
Abstract
Background
Children are at higher risk of acquiring infections and developing severe disease. This study assessed the health care seeking behavior and associated factors of urban and rural mothers for common childhood illness in Northwest Ethiopia.
Methods
A comparative community based cross-sectional study was conducted among urban and rural mothers living in the district. A multistage sampling technique was used to select the study participants. A pre-tested and structured questioner via interview was used to collect the data. Binary logistic regression analysis was used to identify associated factors. Odds ratio with 95% CI was computed to assess the strength of the associations.
Result
A total of 827 (274 urban and 553 rural) mothers were interviewed. Among these, 79.3% (95% CI: (76.5%, 82.06%)) of the mothers were sought health care in the district. Health care seeking behavior was higher among urban mothers (84.6%) than rural mothers (76.7%). Marital status, completion health extension package, and sex of child were significantly associated with health care seeking behavior of urban mothers. Whereas age of child, age and occupation of mothers, educational level of fathers, wealth quintile, and type of reported illness were significantly associated with rural mothers. Perceived severity of illness was significantly associated with both urban and rural mothers for health care seeking behavior.
Conclusion
The overall health seeking behaviors of mothers for common childhood illness was high. However, urban mothers seek health care more than rural. Socio Economic position and types of reported illness has an effect for health seeking behavior of rural mothers. Whereas child sex preference and graduation status for health extension package has an effect for health care seeking behavior of urban mothers. Work on strengthen accessibility of health care services in the rural mothers and increase awareness of mothers about the disadvantage of sex preferences will improve the health care seek behavior of families regardless of the severity of illness and types of illnesses.
Similar content being viewed by others

Background
Millions of mothers and their children through the world are living in a social environment that doesn’t encourage health care seeking behavior [1]. Reduction of childhood mortality is a worldwide health priority and one of the Millennium Developmental Goals (MDG). According to the United Nations Children’s Fund (UNICEF) 2012 report globally 6.9 million children die before the age of five years annually. The majority of these death occurred in Sub-Saharan Africa. Ethiopia is one of the countries with a consistently high under- five mortality rate. It is ranked 36th among Sub- Saharan Africa countries [2].
Rural and urban populations have differences in socio- demographic, socio-economic and cultural compositions which have an effect on their health care seeking behavior. In sub Saharan Africa, child mortality is higher among rural, poor and less educated families [3]. Early health care seeking behavior of mothers has a potential to reduce child mortality particularly in developing countries like Ethiopia [4]. However, different studies showed that mothers health care seeking behavior for common childhood illness are influenced by socio-demographic and cultural, educational factors. Studies also indicated that timely decision to seek remedies, and times of health seeking after the onset of illness are influenced by residence [5–7]. Children from rural communities often have the highest risk of infection and severe disease especially for diarrhea, fever and acute respiratory illness (ARI), mothers are less likely to seek appropriate health care for them as compared to urban mothers [8]. Little is known about the magnitude and determinants of health care seeking behaviors of mothers’ for their children when they ill in Ethiopia especially in the study area. However, recent evidence indicates that health care seeking behaviors of mothers are increasing because of it considers only the urban dwellers.
Thus, this study aimed to identify the prevalence of health care seeking behaviors and associated factors of health care seeking behaviors among mothers for their children living in urban and rural areas.
Methods
A community based comparative cross – sectional study was conducted in Bure district from April to June, 2103. It is about 419 km away from Northwest of Addis Ababa, the capital city of Ethiopia. According to the 2007 census projection, the district has a total population of 161,480. It has five urban and twenty three rural kebeles[9].
Multistage sampling technique was used to select the study participants. The district was classified into two strata; urban and rural. Then three urban and six rural kebeles were randomly selected. For the purpose of this study, census was conducted in the selected kebele to estimate the approximate number of eligible mothers. Mothers who had under – five children with common childhood illnesses two weeks preceding the data collection period were included. Whenever there was more than one mother having under - five children in the household, one of them were selected using lottery method. The sample size was calculated using a two population proportion formula; considering 37.2% proportion of urban mothers and 22.4% rural mothers seeking health care for fever according to EDHS report [10], a 5% significance level, power of 80%,1:2 urban to rural ratio, design effect 2 and 10% possible non – response rate. The sample size was estimated to be 786 (274 urban and 553 rural). While a sample size was regionally computed to be 786, a preliminary survey prior to a data collection shows that 886 mothers were eligible.
Data were collected via interview with a pre-tested and structured questionnaire. Data collectors and supervisors were health professionals. Training was given to the data collectors and supervisors on the objective, confidentiality of information, respondent’s right and techniques of interview prior to data collection.
Socio – demographic data; sex, age, occupation, religion, educational level, and wealth quintiles were collected. Wealth quintile was collected by asking the presence or absence of durable assets and services at the house hold level. Different indicators were used for urban and rural areas to measure wealth quintiles. A score of 1 was given if the asset was present and 0 if absent. The asset mean scores were re categorized into five different wealth quintiles of equal proportion (Lowest, Second, Middle, Fourth and Highest wealth control groups) by using Principal Component Analysis (PCA).
Health care seeking behavior was the outcome variable which was dichotomized as “yes” (seeking health care) or “no” (did not seeking health care) when their children were ill. Mothers were considered as seeking health when they visited any health facilities (Hospital, Health Center, Health Post, Privet Clinic) after perceiving the illness of their child within two weeks of data collection period.
The returned questionnaires were checked for completeness by the investigator. The data were entered into Epi INFO version 3.5.3 and analyzed by SPSS version 20. Descriptive statistics were done to summarize the data in relation to the different variables. Binary logistic regression model was used to assess the association between the dependent and independent variables. Variables having P value ≤0.2 in the bivariate analysis were entered into multivariate logistic regression models to control the effect of confounding. Both Crude Odds Ratio (COR) and Adjusted Odds Ratio (AOR) with 95% confidence interval (CI) were calculated to measure associations.
Ethical clearance was obtained from the institutional review board of the University of Gondar. A formal letter of communication to the district health office was secured. Verbal informed consent was obtained from each study participants prior to the interview. They were also informed that participation was on voluntary basis and they can withdraw at any time if they are not comfortable about the interview.
Results
Socio-demographic characteristics of participants
A total of 827 mothers (with a response rate of 93.3%) were interviewed. Nearly one third (33.1%) were urban dwellers. Among the study participants only 94(34.3%) urban and 73(13.2%) rural mothers were attended formal education. The mean age (SD) of the mothers children was 31.4 (6.2) years and 23.6 (15.7) months, respectively. Seventy - seven (28.1%) of urban and 430 (78%) of rural households had graduated from the health extension package in the community.
Health care seeking behaviors
The overall health care seeking behavior of mothers for common childhood illness was 79.3% (95% CI: (76.5%, 82.06%)). A total of 84.6%: (95% CI: (80.3%, 88.8%)) urban mothers and (76.7%: (95% CI: (73.2%, 80.2%)) rural mothers were seeking health care for common childhood illness.
Governmental health center and hospitals were the most common place where mothers sought health care [79.1%: (80% urban and 54.3% rural)]. The main reasons reported for not seeking health care were the thought that the disease may resolve by itself over time [Table 1].
Factors associated with health care seeking behaviors
We have fitted three different models to assess health care seeking behavior. The first model was fitted to assess the overall factors of health care seeking behavior for common child hood illness. Variables such as residence, perceived severity, marital status, health extension package graduation status, sex and age of child’s, age and occupation of mothers, educational level of fathers, wealth quintiles, and types of reported illness were significantly associated with health care seeking behaviors for the whole mothers irrespective of residence. Mothers who lived in urban [AOR: 11.5, 95% CI (5.407, 24.483)], and perceived severity of illness [AOR: 9.23, 95% CI (5.88, 14.562] were more likely to seek health care than the counter parts. Mothers who graduated from health extension package 96.6% times [AOR: 0.034, 95% CI (0.016, 0.074)] and male sex preference children 61.0% [AOR: 1.610, 95% CI, (1.040, 2. 495)] were more likely to seek health care when compared to the counterpart. Mothers in the fourth wealth Quintiles were 5.126 times more likely to seek health care than those in the lowest Quintiles [AOR: 5.126 95% CI: (2.544, 10.331)].
Furthermore, mothers’ whose husband attend formal education were 2.467 times more likely to seek health care than those mothers whose husband didn’t attend formal education (AOR: 2.467, 95% CI: (1.385, 4.380)) [Table 2].
The second model was fitted only for rural mothers. Accordingly, age and occupation of mothers’, educational level of fathers, wealth Quintiles, age of child’s, types of reported illness showed a significant association. Rural mothers with relatively younger age were 1.79 times more likely to seek health care as compared to older age mothers [AOR: 0.558, 95% CI, (0.339, 0.919)] and mothers who had younger children were 4 times more likely to seek health care as compared to mothers who have older children [AOR: 0.240, 95% CI: (0.083, 0.699)]. In addition, mothers who are in third and fourth wealth quintiles were also more likely to seek health care compared to in the lowest Quintiles [AOR: 4.456, 95% CI: (2.091, 9.965)] and [AOR: 2.522, 95% CI: (1.186, 5.365)], respectively.
Mothers who had formal education attended husbands [AOR: 3.170, 95% CI: ( 1.490, 6.746)] and a child with diarrheal disease [AOR: 0.538, 95% CI: ( 0.306, 0.946)] were more likely to seek health care as compared to their counterparts. Moreover, mothers’ who gave birth in the health center [AOR: 0.484, 95% CI: (0.257, 0.913)] and hospital [AOR: 0.328, 95% CI: (0.128, 0.890)] seek health care more likely than those who give birth at home [Table 3].
The third model was fitted for urban mothers only. As a result, urban mothers who were married were 1.7 times more likely to seek health care than unmarried mothers’ [AOR: 0.228, 95% CI: (0.027, 0.719)]. Mothers who had male children seek health care 6.2 times more likely than those who had female children [AOR: 6.222, 95% CI: (2.263, 17.109)]. Mothers who were graduated for health extension package were 97.6% times more likely to seek health care than the counterpart [AOR: 0.024, 95% CI: (0.007, 0.085)] [Table 4].
Discussion
Seeking health care for common childhood illnesses from health institution has a great potential to reduce child mortality [4]. In this study, health care seeking behavior of mothers was 79.3% (95% CI: 76.5%, 82.06%). There was a significant difference of health care seeking behaviors between rural (76.7%) and urban mothers (84.6%). Urban mothers were 11.5 times more likely to seek health care than rural mothers. This might be due to the accessibility of health care for urban mothers. In Ethiopia, health care coverage is relatively high in urban than rural [11]. It could be also due to accessibility of information about the importance of seeking of health care for childhood illness.
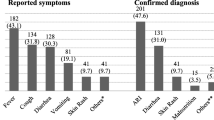
Both urban and rural mothers sought health care for diarrheal illness than ARI. This finding was similar with other study done in Bahir Dar and EDHS 2011 report [10, 12]. This could be due to the reason that diarrhea is more visible for the mothers than ARI. And it could be difficult for uneducated mother to feel the severity of fever and ARI. But it is inconsistent with a study done in Derra district, Ethiopia [5] and Rural Uganda [13] in which they sought health care more for fever.
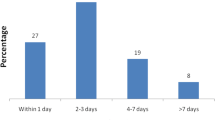
This result showed that residence has a great effect in the mothers’ health care seeking behavior for common childhood illness. The study result is consistent with similar studies done in Ethiopia [5, 11] and, in Africa [14, 15]; South Africa (14) and South East Nigeria [15]. The time of seeking health care after the perception of illness was also significantly differ between urban and rural mothers. Urban mothers’ seek health care on the first day of perceived onset of illness than rural mothers’. The possible reason for delaying of rural mothers to seek health care might be their attempt to try home remedies, lack of money, or socio – cultural factors like consulting the elders and relatives.
The main factors influencing mothers’ health care seeking behavior of the district identified in this study were perception of severity of illness, graduation of health extension package, type of reported illnesses, sex of the child, educational status of husband and wealth quintile.
Even though, the principle of health care service delivery system of Ethiopia assumed that health care seeking behavior of mothers is equal. This study revealed that mothers’ health care seeking behaviors were more likely influenced by perception of severity illness. This is consistent with report of other studies [5, 15–20].
Poverty is a serious constraint on mothers’ choices about seeking health care. The finding of this study also indicated that socio–economic and graduation status of the household health extension package was significant predictors of health care seeking behaviors of mothers’. Studies done in Ethiopia also showed that urban inhabitants are in the highest quintiles than rural [5, 11]. But in this study, both urban and rural dwellers found in equal proportion from the lowest to the highest quintiles.
Mothers who had male children were more likely to seek health care than who had female. This is supported by a study done in Ethiopia and Kenya [11, 18]. Though, other studies done in rural parts of Nigeria and India reported that sex had no association with mothers’ health care seeking behavior [18, 19]. This is due to the fact that in Ethiopia there is a cultural influence in which mother are giving priority for male child than female child. Moreover, the starting of health extension program was lately in urban areas can be a reason for the difference [10].
The present studies also documented that husband’s educational status had a significant effect on mothers’ health care seeking behavior.
This study has the following limitation: first the study didn’t include other child hood illness though they are not common in the study area. Second, as it needs longer time to see the seasonal variation they didn’t consider the seasonal variation as independent variables.
Conclusion
Residence has an effect on the mothers’ health care seeking behaviors for common childhood illness. Urban mothers seek health care more than rural mothers. Age and occupation of the mothers’, educational level of the fathers, wealth quintiles, age of child, types of reported illness showed a significant association for health seeking behavior of rural mothers for common child hood illness. Whereas marital status, graduation status for health extension package and sex of children’s showed a significant association for health care seeking behavior of urban mothers. It is better to give infancies especially for rural mothers to seek health care regardless of the severity of illness and types of illnesses.
References
WHO: World Health Organization statistics. 2009, France: WHO
UNICEF: Committing to Child Survival Progress Report 2012. 2012, United Nations Plaza, New York, USA: UNICEF
Molyneux S, Muga’ala V, Harpham T, Snow W: Maternal responses to childhood fevers: a comparison of rural and urban residents in coastal Kenya. Trop Med Int Health. 1999, 4 (12): 836-45. 10.1046/j.1365-3156.1999.00489.x.
UNICEF: The State of World’s children. 2008, New York, USA: UNICEF
Assefa T, Tegegn T, Deribew A: Mothers’ Health care seeking behavior for childhood illness in Derra district, North Shoa zone, Oromia Regional State, Ethiopia. 2008, Addis Ababa, Ethiopia: Ethiop J Health Science, 87-
Mohamed E, Hanafi K, Hussein S, Salim E, Awad K: Treatment-seeking behavior for malaria in children under five years of age: implication for home management in rural areas with high seasonal transmission in Sudan. Malar J. 2006, 5: 60-10.1186/1475-2875-5-60.
Mbagaya GM, Odhiambo MO, Oniang’o RK: Mother’s health seeking behavior during child illness in a rural western Kenya community. Afr Health Sci. 2005, 5 (4): 322-7.
UNICEF: Pneumonia and diarrhea tackling the deadliest diseases for the world’s poorest children. 2012, New York, USA: UNICEF
Comission FPC: Summary and Statistical Report o f the 2007 population and housing census of Ethiopia. 2008, Addis Ababa: CSA, 57-60.
CSA: Ethiopia Demographic and Health Survey 2011. 2012, Addis Ababa, Ethiopia: Entral Statistical Agency [Ethiopia] and ICF International
FMOH: Ethiopia health sector development programme IV annual performance report. 2011/2012, Addis Ababa, Ethiopia: FMOH
Worku A: Prevalence of childhood illness and mothers’/caregivers’ care seeking behavior in Bahir Dar, Ethiopia: A descriptive community based cross sectional study. Open J Prev Med. 2013, 3 (2): 155-9. 10.4236/ojpm.2013.32020.
Mbonye AK: Prevalence of childhood illnesses and care-seeking practices in rural Uganda. Sci World J. 2003, 3: 721-30.
Promtussananon S, Peltzer K: Health care-seeking behavior for child illnesses among rural mothers in South Africa: a pilot study. Health SA Gesondheid. 2003, 8 (2): 43-
Ezeoke U, Nwobi E, Ekwueme O, Tagbo B, Aronu E, Uwaezuoke S: Pattern of health seeking behavior of mothers for common childhood illness in Engumetropolis South East zone Nigeria. Niger J Clin Pract. 2010, 13 (1): 37-40.
Benjamin S, Onwujeke O, Onoka A, Ughasoro D: Rural-urban differences in maternal responses to childhood fever in South East Nigeria. PLoS One. 2008, 3 (3): 1788-10.1371/journal.pone.0001788.
Sreeramaredy T, Shankar P, Sreekumaran B, Subba S, Joshi H, Ramachandran U: Care seeking behavior for childhood illness-a questionnaire survey in western Nepal. BMC Int Health Human Rights. 2006, 6 (7): 1472-698.
Taffa N, Chepngeno G: Determinants of health care seeking for childhood illnesses in Nairobi slums. J Trop Med Int Health. 2005, 10 (3): 240-5. 10.1111/j.1365-3156.2004.01381.x.
Sreeramareddy T, Sathyanarayana N, Harsha K: Utilization of health care services for childhood morbidity and associated factors in India. PLoS One. 2012, 7 (12): 51904-10.1371/journal.pone.0051904.
Abdulraheem S, Parakoyi D: Factors Affecting Mothers' Healthcare-Seeking Behavior for Childhood Illnesses in a Rural Nigerian Setting. Early Child Dev Care. 2009, 179 (5): 671-83. 10.1080/03004430701500885.
Acknowledgement
Bure zuria district and Bure town health office and mothers of the study participants are acknowledged for their cooperation and assistance. We would like to thank Mr. Gedefaw Abeje for his valuable support during this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YA designed the study, performed the statistical analysis, and drafted the paper. GA and KA participated in the paper writing. All authors contributed to the data analysis and read and approved the final paper.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Gelaw, Y.A., Biks, G.A. & Alene, K.A. Effect of residence on mothers’ health care seeking behavior for common childhood illness in Northwest Ethiopia: a community based comparative cross – sectional study. BMC Res Notes 7, 705 (2014). https://doi.org/10.1186/1756-0500-7-705
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1756-0500-7-705