
Abstract
Background
Stress hyperglycemia is a common condition in patients suffering from critical illness such as spontaneous intracerebral hemorrhage (ICH). Our study aimed to use glucose-to-glycated hemoglobin (HbA1c) ratio to investigate the impact of stress hyperglycemia on clinical outcomes in patients with ICH.
Methods
A sample of eligible 586 patients with spontaneous intracerebral hemorrhage from a multicenter, hospital-based cohort between 2014 and 2016 were recruited in our study. Stress hyperglycemia was evaluated by the index of the glucose-to-HbA1c ratio that was calculated by fasting blood glucose (mmol/L) divided by HbA1c (%). Patients were divided into two groups based on the median of the glucose-to-HbA1c ratio. The main outcomes were poor functional outcomes (modified Rankin Scale score of 3–6) at discharge and 90 days. Multivariable logistic regression and stratified analyses were performed to explore the association of stress hyperglycemia with poor prognosis of ICH.
Results
On multivariable analysis, higher glucose-to-HbA1c ratio (≥1.02) was independently correlated with poor functional outcomes at discharge (adjusted OR = 3.52, 95%CI: 1.98–6.23) and 90 days (adjusted OR = 2.27, 95%CI: 1.38–3.73) after adjusting for potential confounding factors. The correlation between glucose-to-HbA1c ratio and worse functional outcomes still retained in patients with or without diabetes mellitus.
Conclusions
Stress hyperglycemia, calculated by glucose-to-HbA1c ratio, was independently correlated with worse functional outcomes at discharge and 90 days in patients with ICH. Moreover, glucose-to-HbA1c ratio, might not only be used as a simple and readily available index to predict clinical outcomes of ICH but also provide meaningful insight into future analysis to investigate the optimal range of glucose levels among ICH patients and develop tailored glucose-lowering strategies.
Similar content being viewed by others

Background
Intracerebral hemorrhage remains the second leading cause of stroke [1,2,3], leading to a higher mortality rate and severe neurological deficits [4, 5]. Considering that there are limited treatment options for ICH patients [4, 6], early detection and management of the risk factors for adverse consequences is extremely essential to optimize outcomes.
Stress hyperglycemia refers to the relative transient condition of elevated blood glucose levels, which is commonly observed in critical illness such as myocardial infarction, ischemic stroke and intracerebral hemorrhage [7,8,9]. Several previous studies have indicated that stress hyperglycemia was related to elevated risk of death and poor functional outcomes following ICH although these trends have not been described consistently [7, 10,11,12,13,14]. In addition, in most previous studies, stress hyperglycemia was usually defined as absolute hyperglycemia based on the random or fasting blood glucose levels without excluding the effect of chronically background hyperglycemia [7, 8, 12]. Glycated hemoglobin (HbA1c) is a reliable measure of the mean levels of glucose concentration over 2–3 months before the onset of the acute illness [15, 16]. In recent studies, glucose-to-HbA1c ratio, which assessed the degree of the stress hyperglycemia with consideration of the background glucose concentration has gained its popularity and has shown a better predictive value for outcomes of critical illness than absolute hyperglycemia [9, 17]. Moreover, this novel parameter is associated with unfavorable clinical outcomes in patients with ischemic stroke [18,19,20,21,22,23]. However, the effect of stress hyperglycemia on the poor prognosis of ICH with taking the background glucose levels into account has been rarely discussed in multi-center studies with relatively large sample size and consecutive information of functional outcomes.
Therefore, in our study, we aimed to investigate the association between stress hyperglycemia, which was calculated by glucose-to-HbA1c ratio, and clinical outcomes in patients with ICH.
Methods
Study design and population
The study was a prospective, multicenter, observational cohort study, conducted in 13 hospitals in Beijing from 2014 to 2016. In each participating center, clinical data was collected and submitted it online to the coordinating center at Beijing Tiantan Hospital, Capital Medical University for further analysis. The study was performed in accordance with the ethical guidelines from the Helsinki Declaration and was approved by the Institutional Review Board (IRB) of Beijing Tiantan Hospital, Capital Medical University. All the patients or their legal proxies signed the written informed consent.
The inclusion criteria were 1) ICH was diagnosed based on WHO standard and confirmed by CT scan, 2) first-ever acute-onset ICH, 3) age of 18 years or older and 4) arriving at hospital within 72 h after symptom onset.
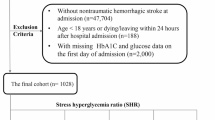
The exclusion criteria were patients complicated with major comorbidities or late-stage diseases. A total of 1964 ICH patients were screened. The additional exclusion criteria of our analysis were as follows: 1) patients with secondary ICH, which attribute to trauma, aneurysms, cerebral venous thrombosis, cerebrovascular malformations, tumor or hemorrhagic transformation of ischemic stroke, 2) patients with primary ventricular hemorrhage, 3) patients without the fasting blood glucose and HbA1c recording and 4) patients without the follow-up information. Finally, 586 patients were included in this study (Fig. 1).

Flow diagram of study patients. ICH: intracerebral hemorrhage; FBG: fasting blood glucose; HbA1c: Glycated hemoglobin
Baseline information
Baseline information including demographics (age and sex), medical history (hypertension, diabetes mellitus, dyslipidemia and cerebral infarction) and health habits (smoking and alcohol consumption) were documented using standard questionnaires by trained research coordinators. Hypertension was defined as a self-reported history, receiving any antihypertensive treatment or a systolic blood pressure ≥ 140 mmHg, or diastolic blood pressure ≥ 90 mmHg at baseline. Dyslipidemia was noted as a self-reported history, taking lipid-lowering medicine, or a total cholesterol level ≥ 6.22 mmol/L or low-density lipoprotein ≥4.14 mmol/L or triglyceride ≥2.26 mmol/L at baseline. Diabetes mellitus was diagnosed when a patient had a prior history of diabetes or a HbA1c level of ≥6.5% [24]. Smoking was noted when a patient smoked at least one cigarette per day for over a year. Alcohol consumption was documented as an intake of at least 80 g of liquor 1 day for over a year. Prior use of antidiabetic agents and treatment of hyperglycemia during hospitalization were also collected. In this study, anti-hyperglycemic therapy was determined by our stroke physicians based on the patient’s blood glucose levels and general clinical condition and we do not have a standard prescribing routine for blood glucose management during hospitalization.
Stroke severity was assessed using the Glasgow Coma Scale (GCS) and the National Institutes of Health Stroke Scale (NIHSS) by physicians at the timing of arriving at hospital. On the initial CT scan, which was performed within 24 hours after admission, we documented the hematoma volume (ABC/2 method) [25] and location (lobar, basal ganglia, thalamus,,cerebellum brainstem).
Laboratory examinations and assessment of stress hyperglycemia
Fasting blood glucose was measured the next morning after an overnight fast for at least 8 hours. HbA1c was measured during the first 7 days of acute hospitalization. Other laboratory examinations, including triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and high- sensitivity C-reactive protein (Hs-CRP) were also evaluated during admission. Estimated glomerular filtration rate (eGFR) was calculated based on the Chronic Kidney Disease Epidemiology Collaboration creatinine equation with an adjusted coefficient of 1.1 for the Asian population [26].
Stress hyperglycemia was evaluated by the index of the glucose-to-HbA1c ratio that was calculated by fasting blood glucose (mmol/L) divided by HbA1c (%) [17]. The reasons for using fasting blood glucose as numerator instead of admission random blood glucose were its better predictive value on stroke outcomes [27,28,29,30,31] and almost unaffected by food or other sugary infusion [27, 32] as well as its little variation between individuals [27]. The patients were then categorized into 2 groups according to the median of the glucose-to-HbA1c ratio for further comparisons. The index, which takes the baseline blood glucose levels into consideration, quantifies the extent of stress hyperglycemia.
Follow-up information and clinical outcome
All the patients were followed up by face-to-face interviews at discharge and by telephone interviews at 90-day after ICH onset. Trained research personals, who were blinded to patients’ clinical information, followed the interview protocol to assess the scores of mRS according to the functional status reported by the patients or their relatives or caregivers at each follow-up. An unfavorable clinical outcome was defined as a score of 3 to 6 on mRS.
Statistics analysis
Categorical variables were expressed as numbers (proportions), while continuous variables were described as means ± standard deviation (SD) or medians (interquartile range, IQR) as appropriate. Continuous variables that were normally distributed were compared using Student t-tests while if were not distributed normally, Wilcoxon rank-sum tests were applied. For categorical variables, chi-squared tests were used to perform comparisons. Multivariate logistic regression model was performed to calculate the odds ratios (OR) and 95% confidence intervals (CI) for the relationship between glucose-to-HbA1c ratio and poor clinical outcomes. Potential confounders with p-value<0.2 in comparisons of baseline characteristics grouped by glucose-to-HbA1c ratio were included in multivariate analysis. Confounders that were known to be correlated with poor clinical outcomes after ICH were also entered into our multivariate model. These variables included age, gender, current smoking, alcohol consumption, hypertension, diabetes mellitus, dyslipidemia, history of cerebral infarction, prior antidiabetic agents, systolic blood pressure, GCS score, NIHSS score, location of hematoma, hematoma volume, hsCRP, eGFR, post-stroke treatment of hyperglycemia, surgical treatment and intraventricular extension. Moreover, stratified analysis was conducted according to the diagnosis of diabetes mellitus. Receiver operating characteristic (ROC) curves and area under the curves (AUC) were used to evaluate the predictive power of glucose-to-HbA1c ratio for unfavorable clinical outcomes. All statistical analyses were conducted by SAS software (version 9.4; SAS Institute, Cary, North Carolina, USA). A two-sided P < 0.05 was considered to be statistically significant.
Results
A total of 586 patients were finally recruited in the present study. The mean age was 58.5 years old, among which 412 (70.3%) patients were male. As the median of the glucose-to-HbA1c ratio was 1.02, patients were classified into a higher glucose-to-HbA1c ratio group and a lower glucose-to- HbA1c ratio group and their baseline characteristics were presented in Table 1. Patients in the higher glucose-to-HbA1c ratio group were significantly older, had higher proportion of diabetes mellitus, and had higher systolic blood pressure, lower GCS score as well as higher NIHSS score. Initial hematoma volume in the higher glucose-to-HbA1c ratio group was larger and was more prone to break into ventricle. Additionally, patients with elevated glucose-to-HbA1c ratio had higher level of FBG and were more likely to receive treatment of hyperglycemia and surgical intervention. For the poor functional outcome, the proportions of disability or death decreased from discharge to 90-day follow-up in both groups, but remained higher in patients with elevated glucose-to-HbA1c ratio (65.5% vs 34.1% at discharge and 58.4% vs 29.0% at 90-day respectively, all p < 0.001) (Table 1, Fig. 2). The baseline characteristics between included and excluded participants in the present study were shown in Additional file 2. Excluded patients were younger, less likely to smoke or drink and had lower proportions of hypertension, diabetes mellitus, dyslipidemia, history of cerebral infarction, prior antidiabetic agents and post-stroke treatment of hyperglycemia. We also found that patients in the excluded group had lower GCS scores, higher NIHSS scores, larger hematoma volume, more often intraventricular extension and tend to receive surgical treatment.

Distribution of scores on mRS at discharge and 90 days in different glucose-to-HbA1c ratio groups. mRS: modified Rankin Scale; HbA1c: Glycated hemoglobin
On multivariable analysis, higher glucose-to-HbA1c ratio (≥1.02) remained to be independently correlated with poor functional outcomes at discharge (OR 3.52 95%CI 1.98–6.23) and 90 days (OR 2.27 95%CI 1.38–3.73) after adjusting for potential confounding factors (Table 2).
Subgroup analysis revealed that diabetes mellitus had no interaction effect on the relationship between glucose-to-HbA1c ratio and unfavorable clinical outcomes in patients with ICH (p for interaction>0.05), although some OR values were significant in some subgroups (Table 3).
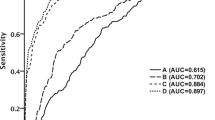
Furthermore, the ROC curve analysis demonstrated that glucose-to-HbA1c ratio produced greater AUC values (0.689, 95% CI: 0.646–0.732) than did FBG (AUROC: 0.653, 95% CI: 0.608–0.698, P = 0.01) and HbA1c (AUROC: 0.517, 95% CI: 0.471–0.564, P<0.0001) for predicting poor clinical outcomes at discharge in pairwise comparison (Fig. 3). In terms of poor clinical outcomes at 90 days, similar results were observed for the superior predictive value of glucose-to-HbA1c ratio (0.699, 95% CI: 0.656–0.742) than did FBG (AUROC: 0.671, 95% CI: 0.627–0.715, P = 0.04) and HbA1c (AUROC: 0.475, 95% CI: 0.429–0.522, P<0.0001) (Fig. 4).

The ROC analysis of glucose-to-HbA1c ratio, FBG and HbA1c levels for predicting poor outcomes at discharge. ROC: receiver operating characteristic; AUC: area under the curve; FBG: fasting blood glucose; HbA1c: Glycated hemoglobin

The ROC analysis of glucose-to-HbA1c ratio, FBG and HbA1c levels for predicting poor outcomes at 90-day. ROC: receiver operating characteristic; AUC: area under the curve; FBG: fasting blood glucose; HbA1c: Glycated hemoglobin
Discussion
In this prospective, observational cohort study conducted in Beijing, we discovered that stress hyperglycemia represented by glucose-to-HbA1c ratio was independently associated with poor clinical outcomes at discharge and 90 days in patients with ICH. The correlation still retained irrespective of diabetes mellitus. In addition, our data also implicated that glucose-to-HbA1c ratio had greater discriminative power compared to FBG and HbA1c in predicting poor functional outcomes of ICH.
There were conflicting results regarding the relationship between stress hyperglycemia and poor clinical outcomes in patients with ICH. Prior studies have found that stress hyperglycemia was correlated with increased risk of early mortality and long-term death in patients with ICH [14, 33,34,35]. Other studies also demonstrated that hyperglycemia was a surrogate marker to predict poor functional outcome at discharge and 90 days after ICH [12, 36,37,38]. However, some research did not indicate a significant association between hyperglycemia and poor prognosis in patients with ICH [10, 11]. A meta-analysis also shown that stress hyperglycemia did not appear to be independently related to short-term mortality after hemorrhagic stroke [7]. The discrepancies between different studies may be contribute to the study population, confounding factors adjusted in multivariate analysis as well as the definition of stress hyperglycemia. In most of the studies, stress hyperglycemia was usually measured as the absolute hyperglycemia without considering the previous diabetes status or deterioration of pre-illness blood glucose control with preexisting diabetes mellitus [7, 8]. Moreover, given that the absolute hyperglycemia failed to take the background hyperglycemia into account, it was difficult to differentiate stress hyperglycemia from newly diagnosed or previously unknown diabetes mellitus. In contrast, glucose-to-HbA1c ratio, a novel index we used to calculate the degree of stress hyperglycemia, represents a reliable assessment of relatively elevating blood glucose levels, hence can eliminate the influence of background hyperglycemia. Based on recent studies, relative measurements adjusting for prior glycemic status, such as glucose-to-HbA1c ratio or admission glucose level divided by estimated average blood glucose derived from HbA1c, could facilitate better prediction for poor outcomes of critical illness than absolute elevated glucose concentration [9, 17]. Also, HbA1c levels, reflecting the previous glycemic control over 2–3 months [15,16,17], are characterized by lower biological variability and remain stable even at the acute phase of diseases [39, 40], thus can accurately quantify the degree of stress hyperglycemia. Moreover, relative measurements to asses stress hyperglycemia were considered to be useful indicators of adverse cardiovascular and cerebrovascular events after percutaneous coronary intervention [41], and also elevated risk of poor functional outcomes, all-cause death and hemorrhagic transformation after acute ischemic stroke [18, 19, 42]. In the current study, we further elaborated that stress hyperglycemia, represented by glucose-to-HbA1c ratio could better predict the unfavorable functional outcomes in patents with ICH.
Although the mechanisms underlying the correlation between stress hyperglycemia and poor functional outcomes in patients with ICH are incompletely understood, several possible explanations may account for our findings. First of all, stress hyperglycemia reflects the relative rapid increase of blood glucose and is secondary to a status of neuroendocrine derangements and inflammatory response that occur after an acute major diseases like stroke [18, 19, 42]. Neuroendocrine derangements and inflammatory response are characterized by glycogenolysis, excessive output of glucose from hepatic storage and increasing insulin resistance [9, 21, 43]. Therefore, we can speculate that stress hyperglycemia may be an indicator of the extent of severe stroke, which contribute to poor prognosis after ICH occurs. However, it is interesting to notice that stress hyperglycemia remained significantly associated with poor functional outcomes in patients with ICH even after adjusting the NIHSS score and hematoma volume, further indicating that stress hyperglycemia represents not merely the severity of stroke or not just simply an epiphenomenon of stress response. Second, stress hyperglycemia might exert a direct toxic damage to the brain tissue by exacerbating the accumulation of lactate and intracellular acidosis [20, 23, 36]. And intracellular acidosis could further aggravate free radical formation and lipid peroxidation, which in turn may accelerate the process of nerve injuries [7, 23, 44]. Third, stress hyperglycemia could cause the acute rising of free calcium in the cytoplasm that results in calcium influx into mitochondria and then interferes with the process of ATP generation, leading to cytotoxic edema and neuronal apoptosis [45,46,47]. Fourth, the downregulation of aquaporin-4 expression in the brain induced by stress hyperglycemia can exacerbate the blood brain barrier destruction, which promotes severe vasogenic brain edema [12, 48], eventually leading to worse functional outcomes after ICH. In addition, stress hyperglycemia is responsible for aggravating hematoma enlargement via plasma kallikrein [13, 34, 49], further resulting in unfavorable outcomes when ICH occurs.
Previous studies found that stress hyperglycemia contributed to worse functional outcomes after ICH particularly in patients without diabetes mellitus [12, 35, 38]. This could be possibly explained by the better tolerance to hyperglycemia in diabetic patients because of the cellular adaptation to chronically exposure to high blood glucose levels [21, 22]. However, in our subgroup analysis, stress hyperglycemia, measured by glucose-to-HbA1c ratio did not have the effect on poor functional outcomes after ICH stratified by diabetes status. This discrepancy might due to the different definition of stress hyperglycemia. Our study, using the glucose-to-HbA1c ratio to calculate stress hyperglycemia rather than the absolute rising of blood glucose levels, have taken the background hyperglycemia into account, further implicating those diabetic patients could also have stress hyperglycemia.
There are several limitations in our study that should be considered. First of all, the cause-and-effect relationship between stress hyperglycemia and clinical outcomes was not verified due to the nature of the observational study. Therefore, further studies should be conducted to establish the causal link. Second, we enrolled patients within 72 hours after symptom onset and patients without the FBG or HbA1c recording or loss to follow-up were excluded. Considering that the mortality rate of ICH within the first 48 h may be as high as 14.9% [50] and the excluded patients had worse neurological status,lower levels of consciousness and larger hematoma volume, thus the present study rule out the most severe patients. Furthermore, participants included in our study were all come from Beijing, China. Therefore, selection bias might exist and our findings may not be generalizable to patients with more serious clinical conditions and wider racial diversity. Thirdly, the extent of hematoma expansion at the early stage was not measured in our study cohort, which may potentially influence the relationship between stress hyperglycemia and ICH outcomes. At the same time, moderate and severe persistent hyperglycemia could have an impact on disability or death after ICH [51]. However, the temporal profile of stress hyperglycemia assessed by glucose-to-HbA1c ratio was not documented, and the influence of severity and duration of stress hyperglycemia on prognosis of ICH was not explored further. Hence, the impact of the dynamic change of glucose-to-HbA1c ratio on ICH outcomes requires further investigation in our future analysis. Finally, some parameters, such as the glycemic variability and the glycemic control were not documented in our study, which could have the residual confounding effects on the functional outcomes.
Conclusions
In conclusion, our study indicated that stress hyperglycemia, calculated by glucose-to-HbA1c ratio was independently associated with worse functional outcomes at discharge and 90 days in patients with ICH. Moreover, glucose-to-HbA1c ratio, might not only be used as a simple and readily available index to predict clinical outcomes of ICH but also provide meaningful insight into future analysis to investigate the optimal range of glucose levels among ICH patients and develop tailored glucose-lowering strategies.
Availability of data and materials
All data generated or analyzed during this study are included in Additional file 1.
Abbreviations
- ICH:
-
Intracerebral hemorrhage
- HbA1c:
-
Glycated hemoglobin
- FBG:
-
Fasting blood glucose
- GCS:
-
Glasgow Coma Scale
- NIHSS:
-
National Institutes of Health Stroke Scale
- TG:
-
Triglyceride
- TC:
-
Total cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- Hs-CRP:
-
High- sensitivity C-reactive protein
- eGFR:
-
Estimated glomerular filtration rate
- mRS:
-
Modified Rankin Scale score
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curves
References
Feigin VL, Lawes CMM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8(4):355–69.
Wu S, Wu B, Liu M, Chen Z, Wang W, Anderson CS, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019;18(4):394–405.
van Asch CJJ, Luitse MJA, Rinkel GJE, van der Tweel I, Algra A, Klijn CJM. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–76.
Hemphill JC 3rd, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(7):2032–60.
Keep RF, Hua Y, Xi G. Intracerebral haemorrhage: mechanisms of injury and therapeutic targets. Lancet Neurol. 2012;11(8):720–31.
Steiner T, Al-Shahi Salman R, Beer R, Christensen H, Cordonnier C, Csiba L, et al. European stroke organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. 2014;9(7):840–55.
Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients - a systematic overview. Stroke. 2001;32(10):2426–32.
Dungan KM, Braithwaite SS, Preiser JC. Stress hyperglycaemia. Lancet. 2009;373(9677):1798–807.
Roberts GW, Quinn SJ, Valentine N, Alhawassi T, O'Dea H, Stranks SN, et al. Relative hyperglycemia, a marker of critical illness: introducing the stress hyperglycemia ratio. J Clin Endocrinol Metab. 2015;100(12):4490–7.
Zhao Y, Yang J, Zhao H, Ding Y, Zhou J, Zhang Y. The association between hyperglycemia and the prognosis of acute spontaneous intracerebral hemorrhage. Neurol Res. 2017;39(2):152–7.
Tetri S, Juvela S, Saloheimo P, Pyhtinen J, Hillbom M. Hypertension and diabetes as predictors of early death after spontaneous intracerebral hemorrhage. J Neurosurg. 2009;110(3):411–7.
Yoon JA, Kim DY, Sohn MK, Lee J, Lee SG, Lee YS, et al. Effect of stress hyperglycemia and intensive rehabilitation therapy in non-diabetic hemorrhagic stroke: Korean stroke cohort for functioning and rehabilitation. Eur J Neurol. 2016;23(11):1658–65.
Zheng J, Yu Z, Ma L, Guo R, Lin S, You C, et al. Association between blood glucose and functional outcome in Intracerebral hemorrhage: a systematic review and Meta-analysis. World Neurosurg. 2018;114:e756–e65.
Guo X, Li H, Zhang Z, Li S, Zhang L, Zhang J, et al. Hyperglycemia and mortality Risk in patients with primary Intracerebral hemorrhage: a Meta-analysis. Mol Neurobiol. 2016;53(4):2269–75.
Welsh C, Welsh P, Celis-Morales CA, Mark PB, Mackay D, Ghouri N, et al. Glycated hemoglobin, Prediabetes, and the links to cardiovascular disease: data from UK biobank. Diabetes Care. 2020;43(2):440–5.
Emerging Risk Factors C, Di Angelantonio E, Gao P, Khan H, Butterworth AS, Wormser D, et al. Glycated hemoglobin measurement and prediction of cardiovascular disease. JAMA. 2014;311(12):1225–33.
Su YW, Hsu CY, Guo YW, Chen HS. Usefulness of the plasma glucose concentration-to-HbA1c ratio in predicting clinical outcomes during acute illness with extreme hyperglycaemia. Diabetes Metab. 2017;43(1):40–7.
Li J, Quan K, Wang Y, Zhao X, Li Z, Pan Y, et al. Effect of stress hyperglycemia on neurological deficit and mortality in the acute ischemic stroke people with and without diabetes. Front Neurol. 2020;11:576895.
Zhu B, Pan Y, Jing J, Meng X, Zhao X, Liu L, et al. Stress hyperglycemia and outcome of non-diabetic patients after acute ischemic stroke. Front Neurol. 2019;10:1003.
Wang L, Zhou Z, Tian X, Wang H, Yang D, Hao Y, et al. Impact of relative blood glucose changes on mortality Risk of patient with acute ischemic stroke and treated with mechanical Thrombectomy. J Stroke Cerebrovasc Dis. 2019;28(1):213–9.
Chen X, Liu Z, Miao J, Zheng W, Yang Q, Ye X, et al. High stress hyperglycemia ratio predicts poor outcome after mechanical Thrombectomy for ischemic stroke. J Stroke Cerebrovasc Dis. 2019;28(6):1668–73.
Ngiam JN, Cheong CWS, Leow AST, Wei YT, Thet JKX, Lee IYS, et al. Stress Hyperglycaemia is associated with poor functional outcomes in patients with acute Ischaemic stroke after intravenous thrombolysis. QJM. 2022;115(1):7–11.
Merlino G, Smeralda C, Gigli GL, Lorenzut S, Pez S, Surcinelli A, et al. Stress hyperglycemia is predictive of worse outcome in patients with acute ischemic stroke undergoing intravenous thrombolysis. J Thromb Thrombolysis. 2021;51(3):789–97.
American Diabetes A. 2. Classification and diagnosis of diabetes: standards of medical Care in Diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S13–27.
Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. 1996;27(8):1304–5.
Teo BW, Xu H, Wang D, Li J, Sinha AK, Shuter B, et al. GFR estimating equations in a multiethnic Asian population. Am J Kidney Dis. 2011;58(1):56–63.
Kang K, Lu J, Ju Y, Wang W, Shen Y, Wang A, et al. Association of pre- and post-stroke glycemic status with clinical outcome in spontaneous intracerebral hemorrhage. Sci Rep. 2019;9(1):19054.
Frontera JA, Fernandez A, Claassen J, Schmidt M, Schumacher HC, Wartenberg K, et al. Hyperglycemia after SAH: predictors, associated complications, and impact on outcome. Stroke. 2006;37(1):199–203.
Kruyt ND, Roos YW, Dorhout Mees SM, van den Bergh WM, Algra A, Rinkel GJ, et al. High mean fasting glucose levels independently predict poor outcome and delayed cerebral ischaemia after aneurysmal subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2008;79(12):1382–5.
Shen CL, Xia NG, Wang H, Zhang WL. Association of Stress Hyperglycemia Ratio with Acute Ischemic Stroke Outcomes Post-thrombolysis. Front Neurol. 2021;12:785428.
Chen G, Ren J, Huang H, Shen J, Yang C, Hu J, et al. Admission random blood glucose, fasting blood glucose, stress hyperglycemia ratio, and functional outcomes in patients with acute ischemic stroke treated with intravenous thrombolysis. Front Aging Neurosci. 2022;14:782282.
Ye XH, Cai XL, Nie DL, Chen YJ, Li JW, Xu XH, et al. Stress-induced hyperglycemia and remote diffusion-weighted imaging lesions in primary Intracerebral hemorrhage. Neurocrit Care. 2020;32(2):427–36.
Samiullah S, Qasim R, Imran S, Mukhtair J. Frequency of stress hyperglycaemia and its' influence on the outcome of patients with spontaneous intracerebral haemorrhage. J Pak Med Assoc. 2010;60(8):660–3.
Kimura K, Iguchi Y, Inoue T, Shibazaki K, Matsumoto N, Kobayashi K, et al. Hyperglycemia independently increases the risk of early death in acute spontaneous intracerebral hemorrhage. J Neurol Sci. 2007;255(1–2):90–4.
Passero S, Ciacci G, Ulivelli M. The influence of diabetes and hyperglycemia on clinical course after intracerebral hemorrhage. Neurology. 2003;61(10):1351–6.
Saxena A, Anderson CS, Wang X, Sato S, Arima H, Chan E, et al. Prognostic significance of hyperglycemia in acute Intracerebral hemorrhage: the INTERACT2 study. Stroke. 2016;47(3):682–8.
Bejot Y, Aboa-Eboule C, Hervieu M, Jacquin A, Osseby GV, Rouaud O, et al. The deleterious effect of admission hyperglycemia on survival and functional outcome in patients with intracerebral hemorrhage. Stroke. 2012;43(1):243–5.
Stead LG, Jain A, Bellolio MF, Odufuye A, Gilmore RM, Rabinstein A, et al. Emergency department hyperglycemia as a predictor of early mortality and worse functional outcome after intracerebral hemorrhage. Neurocrit Care. 2010;13(1):67–74.
Yang CJ, Liao WI, Tang ZC, Wang JC, Lee CH, Chang WC, et al. Glycated hemoglobin A1c-based adjusted glycemic variables in patients with diabetes presenting with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2017;12:1923–32.
Liao WI, Wang JC, Lin CS, Yang CJ, Hsu CC, Chu SJ, et al. Elevated glycemic gap predicts acute respiratory failure and in-hospital mortality in acute heart failure patients with diabetes. Sci Rep. 2019;9(1):6279.
Yang Y, Kim TH, Yoon KH, Chung WS, Ahn Y, Jeong MH, et al. The stress hyperglycemia ratio, an index of relative hyperglycemia, as a predictor of clinical outcomes after percutaneous coronary intervention. Int J Cardiol. 2017;241:57–63.
Yuan C, Chen S, Ruan Y, Liu Y, Cheng H, Zeng Y, et al. The stress hyperglycemia ratio is associated with hemorrhagic transformation in patients with acute ischemic stroke. Clin Interv Aging. 2021;16:431–42.
Marik PE, Bellomo R. Stress hyperglycemia: an essential survival response! Crit Care. 2013;17(2):305.
Siesjo BK, Bendek G, Koide T, Westerberg E, Wieloch T. Influence of acidosis on lipid peroxidation in brain tissues in vitro. J Cereb Blood Flow Metab. 1985;5(2):253–8.
Zheng J, Shi L, Liang F, Xu W, Li T, Gao L, et al. Sirt3 ameliorates oxidative stress and mitochondrial dysfunction after Intracerebral hemorrhage in diabetic rats. Front Neurosci. 2018;12:414.
Araki N, Greenberg JH, Sladky JT, Uematsu D, Karp A, Reivich M. The effect of hyperglycemia on intracellular calcium in stroke. J Cerebr Blood F Met. 1992;12(3):469–76.
Massry SG, Smogorzewski M. Role of elevated cytosolic calcium in the pathogenesis of complications in diabetes mellitus. Miner Electrolyte Metab. 1997;23(3–6):253–60.
Chiu CD, Chen CC, Shen CC, Chin LT, Ma HI, Chuang HY, et al. Hyperglycemia exacerbates intracerebral hemorrhage via the downregulation of aquaporin-4: temporal assessment with magnetic resonance imaging. Stroke. 2013;44(6):1682–9.
Liu J, Gao BB, Clermont AC, Blair P, Chilcote TJ, Sinha S, et al. Hyperglycemia-induced cerebral hematoma expansion is mediated by plasma kallikrein. Nat Med. 2011;17(2):206–10.
Bejot Y, Grelat M, Delpont B, Durier J, Rouaud O, Osseby GV, et al. Temporal trends in early case-fatality rates in patients with intracerebral hemorrhage. Neurology. 2017;88(10):985–90.
Qureshi AI, Huang W, Lobanova I, Chandrasekaran PN, Hanley DF, Hsu CY, et al. Effect of moderate and severe persistent hyperglycemia on outcomes in patients with Intracerebral hemorrhage. Stroke. 2022;53(4):1226–34.
Acknowledgements
Not applicable.
Funding
The study was supported by National Key Research and Development Program of China (2018YFC1312200/2018YFC1312204), Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029), Beijing Municipal Committee of Science and Technology (Z201100005620010), Beijing Natural Science Foundation (Z200016), Beijing key clinical specialty and Ministry of Science and Technology of the People’s Republic of China (National Key R&D Programme of China, 2018YFC1705003). The funding bodies did not have any impact on the study design, nor on the collection, analysis, and interpretation of data or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
SL analyzed, interpreted the data, and drafted the original manuscript. YW and QZ contributed to data interpretation. WW design the research. AW performed the statistical analyses. XZ designed the research, handled funding and supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the ethical guidelines from the Helsinki Declaration and was approved by the Institutional Review Board (IRB) of Beijing Tiantan Hospital, Capital Medical University. All participants were above 18 years of age and all of them or their legal proxies signed the written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Included the source of data generated or analyzed during this study. It is an excel file encompassing 2 separated tables. The first table of the excel file including the specific value of each variable while the second table of the excel file including the meaning of each variable.
Additional file 2.
Included the baseline characteristics and their comparisons between included and excluded participants.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, S., Wang, Y., Wang, W. et al. Stress hyperglycemia is predictive of clinical outcomes in patients with spontaneous intracerebral hemorrhage. BMC Neurol 22, 236 (2022). https://doi.org/10.1186/s12883-022-02760-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-022-02760-9