
Background
Obesity is an increasing epidemic in both the US and veteran populations, yet it remains largely understudied in the Veteran's Health Administration (VHA) setting. The purpose of our study was to identify barriers to the effective management of obesity in VHA primary care settings.
Methods
Three focus groups of clinicians from a Veteran's Affairs Medical Center (VAMC) and an affiliated Community Based Outpatient Center (CBOC) were conducted to identify potential barriers to obesity management. The focus groups and previously published studies then informed the creation of a 47-item survey that was then disseminated and completed by 55 primary care clinicians.
Results
The focus groups identified provider, system, and patient barriers to obesity care. Lack of obesity training during medical school and residency was associated with lower rates of discussing diet and exercise with obese patients (p < 0.05). Clinicians who watched their own diets vigorously were more likely to calculate BMI for obese patients than other clinicians (42% vs. 13%, p < 0.05). Many barriers identified in previous studies (e.g., attitudes toward obese patients, lack of insurance payments for obesity care) were not prevalent barriers in the current study.
Conclusion
Many VHA clinicians do not routinely provide weight management services for obese patients. The most prevalent barriers to obesity care were poor education during medical school and residency and the lack of information provided by the VHA to both clinicians and patients about available weight management services.
Similar content being viewed by others


Background
Obesity is an increasing epidemic in both the general US population [1] and veterans [2] and is an important etiologic factor in heart disease, diabetes, arthritis, depression, and various types of cancers [3, 4]. It is estimated that among the 6 million users of Veterans Health Administration (VHA) services, 44% are overweight and an additional 25% are obese [5]. Although the U.S. Veterans Health Administration (VHA) is the largest integrated health care system in the United States [6], obesity in this setting has remained vastly understudied.
Despite numerous studies that have defined optimal body mass index (BMI) targets for patients, numerous provider-level barriers exist to the effective management of obesity in primary care. These barriers include lack of formal training of primary care practitioners in nutrition, obesity, and counseling on weight-related topics [7–12], perceived inability to change patient behaviors [12], lack of known effectiveness of treatments [8, 13, 14], negative attitudes toward obese patients [15–17], beliefs that patients are not interested or ready for treatment [9, 12, 19, 20], and beliefs that obesity is the responsibility of the patient [21]. In addition, even though previous research has determined that patients have more confidence in weight counseling made by nonobese physicians, vegetarians, and those who used to be obese [20] and that nurse's weight impacts attitudes towards obesity and its treatment [19], it is unclear how provider's personal weight and exercise practices influence their obesity-related patient practices.
Even when providers do initiate health education and dietary counseling, there is still some controversy over whether these practices actually motivate patient behavior. Although previous studies have determined that the contextual framing of health behavior counseling in a positive (i.e., emphasizing the benefits of weight loss) versus negative (i.e., emphasizing the detriments of remaining obese) manner affects patient's receptivity [22, 23], it is unknown whether framing style has an impact on the successful implementation of weight-related recommendations. Nonetheless, the manner by which clinicians discuss obesity with patients does affect patients' receptiveness to counseling [16], and even modest reductions in weight can lead to significant health benefits [24, 25]. For example, it is estimated that a 10% reduction in weight can extend life expectancy an average of 2–7 months and can reduce lifetime medical expenditures of associated chronic conditions (e.g., heart disease, diabetes) by $2200–$5300 [26].
In addition to provider-related barriers, several previous studies have identified system-level barriers to obesity care. These include lack of payment by insurance companies for weight-related counseling and care [12, 13, 17], lack of time during patient visits [9, 12, 13], lack of available teaching materials for patients [9, 12] and lack of infrastructure support/places to refer patients [27].
Although studies have been conducted to identify barriers to primary care management of obesity, it is unknown whether these barriers exist in the context of the VHA. For one, veterans have different characteristics than the general population (e.g., they are older, more likely to be male, possibly more resistant to change, possibly more functionally limited making exercise difficult) and the VHA system may not have the same barrier profiles as healthcare settings found in other sectors. The goal of this study was to explore obesity management practices in VHA primary health care. Specifically, we sought to identify provider- and system-level barriers to the effective management of obesity and to determine whether the identified barriers impacted obesity care in these settings. The identification of such barriers is an essential step in the development of more potent strategies for managing obesity and for decreasing the adverse effects of obesity in veterans.
The specific aims of the study were to:
• Describe weight management practices by VHA primary care clinicians
• Examine the relative importance of provider- and system-level barriers to the effective management of obesity
• Study whether barriers and/or personal weight management practices of clinicians impact care for obese patients
Methods
Our aims were addressed by using focus groups to inform the creation and administration of a survey to primary care clinicians (attending physicians and physician assistants, resident physicians) in the Iowa City Veteran's Affairs Medical Center (VAMC) and primary care clinicians practicing at the Bettendorf Community Based Outpatient Clinic (CBOC). All research was approved by the University of Iowa Institutional Review Board (IRB) and the Veteran's Affairs (VA) Research and Development committees prior to initiation.
Focus groups
Based on previous research, we developed a list of four open-ended focus group questions to ask participants. Three focus groups were conducted on 1) Iowa City VAMC attending clinicians (n = 3), 2) Iowa City resident physicians (n = 3), and 3) Bettendorf CBOC attending clinicians (n = 3). We asked each group of clinicians four open-ended questions about barriers to addressing and treating obesity, whether barriers were unique to the VA setting, and suggestions for improving current system of obesity care in the VA. Focus groups lasted approximately 45 minutes each, and responses were recorded by two members of the study team (VFH, AL). Themes emerging from the responses were compiled and combined into a master list of barriers identified (see Table 1).
Survey
Based on previous studies and focus group responses, we then created our 47-item survey. Questions addressed weight management practices for obese patients, both provider- and system-level barriers to weight management, beliefs about obesity and obesity care, usefulness of additional obesity-related services, provider personal weight management characteristics, context of weight framing (positive vs. negative), and demographic information. The context of the weight framing question is shown in Table 2. We included items on the clinicians' personal weight management practices to explore whether personal practices affected the likelihood of providing weight management services to obese patients. To test the face and content validity of the survey, we distributed it to a subset of three primary care clinicians to review its content and ease of use prior to the distribution of the survey to all eligible clinicians. We made several small changes to our survey to improve the flow of the questions.
Participants
All primary care physician assistants (PAs) and physicians (attendings and residents) at the Iowa City VAMC and the Bettendorf CBOC were eligible to complete the study survey (n = 22 attendings and PAs and n = 75 residents).
Survey administration
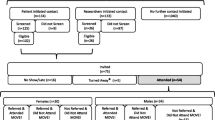
We administered the surveys in person to each of the three test groups (VAMC attending clinicians, VAMC resident physicians, CBOC attending clinicians) at normally scheduled meetings. The survey took 10–15 minutes to complete. We included a signature card with the survey to sign if they either a) did complete the survey or b) did not wish to complete the survey. This response card was collected separately from the surveys to protect anonymity and to facilitate follow-up of eligible providers who were present during the initial survey administration. We did not follow-up with anyone who returned the survey response card. To increase response rates, we followed-up with eligible clinicians who did not sign the signature card by sending the survey through email for completion. Our final sample consisted of 17 attending physicians and physician assistants (77% response rate) and 38 resident physicians (51% response rate).
Data entry and analysis
Data was double-entered and imported into SPSS version 10 statistical software. We conducted simple descriptive statistics such as means and frequency tables for all variables. Body mass index (BMI) of the providers was calculated by dividing weight in kilograms by height in meters squared. We also recoded many of the likert scale variables into dichotomous variables to ease interpretation.
Weight management practices
- Always vs. Sometimes/Rarely/Never
We categorized responses to weight management practices into Always vs. Sometimes/Rarely/Never since nearly all respondents reported at least "Sometimes" performing these practices, and because guidelines suggest performing these practices always on overweight and obese patients.
Barriers, beliefs, and usefulness of additional services
- Strongly Agree/Agree vs. Neutral/Disagree/Strongly Disagree
We dichotomized in this manner since we wanted to compare affirmed responses to those with neutral or negative responses.
Provider body mass index (BMI)
- Overweight (BMI of 25+) vs. Not Overweight (BMI < 25)
We dichotomized in this manner based on the current definition for overweight (BMI of 25+).
Weight loss attempts
- Never vs. At Least Once or more frequent
We dichotomized in this manner so that we could distinguish never dieters from those who dieted at least once.
Dietary vigilance
- Moderately/Vigilantly/Very Vigilantly vs. Not at All/Slightly
We dichotomized in this manner given the distribution and interest in providers with at least moderate levels of dietary vigilance.
Exercise
- 3+ times per week vs. < 3 times per week
We dichotomized in this manner given our interest in providers with at least moderate levels of exercise, weekly.
We performed chi-square tests to assess the association between sets of two dichotomous variables of interest. For analyses where at least one expected cell size of the 2 × 2 table was less than 5, we used the Fisher's Exact Test to test for significance. We examined relationships between actual weight management practices and barriers, personal weight management practices of clinicians, framing of counseling practices, and demographic variables of clinicians. Barriers were identified as those items that most impacted rates of actual weight management practices.
Results
Our sample was mostly comprised of males (63.6%), residents (69.1%), and clinicians from the Iowa City VAMC (85.5%). Over 40% of providers were overweight, most had tried to lose weight in the past (64.8%), most reported moderately to very vigilantly watching their diets (72.3%), and 29.6% reported exercising 3 or more times per week.
Clinician-reported rates of current weight management practices for obese patients were moderately low (Table 3). With respect to provider-level barriers to obesity care, few clinicians reported learning good obesity management practices in medical school (23.6%) and residency training programs (30.9%). Only 32.7% believed most obese patients are not ready to do anything about their weight, and few agreed (5.5%) that there are few effective treatments for obesity (Table 4). System-level barriers to obesity care included clinicians wanting more education about weight management services offered by the VA (94.4%), as well as recognition of the need for the VA to develop more comprehensive weight management services (83.6%) and to make obesity a higher priority (76.4%). Relatively few (27.3%) agreed that lack of payment by insurers hinders weight management practices in the VA healthcare system. Obesity-related beliefs included believing obesity to be a major public health problem and difficult to treat (98.2% and 96.4%, respectively) and considering obesity to be a disease (85.5%). Clinicians stated that older obese patients and those with comorbidity increase the likelihood of addressing and/or treating obesity. The need for more educational materials about weight management to pass out to patients (90.9%) and the need for an obesity educator (87.3%) and dietician (85.5%), physical therapist (81.8%) and behavioral counselor (83.6%) referrals for obese patients were expressed by most respondents. Most clinicians also believed that both group appointments for obese patients (72.7%) and having patients fill out readiness to change questionnaires about obesity prior to the visit (72.7%) would be helpful. Most respondents did not believe in patient monetary incentives for weight loss (44.4%) or that adding weight loss drugs to the formulary would lead to more frequent prescribing practices (25.5%). When asked to describe the context of their weight counseling messages, a majority of providers reported usually using positively framed messages to patients (77.8%) rather than negatively framed messages (22.2%).
The barrier that most greatly impacted discussing diet or exercise with patients was lack of learning good obesity practices during medical school and residency training programs (Table 5). Clinicians who learned good obesity practices in medical school were more likely to discuss diet or exercise with obese patients than those who reported that they did not learn good obesity practices in medical school (62% vs. 31%, respectively, p < 0.05). Likewise, clinicians who learned good obesity practices in residency training programs were more likely to always discuss diet or exercise with obese patients than those who reported that they did not learn good obesity practices in residency training programs (59% vs. 29%, respectively, p < 0.05). The vigilance with which clinicians reported watching their own diets was significantly associated with the likelihood of calculating the BMI of their obese patients. Whereas 42% of clinicians who moderately to very vigilantly watched their diets reported always calculating BMIs of obese patients, only 13% of providers who less vigilantly watched their diets did so.
With respect to whether clinicians reported typically counseling obese patients in a positive or negative context, responses to this item differed (nearly significantly) by one obesity belief item and one clinical characteristic. While 83% of clinicians who agreed that obesity is a disease counseled obese patients in a positive context, only 50% of clinicians who did not agree that obesity is a disease counseled obese patients in a positive context (p < 0.10). Likewise, 94% of attending clinicians reported counseling obese patients positively while 70% of residents reported counseling obese patients positively (p < 0.10).
Discussion
Our study shows that many primary care clinicians in the VA do not regularly counsel and refer obese patients to weight management services. The barrier most strongly related to providing diet and exercise counseling was poor obesity education during medical school and residency training programs. In fact, less than a third of respondents reported that they had learned good obesity management practices during medical school and residency training programs. This finding of poor nutrition, exercise, and behavioral counseling in medical and residency training programs has been corroborated in a number of previous studies [7, 8, 12]. In our study, personal dietary vigilance by clinicians also impacted the likelihood of regularly calculating the BMI of obese patients, with more vigilant clinicians being more likely to calculate BMI. Previous studies, too, have found similar results in that physicians with a personal history of obesity or vegetarianism were more likely to provide nutrition and weight counseling to patients [28]. Another study by Hash et al. [20] concluded that patients were more receptive to health counseling given by nonobese physicians.
Contrary to previous studies [17, 29], our study did not find that clinicians feel that their weight loss efforts are futile. Our surveyed clinicians largely believed that many obese patients are ready for weight loss, that physician-delivered weight counseling can be successful, and that effective weight management tools are available.
Although a number of barriers identified in previous studies were confirmed in the current study, several barriers such as attitudes toward obese patients and lack of insurance payments for obesity care were not related to actual weight management practices. Insurance coverage may not have been a barrier since most veterans receiving care in the VHA have coverage for a wide array of services, including obesity-related services, unlike many patients found in the general population.
In addition, clinicians reported access to educational materials for obese patients, ability to refer patients to an obesity educator, dietician, physical therapist, behavioral counselor, and group obesity appointments, and use of a readiness to change questionnaire about weight loss for obese patients as useful weight management services for the VA to implement. Many of these services will be offered as the VHA's Managing Overweight and Obesity in Veterans Everywhere (MOVE!) Program is nationally rolled-out. The program is multidisciplinary in nature and includes five steps of care ranging from patient education to bariatric surgery provided by dieticians, behavioral counselors, obesity educators, clinicians, nurses, physical therapists, and surgeons.
Our study found that the context of weight management counseling practices vary, and that these practices differ by beliefs about obesity and by training level. Clinicians who believe obesity is a disease are more likely to counsel obese patients in a positive context than clinicians who do not believe obesity to be a disease. This may imply that clinicians who believe obesity to be a real clinical entity would be more compassionate towards obese patients than clinicians who feel that obesity is a character flaw or linked to lack of willpower. This finding supports that of Scott et al. [30], who found that clinicians who were the most likely to counsel patients on weight management initiated conversations by "medicalizing" the obesity. Our results also showed that attending clinicians were more likely than resident physicians to counsel positively. Whether this finding is due to the years of experience of the attending physicians or to a shift in obesity counseling norms is indeterminable by this study. In addition, our sample sizes were very small in these analyses, and most context of counseling items required Fisher's Exact Tests for 2 × 2 analyses given the small cell sizes for several of the cells.
Other limitations of our study include our small response rate of resident physicians, our exclusion of nurses, and our sample of only one VAMC and one CBOC. This project served to pilot test our survey, which we plan to distribute to more VAMCs and CBOCs in the near future. We note that the generalizability of our findings may be limited to our region and therefore, should be interpreted with caution. In addition, our pilot study resources prohibited our study of nurses, although future studies are planned to identify obesity-related practices and barriers that nurses in the VA healthcare system face, given their important role in obesity management. High response rates from resident physicians are difficult to capture given their busy schedules and demands from other research projects. We recognize, however, that the residents most likely to have responded may be more conscientious than non-responders, and therefore the rates of various obesity practices may be over-inflated in this study. Nevertheless, our rates of most practices were sufficiently low to warrant additional attention to obesity management in the VA healthcare system. Lastly, due to time constraints, we were not able to perform all of the appropriate reliability testing on our survey instrument, such as test-retest reliability. We are currently conducting these tests and will have completed them before our next round of survey administration.
Our study does, however, have several strengths. For one, this is the first time primary care management of obesity has been examined empirically in the VA to our knowledge. Secondly, although we only gathered respondents from two settings, we did administer the survey to one large VAMC and one smaller CBOC, and also had respondents with two different training levels (attendings and residents). This mix of providers will help increase the reliability of our findings.
Conclusion
Our initial results suggest that efforts to impact the current epidemic of obesity in veterans focus on interventions to improve clinicians' knowledge of obesity management and nutrition and to increase awareness of available obesity management services. This research is necessary to understand how VHA can improve the quality of obesity management. This focus on quality of care and evidence-based practices has accompanied the VHA's shift from a system of tertiary/specialty and inpatient-based care to a primary, outpatient-based care [31, 32].
As the VA rolls out the MOVE! initiative, we can use the results of our study to modify the program appropriately in response to the identified provider-level and system-level barriers. Additionally, our pilot study findings will inform future multi-site provider surveys administered across multiple VAMCs. In addition, given the broad effects of obesity, the results of this study are relevant to many of the other initiatives developed by the VA to improve the control of blood pressure, serum lipids, and blood glucose in an effort to decrease cardiovascular morbidity and mortality, as well as to other healthcare settings incorporating evidence-based care practices into their quality improvement initiatives.
References
Flegal KM, Carroll MD, Ogden CL, Johnson CL: Prevalence and trends in obesity among US adults, 1999–2000. JAMA. 2002, 288 (14): 1723-1727. 10.1001/jama.288.14.1723.
Perlin JB: Undersecretary for Health's information letter. The managing overweight and/or obesity for veterans everywhere (MOVE!) program. 2004, 10-2004-013
Bray GA: Health hazards of obesity. Endocrinol Metab Clin North Am. 1996, 25 (4): 907-919. 10.1016/S0889-8529(05)70361-3.
National Institutes of Health (NIH): National Heart, Lung and Blood Institutes. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults:jj the evidence report. 1998, Bethesda, MD: NIH
Wang A, Kinsinger LS, Kahwati LC, et al: Obesity and weight control practices in 2000 among veterans using VA facilities. Obes Res. 2005, 13 (8): 1405-1411.
Department of Veterans Affairs. Office of Public Affairs, Media Relations. April 2003. : VA Fact Sheet: Facts about the Department of Veterans Affairs. Accessed May 1, 2006, [http://www1.va.gov/opa/fact/docs/vafacts.pdf]
Huang J, Yu H, Marin E, et al: Physicians' weight loss counseling in two public hospital primary care clinics. Acad Med. 2004, 79 (2): 156-161. 10.1097/00001888-200402000-00012.
Fogelman Y, Vinker S, Lachter J, et al: Managing obesity: a survey of attitudes and practices among Israeli primary care physicians. Int J Obes Relat Metab Disord. 2002, 26 (10): 1393-1397. 10.1038/sj.ijo.0802063.
Timmerman GM, Reifsnider E, Allan JD: Weight management practices among primary care providers. J Am Acad Nurse Pract. 2000, 12 (4): 113-116. 10.1111/j.1745-7599.2000.tb00289.x.
Moore H, Adamson AJ, Gill T, Waine C: Nutrition and the health care agenda: a primary care perspective. Fam Pract. 2000, 17 (2): 197-202. 10.1093/fampra/17.2.197.
Block JP, DeSalvo KB, Fisher WP: Are physicians equipped to address the obesity epidemic? Knowledge and attitudes of internal medicine residents. Prev Med. 2003, 36 (6): 669-675. 10.1016/S0091-7435(03)00055-0.
Kushner RF: Barriers to providing nutrition counseling by physicians: a survey of primary care practitioners. Prev Med. 1995, 24 (6): 546-552. 10.1006/pmed.1995.1087.
Billington CJ: The challenge of obesity management in primary care. J Am Board Fam Pract. 2000, 13 (3): 222-223.
Campbell K, Engel H, Timperio A, et al: Obesity management: Australian general practitioners' attitudes and practices. Obes Res. 2000, 8 (6): 459-466.
Price JH, Desmond SM, Krol RA, et al: Family practice physicians' beliefs, attitudes, and practices regarding obesity. Am J Prev Med. 1987, 3 (6): 339-345.
Anderson DA, Wadden TA: Treating the obese patient. Suggestions for primary care practice. Arch Fam Med. 1999, 8 (2): 156-167. 10.1001/archfami.8.2.156.
Foster GD, Wadden TA, Makris AP, et al: Primary care physicians' attitudes about obesity and its treatment. Obes Res. 2003, 11 (10): 1168-1177.
Mercer SW, Tessier S: A qualitative study of general practitioners' and practice nurses' attitudes to obesity management in primary care. Health Bull (Edinb). 2001, 59 (4): 248-253.
Hoppe R, Ogden J: Practice nurses' beliefs about obesity and weight related interventions in primary care. Int J Obes Relat Metab Disord. 1997, 21 (2): 141-146. 10.1038/sj.ijo.0800379.
Epstin L, Ogden J: A qualitative study of general practitioners' views of treating obesity. Brit J Gen Pract. 2005, 55: 750-754.
Hash RB, Munna RK, Vogel RL, Bason JJ: Does physician weight affect perception of health advice?. Prev Med. 2003, 36 (1): 41-44. 10.1006/pmed.2002.1124.
Rothman AJ, Salovey P: Shaping perceptions to motivate healthy behavior: the role of message framing. Psychol Bull. 1997, 121 (1): 3-19. 10.1037/0033-2909.121.1.3.
Campbell MK, DeVellis BM, Strecher VJ, et al: Improving dietary behavior: the effectiveness of tailored messages in primary care settings. Am J Public Health. 1994, 84 (5): 783-787.
Williamson DF: Intentional weight loss: patterns in the general population and its association with morbidity and mortality. Int J Obes Relat Metab Disord. 1997, 21 (Suppl 1): S14-S19.
Blackburn G: Effect of degree of weight loss on health benefits. Obes Res. 1995, 3 (Suppl 2): 211s-216s.
Oster G, Thompson D, Edelsberg J, et al: Lifetime health and economic benefits of weight loss among obese persons. Am J Public Health. 1999, 89 (10): 1536-1542.
Frank E, Wright EH, Serdula MK, et al: Personal and professional nutrition-related practices of US female physicians. Am J Clin Nutr. 2002, 75 (2): 326-332.
Hiddink GJ, Hautvast JG, van Woerkum CM, et al: Nutrition guidance by primary-care physicians: perceived barriers and low involvement. Eur J Clin Nutr. 1995, 49 (11): 842-851.
Scott JG, Cohen D, DiCicco-Bloom B, et al: Speaking of weight: how patients and primary care clinicians initiate weight loss counseling. Prev Med. 2004, 8 (6): 819-827. 10.1016/j.ypmed.2004.01.001.
Kizer KW: The new VA: a national laboratory for healthcare quality improvement. Am J Med Qual. 2000, 14: 3-20.
Kizer KW, Pane GA: The "new VA": Delivering healthcare value through integrated service networks. Ann Emerg Med. 1997, 30: 804-7. 10.1016/S0196-0644(97)70053-2.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2296/7/35/prepub
Acknowledgements
The research reported here was supported by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development Service (grant MRP 04-220-1). Dr. Hoffman is a Career Development Awardee and Core Investigator in the Center for Research in the Implementation of Innovative Strategies in Practice (CRIISP) at the VA Iowa City Health Care System.
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
We would like to thank Dawn Howell from the Iowa City VAMC, Ananda Reddy from the Bettendorf CBOC, and Chief Internal Medicine Residents Chris Dyer, Greg Davis, and Stacy Sattovia for help with organizing the focus groups and encouraging survey completion by study participants.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
VFH designed the study, performed the statistical analyses, and drafted the manuscript. AL assisted with the focus groups and study coordination, helped performed the literature search, and helped with manuscript drafting. TW assisted with the conceptualization of the study design, as well as reviewing and revising manuscript drafts.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Forman-Hoffman, V., Little, A. & Wahls, T. Barriers to obesity management: a pilot study of primary care clinicians. BMC Fam Pract 7, 35 (2006). https://doi.org/10.1186/1471-2296-7-35
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2296-7-35