
Abstract
Background
The glucose-to-glycated hemoglobin ratio (GAR) represents stress hyperglycemia, which has been closely associated with adverse outcomes in cardio-cerebrovascular diseases. No studies have examined the association between stress hyperglycemia and atrial fibrillation (AF) in critically ill patients. This study aims to explore the relationship between GAR and the prognosis of critically ill patients with AF.
Methods
A retrospective cohort of patients was selected from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. The GAR was calculated based on fasting blood glucose and glycated hemoglobin levels measured after admission. The primary outcome was the 30-day mortality rate, with secondary outcomes being the 90-day and 365-day mortality rates. The GAR was divided into tertiles, and Kaplan–Meier analysis was employed to compare differences in mortality rates between groups. The Cox proportional hazards model and restricted cubic splines (RCS) were utilized to evaluate the relationship between the GAR and mortality. Subsequently, a segmented regression model was constructed to analyze threshold effects in cases where nonlinear relationships were determined.
Results
In this cohort, the second tertile of the GAR exhibited lower mortality rates at 30 days (10.56% vs 6.33% vs 14.51%), 90 days (17.11% vs 10.09% vs 17.88%), and 365 days (25.30% vs 16.15% vs 22.72%). In the third tertile, the risk of mortality at 30 days increased by 165% (HR = 2.65, 95% CI 1.99–3.54, p < 0.001), at 90 days increased by 113% (HR = 2.13, 95% CI 1.68–2.70, p < 0.001), and at 365 days increased by 70% (HR = 1.70, 95% CI 1.68–2.70, p < 0.001). The association between the GAR and patient mortality demonstrated a “J-shaped” non-linear correlation. Once the GAR exceeded 15.915, each incremental unit increase in the ratio was associated with a 27.2% increase in the risk of 30-day mortality in critically ill atrial fibrillation patients (HR = 1.262, 95% CI 1.214–1.333, p < 0.001).
Conclusion
The GAR is associated with both short-term and long-term mortality in critically ill patients with AF in a J-shaped relationship. Both low and excessively high GAR values indicate poor prognosis.
Similar content being viewed by others

Introduction
AF is the most common cardiac arrhythmia worldwide, associated with increased risks of heart failure, myocardial infarction, and stroke, consequently elevating the burden of mortality [1]. Critically ill patients often face the risk of new-onset AF [2], and those with either new-onset AF or pre-existing AF during Intensive Care Unit (ICU) admission have a higher mortality rate compared to patients with no history of AF [3]. However, research on adverse prognostic factors in critically ill AF patients is limited.
Stress hyperglycemia is a physiological response to a sudden clinical event that causes an increase in blood glucose levels, a common occurrence in ICU patients [4, 5], which can induce myocardial injury through multiple mechanisms, including acidosis from lactate accumulation, heightened inflammatory responses, intracellular calcium overload, and disturbances in lipid metabolism [6]. Given that the myocardium predominantly utilizes fatty acids as its energy source [7], patients with AF experience exacerbated cardiac damage due to increased myocardial glycolysis and the accumulation of late-stage glucose metabolic byproducts, which result from myocardial injury and rapid, disorganized electrical activity [8]. Meanwhile, hypoglycemia is a risk factor for cardiovascular disease and mortality, particularly among individuals with concomitant arrhythmias [9]. Evaluating the association between stress hyperglycemia and critically ill AF patients is essential. The GAR, representing the ratio of plasma glucose concentration to glycated hemoglobin (the baseline average glucose over the past 3 months), quantifies acute plasma glucose elevation. Additionally, the GAR quantifies acute plasma glucose elevation. Previous studies have linked elevated GAR indices to outcomes following ischemic stroke and thrombolytic therapy [10,11,12]. This study represents the inaugural assessment of the correlation between stress hyperglycemia, delineated by the GAR, and the prognosis of critically ill AF patients, thereby furnishing valuable insights for tailored glucose management strategies.
Methods and materials
Study population
This retrospective study extracted data on patients with AF from the MIMIC-IV database, a large database developed and managed by the Laboratory for Computational Physiology at the Massachusetts Institute of Technology. The database contains medical information on patients admitted to the intensive care units of the Beth Israel Deaconess Medical Center. The first author of this study obtained permission to access the dataset and extracted the relevant data. The use of this database for research has been approved by the institutional review boards of the Massachusetts Institute of Technology and the Beth Israel Deaconess Medical Center.
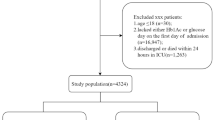
In this study, 12,255 patients with AF who were admitted to the ICU for the first time were included, diagnosed according to the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes. Exclusions were made for 253 cases lacking glucose data, 56 cases with anomalous death times, and 8,661 cases lacking data on glycated hemoglobin, ultimately resulting in the inclusion of 3,285 critically ill patients with AF. A flowchart of patient selection was shown as Fig. 1.

A flowchart of patient selection
Data extractions
PostgreSQL software (version 13.7.2) was used to extract data via Structured Query Language (SQL). Potential covariates included in this study were: (1) Baseline demographic information: age, gender, race, and body mass index (BMI). (2) Comorbidities: hypertension, diabetes, acute kidney injury (AKI), chronic kidney disease (CKD), acute myocardial infarction (AMI), heart failure (HF), stroke, cancer, and hyperlipidemia. (3) Laboratory parameters: fasting blood glucose, glycated hemoglobin(HbA1c), white blood cells (WBC), hemoglobin (HGB), serum creatinine, serum uric acid, serum lactate, international normalized ratio (INR), D-dimer, triglycerides, and low-density lipoprotein cholesterol (LDL-C). (4) Disease severity scores: Oxford Acute Severity of Illness Score (OASIS) and Sequential Organ Failure Assessment (SOFA) score. Due to more than 30% missing data for serum lipids, serum uric acid and D-dimer these were not included in the statistical analysis. Missing data for other variables included in the analysis were imputed using the random forest method for all serological indicators.
Exposure variables
Stress hyperglycemia syndrome was estimated using the GAR, calculated by the formula: fasting blood glucose (mg/dL) / HbA1c (%). As critically ill patients in the MIMIC database do not have a separately defined fasting blood glucose, the lowest blood glucose level during hospitalization was used as a proxy for fasting blood glucose. Patients were stratified into three groups based on the tertiles of the GAR.
Outcome events
The primary outcome of this study was all-cause mortality at 30 days following ICU admission, with secondary outcomes including all-cause mortality at 90 days and 365 days post-admission.
Statistical analysis
For this study, categorical variables were presented as percentages, and chi-square tests were employed to evaluate the significance of differences in categorical variables among various GAR groups. Normality tests were performed for all continuous variables; non-normally distributed variables were represented by median (interquartile range) and compared using non-parametric rank-sum tests. Patients were divided into three groups based on GAR tertiles, with the second tertile serving as the reference. The Cox proportional hazards model was used to assess hazard ratio (HR) for outcome events, incorporating age, gender, race, BMI, AKI, CKD, HF, hypertension, cancer, stroke, WBC, hemoglobin, creatinine, serum lactate, SOFA score and OASIS score as confounders in the multivariate Cox regression model. AMI and diabetes did not meet the Cox proportional hazards assumption and were therefore not included in the model.
Survival analysis was conducted using the Kaplan–Meier method based on GAR tertiles, with inter-group differences assessed using the log-rank test. Restricted cubic splines (RCS) were utilized to explore the correlation between GAR and outcome events, and a threshold effect model was established to analyze the inflection points of GAR. Subgroup analyses were performed to verify the robustness of the results. Statistical analyses in this study were conducted using R Studio (version R4.2.3) and IBM SPSS Statistics (version V22.0). A two-sided P-value of < 0.05 was considered statistically significant.
Results
Patients' baseline information
The study cohort comprised 3,285 patients with critical illness and a diagnosis of AF. Mortality rates within the cohort were as follows: 344 patients (10.47%) succumbed within 30 days, 494 patients (15.04%) within 90 days, and 703 patients (21.40%) within 1 year of the initial diagnosis. The baseline characteristics patient according to tertile of GAR (1099 patients in tertile 1 [1.97–14.03]; 1090 patients in tertile 2 [14.04–16.54]; and 1096 patient in tertile 3 [16.55–40.32] are summarized in Table 1. Compared to patients in Tertile 2, those with lower and higher GAR values exhibited increased short-term and long-term mortality rates. Meanwhile, Tertile 3 had a higher proportion of diabetics than Tertile 1, but similar to Tertile 2.
Survival analysis
Kaplan–Meier survival analysis based on GAR tertiles revealed that the 30-day, 90-day, and 365-day mortality rates were significantly lower in the Tertile 2, with statistically significant differences between the three groups (P < 0.001) (Fig. 2). This indicates that both high and low levels of GAR are associated with worse short-term and long-term outcomes in critically ill patients with AF.

Kaplan–Meier all-cause mortality survival analysis curve. A Relationship between GAR tertile groups and 30-day mortality; B Relationship between GAR tertile groups and 90-day mortality; C Relationship between GAR tertile groups and 365-day mortality
The association between GAR and patient clinical outcomes
Two Cox regression models were employed to investigate the independent influence of the GAR on mortality (Table 2), both unadjusted and adjusted for age, gender, race, AKI, CKD, HF, hypertension, cancer, stroke, WBC, hemoglobin, creatinine, SOFA score and OASIS score. Using the tertiles 2 as the reference in both models, heightened mortality risks were evident in the other two groups at 30 days, 90 days, and 365 days. In the unadjusted model, compared to the reference group (Tertile 2), the 30-day mortality risk for the third tertile was 2.42 (95% CI 1.83–3.21, P < 0.001), and for the first tertile, it was 1.69 (95% CI 1.25–2.28, P = 0.001). In the multivariate-adjusted model, the HR for the first tertile (reference: the second tertile, 1.00) was 1.53 (95% CI 1 ~ 1.83, P = 0.052), and for the third group, it was 2.56 (95% CI 1.99 ~ 3.54, P < 0.001), with a similar trend observed at 90 days and 365 days.
The dose–response association between the GAR and 30-day, 90-day, and 365-day mortality rates is depicted in Fig. 3, revealing a nonlinear "J-shaped" relationship across all three time points (P non-linear < 0.001). Given the reliability of this nonlinear relationship, a threshold effect analysis was conducted, with the results presented in Table 3. The thresholds for mortality risk at 30-day, 90-day, and 365-day were determined to be 15.915, 17.363 and 18.214, respectively. Beyond these thresholds, the risk of mortality significantly increased with increasing GAR.

Restricted cubic spline curve analysis for GAR and mortality hazard ratio in critically ill patients with AF. A Restricted cubic spline curve for the mortality rate of patients within 30 days; B Restricted cubic spline curve for the mortality rate of patients within 90 days; C Restricted cubic spline curve for the mortality rate of patients within 365 days
Subgroup analysis
Subgroup analyses were conducted for multiple characteristics includingage, gender, race, AKI, CKD, HF, hypertension, cancer, stroke and BMI. No interactions were found (P for interaction > 0.05), indicating robustness of the outcomes, as shown in Tables 4, 5, 6.
Discussion
This study explored the relationship between the GAR, a representative marker of stress-induced hyperglycemia, and the risk of mortality in critically ill patients with AF. We observed that both excessively high and low levels of the GAR are associated with increased risks of short-term and long-term mortality. This relationship persisted even after adjusting for multiple confounding factors. Based on the restricted cubic splines (RCS) curve, a “J-shaped” relationship was established, and threshold analysis of continuous variables was employed to explore the inflection points of the GAR at various survival time points. Additionally, subgroup analyses revealed no interaction effects.
The occurrence of AF is associated with the cardiac electrophysiology, defects in specific molecular pathways, and structural changes in the left atrium [13]. Improvements in the prognosis of AF patients primarily focus on heart rate control, anticoagulation, and stroke prevention [14]. Although catheter ablation can cure AF, it often accompanies uncontrollable recurrence postoperatively. Current research has also demonstrated that preventing nicotinamide adenine dinucleotide (NAD) depletion and subsequent myocardial cell dysfunction, inhibiting inflammatory compounds, and regulating calcium ion homeostasis can improve the prognosis of AF [13].
In fact, as mentioned earlier, myocardial metabolism primarily relies on fatty acids rather than glucose. During periods of stress hyperglycemia, activation of adrenergic responses, increased inflammation and oxidative stress, formation of glycation end products due to high glucose levels, and myocardial dysfunction caused by vigorous glucose metabolism in the myocardium may occur [15]. Additionally, epicardial adipose tissue (EAT) [16] is considered relevant to AF. Against the backdrop of AF, the inflammatory response in EAT can induce fibrosis in atrial myocytes and disrupt neurohormonal factors through regional secretion, accelerating the progression of heart failure. A randomized controlled trial has shown that SGLT-2 inhibition selectively reduces glucose uptake in EAT among patients with type 2 diabetes, decreasing EAT inflammation and thereby enhancing myocardial blood flow to provide a protective effect [16]. Meanwhile, metabolic abnormalities induced by stress hyperglycemia may promote the onset and persistence of AF by regulating atrial substrates, disrupting myocardial energy metabolism and electrical remodeling, and modulating myocardial ion channels, ultimately leading to poor prognosis in AF [17,18,19,20]. Epidemiologically, the impact of stress hyperglycemia on new-onset AF following myocardial infarction has been studied utilizing the stress hyperglycemia ratio (SHR) [21]. Some studies have revealed multifaceted associations between insulin resistance and AF prognosis, post-ablation recurrence, and incident cases in the general populace [22,23,24,25]. Additionally, Terauchi et al. proposed a correlation between HbA1c levels ≥ 8.0% and heightened all-cause mortality risk among AF patients [22]. Although stress-induced hyperglycemia and AF are considered to be related, evidence is lacking regarding the impact of stress hyperglycemia on the prognosis of AF.
Critically ill patients are particularly susceptible to stress-induced hyperglycemia, a phenomenon more prevalent among them compared to individuals in general wards and healthy populations [4, 5]. The intricate interplay of acute systemic inflammation, hormonal fluctuations, and cytokine dysregulation precipitates excessive hepatic glucose secretion, lipid peroxidation, gluconeogenesis, and heightened insulin resistance, collectively contributing to the development of stress-induced hyperglycemia [5, 26,27,28]. Notably, diverse metrics serve as proxies for stress-induced hyperglycemia [29]. Our study found robust J-shaped curve outcomes for both short-term and long-term prognosis in critically ill patients with AF when stress-induced hyperglycemia was represented by the GAR. Moreover, no matter which time point was considered as the observed outcome, the risk of mortality increased with the increase in GAR beyond a certain threshold. Additionally, when the 365-day mortality risk was considered as the study outcome, GAR exhibited a protective factor as it decreases below the threshold. These findings hold substantial clinical significance, particularly given the ongoing debate surrounding glycemic management in critically ill patients [30,31,32,33,34]. A recent article in The Lancet Diabetes & Endocrinology underscored the importance of glycemic management in both diabetic and non-diabetic critically ill populations [35].
Considering the high prevalence of AF in ICU settings [2], coupled with the close association between AF and stress-induced hyperglycemia, our study provides valuable insights for guiding future glycemic targets in critically ill patients with AF. Additionally, it aids in identifying critically ill AF patients at high risk of mortality.
Limitations
This is a retrospective study and cannot establish causality. The lowest blood glucose value may not actually represent fasting blood glucose. Additionally, glycated hemoglobin has limitations and is influenced by factors such as ethnicity, blood transfusions, certain hemoglobinopathies, hemolytic anemia, post-splenectomy status, polycythemia, and even iron-deficiency anemia. According to previous studies, blood lipids and are significant confounding factors for AF. However, due to over 30% missing data for these indicators, they had to be excluded, which may impact the study results.
Conclusion
The GAR levels exhibited a "J-shaped" linear correlation with both short-term and long-term outcomes in critically ill AF patients. Elevated or reduced GAR levels may indicate adverse prognoses for these patients. This conclusion provides a basis for glucose management in critically ill AF patients.
Availability of data and materials
Data used can be obtained upon a reasonable request to the corresponding author.
Abbreviations
- GAR:
-
Glucose-to-glycated hemoglobin ratio
- AF:
-
Atrial fibrillation
- HbA1c:
-
Glycosylated hemoglobin
- ICU:
-
Intensive care unit
- MIMIC-IV:
-
Medical Information Mart for Intensive Care IV
- AMI:
-
Acute myocardial infarction
- HF:
-
Heart failure
- CKD:
-
Chronic kidney disease
- WBC:
-
White blood cells
- HGB:
-
Hemoglobin
- SOFA:
-
Sepsis-organ failure assessment score
- OASIS:
-
Oxford acute severity of illness score
- RCS:
-
Restricted cubic spline
- HR:
-
Hazard ratio
- SHR:
-
Stress hyperglycemia ratio
- EAT:
-
Epicardial adipose tissue
References
Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, Gillum RF, Kim YH, McAnulty JH Jr, Zheng ZJ, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129(8):837–47.
Bosch NA, Cimini J, Walkey AJ. Atrial fibrillation in the ICU. Chest. 2018;154(6):1424–34.
Carrera P, Thongprayoon C, Cheungpasitporn W, Iyer VN, Moua T. Epidemiology and outcome of new-onset atrial fibrillation in the medical intensive care unit. J Crit Care. 2016;36:102–6.
Roberts GW, Quinn SJ, Valentine N, Alhawassi T, O’Dea H, Stranks SN, Burt MG, Doogue MP. Relative hyperglycemia, a marker of critical illness: introducing the stress hyperglycemia ratio. J Clin Endocrinol Metab. 2015;100(12):4490–7.
Dungan KM, Braithwaite SS, Preiser JC. Stress hyperglycaemia. Lancet. 2009;373(9677):1798–807.
Lorenzo-Almorós A, Casado Cerrada J, Álvarez-Sala Walther LA, Méndez Bailón M, Lorenzo González Ó. Atrial fibrillation and diabetes mellitus: dangerous liaisons or innocent bystanders? J Clin Med. 2023;12(8):2868.
Stanley WC, Recchia FA, Lopaschuk GD. Myocardial substrate metabolism in the normal and failing heart. Physiol Rev. 2005;85(3):1093–129.
Dillmann WH. Diabetic cardiomyopathy. Circ Res. 2019;124(8):1160–2.
Amiel SA, Aschner P, Childs B, Cryer PE, Galan BE, Frier BM, Gonder-Frederick L, Heller SR, Jones T, Khunti K, Leiter LA, Luo Y, McCrimmon RJ, Pedersen-Bjergaard U, Seaquist ER, Zoungas S. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management. Lancet Diabetes Endocrinol. 2019;7(5):385–96.
Su YW, Hsu CY, Guo YW, Chen HS. Usefulness of the plasma glucose concentration-to-HbA(1c) ratio in predicting clinical outcomes during acute illness with extreme hyperglycaemia. Diabetes Metab. 2017;43(1):40–7.
Merlino G, Pez S, Gigli GL, Sponza M, Lorenzut S, Surcinelli A, Smeralda C, Valente M. Stress hyperglycemia in patients with acute ischemic stroke due to large vessel occlusion undergoing mechanical thrombectomy. Front Neurol. 2021;12:725002.
Merlino G, Smeralda C, Gigli GL, Lorenzut S, Pez S, Surcinelli A, Marini A, Valente M. Stress hyperglycemia is predictive of worse outcome in patients with acute ischemic stroke undergoing intravenous thrombolysis. J Thromb Thrombolysis. 2021;51(3):789–97.
Brundel B, Ai X, Hills MT, Kuipers MF, Lip GYH, de Groot NMS. Atrial fibrillation. Nat Rev Dis Primers. 2022;8(1):21.
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498.
Karam BS, Chavez-Moreno A, Koh W, Akar JG, Akar FG. Oxidative stress and inflammation as central mediators of atrial fibrillation in obesity and diabetes. Cardiovasc Diabetol. 2017;16(1):120.
Cinti F, Leccisotti L, Sorice GP, Capece U, D’Amario D, Lorusso M, Gugliandolo S, Morciano C, Guarneri A, Guzzardi MA, et al. Dapagliflozin treatment is associated with a reduction of epicardial adipose tissue thickness and epicardial glucose uptake in human type 2 diabetes. Cardiovasc Diabetol. 2023;22(1):349.
Zhang Q, Liu T, Ng CY, Li G. Diabetes mellitus and atrial remodeling: mechanisms and potential upstream therapies. Cardiovasc Ther. 2014;32(5):233–41.
Yuan M, Gong M, Zhang Z, Meng L, Tse G, Zhao Y, Bao Q, Zhang Y, Yuan M, Liu X, et al. Hyperglycemia induces endoplasmic reticulum stress in atrial cardiomyocytes, and mitofusin-2 downregulation prevents mitochondrial dysfunction and subsequent cell death. Oxid Med Cell Longev. 2020;2020:6569728.
Uemura K, Kondo H, Ishii Y, Kobukata M, Haraguchi M, Imamura T, Otsubo T, Ikebe-Ebata Y, Abe I, Ayabe R, et al. Mast cells play an important role in the pathogenesis of hyperglycemia-induced atrial fibrillation. J Cardiovasc Electrophysiol. 2016;27(8):981–9.
Koracevic GP, Petrovic S, Damjanovic M, Stanojlovic T. Association of stress hyperglycemia and atrial fibrillation in myocardial infarction. Wien Klin Wochenschr. 2008;120(13–14):409–13.
Luo J, Li Z, Qin X, Zhang X, Liu X, Zhang W, Xu W, Liu B, Wei Y. Association of stress hyperglycemia ratio with in-hospital new-onset atrial fibrillation and long-term outcomes in patients with acute myocardial infarction. Diabetes Metab Res Rev. 2024;40(2):e3726.
Terauchi Y, Inoue H, Yamashita T, Akao M, Atarashi H, Ikeda T, Koretsune Y, Okumura K, Suzuki S, Tsutsui H, et al. Impact of glycated hemoglobin on 2-year clinical outcomes in elderly patients with atrial fibrillation: sub-analysis of ANAFIE Registry, a large observational study. Cardiovasc Diabetol. 2023;22(1):175.
Jia S, Yin Y, Mou X, Zheng J, Li Z, Hu T, Zhao J, Lin J, Song J, Cheng F, et al. Association between triglyceride-glucose index trajectories and radiofrequency ablation outcomes in patients with stage 3D atrial fibrillation. Cardiovasc Diabetol. 2024;23(1):121.
Wang Z, He H, Xie Y, Li J, Luo F, Sun Z, Zheng S, Yang F, Li X, Chen X, et al. Non-insulin-based insulin resistance indexes in predicting atrial fibrillation recurrence following ablation: a retrospective study. Cardiovasc Diabetol. 2024;23(1):87.
Liu X, Abudukeremu A, Jiang Y, Cao Z, Wu M, Ma J, Sun R, He W, Chen Z, Chen Y, et al. U-shaped association between the triglyceride-glucose index and atrial fibrillation incidence in a general population without known cardiovascular disease. Cardiovasc Diabetol. 2023;22(1):118.
Barth E, Albuszies G, Baumgart K, Matejovic M, Wachter U, Vogt J, Radermacher P, Calzia E. Glucose metabolism and catecholamines. Crit Care Med. 2007;35(9 Suppl):S508-518.
Zauner A, Nimmerrichter P, Anderwald C, Bischof M, Schiefermeier M, Ratheiser K, Schneeweiss B, Zauner C. Severity of insulin resistance in critically ill medical patients. Metabolism. 2007;56(1):1–5.
Stentz FB, Umpierrez GE, Cuervo R, Kitabchi AE. Proinflammatory cytokines, markers of cardiovascular risks, oxidative stress, and lipid peroxidation in patients with hyperglycemic crises. Diabetes. 2004;53(8):2079–86.
Hu Y, Zhao Y, Zhang J, Li C. The association between triglyceride glucose-body mass index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective study from MIMIC-IV database. Cardiovasc Diabetol. 2024;23(1):64.
Jacobi J, Bircher N, Krinsley J, Agus M, Braithwaite SS, Deutschman C, Freire AX, Geehan D, Kohl B, Nasraway SA, et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40(12):3251–76.
Ichai C, Cariou A, Léone M, Veber B, Barnoud D. Expert’s formalized recommendations. Glycemic control in ICU and during anaesthesia: useful recommendations. Ann Fr Anesth Reanim. 2009;28(7–8):717–8.
Mitchell I, Finfer S, Bellomo R, Higlett T. Management of blood glucose in the critically ill in Australia and New Zealand: a practice survey and inception cohort study. Intensive Care Med. 2006;32(6):867–74.
Mackenzie I, Ingle S, Zaidi S, Buczaski S. Tight glycaemic control: a survey of intensive care practice in large English hospitals. Intensive Care Med. 2005;31(8):1136.
Krinsley JS, Egi M, Kiss A, Devendra AN, Schuetz P, Maurer PM, Schultz MJ, van Hooijdonk RT, Kiyoshi M, Mackenzie IM, et al. Diabetic status and the relation of the three domains of glycemic control to mortality in critically ill patients: an international multicenter cohort study. Crit Care. 2013;17(2):R37.
von Loeffelholz C, Birkenfeld AL. Tight versus liberal blood-glucose control in the intensive care unit: special considerations for patients with diabetes. Lancet Diabetes Endocrinol. 2024;12(4):277–84.
Acknowledgements
We wish to show our gratitude to all those who were involved in this study.
Funding
There were no external funding sources for this study.
Author information
Authors and Affiliations
Contributions
Author FYQ collected and processed the data, as well as wrote this article. XC and WX provided language help and writing assistance. WGF proofread the article. WX helped review the revised manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The review boards of the Massachusetts Institute of Technology (MIT) and Beth Israel Deaconess Medical Center approved the use of the MIMIC-IV database. Since the participants in the study were anonymized and de-identified, this study was exempt from the requirements for ethical approval and informed consent.
Consent for publication
All authors agree to publish this work.
Competing interests
The authors have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fu, Y., Wei, X., Cong Xu et al. Independent effects of the glucose-to-glycated hemoglobin ratio on mortality in critically ill patients with atrial fibrillation. Diabetol Metab Syndr 16, 171 (2024). https://doi.org/10.1186/s13098-024-01401-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-024-01401-0