
Abstract
Purpose
Combination therapy of male lower urinary tract symptoms with α1-adrenoceptor and muscarinic receptor antagonists attracts increasing interest. Propiverine is a muscarinic receptor antagonist possessing additional properties, i.e., block of L-type Ca2+ channels. Here, we have investigated whether propiverine and its metabolites can additionally antagonize α1-adrenoceptors.
Methods
Human prostate and porcine trigone muscle strips were used to explore inhibition of α1-adrenoceptor-mediated contractile responses. Chinese hamster ovary (CHO) cells expressing cloned human α1-adrenoceptors were used to determine direct interactions with the receptor in radioligand binding and intracellular Ca2+ elevation assays.
Results
Propiverine concentration-dependently reversed contraction of human prostate pre-contracted with 10 μM phenylephrine (−log IC50 [M] 4.43 ± 0.08). Similar inhibition was observed in porcine trigone (−log IC50 5.01 ± 0.05), and in additional experiments consisted mainly of reduced maximum phenylephrine responses. At concentrations ≥1 μM, the propiverine metabolite M-14 also relaxed phenylephrine pre-contracted trigone strips, whereas metabolites M-5 and M-6 were ineffective. In radioligand binding experiments, propiverine and M-14 exhibited similar affinity for the three α1-adrenoceptor subtypes with −log K i [M] values ranging from 4.72 to 4.94, whereas the M-5 and M-6 did not affect [3H]-prazosin binding. In CHO cells, propiverine inhibited α1-adrenoceptor-mediated Ca2+ elevations with similar potency as radioligand binding, again mainly by reducing maximum responses.
Conclusions
In contrast to other muscarinic receptor antagonists, propiverine exerts additional L-type Ca2+-channel blocking and α1-adrenoceptor antagonist effects. It remains to be determined clinically, how these additional properties contribute to the clinical effects of propiverine, particularly in male voiding dysfunction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The medical treatment of male lower urinary tract symptoms (LUTS) typically consists primarily of α1-adrenoceptor antagonists, but in many patients this provides insufficient symptom relief. A combination of α1-adrenoceptor and muscarinic receptor antagonists may be more effective, particularly against storage symptoms [1, 2]. While most combination studies have used tolterodine as the muscarinic antagonist, several have also been based on propiverine [1–4].
Propiverine is an antagonist with similar affinity for all muscarinic receptor subtypes [5, 6] which also inhibits voltage-gated L-type Ca2+-channels [9–13]. As contractions of prostate [7] and bladder smooth muscle [8] at least partly depend on such channels, their inhibition may contribute to the therapeutic effects of propiverine in LUTS suggestive of benign prostatic hyperplasia and overactive bladder (OAB), respectively.
Based upon the growing interest in a combination treatment of male LUTS, we have explored possible α1-adrenoceptor antagonist effects of propiverine and its metabolites M-5, M-6, and M-14, which share the anti-muscarinic and/or L-type Ca2+-channel-blocking activity of propiverine [16, 17].
Materials and methods
Prostate and trigone detrusor contraction
Human prostate was obtained with informed written consent in accordance with the regulations of the local hospital ethical committee (permit EK 194092004) from six patients undergoing combined prostectomy and radical cystectomy for invasive bladder cancer (65 ± 3 years). Urinary bladder trigone from juvenile and adult female pigs were obtained from a local abattoir. Prostate strips (10 mm long and 3–4 mm wide) and trigone strips (7–10 mm long and 2–4 mm wide without urothelium) were prepared and mounted in organ baths as previously described [7, 18] except for a resting load of 5 mN. After an equilibration period of 60 min, the strips were challenged with a single concentration of α1-adrenoceptor agonist phenylephrine (10 μM) to reach a stable pre-contraction after 60 min. Then, increasing concentrations of test compounds were added cumulatively (15 min between concentration steps). Relaxation values were normalized to the 10 μM forskolin effect, as determined at the end of each experiment, and were corrected for spontaneous decline of force in time-matched control (TMC) experiments.
In other experiments, porcine trigone strips were exposed to cumulatively increasing concentrations of phenylephrine (30 nM–100 μM) with 5 min of stabilization between two subsequent additions. After maximum contraction was observed, phenylephrine was removed by washing 3 times with drug-free solution and re-equilibrating for 60 min. Then a single concentration of test compound was added and after additional 30 min, a second concentration-response curve for phenylephrine was generated.
Radioligand binding
Binding of propiverine and its metabolites to human α1-adrenoceptor subtypes was analyzed in Chinese hamster ovary (CHO) cells, expressing approximately 2 pmol receptor/mg protein, by competition binding against [3H]-prazosin as previously described [19, 20]. Phentolamine was used as a reference antagonist. Radioactivity adherent to the filters was quantified in a Topcount NXT (Perkin Elmer, Zaventem, Belgium) using Microsint O (Perkin Elmer) scintillator.
Intracellular Ca2+
Cells were plated in black, clear bottom 96 wells plates at 50,000 cells per well. After 24 h in serum-free medium, cells were loaded for 1 h with 4 μM Fluo-4 AM ester in buffer (HBSS containing 20 mM HEPES and 250 mM probenecid and 0.42% v/v pluronic acid). They were then washed twice and incubated for 45 min with buffer. Fluorescence was measured using an excitation filter at 485 nm and emission filter at 520 nm on a NOVOstar (BMG Labtech, via Isogen, IJselstein, the Netherlands). After measuring the basal level for 10 s, phenylephrine (100 pM–10 μM) was added and measured for 50 s, then 5% v/v triton X-100 in basic buffer was added at 10% v/v to determine the maximal signal (Fmax). After 20 s, 0.1 M EGTA in buffer was added at 10% v/v to determine the minimal signal (Fmin). The increase in free intracellular Ca2+ ([Ca2+]i) was calculated as the difference between the [Ca2+]i for the basal level and after adding a ligand. [Ca2+]i was calculated by the equation:
K d is the dissociation constant of the binding of Fluo-4 to Ca2+ (345 nM). Concentration-response curves for phenylephrine were generated in duplicate in the absence and presence of propiverine, its metabolites M-5, M-6, and M-14 and the reference antagonist phentolamine (added 15 min prior to phenylephrine).
Data analysis
Experimental data were analyzed, by non-linear curve fitting of each individual experiment using GraphPad Prism® 4.00 (GraphPad Software, San Diego, CA, USA). Potencies of propiverine, tamsulosin, and prazosin on phenylephrine pre-contracted human prostate and porcine trigone strips were determined as −log IC50 [M] values. The potency (−log EC50 [M]) and efficacy of phenylephrine-induced contractions and [Ca2+]i elevations were determined in the absence and presence of the indicated test compounds. Maximum contraction during the second concentration-response curve for phenylephrine (Effmax) was expressed as percent of the maximum effects during the first concentration-response curve (=100%). Inhibitory potency as determined from competition binding experiments was transformed to −log K i values using the Cheng and Prusoff equation. Statistical differences were tested by Student’s t-test and were considered significant for P < 0.05.
Chemicals
[3H]-prazosin (specific activity 80 Ci/mmol) was purchased from Perkin Elmer (Zaventem, Belgium). Propiverine hydrochloride, M-5 (2,2-diphenyl-2-propoxy-acetic acid [1-methyl-piperid-4-yl]-ester-N-oxide-trans), M-6 (2,2-diphenyl-2-hydroxy-acetic acid [1-methyl-piperid-4-yl]-ester-N-oxide-trans), M-14 (2,2-diphenyl-2-propoxy-acetic acid [piperid-4-yl]-ester), and tamsulosin were synthesized at APOGEPHA Arzneimittel GmbH. Prazosin was from TOCRIS (Bristol, UK). Fluo-4 AM ester and pluronic acid were from Molecular Probes (via Invitrogen, Breda, The Netherlands). Phentolamine, phenylephrine, and all other chemicals were from SIGMA–ALDRICH (Taufkirchen, Germany).
Results
Effects on α1-adrenoceptor-mediated prostate contraction
At the end of the equilibration period, human prostate strips exhibited a passive tension of 0.06 ± 0.01 mN/mg wet weight (n = 16 strips/five patients). Phenylephrine (10 μM) increased force of contraction to peak values of 0.16 ± 0.02 mN/mg (n = 19/6), which stabilized at steady-state values of 0.10 ± 0.02 mN/mg (n = 16/5) within 45 min (Fig. 1a). The maximum relaxation induced by 10 μM forskolin was 0.07 ± 0.01 mN/mg (n = 16/5). Propiverine, tamsulosin, and prazosin relaxed phenylephrine-induced contractions in a concentration-dependent manner (Fig. 1b).

a Original recordings of force of contraction in a human prostate tissue strip. The preparation was pre-contracted with phenylephrine (PE, 10 μM) (left arrow). After stabilization of force, propiverine or vehicle were added in increasing concentrations (0.1–100 μM). Finally, forskolin (10 μM) was added for complete relaxation. The difference between force prior to addition of the test compound and force in the presence of forskolin was taken as maximum relaxation (=100%). b Effects of tamsulosin, prazosin, and propiverine on α1-adrenoceptor-mediated contractions in the human prostate (calculated –log IC50 values 10.39 ± 0.04, 7.73 ± 0.04, and 4.43 ± 0.08, respectively). Values were corrected for spontaneous relaxation during time-matched controls, normalized to percent relaxation by forskolin and expressed as means ± SEM
Effects on α1-adrenoceptor-mediated trigone contraction
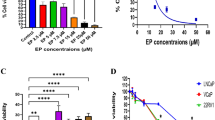
Phenylephrine concentration-dependently contracted adult porcine trigone (but not bladder wall) with maximum contractions of 1.24 ± 0.23 mN/mg wet weight and a −log EC50 [M] of 5.74 ± 0.04 (n = 6). In juvenile tissues, these contractions were concentration-dependently reversed by tamsulosin, prazosin, and propiverine (Fig. 2a). The overall relaxing effect of propiverine on contractions was similar in tissue from mature and juvenile animals, but the potency was lower in mature than in juvenile pigs (−log IC50 [M] 5.01 ± 0.05 vs. 6.21 ± 0.10, respectively; n = 5–7; P < 0.05; Fig. 2a,b). In trigone from mature pigs M-14 caused similar relaxation when compared to propiverine but with lower potency (4.84 ± 0.08; n = 8; Fig. 2b). M-5 and M-6 did not influence trigone contractions in concentrations up to 100 μM (data not shown).

a Effects of cumulatively added concentrations of phenylephrine on adult pig detrusor tissue from the trigone and the wall area of the urinary bladder. Data were normalized to mN/mg wet weight of the detrusor strip. b Effects of increasing concentrations of propiverine in comparison to those of the α1-adrenoceptor antagonists tamsulosin and prazosin on juvenile porcine detrusor strips from the trigone area of the urinary bladder. Strips were pre-contracted with 10 μM of the α1-adrenoceptor agonist phenylephrine. c Effects of increasing concentrations of propiverine and its metabolites M-5 and M-6 and d effects of propiverine and M-14 on trigone detrusor strips from mature pigs pre-contracted with phenylephrine (10 μM). Data in b–d were normalized to percent relaxation by forskolin (10 μM) and corrected for spontaneous relaxation during time-matched controls. Means ± SEM
Concentration-response curves for phenylephrine in porcine trigone strips in the presence of increasing propiverine concentrations demonstrated that inhibition was largely insurmountable, i.e., mainly consisting of reduced maximum responses with only minor if any reductions in apparent potency (Fig. 3).

Effect of increasing concentrations of propiverine on concentration-response curves for phenylephrine in adult porcine detrusor strips from the trigone area. Each strip underwent one phenylephrine curve in the absence of propiverine, and the result maximum response was defined as 100%. Then, phenylephrine response curves were repeated in the absence (time-matched control, TMC) and presence of 10, 30, and 100 μM propiverine yielding phenylephrine potencies (−log EC50) of 5.82 ± 0.19, 5.46 ± 0.38, 5.48 ± 0.28, and 5.90 ± 0.22, respectively. Corresponding Effmax values were 58 ± 9, 39 ± 6, 28 ± 6*, and 9 ± 2** (expressed as % of values in corresponding first phenylephrine curve; * and **: P < 0.05 and < 0.01, respectively, vs. TMC). Means ± SEM from 5–8 experiments
Binding to α1-adrenoceptor subtypes
Direct α1-adrenoceptor inhibition was evaluated in radioligand binding assays with CHO cells. Propiverine, M-14, and phentolamine competed for [3H]-prazosin binding with −log Ki values of 4.72 ± 0.01, 4.72 ± 0.04, and 8.62 ± 0.19 at α1A-, 4.94 ± 0.02, 5.02 ± 0.11 and 7.96 ± 0.22 at α1B-, and 4.73 ± 0.02, 4.57 ± 0.06 and 7.87 ± 0.04 at α1D-adrenoceptors, respectively (Fig. 4). In contrast, the metabolites M-5 and M-6 had little effect at up to 100 μM.

Effects of propiverine and its metabolites M-5, M-6, and M-14 on [3H]-prazosin binding in human α1A-, α1B-, and α1D-adrenoceptor-expressing CHO cells. The α1-adrenoceptor antagonist phentolamine was used for comparison. Data in the presence of increasing concentrations of test compound are expressed in percent binding of [3H]-prazosin. For control experiments only DMSO was added as a vehicle. Means ± SEM from 3 experiments
α1A-Adrenoceptor-mediated intracellular Ca2+ elevation
The [Ca2+]i increase with 10 μM phenylephrine was about 1,600 nM, and all subsequent data values are normalized to that response as measured within a given experiment (=100%). Propiverine and M-14 concentration-dependently inhibited the [Ca2+]i elevations, but this inhibition largely consisted of reduced maximum responses with small if any effects on phenylephrine potency (Fig. 5a,b). M-5 or M-6 had little effect (Fig. 5c), whereas antagonism by phentolamine was surmountable (Fig. 5d).

Phenylephrine-stimulated elevation of [Ca2+]i in α1A-adrenoceptor-expressing CHO cells. a Control concentration-response curves in the presence of DMSO, and responses to increasing concentrations of propiverine. The vehicle DMSO did not significantly affect the efficacy or potency of phenylephrine to raise [Ca2+]i (n = 4), data not shown. b Responses to M-14 and c responses to M-5 and M-6. d Responses to phentolamine. Data were normalized to [Ca2+]i increase in the presence of 10 μM phenylephrine (=100%). Means ± SEM from 4–5 experiments
Discussion
Propiverine differs from most other OAB drugs as it is not only a muscarinic receptor antagonist [5, 6] but also inhibits L-type Ca2+ channels [9–13]. Based upon the increasing interest in a combination treatment of male LUTS [14–16], we have explored possible α1-adrenoceptor antagonism of propiverine and three of its main metabolites. The α1-adrenoceptor antagonists phentolamine, prazosin, and tamsulosin were used as reference compounds and exhibited the expected potency for interaction with α1-adrenoceptors, thereby validating our model systems and techniques. Due to limited access to human prostate specimen for organ bath experiments as well as smaller signal/noise ratios, we have used porcine trigone as a well established animal model of α1-adrenoceptor-mediated contraction of urological tissue for more detailed analysis.
Our data demonstrate concentration-dependent relaxation of phenylephrine-induced tone of human prostate and porcine trigone. At least in trigone, similar relaxation was observed with the propiverine metabolite M-14 but not with M-5 or M-6. As phenylephrine-induced contraction in these two preparations is α1-adrenoceptor-mediated [17], this relaxation provided initial evidence for α1-adrenoceptor antagonism by propiverine and M-14. However, L-type Ca2+ channels contribute to prostate and bladder contraction [9, 10]. The direct interaction of propiverine and its metabolites with α1-adrenoceptors was demonstrated in competition binding studies with cloned human α1-adrenoceptor subtypes, yielding affinities in line with their potency to relax human prostate and porcine trigone. To verify that the inhibition of radioligand binding was indeed associated with receptor antagonism, concentration-dependent inhibition of phenylephrine-induced [Ca2+]i elevation was demonstrated. In contrast to tissue relaxation experiments, inhibition of [Ca2+]i elevation in CHO cells cannot be explained by Ca2+ channel-blocking properties of propiverine, because CHO cells do not express such L-type Ca2+ channels. Together these experiments demonstrate that propiverine and its metabolite M-14 bind to and inhibit human α1-adrenoceptors and accordingly can relax α1-adrenoceptor-mediated contraction of human prostate and porcine trigone.
Propiverine is a competitive antagonist with similar affinity for all muscarinic receptor subtypes [5, 6, 11]. However, the antagonism of [Ca2+]i elevations in CHO cells and of contraction in porcine trigone was insurmountable. Thus, the molecular interaction of propiverine with α1-adrenoceptors and muscarinic receptors occurs in a different way despite the drug being an antagonist for both receptor families. This differential interaction is also supported by the fact that the propiverine metabolites M-5 and M-6 lacked α1-adrenoceptor effects but inhibit muscarinic receptor function [5, 10, 18, 19].
The affinity of propiverine for α1-adrenoceptors in the present study differs from that for human M3 receptors by 50- to 100-fold [5, 6, 12] but is very similar to its potency for inhibition of L-type Ca2+ channels [12]. As muscarinic antagonists typically are dosed to yield high receptor occupancy rates [20], it can be expected that therapeutic doses of propiverine exhibit some degree of α1-adrenoceptor antagonism and L-type Ca2+ channel blockade. Based upon reported plasma concentrations of propiverine (parent compound alone) [21] and our affinity estimates from the radioligand binding studies, therapeutic propiverine concentrations could occupy up to 10% of α1-adrenoceptors. While this may be less pronounced than the blockade of muscarinic receptors, it may nevertheless contribute to the clinical profile of propiverine and specifically may be beneficial for the treatment of male LUTS. Moreover, the insurmountable antagonism at α1- (but not muscarinic) receptors raises the possibility that even limited α1-adrenoceptor occupancy will yield considerable inhibition over time. Interestingly, a large recent observational study reported that the clinical effects of propiverine against OAB symptoms were quantitatively similar in men when administered alone or as add-on to an existing α-blocker treatment [22]. While these findings do not prove α1-antagonism of propiverine in vivo, they are in line with this proposal. However, dedicated studies will be required to determine the clinical relevance of such effects. They should also take into account that propiverine and its various metabolites differ in their in vivo plasma concentrations [23]. For each of them, the relative contribution of the three molecular targets may differ in the generation of bladder selectivity and the overall relaxing effect in the lower urinary tract [24]. Even if propiverine itself turns out to have too little α1-antagonism in vivo, it is an exciting starting point for the future synthesis of balanced α1/muscarinic receptor antagonists.
Conclusions
In contrast to other drugs used for the treatment of OAB, propiverine is not only a muscarinic receptor antagonist but also has L-type Ca2+ channel blocking and α1-adrenoceptor antagonist effects. While each of these effects may be beneficial in the treatment of voiding dysfunction, including male LUTS, the relative contribution of these mechanisms and of the propiverine metabolites to the overall therapeutic effects upon oral administration of propiverine remains to be determined.
References
Saito H, Yamada T, Oshima H et al (1999) A comparative study of the efficacy and safety of tamsulosin hydrochloride (Harnal capsules) alone and in combination with propiverine hydrochloride (BUP-4 tablets) in patients with prostatic hypertrophy associated with pollakiuria and/or urinary incontinence. Jpn J Urol Surg 12:525–536
Lee K-S, Choo M-S, Kim D-Y et al (2005) Combination treatment with propiverine hydrochloride plus doxazosin controlled release gastrointestinal therapeutic system formulation for overactive bladder and coexisting benign prostatic obstruction: a prospective, randomized, controlled multicenter study. J Urol 174:1334–1338
Maruyama O, Kawachi Y, Hanazawa K et al (2006) Naftopidil monotherapy vs naftopidil and an anticholinergic agent combined therapy for storage symptoms associated with benign prostatic hyperplasia: a prospective randomized controlled study. Int J Urol 13:1280–1285
Yokoyama T, Uematsu K, Watanabe T et al (2009) Naftopidil and propiverine hydrochloride for treatment of male lower urinary tract symptoms suggestive of benign prostatic hyperplasia and concomitant overactive bladder: a prospective randomized controlled study. Scand J Urol Nephrol 43:307–314
Wuest M, Weiss A, Waelbrock M et al (2006) Propiverine and metabolites: differences in binding to muscarinic receptors and in functional models of detrusor contraction. Naunyn-Schmiedeberg’s Arch Pharmacol 374:87–97
Maruyama S, Oki T, Otsuka A et al (2006) Human muscarinic receptor binding characteristics of antimuscarinic agents to treat overactive bladder. J Urol 175:365–369
Chueh S-C, Guh J-H, Chen J et al (1996) Inhibition by tamsulosin of tension responses of human hyperplastic prostate to electrical field stimulation. Eur J Pharmacol 305:177–180
Frazier EP, Peters SLM, Braverman AS et al (2008) Signal transduction underlying control of urinary bladder smooth muscle tone by muscarinic receptors and β-adrenoceptors. Naunyn-Schmiedeberg’s Arch Pharmacol 377:449–462
Christ T, Wettwer E, Wuest M et al (2008) Electrophysiological profile of propiverine—relationship to cardiac risk. Naunyn-Schmiedeberg’s Arch Pharmacol 376:431–440
Wuest M, Hecht J, Christ T et al (2005) Pharmacodynamics of propiverine and three of its metabolites on detrusor contraction. Br J Pharmacol 145:608–619
Tokuno H, Chowdhury JU, Tomita T (1993) Inhibitory effects of propiverine on rat and guinea-pig urinary bladder muscle. Naunyn-Schmiedeberg’s Arch Pharmacol 348:659–662
Uchida S, Kurosawa S, Fujino T et al (2007) Binding activities by propiverine and its N-oxide metabolites of L-type calcium channel antagonist receptors in the rat bladder and brain. Life Sci 80:2454–2460
Zhu H-L, Brain KL, Aishima M et al (2008) Actions of two main metabolites of propiverine (M-1 and M-2) on voltage-dependent L-type Ca2+ currents and Ca2+ transients in murine urinary bladder myocytes. J Pharmacol Exp Ther 324:118–127
Lee K-S, Lee HW, Han DH (2008) Does anticholinergic medication have a role in treating men with overactive bladder and benign prostatic hyperplasia? Naunyn-Schmiedeberg’s Arch Pharmacol 377:491–501
Andersson K-E (2007) LUTS treatment: future treatment options. Neurourol Urodyn 26:934–947
Athanasopoulos A, Perimenis P (2005) Efficacy of the combination of an α1-blocker with an anticholinergic agent in the treatment of lower urinary symptoms associated with bladder outlet obstruction. Exp Opin Pharmacother 6:2429–2433
Michel MC, Vrydag W (2006) α1-, α2- and β-adrenoceptors in the urinary bladder, urethra and prostate. Br J Pharmacol 147:S88–S119
Wuest M, Braeter M, Schoeberl C et al (2005) Juvenile pig detrusor: effects of propiverine and three of its metabolites. Eur J Pharmacol 524:145–148
Propping S, Braeter M, Grimm M-O et al (2010) Anticholinergic effects of cis- and trans-isomers of two metabolites of propiverine. Naunyn-Schmiedeberg’s Arch Pharmacol 381:329–338
Hegde SS (2006) Muscarinic receptors in the bladder: from basic research to therapeutics. Br J Pharmacol 147:S80–S87
Guay DRP (2003) Clinical pharmacokinetics of drugs used to treat urge incontinence. Clin Pharmacokin 42:1243–1285
Oelke M, Murgas S, Baumann I et al (2011) Efficacy of propiverine ER with or without α-blockers related to maximum urinary flow rate in adult men with OAB: results of a 12-week, multicenter, non-interventional study. World J Urol. doi:10.1007/s00345-011-0654-7
May K, Westphal K, Giessmann T et al (2008) Disposition and antimuscarinic effects of the urinary bladder spasmolytics propiverine: influence of dosage forms and circadian-time rhtyhms. J Clin Pharmacol 48:570–579
Yamada S, Ito Y, Taki Y et al (2010) The N-oxide metabolite contributes to bladder selectivity resulting from oral propiverine: muscarinic receptor binding and pharmacokinetics. Drug Metab Dispos 38:1314–1321
Acknowledgments
This study was funded and supported in part by the Bundesministerium für Wirtschaft, Germany (PRO INNO II, KA0558501UL7), Coordination Theme 1 (Health) of the European Community’s FP7, Grant agreement number HEALTH-F2-2008-223234, and by APOGEPHA Arzneimittel GmbH, Dresden, Germany. MB and GJS are employees of Apogepha. MC Michel has received research support, lecturer and/or consultant honoraria in the anti-muscarinic field from Allergan, Astellas, Bayer, Boehringer Ingelheim, Pfizer, Schwarz Pharma, Theravance.
Conflict of interest
The other authors do not report a conflict of interest other than those listed under Acknowledgments.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Topic paper for the WJUR BPH-issue invited by Dr. Oelke.
Melinda Wuest, Lambertus P. Witte have equally contributed to the manuscript.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Wuest, M., Witte, L.P., Michel-Reher, M.B. et al. The muscarinic receptor antagonist propiverine exhibits α1-adrenoceptor antagonism in human prostate and porcine trigonum. World J Urol 29, 149–155 (2011). https://doi.org/10.1007/s00345-011-0655-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-011-0655-6