
Abstract
Background
Vitrification procedures decrease intracytoplasmic lipid content and impair developmental competence. Adding fatty acids (FAs) to the warming solution has been shown to recover the lipid content of the cytoplasm and improve developmental competence and pregnancy outcomes. However, the influence of the FA supplementation on live birth rates after embryo transfers and perinatal outcomes remains unknown. In the present study, we examined the influence of FA-supplemented warming solutions on live birth rates, pregnancy complications, and neonatal outcomes after single vitrified-warmed cleavage-stage embryo transfers (SVCTs).
Methods
The clinical records of 701 treatment cycles in 701 women who underwent SVCTs were retrospectively analyzed. Vitrified embryos were warmed using solutions (from April 2022 to June 2022, control group) or FA-supplemented solutions (from July 2022 to September 2022, FA group). The live birth rate, pregnancy complications, and perinatal outcomes were compared between the control and FA groups.
Results
The live birth rate per transfer was significantly higher in the FA group than in the control group. Multivariate logistic regression analysis further demonstrated a higher probability of live births in the FA group than in the control group. Miscarriage rates, the incidence and types of pregnancy complications, the cesarean section rate, gestational age, incidence of preterm delivery, birth length and weight, incidence of low birth weight, infant sex, and incidence of birth defects were all comparable between the control and FA groups. Multivariate logistic regression analysis further demonstrated no adverse effects of FA-supplemented warming solutions.
Conclusions
FA-supplemented warming solutions improved live birth rates after SVCTs without exerting any adverse effects on maternal and obstetric outcomes. Therefore, FA-supplemented solutions can be considered safe and effective for improving clinical outcomes and reducing patient burden.
Similar content being viewed by others


Background
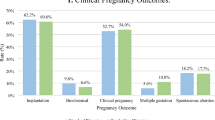
The cycle number of frozen embryo transfers (FETs) has recently increased owing to improvements in vitrification techniques and increased application of the freeze-all strategy [1,2,3]. However, previous studies have indicated adverse effects of vitrification on subsequent development after warming [4,5,6]. The altered characteristics of cytoplasmic organelles and increased abnormalities in chromosomal segregation reduce the developmental competence of vitrified-warmed oocytes and embryos [7,8,9]. Furthermore, our recent study revealed that vitrification procedures decrease intracytoplasmic lipid droplets and impair developmental competence [10]. However, lipid droplets in the cytoplasm could be recovered and developmental competence was improved by the addition of long-chain fatty acids (FAs) to the warming solutions (Supplementary Table 1). Moreover, we demonstrated that the rates of implantation, clinical pregnancy, and ongoing pregnancy after single vitrified-warmed cleavage-stage embryo transfer (SVCT) significantly increased after warming with FA-supplemented solutions. However, whether FA supplementation improves live birth rates following SVCTs is currently unknown. In addition, previous studies have indicated that pregnancies resulting from in vitro fertilization are associated with a higher risk of adverse maternal and perinatal outcomes such as hypertensive disorders of pregnancy, low birth weight, small for gestational age (SGA) and large for gestational age (LGA), preeclampsia, and placental anomalies [11,12,13,14,15]. Therefore, one future focus in reproductive medicine should be to assess whether assisted reproduction technology (ART) is associated with increased risks of these complications. From this perspective, the effectiveness and safety of FA-supplemented solutions should be evaluated. Accordingly, in the present study, we retrospectively analyzed the live birth rates, maternal outcomes, and perinatal outcomes after the transfer of cleavage-stage embryos warmed with FA-supplemented solutions.
Methods
Ethical approval
This retrospective cohort study was approved by the Institutional Review Board of our center (approval number: 21–12). Written informed consent for the retrospective use of data was obtained from all patients.
Study patients
The clinical records of 730 treatment cycles in 730 women who underwent SVCTs in natural cycles between April 2022 and September 2022 were reviewed. Patients with recurrent implantation failure (four or more unsuccessful FETs [16], n = 25), those who underwent procedures involving artificial oocyte activation (n = 3), and those with surgically retrieved sperm (n = 1) were excluded. Each case in this study involved only one cycle per patient.
Embryo warming
From April 2022 to June 2022, vitrified embryos were warmed using solutions that were not supplemented with FAs (VT506; Kitazato Corporation, Shizuoka, Japan; control group). From July 2022 to September 2022, vitrified embryos were warmed in FA-supplemented solutions (VT526; Kitazato Corporation, FA group; Supplementary Table 1). The warming procedures were performed using the Cryotop method [10, 17]. Briefly, the Cryotop was placed in a solution of 1.0 M sucrose at 37 °C for 1 min. The blastocysts were then removed after warming and transferred to a diluent sucrose solution (0.5 M) at 26–28 °C. After 3 min, the cells were transferred to a washing solution without sucrose and washed for 1 min.
Embryo transfer
SVCT was performed under vaginal ultrasound guidance using a specially designed soft silicone inner catheter (Kitazato Corporation), as previously described [18]. A single embryo was placed in a minimal volume in the upper part of the uterine cavity on day 2 after ovulation in a natural cycle. Dydrogesterone (30 mg/day; Mylan EPD G.K.) was orally administered during the early luteal phase after SVCT.
Live birth was defined as delivery at ≥ 22 weeks of gestation. Miscarriage was defined as the absence of live birth after confirmation of a gestational sac [19]. Maternal and obstetric outcomes were obtained from a self-reported questionnaire completed by each patient after the infant’s 1-month examination. All pregnant women were invited to respond to the questionnaire at 9 weeks of gestation, in the second trimester, and after delivery [20]. Maternal and obstetric outcomes included hypertensive disorders of pregnancy, gestational diabetes mellitus, hemolysis-elevated liver enzymes, low platelet count syndrome, low-lying placenta, placenta previa, placental abruption, and cesarean section. A low-lying placenta was determined in cases where the edge of the placenta was < 20 mm from the cervix, but not overlying it. When the placenta completely covered the cervix, it was classified as placenta previa [21]. Neonatal outcomes included gestational age, birth length and weight, SGA, and LGA. SGA and LGA were defined as birth weights below the 10th percentile and above the 90th percentile, respectively, according to the Japanese National Reference for neonates [22]. Congenital anomalies were classified using the Q codes of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, by reformatting the answers provided by parents in the questionnaires [23]. Major congenital anomalies were classified according to the European Surveillance of Congenital Anomalies guidelines [24].
Statistical analysis
Statistical analyses were performed using JMP software (SAS, Cary, NC, USA). Data proportions were analyzed using the chi-square and Fisher’s exact tests. Continuous parameters were compared using the Mann–Whitney U test. Univariate regression analysis was used to identify potential confounders associated with the outcomes. The likelihood ratio test for the significance of the regression coefficient was used, and variables with P < 0.10 were designated as confounders (Supplementary Table 2). Multivariate logistic regression analysis was performed to adjust for bias and to verify statistical significance. Adjusted odds ratios are reported with 95% confidence intervals for each group. P < 0.05 was considered significant.
Results
Live births after SVCTs
The patient and cycle characteristics were comparable between the control and FA groups (Table 1). The delivery rate was significantly higher in the FA group than in the control group (Table 2). As the live birth rate per delivery was 100% in both groups, the live birth rate per transfer was significantly higher in the FA group than in the control group. Miscarriage rates were comparable between the two groups. Multivariate logistic regression analysis also demonstrated a higher probability of live births in the FA group than in the control group (Table 3).
Patients were stratified by median maternal age for further analysis (37 years; Supplementary Table 3). This subgroup analysis showed that the live birth rate per transfer was significantly higher in the FA group than in the control group in women younger than 37 years of age. Multivariate logistic regression analysis also demonstrated a higher probability of live births in the FA group than in the control group in the young cohort. However, the live birth rate per transfer was comparable between the two groups for women aged 37 years or older. The incidence of miscarriage was comparable between the groups in both the young and advanced-age cohorts.
Maternal and obstetric outcomes after SVCTs
The incidence and types of pregnancy complications were comparable between the control and FA groups (Table 4). Furthermore, cesarean section rates were similar between the groups (Table 4). The average gestational age and incidence of preterm delivery were comparable between the groups. Birth length and weight, incidence of low birth weight, incidence of SGA and LGA, and infant sex were comparable between the groups. The incidence of birth defects was also similar between the groups. Multivariate logistic regression analysis revealed a similar trend (Table 5).
Discussion
To the best of our knowledge, this is the first report to show a significant improvement in live birth rates after the transfer of cleavage-stage embryos warmed with FA-supplemented solutions. Furthermore, we confirmed that these solutions had no adverse effects on maternal or obstetric outcomes.
In the present study, we first examined the effects of FA-supplemented warming solutions on live birth rates after SVCTs. The live birth rate per transfer was significantly higher in the FA group than in the control group. This result validates our previous finding that FA-supplemented solutions improved the ongoing pregnancy rate [17]. Furthermore, the miscarriage rate was unchanged when FA-supplemented solutions were used. The enzyme-mediated β-oxidation of FAs is a crucial metabolic process in mitochondria and is essential for early embryo development [25, 26]. Through β-oxidation, FAs are catabolized to acetyl-CoA, which leads to adenosine triphosphate (ATP) production via the mitochondrial electron transport chain [26,27,28]. Furthermore, the FA-supplemented solutions stimulate the blastocyst formation rate and improve embryo quality [10, 17], suggesting that β-oxidation-induced developmental improvements would lead to an increased chance to achieve live birth after warming of cleavage stage embryos with FA-supplemented solutions. Furthermore, we performed a subgroup analysis in which patients were stratified according to the median maternal age. The probability of live births significantly improved using FA-supplemented solutions only when the patients were young (< 37 years of age). A recent study indicated that mitochondrial function in embryos declines as maternal age increases [29]. Therefore, we speculated that even if the embryos from the advanced age patients possess sufficient metabolic substances, such as FAs, they could not produce sufficient ATP through β-oxidation. Further molecular studies are required to compare the activity of β-oxidation after warming with the FA-supplemented solutions between young females and those of advanced age.
Our data also demonstrate that the incidence of pregnancy-related complications was not affected by the FA-supplemented solutions. Furthermore, the perinatal outcomes, including infant health, were comparable between the control and FA groups. Previous studies have reported that vitrification increases the risk of pregnancy-related complications [11, 12]. However, most FETs in these studies were performed during hormone replacement cycles. In a previous study, we found that endometrial preparation during the hormone replacement cycle, rather than vitrification procedures, adversely affected pregnancy complications compared to endometrial preparation during the natural cycle [30]. The FA-supplemented solutions did not have adverse effects on maternal or obstetric outcomes. Therefore, we determined the efficacy and safety of the solutions in the present study.
One strength of this study is that we examined maternal and obstetric data obtained from a single center, and the culture conditions and SVCT procedures were uniform. Moreover, we included the characteristics of patients, cycles, and embryos as confounders that were significantly associated with the live birth rate and incidence of adverse maternal and perinatal outcomes after SVCTs in multivariate logistic regression analysis. Naturally, this study had certain limitations. For example, the single-center retrospective design limits the strength of the study, necessitating further multicenter studies to ascertain the generalizability of these findings to other clinics with different protocols and/or patient demographics. Lipid droplets are regulated at the homeostatic level to participate in cellular membrane formation, and they play a versatile role as an energy source [31,32,33]. The lipid droplets in early cleavage-stage embryos are small and are dispersed throughout the cytoplasm or may be partially clustered, whereas larger lipid droplets are formed after compaction, which allows for increased contact area with other organelles, such as mitochondria, thereby facilitating lipid exchange, replenishment, and FA β-oxidation [32, 34]. Furthermore, it has been recently reported that the biosynthesis of unsaturated FAs is activated at the blastocyst stage in mice and humans, and this activation is necessary for the formation of the apical and basal domains to establish polarity toward blastocyst development [31, 35]. This suggests that the detrimental effects of vitrification on intracellular lipid droplets vary by developmental stage. Further molecular studies, such as a lipidome analysis, are required to reveal which FAs decrease after vitrification at each stage. Although the effectiveness of FA-supplemented warming solutions for frozen blastocyst transfers remains unclear, it is hypothesized that warming of blastocysts using FA-supplemented solutions may positively affect blastocyst viability and competence for implantation since the FA-supplemented solutions contain several unsaturated FAs, such as oleic acid, that are believed to improve embryo membrane fluidity and subsequent development [35]. To test this hypothesis, further experimental and clinical studies are required. Another limitation of our study is that the number of perinatal cycles was low. Therefore, larger cohort studies are required to substantiate our findings. Finally, although the same protocols were used for ovarian stimulation, oocyte retrieval, embryo culture, and embryo transfer, the control and FA group data were collected at different time periods.
Conclusion
The FA-supplemented warming solutions improved the live birth rates after SVCTs, particularly in young patients. Furthermore, infant health and the incidence of pregnancy complications were not affected by the FA-supplemented solutions. As such, FA-supplemented solutions can be considered safe and effective at improving clinical outcomes and reducing patient burden.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Katagiri Y, Jwa SC, Kuwahara A, Iwasa T, Ono M, Kato K, et al. Assisted reproductive technology in Japan: a summary report for 2020 by the ethics Committee of the Japan Society of obstetrics and gynecology. Reprod Med Biol. 2023;22:e12494.
De Geyter C, Wyns C, Calhaz-Jorge C, de Mouzon J, Ferraretti AP, Kupka M, et al. 20 years of the European IVF-monitoring Consortium registry: what have we learned? A comparison with registries from two other regions. Hum Reprod. 2020;35:2832–49.
European IVFMCftESoHR, Embryology, Smeenk J, Wyns C, De Geyter C, Kupka M et al. ART in Europe, 2019: results generated from European registries by ESHREdagger. Hum Reprod. 2023.
Bang S, Shin H, Song H, Suh CS, Lim HJ. Autophagic activation in vitrified-warmed mouse oocytes. Reproduction. 2014;148:11–9.
Oktay K, Cil AP, Bang H. Efficiency of oocyte cryopreservation: a meta-analysis. Fertil Steril. 2006;86:70–80.
Zander-Fox D, Cashman KS, Lane M. The presence of 1 mM glycine in vitrification solutions protects oocyte mitochondrial homeostasis and improves blastocyst development. J Assist Reprod Genet. 2013;30:107–16.
Ducibella T, Fissore R. The roles of Ca2+, downstream protein kinases, and oscillatory signaling in regulating fertilization and the activation of development. Dev Biol. 2008;315:257–79.
Larman MG, Sheehan CB, Gardner DK. Calcium-free vitrification reduces cryoprotectant-induced zona pellucida hardening and increases fertilization rates in mouse oocytes. Reproduction. 2006;131:53–61.
Tamura AN, Huang TT, Marikawa Y. Impact of vitrification on the meiotic spindle and components of the microtubule-organizing center in mouse mature oocytes. Biol Reprod. 2013;89:112.
Ohata K, Ezoe K, Miki T, Kouraba S, Fujiwara N, Yabuuchi A, et al. Effects of fatty acid supplementation during vitrification and warming on the developmental competence of mouse, bovine and human oocytes and embryos. Reprod Biomed Online. 2021;43:14–25.
Maheshwari A, Pandey S, Amalraj Raja E, Shetty A, Hamilton M, Bhattacharya S. Is frozen embryo transfer better for mothers and babies? Can cumulative meta-analysis provide a definitive answer? Hum Reprod Update. 2018;24:35–58.
Ishihara O, Araki R, Kuwahara A, Itakura A, Saito H, Adamson GD. Impact of frozen-thawed single-blastocyst transfer on maternal and neonatal outcome: an analysis of 277,042 single-embryo transfer cycles from 2008 to 2010 in Japan. Fertil Steril. 2014;101:128–33.
Qin JB, Sheng XQ, Wu D, Gao SY, You YP, Yang TB, et al. Worldwide prevalence of adverse pregnancy outcomes among singleton pregnancies after in vitro fertilization/intracytoplasmic sperm injection: a systematic review and meta-analysis. Arch Gynecol Obstet. 2017;295:285–301.
Romundstad LB, Romundstad PR, Sunde A, von During V, Skjaerven R, Vatten LJ. Increased risk of placenta previa in pregnancies following IVF/ICSI; a comparison of ART and non-ART pregnancies in the same mother. Hum Reprod. 2006;21:2353–8.
Vermey BG, Buchanan A, Chambers GM, Kolibianakis EM, Bosdou J, Chapman MG, et al. Are singleton pregnancies after assisted reproduction technology (ART) associated with a higher risk of placental anomalies compared with non-ART singleton pregnancies? A systematic review and meta-analysis. BJOG. 2019;126:209–18.
Coughlan C, Ledger W, Wang Q, Liu F, Demirol A, Gurgan T, et al. Recurrent implantation failure: definition and management. Reprod Biomed Online. 2014;28:14–38.
Amagai A, Ezoe K, Miki T, Shimazaki K, Okimura T, Kato K. Fatty acid supplementation into warming solutions improves pregnancy outcomes after single vitrified-warmed cleavage stage embryo transfers. Reprod Med Biol. 2023;22:e12517.
Onogi S, Ezoe K, Kawasaki N, Hayashi H, Kuroda T, Takeshima K, et al. Maternal and obstetric outcomes are influenced by developmental stage and cryopreservation of transferred embryos after clomiphene citrate-based minimal stimulation IVF. Hum Reprod Open. 2022;2022:hoac018.
Ezoe K, Fukuda J, Takeshima K, Shinohara K, Kato K. Letrozole-induced endometrial preparation improved the pregnancy outcomes after frozen blastocyst transfer compared to the natural cycle: a retrospective cohort study. BMC Pregnancy Childbirth. 2022;22:824.
Takeshima K, Ezoe K, Kawasaki N, Hayashi H, Kuroda T, Kato K. Perinatal outcomes and congenital anomalies associated with letrozole and natural cycles in single fresh cleaved embryo transfers: a single-center, 10-year cohort study. F S Rep. 2022;3:138–44.
Jansen C, Kleinrouweler CE, Kastelein AW, Ruiter L, van Leeuwen E, Mol BW, et al. Follow-up ultrasound in second-trimester low-positioned anterior and posterior placentae: prospective cohort study. Ultrasound Obstet Gynecol. 2020;56:725–31.
Itabashi K, Fujimura M, Kusuda S, Tamura M, Hayashi T, Takahashi T et al. New standard of average size and weight of newborn in Japan. Jap J Pediat 114:1271–93.
World Health Organization. Internatilnal Stastical Classification of Diseases and Related Health Problems 10th Revison. 2016. https://apps.who.int/iris/handle/10665/246208. Accessed September 20 2021.
EUROCAT. EUROCAT Guide 1.5: EUROCAT Subgroups of Congenital Anomalies In: EUROCAT Central Registry. EUROCAT Central Registry. 2022. https://eu-rd-platform.jrc.ec.europa.eu/system/files/public/eurocat/Guide_1.5_Chapter_3.3_June_2022.pdf.
Van Blerkom J. Mitochondria in human oogenesis and preimplantation embryogenesis: engines of metabolism, ionic regulation and developmental competence. Reproduction. 2004;128:269–80.
Dunning KR, Cashman K, Russell DL, Thompson JG, Norman RJ, Robker RL. Beta-oxidation is essential for mouse oocyte developmental competence and early embryo development. Biol Reprod. 2010;83:909–18.
Houten SM, Wanders RJ. A general introduction to the biochemistry of mitochondrial fatty acid beta-oxidation. J Inherit Metab Dis. 2010;33:469–77.
Wanders RJ. Peroxisomes, lipid metabolism, and peroxisomal disorders. Mol Genet Metab. 2004;83:16–27.
Hashimoto S, Morimoto Y. Mitochondrial function of human embryo: decline in their quality with maternal aging. Reprod Med Biol. 2022;21:e12491.
Takeshima K, Ezoe K, Onogi S, Kawasaki N, Hayashi H, Kuroda T, et al. Endometrial preparation and maternal and obstetrical outcomes after frozen blastocyst transfer. AJOG Glob Rep. 2022;2:100081.
Ibayashi M, Tsukamoto S. Lipid remodelling in mammalian development. Nat Cell Biol. 2024.
Aizawa R, Ibayashi M, Tatsumi T, Yamamoto A, Kokubo T, Miyasaka N et al. Synthesis and maintenance of lipid droplets are essential for mouse preimplantation embryonic development. Development. 2019;146.
Ibayashi M, Aizawa R, Mitsui J, Tsukamoto S. Homeostatic regulation of lipid droplet content in mammalian oocytes and embryos. Reproduction. 2021;162:R99–109.
Talari NK, Mattam U, Meher NK, Paripati AK, Mahadev K, Krishnamoorthy T, et al. Lipid-droplet associated mitochondria promote fatty-acid oxidation through a distinct bioenergetic pattern in male Wistar rats. Nat Commun. 2023;14:766.
Zhang L, Zhao J, Lam SM, Chen L, Gao Y, Wang W et al. Low-input lipidomics reveals lipid metabolism remodelling during early mammalian embryo development. Nat Cell Biol. 2024.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KE contributed to study design, data collection, interpretation, writing, and revision. SO, AS, and AA contributed to data collection. KK contributed to interpretation, writing, and revision. All the authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This retrospective cohort study was approved by the Institutional Review Board of Kato Ladies Clinic (approval number: 21 − 12). This study was conducted in accordance with the principles embodied in the Declaration of Helsinki. Written informed consent for analysis was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ezoe, K., Onogi, S., Sawado, A. et al. Maternal and obstetric outcomes following the transfer of embryos warmed with fatty acid-supplemented solutions. BMC Pregnancy Childbirth 24, 343 (2024). https://doi.org/10.1186/s12884-024-06546-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-024-06546-4