly and strongly to minimal variations in the pH and PCO2 of the cerebrospinal fluid and blood. The hydrogen ion seems to be a determinant stimulus [128].
In metabolic acidosis, the physiological response is an increase in alveolar ventilation [129] that is constant, whatever the cause and severity of acidosis [130]. The stimulation of chemoreceptors in metabolic acidosis is responsible for an increase in tidal volume rather than tachypnea [130, 131]. Its efficacy depends not only on alveolar ventilation, but also on the hemodynamic state and integrity of the respiratory system [129, 132].
As yet there are no specific data concerning ventilatory management of intubated-ventilated patients with metabolic acidosis. Though acidosis is conventionally associated with a poor prognosis [133], it has potentially protective effects. Apart from the severity of acidosis, its mechanism and how it arises seem to be prognostic factors that should be taken into account.
The correction of metabolic acidosis by increasing respiratory frequency and/or tidal volume is questionable. Current data on protective ventilation are abundant and recommend keeping a tidal volume of about 6 mL/kg of body mass. Given the hemodynamic effects of metabolic acidosis, it seems reasonable to adapt the respiratory frequency to achieve a pH greater than or equal to 7.15 [134,135,136], without exceeding 35 cycles/min, as data in animal models suggest that a high minute ventilation has deleterious effects [137, 138], which are more marked when there is lung involvement.
Abbreviations
- BE:
-
base excess
- SBE:
-
standard base excess
- AG:
-
anion gap
- cAG:
-
corrected anion gap
- SID:
-
strong ion difference
- eff SID:
-
effective strong ion difference
- app SID:
-
apparent strong ion difference
- IV:
-
intravenous
- SC:
-
subcutaneous
- RRT:
-
renal replacement therapy
References
Kimmoun A, Novy E, Auchet T, Ducrocq N, Levy B. Hemodynamic consequences of severe lactic acidosis in shock states: from bench to bedside. Crit Care Lond Engl. 2015;19:175.
Kraut JA, Madias NE. Treatment of acute metabolic acidosis: a pathophysiologic approach. Nat Rev Nephrol. 2012;8(10):589–601.
Kraut JA, Madias NE. Metabolic acidosis: pathophysiology, diagnosis and management. Nat Rev Nephrol. 2010;6(5):274–85.
Asch MJ, Dell RB, Williams GS, Cohen M, Winters RW. Time course for development of respiratory compensation in metabolic acidosis. J Lab Clin Med. 1969;73(4):610–5.
Fulop M. A guide for predicting arterial CO2 tension in metabolic acidosis. Am J Nephrol. 1997;17(5):421–4.
Batlle D, Chin-Theodorou J, Tucker BM. Metabolic acidosis or respiratory alkalosis? evaluation of a low plasma bicarbonate using the urine anion gap. Am J Kidney Dis Off J Natl Kidney Found. 2017;70(3):440–4.
Bloom BM, Grundlingh J, Bestwick JP, Harris T. The role of venous blood gas in the emergency department: a systematic review and meta-analysis. Eur J Emerg Med Off J Eur Soc Emerg Med. 2014;21(2):81–8.
Ma OJ, Rush MD, Godfrey MM, Gaddis G. Arterial blood gas results rarely influence emergency physician management of patients with suspected diabetic ketoacidosis. Acad Emerg Med Off J Soc Acad Emerg Med. 2003;10(8):836–41.
Arnold TDW, Miller M, van Wessem KP, Evans JA, Balogh ZJ. Base deficit from the first peripheral venous sample: a surrogate for arterial base deficit in the trauma bay. J Trauma. 2011;71(4):793–7 (discussion 797).
Zakrison T, McFarlan A, Wu YY, Keshet I, Nathens A. Venous and arterial base deficits: do these agree in occult shock and in the elderly? A Bland-Altman analysis. J Trauma Acute Care Surg. 2013;74(3):936–9.
Herrington WG, Nye HJ, Hammersley MS, Watkinson PJ. Are arterial and venous samples clinically equivalent for the estimation of pH, serum bicarbonate and potassium concentration in critically ill patients? Diabet Med J Br Diabet Assoc. 2012;29(1):32–5.
Surbatovic M, Radakovic S, Jevtic M, Filipovic N, Romic P, Popovic N, et al. Predictive value of serum bicarbonate, arterial base deficit/excess and SAPS III score in critically ill patients. Gen Physiol Biophys. 2009;28:271–6.
Martin MJ, FitzSullivan E, Salim A, Berne TV, Towfigh S. Use of serum bicarbonate measurement in place of arterial base deficit in the surgical intensive care unit. Arch Surg Chic Ill 1960. 2005;140(8):745–51.
FitzSullivan E, Salim A, Demetriades D, Asensio J, Martin MJ. Serum bicarbonate may replace the arterial base deficit in the trauma intensive care unit. Am J Surg. 2005;190(6):941–6.
Chawla LS, Jagasia D, Abell LM, Seneff MG, Egan M, Danino N, et al. Anion gap, anion gap corrected for albumin, and base deficit fail to accurately diagnose clinically significant hyperlactatemia in critically ill patients. J Intensive Care Med. 2008;23(2):122–7.
Dinh CH, Ng R, Grandinetti A, Joffe A, Chow DC. Correcting the anion gap for hypoalbuminaemia does not improve detection of hyperlactataemia. Emerg Med J EMJ. 2006;23(8):627–9.
Moviat M, van Haren F, van der Hoeven H. Conventional or physicochemical approach in intensive care unit patients with metabolic acidosis. Crit Care Lond Engl. 2003;7(3):R41–5.
Mallat J, Michel D, Salaun P, Thevenin D, Tronchon L. Defining metabolic acidosis in patients with septic shock using Stewart approach. Am J Emerg Med. 2012;30(3):391–8.
Chawla LS, Shih S, Davison D, Junker C, Seneff MG. Anion gap, anion gap corrected for albumin, base deficit and unmeasured anions in critically ill patients: implications on the assessment of metabolic acidosis and the diagnosis of hyperlactatemia. BMC Emerg Med. 2008;8:18.
Dubin A, Menises MM, Masevicius FD, Moseinco MC, Kutscherauer DO, Ventrice E, et al. Comparison of three different methods of evaluation of metabolic acid–base disorders. Crit Care Med. 2007;35(5):1264–70.
Story DA, Poustie S, Bellomo R. Estimating unmeasured anions in critically ill patients: anion-gap, base-deficit, and strong-ion-gap. Anaesthesia. 2002;57(11):1109–14.
Balasubramanyan N, Havens PL, Hoffman GM. Unmeasured anions identified by the Fencl–Stewart method predict mortality better than base excess, anion gap, and lactate in patients in the pediatric intensive care unit. Crit Care Med. 1999;27(8):1577–81.
Lautrette A, Fejjal M, Aithssain A, Phan TN, Caillot N, Fogli A, et al. Comparison of three methods of diagnosis of plasma unmeasured anions in critically ill patients. Minerva Anestesiol. 2013;79(10):1164–72.
Boniatti MM, Cardoso PRC, Castilho RK, Vieira SRR. Acid–base disorders evaluation in critically ill patients: we can improve our diagnostic ability. Intensive Care Med. 2009;35(8):1377–82.
Nanji AA, Campbell DJ, Pudek MR. Decreased anion gap associated with hypoalbuminemia and polyclonal gammopathy. JAMA. 1981;246(8):859–60.
Figge J, Jabor A, Kazda A, Fencl V. Anion gap and hypoalbuminemia. Crit Care Med. 1998;26(11):1807–10.
Fencl V, Jabor A, Kazda A, Figge J. Diagnosis of metabolic acid–base disturbances in critically ill patients. Am J Respir Crit Care Med. 2000;162(6):2246–51.
Kraut JA, Madias NE. Differential diagnosis of nongap metabolic acidosis: value of a systematic approach. Clin J Am Soc Nephrol CJASN. 2012;7(4):671–9.
Adrogué HJ, Madias NE. Assessing acid–base status: physiologic versus physicochemical approach. Am J Kidney Dis Off J Natl Kidney Found. 2016;68(5):793–802.
Tuhay G, Pein MC, Masevicius FD, Kutscherauer DO, Dubin A. Severe hyperlactatemia with normal base excess: a quantitative analysis using conventional and Stewart approaches. Crit Care Lond Engl. 2008;12(3):R66.
Guérin C, Nesme P, Leray V, Wallet F, Bourdin G, Bayle F, et al. Quantitative analysis of acid–base disorders in patients with chronic respiratory failure in stable or unstable respiratory condition. Respir Care. 2010;55(11):1453–63.
Magder S, Emami A. Practical approach to physical–chemical acid–base management Stewart at the bedside. Ann Am Thorac Soc. 2015;12(1):111–7.
Galbois A, Ait-Oufella H, Baudel J-L, Maury E, Offenstadt G. An adult can still die of salicylate poisoning in France in 2008. Intensive Care Med. 2009;35(11):1999.
Pernet P, Bénéteau-Burnat B, Vaubourdolle M, Maury E, Offenstadt G. False elevation of blood lactate reveals ethylene glycol poisoning. Am J Emerg Med. 2009;27(1):132.e1–2.
Adrogué HJ, Wilson H, Boyd AE, Suki WN, Eknoyan G. Plasma acid–base patterns in diabetic ketoacidosis. N Engl J Med. 1982;307(26):1603–10.
Richardson RM, Halperin ML. The urine pH: a potentially misleading diagnostic test in patients with hyperchloremic metabolic acidosis. Am J Kidney Dis Off J Natl Kidney Found. 1987;10(2):140–3.
Kraut JA, Mullins ME. Toxic alcohols. N Engl J Med. 2018;378(3):270–80.
Noritomi DT, Soriano FG, Kellum JA, Cappi SB, Biselli PJC, Libório AB, et al. Metabolic acidosis in patients with severe sepsis and septic shock: a longitudinal quantitative study. Crit Care Med. 2009;37(10):2733–9.
Rastegar M, Nagami GT. Non-anion gap metabolic acidosis: a clinical approach to evaluation. Am J Kidney Dis Off J Natl Kidney Found. 2017;69(2):296–301.
Kim HY, Han JS, Jeon US, Joo KW, Earm JH, Ahn C, et al. Clinical significance of the fractional excretion of anions in metabolic acidosis. Clin Nephrol. 2001;55(6):448–52.
Batlle DC, Hizon M, Cohen E, Gutterman C, Gupta R. The use of the urinary anion gap in the diagnosis of hyperchloremic metabolic acidosis. N Engl J Med. 1988;318(10):594–9.
Brunner R, Drolz A, Scherzer T-M, Staufer K, Fuhrmann V, Zauner C, et al. Renal tubular acidosis is highly prevalent in critically ill patients. Crit Care Lond Engl. 2015;19:148.
Guyette FX, Meier EN, Newgard C, McKnight B, Daya M, Bulger EM, et al. A comparison of prehospital lactate and systolic blood pressure for predicting the need for resuscitative care in trauma transported by ground. J Trauma Acute Care Surg. 2015;78(3):600–6.
Contenti J, Corraze H, Lemoël F, Levraut J. Effectiveness of arterial, venous, and capillary blood lactate as a sepsis triage tool in ED patients. Am J Emerg Med. 2015;33(2):167–72.
Musikatavorn K, Thepnimitra S, Komindr A, Puttaphaisan P, Rojanasarntikul D. Venous lactate in predicting the need for intensive care unit and mortality among nonelderly sepsis patients with stable hemodynamic. Am J Emerg Med. 2015;33(7):925–30.
Barfod C, Lundstrøm LH, Lauritzen MMP, Danker JK, Sölétormos G, Forberg JL, et al. Peripheral venous lactate at admission is associated with in-hospital mortality, a prospective cohort study. Acta Anaesthesiol Scand. 2015;59(4):514–23.
Bouzat P, Schilte C, Vinclair M, Manhes P, Brun J, Bosson J-L, et al. Capillary lactate concentration on admission of normotensive trauma patients: a prospective study. Scand J Trauma Resusc Emerg Med. 2016;24:82.
Gaieski DF, Drumheller BC, Goyal M, Fuchs BD, Shofer FS, Zogby K. Accuracy of handheld point-of-care fingertip lactate measurement in the emergency department. West J Emerg Med. 2013;14(1):58–62.
Kim C, Kim H. Emergency medical technician-performed point-of-care blood analysis using the capillary blood obtained from skin puncture. Am J Emerg Med. 2018;36(7):1215–21.
Collange O, Garcia V, Kindo M, Meyer N, Lavaux T, Mertes PM, et al. Comparison of capillary and arterial lactate levels in patients with shock. Anaesth Crit Care Pain Med. 2017;36(3):157–62.
Seoane L, Papasidero M, De Sanctis P, Posadas-Martínez LM, Soler S, Rodríguez M. Capillary lactic acid validation in an ED. Am J Emerg Med. 2013;31(9):1365–7.
Tanner RK, Fuller KL, Ross MLR. Evaluation of three portable blood lactate analysers: lactate pro, lactate scout and lactate plus. Eur J Appl Physiol. 2010;109(3):551–9.
Manzon C, Barrot L, Besch G, Barbot O, Desmettre T, Capellier G, et al. Capillary lactate as a tool for the triage nurse among patients with SIRS at emergency department presentation: a preliminary report. Ann Intensive Care. 2015;5:7.
Kraut JA, Madias NE. Lactic acidosis. N Engl J Med. 2014;371(24):2309–19.
Vernon C, Letourneau JL. Lactic acidosis: recognition, kinetics, and associated prognosis. Crit Care Clin. 2010;26(2):255–83.
Blohm E, Lai J, Neavyn M. Drug-induced hyperlactatemia. Clin Toxicol Phila Pa. 2017;55(8):869–78.
Suetrong B, Walley KR. Lactic acidosis in sepsis: it’s not all anaerobic: implications for diagnosis and management. Chest. 2016;149(1):252–61.
Laffel LMB, Wentzell K, Loughlin C, Tovar A, Moltz K, Brink S. Sick day management using blood 3-hydroxybutyrate (3-OHB) compared with urine ketone monitoring reduces hospital visits in young people with T1DM: a randomized clinical trial. Diabet Med J Br Diabet Assoc. 2006;23(3):278–84.
Taboulet P, Deconinck N, Thurel A, Haas L, Manamani J, Porcher R, et al. Correlation between urine ketones (acetoacetate) and capillary blood ketones (3-beta-hydroxybutyrate) in hyperglycaemic patients. Diabetes Metab. 2007;33(2):135–9.
Voulgari C, Tentolouris N. The performance of a glucose-ketone meter in the diagnosis of diabetic ketoacidosis in patients with type 2 diabetes in the emergency room. Diabetes Technol Ther. 2010;12(7):529–35.
Arora S, Henderson SO, Long T, Menchine M. Diagnostic accuracy of point-of-care testing for diabetic ketoacidosis at emergency-department triage: {beta}-hydroxybutyrate versus the urine dipstick. Diabetes Care. 2011;34(4):852–4.
Charles RA, Bee YM, Eng PHK, Goh SY. Point-of-care blood ketone testing: screening for diabetic ketoacidosis at the emergency department. Singapore Med J. 2007;48(11):986–9.
Kuru B, Sever M, Aksay E, Dogan T, Yalcin N, Eren ES, et al. Comparing finger-stick β-hydroxybutyrate with dipstick urine tests in the detection of ketone bodies. Turk J Emerg Med. 2014;14(2):47–52.
Shin J, Lim YS, Kim K, Lee HJ, Lee SJ, Jung E, et al. Initial blood pH during cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients: a multicenter observational registry-based study. Crit Care Lond Engl. 2017;21(1):322.
Spindelboeck W, Gemes G, Strasser C, Toescher K, Kores B, Metnitz P, et al. Arterial blood gases during and their dynamic changes after cardiopulmonary resuscitation: a prospective clinical study. Resuscitation. 2016;106:24–9.
Denton R, Thomas AN. Cardiopulmonary resuscitation: a retrospective review. Anaesthesia. 1997;52(4):324–7.
Kaplan LJ, Kellum JA. Initial pH, base deficit, lactate, anion gap, strong ion difference, and strong ion gap predict outcome from major vascular injury. Crit Care Med. 2004;32(5):1120–4.
Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336(4):243–50.
Renaud B, Labarère J, Coma E, Santin A, Hayon J, Gurgui M, et al. Risk stratification of early admission to the intensive care unit of patients with no major criteria of severe community-acquired pneumonia: development of an international prediction rule. Crit Care Lond Engl. 2009;13(2):R54.
Shapiro NI, Howell MD, Talmor D, Nathanson LA, Lisbon A, Wolfe RE, et al. Serum lactate as a predictor of mortality in emergency department patients with infection. Ann Emerg Med. 2005;45(5):524–8.
Casserly B, Phillips GS, Schorr C, Dellinger RP, Townsend SR, Osborn TM, et al. Lactate measurements in sepsis-induced tissue hypoperfusion: results from the Surviving Sepsis Campaign database. Crit Care Med. 2015;43(3):567–73.
Park YJ, Kim DH, Kim SC, Kim TY, Kang C, Lee SH, et al. Serum lactate upon emergency department arrival as a predictor of 30-day in-hospital mortality in an unselected population. PLoS ONE. 2018;13(1):e0190519.
Puskarich MA, Kline JA, Summers RL, Jones AE. Prognostic value of incremental lactate elevations in emergency department patients with suspected infection. Acad Emerg Med Off J Soc Acad Emerg Med. 2012;19(8):983–5.
Raux M, Le Manach Y, Gauss T, Baumgarten R, Hamada S, Harrois A, et al. Comparison of the prognostic significance of initial blood lactate and base deficit in trauma patients. Anesthesiology. 2017;126(3):522–33.
Régnier M-A, Raux M, Le Manach Y, Asencio Y, Gaillard J, Devilliers C, et al. Prognostic significance of blood lactate and lactate clearance in trauma patients. Anesthesiology. 2012;117(6):1276–88.
Ryoo SM, Lee J, Lee Y-S, Lee JH, Lim KS, Huh JW, et al. Lactate level versus lactate clearance for predicting mortality in patients with septic shock defined by sepsis-3. Crit Care Med. 2018;46(6):e489–95.
Dezman ZDW, Comer AC, Smith GS, Narayan M, Scalea TM, Hirshon JM. Failure to clear elevated lactate predicts 24-hour mortality in trauma patients. J Trauma Acute Care Surg. 2015;79(4):580–5.
May ME, Young C, King J. Resource utilization in treatment of diabetic ketoacidosis in adults. Am J Med Sci. 1993;306(5):287–94.
Moss JM. Diabetic ketoacidosis: effective low-cost treatment in a community hospital. South Med J. 1987;80(7):875–81.
Marinac JS, Mesa L. Using a severity of illness scoring system to assess intensive care unit admissions for diabetic ketoacidosis. Crit Care Med. 2000;28(7):2238–41.
Gershengorn HB, Iwashyna TJ, Cooke CR, Scales DC, Kahn JM, Wunsch H. Variation in use of intensive care for adults with diabetic ketoacidosis. Crit Care Med. 2012;40(7):2009–15.
Andrade-Castellanos CA, Colunga-Lozano LE, Delgado-Figueroa N, Gonzalez-Padilla DA. Subcutaneous rapid-acting insulin analogues for diabetic ketoacidosis. Cochrane Database Syst Rev. 2016;1:CD011281.
Vincent M, Nobécourt E. Treatment of diabetic ketoacidosis with subcutaneous insulin lispro: a review of the current evidence from clinical studies. Diabetes Metab. 2013;39(4):299–305.
Fisher JN, Shahshahani MN, Kitabchi AE. Diabetic ketoacidosis: low-dose insulin therapy by various routes. N Engl J Med. 1977;297(5):238–41.
Umpierrez GE, Latif K, Stoever J, Cuervo R, Park L, Freire AX, et al. Efficacy of subcutaneous insulin lispro versus continuous intravenous regular insulin for the treatment of patients with diabetic ketoacidosis. Am J Med. 2004;117(5):291–6.
Umpierrez GE, Cuervo R, Karabell A, Latif K, Freire AX, Kitabchi AE. Treatment of diabetic ketoacidosis with subcutaneous insulin aspart. Diabetes Care. 2004;27(8):1873–8.
Karoli R, Fatima J, Salman T, Sandhu S, Shankar R. Managing diabetic ketoacidosis in non-intensive care unit setting: role of insulin analogs. Indian J Pharmacol. 2011;43(4):398–401.
Kitabchi AE, Murphy MB, Spencer J, Matteri R, Karas J. Is a priming dose of insulin necessary in a low-dose insulin protocol for the treatment of diabetic ketoacidosis? Diabetes Care. 2008;31(11):2081–5.
Goyal N, Miller JB, Sankey SS, Mossallam U. Utility of initial bolus insulin in the treatment of diabetic ketoacidosis. J Emerg Med. 2010;38(4):422–7.
Page MM, Alberti KG, Greenwood R, Gumaa KA, Hockaday TD, Lowy C, et al. Treatment of diabetic coma with continuous low-dose infusion of insulin. Br Med J. 1974;2(5921):687–90.
Semple PF, White C, Manderson WG. Continuous intravenous infusion of small doses of insulin in treatment of diabetic ketoacidosis. Br Med J. 1974;2(5921):694–8.
El-Solh AA, Abou Jaoude P, Porhomayon J. Bicarbonate therapy in the treatment of septic shock: a second look. Intern Emerg Med. 2010;5(4):341–7.
Kim HJ, Son YK, An WS. Effect of sodium bicarbonate administration on mortality in patients with lactic acidosis: a retrospective analysis. PLoS ONE. 2013;8(6):e65283.
Wilson RF, Spencer AR, Tyburski JG, Dolman H, Zimmerman LH. Bicarbonate therapy in severely acidotic trauma patients increases mortality. J Trauma Acute Care Surg. 2013;74(1):45–50 (discussion 50).
Jung B, Rimmele T, Le Goff C, Chanques G, Corne P, Jonquet O, et al. Severe metabolic or mixed acidemia on intensive care unit admission: incidence, prognosis and administration of buffer therapy. A prospective, multiple-center study. Crit Care Lond Engl. 2011;15(5):R238.
Mathieu D, Neviere R, Billard V, Fleyfel M, Wattel F. Effects of bicarbonate therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis: a prospective, controlled clinical study. Crit Care Med. 1991;19(11):1352–6.
Cooper DJ, Walley KR, Wiggs BR, Russell JA. Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled clinical study. Ann Intern Med. 1990;112(7):492–8.
Jaber S, Paugam C, Futier E, Lefrant J-Y, Lasocki S, Lescot T, et al. Sodium bicarbonate therapy for patients with severe metabolic acidaemia in the intensive care unit (BICAR-ICU): a multicentre, open-label, randomised controlled, phase 3 trial. Lancet Lond Engl. 2018;392(10141):31–40.
Weng Y-M, Wu S-H, Li W-C, Kuo C-W, Chen S-Y, Chen J-C. The effects of sodium bicarbonate during prolonged cardiopulmonary resuscitation. Am J Emerg Med. 2013;31(3):562–5.
Kawano T, Grunau B, Scheuermeyer FX, Gibo K, Dick W, Fordyce CB, et al. Prehospital sodium bicarbonate use could worsen long term survival with favorable neurological recovery among patients with out-of-hospital cardiac arrest. Resuscitation. 2017;119:63–9.
Kim J, Kim K, Park J, Jo YH, Lee JH, Hwang JE, et al. Sodium bicarbonate administration during ongoing resuscitation is associated with increased return of spontaneous circulation. Am J Emerg Med. 2016;34(2):225–9.
Wang C-H, Huang C-H, Chang W-T, Tsai M-S, Yu P-H, Wu Y-W, et al. The effects of calcium and sodium bicarbonate on severe hyperkalaemia during cardiopulmonary resuscitation: a retrospective cohort study of adult in-hospital cardiac arrest. Resuscitation. 2016;98:105–11.
Bar-Joseph G, Abramson NS, Kelsey SF, Mashiach T, Craig MT, Safar P, et al. Improved resuscitation outcome in emergency medical systems with increased usage of sodium bicarbonate during cardiopulmonary resuscitation. Acta Anaesthesiol Scand. 2005;49(1):6–15.
Vukmir RB, Katz L, Sodium Bicarbonate Study Group. Sodium bicarbonate improves outcome in prolonged prehospital cardiac arrest. Am J Emerg Med. 2006;24(2):156–61.
Monsieurs KG, Nolan JP, Bossaert LL, Greif R, Maconochie IK, Nikolaou NI, et al. European resuscitation council guidelines for resuscitation 2015: section 1. Executive summary. Resuscitation. 2015;95:1–80.
Joffre J, Bourcier S, Hariri G, Miailhe A-F, Bigé N, Dumas G, et al. Reversible microvascular hyporeactivity to acetylcholine during diabetic ketoacidosis. Crit Care Med. 2018;46(8):e772–8.
Duhon B, Attridge RL, Franco-Martinez AC, Maxwell PR, Hughes DW. Intravenous sodium bicarbonate therapy in severely acidotic diabetic ketoacidosis. Ann Pharmacother. 2013;47(7–8):970–5.
Viallon A, Zeni F, Lafond P, Venet C, Tardy B, Page Y, et al. Does bicarbonate therapy improve the management of severe diabetic ketoacidosis? Crit Care Med. 1999;27(12):2690–3.
Temple AR. Pathophysiology of aspirin overdosage toxicity, with implications for management. Pediatrics. 1978;62(5):873–6.
Juurlink DN, Gosselin S, Kielstein JT, Ghannoum M, Lavergne V, Nolin TD, et al. Extracorporeal treatment for salicylate poisoning: systematic review and recommendations from the EXTRIP Workgroup. Ann Emerg Med. 2015;66(2):165–81.
Prescott LF, Balali-Mood M, Critchley JA, Johnstone AF, Proudfoot AT. Diuresis or urinary alkalinisation for salicylate poisoning? Br Med J Clin Res Ed. 1982;285(6352):1383–6.
Legrand M, Darmon M, Joannidis M, Payen D. Management of renal replacement therapy in ICU patients: an international survey. Intensive Care Med. 2013;39(1):101–8.
Wald R, McArthur E, Adhikari NKJ, Bagshaw SM, Burns KEA, Garg AX, et al. Changing incidence and outcomes following dialysis-requiring acute kidney injury among critically ill adults: a population-based cohort study. Am J Kidney Dis. 2015;65(6):870–7.
Zarbock A, Kellum JA, Schmidt C, Aken HV, Wempe C, Pavenstädt H, et al. Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: the ELAIN randomized clinical trial. JAMA. 2016;315(20):2190–9.
Gaudry S, Hajage D, Schortgen F, Martin-Lefevre L, Pons B, Boulet E, et al. Initiation strategies for renal-replacement therapy in the intensive care unit. N Engl J Med. 2016;375(2):122–33.
Barbar SD, Clere-Jehl R, Bourredjem A, Hernu R, Montini F, Bruyère R, et al. Timing of renal-replacement therapy in patients with acute kidney injury and sepsis. N Engl J Med. 2018;379(15):1431–42.
Yeh H-C, Ting I-W, Tsai C-W, Wu J-Y, Kuo C-C. Serum lactate level and mortality in metformin-associated lactic acidosis requiring renal replacement therapy: a systematic review of case reports and case series. BMC Nephrol. 2017;18(1):229.
Mariano F, Pozzato M, Inguaggiato P, Guarena C, Turello E, Manes M, et al. Metformin-associated lactic acidosis undergoing renal replacement therapy in intensive care units: a five-million population-based study in the North-West of Italy. Blood Purif. 2017;44(3):198–205.
Calello DP, Liu KD, Wiegand TJ, Roberts DM, Lavergne V, Gosselin S, et al. Extracorporeal treatment for metformin poisoning: systematic review and recommendations from the extracorporeal treatments in poisoning workgroup. Crit Care Med. 2015;43(8):1716–30.
Hovda KE, Hunderi OH, Tafjord A-B, Dunlop O, Rudberg N, Jacobsen D. Methanol outbreak in Norway 2002–2004: epidemiology, clinical features and prognostic signs. J Intern Med. 2005;258(2):181–90.
Kute VB, Godara SM, Shah PR, Gumber MR, Goplani KR, Vanikar AV, et al. Hemodialysis for methyl alcohol poisoning: a single-center experience. Saudi J Kidney Dis Transplant Off Publ Saudi Cent Organ Transplant Saudi Arab. 2012;23(1):37–43.
Liu JJ, Daya MR, Carrasquillo O, Kales SN. Prognostic factors in patients with methanol poisoning. J Toxicol Clin Toxicol. 1998;36(3):175–81.
Coulter CV, Farquhar SE, McSherry CM, Isbister GK, Duffull SB. Methanol and ethylene glycol acute poisonings—predictors of mortality. Clin Toxicol Phila Pa. 2011;49(10):900–6.
Brent J, McMartin K, Phillips S, Aaron C, Kulig K, Methylpyrazole for Toxic Alcohols Study Group. Fomepizole for the treatment of methanol poisoning. N Engl J Med. 2001;344(6):424–9.
Mégarbane B, Borron SW, Baud FJ. Current recommendations for treatment of severe toxic alcohol poisonings. Intensive Care Med. 2005;31(2):189–95.
Roberts DM, Yates C, Megarbane B, Winchester JF, Maclaren R, Gosselin S, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning: a systematic review and consensus statement. Crit Care Med. 2015;43(2):461–72.
McCabe DJ, Lu JJ. The association of hemodialysis and survival in intubated salicylate-poisoned patients. Am J Emerg Med. 2017;35(6):899–903.
Dempsey JA, Smith CA. Pathophysiology of human ventilatory control. Eur Respir J. 2014;44(2):495–512.
Lumb A. Nunn’s applied respiratory physiology. 8th ed. New York: Elsevier; 2016.
Javaheri S, Corbett W, Wagner K, Adams JM. Quantitative cerebrospinal fluid acid–base balance in acute respiratory alkalosis. Am J Respir Crit Care Med. 1994;150(1):78–82.
Javaheri S, Herrera L, Kazemi H. Ventilatory drive in acute metabolic acidosis. J Appl Physiol. 1979;46(5):913–8.
Fulop M. Ventilatory response in patients with acute lactic acidosis. Crit Care Med. 1982;10(3):173–5.
Curley GF, Laffey JG. Acidosis in the critically ill—balancing risks and benefits to optimize outcome. Crit Care Lond Engl. 2014;18(2):129.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;45:486–552.
Stengl M, Ledvinova L, Chvojka J, Benes J, Jarkovska D, Holas J, et al. Effects of clinically relevant acute hypercapnic and metabolic acidosis on the cardiovascular system: an experimental porcine study. Crit Care Lond Engl. 2013;17(6):R303.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45(3):486–552.
Brochard L, Slutsky A, Pesenti A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am J Respir Crit Care Med. 2017;195(4):438–42.
Mascheroni D, Kolobow T, Fumagalli R, Moretti MP, Chen V, Buckhold D. Acute respiratory failure following pharmacologically induced hyperventilation: an experimental animal study. Intensive Care Med. 1988;15(1):8–14.
Acknowledgements
Not applicable.
Funding
This work was financially supported by the Société de Réanimation de Langue Française (SRLF) and the Société Française de Médecine d’Urgence (SFMU).
Author information
Authors and Affiliations
Consortia
Contributions
BJ and MM proposed the elaboration of this recommendation and manuscript in agreement with the “Société de Réanimation de Langue Française” and “Société Française de Médecine d’Urgence”; NB and PGC wrote the methodology section and gave the final version with the final presentation. DV, AL, EM, MD, MM, and JL contributed to elaborate recommendations and wrote the rationale of « Diagnostic strategy ». YEC, JL , and MO contributed to elaborate recommendations and to write the rationale of « Patient assessment and referral ». YY, BJ, KK , and NT contributed to elaborate recommendations and to write the rationale of « Therapeutic management ». All authors provided references. BJ, MM, PGC, and NB drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare the following competing interests: B. Jung: Sedana Medical, Medtronic; M. Martinez: Astra Zeneca, Actélion; YE Claessens: Roche diagnostics, BioMérieux, Sanofi, Pfizer; M. Darmon: Sanofi, Gilead-Kite, Astute Medical, MSD, Astellas; A. Lautrette: Baxter, Frésénius; J. Levraut: LFB, Nova-Biomedical; E. Maury: General Electric Healthcare, Doran International, Vygon, AstraZeneca; N. Terzi: Boehringer Ingelheim, Pfizer; D. Viglino: Astra Zeneca, Mundipharma; Y. Yordanov: Mundipharma, Sanofi; PG Claret: Aspen, AstraZeneca, Daiichi Sankyo, Roche Diagnostics, Sanofi, Thermo Fisher Scientific. The remaining authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Jung, B., Martinez, M., Claessens, YE. et al. Diagnosis and management of metabolic acidosis: guidelines from a French expert panel. Ann. Intensive Care 9, 92 (2019). https://doi.org/10.1186/s13613-019-0563-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-019-0563-2