
Abstract
Background
Childhood illnesses and mortality rates have declined over the past years in sub-Saharan African countries; however, under-five mortality is still high in the region. This study investigated the magnitude and factors associated with health care seeking behaviour for children with childhood illnesses in 24 sub-Saharan African countries.
Methods
We used secondary data from Demographic and Health Surveys (DHSs) conducted between 2013 and 2018 across the 24 sub-Saharan African countries. Binary logistic regression models were applied to identify the factors associated with health care seeking behaviour for children with acute childhood illnesses. The results were presented using adjusted odds ratios (aOR) with 95% confidence intervals (CIs).
Results
Overall, 45% of children under-5 years with acute childhood illnesses utilized health care facilities. The factors associated with health care seeking behaviour for children with acute illnesses were sex of child, number of living children, education, work status, wealth index, exposure to media and distance to a health facility.
Conclusions
Over half of mothers did not seek appropriate health care for under-five childhood illnesses. Effective health policy interventions are needed to enhance health care seeking behaviour of mothers for childhood illnesses in sub-Saharan African countries.
Similar content being viewed by others
Background
Childhood illnesses such as fever, diarrhea and acute respiratory infection (ARI) are serious child health issues in low income countries [1, 2]. Globally, in 2015, about 5.9 million under five children died due to preventable causes [1, 3,4,5], and approximately three out of every four under-five deaths occur due to ARI, diarrhea and fever [1, 6]. This phenomenon is more pronounced in low-income and middle-income countries [7], where childhood deaths and illnesses are serious health issues [1, 8], especially in sub-Saharan Africa [4, 9,10,11]. Although under-five mortality has generally declined globally, it is still a critical issue in sub-Saharan Africa [12, 13], as the region accounts for about 50% of under-five preventable mortality [14].
Prior evidence showed that pneumonia and diarrhea are among the most common causes of childhood illnesses and deaths in many African countries [15, 16]. Addressing the burden of childhood illnesses is critical in sub-Saharan Africa, because sub-Saharan African countries have a greater burden of childhood illnesses in contemporary time [17,18,19]. In addition, progress to achieve Sustainable Development Goal (SDG) 3.2 (elimination of preventable child death, reduction in neonatal mortality to less than 12 per 1000 live births and those of under-five mortality to less than 25 per 1000 live births for every country by 2030) is slower, and without the necessary policies and interventions, sub-Saharan Africa may not meet the SDG 3.2 target by 2030 [20]. There is evidence that at least one child dies out of every 12 births in sub-Saharan Africa before age five compared to one out of every 147 in developed countries [3]. The majority of under-five mortality in sub-Saharan Africa is due to infectious and parasitic diseases, such as malaria, respiratory infections, meningitis and diarrhea [5, 13, 14, 21]. Diarrhea, for instance, is a major cause of morbidity and mortality globally, as it accounts for 1.3 million deaths among children under-5 years of age each year [21]. Although childhood illnesses can be managed efficiently in sub-Saharan Africa, evidence suggest poor health care seeking behaviour among mothers for childhood illnesses in the region [18, 22]. Evidence based information is thus needed on health care seeking behaviour of mothers for effective policies and interventions in sub-Saharan Africa [22]. Meanwhile, prompt and adequate health care seeking behaviour interventions among mothers can substantially reduce childhood mortality due to childhood illnesses in low-income and middle-income countries [10].
Efforts have been made globally and by various countries in sub-Saharan Africa to reduce morbidity and mortality of under-five resulting from childhood illnesses through policies that will promote child health care services among mothers [23,24,25,26]. To achieve the Sustainable Development Goal target of at most 25 deaths per 1000 live births by the year 2030, there are efforts and high-level commitments towards addressing the issues. For instance, at the global level are the Integrated Management of Childhood Illness (IMCI) strategy developed by the World Health Organization (WHO), the Every Woman Every Child Strategy and the Partnership for Maternal Newborn and Child Health [3, 10, 27, 28]. Moreover, many countries in sub-Saharan Africa have policies and programmes that are aimed at reducing under-five morbidity and mortality. For instance, Nigeria introduced the Maternal and Child Health Policy in 1994, National Immunization Policy and Standards Practice in 1996 and Breastfeeding Policy in 1999 [14]. Many African countries have also embraced the International Child Rights Policy, emphasizing and promoting child health care services among [29].
Although prior studies have provided some evidence on factors affecting childhood illnesses in low-income and middle-income countries [30,31,32], there is little knowledge on health care seeking behaviour among mothers for childhood illnesses in sub-Saharan Africa. The factors associated with health care seeking behaviour from studies conducted in different countries include knowledge of danger signs, occupation, residence, education, age, marital status, birth order, mass media exposure [1, 13, 33] and income [34]. Community level promotion of prompt health care seeking behaviour among mothers for childhood illnesses to enhance the health care of under-five children has been emphasised [5, 35]. Meanwhile, under-five mortality is still high in sub-Saharan Africa despite the progress made in the last few decades. Proper health care seeking behaviour of mothers for childhood illnesses can prevent or reduce the magnitude of child mortality resulting from childhood illnesses [10, 36, 37]. This study, therefore, seeks to examine the factors associated with under-five children illnesses such as diarrhea and fever and health care service utilization in sub-Saharan African countries. Assessing health care services for childhood diseases and associated risk factors may help prevent and reduce under-five morbidity and mortality in sub-Saharan African countries [5].
Methods
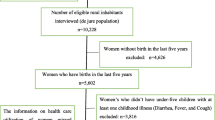
The study used secondary data from the Demographic and Health Surveys (DHSs) of 24 countries in sub-Saharan Africa. The countries were selected if the surveys were conducted between 2010 and 2018 [33, 38], and outcome and explanatory variables were available. The DHSs use multi-stage stratified sampling method [33, 38, 39]. These DHSs are nationally representative and comparable surveys conducted worldwide in more than 85 countries [40]. The surveys usually collect a wide range of self-reported and objective data with a strong focus on indicators of reproductive health, fertility, child and maternal health, nutrition, mortality, and self-reported health behaviours among adults [41]. The sample for the final analyses was 98,590. It included children who had diarrhea and/or fever or cough in the 2 weeks preceding the surveys, whether they sought private or public health care or not. The country specific details are presented in Additional file 1.
Measurement of variables
Outcome variable
The outcome of interest was under-five children with incidence of diarrhea and/or cough or fever in the past 2 weeks before the surveys. Those who went for consultation in a public or private health care service provider and those who did not go were classified as users and non-users, respectively [14].
Explanatory variables
The explanatory variables considered were maternal education (no formal education, primary and secondary plus), age of mother (15–24, 25–34 and 35–49), occupation of mother (working and not working), wealth index (poorest, poorer, middle, richer and richest), marital status (never married and ever married), residence (urban and rural), distance to health facility (experience no difficulty in getting to a health facility/not a problem in getting to a health facility or experienced difficulty in getting to a health facility/a problem to in getting to a health facility), media access (no access and have access) and sex of the child (male and female) [14].
Data analyses
First, descriptive analyses were performed using frequency and percentage distributions to examine the characteristics of participants and prevalence of health care seeking behaviour among mothers for children with childhood illnesses. Differences in prevalence were examined using chi-square test. Furthermore, to assess multicollinearity, correlation test was performed among independent variables. The findings showed that the assumptions of multicollinearity were not violated. The tolerance value was greater than 0.10 [42]. Non-response and missing data were excluded to arrive at the weighted sample size. Second, a binary logistic regression model was fitted to examine the relationship between explanatory variables and health care seeking behaviour of mothers. To adjust for sampling variability, DHSs incorporate two-stage cluster sampling [33, 38, 39, 43] and sampling weight was applied to account for the complex survey design including weight, cluster, and strata. Stata version 14 (Stata Corp, College Station, Texas, USA) was used to estimate the prevalence of health seeking behaviour of mothers and odds ratios with 95% confidence intervals (95% CI).
Results
Characteristics of the sample population
The descriptive characteristics of respondents are shown in Table 1. The analysis involved a weighted sample of 98,590 under-five children in sub-Saharan African countries, with a fairly even gender distribution (male: 50.7% vs. female: 49.3%). Approximately 54% of children under-5 years of age with acute childhood illnesses did not utilize any health care service. Almost half of mothers were between 25 and 34 years (48.1%). More than one-third of the mothers had primary education (37.6%) and 34.7% had no formal education. A greater proportion of mothers reported they were ever married (93.7%), and 40.0% had no access to media. About 71.1% were living in rural areas, and 39.2% indicated that distance to a health care facility was a problem.
Prevalence of health care seeking behaviour for children with childhood illnesses
Table 1 presents the prevalence of health care seeking behaviour for a sick child in different sub-Saharan African countries. The gender differences in seeking health care were not large. There were preferences for male child care in all countries except Lesotho, Sierra Leone and Zimbabwe. Table 2 also presents the prevalence of health care seeking behaviour of mothers for sick children by socio-demographic characteristics. The prevalence of health care seeking behaviour of mothers for sick children was higher for male children (46.1%), among respondents with formal education (65.3% had at least primary education), women aged 15–24 (46.6%), richer household category (45.8%), never married (47.9%), working (46.5%), exposed to media (47.3%) and those who had no problem (experience no difficulty) accessing the health care services (46.7%). The highest prevalence of health care seeking behaviour among mothers for children with acute childhood illnesses was found in Sierra Leone (65.1%) and the lowest in Cameroon (22.1%) (see Additional file 1).
Binary logistic regression
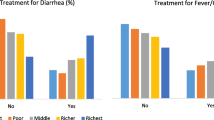
The results of the adjusted odds ratios (aOR) and 95% CI for the relationship between socio-demographic variables and health care seeking behaviour of mothers for childhood illnesses are presented in Table 3. The findings showed that the odds of health care service utilization for childhood illnesses were significantly higher among mothers with male children (OR 1.06; 95% CI 1.03–1.08) compared to mothers with female children. The odds of health care service utilization for childhood illnesses were found to be higher among mothers who had primary education (OR 1.19; 95% CI 1.16–1.23) and higher education (OR 1.18; 95% CI 1.14–1.23) compared to those with no formal education. Mothers who were working (OR 1.15; 95% CI 1.12 to 1.18), exposed to media (OR 1.20; 95% CI 1.17–1.23) were more likely to utilize health care service for childhood illnesses compared to their counterparts who were not working or exposed to the media, respectively. The odds of health care service utilization for childhood illnesses were, however, found to be significantly lower among mothers of 3–4 children (OR 0.90; 95% CI 0.87 to 0.93) and mothers of 5+ children (OR 0.85; 95% CI 0.81 to 0.88) compared to those with 1–2 children. In addition, the odds were lower for women in the richer household category (OR 0.90; 95% CI 0.86 to 0.94) and the richest household category (OR 0.85; 95% CI 0.81 to 0.89) compared to the poorest household category. Women who reported that distance was a problem in accessing health care services had lower odds (OR 0.87; 95% CI 0.85 to 0.89) of health care service utilization for childhood illnesses than those who reported that distance was not a problem in accessing health care services.
Discussion
This study investigated the predictors of health care service seeking behaviour among mothers for childhood illnesses in sub-Saharan African countries. Overall, 98,590 children under-5 years of age in sub-Saharan African countries born within 5 years preceding the surveys, and reported incidence of diarrhea and/or cough or fever in the past 2 weeks before the surveys [14] were included in the study. The findings revealed disparities in health care seeking behaviour among mothers for children with acute childhood illnesses in sub-Saharan African countries. Hence, much is needed to be done to enhance health care seeking behaviour among mothers for children with acute childhood illnesses. For instance, the highest prevalence of health care seeking behaviour of mothers for children with acute childhood illnesses was found in Sierra Leone (65.1%), while the lowest was found in Cameroon (22.1%), (see Additional file 1). These findings reinforce the need for concerted efforts to enhance health care seeking behaviour of mothers for children with acute childhood illnesses in the region [18].
Overall, less than half (45%) of under-five children with acute childhood illnesses utilized health care services, consistent with previous findings [1, 34, 37, 44]. Low health care seeking behaviour among mothers has been shown to be a major determinant of childhood morbidity and mortality in sub-Saharan African countries [22, 45], which has been attributed to child, social and maternal factors [1, 13, 33, 34]. For example, there is evidence of an association between mothers’ education and health care seeking behaviour for their children, where women with higher levels of education are more likely to seek health care services for their children [33, 46, 47]. Thus, proper health care seeking behaviour of mothers could prevent and reduce childhood illnesses [10, 36, 37], and childhood mortality in low-income and middle-income countries [1, 34]. In many sub-Saharan African countries, poor and inadequate medical facilities and poor health seeking behaviour are known risk factors for infant and child mortality [1].
In this study, we found sex of child, number of living children, education, work status, wealth index, exposure to media and distance to a health facility to be predictors of health care seeking behaviour of mothers for children with acute illnesses. We observed higher odds of health care seeking behaviour for male children as compared with female children. This finding corroborates previous findings [48, 49], where culture and traditional beliefs have been implicated for this outcome [50]. Male-child preference by some cultures and traditional expectations of men as breadwinners for families are some of the reasons for the extra-care of male children [50]. Furthermore, we observed that education is an important factor in mothers’ health care seeking behaviour, especially for childhood illnesses [2, 35, 51, 52]. Thus, enhancing women’s educational levels will help advance health care seeking behaviour for childhood illnesses [45, 48, 53].
The higher odds of health care seeking behaviour found among employed mothers [1] may be linked to empowerment [54,55,56], and women’s ability to decide on certain maternal issues [55] and pay for health care service [55, 56]. Health care seeking behaviour of mothers had been associated with skilled or semi-skilled employment [36], which can also be linked with women empowerment. Low health care seeking behaviour among the "richer and richest" wealth indices contrast other findings from previous study [2, 14, 57, 58]. This study speculates that geographical location, educational attainment of women and level of awareness may explain the differences in findings. Meanwhile, low socio-economic conditions including poverty has also been shown to be a factor influencing the attitude of mothers towards seeking health care services for their children [36]. For instance, children might not get the required medical attention due to the mothers’ inability to pay for health services. Prior studies also noted the importance of access to health care facilities in enhancing mothers health care seeking behaviour, and further reducing childhood illnesses [1, 2, 48, 51].
Strengths and limitations
The study has both limitations and strengths. One of the strengths of the study is that the data sets are from several sub-Saharan African countries and are nationally representative. This permits generalisation of the results in sub-Saharan African countries, despite the time lag in data collection periods. However, comparison of result from different surveys should be done carefully and with caution due to differences in data collection periods [56]. Furthermore, the sample size is sufficiently large as it increases the validity of the findings. Nonetheless, the study is subject to social desirability and recall bias [50, 59], because it was based on self-reported data [59]. Finally, the surveys are cross-sectional, and they only permit association and not causal relationship [30, 38].
Conclusion
The study analysed secondary data from 24 sub-Saharan African countries on acute childhood illnesses and health care seeking behaviour of mothers in sub-Saharan Africa. The findings indicate a low prevalence of health care seeking behaviour of mothers for childhood illnesses. Socio-economic factors including maternal education were found to be associated with health care seeking behaviour. Public health policies and programmes that target women's empowerment and development are critical to addressing the issue. This may help increase the prevalence of health care seeking behaviour of mothers for childhood illnesses, and consequently improve child health outcomes in sub-Saharan African countries.
Availability of data and materials
Data used in this study were obtained from the DHS Program and available at: https://dhsprogram.com/data/available-datasets.cfm.
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- DHS:
-
Demographic and Health Survey
- IMCI:
-
Integrated Management of Childhood Illness
- WHO:
-
World Health Organization
References
Kebede ZT, Gelaye KA, Merid MW, Akalu TY, Amare AT, Toni AT, et al. High common childhood illnesses while treatment seeking behavior of mothers’/care givers’ was low at rural northwest Ethiopia. In Review; 2020. https://www.researchsquare.com/article/rs-7641/v3. Accessed 2 Oct 2020.
Bennett A, Eisele T, Keating J, Yukich J. Global trends in care seeking and access to diagnosis and treatment of childhood illnesses. 2015. https://dhsprogram.com/publications/publication-wp116-working-papers.cfm. Accessed 1 June 2021.
Azuh DE, Chinedu S, Samuel OW, Azuh A, Joshua G, Amoo EO. Factors influencing the survival of under-five children among women visiting government health care facility in semi-urban communities in Nigeria. Cogent Arts Humanit. 2019;6(1): 1686800.
Kalipeni E, Iwelunmor J, Grigsby-Toussaint D. Maternal and child health in Africa for sustainable development goals beyond 2015. Glob Public Health. 2017. https://doi.org/10.1080/17441692.2017.1304622.
Kolola T, Gezahegn T, Addisie M. Health care seeking behavior for common childhood illnesses in Jeldu District, Oromia Regional State, Ethiopia. PLoS ONE. 2016;11(10): e0164534.
WHO | Levels and trends in child mortality report 2018. World Health Organization. http://www.who.int/maternal_child_adolescent/documents/levels_trends_child_mortality_2018/en/. Accessed 7 Oct 2020.
Mishra K, Mohapatra I, Kumar A. A study on the health seeking behavior among caregivers of under-five children in an urban slum of Bhubaneswar, Odisha. J Fam Med Prim Care. 2019;8(2):498–503.
Levels and trends in child mortality. UNICEF data. 2019. https://data.unicef.org/resources/levels-and-trends-in-child-mortality-2019/. Accessed 1 June 2021.
Adedokun ST, Uthman OA, Adekanmbi VT, Wiysonge CS. Incomplete childhood immunization in Nigeria: a multilevel analysis of individual and contextual factors. BMC Public Health. 2017;17(1):236.
Ogundele OA, Ogundele T, Olajide OS, Agunbiade OI. Effect of community integrated management of childhood illness on mothers’ healthcare-seeking behaviour and home management of childhood illness in Ile Ife, South-West Nigeria: a household survey. S Afr J Child Health. 2016;10(1):16–9.
Doctor HV, Nkhana-Salimu S, Abdulsalam-Anibilowo M. Health facility delivery in sub-Saharan Africa: successes, challenges, and implications for the 2030 development agenda. BMC Public Health. 2018;18(1):1–12.
Lungu EA, Darker C, Biesma R. Determinants of healthcare seeking for childhood illnesses among caregivers of under-five children in urban slums in Malawi: a population-based cross-sectional study. BMC Pediatr. 2020;20(1):1–13.
Wambui WM, Kimani S, Odhiambo E. Determinants of health seeking behavior among caregivers of infants admitted with acute childhood illnesses at Kenyatta National Hospital, Nairobi, Kenya. Int J Pediatr. 2018;2018: e5190287.
Adedokun ST, Adekanmbi VT, Uthman OA, Lilford RJ. Contextual factors associated with health care service utilization for children with acute childhood illnesses in Nigeria. PLoS ONE. 2017;12(3): e0173578.
Despite progress, childhood diseases remain major threat in sub-Saharan Africa. World Bank. https://www.worldbank.org/en/news/press-release/2013/09/04/despite-progress-childhood-diseases-remain-major-threat-in-sub-saharan-africa. Accessed 21 Oct 2021.
Child health. WHO | Regional Office for Africa. https://www.afro.who.int/health-topics/child-health. Accessed 15 Oct 2021.
Thomas AR. Childhood diseases—a major threat in Sub-Saharan Africa. The Sierra Leone telegraph. 2013. https://www.thesierraleonetelegraph.com/childhood-diseases-a-major-threat-in-sub-saharan-africa/. Accessed 21 Oct 2021.
Akinyemi JO, Banda P, De Wet N, Akosile AE, Odimegwu CO. Household relationships and healthcare seeking behaviour for common childhood illnesses in sub-Saharan Africa: a cross-national mixed effects analysis. BMC Health Serv Res. 2019;19(1):308.
Apuleni G, Jacobs C, Musonda P. Predictors of health seeking behaviours for common childhood illnesses in poor resource settings in Zambia, a community cross sectional study. Front Public Health. 2021;9: 569569.
Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the global burden of disease study 2019. Institute for Health Metrics and Evaluation. 2021. http://www.healthdata.org/research-article/global-regional-and-national-progress-towards-sustainable-development-goal-32. Accessed 21 Oct 2021.
Nyasulu PS, Ngamasana E, Kandala N-B. Sources of health care among under-5 Malawian children with diarrhea episodes: an analysis of the 2017 demographic and health survey. Glob Pediatr Health. 2019. https://doi.org/10.1177/2333794X19855468.
Geldsetzer P, Williams TC, Kirolos A, Mitchell S, Ratcliffe LA, Kohli-Lynch MK, et al. The recognition of and care seeking behaviour for childhood illness in developing countries: a systematic review. PLoS ONE. 2014;9(4): e93427.
Malaria in Africa. UNICEF data. https://data.unicef.org/topic/child-health/malaria/. Accessed 3 Nov 2020.
WHO | Malaria in children under five. World Health Organization. http://www.who.int/malaria/areas/high_risk_groups/children/en/. Accessed 3 Nov 2020.
Diarrhoea. UNICEF data. https://data.unicef.org/topic/child-health/diarrhoeal-disease/. Accessed 3 Nov 2020.
Adedokun ST, Yaya S. Childhood morbidity and its determinants: evidence from 31 countries in sub-Saharan Africa. BMJ Glob Health. 2020;5(10): e003109.
Every woman every child. https://www.everywomaneverychild.org. Accessed 1 June 2021.
PMNCH, the Partnership for Maternal, Newborn, and Child Health. Resource Centre. https://resourcecentre.savethechildren.net/publishers/pmnch-partnership-maternal-newborn-and-child-health. Accessed 1 June 2021.
Convention on the rights of the child text. https://www.unicef.org/child-rights-convention/convention-text. Accessed 3 Nov 2020.
Amin R, Shah NM, Becker S. Socioeconomic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: a cross-sectional analysis. Int J Equity Health. 2010;9(1):9.
Benova L, Campbell OMR, Ploubidis GB. Socio-economic inequalities in curative health-seeking for children in Egypt: analysis of the 2008 demographic and health survey. BMC Health Serv Res. 2015;15(1):482.
Mbagaya GM, Odhiambo MO, Oniang’o RK. Mother’s health seeking behaviour during child illness in a rural western Kenya community. Afr Health Sci. 2005;5(4):322–7.
Adedokun ST, Yaya S. Factors influencing mothers’ health care seeking behaviour for their children: evidence from 31 countries in sub-Saharan Africa. BMC Health Serv Res. 2020;20(1):1–9.
Abdulraheem IS, Parakoyi DB. Factors affecting mothers’ healthcare-seeking behaviour for childhood illnesses in a rural Nigerian setting. Early Child Dev Care. 2009;179(5):671–83.
Kagabo DM, Kirk CM, Bakundukize B, Hedt-Gauthier BL, Gupta N, Hirschhorn LR, et al. Care-seeking patterns among families that experienced under-five child mortality in rural Rwanda. PLoS ONE. 2018;13(1): e0190739.
Sigdel D, Onta M, Bista AP. Factors affecting health seeking behaviors for common childhood illnesses among rural mothers in Chitwan. Int J Health Sci Res. 2018;8(11):177–84.
Assefa T, Belachew T, Tegegn A, Deribew A. Mothers’ health care seeking behavior for childhood illnesses in Derra district, Northshoa zone, Oromia regional state, Ethiopia. Ethiop J Health Dev. 2008;18(3):87–94.
Ahinkorah BO, Budu E, Seidu A-A, Agbaglo E, Adu C, Ameyaw EK, et al. Barriers to healthcare access and healthcare seeking for childhood illnesses among childbearing women in sub-Saharan Africa: a multilevel modelling of demographic and health surveys. PLoS ONE. 2021;16(2): e0244395.
Cochran WG. Sampling techniques, 3rd edition. 1977. http://archive.org/details/Cochran1977SamplingTechniques_201703. Accessed 14 Nov 2021.
Corsi DJ, Neuman M, Finlay JE, Subramanian SV. Demographic and health surveys: a profile. Int J Epidemiol. 2012;41(6):1602–13.
Short Fabic M, Choi Y, Bird S. A systematic review of demographic and health surveys: data availability and utilization for research. Bull World Health Organ. 2012;90(8):604–12.
Tabachnick BG, Fidell LS, Ullman JB. Using multivariate statistics, vol. 5. Boston: Pearson; 2007.
Lê T. An analysis of sample designs and sampling errors of the demographic and health surveys. Calverton: Macro International; 1997.
Mothers’ health care seeking behavior and associated factors for common childhood illnesses, Northwest Ethiopia: community based cross-sectional study. springermedizin.de. https://www.springermedizin.de/mothers-health-care-seeking-behavior-and-associated-factors-for-/16415620. Accessed 2 Oct 2020.
PRIME PubMed | Mothers/caregivers healthcare seeking behavior towards childhood illness in selected health centers in Addis Ababa, Ethiopia: a facility-based cross-sectional study. https://www.unboundmedicine.com/medline/citation/31269920/Mothers/caregivers_healthcare_seeking_behavior_towards_childhood_illness_in_selected_health_centers_in_Addis_Ababa_Ethiopia:_a_facility_based_cross_sectional_study_. Accessed 2 Oct 2020.
Ghosh N, Chakrabarti I, Chakraborty M, Biswas R. Factors affecting the healthcare-seeking behavior of mothers regarding their children in a rural community of Darjeeling District, West Bengal. Int J Med Public Health. 2013;3(1):12–6.
Chandwani H, Pandor J. Healthcare-seeking behaviors of mothers regarding their children in a tribal community of Gujarat, India. Electron Physician. 2015;7(1):990.
Nega B, Bogale KA, Nigussie ZM. Health care seeking behavior and associated factor among mothers/caregivers of under-five children with acute diarrhea in Dangila zuria Woreda, North west Ethiopia. Epidemiology. 2019. https://doi.org/10.1101/667923.
Katiyar R, Ahmed N, Singh JV, Singh VK. Gender difference in health seeking behaviour among mothers of under five children in Lucknow. Int J Community Med Public Health. 2017;5(1):272–4.
Odusina EK, Ayotunde T, Kunnuji M, Ononokpono DN, Bishwajit G, Yaya S. Fertility preferences among couples in Nigeria: a cross sectional study. Reprod Health. 2020;17(1):1–9.
Sisay S, Endalew G, Hadgu G. Assessment of mothers/care givers health care seeking behavior for childhood illness in rural Ensaro District, North Shoa Zone, Amhara Region, Ethiopia 2014. Glob J Life Sci Biol Res. 2017;1:15.
Ogunlesi TA, Olanrewaju DM. Socio-demographic factors and appropriate health care-seeking behavior for childhood illnesses. J Trop Pediatr. 2010;56(6):379–85.
Chakrabarti I, Chakraborty M, Biswas R, Ghosh N. Factors affecting the healthcare-seeking behavior of mothers regarding their children in a rural community of Darjeeling district, West Bengal. Int J Med Public Health. 2013;3(1):12.
Duflo E. Women empowerment and economic development. J Econ Lit. 2012;50(4):1051–79.
Kabeer N. Resources, agency, achievements: reflections on the measurement of women’s empowerment. Dev Chang. 1999;30(3):435–64.
Yaya S, Odusina EK, Uthman OA, Bishwajit G. What does women’s empowerment have to do with malnutrition in sub-Saharan Africa? Evidence from demographic and health surveys from 30 countries. Glob Health Res Policy. 2020;5:1.
Simieneh MM, Mengistu MY, Gelagay AA, Gebeyehu MT. Mothers’ health care seeking behavior and associated factors for common childhood illnesses, Northwest Ethiopia: community based cross-sectional study. BMC Health Serv Res. 2019;19(1):1–7.
Nzioki JM, Onyango RO, Ombaka JH. Socio-demographic factors influencing maternal and child health service utilization in Mwingi; a rural semi-arid district in Kenya. Am J Public Health Res. 2015;3(1):21–30.
Yaya S, Odusina EK, Bishwajit G. Prevalence of child marriage and its impact on fertility outcomes in 34 sub-Saharan African countries. BMC Int Health Hum Rights. 2019;19(1):33.
Acknowledgements
The authors thank the MEASURE DHS project for their support and for free access to the original data.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
EKO and SY conceptualised and designed the study, acquired, analysed, interpreted the data, and drafted the manuscript. NKA critically reviewed the manuscript. SY had final responsibility to submit for publication. All authors agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was not required for this study, since the data are secondary and is available in the public domain. More details regarding DHS data and ethical standards are available at: http://goo.gl/ny8T6X.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Survey characteristics.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yaya, S., Odusina, E.K. & Adjei, N.K. Health care seeking behaviour for children with acute childhood illnesses and its relating factors in sub-Saharan Africa: evidence from 24 countries. Trop Med Health 49, 95 (2021). https://doi.org/10.1186/s41182-021-00385-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41182-021-00385-1