
Abstract
Globally, 4.9 million under-five deaths occurred before celebrating their fifth birthday. Four in five under-five deaths were recorded in sub-Saharan Africa and Southern Asia. Childhood diarrhea is one of the leading causes of death and is accountable for killing around 443,832 children every year. Despite healthcare utilization for childhood diarrhea has a significant effect on the reduction of childhood mortality and morbidity, most children die due to delays in seeking healthcare. Therefore, this study aimed to assess healthcare utilization for childhood diarrhea in the top high under-five mortality countries. This study used secondary data from 2013/14 to 2019 demographic and health surveys of 4 top high under-five mortality countries. A total weighted sample of 7254 mothers of under-five children was included. A multilevel binary logistic regression was employed to identify the associated factors of healthcare utilization for childhood diarrhea. The statistical significance was declared at a p-value less than 0.05 with a 95% confidence interval. The overall magnitude of healthcare utilization for childhood diarrhea in the top high under-five mortality countries was 58.40% (95% CI 57.26%, 59.53%). Partner/husband educational status, household wealth index, media exposure, information about oral rehydration, and place of delivery were the positive while the number of living children were the negative predictors of healthcare utilization for childhood diarrhea in top high under-five mortality countries. Besides, living in different countries compared to Guinea was also an associated factor for healthcare utilization for childhood diarrhea. More than four in ten children didn’t receive health care for childhood diarrhea in top high under-five mortality countries. Thus, to increase healthcare utilization for childhood diarrhea, health managers and policymakers should develop strategies to improve the household wealth status for those with poor household wealth index. The decision-makers and program planners should also work on media exposure and increase access to education. Further research including the perceived severity of illness and ORS knowledge-related factors of healthcare utilization for childhood diarrhea should also be considered by other researchers.
Similar content being viewed by others


Introduction
Globally, 4.9 million under-five deaths (one child every six seconds) were recorded in 2022. Of the total 4.9 million under-five deaths, 2.3 million occurred during the first thirty days of life, and 2.6 million deaths happened between the ages of 1 and 59 months. Four in five under-five deaths occurred in sub-Saharan Africa and Southern Asia; they account for 57% and 26% of under-five deaths, respectively1. Although the death rate significantly declined by more than half from the 2000 report, further efforts are needed to accelerate progress towards the Sustainable Development Goal (SDG) target of 25 child deaths per 1000 live births by 20302. Evidence showed that most under-five deaths in low-and middle-income countries are caused by preventable and treatable diseases such as diarrhea, fever, cough, pneumonia, and malaria1,3.
Childhood diarrhea is one of the leading causes of death and is responsible for killing around 443,832 children every year3,4. According to a UNICEF report in Mali, Niger, and Chad childhood diarrhea causes 18.5%, 17.5%, and 17.2% of child mortality, respectively5. In addition, 10.6% of child mortality in Guinea also due to the diarrheal diseases5. Despite healthcare utilization for childhood diarrhea having a significant effect on the reduction of childhood mortality and morbidity, most children die due to delays in seeking health care in developing countries6,7,8. Different studies reported that distance from healthcare facilities, limited healthcare access, poor knowledge about the symptoms of diseases, perceived curability of illness, lack of money, and a long period of waiting for medical services were the main barriers to low healthcare utilization in developing countries6,7,9,10,11,12.
Healthcare utilization for childhood diarrhea was low in developing countries10,12,13,14. For example, a study conducted in Nigeria showed that only 27% of children seek healthcare14. Correspondingly, in Ethiopia, the magnitude of healthcare utilization for childhood diarrhea was 35%15. Additionally, a systematic review conducted in sub-Saharan Africa also revealed that only 45% of children utilized healthcare for childhood illnesses16.
Literature showed that different factors affecting healthcare utilization for childhood diarrhea include place of residence12,15,17,18, maternal age18,19,20,21,22, maternal educational status6,16,21,22,23,24, sex of the child22,25, age of the child6,15,19,22, husband educational status19,23, marital status17,19,26, household wealth index 12,18,19,21,22,23,24,25, media exposure16,18,22,25, distance to health facilities16,20,21,27, information about oral rehydration15,25, place delivery6,14, and child birth order23.
Different studies related to healthcare utilization have been conducted at the country level6,10,13,14,20,21,28. However, there is no evidence of healthcare utilization for childhood diarrhea in top high under-five mortality countries. Therefore, this study aimed to generate evidence of healthcare utilization for childhood diarrhea in the top high under-five mortality countries by including DHS data from 2013/14 to 2019. The result will help to improve healthcare utilization for childhood diarrhea and to design an intervention strategy to address poor child health status and outcomes in high under-five mortality countries.
Methods
Study setting and design
The study used pooled data from the top high under-five child mortality countries Demographic and Health Survey (DHS) data collected between 2013/14 and 2019, which was obtained using a community-based cross-sectional study design. The countries identified as having the top ten highest under-five mortality rates were selected from the United Nations (UN) child mortality estimation report of 20231. According to the UN report; Niger, Nigeria, Somalia, Chad, Sierra Leone, South Sudan, Central Africa Republic, Guinea, Mali, and DRC were the top ten high under-five mortality countries. Somalia and South Sudan were not included due to the lack of a DHS dataset. In addition, the Central African Republic and Niger were also excluded due to the long period since their last standard DHS (Table 1).
Data source and study population
The analysis was based on the secondary data from the most recent DHS of the top high under-five mortality countries. The DHS program collects standard and comparable data in low-and middle-income countries. The surveys are nationally representative and population-based, with large sample sizes of the same manual, variable name, code, value level, and procedure in more than 90 countries across the world29. The survey used a two-stage stratified sampling technique every five years. In the first stage, enumeration area (EA) clusters were selected by the proportional sample size method. Then, a fixed number of households per cluster was selected by equal probability systematic sampling following the list of households29. The DHS data were collected using face-to-face interviews with reproductive-aged 15–49-year-old women. Detailed survey methodology and sampling methods used in gathering the data are available29. The surveys collect a wide range of self-reported and objective data, with a strong focus on indicators of maternal and child health, reproductive health, nutrition, fertility, mortality, and self-reported health behaviors among adults30. Before analysis, weighting was done to get a representative sample by dividing the individual weight for women (v005) by 1,000,000 to estimate the number of cases29. The total weighted sample size for this study was 7254, which included Guinea (1043), Mali (1631), Nigeria (3950), and Sierra Leone (630). Chad and the Democratic Republic Congo (DRC) were excluded after appending the data because they had no observation of the outcome variable. The study included children who had diarrhea in the 2 weeks preceding the surveys, whether they sought public or private healthcare or not (Fig. 1).

Final sample size and schematic presentation of how the study sample size was selected.
Study variables
Outcome variable
The outcome variable for this study was healthcare utilization for childhood diarrhea reported by the mother or caregiver. The DHS collected data on whether the child had diarrhea in the 2 weeks preceding the survey, and the healthcare utilization for childhood diarrhea was also assessed by interviewing the mothers. The mothers were considered to have utilized healthcare if they sought medical treatment from a defined governmental or non-governmental health facility for childhood diarrhea coded as “1”, and mothers not seeking healthcare were coded as “0”.
Independent variables
We considered individual and community-level variables for this study. At the individual level; sex of the child, age of the child, maternal age, maternal educational status, husband’s educational status, current marital status, sex of household head, wealth index, media exposure, information about oral rehydration, covered by health insurance, wanted last child, place of delivery, birth order, and number of living children were included. At the community level, place of residence, distance to the health facility, community-level poverty, community-level media exposure, community-level education, and countries were considered.
Community-level variables used in the analysis were from two sources; direct community-level variables (including place of residence, country, and distance to health facility) that were used without any aggregation and aggregated community-level variables that were generated by aggregating individual-level variables at the cluster level. The community-level education, community-level poverty, and community-level media exposure were generated by aggregating the individual-level variables at the cluster level and categorized them as low if the proportion is < 50% and high if the proportion is ≥ 50% based on the national median value by considering their frequency distribution31.
Media exposure
Was generated from the frequency of listening to the radio, watching television, and reading a newspaper or magazine. Respondents who never listened to the radio, read newspapers, or watched television were considered to have no exposure to mass media, and were otherwise exposed to mass media.
Wealth index
The variable wealth index was re-categorized as “poor”, “middle”, and “rich” by merging poorest and poorer as “poor” and richest with richer as “rich”.
Data collection procedure
The research was performed based on the DHS data by accessing it from the official database of the MEASURE DHS program www.measuredhs.com. For the study, we used the Birth Record (BR) data set file.
Data management and analysis
The variables in this study were extracted and analyzed from the BR dataset using STATA version 17.0 (StataCorp, College Station, Texas 77,845 USA) statistical software which is available at https://www.stata.com. The extracted data from the included countries were weighted using sampling weight (v005) to obtain a valid statistical estimation. In DHS, multi-stage stratified cluster sampling techniques were employed, and the data were hierarchical. So, to draw valid inferences and conclusions, a multilevel model was fitted. A two-level binary logistic regression model was used to estimate the effect size of independent variables on healthcare utilization for childhood diarrhea. Four models were fitted. The first model was the null model (a model without the independent variable), which was a model fitted to calculate the extent of cluster variability on healthcare utilization for childhood diarrhea. It was assessed using the Intraclass Correlation Coefficient (ICC), Likelihood Ratio test (LR), Median Odds Ratio (MOR), and Proportional Change in Variance (PCV). The Intraclass Correlation Coefficient (ICC) was used to quantify the degree of heterogeneity of healthcare utilization for childhood diarrhea between clusters. The null model provides the variance of the outcome variable due to the cluster without the independent variables (to evaluate the extent of the cluster variation in healthcare utilization for childhood diarrhea). Considering clusters as a random variable, the MOR indicates the median value of the odds ratio between the area at the highest risk and the area at the lowest risk of healthcare utilization for childhood diarrhea when randomly picking out two different clusters. Proportional Change in Variation (PCV) was reported to assess the total variation of healthcare utilization for childhood diarrhea explained by the final model (a model with individual-level and community-level variables) relative to the null model (a model without explanatory variables). Model I (a model that includes only individual-level factors), model II (a model that includes only community-level factors), and model III (a model adjusted with both individual and community-level factors) were fitted, and a model comparison was made by using deviance.
Both bi-variable and multivariable analyses were done. In the bi-variable, two-level binary logistic regression analysis, variables with a p-value ≤ 0.2 were considered in the multivariable analysis. The Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI) at p-value < 0.05 in the multivariable multilevel analysis was reported to declare the statistical significance and strength of the association between healthcare utilization for childhood diarrhea and independent variables. Before multi-variable analysis, multi-collinearity was checked using the Variance Inflation Factor (VIF), and the mean VIF was 2.02.
Ethical approval
The data were accessed from the DHS website https://dhsprogram.com/data/available-datasets.cfm after getting registered and permission. The retrieved data were used for this registered research only. The data were kept confidential and no identifier was made to identify any household or individual respondent.
Result
Individual level characteristics
A total of 7254 mothers who have under-five children were included in this study. Out of the study participants, 3373 (46.50%) were aged between 25 and 34 years. Of the respondents, 4611 (63.57%) of them had no formal education, and the majority (94.95%) were in union in marital status. More than half (52.73%) of the participants were from poor household wealth status. Most (85.81%) of respondents had information about oral rehydration, but 97.58% of participants were not covered by health insurance. Of the involved children, nearly half (48.64%) of them were females, and 54.74% of them were less than two years old (Table 2).
Community level characteristics
Of the participants, 72.63% of mothers/caregivers were rural dwellers. About half of the participants were from communities with a high proportion of community-level poverty and a low proportion of community-level education. The highest number of participants was from Nigeria, 3950 (54.45%), and the lowest number of study participants was from Sierra Leone, 630 (8.68%) (Table 3).
Healthcare utilization for childhood diarrhea
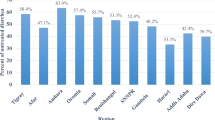
The overall utilization of healthcare for childhood diarrhea in countries with high under-five mortality was 58.40% (95% CI 57.26%, 59.53%). The highest magnitude of healthcare utilization was in Sierra Leone (71.61%) and the lowest magnitude of healthcare utilization for childhood diarrhea was in Mali (45.25%) (Fig. 2).

magnitude of healthcare utilization for childhood diarrhea in top high under-five mortality countries.
Factors associated with healthcare utilization for childhood diarrhea in top high under-five mortality countries.
Fixed effects (measures of association) result
The third model was the complete model, which shows the association of individual and community-level factors of healthcare utilization for childhood diarrhea among mothers in top high under-five mortality countries. The husband’s educational status, household wealth index, media exposure, information about oral rehydration, place of delivery, number of living children, and country of residence were significant predictors of healthcare utilization for childhood diarrhea.
Accordingly, mothers who had husbands with primary education (AOR = 1.29; 95% CI 1.07, 1.56) and secondary or higher education (AOR = 1.28; 95% CI 1.09, 1.51) were 1.29 times and 1.28 times more likely to seek healthcare for childhood diarrhea than mothers with an uneducated husband, respectively. The likelihood of healthcare utilization for childhood diarrhea among mothers/caregivers from middle household wealth status increased by 21% (AOR = 1.21; 95% CI 1.03, 1.43) as compared to mothers/caregivers from poor household wealth status. Mothers/caregivers who had media exposure had 1.31 times (AOR = 1.31; 95% CI 1.15, 1.50) higher likelihood of seeking healthcare for childhood diarrhea as compared to their counterparts. Mothers/caregivers who had information about oral rehydration were twice (AOR = 2.09; 95% CI 1.77, 2.46) more likely to utilize healthcare for childhood diarrhea than their counterparts. Concerning place of delivery, mothers who delivered in a health facility were 1.26 times (AOR = 1.26; 95% CI 1.10, 1.44) more likely to utilize healthcare for childhood diarrhea than those who delivered at home. Additionally, mothers/caregivers who had 3 – 4 children and five or more children were 23% (AOR = 077; 95 CI% 0.62, 0.95) and 28% (AOR = 0.72; 95% CI 0.56, 0.94) less likely to utilize healthcare for childhood diarrhea as compared to mothers who had 1 – 2 children, respectively. Furthermore, the odds of utilizing healthcare for childhood diarrhea were 64% (AOR = 0.34; 95% CI 0.28, 0.42) and 34% (AOR = 0.66; 95% CI 0.54, 0.80) lower in Mali and Nigeria as compared to Guinea, respectively (Table 4).
Random effect (measures of variation) result
The final model (model III) was the best-fitted model since it had the lowest deviance. The ICC in the null model was 15.75%, which revealed that about 15.75% of the total variability of healthcare utilization for childhood diarrhea was due to cluster differences. Moreover, the MOR was 2.02 in the null model, and this indicated that there was a variation between clusters. A mother/caregiver in the cluster with a high likelihood of utilizing healthcare for childhood diarrhea had twice higher odds of being utilizing healthcare compared with a mother/caregiver in a cluster with a low likelihood of healthcare utilization for childhood diarrhea during random selection of mothers/caregivers in two different clusters. The full model explained 11.5% of the variability in seeking healthcare for childhood diarrhea, and deviance was used for model fitness (Table 4).
Discussion
This study aimed to determine the magnitude and identify the determinant factors of healthcare utilization for childhood diarrhea in top high under-five mortality countries. The result of this study showed that the magnitude of utilization of healthcare for childhood diarrhea in countries with high under-five mortality was 58.40%. Regarding the detrminants of healthcare utilization for childhood diarrhea; the husband's educational status, household wealth index, media exposure, information about oral rehydration, place of delivery, number of living children, and country of residence were identified as predictors of healthcare utilization for childhood diarrhea in high under five mortality countries.
The overall magnitude of healthcare utilization for childhood diarrhea in the top high under-five mortality countries was 58.40% (95% CI 57.26%, 59.53%), which is consistent with studies conducted in Ethiopia17,26,32. However, the finding of this study is higher than a study conducted in Ethiopia6,15,23,33, and Nigeria14. The possible explanation for the difference might be the study sample size, this study has a larger sample size than the previous studies conducted in the single study setting. In this regard, the larger sample size might lead to a high magnitude of healthcare utilization for childhood diarrhea in this study. Additonally, it is higher than a study done in SSA16, which might be due to the survey year differnces in which as the survey year increases the awareness to use modern healthcare for illness may inceases.
The current study finding showed a lower magnitude of healthcare utilization for childhood diarrhea than study reports in Ethiopia9,12 and Indonesia28. The discrepancy might be explained by the definition of the outcome variable, where the previous studies assessed healthcare utilization for common childhood illnesses, whereas this study focused only on childhood diarrhea.
This study revealed that mothers/caregivers who had primary or above-educated husbands were more likely to utilize healthcare for childhood diarrhea than mothers with uneducated husbands. This finding is consistent with studies done in Ethiopia19,23,33. The possible justification might be that education can be assumed to be related to an increased awareness of symptoms, illnesses, and the availability of services. Moreover, educational level is a major factor in higher employment opportunities, which may in turn increase healthcare utilization by enhancing the ability to cope with the various costs involved23. The finding indicates the government should strengthen education programs to improve healthcare utilization.
The odd of healthcare utilization for childhood diarrhea was high among mothers/caregivers of middle household wealth status as compared to poor household wealth status. Other studies in Ethiopia12,18,19,23,24, Bangladesh21,22, SSA16, Zimbabwe34 and Gambia25 also supported our findings. The possible reason might be that children might not get the required medical attention due to the mother’s inability to pay for health services from poor household wealth status. Media exposure was also found to be a positive predictor of healthcare utilization for childhood diarrhea, which is supported by studies done in Ethiopia18, SSA16, and Bangladesh22. This could be explained by media can be useful for the dissemination of health information and healthcare, which could enhance people's understanding, attitudes, and behaviors about the utilization of health services.
Oral rehydration information is also another determinant of healthcare utilization for childhood diarrhea. Mothers/caregivers who had information about oral rehydration had a higher likelihood of healthcare utilization for childhood diarrhea as compared to their counterparts. This study finding is consistent with studies done in Ethiopia15,18 and Gambia25. The possible explanation for this might be those mothers aware of the oral rehydration may go to the health facilities immediately to seek care for their children, as they may have a better understanding of oral rehydration treatment. This implies that awareness creation about oral rehydration through media and other strategies will improve healthcare utilization for childhood diarrhea.
Mothers/caregivers who gave their last birth in a health facility were more likely to utilize healthcare for childhood diarrhea than those who gave birth at home. This study finding is comparable with studies conducted in Nigeria14 and Ethiopia6. The possible explanation for this result might be that facility birth enable mothers to be aware of the advantages of seeking healthcare at the time of a child's illness. This finding implies the government needs to develop strategies to enhance health facility delivery.
Additionally, this study also found that the number of living children was negatively associated with maternal healthcare utilization for childhood diarrhea. This could be explained by mothers’ high workload due to large family size, could bring about giving less attention to the sick child. This finding contradicts the finding from Burundi27 which reported that children of mothers who had three and four children were more likely to get healthcare for childhood illnesses compared to those whose mothers had one child. The reason for the variation might be due to the definition of the outcome variable, where the previous study dealt with common childhood illnesses while our study was specifically focused on childhood diarrhea. Furthermore, the odds of utilizing healthcare for childhood diarrhea were lower in Mali and Nigeria as compared to Guinea. The possible reason might be due to the countries' differences in terms of their health systems, policies, government structures, and health institutions.
Strengths and limitations of the study
The secondary data used for the analysis was extracted from a nationally representative survey collected by employing a two-stage stratified sampling technique. The analysis with multilevel models using confidence intervals helps to determine the cluster variation in the hierarchical data of DHS. However, the cross-sectional nature of the survey limits to establish a cause-and-effect relationship. Additionally, since the study used secondary data variables related to perceived severity of illness, ORS knowledge and distance to health facilities couldn’t be addressed. Measuring mothers’ perceptions of childhood illness may not always be true.
Conclusion
More than four in ten children didn’t receive health care for childhood diarrhea in the top under-five mortality countries. Thus, to increase healthcare utilization for childhood diarrhea, health managers and policymakers should develop strategies to improve the household wealth status of those with poor household wealth indexes. The decision-makers and the government of these countries should increase access to education and work on mass media to sensitize women about oral rehydration and facility birth.
Data availability
Data used in our study are publicly available upon request from the DHS program website. (https://dhsprogram.com/).
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- DHS:
-
Demographic and health survey
- ICC:
-
Intra-class correlation coefficient
- IQR:
-
Interquartile range
- LR:
-
Likelihood ratio
- MOR:
-
Median odds ratio
- PCV:
-
Proportional change in variance
- SDG:
-
Sustainable development goal
- SSA:
-
Sub-Saharan Africa
References
UNICEF and World Health Organization, Levels and Trends Child Mortality-Report 2023: Estimates Developed by the United Nations Inter-agency Group for Child Mortality Estimation. 2024.
UN. The sustainable development goals report 2020. Geneva: United Nations, 2020. https://unstats.un.org/sdgs/report/2020/TheSustainable-Development-Goals Report-2020.pdf.
WHO, Child mortality (under 5 years).
WHO, Diarrhoeal disease. 2024.
UNICEF, Diarrhoea remains a leading killer of young children, despite the availability of a simple treatment solution, in Diarrhoeal disease. 2024.
Alene, M. et al. Health care utilization for common childhood illnesses in rural parts of Ethiopia: evidence from the 2016 Ethiopian demographic and health survey. BMC Public Health 19, 1–12 (2019).
Nasrin, D. et al. Health care seeking for childhood diarrhea in developing countries: evidence from seven sites in Africa and Asia. Am. J. Trop Med. Hyg. 89(1 Suppl), 3–12 (2013).
Fikire, A., Ayele, G. & Haftu, D. Determinants of delay in care seeking for diarrheal diseases among mothers/caregivers with under-five children in public health facilities of Arba Minch town, southern Ethiopia; 2019. PloS ONE 15(2), e0228558 (2020).
Dagnew, A. B., Tewabe, T. & Murugan, R. Level of modern health care seeking behaviors among mothers having under five children in Dangila town, north West Ethiopia, 2016: a cross sectional study. Italian J. Pediatrics 44, 1–6 (2018).
Ndungu, E. W., Okwara, F. N. & Oyore, J. P. Cross sectional survey of care seeking for acute respiratory illness in children under 5 years in rural Kenya. Am. J. Pediatr. 4(3), 69–79 (2018).
Strasser, R., Kam, S. M. & Regalado, S. M. Rural health care access and policy in developing countries. Ann. Rev. Public Health 37, 395–412 (2016).
Zenebe, G. A. et al. Level of mothers’/caregivers’ healthcare-seeking behavior for child’s diarrhea, fever, and respiratory tract infections and associated factors in ethiopia: a systematic review and meta-analysis. BioMed Res. Int. 2022(1), 4053085 (2022).
Onyeonoro, U. U. et al. Urban–rural differences in health-care-seeking pattern of residents of Abia state, Nigeria, and the implication in the control of NCDS. Health Serv. Insights 9, HSI. S31865 (2016).
Adeoti, I. G. & Cavallaro, F. L. Determinants of care-seeking behaviour for fever, acute respiratory infection and diarrhoea among children under five in Nigeria. Plos ONE 17(9), e0273901 (2022).
Azage, M. & Haile, D. Factors affecting healthcare service utilization of mothers who had children with diarrhea in Ethiopia: evidence from a population based national survey. Rural Remote Health 15(4), 1–10 (2015).
Yaya, S., Odusina, E. K. & Adjei, N. K. Health care seeking behaviour for children with acute childhood illnesses and its relating factors in sub-Saharan Africa: evidence from 24 countries. Trop. Med. Health 49, 1–8 (2021).
Begashaw, B., Tessema, F. & Gesesew, H. A. Health care seeking behavior in Southwest Ethiopia. PloS ONE 11(9), e0161014 (2016).
Woldeamanuel, B. T. Trends and factors associated with healthcare utilization for childhood diarrhea and fever in Ethiopia: further analysis of the demographic and health surveys from 2000 to 2016. J. Environ. Public Health 2020(1), 8076259 (2020).
Gelaw, Y. A., Biks, G. A. & Alene, K. A. Effect of residence on mothers’ health care seeking behavior for common childhood illness in Northwest Ethiopia: a community based comparative cross–sectional study. BMC Res. Notes 7, 1–8 (2014).
Muhumuza, J. et al. Factors influencing timely response to health care seeking for diarrheal episodes among children under five by caregivers in rural Uganda. Sci. J. Public Health 5(3), 246–253 (2017).
Saha, S., Haque, M. A. & Chowdhury, M. A. B. Health-seeking behavior and associated factors during the first episode of childhood diarrhea and pneumonia in a coastal area of Bangladesh. Int. J. Commun. Med. Public Health 9(2), 575–582 (2022).
Sarker, A. R. et al. Prevalence and health care–seeking behavior for childhood diarrheal disease in Bangladesh. Glob. Pediatric Health 3, 2333794X16680901 (2016).
Ayalneh, A. A., Fetene, D. M. & Lee, T. J. Inequalities in health care utilization for common childhood illnesses in Ethiopia: evidence from the 2011 Ethiopian demographic and health survey. Int. J. Equity Health 16, 1–9 (2017).
Gebrehiwot, E. M. et al. Childhood diarrhea in central Ethiopia: determining factors for mothers in seeking modern health treatments. Sci. J. Clin. Med. 4(1), 4–9 (2015).
Terefe, B. et al. Individual and community level factors associated with medical treatment-seeking behavior for childhood diarrhea among the Gambian mothers: evidence from the Gambian demographic and health survey data, 2019/2020. BMC Public Health 23(1), 579 (2023).
Kolola, T., Gezahegn, T. & Addisie, M. Health care seeking behavior for common childhood illnesses in Jeldu District, Oromia Regional State, Ethiopia. PloS ONE 11(10), e0164534 (2016).
Ahinkorah, B. O. et al. Barriers to healthcare access and healthcare seeking for childhood illnesses among childbearing women in sub-Saharan Africa: a multilevel modelling of Demographic and Health Surveys. Plos ONE 16(2), e0244395 (2021).
Khasanah, U. et al. Healthcare-seeking behavior for children aged 0–59 months: evidence from 2002–2017 Indonesia Demographic and Health Surveys. Plos ONE 18(2), e0281543 (2023).
Croft, Trevor N., Aileen M. J. Marshall, Courtney K. Allen, et al. 2018. Guide to DHS Statistics. Rockville, Maryland, USA: ICF.
Fabic, M. S., Choi, Y. & Bird, S. A systematic review of demographic and health surveys: data availability and utilization for research. Bull. World Health Org. 90, 604–612 (2012).
Liyew, A. M. & Teshale, A. B. Individual and community level factors associated with anemia among lactating mothers in Ethiopia using data from Ethiopian demographic and health survey, 2016; a multilevel analysis. BMC Public Health 20, 1–11 (2020).
Adane, M. et al. Utilization of health facilities and predictors of health-seeking behavior for under-five children with acute diarrhea in slums of Addis Ababa, Ethiopia: a community-based cross-sectional study. J. Health, Populat. Nutr. 36, 1–12 (2017).
Geda, N. R. et al. Disparities in mothers’ healthcare seeking behavior for common childhood morbidities in Ethiopia: based on nationally representative data. BMC Health Serv. Res. 21, 1–11 (2021).
Musuka, G. et al. Associations of diarrhea episodes and seeking medical treatment among children under five years: insights from the Zimbabwe Demographic Health Survey (2015–2016). Food Sci. Nutr. 9(11), 6335–6342 (2021).
Acknowledgements
We acknowledge the DHS programs, for the permission to use all the relevant DHS data for this study.
Author information
Authors and Affiliations
Contributions
M.G.T. conceptualized the study, reviewed the literature, carried out the methodology, and statistical analysis, and interpreted the results. M.J., K.A.D.T.Z.T., D.M.G., A.H., L.D.B. and G.T. were involved in the methodology, involved in formal analysis, and interpretation. M.G.T. and G.T. were prepared and revised the manuscript. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tiruneh, M.G., Jejaw, M., Demissie, K.A. et al. Multilevel analysis of healthcare utilization for childhood diarrhea in high under five mortality countries. Sci Rep 14, 15375 (2024). https://doi.org/10.1038/s41598-024-65860-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-65860-1
- Springer Nature Limited