
Abstract
Background
Quality, evidence-based obesity management training for family medicine residents is needed to better support patients. To address this gap, we developed a comprehensive course based on the 5As of Obesity Management™ (ASK, ASSESS, ADVISE, AGREE, ASSIST), a framework and suite of resources to improve residents’ knowledge and confidence in obesity counselling. This study assessed the course’s impact on residents’ attitudes, beliefs, and confidence with obesity counselling.
Methods
The course combines lectures with a bariatric empathy suit experience, standardized and in-clinic patient practice, and narrative reflections. Using a multi-methods design we measured changes in 42 residents’ attitudes, beliefs, and self-confidence and thematically analyzed the narrative reflections to understand residents’ experience with the course content and pedagogy.
Results
Following the course, residents reported improved attitudes towards people living with obesity and improved confidence for obesity counselling. Pre/post improvement in BAOP scores (n = 32) were significant (p < .001)., ATOP scores did not change significantly. Residents showed improvement in assessing root causes of weight gain (p < .01), advising patients on treatment options (p < .05), agreeing with patients on health outcomes (p < .05), assisting patients in addressing their barriers (p < .05), counseling patients on weight gain during pregnancy, (p < .05), counseling patients on depression and anxiety (p < .01), counseling patients on iatrogenic causes of weight gain (p < .01), counseling patients who have children with obesity (p < .05), and referring patients to interdisciplinary providers for care (p < .05).
Qualitative analysis of narrative reflections illustrates that experiential learning was crucial in increasing residents’ ability to empathically engage with patients and to critically reflect on implications for their practice.
Conclusion
The 5AsT-MD course has the potential to increase residents’ confidence and competency in obesity prevention and management. Findings reflect the utility of the 5As to improve residents’ confidence and competency in obesity management counselling.
Similar content being viewed by others


Background
The prevention and management of obesity and related chronic diseases is an integral aspect of family medicine. These conditions are affecting increasing numbers of adults and children [1, 2]. Both the United States Preventive Services Task Force and the Canadian Task Force on Preventive Health Care recommends that primary care practitioners screen patients, counsel regarding weight loss, and refer to structured behavioural interventions aimed at weight loss [3, 4]. However, addressing obesity in a clinical consultation can be challenging for both physicians and patients. In fact, many physicians are not routinely discussing weight and report a lack of confidence in obesity management skills, lack of time, and fear of endangering their relationship to patients by discussing weight [5,6,7,8,9,10,11]. Predominant societal negative attitudes towards persons living with obesity also affect care and further complicate clinical conversations [12, 13]. As a result, patients often feel uncomfortable bringing up weight concerns despite expressing their need for physicians to initiate such a conversation [14,15,16,17].
One of the challenges for effective obesity counselling is that medical residents and students do not receive sufficient training on the complex biopsychosocial etiology of obesity and evidence-based management strategies, and these topics are not well covered in medical exams [18,19,20,21,22]. A recent review concluded that across the world there is a paucity of obesity education programs for learners in health professions [23]. Reasons include the relative newness of classifying obesity as a disease, the complexity of causation and management, and the socio-cultural and personal associations that physicians, residents, medical educators, and patients bring to each interaction that addresses obesity [13, 24,25,26,27]. The result is a substantial lack of capacity in primary health care to deliver comprehensive, tailored, and effective obesity prevention and management [28,29,30,31]. Despite calls from international health and professional organizations to improve curriculum and training in obesity and evidence that high-quality education programs can improve outcomes [23], progress has been slow and no widely recognized courses have been implemented to date [30, 32,33,34].
It is essential that family medicine residents are prepared to: 1) identify complex causes of obesity and its associations with comorbidities and mental health, 2) counsel on appropriate weight management options, and 3) navigate interdisciplinary teams and resources to best assist the patient. There is a pressing need to create high quality, evidence-based obesity management training courses for family medicine residents so they can deliver quality patient care.
This paper reports on the pilot run of a new educational intervention to better prepare family medicine residents for obesity management, the 5AsT-MD course. The course draws on the “5As of Obesity Management™”(ASK, ASSESS, ADVISE, AGREE, ASSIST), which is an evidence-based framework to guide practitioners’ obesity counseling [35,36,37], and utilizes available 5AsT tools and resources developed by the 5As Team to support primary care obesity conversations [38]. In addition to introducing these counseling supports, the course aimed at fostering transformative learning through combining interactive lectures with experiential learning including wearing bariatric empathy suits, patient practice, and reflection. The purpose of the study was to understand the courses’ impact on residents’ knowledge, attitudes, and confidence with obesity counselling.
Methods
The 5AsT-MD course was delivered to two cohorts (fall 2015 and spring 2016) of first year family medicine residents training at the University of Alberta (n = 61) as part of the mandatory Doctor-Patient Relationship (DPR) course. Course elements are described in detail in Table 1.
In summary, the 5As approach to obesity management understands root causes of obesity as more than diet and exercise, and considers the impact of mental health, social situations, obesogenic medications, and comorbid diseases on peoples’ ability to change. The course drew on transformative pedagogy that emphasizes critical reflection and experiential learning [42]. The 5As approach and tools were reviewed in the interactive lectures and practiced both with standardized patients during the course and with patients in clinic. Because of time restrictions through departmental course restructuring, we condensed and refined some of the lecture material and optimized scheduling of the activities for the second cohort using feedback from the first cohort.
We used a multi-methods research design to assess: 1) Did the 5AsT-MD course improve attitutdes and beliefs by increasing awareness of the complexity and lived reality of obesity? 2) Did the 5As approach and 5AsT resources improve residents’ confidence in their obesity counselling practice? All residents, regardless of whether they consented to participate in the research study, were asked to complete the course assignments (questionnaires and narrative reflections) which were not graded. Written consent was obtained from residents before the first lecture of the course. These assignments were de-identified by a neutral third party. Researchers were only given access to data from residents who consented.
Quantitative methods: beliefs, attitudes, and confidence measures
Residents completed the Beliefs About Obese Persons Scale (BAOP), and Attitudes Towards Obese Persons Scale (ATOP) prior to and immediately following the course. Both are brief and well validated measures that made participation in an evaluation more feasible for our residents cohort. The BAOP is a continuous scale, derived from eight Likert Scale questions, that measures beliefs about the causes of obesity [43]. Scores range from 0 to 48 with higher scores suggesting a stronger belief that an individual may not control and not be responsible for their disease, as compared to the inverse of blaming or assigning fault to the individual. Previous research has reported adequate internal reliability (Chronbach’s α = 0.65 to 0.82) [44].
The ATOP is also a continuous scale, derived from 20 Likert scale questions measuring perceptions and attitudes about persons living with obesity. Scores range from 0 to 120 with higher scores reflecting more positive attitudes. Previous research has reported adequate internal reliability (Chronbach’s α = 0.76 to 0.84) [43].
Changes in residents’ level of confidence was assessed using a 29-item questionnaire which was developed specifically for this course (see additional file 1). The questionnaire collects demographic information (age, gender, years of medical training), and uses a 5-point Likert scale to rate: 1) the importance of obesity management as part of family physicians’ role; 2) perceptions on the adequacy of previous training in obesity management; 3) movitation to learn more about this area; and, 4) 22 items about comfort using the 5As in their consultations with patients.
Data from participants who completed all three pre- and post- questionnaires were included in the analysis. Mean scores and standard deviations were calculated for each questionnaire. Two tailed, paired t-tests were applied, in order to assess change between pre and post using Microsoft Excel 2010. P values less than 0.05 were considered statistically significant.
Qualitative methods: narrative reflections
To facilitate critical reflection, learning, and foster sharing and support among plural - residents, participants wrote two brief narrative reflections as part of their course assignment: one after wearing the empathy suit; and the second after the in-clinic practice. To mitigate challenges with residents’ ability to reflect on their experience, revealed through preliminary analysis of the fall cohort, we added guiding questions to the instruction sheets for the spring cohort (see additional file 2).
Narratives of consenting residents were analyzed to gain insights into their experience of the course content and pedagogy. Narratives were de-identified and imported into NVivo11 for thematic analysis. To capture insights not anticipated by the research team and literature, TL first coded inductively and noted emerging patterns. Analyst triangulation was used in two steps. First, data, codes, and emergent themes were discussed during monthly team meetings that included researchers, course instructors, and a patient champion until consensus was reached. Second, guided by these patterns, TL and EC reviewed the literature in education and added theoretically derived codes to the node manual to generate findings that can be analyzed and situated in existing pedagogical theory. All narratives were re-coded using the revised manual including inductive and deductive nodes. Because logistical changes were made to the course from fall to spring cohorts, we compared between cohorts as well as comparing first and second reflections within cohorts to crystallize patterns and themes.
Results
Demographic data
Written consent was obtained from 42 (69%) of the 61 residents who were enrolled in the DPR course from the fall and spring cohort. Demographic characteristics are detailed in Table 2. Of the 42 residents who consented, 32 completed all three questionnaires. All 42 residents submitted a narrative reflection on their experience with the empathy suit and 31 residents submitted a narrative reflection based on their experience with a patient in clinic.
Changes in beliefs, attitudes, and confidence
Mean scores on the BAOP questionnaire revealed a significant improvement in study participants’ positive beliefs about people living with obesity following the course. ATOP questionnaires which started out high, yielded no meaningful change in attitudes toward people living with obesity (see Table 3).
Prior to the course, all of the residents who submitted questionnaires (n = 32) believed that obesity management was an important part of their job as a physician, 28% felt that they had received adequate medical training to manage obesity, and 91% were motivated to learn more about the topic (see Table 4). Following the course, residents still felt that obesity management was an important part of their job, but 47% of the residents felt better trained and 88% wanted to learn more.
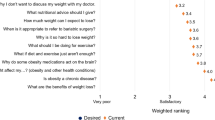
Statistically significant results were found in 9 of the 22 parameters on the course questionnaire, which measured changes in residents’ self-reported confidence in their weight management encounters (see Table 5). Following the course, residents felt more comfortable assessing root causes, advising on treatment options, agreeing with patients on goals, assisting patients in addressing barriers, counseling on weight gain during pregnancy, counseling on weight-related depression and anxiety, counseling on iatrogenic causes of weight gain, counseling patients who have children with obesity, and referring patients to interdisciplinary healthcare providers for care.
Narrative reflections on course experience and utility for practice
Overall, residents perceived the teaching content and methods as useful and offering value for their practice. The majority expressed appreciation for the experiential elements of the course. Four themes emerged during analysis; representative quotes are given in Table 6.
Experiential learning: increased empathy and evoked resistance
Experiential learning elements of the course proved crucial in increasing residents’ stated ability to empathically engage with patients and critically reflect on the implications for their practice. The empathy suit experience emotionally impacted residents who did not have previous lived experience with overweight or obesity. This helped them examine their assumptions about living with obesity. Most noted surprise about how cumbersome tasks of daily living were in the empathy suit. They described feeling exhausted, breathless, afraid of not being able to get out of bed, insecure about falling, and wanting to avoid unnecessary energy expenditure. Many wrote about how the experience of imagining themselves in a larger body, caused feelings of shock, shame, self-consciousness, and embarrassment.
Many critically examined their counselling practice of recommending specific amounts of exercise after having an embodied sense of the practical and emotional reality of living with obesity. Residents wrote about how they came to realize that their recommendations to patients might have been unrealistic and unhelpful. Most concluded that this experience allowed them to feel more empathetic to their patients.
Two residents felt disoriented as to the purpose of the empathy suit session and perceived it as ineffective and a waste of time.
Reflexivity: examining assumption to improve practice
Learning about the complexity and chronicity of obesity encouraged residents to re-investigate their assumptions about the causes of obesity, management and counselling, and their professional identity with regards to supporting patients. For the majority, this reflection led to forming intentions to adopt more empathetic and comprehensive approaches to weight management.
The narratives illustrated a wide range of beliefs about and attitudes toward people with obesity that affect residents’ counselling practice. Some described their “personal frustration with being unable to help them manage their obesity” (participant 12). Others explained their difficulties accepting obesity as a disease (participant 22) and postulated that “in terms of science and numbers, it is possible for every single patient to lose weight” (participant 34). However, many described a shift in their knowledge and a re-thinking of their previously held assumptions resulting from the course. For example, residents described how lack of awareness of physiological and medical barriers to losing weight may have led to inappropriate weight loss expectations. Some reflected on the psychological impact that clinic environment or procedures, such as ill-fitting gowns or larger blood pressure cuffs, has on patients with obesity.
Furthemore, many explained how the course helped them recognize the important role they play in helping patients understand the complex factors contributing to weight, finding realistic strategies to improve health, and supporting them throughout their efforts. Others emphasized that they now recognized the importance of contextual factors of patients’ life history and circumstances. Many highlighted learning about prevention as a crucial part of their role as physicians.
Again, a small number of residents questioned the importance of the topic and were not open to reflect on their practice.
The 5As and 5AsT tools: supported confidence
Most residents described the 5As of obesity management as a useful framework, and the 5AsT tools as helpful, to improve the quality of their practice and increase their confidence with weight counselling.
Almost all residents applied the 5As approach during their in-clinic practice. Many highlighted the importance of beginning the the conversation by asking the patient for permission to talk about weight. As a result, they felt they were able to create a respectful relationship with patients; and patients were more open to the discussion. Others emphasized the benefit of asking the patient about their story of weight gain for comprehensively assessing root causes. A number reflected on how the 5As approach requires practice, a long-term physician-patient relationship, and repeated follow-up encounters.
Many felt that using the 5As approach and tools in clinic allowed them to feel more comfortable with discussing weight and to experience more successful encounters. With these positive experiences, residents imagined themselves playing a positive role in supporting patients with obesity. Many expressed their intention to use the 5As for obesity management in their own practice, to adjust them to their patients’ needs, and refine their skill in using the approach.
Complexity of obesity: challenges for practice
Narratives reflected how residents’ own experiences are enmeshed with societal values and beliefs about obesity, which can pose challenges in their encounters with patients.
Some described discomfort with the subject and fear of offending patients. Others wrote about how they perceived patients to “fail” with weight management and, as a result, feel frustrated with being unable to help. Residents described how they noticed themselves judging patients’ motivation or intelligence, feeling challenged by patients’ questions, frustrated, and questioning the utility of weight counselling all together. Time limitations were mentioned as another challenge. A small number explained the difficulty of letting go of expectations of weight loss for both patients and for themselves as physicians.
Many of these reflections on challenges demonstrate that obesity is often perceived as a product of the patients’ lifestyle and personal qualities.
Discussion
The 5AsT-MD course proved a promising approach to better prepare residents for obesity counselling. The course improved residents’ knowledge, confidence, and attitudes to engage in patient-centred conversations about obesity. The study findings demonstrate the overall success of the course, yet they also reveal the unique challenges of teaching obesity management in residency programs. These challenges highlight precisely why there is a need for obesity prevention and management training in family medicine. Due to insufficient training in medical school and lack of understanding of the disease, an over-simplified approach may perpetuate unsupportive blame and shame. While most residents considered obesity prevention and management an important aspect of their work, less than a third felt they had received sufficient training. After the course about half felt better prepared and a large majority felt inspired to learn more about the subject in order to improve their practice.
Using a multi-methods approach provided a richer understanding of how the content and pedagogical approach of the 5AsT-MD course impacted learners. Findings elucidate that understanding the complexity and chronicity of obesity is important for developing empathy. Experiential learning components of the course were particularly impactful and facilitated critical reflection that served to enhance professional identity development around non-judgemental and compassionate care of patients living with obesity.
Medical education has not responded adequately to the complexity of obesity and the need for tailored coordinated primary care. As a result, individual physicians’ approach to obesity largely focuses on treating comorbidities and counselling lifestyle changes such as diet and exercise. As our findings confirm, this approach is often ineffective and leads both the patient and the physician to have unrealistic expectations, feel frustration, and contribute to feelings of shame and blame [14]. Avoiding stigmatization in health care, as well as addressing the psychological aspects of living with obesity, have been emphasized as one of the most important tasks for primary care obesity management in the recently developed guidelines for patient-centred obesity management in Europe [45].
Because of the entanglement of obesity in societal attitudes, merely increasing didactic teaching of obesity content is not sufficient. Our results demonstrate that residents need support to examine the assumptions that underlie their practice and transform their approach to be more evidence-based and patient-centred. There are calls for educational approaches that will help address the growing inequalities within health care systems worldwide. Just as the Flexner report changed the landscape of medical education in North America in the twentieth century [46], the Lancet Commission Report is raising the need for transformative learning as an approach that will support global complexities while responding to local contextualities [42]. Transformative pedagogy is about inviting “deep structural shifts” in thinking [47]. by providing learners with the the opportunities to reframe their thinking and meaning structures in order to alter their behaviours, attitudes, and beliefs [48, 49]. In a recent scoping review [50]. transformative learning in health professional education was found to occur when: learners critically engaged with their beliefs, biases, and habits of mind; learners were encouraged to become independent, reflective, and critical thinkers; learners were immersed in different contexts, specifically outside of the classroom; learners were exposed to interactive and experiential learning; and, learners practiced competencies that supportted new ways of thinking (i.e., empathetic listening). Importantly, this review outlined that transformative learning has been shown to influence professional identity development by heightening the awareness of others and enhancing humanistic values, key components of delivering quality and safe care to patients and families. The empathy suit experience was designed for this purpose and allowed residents to confront their assumptions about persons living with obesity and expose the difficulties involved with routine daily activities. Our findings suggest such an approach can help foster critical consciousness [51] —a reorientation of perspective towards social justice—that can “rehumanize” relationships and improve patient care.
While the 5AsT-MD course resulted in a shift towards a more empathic, engaged, and comprehensive approach, the outcomes varied depending on beliefs and attitudes of individual residents prior to the course. It is important to “scaffold” the information when designing obesity training and build from where the learner audience is at [52]. The narratives reflected how emotionally laden the topic is for many. As a result, there is a danger to create a level of discomfort and disorientation that hinders reflection and learning. On the other hand, discomfort and embodied experiences can facilitate learning about how to improve practice [53]. Findings underscore the need for further research on effective pedagogical strategies for training courses focused on improving the confidence, knowledge, and attitudes of family medicine residents working with people with obesity. Disseminating and adapting the course to various different educational contexts requires drawing on research on different modes of delivery including, online resources, that allow for experiential and transformative learning [54].
Overall, residents greatly appreciated the 5As of obesity management as a framework and the 5AsT tools to guide them through their conversation with the patient.
Limitations
While the sample size is small comparatively, the course took place in a large residency program in Canada and, therefore, we feel reflects a valid sample with findings that will be of interest and practicality for medical educators. Mean scores for both the BAOP and ATOP were higher than means found in other studies [43, 48, 49, 51]. This may suggest that residents may not have felt comfortable expressing negative views for fear that they would be evaluated poorly. However, narrative reflections contained a number of negative responses suggesting that residents felt free to express their opinion.
Conclusions
Tailored and co-ordinated primary care is crucial to reducing obesity and improving health. 5AsT-MD has the potential as a course for increasing residents’ knowledge of obesity and its complexity, as well as their competency and confidence in engaging patients in effective obesity management. The course’ pedagogical orientation and experiential components offer a novel approach to obesity management training that stretches beyond the biomedical realm and introduces the human complexity and contextuality of living with obesity. This study illustrates how this course fostered transformative learning through engaging learners in experiences offered spaces to reflect and think about what it is like to live with obesity. Our results inform an ongoing process of further refining and disseminating the course to other institutions.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 5As:
-
5As of Obesity Management™: ASK, ASSESS, ADVISE, AGREE, ASSIST
- 5AsT:
-
5As Team research program
- 5AsT-MD:
-
5AsT for Doctors of Medicine
- ATOP:
-
Attitudes Towards Obese Persons Scale
- BAOP:
-
Beliefs About Obese Persons Scale
- DPR:
-
Doctor-Patient Relationship course
References
Canadian Medical Association. CMA recognizes obesity as a disease [Internet]. Available from: https://www.cma.ca/En/Pages/cma-recognizes-obesity-as-a-disease.aspx. [cited 2016 Mar 14].
Government of Canada SC. Body mass index, overweight or obese, self-reported, adult, age groups (18 years and older) [Internet]. 2018. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009620. [cited 2018 Aug 3].
Brauer P, Connor Gorber S, Shaw E, Singh H, Bell N, Shane AR, et al. Recommendations for prevention of weight gain and use of behavioural and pharmacologic interventions to manage overweight and obesity in adults in primary care. CMAJ. 2015 Feb 17;187(3):184–95.
Final Recommendation Statement: Obesity in Adults: Screening and Management - US Preventive Services Task Force [Internet]. Available from: https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/obesity-in-adults-screening-and-management. [cited 2018 Aug 3].
Kirk SFL, Penney TL, McHugh T-L, Sharma AM. Effective weight management practice: a review of the lifestyle intervention evidence. Int J Obes. 2011;36(2):178–85.
Sinclair J, Lawson B, Burge F. Which patients receive advice on diet and exercise? Do certain characteristics affect whether they receive such advice? Can Fam Physician Médecin Fam Can. 2008;54(3):404–12.
Brauer PM, Sergeant LA, Davidson B, Goy R, Dietrich L. Patient reports of lifestyle advice in primary care. Can J Diet Pract Res Publ Dietit Can Rev Can Prat Rech En Diététique Une Publ Diététistes Can. 2012;73(3):122–7.
Jay M, Chintapalli S, Squires A, Mateo KF, Sherman SE, Kalet AL. Barriers and facilitators to providing primary care-based weight management services in a patient centered medical home for Veterans: a qualitative study. BMC Fam Pract. 2015;16 Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4647798/. [cited 2016 Apr 13].
Salinas GD, Glauser TA, Williamson JC, Rao G, Abdolrasulnia M. Primary care physician attitudes and practice patterns in the management of obese adults: results from a national survey. Postgrad Med. 2011;123(5):214–9.
Jochemsen-van der Leeuw HGA, van Dijk N, Wieringa-de Waard M. Attitudes towards obesity treatment in GP training practices: a focus group study. Fam Pract. 2011;28(4):422–9.
Davis NJ, Shishodia H, Taqui B, Dumfeh C, Wylie-Rosett J. Resident physician attitudes and competence about obesity treatment: need for improved education. Med Educ Online. 2008;13:5.
Phelan S, Burgess D, Yeazel M, Hellerstedt W, Griffin J, van Ryn M. Impact of weight bias and stigma on quality of care and outcomes for patients with obesity. Obes Rev. 2015;16(4):319–26.
Forhan M, Salas XR. Inequities in healthcare: a review of Bias and discrimination in obesity treatment. Can J Diabetes. 2013;37(3):205–9.
Kirk SF, Price SL, Penney TL, Rehman L, Lyons RF, Piccinini-Vallis H, et al. Blame, shame, and lack of support a multilevel study on obesity management. Qual Health Res. 2014;24(6):790–800.
Janke EA, Ramirez ML, Haltzman B, Fritz M, Kozak AT. Patient’s experience with comorbidity management in primary care: a qualitative study of comorbid pain and obesity. Prim Health Care Res Dev. 2016;17(01):33–41.
Kirk SF, Tytus R, Tsuyuki RT, Sharma AM. Others. Weight management experiences of overweight and obese Canadian adults: findings from a national survey. Chronic Inj Can. 2012;32(2):63–9.
Torti J, Luig T, Borowitz M, Johnson J, Sharma A, Campbell-Scherer D. The 5As team patient study: patient perspectives on the role of primary care in obesity management. BMC Fam Pract. 2017;18(19):1–10.
Stanford FC, Johnson ED, Claridy MD, Earle RL, Kaplan LM. The role of obesity training in medical school and residency on bariatric surgery knowledge in primary care physicians [internet]. Int J Family Med. 2015; Available from: https://www.hindawi.com/journals/ijfm/2015/841249/.
Rincon-Subtirelu M. Education as a tool to modify anti-obesity bias among pediatric residents. Int J Med Educ. 2017;8:77–8.
Brown I, Flint SW. Weight Bias and the training of health professionals to better manage obesity: what do we know and what should we do? Curr Obes Rep. 2013;2(4):333–40.
Kushner RF. Clinical assessment and Management of Adult Obesity. Circulation. 2012;126(24):2870–7.
Martins C, Norsett-Carr A. Obesity knowledge among final-year medical students in Norway. Obes Facts. 2017;10(6):545–58.
Mastrocola MR, Roque SS, Benning LV, Stanford F. Obesity education in medical schools, residencies, and fellowships throughout the world: a systematic review. Int J Obes. 2019;24. https://doi.org/10.1038/s41366-019-0453-6.
Block JP, DeSalvo KB, Fisher WP. Are physicians equipped to address the obesity epidemic? Knowledge and attitudes of internal medicine residents. Prev Med. 2003;36(6):669–75.
Baltimore RS, Gewitz M, Baddour LM, Beerman LB, Jackson MA, Lockhart PB, et al. Infective endocarditis in childhood: 2015 update: a scientific statement from the American Heart Association. Circulation. 2015;132(15):1487–515.
Huizinga MM, Cooper LA, Bleich SN, Clark JM, Beach MC. Physician respect for patients with obesity. J Gen Intern Med. 2009;24(11):1236–9.
Richard P, Ferguson C, Lara AS, Leonard J, Younis M. Disparities in physician-patient communication by obesity status. Inq J Health Care Organ Provis Financ. 2014;51:0046958014557012.
Asselin J, Osunlana A, Ogunleye A, Sharma A, Campbell-Scherer D. Missing an opportunity: the embedded nature of weight management in primary care. Clin Obes. 2015;5(6):325–32.
Rippe JM, McInnis KJ, Melanson KJ. Physician involvement in the Management of Obesity as a primary medical condition. Obes Res. 2001;9(S11):302S–11S.
Dietz WH, Baur LA, Hall K, Puhl RM, Taveras EM, Uauy R, et al. Management of obesity: improvement of health-care training and systems for prevention and care. Lancet. 2015;385(9986):2521–33.
Forman-Hoffman V, Little A, Wahls T. Barriers to obesity management: a pilot study of primary care clinicians. BMC Fam Pract. 2006;7(1):1.
RCP report concludes that all health professionals need obesity training [Internet]. RCP London. 2010. Available from: https://www.rcplondon.ac.uk/news/rcp-report-concludes-all-health-professionals-need-obesity-training. [cited 2016 Apr 29].
Vitolins MZ, Crandall S, Miller D, Ip E, Marion G, Spangler JG. Obesity Educational Interventions in U.S. Medical Schools: A Systematic Review and Identified Gaps. Teach Learn Med. 2012;24(3):267–72.
Smith S, Seeholzer EL, Gullett H, Jackson B, Antognoli E, Krejci SA, et al. Primary care residents’ knowledge, attitudes, self-efficacy, and perceived professional norms regarding obesity, nutrition, and physical activity counseling. J Grad Med Educ. 2015;7(3):388–94.
Sharma AM. The 5A model for the management of obesity. CMAJ Can Med Assoc J. 2012;184(14):1603–1603 1p.
Fitzpatrick SL, Wischenka D, Appelhans BM, Pbert L, Wang M, Wilson DK, et al. An Evidence-based Guide for Obesity Treatment in Primary Care. Am J Med. 2016;129(1):115.e1.
Jay M, Gillespie C, Schlair S, Sherman S, Kalet A. Physicians’ use of the 5As in counseling obese patients: is the quality of counseling associated with patients’ motivation and intention to lose weight? BMC Health Serv Res. 2010;10(1):1–10.
Osunlana AM, Asselin J, Anderson R, Ogunleye AA, Cave A, Sharma AM, et al. 5As team obesity intervention in primary care: development and evaluation of shared decision-making weight management tools. Clin Obes. 2015;5(4):219–25.
Health Sciences Education and Research Commons. HSERC Spaces. Smart Condo [Internet]. University of Alberta; Available from: https://www.ualberta.ca/health-sciences-education-research/simulation-experiences/hserc-spaces/smart-condo. [cited 2019 Oct 16].
Health Sciences Education and Research Commons. HSERC Spaces. Bariatric/Specialized Care Suite. [Internet]. University of Alberta; Available from: https://www.ualberta.ca/health-sciences-education-research/simulation-experiences/hserc-spaces/specialized-care-suite. [cited 2019 Oct 16].
XXL-Rehab. XXL-Rehab Bariatric Suit. Available from http://www.xxl-rehab.dk/educational_products/fat_suit/. [Internet; cited 2019 Nov 22].
Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376:1923–58.
Allison DB, Basile VC, Yuker HE. The measurement of attitudes toward and beliefs about obese persons. Int J Eat Disord. 1991;10(5):599–607.
Puhl RM, Brownell KD. Confronting and coping with weight stigma: an investigation of overweight and obese adults. Obesity. 2006;14(10):1802–15.
Durrer Schutz D, Busetto L, Dicker D, Farpour-Lambert N, Pryke R, Toplak H, et al. European practical and patient-Centred guidelines for adult obesity management in primary care. Obes Facts. 2019;12(1):40–66.
Prislin MD, Saultz JW, Geyman JP. The Generalist Disciplines in American Medicine One Hundred Years Following the Flexner Report: A Case Study of Unintended Consequences and Some Proposals for Post-Flexnerian Reform. Acad Med. 2010;85(2):228–35.
O’Sullivan E, Morrell A, O’Connor MA. Expanding the boundaries of transformative learning: essays on theory and praxis. New York: Palgrave MacMillan; 2004.
Poustchi Y, Saks NS, Piasecki AK, Hahn KA, Ferrante JM. Brief intervention effective in reducing weight Bias in medical students. Fam Med. 2013;45(5):345–8.
Gujral H, Tea C, Sheridan M. Evaluation of nurse’s attitudes toward adult patients of size. Surg Obes Relat Dis. 2011;7(4):536–40.
Van Schalkwyk SC, Hafler J, Brewer TF, Maley MA, Margolis C, McNamee L, et al. Transformative learning as pedagogy for the health professions: a scoping review. Med Educ [Internet]. 2019 14 ; Available from: [cited 2019 May 2] doi:https://doi.org/10.1111/medu.13804
Flint SW, Hudson J, Lavallee D. Counter-conditioning as an intervention to modify anti-fat attitudes. Health Psychol Res. 2013;1(2):24.
Cameron E. Toward a fat pedagogy: a study of pedagogical approaches aimed at challenging obesity discourse in post-secondary Education. Fat Stud. 20152;4(1):28–45.
Zembylas M, McGlynn C. Discomforting pedagogies: emotional tensions, ethical dilemmas and transformative possibilities. Br Educ Res J. 2012;38(1):41–59.
Nickel F, Tapking C, Benner L, Schüler S, Ottawa GB, Krug K, et al. Video teaching leads to improved attitudes towards obesity-a randomized study with 949 participants. Obes Surg. 2019;29(7):2078–86.
Acknowledgements
The authors acknowledge the most valuable contributions of Karen Moniz for her outstanding administrative and logistical support; of Rena LeFrance and Alison Connors for developing and delivering the pediatrics content of the course; of Shuai Li for performing the statistical analysis in his role as a research assistant; and of Tyler Myroniuk for providing feedback on the quantitative analysis.
Funding
The 5AsT-MD study was funded by Alberta Innovates–Health Solutions (AI-HS), with significant in kind support from the Department of Family Medicine at the University of Alberta, and an unrestricted educational grant through Obesity Canada supported by Novo Nordisk to support training of physicians and teams in obesity prevention and management. None of the funders had a role or influence in the design of the study or in collection, analysis and interpretation of data, or in writing of the manuscript.
Author information
Authors and Affiliations
Contributions
DLC-S, SW, AMS, AV, and DK conceived of the course, delivered the course, and designed the evaluation study. TL performed the qualitative analysis with input from DLC-S and wrote the first draft of the manuscript. MH coordinated the quantitative data analysis, with support from DLC-S, and wrote all parts of the manuscript relevant to quantitative methods and results. EC provided substantial intellectual input with regards to the pedagogical approach and the theoretical frame for transformative learning. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the University of Alberta Health Research Ethics Board – Health Panel (Pro00058323). Written consent was obtained from residents before the first lecture of the course.
Consent for publication
Not applicable.
Competing interests
DCS, received an unrestricted educational grant from Novo Nordisk via Obesity Canada to support the training of physicians and teams in obesity prevention and management. AMS is a member of an advisory board and speaker’s bureau with Novo Nordisk and Valeant and was a member of the Data Safety Monitoring Board for an anti-obesity trial (Takeda).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Pre/post Workshop Assessment.
Additional file 2.
Narrative Reflection Instructions.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Luig, T., Wicklum, S., Heatherington, M. et al. Improving obesity management training in family medicine: multi-methods evaluation of the 5AsT-MD pilot course. BMC Med Educ 20, 5 (2020). https://doi.org/10.1186/s12909-019-1908-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-019-1908-0