
Abstract
Background
Medication-induced salivary gland dysfunction (MISGD), xerostomia (sensation of oral dryness), and subjective sialorrhea cause significant morbidity and impair quality of life. However, no evidence-based lists of the medications that cause these disorders exist.
Objective
Our objective was to compile a list of medications affecting salivary gland function and inducing xerostomia or subjective sialorrhea.
Data Sources
Electronic databases were searched for relevant articles published until June 2013. Of 3867 screened records, 269 had an acceptable degree of relevance, quality of methodology, and strength of evidence. We found 56 chemical substances with a higher level of evidence and 50 with a moderate level of evidence of causing the above-mentioned disorders. At the first level of the Anatomical Therapeutic Chemical (ATC) classification system, 9 of 14 anatomical groups were represented, mainly the alimentary, cardiovascular, genitourinary, nervous, and respiratory systems. Management strategies include substitution or discontinuation of medications whenever possible, oral or systemic therapy with sialogogues, administration of saliva substitutes, and use of electro-stimulating devices.
Limitations
While xerostomia was a commonly reported outcome, objectively measured salivary flow rate was rarely reported. Moreover, xerostomia was mostly assessed as an adverse effect rather than the primary outcome of medication use. This study may not include some medications that could cause xerostomia when administered in conjunction with others or for which xerostomia as an adverse reaction has not been reported in the literature or was not detected in our search.
Conclusions
We compiled a comprehensive list of medications with documented effects on salivary gland function or symptoms that may assist practitioners in assessing patients who complain of dry mouth while taking medications. The list may also prove useful in helping practitioners anticipate adverse effects and consider alternative medications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
We compiled a comprehensive list of medications with documented effects on salivary gland function or symptoms that may assist practitioners assessing patients who complain of dry mouth while taking medications. |
The list may also prove useful in helping practitioners anticipate oral adverse effects and consider alternative medications. |
1 Introduction
Increased life expectancy, aging populations, and the association of these with polypharmacy have been intriguing topics over the last few decades. The World Health Statistics of 2014 published on the World Health Organization website reports a life expectancy of 55–87 years in its various constituent countries, with even the lower economy countries reporting rapid increases in life expectancy. However, with increased age comes a greater number of ailments, which in turn is indicative of a higher intake of medications.
Medications for the treatment of various diseases may also cause adverse effects, including those related to the oral cavity by their effects on the salivary glands. Apart from medications used to treat salivary gland disorders, other medications can also have the following adverse effects: salivary gland dysfunction (SGD), including salivary gland hypofunction (SGH) (an objectively measured decrease in salivation) or objective sialorrhea (an excessive secretion of saliva), xerostomia (subjective feeling of dry mouth), or subjective sialorrhea (feeling of having too much saliva). Medication-induced SGH and objective sialorrhea are collectively termed medication-induced salivary gland dysfunction (MISGD). The possible adverse effects associated with these disorders, especially SGH, include dental caries, dysgeusia, oral mucosal soreness, and oral candidiasis.
Current literature guiding clinicians in the prescribing of medications while considering the relevant adverse effects on salivary glands is very scarce. Most of the available literature attempting to list relevant drugs comprises a compendium based on manufacturers’ drug profiles, narrative reviews, and case reports, or original research papers not containing a overall list of medications [1–10]. A systematic evidence-based list that identifies and lists medications that could objectively be associated with MISGD, xerostomia, or subjective sialorrhea is lacking. Hence, the MISGD group of the World Workshop on Oral Medicine VI (WWOM VI) aimed to review the current knowledge on this subject and compile a list of medications and their objective effects on salivary gland function, based on a high level of evidence and relevance.
2 Materials and Methods
The MISGD group comprised five reviewers (AA, RJ, NN, YS, and AlV), six consultants (senior experts in fields related to MISGD: DA, CD, JE, AMP, GP, and ArV), one research librarian (RM), one group head (AW), and two supervisors on behalf of the WWOM VI Steering Committee (SBJ and ARK). This review addresses one of the MISGD topics covered by the group, an updated classification of medications reported to cause objective SGD. The research method was based on the policies and standards set forth by a task force for WWOM IV [11] and by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [12], which was adapted to the current review.
2.1 Step 1: Scope Definition
The current review covered seven research questions, as follows:
Which medications have been reported to induce:
-
1.
SGD in humans?
-
2.
SGD in animals?
-
3.
xerostomia but not SGD?
-
4.
drooling but not SGD?
-
5.
xerostomia-related oral symptoms (but not SGD) other than excessive dryness/wetness?
-
6.
xerostomia but have not been tested yet for induction of SGD?
-
7.
drooling but have not been tested yet for induction of SGD?
2.2 Step 2: Search Term Selection
The following keywords and subject headings were selected for each research question:
-
Q1.
Medication/drugs/humans AND salivary gland dysfunction, xerostomia, dry mouth, reduced salivary flow rate, hyposalivation, sialorrhea, drooling.
-
Q2.
Medication/drugs/animals AND salivary gland dysfunction, reduced salivary flow rate, hyposalivation, drooling.
-
Q3.
Medication/drugs AND xerostomia, dry mouth, hyposalivation AND NOT salivary dysfunction.
-
Q4.
Medication/drugs AND drooling/sialorrhea/hypersalivation/ptyalism/increased salivary flow rate AND NOT salivary dysfunction.
-
Q5.
Medication/drugs AND salivary glands/saliva/xerostomia/dry mouth/hyposalivation AND NOT salivary gland dysfunction, oral sensory complaints.
-
Q6.
Medication/drugs AND salivary glands/saliva/xerostomia/dry mouth/hyposalivation AND NOT salivary gland dysfunction/assessment.
-
Q7.
Medication/drugs AND drooling/sialorrhea/hypersalivation/ptyalism AND NOT salivary gland dysfunction/assessment.
2.3 Step 3: Literature Search
Our literature search was conducted, through June 2013, in the PubMed, Embase, and Web of Science databases based on our chosen keywords and subject headings where applicable and was not limited by publication date, publication type or language. In addition, group members were encouraged to submit articles of interest located through referral or hand searching. The search was completed by a hand search of the reference lists in the eligible papers. After duplicates were removed, 3867 records were retained for Step 4.
2.4 Step 4: Record Screening for Eligibility
Each of the 3867 records was screened independently by the reviewers, who were supervised by the consultants. Papers were either retained for further analysis or excluded because they lacked relevance to any of the research questions; 269 papers relevant to the aforementioned topics were retained.
2.5 Step 5: Paper Selection for Type of Study, Relevance, and Level of Evidence
This step started with calibration among the reviewers to ensure they applied similar standards in the performance of their reviews. Papers were then divided among the reviewers, who analyzed publication titles, abstracts, and the materials and methods sections for key parameters.
2.6 Medication General Inclusion and Exclusion Criteria
-
1.
Particular drugs for which MISGD has been reported were included.
-
2.
A group of drugs or a combination of two or more drugs without specifying the individual MISGD of each drug under the group or combination were excluded.
-
3.
Drugs reported to induce SGD or used in therapeutic aspects of SGD were excluded. Thus, parasympathomimetics (e.g., pilocarpine and cevimeline) and the anti-cholinesterases (e.g., physostigmine and neostigmine), which are used for stimulation of salivary flow in patients experiencing a dry mouth, were not included.
-
4.
Research drugs that were not yet marketed by the time of writing this manuscript, or that were subsequently removed from the market, were excluded.
Next, the retained articles were given scores based on the following assessments:
-
(1)
The degree of relevance: level A (study dedicated to MISGD or xerostomia) or level B (study dedicated to adverse effects of medications).
-
(2)
The strength of methodology provided in the paper: level 1 (typically meta-analyses, systematic reviews, and randomized controlled trials [RCTs]), level 2 (typically open-label trials, observational studies, animal studies, and epidemiological studies), or level 3 (typically narrative reviews and textbooks).
It should be noted that, in addition to the type of study (RCT, review, etc.), the quality of study design and performance were considered in assigning the level of evidence. Hence, articles were assigned scores in order of decreasing levels of evidence as follows: A1 > B1 > A2 > B2 > A3 > B3.
2.7 Step 6: In-Depth Analysis
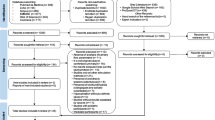
In-depth analysis was based on expert interpretation of the evidence. Supervised by the group head and consultants CD and JE, reviewer RJ screened the remaining 332 selected publications by reading the full text. Another 63 papers were excluded for reasons such as assessing MISGD and xerostomia as an outcome of minor importance, leaving 269 articles for in-depth analysis. Figure 1 depicts the steps of our work process and the distribution of the selected publications according to their score for level of evidence.

Adapted PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the paper-selection process
As a consequence of step 6, we derived three lists of medications:
-
1.
56 medications with strong evidence that were quoted in articles with scores A1 or B1.
-
2.
50 medications with moderate evidence that were quoted in articles with scores A2 or B2 but not A1 or B1.
-
3.
48 medications with weak evidence that were quoted in articles with scores not higher than A3 or B3.
3 Results
3.1 Anatomical Therapeutic Chemical (ATC) Classification of Drugs
The World Health Organization Collaborating Centre for Drug Statistics Methodology developed the Anatomical Therapeutic Chemical (ATC) classification system with defined daily doses (DDDs) as a system to classify therapeutic drugs. This system, which we also used, divides drugs into five different groups according to the organ or system on which they act and their chemical, pharmacological, and therapeutic properties. The first level contains 14 main groups according to anatomical site of action, with therapeutic subgroups (second level). The third and fourth levels are pharmacological and chemical subgroups, respectively, and the fifth level is the chemical compound itself.
We found that nine of the 14 groups in the first level contained medications reported with a strong or moderate level of evidence to be associated with SGD, xerostomia, or subjective sialorrhea: alimentary tract and metabolism, cardiovascular system, genitourinary system and sex hormones, anti-infectives for systemic use, anti-neoplastic and immunomodulating agents, musculoskeletal system, nervous system, respiratory system, and sensory organs. Among the 94 subgroups under the second level, 26 contain agents were reported to be associated with SGD, with 22 having strong evidence, namely drugs for functional gastrointestinal disorders, anti-emetics and anti-nauseants, anti-obesity preparations, anti-hypertensives, diuretics, beta-blocking agents, calcium channel blockers, urologicals, anti-neoplastic agents, muscle relaxants, drugs for the treatment of bone diseases, analgesics, anti-epileptics, anti-Parkinson drugs, psycholeptics, psychoanaleptics, other nervous system drugs, anti-muscarinic drugs for obstructive airway diseases, anti-histamines for systemic use, and ophthalmologicals. The third level is not included in Table 1 since it would add very little information. For the fourth level and its 882 subgroups described in the ATC/DDD system, 64 medication classes were found to be associated with SGD, and in 37 of these subgroups the association of SGD with the medications had stronger evidence. At the fifth level, 106 substances of the 4679 specified in the system were reported with a strong or moderate level of evidence to be associated with SGD. Of those, 56 drugs had a higher level of evidence of association with SGD (see Table 2).
3.2 Medications with Strong Evidence
Fifty-six medications had strong evidence of interference with salivary gland function. These medications could be categorized into the following eight of the ten anatomical main groups (first level in the ATC system): alimentary tract and metabolism (A), cardiovascular system (C), genitourinary system and sex hormones (G), anti-neoplastic and immunomodulating agents (L), musculoskeletal system (M), nervous system (N), respiratory system (R), and sensory organs (S). More than half (36) belong to the ATC main category of nervous system, and the most cited in the literature are oxybutynin (21 papers), tolterodine (19), duloxetine (19), quetiapine (14), bupropion (12), olanzapine (11), solifenacin (11), clozapine (9), fluoxetine (9), and venlafaxine (8). Oxybutynin, tolterodine, and solifenacin are urologicals, while the remainder act on the nervous system. All medications on this list except alendronate, bendroflumethiazide, and clonidine have been reported to cause xerostomia, whereas SGH has been verified (via measurement of salivary flow rate) for alendronate, amitriptyline, atropine, bendroflumethiazide, clonidine, fluoxetine, furosemide, oxybutynin, paroxetine, propiverine, propiverine, scopolamine, sertraline, solifenacin, and tolterodine. Sialorrhea was found to be an adverse effect of clozapine, olanzapine, and venlafaxine, as objectively assessed excess salivation, and of quetiapine and risperidone, as a symptom. Animal experiments offer an explanation for the dual action (oral dryness and sialorrhea) of clozapine [63, 120]. Dysgeusia was reported after administration of amitriptyline, bevacizumab, buprenorphine, fluoxetine loxapine, quetiapine, and sertraline; dental caries were associated with chlorpromazine and lithium; oral candidiasis was associated with olanzapine; and burning mouth sensation was associated with amitriptyline (not in Table 2). The properties of the various drugs listed in column 3 of Tables 2 and 3 were primarily derived from the textbook Goodman and Gilman’s The Pharmacological Basis of Therapeutics [202].
3.3 Medications with Moderate Evidence
Fifty medications had a moderate level of evidence of effects on salivary glands. These medications belonged to the following seven of the ten main anatomical groups (first level according to the ATC classification system): alimentary tract and metabolism, cardiovascular system, genitourinary system and sex hormones, anti-infectives for systemic use, nervous system, and respiratory system. Medications under the ATC category ‘nervous system’ were also the most commonly quoted medications in Table 3. Xerostomia is an adverse effect of all the drugs listed in Table 3 except clobazam, whereas SGH was reported with darifenacin and metoprolol. Enalapril, haloperidol, and methyldopa were reported to cause a subjective feeling of sialorrhea. Objective sialorrhea was reported only with clobazam. Three medications (azelastine, enalapril, and fluvoxamine) were reportedly associated with dysgeusia, and one (haloperidol) was associated with dental caries (not in Table 3).
3.4 Medications with Weak Evidence
In total, 48 medications were reported to cause a range of adverse oral effects, such as xerostomia, SGH, sialorrhea, burning mouth sensation, dysgeusia, and dental caries (Table 4).
4 Discussion
Saliva plays a crucial role in maintaining the health and functioning of the mouth. Its functions include (1) maintaining a moist oral mucosa, (2) mucinous content acting as a lubricant in the mouth and oesophagus, (3) taste recognition by acting as a medium for suspension of tastants, (4) digestion of starches with the help of amylase, (5) acid buffering in the mouth and oesophagus mainly by bicarbonate, (6) protection of teeth from acids by being supersaturated with respect to tooth mineral and by contributing to the acquired enamel pellicle, (7) modulation of the oral microbiota with the help of anti-bacterial, anti-viral, and anti-fungal components, and (8) facilitating wound healing in the oral cavity [272]. Medications may act on the central nervous system and/or at the neuroglandular junction, explaining the pathogenesis of MISDG. The secretory cells are supplied with muscarinic M1 and M3 receptors, α1- and β1-adrenergic receptors, and certain peptidergic receptors that are involved in the initiation of salivary secretion [273]. It is therefore understandable that drugs that have antagonistic actions on the autonomic receptors but that are used to treat dysfunctions in the various effectors of the autonomic nervous system may also affect the functions of salivary glands and thus cause oral dryness. However, in some cases, the cause of oral dryness is not as evident, as with the bisphosphonate alendronate that was reported to reduce the unstimulated secretion of saliva [13].
The anti-muscarinic drugs are well-known inducers of oral dryness as they prevent parasympathetic (cholinergic) innervation from activating the secretory cells. Surprisingly, clinical studies directly focusing on the secretion of saliva and the flagship of the anti-muscarinics, atropine, seem few. This is in contrast to numerous studies on animals, starting with the observations of the pioneers of salivary physiology in the 1870s.
The number of patients adversely affected by a specific drug, as well as the severity of the effect of this drug, are usually dose dependent. Figures for these parameters are not presented in the current study. Lack of saliva is often manifested as the sensation of dry mouth (xerostomia). A number of studies have suggested an association between the incidence of xerostomia and the number and dose of medications [274]. That study also discussed secondary effects of MISGD in promoting caries or oral mucosal alterations.
Management of MISGD has mainly been based on a trial-and-error approach. Use of intraoral topical agents, such as a spray containing malic acid, sugar-free chewing gums or candy, saliva substitutes, or non-alcoholic mouthwashes to moisten or lubricate the mouth have served as the mainstay of treatment for patients with a dry mouth. Parasympathomimetic agents with potent muscarinic-stimulating properties, such as pilocarpine and cevimeline, and anti-cholinesterases, which reduce the rate of acetylcholine metabolism, have been used as systemic sialogogues. Although they increase salivation significantly, the adverse effect profile of these drugs upon systemic administration restricts their use in patients with MISGD. A local application of these categories of drugs onto the oral epithelium, with the aim of activating the underlying minor glands, may be an alternative approach. It is also necessary to ensure salivary gland functionality before administering these medications. Newer management methods include electrostimulation. Other management options for MISGD include possibly reducing the number of medications or the dosage or replacing them with medications or formulations with fewer xerogenic effects. Little evidence is available on this important topic; however, when dental treatment is needed, close communication between the dentist (who has to deal with the adverse effects) and the prescribing physician is warranted to obtain the best outcome for the patient [275].
The present paper tries to fill the lacunae in regard to evidence-based listing of the effects of medications on salivary function as found in the current scientific literature. We conducted an extensive search of the literature related to MISGD, followed by meticulous scrutiny and analysis of the articles. However, it is still possible that a few medications were missed, and the lists in Tables 2 and 3 may not be exhaustive. Grading the evidence and relevance of each scientific article was a major issue. Consequently, the number of medications with strong or moderate evidence of being associated with SGD and xerostomia in our lists is much smaller than in other lists [1–6, 9]. Moreover, some studies may have recorded salivary disorders only in an adverse effect table, and these would have been missed by our search. An additional issue is that our study does not include preparations containing more than one agent. However, any medication included in a mixed medication in these lists may have the potential to influence the salivary effects of the overall preparation. A further matter that warrants consideration is the possibility that certain drugs, while not exerting xerogenic effect when taken individually (and therefore not appearing in these lists), may do so as a result of drug–drug interaction if consumed together in a polypharmacy context [7, 8]. It should also be noted that, for some medications not included in this review because peer-reviewed publications on their salivary side effects were lacking, such side effects could have been mentioned on their monographs according to their manufacturer’s controlled clinical trial. Finally, this article does not report the potency and frequency of salivary effects of the medications, as these data were rarely available.
The study suggests that medications acting on almost all systems of the body may also cause side effects related to the salivary system. At higher levels of the classification tree, the analysis seems to yield more specific details of the medications and their modes of action leading to SGD and xerostomia. Hence, the selection of an alternate drug with a similar effect on the desired system but fewer adverse salivary effects may be attempted based on this list. However, the possibility exists that other drugs that belong to the same level, especially at the fourth level of the ATC/DDD classification, may have a similar effect on salivary glands as the drug to be replaced.
Very few studies used objective measurements of salivary flow rates in the context of a medication adverse effect [7, 8, 13, 48]. Further, few articles seem to have correlated the results of such objective measurements with the subjective feelings of the patients receiving these drugs. Though animal studies have established a reduced salivary flow rate as an effect of medications, the subjective feeling of dryness (xerostomia) obviously cannot be registered in animals; hence, the relationship between changes in salivary flow rate and subjective feelings of dryness/drooling has been ambiguous [104, 120, 138–140, 148].
It has been reported that xerostomia in healthy subjects is not experienced until the unstimulated flow rate of whole saliva has been reduced to 40–50% of normal [27]. Furthermore, whether changes in the composition of the salivary secretion can also affect the subjective feelings of the patient remains to be clarified. However, the main difficulty encountered was the rarity of studies in which salivary flow rate or composition was actually measured before and after patients were prescribed medication. Moreover, baseline data were available for virtually no patients regarding their unstimulated saliva flow rates before they require medications. It seems to be only in Sweden that dental students are taught to measure the salivary flow rates of their patients to provide baseline values for any subsequent salivary problems that may develop. We suggest this is a valuable approach that should also be introduced in other countries.
Medications were also reported to cause other oral adverse effects. Aliko et al. [274] point out that although independent reports relate a burning sensation of the oral mucosa and/or dysgeusia with MISGD, the relationship has not been established objectively. A few articles (albeit of moderate or weak level of evidence) mention that candidiasis and dental caries are associated with the use of certain drugs. None of these studies has tested the relationship between the pharmacokinetics of the drug, its effect on salivary glands, and other oral adverse effects reported [274]. Dawes et al. [272] reported that constituents of saliva have anti-fungal, anti-viral, and anti-bacterial properties, which indicates the role of saliva in controlling the oral microbiota and correlates SGH with occurrence of oral candidiasis. The relationship between SGH, dental caries, and oral candidiasis is well known and established. However, the same has not been tested in the context of MISGD in the current literature.
The present paper may help clinicians and researchers consider whether the medications they prescribe or investigate may lead to SGD or xerostomia. A few scenarios follow:
-
(a)
A clinician needs to evaluate which drugs from the medication list of his/her patient have potential adverse salivary effects. The clinician may take the following steps:
-
(i)
Search in Tables 2 and 3 for the medications by alphabetical order.
-
(ii)
If the medications are not found, there is probably no published evidence for a salivary adverse effect.
-
(iii)
If found and they wish to know more about the medication type, they can search Table 1 using the ATC code(s) found in column 2 of Tables 2 and 3. These codes are in the last column of Table 1 in alphabetical and numerical order.
-
(i)
-
(b)
Before prescribing a medication, a clinician wishes to assess its potential salivary adverse effects. The above decision tree is also recommended in this situation.
-
(c)
A treated patient complains of salivary symptoms but the clinician cannot find any of the medications in Tables 2 or Table 3. However, it is plausible that additional medications not included in these tables could also affect salivary glands if they belong to the same ATC category at any level. For example, the anti-obesity medications fenfluramine, amfepramone, mazindol, etilamfetamine, cathine, clobenzorex, mefenorex, and lorcaserin are all ‘centrally acting anti-obesity products’, ATC A08AA [276], and may act similarly to dexfenfluramine, which belongs to the same category and appears in Table 3. Such an association may provide an explanation for the patient’s symptoms.
-
(d)
A clinician needs to prescribe medication to a patient with Sjögren’s syndrome or who has undergone radiotherapy to the head and neck area and wishes to avoid worsening the patient’s xerostomia. If, for example, the required drug is a muscle relaxant, the clinician may search the ATC website [277] under ‘muscle relaxants’ and then double check the subgroups and Table 1. There, they will find that ‘other centrally acting agents’ may have salivary effects and thus choose a medication belonging to any of the other subgroups.
-
(e)
A researcher wishes to know whether a certain type of medication has salivary effects and at what level of evidence.
-
(i)
The researcher may start searching Table 1 for the type of medication according to the anatomical site of action (first level), therapeutic effect (second level), chemical characteristic (fourth level), or generic name (fifth level).
-
(ii)
If no relevant category is found, there is probably no published evidence for adverse salivary effects of this drug type.
-
(iii)
If the drug type is found at any of the levels in bold text, one of the drugs at the fifth level belonging to the category may be searched for in Table 2, where the medications are in alphabetical order and information is available, i.e., type and number of publications and references.
-
(iv)
If the drug type is found but not in bold text, the researcher may proceed as in (iii) above but in Table 3 instead of Table 2.
-
(i)
5 Conclusions
Most investigators relied on the subjective opinion of the individuals or patients about whether they had too little or an excessive secretion of saliva. Thus, we conclude that further RCTs that include saliva collection are warranted for the assessment of potential salivary effects of many medications. Unstimulated and stimulated salivary flow rates should be measured before and at intervals after starting the drug. In addition, a record of changes in the patients’ subjective feelings over time should also be kept. Ideally, studies should also aim to assess changes in salivary composition, since these may also relate to SGD.
References
Smith RG, Burtner AP. Oral side-effects of the most frequently prescribed drugs. Spec Care Dentist. 1994;14:96–102.
Sreebny LM, Schwartz SS. A reference guide to drugs and dry mouth. Gerodontology. 1997;14:33–7.
Sreebny LM. The causes of dry mouth: a broad panoply. In: Sreebny LM, Vissink A, editors. Dry mouth, the malevolent symptom: a clinical guide. Ames: Wiley-Blackwell; 2010. p. 103–22.
Wolff A, Stahl B. Reference guide to xerogenic drugs in Israel. J Isr Dent Assoc. 1999;16:51–76.
Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9:165–76.
Scully C, Bagan-Sebastian JV. Adverse drug reactions in the orofacial region. Crit Rev Oral Biol Med. 2004;15:221–40.
Smidt D, Torpet LA, Nauntofte B, Heegaard KM, Pedersen AM. Associations between oral and ocular dryness, labial and whole salivary flow rates, systemic diseases and medications in a sample of older people. Community Dent Oral Epidemiol. 2011;39:276–88.
Smidt D, Torpet LA, Nauntofte B, Heegaard KM, Pedersen AM. Associations between labial and whole salivary flow rates, systemic diseases and medications in a sample of older people. Community Dent Oral Epidemiol. 2010;38:422–35.
Nguyen CT, MacEntee MI, Mintzes B, Perry TL. Information for physicians and pharmacists about drugs that might cause dry mouth: a study of monographs and published literature. Drugs Aging. 2014;31:55–65.
Lynge Pedersen AM, Nauntofte B, Smidt D, Torpet LA. Oral mucosal lesions in older people: relation to salivary secretion, systemic diseases and medications. Oral Dis. 2015;21:721–9.
Baccaglini I, Brennan MT, Lockhart PB, Patton LL. World Workshop on Oral Medicine IV. Process and methodology for systematic review and developing management recommendations. Reference manual for management recommendations writing committees. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(Suppl S3);e1–19.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151:264–9.
Eviö S, Tarkkila L, Sorsa T, Furuholm J, Välimäki MJ, Ylikorkala O, et al. Effects of alendronate and hormone replacement therapy, alone and in combination, on saliva, periodontal conditions and gingival crevicular fluid matrix metalloproteinase-8 levels in women with osteoporosis. Oral Dis. 2006;12:187–93.
Narhi TO, Meurman JH, Ainamo A. Xerostomia and hyposalivation: causes, consequences and treatment in the elderly. Drugs Aging. 1999;15:103–16.
Pawar PS, Woo DA. Extrapyramidal symptoms with concomitant use of amitriptyline and amiodarone in an elderly patient. Am J Geriatr Pharmacother. 2010;8:595–8.
Rani PU, Naidu MU, Prasad VB, Rao TR, Shobha JC. An evaluation of antidepressants in rheumatic pain conditions. Anesth Analg. 1996;83:371–5.
Sauer H, Huppertz-Helmhold S, Dierkes W. Efficacy and safety of venlafaxine ER vs. amitriptyline ER in patients with major depression of moderate severity. Pharmacopsychiatry. 2003;36:169–75.
Montgomery SA. Safety of mirtazapine: a review. Int Clin Psychopharmacol. 1995;10(Suppl 4):37–45.
Nagata E. Antidepressants in migraine prophylaxis. Brain Nerve. 2009;61:1131–4.
Jain T, Bhandari A, Ram V, et al. Drug interactions and adverse drug reactions in hospitalized psychiatric patients: a critical element in providing safe medication use. German J Psychiatry. 2011;14:26–34.
Biederman J, Mick E, Spencer T, Doyle R, Hoshi G, Hammerness R, et al. An open-label trial of aripiprazole monotherapy in children and adolescents with bipolar disorder. CNS Spectr. 2007;12:683–9.
Fountoulakis KN, Vieta E. Efficacy and safety of aripiprazole in the treatment of bipolar disorder: a systematic review. Ann Gen Psychiatry. 2009;8:16–30.
Tramontina S, Zeni CP, Pheula GF, Pheula GF, Narvaez J, Rohde LA. Aripiprazole in juvenile bipolar disorder comorbid with attention-deficit/hyperactivity disorder: an open clinical trial. CNS Spectr. 2007;2:758–62.
Veselinovic T, Schorn H, Vernaleken I, Hiemke C, Zernig G, Gur R, et al. Effects of antipsychotic treatment on psychopathology and motor symptoms. A placebo-controlled study in healthy volunteers. Psychopharmacol. 2011;218:733–48.
Hewer RD, Jones PM, Thomas PS, McKenzie DK. A prospective study of atropine premedication in flexible bronchoscopy. Aust N Z J Med. 2000;30:466–9.
Diamond JP. Systemic adverse effects of topical ophthalmic agents. Implications for older patients. Drugs Aging. 1997;11:352–60.
Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66(Spec Iss):648–53.
Chou R, Peterson K, Helfand M. Comparative efficacy and safety of skeletal muscle relaxants for spasticity and musculoskeletal conditions: a systematic review. J Pain Symptom Manag. 2004;28:140–75.
Nederfors T, Nauntofte B, Twetman S. Effects of furosemide and bendroflumethiazide on saliva flow rate and composition. Arch Oral Biol. 2004;49:507–13.
Fang P, Hu JH, Cheng ZG, Liu ZF, Wang JL, Jiao SC. Efficacy and safety of bevacizumab for the treatment of advanced hepatocellular carcinoma: a systematic review of phase II trials. PLoS One. 2012;7:e49717.
Walters TR. Development and use of brimonidine in treating acute and chronic elevations of intraocular pressure: a review of safety, efficacy, dose response, and dosing studies. Surv Ophthalmol. 1996;41(Suppl 1):S19–26.
Schuman JS, Horwitz B, Choplin NT, David R, Albracht D, Chen K. A, 1-year study of brimonidine twice daily in glaucoma and ocular hypertension. A controlled, randomized, multicenter clinical trial. Chronic Brimonidine Study Group. Arch Ophthalmol. 1997;115:847–52.
Gordon A, Callaghan D, Spink D, Cloutier C, Dzongowski P, O’Mahoney W. Buprenorphine transdermal system in adults with chronic low back pain: a randomized, double-blind, placebo-controlled crossover study, followed by an open-label extension phase. Clin Ther. 2010;32:844–60.
Cipriani A, Santilli C, Furukawa TA, Signoretti A, Nakagawa A, McGuire H, et al. Escitalopram versus other antidepressive agents for depression. Cochrane Database Syst Rev. 2009;(2): CD006532.
Graham J, Coghill D. Adverse drug reactions in hospital in-patients: a pilot study. CNS Drugs. 2008;22:213–37.
Hewett K, Chrzanowski W, Schmitz M, Milanova V, Gee M, Krishen A, et al. Eight-week, placebo-controlled, double-blind comparison of the antidepressant efficacy and tolerability of bupropion XR and venlafaxine XR. J Psychopharmacol. 2009;23:531–8.
Jafarinia M, Mohammadi MR, Modabbernia A, Ashrafi M, Khajavi D, Tabrizi M, et al. Bupropion versus methylphenidate in the treatment of children with attention-deficit/hyperactivity disorder: randomized double-blind study. Hum Psychopharmacol. 2012;27:411–8.
Greenway FL, Fujioka K, Plodkowski RA, Mudaliar S, Guttadauria M, Erickson J. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376:595–605.
James WA, Lippmann S. Bupropion: overview and prescribing guidelines in depression. S Med J. 1991;84:222–4.
Semenchuk MR, Sherman S, Davis B. Double-blind, randomized trial of bupropion SR for the treatment of neuropathic pain. Neurol. 2001;57:1583–8.
Weihs KL, Settle EC Jr, Batey SR, Houser TL, Donahue RM, Ascher JA. Bupropion sustained release versus paroxetine for the treatment of depression in the elderly. J Clin Psychiatry. 2000;61:196–202.
Zwar N, Richmond R. Bupropion sustained release. A therapeutic review of Zyban. Aust Fam Physician. 2002;31:443–7.
Andrews JM, Nemeroff CB. Contemporary management of depression. Am J Med. 1994;97:(6A)24S–32S.
Muller F, Wehbe L. Smoking and smoking cessation in Latin America: a review of the current situation and available treatments. Int J COPD. 2008;3:285–93.
Kalman D, Herz L, Monti P, Kahler CW, Mooney M, Rodrigues S, et al. Incremental efficacy of adding bupropion to the nicotine patch for smoking cessation in smokers with a recent history of alcohol dependence: results from a randomized, double-blind, placebo-controlled study. Drug Alcohol Depend. 2011;118:111–8.
Wang F, Shen X, Liu Y, Xu S, Guo X. Continuous infusion of butorphanol combined with intravenous morphine patient-controlled analgesia after total abdominal hysterectomy: a randomized, double-blind controlled trial. Eur J Anaesthesiol. 2009;26:28–34.
Adams CE, Rathbone J, Thornley B, Clarke M, Borrill J, Wahlbeck K, et al. Chlorpromazine for schizophrenia: a Cochrane systematic review of 50 years of randomised controlled trials. BMC Med. 2005;3:15.
de Almeida Pdel V, Gregio AM, Brancher JA, de Lima AA, Azevedo LR. Effects of antidepressants and benzodiazepines on stimulated salivary flow rate and biochemistry composition of the saliva. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:58–65.
Hellerstein DJ, Batchelder S, Miozzo R, Kreditor D, Hyler S, Gangure D. Citalopram in the treatment of dysthymic disorder. Int Clin Psychopharmacol. 2004;19:143–8.
Webster J, Koch HF. Aspects of tolerability of centrally acting antihypertensive drugs. J Cardiovasc Pharmacol. 1996;27(Suppl 3):S49–54.
Geyer O, Schmidt KG, Pianka P, Neudorfer M, Lazar M. Clonidine provides an allergy-free alternative in glaucoma patients with proven allergy to apraclonidine. Graefes Arch Clin Exp Ophthalmol. 2000;238:149–52.
Villaseca P. Non-estrogen conventional and phytochemical treatments for vasomotor symptoms: what needs to be known for practice? Climacteric. 2012;15:115–24.
van Zwieten PA. Centrally acting antihypertensives: a renaissance of interest. Mechanisms and haemodynamics. J Hypertens Suppl. 1997;15:S3–8.
Plänitz V. Crossover comparison of moxonidine and clonidine in mild to moderate hypertension. Eur J Clin Pharmacol. 1984;27:147–52.
Essali A, Al-Haj Haasan N, Li C, Rathbone J. Clozapine versus typical neuroleptic medication for schizophrenia. Cochrane Database Syst Rev. 2009;(1):CD000059.
Tollefson GD, Birkett MA, Kiesler GM, Wood AJ. Double-blind comparison of olanzapine versus clozapine in schizophrenic patients clinically eligible for treatment with clozapine. Biol Psychiatry. 2001;49:52–63.
Ekström J, Godoy T, Riva A. Clozapine: agonistic and antagonistic salivary secretory actions. J Dent Res. 2010;89:276–80.
Soler Roibal MA, Oca Bravo L, Montejo Iglesias LM. The clozapine-induced hypersalivation and its treatment. Actas Esp Psiquiatr. 1999;27:408–11.
Immadisetty V, Agrawal P. A successful treatment strategy for clozapine-induced parotid swelling: a clinical case and systematic review. Therap Adv Psychopharmacol. 2012;2:235–9.
Bennett JP Jr, Landow ER, Schuh LA. Suppression of dyskinesias in advanced Parkinson’s disease. II. Increasing daily clozapine doses suppress dyskinesias and improve Parkinsonism symptoms. Neurology. 1993;43:1551–5.
Ekström J, Khosravani N, Castagnola M, Messana I. Saliva and the control of its secretion. In: Ekberg O, editor. Dysphagia: diagnosis and treatment. Berlin: Springer-Verlag; 2012. p. 19–47.
Godoy T, Riva A, Ekström J. Clozapine-induced salivation: interaction with N-desmethylclozapine and amisulpride in an experimental rat model. Eur J Oral Sci. 2011;119:275–81.
Praharaj SK, Jana AK, Goswami K, Das PR, Goyal N, Sinha VK. Salivary flow rate in patients with schizophrenia on clozapine. Oral Dis. 2012;18:680–91.
Darwish M, Hellriegel ET. Steady-state pharmacokinetics of once-daily cyclobenzaprine extended release: a randomized, double-blind, 2-period crossover study in healthy volunteers. Clin Ther. 2011;33:746–53.
Moldofsky H, Harris HW, Archambault WT, Kwong T, Lederman S. Effects of bedtime very low dose cyclobenzaprine on symptoms and sleep physiology in patients with fibromyalgia syndrome: a double-blind randomized placebo-controlled study. J Rheumatol. 2011;38:2653–63.
Weil AJ, Ruoff GE, Nalamachu S, Altman CA, Xie F, Taylor DR. Efficacy and tolerability of cyclobenzaprine extended release for acute muscle spasm: a pooled analysis. Postgrad Med. 2010;122:158–69.
Lower EE, Fleishman S, Cooper A, Zeldis J, Faleck H, Yu Z, et al. Efficacy of dexmethylphenidate for the treatment of fatigue after cancer chemotherapy: a randomized clinical trial. J Pain Symptom Manage. 2009;38:650–62.
Doody RS, Gavrilova SI, Sano M, Thomas RG, Aisen PS, Bachurin SO, et al. Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer’s disease: a randomised, double-blind, placebo-controlled study. Lancet. 2008;372:207–15.
Koren G, Clark S, Hankins GDV, Caritis SN, Miodovnik M, Umans JG, et al. Effectiveness of delayed-release doxylamine and pyridoxine for nausea and vomiting of pregnancy: a randomized placebo controlled trial. Am J Obstet Gynecol. 2010;203:571.e571–571.e577.
Gahimer J, Wernicke J, Yalcin I, Ossanna MJ, Wulster-Radcliffe M, Viktrup L. A retrospective pooled analysis of duloxetine safety in 23,983 subjects. Curr Med Res Opin. 2007;23:175–84.
Arnold LM, Clauw D, Wang F, Ahl J, Gaynor PJ, Wohlreich MM. Flexible dosed duloxetine in the treatment of fibromyalgia: a randomized, double-blind, placebo-controlled trial. J Rheumatol. 2010;37:2578–86.
Arnold LM, Zhang S, Pangallo BA. Efficacy and safety of duloxetine 30 mg/d in patients with fibromyalgia: a randomized, double-blind, placebo-controlled study. Clin J Pain. 2012;28:775–81.
Carter NJ, McCormack PL. Duloxetine: a review of its use in the treatment of generalized anxiety disorder. CNS Drugs. 2009;23:523–41.
Frampton JE, Plosker GL. Duloxetine: a review of its use in the treatment of major depressive disorder. CNS Drugs. 2007;21:581–609.
Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Int Clin Psychopharmacol. 2012;27:215–23.
Norman TR, Olver JS. Duloxetine in the treatment of generalized anxiety disorder. Neuropsychiatric Dis Treat. 2008;4:1169–80.
Ormseth MJ, Scholz BA, Boomershine CS. Duloxetine in the management of diabetic peripheral neuropathic pain. Patient Prefer Adherence. 2011;5:343–56.
Perahia DGS, Kajdasz DK, Royer MG, Raskin J, Tylee A. Duloxetine in the treatment of major depressive disorder: an assessment of the relationship between outcomes and episode characteristics. Int Clin Psychopharmacol. 2006;21:285–95.
Stewart DE, Wohlreich MM, Mallinckrodt CH, Watkin JG, Kornstein SG. Duloxetine in the treatment of major depressive disorder: comparisons of safety and tolerability in male and female patients. J Affect Disord. 2006;94:183–9.
Wright A, VanDenBerg C. Duloxetine in the treatment of generalized anxiety disorder. Int J Gen Med. 2009;2:153–62.
Ball SG, Desaiah D, Zhang Q, Thase ME, Perahia DG. Efficacy and safety of duloxetine 60 mg once daily in major depressive disorder: a review with expert commentary. Drugs Context. 2013;212245.
Detke MJ, Lu Y, Goldstein DJ, McNamara RK, Demitrack MA. Duloxetine, 60 mg once daily, for major depressive disorder: a randomized double-blind placebo-controlled trial. J Clin Psychiatry. 2002;63:308–15.
Michel MC, Oelke M. Duloxetine in the treatment of stress urinary incontinence. Womens Health (Lond). 2005;1:345–58.
Pigott TA, Prakash A, Arnold LM, Aaronson ST, Mallinckrodt CH, Wohlreich MM. Duloxetine versus escitalopram and placebo: an 8-month, double-blind trial in patients with major depressive disorder. Curr Med Res Opin. 2007;23:1303–18.
Serretti A, Chiesa A, Calati R, Perna G, Bellodi L, De Ronchi D. Novel antidepressants and panic disorder: evidence beyond current guidelines. Neuropsychobiol. 2010;63:1–7.
Smith HS, Bracken D, Smith JM. Pharmacotherapy for fibromyalgia. Front Pharmacol. 2011;2:17.
Frakes EP, Risser RC, Ball TD, Hochberg MC, Wohlreich MM. Duloxetine added to oral nonsteroidal anti-inflammatory drugs for treatment of knee pain due to osteoarthritis: results of a randomized, double-blind, placebo-controlled trial. Curr Med Res Opin. 2011;27:2361–72.
Guerdjikova AI, McElroy SL, Kotwal R, Welge JA, Nelson E, Lake K. High-dose escitalopram in the treatment of binge-eating disorder with obesity: a placebo-controlled monotherapy trial. Hum Psychopharmacol. 2008;23:1–11.
Montgomery SA, Andersen HF. Escitalopram versus venlafaxine XR in the treatment of depression. Int Clin Psychopharmacol. 2006;21:297–309.
Bhat A, El Solh AA. Management of narcolepsy. Exp Opin Pharmacotherapy. 2008;9:1721–33.
Atkinson JH, Slater MA, Capparelli EV, Wallace MS, Zisook S, Abranson I, et al. Efficacy of noradrenergic and serotonergic antidepressants in chronic back pain: a preliminary concentration-controlled trial. J Clin Psychopharmacol. 2007;27:135–42.
Baker B, Dorian P, Sandor P, Shapiro C, Schell C, Mitchell J, et al. Electrocardiographic effects of fluoxetine and doxepin in patients with major depressive disorder. J Clin Psychopharmacol. 1997;17:15–21.
Newhouse PA, Krishnan KRR, Doraiswamy PM, Richter EM, Batzar ED, Clary CM. A double-blind comparison of sertraline and fluoxetine in depressed elderly outpatients. J Clin Psychiatry. 2000;61:559–68.
Steiner M, Steinberg S, Stewart D, Carter D, Berger C, Reid R, et al. Fluoxetine in the treatment of premenstrual dysphoria. N Engl J Med. 1995;332:1529–34.
Kendirci M, Salem E, Hellstrom WJG. Dapoxetine, a novel selective serotonin transport inhibitor for the treatment of premature ejaculation. Ther Clin Risk Manag. 2007;3:277–89.
Atkinson JC, Shiroky JB, Macynski A, Fox PC. Effects of furosemide on the oral cavity. Gerodontology. 1989;8:23–6.
Gilron I, Bailey JM, Tu D, Holden RR, Jackson AC, Houlden RL. Nortriptyline and gabapentin, alone and in combination for neuropathic pain: a double-blind, randomised controlled crossover trial. Lancet. 2009;374:1252–61.
Homma Y, Yamaguchi O. A randomized, double-blind, placebo- and propiverine-controlled trial of the novel antimuscarinic agent imidafenacin in Japanese patients with overactive bladder. Int J Urol. 2009;16:499–506.
Kasper S, Moller HJ, Montgomery SA, Zondag E. Antidepressant efficacy in relation to item analysis and severity of depression: a placebo-controlled trial of fluvoxamine versus imipramine. Int Clin Psychopharmacol. 1995;9(Suppl 4):3–12.
Billiard M. Narcolepsy: current treatment options and future approaches. Neuropsych Dis Treatment. 2008;4:557–66.
Brown TE, Brams M, Gao J, Gasior M, Childress A. Open-label administration of lisdexamfetamine dimesylate improves executive function impairments and symptoms of attention-deficit/hyperactivity disorder in adults. Postgrad Med. 2010;122:7–17.
Wigal T, Brams M, Gasior M, Gao J, Giblin J. Effect size of lisdexamfetamine dimesylate in adults with attention-deficit/hyperactivity disorder. Postgrad Med. 2011;123:169–75.
Bowden CL, Grunze H, Mullen J, Brecher M, Paulsson B, Jones M, et al. A randomized, double-blind, placebo-controlled efficacy and safety study of quetiapine or lithium as monotherapy for mania in bipolar disorder. J Clin Psychiatry. 2005;66:111–21.
O’Connell AC, Bowen WH. Composition and flow rate of saliva and caries development in young rats following administration of lithium. Caries Res. 1994;28:342–7.
Donaldson SR. Sialorrhea as a side effect of lithium: a case report. Am J Psychiatry. 1982;138:1350–1.
Young AH, McElroy SL, Bauer M, Philips N, Chang W, Olausson B, et al. A double-blind, placebo-controlled of quetiapine and lithium monotherapy in adults in the acute phase of bipolar depression (EMBOLDEN 1). J Clin Psychiatry. 2010;71:150–62.
Allen MH, Feifel D, Lesem MD, Zimbroff DL, Ross R, Munzar P, et al. Efficacy and safety of loxapine for inhalation in the treatment of agitation in patients with schizophrenia: a randomized, double-blind, placebo-controlled trial. J Clin Psychiat. 2011;72:1313–21.
Blader JC, Pliszka SR, Jensen PS, Schooler NR, Kafantaris V. Stimulant-responsive and stimulant-refractory aggressive behavior among children with ADHD. Pediatrics. 2010;126:e796–806.
Devos D, Krystkowiak P, Clement F, Dujardin A, Cottencin O, Waucquier N, et al. Improvement of gait by chronic, high doses of methylphenidate in patients with advanced Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2007;78:470–5.
Lasheen W, Walsh D, Mahmoud F, Davis MP, Rivera N, Khoshknabi DS. Methylphenidate side effects in advanced cancer: a retrospective analysis. Am J Hosp Palliat Care. 2010;27:16–23.
Biederman J, Mick E, Surman C, Doyle R, Hammerness P, Harpold T, et al. A randomized, placebo-controlled trial of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder. Biol Psychiatry. 2006;59:829–35.
Volz HP, Gleiter CH. Monoamine oxidase inhibitors. A perspective on their use in the elderly. Drugs Aging. 1998;13:341–55.
Johnsen E, Jorgensen HA. Effectiveness of second generation antipsychotics: a systematic review of randomized trials. BMC Psychiatry. 2008;8:1–14.
Kumar A, Gupta M, Jiloha RC, Tekur U. Efficacy of olanzapine and sodium valproate given alone or as add-on therapy in acute mania. A comparative study. Methods Find Exp Clin Pharmacol. 2010;32:319–24.
McIntyre RS, Cohen M, Zhao J, Alphs L, Macek TA, Panagides J. Asenapine versus olanzapine in acute mania: a double-blind extension study. Bipolar Disord. 2009;11:815–26.
Bridle C, Palmer S, Bagnall AM, Darba J, Duffy S, Sculpher M, et al. A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder. Health Technol Assess. 2004;8:iii–iv,1–187.
Budman CL, Gayer A, Lesser M, Shi Q, Bruun RD. An open-label study of the treatment efficacy of olanzapine for Tourette’s disorder. J Clin Psychiatry. 2001;62:290–4.
Conley RR, Meltzer HY. Adverse events related to olanzapine. J Clin Psychiatry. 2000;61:6–30.
Fulton B, Goa KL. Olanzapine. A review of its properties and therapeutic efficacy in the management of schizophrenia and related psychoses. Drugs. 1997;53:281–98.
Godoy T, Riva A, Ekström J. Salivary secretion effects of the antipsychotic drug olanzapine in an animal model. Oral Dis. 2013;19:151–61.
Stauffer VL, Sniadecki JL, Piezer KW, Gatz J, Kollack-Walker S, Hoffmann VP, et al. Impact of race on efficacy and safety during treatment with olanzapine in schizophrenia, schizophreniform or schizoaffective disorder. BMC Psychiatry. 2010;10:89–99.
Barkin J, Corcos J, Radomski S, Jammal MP, Micelli PC, Reiz JL. A randomized, double-blind, parallel-group comparison of controlled- and immediate-release oxybutynin chloride in urge urinary incontinence. Clin Therapeutics. 2004;26:1026–36.
Aaron LE, Morris TJ, Jahshan P, Reiz JL. An evaluation of patient and physician satisfaction with controlled-release oxybutynin 15 mg as a one-step daily dose in elderly and non-elderly patients with overactive bladder: results of the STOP study. Curr Med Res Opin. 2012;28:1369–79.
Homma Y, Paick JS, Lee JG, Kawabe K. Clinical efficacy and tolerability of extended-release tolterodine and immediate-release oxybutynin in Japanese and Korean patients with an overactive bladder: a randomized, placebo-controlled trial. BJU Int. 2003;92:741–7.
Lucente VR, Staskin DR, De E. Development of oxybutynin chloride topical gel for overactive bladder. Open Access J Urol. 2011;3:35–42.
Staskin DR, Rosenberg MT, Dahl NV, Polishuk PV, Zinner NR. Effects of oxybutynin transdermal system on health-related quality of life and safety in men with overactive bladder and prostate conditions. Int J Clin Pract. 2008;62:27–38.
Madersbacher H, Halaska M, Voigt R, Alloussi S, Höfner K. A placebo-controlled, multicentre study comparing the tolerability and efficacy of propiverine and oxybutynin in patients with urgency and urge incontinence. BJU Int. 1999;84:646–51.
Garely AD, Burrows LJ. Current pharmacotherapeutic strategies for overactive bladder. Exp Opin Pharmacother. 2002;3:827–33.
Hay-Smith J, Herbison P, Ellis G, Moore K. Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev. 2002;(3):CD003781.
Kay GG, Staskin DR, MacDiarmid S, McIlwain M, Dahl NV. Cognitive effects of oxybutynin chloride topical gel in older healthy subjects: a 1-week, randomized, double-blind, placebo- and active-controlled study. Clin Drug Investig. 2012;32:707–14.
Lauti M, Herbison P, Hay-Smith J, Ellis G, Wilson D. Anticholinergic drugs, bladder retraining and their combination for urge urinary incontinence: a pilot randomised trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:1533–43.
MacDiarmid SA, Anderson RU, Armstrong RB, Dmochowski RR. Efficacy and safety of extended release oxybutynin for the treatment of urge incontinence: an analysis of data from 3 flexible dosing studies. J Urol. 2005;174(4 Pt 1):1301–5 (discussion 1305).
Nabi G, Cody JD, Ellis G, Herbison P, Hay-Smith J. Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev. 2006;(4):CD003781.
Hashim H, Abrams P. Drug treatment of overactive bladder: efficacy, cost and quality-of-life considerations. Drugs. 2004;64:1643–56.
Hegde SS, Eglen RM. Muscarinic receptor subtypes modulating smooth muscle contractility in the urinary bladder. Life Sci. 1999;64:419–28.
Michel MC. A benefit-risk assessment of extended-release oxybutynin. Drug Saf. 2002;25:867–76.
Abrams P, Andersson KE. Muscarinic receptor antagonists for overactive bladder. BJU Int. 2007;100:987–1006.
Naruganahalli KS, Sinha S, Hegde LG, Meru AV, Chugh A, Kumar N, et al. Comparative in vivo uroselectivity profiles of anticholinergics, tested in a novel anesthetized rabbit model. Eur J Pharmacol. 2007;572:207–12.
Oki T, Takeuchi C, Yamada S. Comparative evaluation of exocrine muscarinic receptor binding characteristics and inhibition of salivation of solifenacin in mice. Biol Pharm Bull. 2006;29:1397–400.
Sakaguchi M, Goto K, Ichiki H, Hattori N, Iizuka A, Yamamoto M, et al. Effects of Byakko-ka-ninjin-to on salivary secretion and bladder function in rats. J Ethnopharmacol. 2005;102:164–9.
Sathyan G, Chancellor MB, Gupta SK. Effect of OROS controlled-release delivery on the pharmacokinetics and pharmacodynamics of oxybutynin chloride. Br J Clin Pharmacol. 2001;52:409–17.
Armstrong RB, Luber KM, Peters KM. Comparison of dry mouth in women treated with extended-release formulations of oxybutynin or tolterodine for overactive bladder. Int Urol Nephrol. 2005;37:247–52.
Canuso CM, Turkoz I, Sheehan JJ, Bossie CA. Efficacy and safety of paliperidone extended-release in schizophrenia patients with prominent affective symptoms. J Affect Disord. 2010;120:193–9.
Vieta E, Nuamah IF, Lim P, Yuen EC, Palumbo JM, Hough DW, et al. A randomized, placebo- and active-controlled study of paliperidone extended release for the treatment of acute manic and mixed episodes of bipolar I disorder. Bipolar Disord. 2010;12:230–43.
Kodish I, Rockhill C, Varley C. Pharmacotherapy for anxiety disorders in children and adolescents. Dialogues Clin Neurosci. 2011;13:439–52.
Gadde KM, Allison DB, Ryan DH, Peterson CA, Troupin B, Schwiers ML, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377:1341–52.
Kim KK, Cho HJ, Kang HC, Youn BB, Lee KR. Effects on weight reduction and safety of short-term phentermine administration in Korean obese people. Yonsei Med J. 2006;47:614–25.
Allison DB, Gadde KM, Garvey WT, Peterson CA, Schwiers ML, Najarian T, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity (Silver Spring). 2012;20:330–42.
Scheepe JR, Braun PM, Junemann KP, Alken P. Effects of propiverine and its metabolite propiverine-N-oxide on bladder contraction and salivation in mini pigs. Urol Int. 2008;81:468–73.
Cutler AJ, Montgomery SA, Feifel D, Lazarus A, Aström M, Brecher M. Extended release quetiapine fumarate monotherapy in major depressive disorder: a placebo- and duloxetine-controlled study. J Clin Psychiatry. 2009;70:526–39.
El-Khalili N, Joyce M, Atkinson S, Buynak RJ, Datto C, Lindgren P, et al. Extended-release quetiapine fumarate (quetiapine XR) as adjunctive therapy in major depressive disorder (MDD) in patients with an inadequate response to ongoing antidepressant treatment: a multicentre, randomized, double-blind, placebo-controlled study. Int J Neuropsychopharmacol. 2010;13:917–32.
Suppes T, Datto C, Minkwitz M, Nordenhem A, Walker C, Darko D. Effectiveness of the extended release formulation of quetiapine as monotherapy for the treatment of acute bipolar depression. J Affect Disord. 2010;121:106–15.
Timdahl K, Carlsson A, Stening G. An analysis of safety and tolerability data from controlled, comparative studies of quetiapine in patients with schizophrenia, focusing on extrapyramidal symptoms. Hum Psychopharmacol. 2007;22:315–25.
Weisler RH, Montgomery SA, Earley WR, Szamosi J, Lazarus A. Efficacy of extended release quetiapine fumarate monotherapy in patients with major depressive disorder: a pooled analysis of two 6-week, double-blind, placebo-controlled studies. Int Clin Psychopharmacol. 2012;27:27–39.
Findling RL, McKenna K, Earley WR, Stankowski J, Pathak S. Efficacy and safety of quetiapine in adolescents with schizophrenia investigated in a 6-week, double-blind, placebo-controlled trial. J Child Adolescent Psychopharmacol. 2012;22:327–42.
Merideth C, Cutler AJ, She F, Eriksson H. Efficacy and tolerability of extended release quetiapine fumarate monotherapy in the acute treatment of generalized anxiety disorder: a randomized, placebo controlled and active-controlled study. Int Clin Psychopharmacol. 2012;27:40–54.
Gareri P, De Fazio P, De Fazio S, Marigliano N, Ferreri Ibbadu G, De Sarro G. Adverse effects of atypical antipsychotics in the elderly: a review. Drugs Aging. 2006;23:937–56.
Katzman MA, Brawman-Mintzer O, Reyes EB, Olausson B, Liu S, Eriksson H. Extended release quetiapine fumarate (quetiapine XR) monotherapy as maintenance treatment for generalized anxiety disorder: a long-term, randomized, placebo-controlled trial. Int Clin Psychopharmacol. 2011;26:11–24.
Bauer M, Pretorius HW, Constant EL, Earley WR, Szamosi J, Brecher M. Extended-release quetiapine as adjunct to an antidepressant in patients with major depressive disorder: results of a randomized, placebo-controlled, double-blind study. J Clin Psychiatry. 2009;70:540–9.
Schatzberg AF. Clinical efficacy of reboxetine in major depression. J Clin Psychiatry. 2000;61(Suppl 10):31–8.
Versiani M, Amin M, Chouinard G. Double-blind, placebo-controlled study with reboxetine in inpatients with severe major depressive disorder. J Clin Psychopharmacol. 2000;20:28–34.
López-Muñoz F, Rubio G, Alamo C, Garcia-Garcia P. Reboxetine addition in patients with mirtazapine-resistant depression: a case series. Clin Neuropharmacol. 2006;29:192–6.
Riahi F, Tehrani-Doost M, Shahrivar Z, Alaghband-Rad J. Efficacy of reboxetine in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled clinical trial. Hum Psychopharmacol. 2010;25:570–6.
Malone RP, Gratz SS, Delaney MA, Hyman SB. Advances in drug treatments for children and adolescents with autism and other pervasive developmental disorders. CNS Drugs. 2005;19:923–34.
Wu A, Wagner ML. Rotigotine transdermal system for the treatment of restless legs syndrome. Future Neurol. 2009;4:267–77.
Hening WA, Allen RP, Ondo WG, Walters AS, Winkelman JW, Becker P, et al. Rotigotine improves restless legs syndrome: a 6-month randomized, double-blind, placebo-controlled trial in the United States. Mov Disord. 2010;25:1675–83.
Finlay E, Straton JB, Gavrin JR. Nausea and vomiting: an overview of mechanisms and treatment in older patients. Geriatr Aging. 2007;10:116–21.
Khajavi D, Farokhnia M, Modabbernia A, Ashrafi M, Abbasi SH, Tabrizi M, et al. Oral scopolamine augmentation in moderate to severe major depressive disorder: a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2012;73:1428–33.
Kaya A, Aydin N, Topsever P, Filiz M, Oztürk A, Dağar A, et al. Efficacy of sibutramine, orlistat and combination therapy on short-term weight management in obese patients. Biomed Pharmacother. 2004;58:582–7.
Wilfley DE, Crow SJ, Hudson JI, Mitchell JE, Berkowitz RI, Blakesley V, et al. Efficacy of sibutramine for the treatment of binge eating disorder: a randomized multicenter placebo-controlled double-blind study. Am J Psychiatry. 2008;165:51–8.
But I, Goldstajn MS, Oreskovic S. Comparison of two selective muscarinic receptor antagonists (solifenacin and darifenacin) in women with overactive bladder–the SOLIDAR study. Coll Antropol. 2012;36:1347–53.
Chancellor MB, Zinner N, Whitmore K, Kobayashi K, Snyder JA, Siami P. et al. Efficacy of solifenacin in patients previously treated with tolterodine extended release 4 mg: results of a 12-week, multicenter, open-label, flexible-dose study. Clin Ther. 2008;30:1766–81.
Chu F, Smith N, Uchida T. Efficacy and safety of solifenacin succinate 10 mg once daily: a multicenter, phase III, randomized, double-blind, placebo-controlled, parallel-group trial in patients with overactive bladder. Curr Therap Res Clin Exp. 2009;70:405–20.
Mattiasson A, Masala A, Morton R, Bolodeoku J. Efficacy of simplified bladder training in patients with overactive bladder receiving a solifenacin flexible-dose regimen: Results from a randomized study. BJU Int. 2010;105:1126–35.
Serels SR, Toglia MR, Forero-Schwanhaeuser S, He W. Impact of solifenacin on diary-recorded and patient-reported urgency in patients with severe overactive bladder (OAB) symptoms. Curr Med Res Opin. 2010;26:2277–85.
Metello J, Nogueira B, Torgal M, Colaço J, Vieira A, Gonçalves V, et al. Comparison of the efficacy and tolerability of solifenacin succinate with or without previous use of trospium chloride. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:1021–5.
Astrup A, Madsbad S, Breum L, Jensen TJ, Kroustrup JP, Larsen TM. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372:1906–13.
Oba Y, Zaza T, Thameem DM. Safety, tolerability and risk benefit analysis of tiotropium in COPD. Int J Chron Obstruct Pulmon Dis. 2008;3:575–84.
Kerstjens HAM, Disse B, Schroder-Babo W, Bantje TA, Gahlemann M, Sigmund R, et al. Tiotropium improves lung function in patients with severe uncontrolled asthma: a randomized controlled trial. J Allergy Clin Immunol. 2011;128:308–14.
Chung DE, Te AE, Staskin DR, Kaplan SA. Efficacy and safety of tolterodine extended release and dutasteride in male overactive bladder patients with prostates >30 grams. Urology. 2010;75:1144–8.
Herschorn S, Swift S, Guan Z, Carlsson M, Morrow JD, Brodsky M, et al. Comparison of fesoterodine and tolterodine extended release for the treatment of overactive bladder: a head-to-head placebo-controlled trial. BJU Int. 2010;105:58–66.
Jonas U, Hofner K, Madersbacher H, Holmdahl TH. Efficacy and safety of two doses of tolterodine versus placebo in patients with detrusor overactivity and symptoms of frequency, urge incontinence, and urgency: urodynamic evaluation. The International Study Group. World J Urol. 1997;15:144–51.
McKeage K, Keating GM. Fesoterodine. Drugs. 2009;69:731–8.
Nitti VW, Dmochowski R, Appell RA, Wang JT, Bavendam T, Guan Z, et al. Efficacy and tolerability of tolterodine extended-release in continent patients with overactive bladder and nocturia. BJU Int. 2006;97:1262–6.
Roehrborn CG, Abrams P, Rovner ES, Kaplan SA, Herschorn S, Guan Z. Efficacy and tolerability of tolterodine extended-release in men with overactive bladder and urgency urinary incontinence. BJU Int. 2006;97:1003–6.
Zinner NR, Mattiasson A, Stanton SL. Efficacy, safety, and tolerability of extended-release once-daily tolterodine treatment for overactive bladder in older versus younger patients. J Am Geriatr Soc. 2002;50:799–807.
Griebling TL, Kraus SR, Richter HE, Glasser DB, Carlsson M. Tolterodine extended release is well tolerated in older subjects. Int J Clin Pract. 2009;63:1198–204.
Sacco E, Bientinesi R. Mirabegron: a review of recent data and its prospects in the management of overactive bladder. Ther Adv Urol. 2012;4:315–24.
Speciali JG, Stuginski-Barbosa J. Burning mouth syndrome. Curr Pain Headache Rep. 2008;12:279–84.
Maruyama I, Yonekubo S, Tatemichi S, Maruyama K, Hoyano Y, Yamazaki Y, et al. Effects of ritobegron (KUC-7483), a novel beta3-adrenoceptor agonist, on both rat bladder function following partial bladder outlet obstruction and on rat salivary secretion: a comparison with the effects of tolterodine. J Smooth Muscle Res. 2012;48:115–24.
Khullar V, Amarenco G, Angulo JC, Cambronero J, Høye K, Milsom I, et al. Efficacy and tolerability of mirabegron, a beta3-adrenoceptor agonist, in patients with overactive bladder: Results from a randomised European-Australian phase 3 trial. Eur Urol. 2013;63:283–95.
Barton D, La Vasseur B, Loprinzi C, Novotny P, Wilwerding MP, Sloan J. Venlafaxine for the control of hot flashes: results of a longitudinal continuation study. Oncol Nurs Forum. 2002;29:33–40.
Feighner JP, Entsuah AR, McPherson MK. Efficacy of once-daily venlafaxine extended release (XR) for symptoms of anxiety in depressed outpatients. J Affect Disord. 1998;47:55–62.
Gelenberg AJ, Lydiard RB, Rudolph RL, Aguiar L, Haskins JT, Salinas E. Efficacy of venlafaxine extended-release capsules in nondepressed outpatients with generalized anxiety disorder: a 6-month randomized controlled trial. JAMA. 2000;283:3082–8.
Staab JP, Evans DL. Efficacy of venlafaxine in geriatric depression. Depress Anxiety. 2000;12(Suppl 1):63–8.
Krevsky B, Maurer AH, Niewiarowski T, Cohen S. Effect of verapamil on human intestinal transit. Dig Dis Sci. 1992;37:919–24.
Rothschild AJ, Mahableshwarkar AR, Jacobsen P, Yan M, Sheehan DV. Vortioxetine (Lu AA21004) 5 mg in generalized anxiety disorder: Results of an 8-week randomized, double-blind, placebo-controlled clinical trial in the United States. Eur Neuropsychopharmacol. 2012;22:858–66.
Harrington CA, English C. Adverse drug events related to ziprasidone: a meta-analysis of randomized, placebo-controlled trials. Pharmacotherapy. 2011;31:840–9.
Papakostas GI, Vitolo OV, Ishak WW, Rapaport MH, Zajecka JM, Kinrys G, et al. A 12-week, randomized, double-blind, placebo-controlled, sequential parallel comparison trial of ziprasidone as monotherapy for major depressive disorder. J Clin Psychiatry. 2012;73:1541–7.
Fava M, Asnis GM, Shrivastava RK, Lydiard B, Bastani B, Sheehan DV, et al. Improved insomnia symptoms and sleep-related next-day functioning in patients with comorbid major depressive disorder and insomnia following concomitant zolpidem extended-release 12.5 mg and escitalopram treatment: a randomized controlled trial. J Clin Psychiatry. 2011;72:914–28.
Joffe H, Partridge A, Giobbie-Hurder A, Li X, Habin K, Goss P, Winer E, et al. Augmentation of venlafaxine and selective serotonin reuptake inhibitors with zolpidem improves sleep and quality of life in breast cancer patients with hot flashes: a randomized, double-blind, placebo-controlled trial. Menopause. 2010;17:908–16.
Brunton LL. Goodman & Gilman’s the pharmacological basis of therapeutics. 12th ed. New York: McGraw-Hill Medical; 2011.
Godoy T, Riva A, Ekström J. Atypical antipsychotics—effects of amisulpride on salivary secretion and on clozapine-induced sialorrhea. Oral Dis. 2012;18:680–91.
Timpe EM, Chopra RA. Asenapine: a novel atypical antipsychotic agent for schizophrenia and bipolar I disorder. J Pharmacy Technol. 2010;26:352–61.
Croog SH, Elias MF, Colton T, Baume RM, Leiblum SR, Jenkins CD. Effects of antihypertensive medications on quality of life in elderly hypertensive women. Am J Hypertens. 1994;7:329–39.
Henz BM, Metzenauer P, O’Keefe E, Zuberbier T. Differential effects of new-generation H1-receptor antagonists in pruritic dermatoses. Allergy. 1998;53:180–3.
Wellington K, Jarvis B. Cetirizine/pseudoephedrine. Drugs. 2001;61:2231–2240 (discussion 2241–2232).
Seo T, Nagata R, Ishitsu T, Murata T, Takaishi C, Hori M, et al. Impact of CYP2C19 polymorphisms on efficacy of clobazam therapy. Pharmacogenomics. 2008;9:527–37.
Koller MM, Cowman RA, Humphreys-Beher MG, Scarpace PJ. An analysis of parotid salivary gland function with desipramine and age in female NIA Fischer 344 rats. Exp Gerontol. 2001;36:141–57.
Aberer W. Desloratadine for the relief of nasal and non-nasal allergy symptoms: an observational study. Arch Drug Inf. 2009;2:17–22.
Wilken JA, Daly AF, Sullivan CL, Kim H. Desloratadine for allergic rhinitis. Exp Rev Clin Immunol. 2006;2:209–24.
Kornstein SG, Clayton AH, Soares CN, Padmanabhan SK, Guico-Pabia CJ. Analysis by age and sex of efficacy data from placebo-controlled trials of desvenlafaxine in outpatients with major depressive disorder. J Clin Psychopharmacol. 2010;30:294–9.
Liebowitz MR, Manley AL, Padmanabhan SK, Ganguly R, Tummala R, Tourian KA. Efficacy, safety, and tolerability of desvenlafaxine 50 mg/day and 100 mg/day in outpatients with major depressive disorder. Curr Med Res Opin. 2008;24:1877–90.
Pae CU. Desvenlafaxine: a new antidepressant or just another one? Exp Opin Pharmacotherapy. 2009;10:875–87.
Tourian KA, Pitrosky B, Padmanabhan SK, Rosas GR. A 10-month, open-label evaluation of desvenlafaxine in outpatients with major depressive disorder. Prim Care Companion CNS Disord. 2011;13:e1–10.
Swinburn BA, Carmichael HE, Wilson MR. Dexfenfluramine as an adjunct to a reduced-fat, ad libitum diet: effects on body composition, nutrient intake and cardiovascular risk factors. Int J Obes Relat Metab Disord. 1996;20:1033–40.
Davis R, Faulds D. Dexfenfluramine. An updated review of its therapeutic use in the management of obesity. Drugs. 1996;52:696–724.
Bajwa SJ, Arora V, Kaur J, Singh A, Parmar SS. Comparative evaluation of dexmedetomidine and fentanyl for epidural analgesia in lower limb orthopedic surgeries. Saudi J Anaesth. 2011;5:365–70.
Diz Dios P, Scully C. Antiretroviral therapy: effects on orofacial health and health care. Oral Dis. 2014;20:136–45.
Freye E, Baranowski J, Latasch L. Dose-related effects of controlled release dihydrocodeine on oro-cecal transit and pupillary light reflex. A study in human volunteers. Arzneimittelforschung. 2001;51:60–6.
Davies EC, Green CF, Mottram DR, Pirmohamed M. Adverse drug reactions in hospital in-patients: a pilot study. J Clin Pharm Therap. 2006;31:335–41.
Kalis B. Double-blind multicentre comparative study of ebastine, terfenadine and placebo in the treatment of chronic idiopathic urticaria in adults. Drugs. 1996;52(Suppl 1):30–4.
Storms WW. Clinical studies of the efficacy and tolerability of ebastine 10 or 20 mg once daily in the treatment of seasonal allergic rhinitis in the US. Drugs. 1996;52(Suppl 1):20–5.
Pelaez A. Clinical efficacy of ebastine in the treatment and prevention of seasonal allergic rhinitis. Drugs. 1996;52(Suppl 1):35–8.
Halas CJ. Cost-effectiveness of eszopiclone for the treatment of chronic insomnia. Expert Rev Pharmacoecon Outcomes Res. 2007;7:9–17.
Monti JM, Pandi-Perumal SR. Eszopiclone: Its use in the treatment of insomnia. Neuropsychiatr Dis Treat. 2007;3:441–53.
Pollack M, Kinrys G, Krystal A, McCall WV, Roth T, Schaefer K, et al. Eszopiclone coadministered with escitalopram in patients with insomnia and comorbid generalized anxiety disorder. Arch Gen Psychiatry. 2008;65:551–62.
Tzefos M, Dolder C, Olin JL. Fesoterodine for the treatment of overactive bladder. Ann Pharmacotherapy. 2009;43:1992–2000.
Kay GG, Maruff P, Scholfield D, Malhotra B, Whelan L, Darekar A. Evaluation of cognitive function in healthy older subjects treated with fesoterodine. Postgrad Med. 2012;124:7–15.
Yamaguchi O, Nishizawa O, Takeda M, Yoshida M, Choo MS, Gu Lee J, et al. Efficacy, safety and tolerability of fesoterodine in Asian patients with overactive bladder. Low Urin Tract Symptoms. 2011;3:43–50.
Bova JG, Jurdi RA, Bennett WF. Antispasmodic drugs to reduce discomfort and colonic spasm during barium enemas: comparison of oral hyoscyamine, i.v. glucagon, and no drug. AJR Am J Roentgenol. 1993;161:965–8.
Fang SY, Perng DW, Lee JY, Lin DY, Huangs CY. An open-label, multicentre study of levocetirizine for the treatment of allergic rhinitis and urticaria in Taiwanese patients. Chin J Physiol. 2010;53:199–207.
Gerc V, Begović B, Vehabović M, Voronkov LG, Vataman E, Musić L, et al. Fixed combination lisinopril plus hydro-chlorothiazide in the treatment of essential arterial hypertension: an opened, multi-centre, prospective clinical trial. Bosn J Basic Med Sci. 2007;7:377–82.
McEvoy JP, Citrome L, Hernandez D, Cucchiaro J, Hsu J, Pikalov A, et al. Effectiveness of lurasidone in patients with schizophrenia or schizoaffective disorder switched from other antipsychotics: a randomized, 6-week, open-label study. J Clin Psychiatry. 2013;74:170–9.
Aneja P, Srinivas A, Biswas AD. Comparative clinical study of the efficacy and safety of a S-metoprolol ER tablet versus a racemate metoprolol ER tablet in patients with chronic stable angina. Int J Clin Pharmacol Ther. 2007;45:253–8.
Momo K, Homma M, Osaka Y, Inomata S, Tanaka M, Kohda Y. Effects of mexiletine, a CYP1A2 inhibitor, on tizanidine pharmacokinetics and pharmacodynamics. J Clin Pharmacol. 2010;50:331–7.
Vickers MD, Paravicini D. Comparison of tramadol with morphine for post-operative pain following abdominal surgery. Eur J Anaesthesiol. 1995;12:265–71.
Zacny JP, Lichtor JL, Flemming D, Coalson DW, Thompson WK. A dose-response analysis of the subjective, psychomotor and physiological effects of intravenous morphine in healthy volunteers. J Pharmacol Exp Ther. 1994;268:1–9.
Kim SW, Grant JE, Adson DE, Shin YC. Double-blind naltrexone and placebo comparison study in the treatment of pathological gambling. Biol Psychiatry. 2001;49:914–21.
Ossip DJ, Abrams SM, Mahoney MC, Sall D, Cummings KM. Adverse effects with use of nicotine replacement therapy among quitline clients. Nicotine Tob Res. 2009;11:408–17.
Polosa R, Caponnetto P, Morjaria JB, Papale G, Campagna D, Russo C. Effect of an electronic nicotine delivery device (e-Cigarette) on smoking reduction and cessation: a prospective 6-month pilot study. BMC Public Health. 2011;11:786.
Bull E. Drug review - Pregabalin. Drugs. Context. 2006;2:65–77.
Semel D, Murphy TK, Zlateva G, Cheung R, Emir B. Evaluation of the safety and efficacy of pregabalin in older patients with neuropathic pain: results from a pooled analysis of 11 clinical studies. BMC Fam Pract. 2010;11:85.
Vinik A. Clinical review: use of antiepileptic drugs in the treatment of chronic painful diabetic neuropathy. J Clin Endocrinol Metab. 2005;90:4936–45.
Murdoch D, Keating GM. Sertindole: a review of its use in schizophrenia. CNS Drugs. 2006;20:233–55.
Karamatskos E, Lambert M, Mulert C, Naber D. Drug safety and efficacy evaluation of sertindole for schizophrenia. Expert Opin Drug Saf. 2012;11:1047–62.
Steigerwald I, Muller M, Davies A, Samper D, Sabatowski R, Baron R, et al. Effectiveness and safety of tapentadol prolonged release for severe, chronic low back pain with or without a neuropathic pain component: Results of an open-label, phase 3b study. Curr Med Res Opin. 2012;28:911–36.
Lee E, Lee C. Clinical comparison of selective and non-selective alpha 1A-adrenoreceptor antagonists in benign prostatic hyperplasia: studies on tamsulosin in a fixed dose and terazosin in increasing doses. Br J Urol. 1997;80:606–11.
Semenchuk MR, Sherman S. Effectiveness of tizanidine in neuropathic pain: an open-label study. J Pain. 2000;1:285–92.
Verbalis JG, Adler S, Schrier RW, Berl T, Zhao Q, Czerwiec FS, et al. Efficacy and safety of oral tolvaptan therapy in patients with the syndrome of inappropriate antidiuretic hormone secretion. Eur J Endocrinol. 2011;164:725–32.
Delahaye C, Ferrand B, Pieddeloup C, Musch B. Post marketing surveillance of zopiclone: interim analysis on the first 10,000 cases in a clinical study in general practice. Int Clin Psychopharmacol. 1990;5(Suppl 2):131–8.
Mangel AW, Hicks GA. Asimadoline and its potential for the treatment of diarrhea-predominant irritable bowel syndrome: a review. Clin Exp Gastroenterol. 2012;5:1–10.
Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs. 2004;64:205–22.
Bouwer A. Combination cold and flu medicines: an overview of autonomic nervous system receptors. S Afr Fam Pract. 2012;54:33–6.
Boven E, Westerman M, van Groeningen CJ, Verschraagen M, Ruijter R, et al. Phase I and pharmacokinetic study of the novel chemoprotector BNP7787 in combination with cisplatin and attempt to eliminate the hydration schedule. Br J Cancer. 2005;92:1636–43.
Tutka P, Zatonski W. Cytisine for the treatment of nicotine addiction: From a molecule to therapeutic efficacy. Pharmacol Rep. 2006;58:777–98.
Friedel HA, Fitton A. Flupirtine. A review of its pharmacological properties, and therapeutic efficacy in pain states. Drugs. 1993;45:548–69.
Moreno J, Sahade M, del Giglio A. Low-dose granisetron for prophylaxis of acute chemotherapy-induced nausea and vomiting: a pilot study. Support Care Cancer. 2005;13:850–3.
Vongpatanasin W, Kario K, Atlas SA, Victor RG. Central sympatholytic drugs. J Clin Hypertens (Greenwich). 2011;13:658–61.
Newnham DM. Asthma medications and their potential adverse effects in the elderly: recommendations for prescribing. Drug Saf. 2001;24:1065–80.
Ormseth MJ, Eyler AE, Hammonds CL, Boomershine CS. Milnacipran for the management of fibromyalgia syndrome. J Pain Res. 2010;3:15–24.
Blaya C, Seganfredo AC, Dornelles M, Torres M, Paludo A, Heldt E. et al. The efficacy of milnacipran in panic disorder: An open trial. Int Clin Psychopharmacol. 2007;22:153–8.
Coskun M, Ahmetoglu E, Ozturk M. Mirtazapine treatment for comorbid anxiety/depressive disorders in young subjects with attention-deficit hyperactivity disorder: case series. Klinik Psikofarmakoloji Bulteni. 2010;20:246–51.
Schwartz JRL. Modafinil in the treatment of excessive sleepiness. Drug Des Dev Ther. 2008;2:71–85.
Curran MP, Robinson DM. Mosapride in gastrointestinal disorders. Drugs. 2008;68:981–91.
Tulkens PM, Arvis P, Kruesmann F. Moxifloxacin safety: an analysis of 14 years of clinical data. Drugs R D. 2012;12:71–100.
Prichard BN, Graham BR. I1 imidazoline agonists. General clinical pharmacology of imidazoline receptors: implications for the treatment of the elderly. Drugs Aging. 2000;17:133–59.
Ellingrod VL, Perry PJ. Nefazodone: a new antidepressant. Am J Health Syst Pharm. 1995;52:2799–812.
Davis R, Whittington R, Bryson HM. Nefazodone. A review of its pharmacology and clinical efficacy in the management of major depression. Drugs. 1997;53:608–36.
West D, Chambers S. Drug review—Perindopril. Drugs Context. 2006;2:17–34.
Wilde MI, Benfield P. Tianeptine—a review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in depression and coexisting anxiety and depression. Drugs. 1995;49:411–39.
Dawes C, Pedersen AM, Villa A, Ekström J, Proctor GB, Vissink A, et al. The functions of human saliva: a review sponsored by the World Workshop on Oral Medicine VI. Arch Oral Biol. 2015;60:863–74.
Villa A, Wolff A, Narayana N, Dawes C, Aframian DJ, Lynge Pedersen AM, et al. World Workshop on Oral Medicine VI: a systematic review of medication-induced salivary gland dysfunction. Oral Dis. 2016;22:365–82.
Aliko A, Wolff A, Dawes C, Aframian D, Proctor G, Ekström J, et al. World Workshop on Oral Medicine VI: clinical implications of medication-induced salivary gland dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:185–206.
Villa A, Wolff A, Aframian D, Vissink A, Ekström J, Proctor G, et al. World Workshop on Oral Medicine VI: a systematic review of medication-induced salivary gland dysfunction: prevalence, diagnosis, and treatment. Clin Oral Investig. 2015;19:1563–80.
WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index. http://www.whocc.no/atc_ddd_index/?code=A08AA&showdescription=yes. Accessed 9 Nov 2016.
WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2016. http://www.whocc.no/atc_ddd_index/. Accessed 9 Nov 2016.
Acknowledgements
The authors, including selected members of the WWOM VI Steering Committee, express their sincere appreciation for the opportunity to collaborate with the full WWOM VI Steering Committee over these past 3 years. This committee provided the conceptual framework and logistical support to produce the WWOM VI Conference in April 2014 in Orlando, Florida, USA. In addition, the Steering Committee provided scientific and editorial critiques of this manuscript. The entire Steering Committee is listed below, in alphabetical order: Martin S. Greenberg (USA), Timothy A. Hodgson (UK), Siri Beier Jensen (Denmark), A. Ross Kerr (USA), Peter B. Lockhart (USA), Giovanni Lodi (Italy), Douglas E. Peterson (USA), and David Wray (UK and Dubai).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The authors gratefully acknowledge the following organizations, individuals, and companies that provided unrestricted financial support for WWOM VI: American Academy of Oral Medicine, European Association of Oral Medicine, anonymous gifts from patients of Dr. David Sirois, New York University, College of Dentistry, Biocosmetics, Elsevier, Johnson and Johnson, The Oral Cancer Foundation, and Unilever.
Conflict of interest
AW owns stocks in Saliwell Ltd., a company that deals with electrostimulation devices to treat xerostomia. RKJ, JE, DA, AMLP, GP, NN, A Villa, YWS, AA, RM, ARK, SBJ, A Vissink, and CD have no conflicts of interest that are directly related to the content of this article.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Wolff, A., Joshi, R.K., Ekström, J. et al. A Guide to Medications Inducing Salivary Gland Dysfunction, Xerostomia, and Subjective Sialorrhea: A Systematic Review Sponsored by the World Workshop on Oral Medicine VI. Drugs R D 17, 1–28 (2017). https://doi.org/10.1007/s40268-016-0153-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40268-016-0153-9