
Abstract
Background
Despite its popularity, acceptability, and convenience, the oral route is not the classical route for the administration of all critical bioactives including lipophilic drugs, proteins, and peptides. Recent advances in drug delivery have identified the transdermal route as a compelling alternative channel for improved delivery of essential biomolecules due to the illuminating advantages derived from this route. In order to circumvent the poor permeation of the stratum corneum by transdermal patches, microneedles (MNs) technology, which combine the advantages of parenteral delivery using hypodermic needles and transdermal delivery, has been unveiled as a novel biomimetic technology for efficient and effective transport of payloads across the stratum corneum.
Main body of abstract
The concept of MNs was first documented by Chambers in 1921 when he reported some problems encountered during experimentation using Echinoderm eggs. Since the first patent recorded in 1976, there has been consistent interest and funding in development of MNs for various biomedical applications. MNs have been developed and classified based on their physical attributes and functional profiles into solid, coated, hollow, dissolvable, and swellable or hydrogel-based MNs. These devices are fabricated using advanced techniques like 3D bioprinting, laser methods, photolithography, and molding, and applying materials such as carbohydrates, silica, ceramics, metals, glass and polymers. MNs could be characterized based on their morphological, geometrical, surface, mechanical properties, biocompatibility, and permeability profiles. Evidences have shown that MNs could be commercialized for various clinical adaptations. The numerous biomedical applications of microneedles in drug, peptide, and protein delivery attest to the versatility and dynamic nature of the fabrication techniques, and the pliability of the formulation materials. In spite of the enormous potentials of MNs, extant literature has shown that MNs also have their own share of limitations like every novel technology designed for theranostic purposes.
Short conclusion
In this review, we have escalated discussions on the progress and advances made in the development and use of MNs by summarizing the benefits, limitations, fabrication techniques, fabrication materials, characterization methods, therapeutic applications, sterilization and stability considerations, safety and toxicological concerns, regulatory guidelines, and tips for successful commercialization of MNs.
Similar content being viewed by others

Background
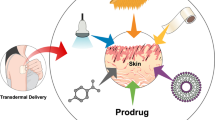
As the most acceptable, prominent, and convenient route for administration of bioactives, oral drug delivery enjoys wide acceptance across all groups of patients (pediatrics, adults, and geriatrics), despite its known disadvantages like first-pass metabolism of drugs, low bioavailability for lipophilic drugs, poor compliance in severe illness. e.g., vomiting, coma, unconsciousness, etc. Parenteral injections, which provide rapid onset of activity of therapeutics with high bioavailability, is limited by low patient adherence, excessive anxiety, pain at injection site as well as rapid manifestation of adverse effects. Over the years, several researchers and formulators have made pivotal attempts at developing advanced and newer strategies and techniques for seamless targeted delivery of drugs and other biomolecules with low side effects. A few of these strategies have progressed from the laboratory scale to the industrial batches for final use in the clinics, while some interventions are still undergoing clinical trials. Of these attempts, the transdermal route has been favored as a vital pathway for enhanced delivery of biomolecules due to its illuminating advantages including absence of pain at administration site, increased patient compliance and decreased anxiety, excellent ease of administration, impressive flexibility of formulation design, use of simple operations to develop systems with sophisticated clinical performance, and possibility of accomplishing improved therapeutic outcomes with low cargo load, and provision of sustained drug release [1, 2]. However, it is difficult for transdermal patches to permeate the stratum corneum barrier for deep drug deposition. This challenge has been confronted by formulating transdermal drug delivery systems incorporating chemical penetrating materials (CPM) like esters and fatty alcohols or through the application of physical methods including electroporation, laser microporation, and iontophoresis. Skin allergies, inflammation, and irritation resulting in decreased product acceptability and patient adherence are possible drawbacks of the incorporation of CPM in transdermal drug delivery systems in addition to adverse and destructive interaction between the active pharmaceutical principles due to molecular incompatibility. The physical methods of improving transdermal drug delivery are expensive and do not guarantee reproducible delivery of encapsulated payload. Further, these methods are sophisticated because they require state-of-the-art equipment and high technical skills, which might not be readily and easily available in the industry [3]. Considering these challenges, it is very imperative to explore other options provided by nanotechnology like microneedle-based drug delivery, which might not require high sophistry to attain efficient and effective transdermal drug delivery. Therefore, this work is aimed at evaluating the recent and emerging perspectives in the application of MN technology as precision tool for drug, peptide, and protein delivery by summarizing its benefits and limitations, and discussing the fabrication techniques and materials for fabricating MN. In addition, characterization methods and biomedical applications of MN will be addressed. Likewise, sterilization and stability, safety and toxicological concerns, and regulatory guidelines and tips for successful commercialization of MN will be covered. The limitations of transdermal drug delivery system are illustrated in Fig. 1.

Schematic illustration of the limitations of transdermal drug delivery system
Main text
Drug disposition using microneedles
Since the innovative concept of microneedles (MNs), a smart delivery device, was first patented in 1976 to its initial public description as an essential tool for transdermal delivery of therapeutics, it has attracted increasing interests and researches from various laboratories as well as funding from grant awarding bodies and companies. This is because MNs can be developed as an easily adaptable, affordable, biocompatible, and flexible device for non-invasive and throughput distribution of biomacromolecules, drugs, vaccines, and micromolecules [4]. The skin is an important beneficiary of this technology because it circumvents physiological stresses on the skin like inflammation, pain, discomfort, and irritability, to enhance transdermal delivery of biomolecules. MNs are described as polymeric devices showing smooth, needle-shaped projections measured in micrometers (up to 2500 µm) and supported by a flexible base impregnated with biomolecules for therapeutic and diagnostic (theranostic) purposes. Essentially, it is a hybrid device that embodies the functional advantages of transdermal patches and hypodermic needles [5,6,7]. It has been used to facilitate, consolidate, and accomplish transdermal delivery of therapeutics across the stratum corneum and into the viable epidermal structures of the skin maintaining the desired local therapeutic concentration for a prolonged period of time, while evading any intimacy with the nervous and venous structures of the dermis, which could trigger inflammatory or immunological damages. Therapeutic agents encapsulated in MNs include drug compounds, peptides, micromolecules, hormones, vaccines, genes, and proteins, for use in chronic wound healing, inflammatory skin conditions, tissue regeneration, tissue printing, cellular therapy, and diabetes mellitus. In addition, several MNs patents have been obtained, some devices are undergoing clinical trials, and scholarly publications on MNs have been documented which present cocktails of information on MNs including fabrication techniques, advantages and disadvantages, characterization methods, and biomedical applications [5, 8, 9]. In spite of its numerous advantages including production of excellent reproducible drug bioavailability devoid of inter-patient variability, MNs possess certain limitations like irritability due to sensitive skin especially if the hair-thick tips of the needles are broken under the epidermis. However, this is a rare occurrence and could be completely avoided by designing and carefully implementing a systematic quality systems during MNs development and complying with instructions during use. Various types of MNs have been fabricated and described including hydrogel-based, hollow, solid, and dissolving MNs, which were formulated using polymers, silica, glass, and sugars through technologies like lithography, thin-film deposition, micromolding, etc. [10, 11]. Biomedical dispositions of microneedles are illustrated in Fig. 2.

Schematic illustrations of the disposition of microneedles to various biomedical objectives
Types of microneedles
Microneedles are fabricated and classified according to their physical attributes and functional techniques as discussed in this section.
Solid microneedles (poke and patch-type)
Solid microneedles puncture the skin layer and deliver payloads to the desired site [12]. Initially, solid MNs were utilized for skin preparation before administering APIs from an external reservoir through the poke-and-patch technique [10]. It is possible to employ solid MNs both with and without engineered drug molecules [13]. Integrating these MNs into a smart patch system helps to achieve controlled drug delivery [14]. These systems enhanced the detection of biomarkers that are most commonly used in clinical laboratories and hospitals with the help of lab-on-a-chip technology [15]. According to a report, it was claimed that using solid MNs enhanced ex vivo transdermal absorption [16]. Compared to conventional approaches used for vaccine delivery, delivering vaccines with a solid MN is advantageous since it lasts much longer and strengthens the immune system [14]. Interstitial fluid (ISF) can also be extracted easily using solid MNs [17]. Solid MNs have some drawbacks, including patient inconvenience, prolonged occlusion time, and increased risk of microbial infection [18]. The stratum corneum is intended to be penetrated by the microneedle structure to optimize drug administration by forming microchannels throughout the layer to the dermis and increased bioavailability and distribution throughout the skin [19]. Silicon, metals, and polymers can be used to manufacture solid microneedles [10]. Solid MNs enhance the penetration of substances through the skin making it possible to administer macromolecules transdermally [20]. Some MNs rollers like Dermaroller®, Medik8®, and other commercially available MNs devices initially created for cosmetics applications have been modified for drug delivery [16].
Coated microneedles (coat and poke-type)
Coated microneedle is prepared by coating solid MNs with the drug solution [21]. Drug loading could be calculated based on the thickness of the coat, and it usually contains a low amount of the drug [22]. Following the insertion of the coated MNs into the skin, the entrapped molecules dissolve and permeate into the skin (coat-and-poke approach) [23]. This is a one-step application process that is simple and convenient for use [24]. Drug-coated microneedles have the benefit of staying active for a long time. Hence, their usage is restricted to potent biomolecules with dosing usually confined to microgram levels [25]. Current developments in coated MNs enable various applications, including the transport and detection of biomolecules, and provide a transdermal delivery system that is more regulated and effective in distribution than the skin pre-treatment method [21]. A functional coating layer can change the biocompatibility and mechanical robustness of coated MNs [23, 24]. PVP and other biocompatible materials are used to coat the probe layer [16]. To avoid using silicon and metal, which are less biocompatible materials, coated polymeric MNs have also been studied in recent years [26]. Agents like peptide stabilizers, viscosity enhancers, and surfactants are used to achieve coating homogeneity, thickness, and active stability [27]. According to an in vivo experiment, coated MNs produce longer-lasting drug levels in the sub-epidermal layer than those produced by subcutaneous injection delivering a reproducible blood concentration [18]. It was also shown that MN patches caused rapid peak plasma levels three times quicker than what was observed following the administration of the subcutaneous comparator, which was likewise independent of the target site [28].
Hollow microneedles (poke and flow-type)
The hollow microneedle has a vacant, hollow core or compartment, which retains drug solutions [10]. This technique helps in the administration of larger amounts of encapsulated drugs than solid and coated MNs, which can only deliver small amounts of payloads [16]. Hollow MNs consist either a solitary needle or an array of numerous needles with different bore diameters (5–70 m wide), which can be fabricated using silicon, metals, or glass [27]. The microneedle bore permits drug administration either passively by diffusion or under pressure from a syringe, pump, or gas [21]. Hollow MNs facilitate flow of the drug solution at 10–100 L/min and continuously deliver its content into specific skin layers (poke and flow). This system is commonly used to administer vaccines and insulin followed by collection of blood and ISF samples for prompt evaluation to quantify and distinguish the analytes present in the body fluids [7, 16]. In accordance with this methodology, analytes (e.g., protein, ions, or glucose in body fluid) would be identified through hollow MN-based sensing systems [29]. Hollow MNs are simple to manufacture, inexpensive, and accurate in controlling drug release from the liquid mixture [30]. An array of MNs also can incorporate a microfluidic chip or micropump to achieve regulated API delivery [31]. Delivering dry formulations, typically utilized to enhance medication stability and simplicity of patch-based delivery, is difficult when reconstituted [29]. The main disadvantages of hollow MNs are technical problems including drug leakage and blockage during administration. To circumvent this drawback, a side opening with off-centered perforations is created [10]. In contrast to solid MNs, hollow MNs are significantly weaker and deserve special attention with regard to needle design and insertion technique [12].
Dissolvable microneedles (poke and release-type)
Considering their attributes, dissolvable microneedle is a promising drug delivery device [10]. Two essential qualities of dissolvable MNs include one-step drug delivery, which facilitates simple medication administration, and the quick release of therapies and biotherapeutics [32]. Besides APIs, soluble matrix including biocompatible polymers or sugars makes up dissolvable MNs [21]. When it contacts the interstitial fluid, MN tips disintegrate releasing the API (poke-and-release approach) [33]. This method is considered superior to others because of the improvement in applying MNs that dissolve after poke and release [34]. When the skin is pierced by the MNs, they dissolve and the breakdown of the needle tip causes the entrapped bioactive to release and distribute [30]. Because of the fact that the rate at which the constituent polymers disintegrate affects how fast the active component is released, drug distribution can be regulated by varying the polymer composition and its use concentration or production process [35]. This class of MNs have good patient compliance and biocompatibility because they are often made with hydrophilic biodegradable polymers or sugars [4]. The micromold fabrication approach is best-suited for manufacturing dissolvable MNs [10]. A sound technical skill is necessary to develop and manufacture dissolvable MNs. Since safe polymers can be employed as raw materials, dissolvable MNs offer a high biocompatibility and loading capacity [25]. However, the major drawback in the clinical application of dissolvable MN is polymer accumulation within the skin, and this is not safe for prolonged use [18]. Since this allows API delivery without generating sharp, non-biodegradable, and bio-contaminated waste materials, dissolvable MNs are becoming increasingly popular and recommended [34]. In addition, it significantly reduces the price of synthesizing MNs due to use of artificial and semisynthetic polymers and polysaccharides. The patient benefits greatly from polymeric MNs that dissolve into the skin after insertion. A one-step medication delivery method provides a user-friendly interface because the medication is kept inside the needles [36]. Due to the total dissolution of the MNs upon application, making it impossible to re-insert the needles into another patient, the chance of infection transmission or needle stick injury is diminished. In comparison to solid and hollow MNs, dissolvable MNs are considerably safer [10].
Hydrogel MNs (swelling microneedles-type)
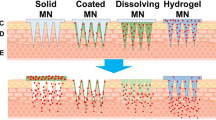
Hydrogel MNs, originally introduced in 2010, swell and increase in size after API is loaded, and through enlarged MNs, it is delivered from the patch [13]. Compared to biodegradable or dissolvable MNs, hydrogel MNs work by inserting a needle into the skin, releasing the payload, and dispensing the needle [37, 38]. Since the hydrogel is hydrophilic, the microneedles will absorb interstitial fluid and swell when it is introduced into the skin. Thus, materials with good swelling characteristics and biocompatibility are usually applied to create hydrogel-based microneedles [39]. This innovative method uses integrated systems which project cross-linked polymeric particles from the solid substrate containing the API. After injection, the interstitial fluid in the tissue is swiftly absorbed by the needles causing the API to diffuse through swollen MNs [40]. Amylopectin and ultra-low viscous carboxymethylcellulose (CMC) have been used to fabricate hydrogel MNs. They were effectively dissolved in the skin after combination with sulforhodamine, bovine serum albumin, or lysozyme, enabling bolus or sustained release administration. Noticeably, the skin was undamaged and free of any polymer remnants after removing the hydrogel MNs [17]. Hydrogel MNs lower the danger of infection transmission as they are sufficiently soft to prevent reapplication. They maintain good mechanical strength, although slightly deformed and can load higher amount of drugs than dissolvable MNs [37]. The different types of microneedles are illustrated in Fig. 3.

Schematic illustration of the different types of microneedles showing A solid B hollow C coated D dissolving, and E hydrogel-forming microneedles. Reprinted from [158]. S. Sharma, K. Hatware, P. Bhadane, S. Sindhikar, D.K. Mishra, Recent advances in microneedle composites for biomedical applications: Advanced drug delivery technologies, Mater. Sci. Eng: C. 103 (2019) 109717. https://doi.org/10.1016/j.msec.2019.05.002, Copyright (2023) with permission from Elsevier
Benefits of microneedles array
Drug delivery
Microneedles (MNs) are effective in delivering molecules of various sizes, including small molecules and biomolecules such as proteins, peptides, genes, and vaccines for viruses like SARS, MERS, and COVID-19. In the cosmetic industry, MN patches incorporating hyaluronic acid (HA) have been applied directly to the skin to improve skin health due to the moisturizing effect of HA. Transdermal delivery using MNs also bypasses first-pass metabolism and enzymatic degradation, thereby improving the efficacy of administered drug over conventional methods like the oral route. Fractional dosing or dose-sparing effect of drugs within microneedles allows enhanced vaccine efficacy when resources are limited and regulated like in the case of pandemics. Temporary and reversible disruption of the skin during MNs insertion reduces skin irritation and the risk of infection. As microneedles can be fabricated using biocompatible materials, they eliminate any cases of inflammation or toxic reactions in the body. Trained personnel is not required for administration as MNs are easy to use but self-administration by the patient improves compliance. MNs design can be modified to meet delivery requirements such as sustained or burst release or combination drug delivery for a specific patient population, and length of microneedles can be modified for targeted drug delivery to precise layers of the skin [41].
Flexibility of microneedles
Microneedles need to be flexible enough to reshape themselves to the surface it is being applied, especially in wound healing applications. Using lithographic techniques, it is possible to fabricate microneedles flexible enough to treat difficult-to-reach areas in cases like chronic wounds where there is a disruption of the skin structure and interference to conventional therapies caused by biofilms generated by the bacteria present. According to a report, MNs were fabricated using a polyethylene terephthalate substrate and loaded with polyvinylpyrrolidone-calcium peroxide to combat tissue hypoxia and antibiotic resistance in wounds. The MNs showed sustained release of oxygen for 6 h leading to better antibacterial activity in both gram-positive and gram-negative (Staphylococcus aureus and Pseudomonas aeruginosa) bacteria and improved oxygen delivery from 8 to 12 ppm to hypoxic wounds over 2 h resulting in better wound healing [42].
Cost of fabrication
To enable seamless translation of microneedles to clinical settings, affordability must be considered. Despite the potential benefits of this relatively new technology, there is still a need for a proper economic evaluation of microneedles, as their fabrication process is complex, their storage requirements are demanding, and the approval process can be time-consuming [5]. A cost-effective method for developing master templates for microneedle patches involves modifying commercially available stainless-steel templates used for tattoo needle cartridges. Polydimethylsiloxane (PDMS), a commercial solution with high flexibility and low adhesive properties, was used to modify the templates. This method supported the removal of polymeric microneedles from the mold and is stable at high temperatures [43]. Fabricating microneedles using microfabrication technique and natural polysaccharides such as chitosan, alginate, and xyloglucan could reduce the cost of production. Particularly, polymeric microneedles made from chitosan-PVA have shown a cumulative release of 20.18% of diclofenac in vitro in 30 h, indicating their potential use as a drug delivery system. This approach is far more economical compared to the use of metals or silicones to make microneedles, which could result in increased cost of production [44].
Safety of microneedles
Various clinical researches confirm that microneedles are safe and effective and do not cause systemic infections, though they are applied to the skin and penetrate the stratum corneum [45]. Skin permeation studies indicated that after microneedle insertion, the skin layer remained intact with no visible injury and microchannels formed precluded S. aureus bacteria transfer across the skin [46]. Studies on microbe permeation did not show signs of E. coli infection when microneedles were delivered to the anal sphincter muscle [47]. However, skin infection owing to skin puncture during microneedle application is always a possibility. In this scenario, MNs have a quick skin-sealing function that prevents microbiological infiltration. Dissolvable MNs are potentially used as they minimize skin punctures, thus reducing the chances of infections [20].
Limitations of microneedles delivery technology
Microneedles have limited drug-carrying capacity prompting difficulties in incorporating drugs with large doses. Polymeric MNs have low mechanical strength and break easily. In some cases, polylactic acid has been used to impart mechanical strength to MNs. The elastic nature of the skin prevents penetration of microneedles and delivery of entrapped drug to the target sight. Accurate dosing with MNs requires factors such as thickness, elasticity, and hydration of the skin to remain constant. Manufacturing microneedles with high-temperature conditions would create challenges in the delivery of thermolabile drugs, scarcity of materials viable for microneedle fabrication, and obstruction of microneedle bore, resulting in low penetration and efficacy. Lack of regulatory guidelines in manufacturing protocols, and poor quality control standards for large-scale manufacturing also hinder development of microneedles [41].
For MNs to show good activity and patient compliance, it depends on factors like the geometry of the MNs, more specifically the shape of the MNs, the diameter of the tip and base as well as the interspacing between microneedles. Delivery of drug and penetration of the MNs at the target site also depends on the health status of the skin, management of the MNs applied on the skin, and material used for the fabrication of the MNs. Depending on the drug of interest and application, certain parameters of MNs such as geometry and composition can be modified for accuracy in drug delivery.
Shape of the microneedles
In a recent study, simulations were performed using computer tomography (CT) scans to determine the mechanical strength, integrity, and penetration of microneedles. It was found that the buckling force of MNs increased as the number of vertices increased (from triangle, square to hexagonal), meaning that MNs with a triangular base will fail first due to buckling. Also, the penetration of microneedles was tested by keeping factors such as needle length and interspacing constant, and changing only the cross-sectional shape of the MNs. This showed that triangular and square base microneedles possess higher penetration potentials compared to hexagonal microneedles [48]. The viability of immunization by the transcutaneous route using dissolvable microneedles with varying needle shapes to deliver ovalbumin (OVA) was studied by Li et al. [49]. It was found that geometry plays an essential role in penetration efficiency and mechanical profile of microneedles because more than 95% of the cone-shaped dissolvable MNs penetrated the skin and the penetration ratio was only 40% in the case of cone-cylinder dissolvable MNs. The hexagonal pyramidal and rectangular-shaped dissolvable MNs showed less penetration efficiency than the cones owing to its dimension. The cone dissolvable MNs also showed 80% fraction of dissolution to the length of needle, while cone cylindrical dissolvable MNs recorded a meager 40%. Zoudani et al. [50] developed a new type of microneedle consisting of a cone with an array of hemispheres. This was proposed to be an improvement over dissolving microneedles of conventional shapes. It was claimed that the drug flux and final drug concentration were higher in tissues due to the unique structure of the hemisphere, resulting in the resolution of inadequate dose administration, which is a common problem in dissolving microneedles.
Tip diameter and sharpness
An investigation assessed the penetration depth and insertion force of MNs in ex vivo skin samples using microneedles with varying tip diameters (5, 15, 24, and 37 µm). It was observed that skin penetration increased linearly with smaller microneedle tip diameters. It was also concluded that force at initial drop increases linearly with the tip diameter and is directly related to the r (radius) of the tip. However, as the tip diameters cross a certain threshold (> 80 µm), the force at initial drop is directly proportional to r2, leading to the conclusion that smaller tip diameters (< 15 µm) are needed for smooth penetration of microneedles into the skin [51].
Force of application
Efficient delivery of drug also depends on the force applied to the microneedles and the elasticity of the skin. If the skin is too elastic, the microneedles push the skin instead of piercing the skin to deliver the drug, resulting in low efficiency of delivery [52]. Dissolvable microneedles have been shown to have an inconsistent release of encapsulated drugs into the skin as the physicochemical property of the skin does not allow complete insertion of dissolvable MNs. A new type of micropillar-dissolvable MNs was fabricated by Lee et al. [53]. The micropillars act like applicators helping in equally distributing the force across the microneedles giving proper insertion into the skin and allowing for a uniform release of the encapsulated drug into the stratum corneum.
Dose limitations
Microneedles have a small drug-loading capacity due to their size constraints. As a result, achieving a continuous drug release or patches with larger doses becomes impractical as microneedle patches need to be applied with higher frequencies to meet daily dose requirements. However, this might lead to poor patient compliance. Improving the solubility of poorly soluble drugs will result in greater drug loading onto microneedle patches. Considerable research has been done on solubilization techniques to improve the hydrophilicity of poorly soluble drugs. One such example is the work done by Kearney et al. [54] on developing hydrogel microneedles with reservoirs. Co-solvents such as PEG 400 and propylene glycol were used to improve the solubility of the hydrophobic drugs, olanzapine and atorvastatin. In vitro permeation study found a direct correlation between the drug loading effect and permeation because increasing the concentration of the drug in the liquid reservoir resulted in a multi-fold increase in permeation across the porcine membrane with the drugs reaching the target compartment within 15 min of MNs application.
Sustained release in microneedles
One of the problems with microneedle delivery is the sustained drug release in the body, which needs extensive patch-wearing hours for optimal drug administration. In a study, easily separated microneedles were used to reduce the time a patch stays on the skin and records sustained drug release. The concept behind separable microneedles is that medications that are coated on dissolvable microneedles, when applied, create cracking at the tip-base contact and allow the microneedles to split and penetrate the skin, eliminating the need to leave the patch on the skin for long periods, enabling good patient compliance and generation of only blunt waste material which can be safely discarded [55]. Li et al. [56] developed separable microneedles using biocompatible polylactic acid–polylactic-co-glycolic acid (PLA–PLGA) for controlled release of levonorgestrel (LNG) and impart mechanical strength to deliver LNG for better control on fertility. PLA-PLGA microneedles underwent slow biodegradation after insertion coupled with the hydrophobicity of LNG resulting in sustained delivery of LNG of over 45 days in vivo, with the release profile comparable to ideal kinetics of once-a-month contraceptive patches [56]. Similarly, effervescent MNs have also been developed to reduce patch application time and provide sustained release of LNG for > 1 month [57].
Materials for constructing microneedles
The materials used for manufacturing MNs are crucial in determining their therapeutic efficacy, manufacturing process, distribution within the body, and stability of entrapped molecules. Previously, materials such as glass, silicon, and metals were commonly used for creating microneedles, which were classified as either biodegradable or non-biodegradable. Non-biodegradable materials like metals, silicon, and ceramics are still used, while biodegradable materials such as polysaccharides and polymers have gained increased interest due to their biocompatibility and ability to overcome natural barriers. Recent advances in polymer technology have facilitated the use of biocompatible polymers in fabricating MNs that possess desirable physicochemical properties, can be easily fabricated, and are compatible with loaded bioactives and physiological functions. To be suitable for bioapplications, the material used for MNs should have excellent tensile strength, biocompatibility, and must be safe for both socioeconomic and health reasons. In some cases, the material must also be able to modulate drug distribution in a sustainable or controlled manner [58]. Additionally, the material should be easily moldable and resilient enough to withstand fabrication and transportation while also degrading effectively within the biological system. Some of the materials for creating MNs are discussed below.
Silicon
Silicon is commonly used in making biochemical detectors, drug delivery devices, and medical implants. Its biocompatibility has been studied for several years, but evidences of its safety are limited. Non-porous silicon has been shown to have low toxicity, which is why it is commonly used in drug delivery. However, there is a risk of chipping or breaking off in tissues during treatment because silicon is brittle, but workers have found that functionalizing silicon with nontoxic metals like gold increases their effectiveness. One example of an FDA-approved device that uses silicon is Micronject® [58]. It would be interesting to investigate the long-term effects of using silicon MNs on tissues since most studies have only reported short-term use. Silicon is expensive to produce and requires a sterile environment. Typically, isotropic and/or anisotropic wet and/or electrochemical deposition processes are used to create MNs profiles on the surface of a silicon chip. For porous MNs, the silicon must be deeply etched on the backside and then matched to the front side sequence. This process requires precise alignment and irradiation. A recent production process for creating MNs for deep brain medication infusion involves attaching a silicon backing layer with predetermined pores to a glass sheet using electrochemical methods [59]. Researchers have created silicon MN grids to deliver gene siRNA to the outer ear of rats and also manufactured long, porous silicon MNs for drug administration. However, solid silicon cannot be broken down by body enzymes and may cause inflammation and stiffness. On the other hand, porous silicon has shown bioactive capability and can bind to healthy cells, making it a biocompatible material [60]. Permeable silicon can be hydrolyzed by biological organisms in alkaline environments, and high-porosity silicon is used in sustainable drug carriers. The release rate of drugs from porous silicon depends on how they interact with the material. It might be surprising to learn that, despite the challenges involved in producing silicon MNs, silicon still has the largest market share in the industry. This is due to the demanding and expensive multi-component production process, as well as the need for specialized sterile equipment. Furthermore, the standard sizes of silicon MNs may not be sufficient for certain medical applications such as drawing blood or accessing blood vessels and nerves. This is because current production techniques for constructing silicon MNs are incompatible with fast manufacturing and lack the flexibility that fabrication techniques like 3D bioprinting can offer [36].
Metals
MNs are made of metals due to their advantageous mechanical and biomedical properties, such as high durability and toughness. Although metals are stronger than silicon, they are less prone to breakage. However, the use of metal MNs for skin penetration may cause negative reactions [61].
Carbohydrates
MNs utilize carbohydrates, such as cellulose, sugars, hyaluronic acid, and synthetic derivatives, either alone or in combination, as an essential component. These carbohydrates are easily recognized and absorbed by the skin and are similar to the natural microenvironment. MNs are specialized tools that can penetrate the skin layers and produce localized or systemic effects. Polysaccharides are macromolecules that have been widely used to create MNs because of their unique physical properties. The diverse range of organic compounds found in complex carbohydrates allows for tunable features and functions in the design and engineering of MNs. Carbohydrate-based microarrays can improve bioactive delivery, detection, and natural defense due to their significant capabilities. Carbohydrates are considered safe for use in MNs as they are metabolized and excreted by the renal system. However, their physical properties and interactions with pharmacological agents can affect drug release, penetration, and biological activity. Properties such as polymer weight, moisture content, and contact with active substances can influence the rate of drug release. Carbohydrates can be categorized as disposable, dissolvable, or lipophilic polymers, and these properties can impact in vivo behavior. Chitin and starch are disposable, dextran and sodium chondroitin sulfate are dissolvable, and methylacrylated hyaluronic acid is a lipophilic polymeric microarray. Using carbohydrates in MNs has numerous advantages including physical compatibility, non-toxicity, biodegradability, and renewable nature, although there are also various obstacles related to their use such as the lack of standardization, variability in form due to source and processing, and inherent changes that may occur over time or during development [62]. The use of carbohydrate-based microneedles can offer several benefits and drawbacks, depending on the specific type.
Sugars
Sugars are a desirable substrate for fabricating MNs due to their safety and biodegradable. Maltose is the most commonly used sugar, but other sugars such as xylitol, trehalose, galactose, mannitol, and sucrose have been used. These natural sugars play an important role in drug delivery systems and can exert specific biochemical actions based on their molecular configurations and chemical bonding. There are passive and active drug targeting methods using sugars for targeted drug delivery to tissues, organs, and cells. In spite of this, there is a dearth of literature regarding the effective and appropriate use of sugars for transdermal drug delivery to the epidermis and/or dermis. Researchers have designed and produced sugar MNs for percutaneous drug delivery and their sizes ranged from 150 to 2 mm and were made of maltose blended with active biomolecules. To test their tolerance on healthy human skin, a clinical trial was conducted on 10 healthy adult volunteers. Microneedles that were 500 µm in size and contained 5% of ascorbate-2-glycoside were embedded into the forearm, cut off, leaving them in the skin. These microneedles dissolved spontaneously through hydrolysis, releasing ascorbate into the epidermis and dermis [63].
Hyaluronic acid
The bioadhesive joint and matrix proteins contain an important component called hyaluronic acid (HA), which is a negatively charged biopolymer that is highly soluble in water. To address skin cancer, dextran nanoparticles were loaded into cross-linked HA MNs to create a nanotechnology-based delivery system. The nanoparticles were evaluated using an acid degradable polymeric matrix consisting of a dextran derivative, alginate, glucose oxidase, and programmed cell death protein-1 (PD1). This microdevice works by converting glucose to gluconic acid, which triggers the release of antibodies at the site of the melanoma [64]. MNs were fabricated with tips containing HA that dissolved within 30 s. The study assessed topical administration and permeability using fluorescein isothiocyanate labeling (FITC). In vivo experiments showed a burst release in the first 30 s, with nearly complete dissolution of the tagged dextran within five minutes. MNs produced comparable pharmacokinetic profiles to subcutaneous injection in rats with type 2 diabetes, indicating possible utility as a substitute therapy for type 2 diabetes [36]. In a different study, HA MNs were combined with adipose-derived stromal vascular fraction cells and polymers to improve the healing of diabetic wounds. The cells with HA microneedles demonstrated better wound healing effect compared to using cells alone indicating a new approach to wound healing [65].
Cellulose
Carboxymethylcellulose and hydroxypropyl methylcellulose are hydrophilic polymers that possess various characteristics such as viscosity modifiers, adhesives, emulsifiers, and coating materials. These polymers are utilized to fabricate microneedles for the treatment of Alzheimer's disease, where donepezil HCL is used and the tip, which is loaded with hydroxypropyl methylcellulose for animal/human testing, revealed that drug release commenced within 5 min of insertion, and complete dissolution of microarrays occurred in the skin within 15 min [66]. To promote hair regrowth, MNs were developed using carboxymethylcellulose-loaded with valproic acid. The release of valproic acid was found to be increased and compared to topical formulations leading to an increase in hair follicle regrowth [67].
Starch
Starch is a commonly used biodegradable polymer in medical applications due to its ease of use and ability to form films. However, it can be brittle and is often combined with other polymers. Pullulan, a hydrophilic biomacromolecule produced by Aureobasidium pullulans in starch and sugar-based fermentation, is a vital biomaterial in medical use. It has novel properties including excellent resistance to oxygen, strength, stability, transparency, film-forming ability, and non-toxicity and lack of mutagenicity. This makes it an ideal component for manufacturing MNs. While starch is a popular biopolymer, the exceptional qualities of pullulan make it an essential ingredient for biomedical applications, particularly in the production of MNs [63].
Chitosan
Chitosan and chitin-derived biopolymers have been employed in creating MNs mostly for hydrophilic drugs, hormones, proteins, and peptides. Chitosan, owing to its acidic nature, and positive charge that enhances adhesion to tissue and mucosal surfaces. It is broken down through the hydrolysis of acetylated residues, and its rate of degradation is affected by its degree of deacetylation and molecular weight. Chitosan has been acknowledged by the FDA as generally recognized as safe (GRAS), and it is extensively utilized in wound dressing, repairing cartilage, and producing MNs for regulated and prolonged administration of drugs. To enhance the performance of chitosan MNs, a biodegradable material composed of poly (l-lactide-co-d, l-lactide) was utilized to prevent the formation of impressions after piercing, and impressions were found to be absent after six hours. In vivo experiments showed that half of the antigen was released in the initial two days, and a minor fluorescence was evident during the manufacturing process of MNs [68]. Chitosan has garnered significant attention as a biomaterial for transdermal and topical drug delivery due to its biodegradability, biocompatibility, and ability to form films. The amine and hydroxyl groups on chitosan allow for modification to achieve desired functionalities and strength. Moreover, chitosan does not elicit an immune response inside the body, making it an ideal biomaterial for the fabrication of MNs [69, 70].
Polymers
Microneedles (MNs) have become increasingly popular as a transdermal drug delivery technique due to their ease of use, simple administration, and potential for improved patient compliance. The ability to produce customized MNs that can encapsulate a broad range of pharmaceuticals and biomolecules, as well as their performance as diagnostic tools, demonstrate their significance in the field. In the beginning, biopolymer-based microneedles were preferred due to their safety, biocompatibility, and biodegradability. However, synthetic polymers with enhanced physical resilience, pliability, and ductility have demonstrated greater potential for commercialization. Microneedles made from synthetic polymers have been used to administer vaccines, protein/enzyme-based therapeutics, and cytotoxic drugs. MNs are made from a variety of synthetic polymers including like polylactic acid, polystyrene, polyvinylpyrrolidone, poly(methylvinyl ether), polyglycolic acid, poly(lactic-co-glycolic acid), and polycaprolactone [1, 71]. The Gantrez® AN139-containing MNs were manufactured using the micromolding technique. These needles had a height of 600 µm and a width of 300 µm. Studies using optical coherence tomography revealed that these MNs penetrated the skin 460 µm deep. MNs penetrated the skin with force greater than 0.03 Newton per needle [72]. MNs containing amphotericin was fabricated using Gantrez® AN-119 by micromolding technique. Properties of MNs were explored using two different concentrations of amphotericin B 4% and amphotericin B 8%. For the 8% drug concentration limit, the load displacement value per needle was measured at 0.54N, and for the 4% limit, it was measured at 0.65N. According to the Franz diffusion studies, 88.88% of the drug successfully reached the skin and the zone of inhibition against Candida albicans for 8% drug-loaded MNs was 40 nm [73]. Micromolding was used to fabricate doxorubicin (DOX)-containing polystyrene MNs. Stability studies revealed that adding DOX to MNs improved the stability of DOX. Through scanning electron microscopy, the length of MNs which was found to be 451.02 ± 8.07 µm and the tip diameter was 1.93 ± 0.49 µm. Skin integrity evaluation revealed that skin disruption was not caused by the base of the MNs, and transepidermal water loss (TEWL) experiments further supported this claim [74]. The administration of meloxicam through MNs improved its anti-inflammatory effects. PVA and polyvinylpyrrolidone were combined to fabricate MNs in a 9:1 ratio. Axial needle fracture force for these MNs was 0.9N, and 100% of meloxicam was released in 1 h with drug deposition of 63.37% in the skin, which was 2.58 times more than meloxicam solution [75].
Glass
Glass is used in MNs production because it is simple to use, easily sterilized, biocompatible, and able to bear high pressure and temperatures [76]. To develop an intraocular device, hollow glass MNs were combined with polydimethylsiloxane (PMDS). Glass provided sufficient strength to pierce the eye, and PMDS was employed as the substrate since it provided flexibility to the device. It was discovered that delivery of 6-aminoquinolone and Rose Bengal using this device was clog-free and unaffected by their chemical characteristics and molecular weight [77]. Similar experiment was conducted for delivery of micro- and nanoparticles to the suprachoroidal space via single MNs to reduce the frequency of dosing [78].
Ceramics
Ceramics are crystalline complexes consisting of mixtures of metal and nonmetal compounds, such as silicon and nitrogen, calcium and oxygen, and aluminum and oxygen (alumina). Ceramics can be used to fabricate MNs since they are physically and chemically inert. Their biocompatibility and ease of production make them one of the favorite candidates for manufacturing of MNs [79]. Delivery of memantine was explored using ceramic nanoporous microneedles, which were prepared using micromolds and double replication process. Thickness, diameter, and reservoir capacity were the factors that influenced drug release from the MNs, although salt concentration and buffer volume had no bearing on the release profile of the drug. The order of release also changed as memantine concentration changed. It used zero-order kinetics for loading at 50 and 100 mg/ml, while first-order kinetics was observed for 35 mg/ml [80]. Both extraction and transdermal drug administration can be done using ceramic MNs. Microporous MNs were prepared using centrifugal casting. Pore size was found to be 1–1.5 µm. These pores improved the biocompatibility, drug loading, and physical stability of the microporous MNs. These MNs had a 95% penetration efficiency, and the skin recovery time was 30 min. Appropriate porosity with good interconnectivity and surface area resulted in detection of glucose in just 15 min with high precision. Insulin delivered via these MNs was found at the depth of 600 µm. In Franz diffusion apparatus, 80% of total insulin was delivered in 4.5 h, indicating that microporous ceramic MNs could be utilized for high loading and faster release of larger molecules [81].
Microneedles fabrication techniques
3D printing
3D printing or additive fabrication is a technology that uses virtual computer-aided designs (CADs) to create physical objects by continuously creating layers. 3D printing provides a wide variety of prototyping and manufacturing processes and one-step manufacturing of highly complex and reproducible objects [82]. 3D printing is a form of photopolymerization technology, which includes continuous layer polymerization of UV-sensitive polymers via a healing process. Digital light processing (DLP), stereolithography (SLA), and two-photon polymerization (TPP) are examples of these technologies [83].
Continuous liquid interface production (CLIP)
The CLIP dead zone eliminates the need to mechanically separate and reorient materials so that MNs production can continuously progress instead of layer-by-layer. Since mechanical separation and realignment steps in traditional processes limit the speed, the continuous movement of CLIP reduces the manufacturing time of MNs by leveraging computer-assisted design files without increasing the manufacturing time at the same time. Continuous production has several advantages including the ability to produce small, delicate, and complex MNs without fear of damage during processing, making it the perfect technique for the manufacture of MNs for the transdermal delivery of drugs [84].
Two-photon polymerization (TPP)
In all 3D manufacturing techniques, the high-precision TPP technology has produced more pointed microneedle arrays with more tunable designs [85]. TPP is based on a nonlinear optical process, two-photon absorption (TPA), in which a single atom or molecule excites from a lower energy level by simulating two photons simultaneously [86]. A laser pulse can produce high peak power within a very short period, and when concentrated in a material, it can produce very high power photon flux. Because diversity, availability, and correct material selection are important factors in structural resolution, components and products in every manufacturing process must also consider these factors for TPP [87]. Within a volume smaller than the wavelength of the laser, two-photon polymerization can occur. By employing high initialization efficiency photoinitiators, managing incident laser intensity, and adjusting laser focus scanning rate, lower than 100 nm structural features may be created. Two-photon polymerization is a new rapid prototype technology that can be used to make microneedles, as well as microneedle arrays of a wider geometric range [88].
Microstereolithography (μSL)
Microstereolithography (μSL) technology has been widely used in many areas over the years especially in biomedical and tissue engineering. Currently, μSL-designed devices include tissue scaffolds, cardiovascular stents, and nerve guidance conduits [89]. A quick prototype method called visible light dynamic mask microstereolithography is used to manufacture microneedles. Additive manufacturing involves layer-by-layer construction of the structure using a computer model. Dynamic mask microstereolithography was carried out in a report using commercial rapid prototype systems that contained digital microscope devices (DMDTMs). Dynamic masks are applied to specifically polymerize light-sensitive materials. The processing timeframes connected with visible-light dynamic mask microstereolithography are significantly shorter than those associated with other quick prototype methods because all layers of materials are polymerized simultaneously [90].
Photolithography
MNs may be produced via photolithography, a well-known microelectronic and microfluidics production technology, in a variety of forms and designed lengths [91]. The MNs formed by photolithography are strongly influenced by the presence of microlens, which deposits the polymer on a convergence path resulting in sharper MNs compared to the cylindrical MNs formed by planar photomasks. In planar photomasks, ultraviolet light passes through the lens with a small deviation (about straight), resulting in a more narrowly oriented cylindrical MNs, while, in a microscope-embedded photomask, UV light passing through the lenses is refracted and converged, leading to the formation of MNs with sharp tips. The lens equation is used as a prediction model for approving MNs length and giving three times the actual length prediction by correlating the microlens focal length. This discrepancy may be due to the flat-convex surface of the microscope, which does not allow light refraction, such as conventional convex lenses [92].
Dry etching
Dry etching is a photolithographical method used to fabricate microneedles with controlled density and shape, and the formation of MNs with cylindrical symmetry is made possible by the lack of crystal plane effects [93]. In this technique, inert or reactive gases are utilized at low pressure. Dry etching is grouped into reactive ion etching (RIE), which uses chemical processes, and ion-beam milling, which mainly uses physical processes [4]. The flexibility of needle shape and density is one of the key benefits of dry etching [94]. In dry etching, high energy, unidirectional electrodes ionize an inert gas such as argon or sulfur hexaflouride. Since the ions impact the silicon substrate rapidly, and in a single route, anisotropic etching is used. The exposed silicon is etched throughout the manufacturing process, but the region protected by the oxide film (sacrificial layer) or photoresistant rarely gets etched. High-pressure plasma etching is a chemical process that employs strong energy to produce a chemically reactive plasma gas as a result of the interaction of the plasma with the surface of the substrate, which turns it into a volatile material that is blasted away and the substrate is isotropically etched. Reactive ion etching employs both physical and chemical methods. Anisotropic and isotropic etching can be controlled by plasma and projectile etching [94].
Wet etching
Due to simultaneous sequential manufacture employing many silicon wafers at once, wet etching provides cheaper tool costs and allows mass production. Nevertheless, it is only suitable for low aspect ratio designs. A single crystal silicon wafer is immersed in chemical etchant solutions during wet etching to either produce an anisotropic (where the etch rate varies for various crystal planes) or an isotropic etch (there is the same etch rate in all directions) [93]. The microneedle arrays fabricated through this method are usually made from standard silicon wafers with exceptional precision and repeatability using potassium hydroxide (KOH). Wet etching is a popular micromachining technology that has advantages over dry etching such as lower processing and production costs. Wet etching of silicon to generate microneedles is a complicated process, but in a study, microneedles shape was regulated using the crystal structure of silicon and its associated etch properties in KOH [95].
Laser methods
Laser ablation
A laser is impinged on a metal plate to generate a bulge in this technique. This top-down technique used to process materials like metals allows the establishment of an inverse mold creating a pattern of microneedles [96]. Laser ablation inscribes the plate into a three-dimensional shape. In this technique, light pulses are employed to give the bulge a specific shape on a metal plate in order to build MNs array. When a substrate is exposed to a laser beam, for example, a carbon dioxide laser beam, energy is absorbed and it is heated to evaporate or sublimate [76]. Solid metallic arrays are made using laser ablation [96].
Laser cutting
An infrared laser is used in this process to cut flat metallic sheets into the shape of microneedles. To develop a 3D MN, 2D MN is bent to 90 degrees. MNs arrays are created by cutting stainless steel or titanium sheets into MN shapes [96]. Laser cutting is typically utilized to create metallic MNs; stainless steel is the most commonly preferred material [76]. Using AutoCAD software, the necessary geometry, shape, and structural dimensions of the MNs are generated. The MNs are washed in hot water at 90 °C from the plane of the base following the laser beam for the predefined shape of the needle. After that, MNs are electropolished in order to remove burr, reduce thickness, and sharpen the tips. This approach can be utilized to develop not only one row of MNs of different geometries, but also rows of metallic MNs with two dimensions [13].
Molding technique
Micromolding
Micromolding involves the utilization of molds to replicate a master structure. This method is also known as solvent casting method. Polydimethylsiloxane (PDMS), which has excellent stability, good thermostability, flexibility, reproducibility of the master structure as well as less adhesion (beneficial to peel off the MNs from female mold), is used to make the majority of the molds [97]. Moreover, a single master template can create many PDMS molds. The fabrication of MNs patches of several polymers, including natural polymers, synthetic or semisynthetic polymers, is done by using micromolding technique [96]. The micromolding process comprises of six main steps: constructing a male MNs mold, female MNs mold, casting the polymeric solution onto the female mold and forcing it into the cavities of the mold by centrifugation, removing bubbles by centrifugation or vacuum, curing MNs by drying (hot air oven or air dry) or photo-crosslinking, and peeling the MNs patch off the female molds [97]. The benefits of this technique include relatively simple, low-cost MNs synthesis at an ambient temperature [13].
Injection molding
Of the available micromolding methods (reaction injection molding, hot embossing, and thermal forming), micro-injection molding is preferentially used. Micro-injection molding is an extension of injection molding, which can make the method of creating products with micron characteristics more effective and affordable. It is a technique that transfers the micron accuracy of metallic molds with microstructures to molded products. Granulated thermoplastic material passes through a hopper and subsequently to a heated barrel, where it melts. Then, to compensate for material shrinkage, this substance is pumped under pressure into cavity of the mold and held there for a predetermined amount of time. The procedure is repeated after a specified period of time has passed after the material solidifies into the shape of the mold and is expelled. Micro-injection molding provides great repeatability, exact dosing, and high injection flow rates after the plasticization and polymer melt injection are segregated [14]. Major drawback of this method is managing the small size, since the commonly used screw is of size of 15–150 mm, and the equipment used in the process [98].
Methods of characterization of microneedles
Microneedle characterization is a key step in their development since it helps to ensure that they are safe, effective, and reliable. Several fundamental methods are frequently used to characterize microneedles.
Geometrical properties
Geometrical evaluation is an important method of microneedle characterization because it impacts penetration depth, tissue damage, and effectiveness of drug delivery. Some of the most important needle geometry parameters are:
Needle length
Needle length is the measurement from the base of the needle to the tip. The depth of penetration into the skin or other tissues can be affected by the needle length. Shorter needles, for example, can be used for transdermal administration of drugs, whilst longer needles can be employed for intramuscular injections.
Needle diameter
Needle diameter denotes the thickness of the needle. The needle diameter can influence the amount of force required to pierce the skin or other tissues. Thinner needles may not be as painful and need less energy to pierce the skin, but they may bend or break more easily [99].
Needle tip
The form of the needle tip is referred to as the tip shape. The form of the tip can influence penetration depth and tissue injury. Conical tips, for example, may cause less tissue injury than blunt points but may not penetrate as deeply.
Needle spacing and arrangement
The distance between the needles on the microneedle device, in addition to the way they are arranged, such as in a linear or array pattern, are collectively referred to as needle spacing and arrangement. The spacing and arrangement of microneedles can impact the density and area of skin covered, as well as the degree of penetration and drug delivery effectiveness [100].
Mechanical properties
Mechanical properties of microneedles relate to the qualities of the microneedles that govern their behavior when exposed to mechanical forces. These characteristics have significance because they impact the effectiveness of the microneedles during usage.
Stiffness
The resistance of the microneedles to bending or deformation when exposed to an external force is measured as stiffness. It is frequently expressed in terms of the Young’s modulus, which is the proportion of stress to strain. Microneedles with a higher stiffness require more power to enter the skin, but they are less likely to bend or break during usage [101].
Strength
Strength is a measure of the maximal stress that microneedles can bear before fracturing or breaking. It is a crucial quantity since it dictates how much force the microneedles can apply to the skin without breaking. Higher strength microneedles may penetrate deeper into the skin without breaking.
Elasticity
Elasticity is a measure of the capacity of the microneedles to recover to its original shape after being deformed. It is an essential characteristic since it impacts the skin-penetration capacity of the microneedles and keep their form while in use. Highly elastic microneedles regain their original shape easily making them less prone to shatter or deform during usage [101].
Surface properties
Surface roughness
This feature refers to the irregularities or peaks and valleys on the surface of the microneedle. Surface roughness influences the adherence of the microneedles to the skin or other surfaces, as well as its capacity to administer medications or collect samples. A smooth surface may improve adherence, but a rough surface may improve penetration and retention inside the skin. Techniques such as atomic force microscopy (AFM) or profilometry can be employed in order to quantify surface roughness.
Surface chemistry
Surface chemistry, which relates to the composition of the microneedle surface and its capacity to interact with the surrounding environment, is another essential surface feature. The surface chemistry of the microneedle can impact its adherence to the skin or other surfaces, as well as its ability to administer drugs or collect samples. A surface with a high degree of hydrophilicity, for example, may encourage greater skin wetting and penetration, whereas a hydrophobic surface may have lesser skin adhesion but may be more suited for some types of drug molecules. Surface chemistry can be studied using X-ray photoelectron spectroscopy (XPS) or Fourier transform infrared spectroscopy (FTIR) [102,103,104].
Surface wettability
Surface wettability is another key surface characteristic that could impact microneedles performance. The term, wettability, describes the capacity of a liquid to cover the surface of a solid substance. The surface wettability of the microneedles can influence how well they can penetrate the skin to administer drugs or collect samples. A highly wettable surface may promote greater skin penetration and drug administration. In contrast, a less wettable surface may have poorer skin adherence but may be more suited for specific types of drug molecules. Techniques like evaluation of contact angle can be used to gauge surface wettability.
Biocompatibility
The ability of a material or device to interact with living tissues without causing an adverse response. In the case of microneedles, biocompatibility is important to ensure that the device can be used safely and effectively in humans or animals without causing harm or discomfort. In vitro or in vivo tests to measure the cytotoxicity, immunogenicity, and inflammatory response of the MNs are frequently used in biocompatibility testing [10, 105].
Morphological characterization
Using techniques like transmission electron microscopy (TEM), scanning electron microscopy (SEM), or atomic force microscopy (AFM), the morphological profile of microneedles may be determined by studying their physical characteristics. The morphology of MNs is widely evaluated using SEM in order to ascertain the length, shape, and base diameter of MNs arrays and individual MN diameters. Techniques like SEM, AFM, and TEM are utilized by researchers to optimize as well as customize MNs for specific biomedical applications [105].
Permeation evaluation
In the permeation test, especially ex vivo permeation study, the rate and percentage of drug penetration across the skin using microneedles are measured. This method usually involves sample preparation and assessment of permeation of the biomolecules across an excised skin. The permeation assessment is carried out immediately after fabricating the microneedles. In this stage, a barrier between the donor and receptor compartments is created by properly mounting the skin tissue onto a diffusion cell. While the receptor compartment serves as a sink for drug molecules that cross the skin, the donor compartment contains the drug-loaded microneedles. For the purpose of simulating physiological circumstances, the entire system is kept at a constant temperature. The drug concentration in the receptor compartment is continuously monitored during the permeation test. The drug molecules that penetrate the skin can be estimated using a variety of analytical methods, including high-performance liquid chromatography (HPLC) and UV–visible spectrophotometry. Researchers can evaluate the effects of microneedle characteristics, including length, density, geometry, and surface changes, on drug delivery efficiency by examining the drug permeation profile. The permeation test offers significant information on the improvement in drug permeation attained by microneedles in comparison with conventional delivery techniques. It aids in choosing the ideal microneedle production and design parameters based on specific drug candidates. The test also permits the evaluation of formulation parameters that may affect drug absorption via the microchannels made by the microneedles, such as drug concentration, viscosity, and pH. Nway et al. [106] performed in vitro and in vivo permeation tests using a Franz diffusion cell and an 8-week-old mice model, respectively. The in vitro permeation test was done on neonatal porcine skin. For that, the skin sample was carefully excised to obtain a subcutaneous layer of the skin. The receptor compartment of the Franz cell was maintained at 37 ± 2 °C and was stirred constantly at 600 rpm using an in-built magnetic starring. The medium used for the test was PBS (pH 7.4), and the experiment was done at various predetermined time points up to 24 h. The quantity of permeated drug was determined using an analytical technique previously developed for the study. The study is usually carried out using controlled treatments such as placebo, negative control, and positive control groups [107].
Animal study using microneedles delivery system
Microneedles are usually tested in vivo to investigate vital factors including biosafety of the array, and the in vivo pharmacodynamic and pharmacokinetic profiles of the active pharmaceutical ingredient. Animals including mice, monkeys, guinea pigs, and rabbits could be used for in vivo evaluations. Additionally, different factors, including TEWL (transepidermal water loss), skin inflammation or irritation, and bioavailability, are assessed in animal studies. The Delfin vapometer is used for TEWL testing both before and after administration of microneedles [108]. To buttress the importance of animal study in MNs delivery, BALB/c mice of both sexes were utilized to evaluate the delivery and immunogenicity of formulations of diphtheria toxoid (DT) adjuvanted with N-trimethylchitosan (TMC) and administered transcutaneously using microneedles,. DT-loaded N-trimethylchitosan nanoparticles, a mixture of N-trimethylchitosan plus diphtheria toxoid (TMC/DT), or diphtheria toxoid solitary were administered to the mice three times, each time with a three-week delay between each dose. Two distinct 300-µm microneedle arrays were used to administer the formulations intradermally to the skin either before or after microneedling. Alum-adjuvanted diphtheria toxoid was administered subcutaneously (SC) as a positive control. The mice were slaughtered three weeks following their most recent vaccination. Total blood from the femoral artery was taken shortly before the animal was put to death, and ELISA was used to identify the antibodies (IgG, IgG1 and IgG2a) in the sera mobilized by the DT-loaded MNs [109].
For SARS-CoV-2 investigation, MNs loaded with SARS-CoV-2-S1fRS09 or SARS-CoV-2-S1 protein were inoculated intracutaneously into female C57BL/6 mice (each set of five animals), with PBS serving as the negative control. Mice were likewise supplemented with equal dose of immunogens after two weeks following the initial immunization. Two mice per group were exposed to gamma irradiation under clinical sterilization to assess the preliminary impact of gamma radiation on the MNs-SARS-CoV-2 vaccination. At weeks 0, 1, 2, 3, and 4, mice were bled through saphenous vein, and ELISA was used to evaluate blood samples for SARSCoV-2-S1 antibodies. It was discovered that MNs vaccines generated higher humoral responses compared to conventional needle injections [110]. In an in vivo drug delivery trial of a combined patch consisting hydrogel-based microneedles loaded with donepezil hydrochloride, male Sprague–Dawley rats were employed. Prior to the experiment, the rats were allowed to acclimatize in a week and rat hair at the back region was removed 24 h before the experiment to reduce or eliminate interference of hair with the application of MNs. Rats were placed under isoflurane anesthesia (2–4% in oxygen) to make MNs administration easier. Rat skin was squeezed, and four MNs set on an adhesive foam border were placed on the back of all the rats using firm finger pressure. Films containing donepezil hydrochloride were placed to the back of the arrays with the drug filling up to 2.5 mg/kg or 5 mg/kg. A Scotchpak®M and Duro®tak adhesive (grade 387–2054) film, an occlusive transdermal backing, was placed on top of the arrays to hold the integrated patch in place, and this was wrapped with Micropore® tape. At predetermined intervals up to 24 h, blood samples (200 µL) were obtained through tail vein bleeds at defined sampling point. Following heart puncture, the Sprague–Dawley rats were killed and blood was withdrawn into heparinized tubes and RP-HPLC analysis of all above samples were performed. The concentration of donepezil HCl in plasma was found to be 51.8 ± 17.6 ng/mL, confirming MNs as an effective delivery system for donepezil HCl [111].
Methotrexate (MTX)-loaded hyaluronic acid-dissolving microneedle patches and methotrexate microneedles were evaluated in BALB/c mice in vivo. To assess the therapeutic and unfavorable effects of different doses of methotrexate-loaded microneedles, a psoriasis mouse model was used. The mice were separated into six groups of five mice each and the first five groups were subjected to topical administration of IMQ (imiquimod) cream (15 mg/day) on their left ears for 6 consecutive days. The control group included mice that did not receive any imiquimod (IMQ) cream topical administration. Every day, a single MN patch was placed on the ear of a mouse as part of the microneedle treatment. To ascertain the minimum dose (LD), median dose (MD), and maximum dose (HD) for all groups, additional ear swelling or thickness was assessed using a vernier caliper, and a psoriasis-like lesion was also determined. In IMQ-administrated BALB/c mice, it was discovered that application of MTX-loaded microneedles on the skin lesions lessened epidermal hyperplasia, lowered IL-23 and IL-17 production, and eventually decreased the inflammation of the skin similar to psoriasis. Additionally, when correlated with oral treatment, the MN-assisted transdermal MTX delivery demonstrated increased efficacy to prevent lesions from exacerbating and produced a comparable therapeutic impact at a lower dose, which could produce negligible systemic toxicity. Considering all of its benefits over traditional delivery methods, the methotrexate-loaded hyaluronic acid dissolving microneedle patch has the potential to replace psoriasis medication in the near future [112].
Therapeutic applications of MNs
Protein and peptide delivery
Calcitonin gene-related peptide (CGRP) is a neuropeptide responsible for inducing neuropathic pain. It is secreted by the sensory nerve endings. Xie et al. [113] selectively targeted CGRP using a microneedle patch which produced a local analgesic effect. CGRP8-37 is a model anti-CGRP peptide. A dissolving microneedle patch was fabricated using sodium carboxymethyl cellulose (SCMC) with CGRP8-37 dissolved in the polymeric solution. Three different rat models for diabetes, neuropathic pain, and nerve injury models were used to investigate the efficacy of the microneedles. Analgesia was observed in the local area without disrupting normal pain function. Polyethylene glycol diacrylate (PEGDA) was used by Liu et al. [114] to fabricate microneedles by photopolymerization. Although small molecules can be loaded in the process of formulation of microneedles, peptides can degrade in the photopolymerization process. Hence, they used a safer method for loading gap junction inhibitor (gap 26) on PEGDA microneedles by exploiting the ability of the polymer to swell in an aqueous solution. The peptide exhibited inhibition of collagen-1 in keloid scar. Furthermore, glucagon-like peptide 1 (GLP1) is an intestinal hormone that regulates the blood glucose level by stimulating insulin production in the presence of higher sugar levels and vice versa in hypoglycaemic conditions. GLP1 is an extremely unstable molecule with a very short half-life and is easily degradable. Lixicenatide is an analog to GLP1 which was delivered using a bilayer dissolving microneedle fabricated using PVP, wherein the peptide was concentrated in the tip region. In a study using db db mice, the blood glucose level was decreased upon application of the transdermal patch [115].
Vaccine delivery
A proof-of-concept work by Patil et al. [116] used the spike glycoprotein of SARS-CoV-2 for the formulation of a noninvasive microneedle vaccine. PLGA microparticles were used to separately encapsulate each of the surface spike protein and adjuvants, Alhydrogel® and AddaVax™. The hydrogel of nanoparticles along with sodium alginate was fabricated into microneedles using PDMS mold. Preclinical studies confirmed antigen-specific humoral immunity as well as cellular immunity. In a study, dissolvable microneedle patch fabricated using polyvinyl pyrrolidone was used for prophylactic delivery of a highly conservative epitope, Qßvirus-like particles, to induce immunity against human papilloma virus (HPV). The amount of HPV 16 L2 IgG antibody mobilized was equal to that of subcutaneous vaccine, by administering a very small amount of the dose compared to the subcutaneous vaccine [117]. In another study, comparative analysis of dermal vaccination and traditional intramuscular route against influenza virus (H1N1) was investigated. Compared with intramuscular injection, the microneedle triggered higher IgG response and higher number of antibody-secreting cells specific to H1N1 in the bone marrow. Increased action of follicular T-cells and rapid virus clearance from lungs and improved survival of rats was observed [118]. Prophylaxis against Staphylococcus enterotoxin B (SEB) was carried out using dissolving microneedles. Prophylaxis using recombinant SEB recorded high titer value of SEB-specific antibody and the challenge study against SEB toxin produced complete protection of the mouse [119].
Hormone therapy
A microneedle patch fabricated using PLGA and PLA was used to deliver the contraceptive, levonorgestrel. The unique design of the microneedle patch by introducing a bubble between the MNs and its backing layer enables the detachment of the needles and backing layer within five seconds after application. The needles remain in the skin and produce sustained release of the contraceptive drug with prolonged activity [120]. A dissolvable microneedle patch containing human parathyroid hormone for the treatment of osteoporosis was fabricated by Naito et al. [121] using micromolding method. The shelf life of parathyroid hormone in microneedles at room temperature was sixfold higher in comparison with that of solution of parathyroid hormone. The patch containing the hormone exhibited high bioavailability of the hormone (~ 100%) in rats. In the rat model of osteoporosis, the thinning of bone density was slowed down after administration of the microneedle patch containing the hormone. Microneedle patch made of PVA was loaded with parathyroid hormone for promotion of collagen production via stimulation of transforming growth factor, Smad3 and mTOR pathway in order to accelerate wound healing [122].
Pain treatment
In a study by Shim and colleagues [123], palmer hyperhydrosis (excessive secretion of sweat) was targeted using botulinum neurotoxin-A, which is widely used for the treatment of the disease and administered by a course of injections in the local area like palm, sole, face, etc. This is inconvenient for patients, and due to the toxicity of botulinum, only limited dose can be administered. Polylactic acid microneedles were coated with the botulinum neurotoxin and were tested in vivo by application of the microneedles to the thick paw skin of BALB/c mice. After 24 h of application of the patch, a significant decrease in production of sweat was recorded. Thus, treatment of hyperhydrosis by microneedles alleviates the need of painful treatment using multiple injections at the site. Local anesthesia in the oral cavity using injections is a painful and unpleasant experience. In order to overcome the problem and improve compliance by the patient, lidocane hydrochloride loaded in dissolving hyaluronic acid microneedle patch was fabricated by Zhu et al. [124]. The transmucosal efficacy of lidocane-loaded hyaluronic acid microneedle was formulated and compared to lidocaine cream.
Cancer therapy
The commercially available Flofirinox® comprising a combination of fluorouracil, leucovorin, irinotecan and oxaliplatin is used in cancer treatment. A novel Christmas tree-shaped microneedle array was fabricated and loaded with Flofirinox® for in situ release. The unique shaped MNs were formulated by 3D printing, and oxaliplatin and leucovorin were entrapped in the upper most layer, whereas the bottom layer contained fluorouracil and irinotecan. The MNs had excellent adhesiveness and unique structure facilitated multiple drug delivery and combination therapy in a single platform against pancreatic cancer [125]. T-cell surface contains programmed cell death-1 (PD-1) protein, which, when combined with programmed cell death ligand-1, lead to suppression of T-cell activity and enhances tumor evasion of the immune system. In a study by Lan et al. [126], anti-PD-1, a PD-1 blocker, inhibits the contact of PD-1 protein with PD-1 ligand, improving the proliferation of T cells resulting in increased anti-tumor activity. MNs array of pH-responsive tumor targeted lipid nanocarriers loaded with anti-PD-1 and cisplatin permitted T cell proliferation by blocking PD-1 and increased immune responses against cancer cells.
In a bid to target superficial tumors like breast cancer, Fu et al. [127] fabricated a vinyl pyrrolidone-vinylacetate copolymer MNs array encapsulating Cisplatin and IR820 as a photosensitizer in the tips of the array. The tips could penetrate the skin targeting the localized tumor, hence delivering cisplatin to the target site. 808-nm laser leads to the production of heat and ROS formation. Thus, photothermal therapy and photodynamic therapy could be carried out by switching on and off IR820 activity by adjusting the laser frequency. Another study exploited the photoresponsive behavior of hypericin for the photodynamic therapy of non-melanoma skin cancer. Hypericin is a hydrophobic drug; hence, it was encapsulated in lipid nanocapsules (LNC). Further, hollow MNs from AdminPen® and hollow MNs fabricated in-house were used to deliver the lipid nanocapsules to the target site. The LNC-encapsulated hypericin delivered via hollow microneedle sevenfold higher drug deposition in the skin and showed 85% tumor destruction activity upon activation of hypericin LNCs at 595-nm irradiation [128].
Ocular delivery
A contact lens styled microneedle patch for ocular delivery of drugs was developed by Roy et al. [129] using pilocarpine as a model drug, which is used in the treatment of glaucoma and ocular hypertension. Dissolvable microneedles were prepared with the combined polymers, PVA and PVP. Pilocarpine HCl was dissolved in PVA and PVP solution and casted in PDMS mold. A high dose of the drug with the microneedle patch permeated across the excised cornea compared with pilocarpine solution. Cui and company [130] created cryomicroneedles for the delivery of predatory bacteria, Bdellovibrio bacteriovirus, as an antibiotic against ocular bacterial infection. The rationale of the work was to design a strategy to administer antibiotics to hitherto difficult-to-administer ocular tissue. In another study, nanoparticle-loaded MNs were fabricated by iontophoresis for drug administration to the posterior eye. To attain this goal, the hollow MNs were attached to the tip of a syringe, which contained electrode. After injecting the nanoparticle-loaded MNs in the suprachoroidal space, iontophoresis was applied to facilitate the distribution of the nanoparticles to the posterior eye [131]. An optical microneedle array was developed for light delivery to the percutaneous region of the eye. Blue light therapy for antimicrobial action was used in the study. Using optical microneedle array, blue light penetration was achieved for 2.5 mm depth, which was ninefold more light penetration as compared to direct light therapy [132].
Drug delivery
Local anesthetic effects using MNs are painless and quick local responses. Researchers have fabricated a lidocaine-coated microneedle that demonstrates in vitro skin permeation with improved drug administration in a relatively short time [133]. Polymeric microneedles of Meloxicam were also developed using a mold of polydimethylsiloxane for pain relief. About 100% of the critical bioactive was released within 60 min by in vivo experiments [74]. Various disorders have been treated using MN patches. Memory loss and language problems are two features of chronic neurodegenerative disorders in Alzheimer's disease (AD). The FDA-approved drug, donepezil hydrochloride (DPH), is used to manage AD84 with a long half-life [134] effectively. In five minutes, only the transdermal administration of 95% DPH from the MN tips recorded desired therapeutic activity in pig skin. Results revealed that encapsulating DPH loaded in dissolving MNs was more efficacious than oral delivery [135]. Furthermore, considering its numerous limitations, such as pain and poor absorption, dihydroergotamine mesylate (DHE) can cure medium-to-intense acute migraine symptoms by nasal spray and subcutaneous injection. To address these constraints, a novel delivery approach combining dissolving microneedle arrays loaded with DHE and PVP allowed for self-administration with significant bioavailability [136]. Hyaluronic acid (HA) microneedles and methacrylate-modified HA microneedles, both loaded with melittin for the treatment of rheumatoid arthritis, were developed. The in vitro release evaluation revealed that HA MNs loaded with melittin released the entire drug within 10 min. In contrast, methacrylate-modified HA MNs loaded with melittin released 56% within 10 min, and the remaining part was released over the next 480 min [137]. Further, MNs loaded with ondansetron nanoparticles for transdermal distribution are suggested as a strong antiemetic medication that lowers vomiting and nausea related to cancer chemotherapy. According to the transdermal permeation study, MNs penetrated the skin more efficiently than basic patches of the same drug by 4.69-fold [138]. A simple micromolding process frequently used for MN fabrication was utilized to optimize and incorporate the hydrophobic, antipsychotic second-generation drug, iloperidone, inclusion complex into dissolving microneedles. Following manufacturing of microarrays, the polymeric matrix stabilized the arrays. It was determined that the properties of inclusion complex which increased solubility in polymeric solution enhanced skin accumulation mainly utilized for active subcutaneous microcirculation [139]. For piercing the skin, propranolol hydrochloride-loaded microneedles were developed with PVP-K90 and hyaluronic acid, which showed adequate mechanical strength, and are quickly dissolved after absorbing interstitial fluid. A two-step technique was employed to concentrate propranolol hydrochloride predominantly in the tip. Most importantly, the additive penetration and tissue accumulation of dissolving MNs of propranolol hydrochloride-treated skin were significantly greater than in skin treated with solid microneedles and in blank skin [140]. To improve transdermal delivery of an anti-diabetic drug, hydrogel-forming MNs array and lyophilized drug reservoir of metformin HCl were developed. Microneedles that form hydrogel have shown a variety of therapeutic efficacy with varying physicochemical properties to improve transdermal delivery [9]. Solid tumors have also been treated with methotrexate, but due to its narrow margin of safety, it must be delivered sustainably at low concentrations. Methotrexate was used to create a novel in situ-forming hydrogel methotrexate microneedle, which showed pronounced results against the disease [141].
Clinical diagnosis
Aqueous humor present in the eye chambers or interstitial fluid in the skin are examples of extracellular fluids that may be accessed by MNs to harvest or detect biomarkers. Generally, MNs can interact directly with the extracellular fluid of the body with negligible interruption of skin processes thanks to its micron-sized, needle-like shape and establishment of a transfer channel that permits exchange of fluids [142]. After the application of microneedles on the surface of the skin, micropores are created which permit the extracellular fluid to emerge on the surface of the skin, where it can be collected using a syringe or a needle assembly or in a collection reservoir. Upon contact with body fluid, hydrogel MNs swell up with the uptake of biomarkers. However, this mechanism presents a major limitation as the chemistry of the hydrogel will determine biomarker uptake, which can vary across different hydrogel materials. Proven by proteomics, off-site analysis of biomarkers requires an extraction process wherein the analyte of interest is washed off the hydrogel surface [143] or pulled out of the hydrogel formulation [144]. The latter is not always accurate; hence, a correlation is required to measure analyte concentration from the amount extracted to the total physiological concentration. Simple sampling and the invasive nature of microneedles make it a good option for specific biomarker capture. Since MNs can capture a wide range of biomarkers in both circulatory and local dermal tissue with high specificity, it makes of great clinical interest [145]. Specific biomarker capture can provide microneedle-dependent diagnosis after microneedle application circumventing the need for analyte extraction and eliminating the limitations of poor extraction yields, low volume of analytes, and dilution by body fluid [146]. Hydrogel microneedles can be formulated by coating with probes for specific molecule detection, which are then mounted on solid needles [21, 147] or a needle array [143]. The swelling mechanism of hydrogels allows the uptake of analytes of interest which are then captured by the probes. The analyte concentration can be detected by conventional method, usually separating the biomarker from the microneedle array or on-site detection using the array itself. Cell populations such as the tissue-resident memory T cell (TRMs) reside within the tissues of humans and mice; they are important for diagnosing immunodeficiency disorders, monitoring vaccination status, and autoimmune disorders with unpredictable immune flashes. Mandal et al. [147] presented an invasive microneedle-based method to monitor TRMs by incorporating the antigen into the microneedle formulation and encapsulating it in nanocapsules which demonstrated reduced lymphatic uptake of the antigen-presenting cells (APC) and improved cell recovery owing to protection by the alginate layer which entrapped them in the microneedle coating. Similarly, Mohan et al. [148] designed a microneedle-based enzymatic biosensor for continuous monitoring of alcohol. Fabrication of the hollow microneedle bore was achieved using a three-way electrode system containing platinum and silver wires over which an AOx-chitosan layer, functioning as catalysis for ethanol and backed by a multilayered PPD-Nafion coating for added protection.
Microneedles as biosensors
Microneedles have very versatile properties and could be integrated with modern technology such as wearable sensors and continuous monitoring devices. Invasive detection of biomarkers from the interstitial fluid (ISF) of the skin without the need for implantable sensors, probes, suction-blister, or micropipette inserts results in increased patient acceptability and practicality of use. As the ISF is in a constant exchange of biomolecules due to blood capillary filtration, essentially, ISF is quite similar to plasma, thereby enabling monitoring of various parts of the body. Various studies have been reported on MNs integration with sensing devices to improve biomarker capture efficiency and sensitivity for proteins and nucleic acids using hydrogel and porous-based microneedles [149,150,151]. In one such study, the hydrogel MNs array managed to swell up and absorb the analyte from the ISF. After extraction using eluting buffer, it detected on an electrochemical microfluidic biosensor. Due to the presence of a molecular probe, [Ru(phen)2(dppz)]BF4, the sensitivity of the sensor increased 100-fold. In vivo studies on Balb/C mice established that by dual extraction, the microneedle system could detect EBV cfDNA on the first day as opposed to the retroorbital blood sampling method wherein detection was seen on day 3, and the target analyte could be isolated within 10 min with an efficiency of 95.4% [151].
Cosmetic therapy
Most cosmeceutical compounds used in cosmetics are applied through the topical route, especially for creams, lotions, and serums, which works on passive diffusion of active compounds into the outermost layer of the skin. Chemical compounds having appropriate physicochemical properties like a low molecular weight of not more than 500 Da, melting point, and very high lipophilicity can permeate the outermost layer of the skin, stratum corneum, which does not allow exterior substances to permeate easily, leading to the loss of cosmetic product from the applied surface. Thus, it results in low permeation though it has to produce a localized effect on the intended site of application [152]. Over the past few years, it is evident that MNs has gained popularity in cosmetics since it shows improved skin penetration, self-administration, and also reduced irritation while applying. The two most important applications of MNs are (i) healing of the skin from the microinjuries caused by needles of the syringes, i.e., scar removal, wrinkle treatment, and decrease in hyperpigmentation, and (ii) increased permeation due to perforation of microneedle in the epidermis [153]. Depending on the situation, these two principles can be used separately or in combination since they frequently reinforce each other. The formation of microchannels during the microneedling procedure allows the molecules to penetrate into the deeper membranes of the skin. This method triggers the release of collagen, which speeds up the healing of skin grooves and dots [154]. Because microneedles are effective at treating disorders including seborrheic keratosis, scars, striae, aging, wrinkles or depigmentation, and alopecia, they have become a common tool in the cosmetic industry [155, 156]. Microneedles are increasingly used for self-administration as well as professional levels in cosmetic products, systems, and therapies. An in vitro release study revealed that HA MNs loaded with melittin released the entire melittin within 10 min. In contrast, methacrylate-modified HA MNs loaded with melittin released 56% within 10 min, and the remainder was released over the next 480 min [157]. The earliest microneedle products were cylindrical rollers covered with a solid metal, which were eventually replaced by polymers, attached to a handle with microneedles that were applied by rolling over a large area of tissue to produce numerous micropunctures on the site of application for improved permeation [158]. Kim et al. [159] created a hyaluronic acid-based dissolvable MNs patch of ascorbic acid and retinyl retinoate for intradermal administration. Using solid MNs, Kumar et al. [160] demonstrated improved local action of eflornithine (used to decrease face hirsutism) through in vitro and in vivo release studies. Moreover, MNs technology was effective in treating patients with alopecia areata condition [161]. Following treatment, their hair grew back. MNs have been successfully used in clinical trials for atrophic face scarring, atrophic acne scarring [162], and hypertrophic burn scarring [163]. Microneedling is thought to be a successful cosmetic procedure for wrinkles, skin lesions, vulgaris, and aging [164]. Microneedles (patches and rollers) have attracted increasing demand due to the rising popularity of cosmetic items.
Microneedles as a polysaccharide-based delivery system
Natural polymers are well explored in MN-assisted drug delivery owing to their prominent characteristics such as easy availability, biodegradability, biocompatibility, low toxicity, sustained drug delivery, cost-effectiveness, and safety for human health. Also, these natural polymers are eco-friendly compared to synthetic polymers. Natural polysaccharides used in microneedle delivery are hyaluronic acid, chondroitin sulfate, cellulose, chitin and chitosan, starch, sodium alginate, xanthan gum, and pullulan, with prominent properties such as good mechanical strength, self-dissolving ability, good penetration, and sustained release profiles. Sugar-based MNs also show promising results in drug and protein delivery. Maltose MNs record long-term residence in the skin by minimizing the risk of needle breakage [58]. Yalcintas et al. [165] used carbohydrate polymers like carboxymethyl cellulose, hyaluronic acid, maltodextrin, trehalose, and glucose for the fabrication of microneedle arrays. Study results demonstrated that all the polymers showed negligible in vitro cytotoxicity except glucose which showed higher toxicity at a concentration more than 50 mg/ml. Hyaluronic acid (HA) is an FDA-approved polymer for soft tissue repair [166]. HA-based MNs for cosmetics delivery are commercially available. Besides good mechanical strength, high drug loading, desired penetration, and dissolving ability make HA the best fit for MNs delivery system. HA is used in dissolving MNs, which dissolves after insertion and penetration into the skin and eventually releasing incorporated drug or protein. The transdermal absorption of insulin from microneedles was investigated by in vivo absorption in diabetic rats. This led to the complete dissolution of microneedles into the rat skin just one hour after administration. The study also compared the transdermal absorption of insulin by subcutaneous insulin injection, concluding that the transdermal absorption of insulin from MNs produced a higher level of serum insulin. Besides, high insulin stability was observed in MNs [66]. HA-based MNs were also used to study the skin permeation and accumulation of higher molecular weight fluorescein isothiocyanate-labeled dextran. The study showed that transdermal permeability of fluorescein isothiocyanate-labeled dextran entrapped within MNs arrays was comparatively higher than that of the plain FD4 solution [167]. Furthermore, HA-based MNs effectively reached the target region by penetrating the stratum corneum and recorded greater stability for the bioactive at room temperature [168, 169]. A review by Saha and Rai [154] elaborated more on recent applications of HA-based MNs in drug delivery and cosmetics. Chitosan, a marine polysaccharide, is used in the fabrication of microneedles. The PVA/chitosan microneedles showed good permeation across tumor-mimicking agarose gel [170]. Further, the introduction of the thiol moiety increased the mechanical properties of chitosan MNs [99]. In vitro sustained release of about 95% within a week of a hydrophilic macromolecule was achieved using chitosan MNs [68]. Furthermore, cellulose microneedles are used for the delivery of gene and anticancer agents [127, 173, 174]. Hyaluronic acid and bacterial nanocellulose-based MNs demonstrated controlled release of therapeutics and was safe and biocompatible following in vivo study [173]. An ex vivo study of sodium alginate microneedles with a model drug, bovine serum albumin recorded 15.4-fold increase in permeation than the sodium alginate-free microneedles [174]. Further, an in vivo study indicated amalgamated maltose and alginate exhibited superior mechanical properties in terms of MNs permeation into the skin [175]. For fast-dissolving MNs, the concentration of a polymer or polymers needs to be optimized to have fast-dissolving scenario and, at the same time, enough strength. Xanthan gum is known for its viscosity-enhancing property in the fabrication of coated MNs. Studies have documented that a concentration range from 0.075%w/v, in combination with trehalose, to 1% w/v recorded suitable viscosity-enhancing property and stability of MNs [176, 177]. Further, pullulan and starch-based microneedles have also shown promising results in skin permeation with good mechanical strength [178, 179]. However, some natural polymers may possess limitations in microneedle delivery such as processing constraints, stability, desired microneedle strength, and unwanted immunological responses. The various applications of microneedles are illustrated in Fig. 4.

Schematic illustration of the various applications of microneedles
Sterilization of microneedles
Microbial penetration through the skin layers is one of the major risk factors while using microneedles. During incorporation, as microneedles form micron-sized channels through the impermeable epidermal layer, the microbes present on the surface of these structures get easy access to the inner layers of the skin and blood vessels [179]. Thus, it has to be ensured that microneedles are sterile before administration. The two ways by which a manufacturer can ensure sterile MNs are by terminal sterilization or by manufacturing MNs through an aseptic technique. MNs are generally sterilized by three processes: steam sterilization, dry heat sterilization, and gamma ray sterilization. Steam sterilization of MNs is generally performed at a temperature of 121 °C for a time period of 15 min and dry heat sterilization at a temperature of 160 °C for a timeframe of 2 h. Gamma ray sterilization is done by exposure of samples to a radiation of 25 kGy for 14 h and temperature monitored during the entire process [180]. The correct sterilization process is chosen depending on the material of the MNs and the physicochemical characteristics of the incorporated critical active. The major factor to be taken into consideration while choosing the sterilization process is the change in the physicochemical characteristics of the microneedle fabric or the drug (if incorporated in the microneedle). In case of microneedles made of metal, silicon or glass, all the three sterilization methods, i.e., steam, dry heat or gamma ray sterilization, can be performed. In case of polymeric microneedles, steam or dry heat sterilization may cause a change in the mechanical property of the polymer, thus hampering its structural integrity. Thus, a better alternative is gamma ray sterilization. Gamma radiations are ionizing radiations, which have the potential of penetrating matrices without any rise in temperature which is the perfect sterilization condition for thermolabile and moisture-sensitive drugs and polymers. However, an appropriate dose of radiation needs to be selected in order to eradicate chances of degradation of the product which happens because of molecular fragmentation [179]. According to the European Pharmacopoeia, substantial sterility of a product is assured when irradiated with an optimum gamma ray intensity of around 25 kGy. Gamma radiation produces its bactericidal effect by breaking down bacterial DNA, hence inhibiting their growth and replication. These rays also produce free radicals, thus causing oxidative stress in the microorganism leading to death [181].
Stability assessment of microneedles
Stability studies for a drug product are mainly performed to test its ability to withstand variations in thermal conditions and to assess its sensitivity to moisture and solvent loss during the course of its shelf life. The study should cover the period from shipment of the product to subsequent use by the end user. The ICH Q1A (R2) guideline for evaluating the stability of new drug substance and product could be applicable to MNs. This guideline provided parameters to be evaluated for stability testing of drug products for storage at room temperature, refrigerated conditions (5 °C) and freezer (− 20 °C) [182]. A study was performed in which MNs-loaded vaccine stability was analyzed at a constant temperature of 4 °C for 3 weeks. These MNs were sealed in aluminum foil pouches containing a desiccant and tested at the above-mentioned conditions [183]. In another study, stability of parathyroid hormone loaded on dissolving microneedles was assessed for a fixed time period of one month at three contrasting temperature conditions [121]. As mentioned in the document of European Medicines Agency (EMA) for quality of transdermal patches, various physical and performance tests could be analyzed at different time points. Changes in physical attributes may be due to active ingredient or excipient evaporation, active ingredient crystallization, changes in the state of excipient or reaction between active and excipient. Physical parameters that could be analyzed during the course of stability studies include morphology, mechanical strength, dissolution, cumulative drug release, and skin penetration efficiency [32]. Periodic assurance of these parameters would guarantee shelf life of MNs. In the report by Choi et al. [184], long-term stability of MNs coated with whole inactivated influenza vaccine was analyzed by observation of morphological changes through optical microscopy, analyzing the haemagglutination activity in vitro on chicken red blood cells and in vivo immunogenicity on female Balb/C mice. Biocompatibility of the material used for the formulation of MNs needs to be assessed in order to prevent any toxic or immunological responses. Solid non-degrading materials such as silicon and metals are said to be biocompatible with a few limitations. Silicon is a relatively brittle material, and hence, chipping or cracking after insertion poses a major problem. Hence, an inert coating material such as gold is generally applied to counter this disadvantage. In case of metals such as stainless steel, their stability depends on the environmental conditions they are exposed to. Corrosion of metals is based on oxygen, moisture and pH conditions. Thus, the performance of metallic MNs would vary from one body part to another. Bioinert ceramics have been used to make bone and dental implants. Biodegradable MNs materials breakdown after contact with body fluids and release the active ingredient. Thus, it has to be ensured that there are no toxic by-products released after its breakdown. Carbohydrate and polymeric MNs are examples of biodegradable MNs. The most common carbohydrates studied for fabrication of MNs are maltose, alginates, hyaluronic acid and dextran. All these polysaccharides are biocompatible, biodegradable and nontoxic [185] (Table 1).
Regulatory considerations
Being a noninvasive device, there are minute risks involved while using MNs. Clinical indications for evaluation should include degree of skin inflammation, blood vessel and nerve damage, scar formation, skin irritation, hyperpigmentation, allergic reactions, and risk of infections. USFDA has classified microneedles into those which are devices and those which are not devices. A detailed outline of differences between the two is given in Table 2. MN devices are majorly classified into classes I and II. According to FDA, a MN device could be termed as class I if its length is 0.3 mm or less which in turn will not penetrate deep into the skin, thus keeping the structure and function of the skin intact. Thus, due to this fact, class I microneedles are exempt from FDA regulations. MN devices with lengths greater than 0.3 mm are generally used for aesthetic purposes or for delivering drug systemically. These are categorized into class II and are regulated by the FDA as they may alter the structure and function of the skin [186, 187].
Clinical adaptation of microneedle-based therapy
Considering the advantages of MNs over hypodermic syringe or intravenous injections, they can be used as a useful alternative in delivery of critical biomolecules. High molecular weight compounds, which do not have the ability to diffuse through the external layer of the epidermis, i.e. stratum corneum, could be delivered via microneedles painlessly. MNs could also circumvent the disadvantages of oral administration such as gastric degradation, irritation, poor absorption, and first-pass metabolism. MNs could be used clinically for diagnostic, prophylactic or therapeutic purposes.
Prophylactic adaption
High molecular weight proteins and inactivated viruses can be delivered through the skin via microneedles. Bypassing the impermeable stratum corneum, immune system triggering moieties could be delivered directly to the skin layers containing abundant immunomodulating cells. Two mechanisms are involved for triggering an immune response through the immune cell rich skin layer. One mechanism is through the activation of dendritic cells and the second is through the activation of Langerhans cells [188]. A number of formulation development, in vitro and preclinical studies, have been performed to test microneedle vaccines of influenza [189, 190], polio [191], rabies [183], smallpox [192] and COVID-19 [193].
Therapeutic adaptation
A) Cancer: Conventional chemotherapy, surgery, and radiation have caused several side effects in patients over the years. Thus, MNs could circumvent these disadvantages by inducing a controlled systemic immune response through introduction of an antigen to the specific target. MNs could facilitate controlled release of drug into the bloodstream, thus maintaining their levels below the minimum toxic dose (MTD) and prolonging its effect. In case of superficial tumors (e.g. oral cancer), MNs could facilitate deep tissue deposition of the drug at the site of tumor. Efficacy testing of a MN patch containing combination of doxorubicin and docetaxel on 4T1 xenograft breast cancer model on mice has shown positive results [194].
b) Diabetes: This is a chronic condition which involves an increase in blood glucose levels. Diabetes mellitus (DM) is divided into two parts—DM 1 and DM 2. DM 1 is insulin-dependent DM wherein islet cells in the pancreas make no insulin. In this case, insulin is given via the subcutaneous route (SC) causing patient discomfort and reduced compliance [195]. The oral route is not an option as insulin gets degraded in the gastric pH. Thus, several studies have been conducted to evaluate the utility of insulin-containing MNs [82, 195]. In case of DM 2 (insulin-independent DM), metformin-loaded hydrogel-forming MNs showed promising pharmacokinetic (PK) profile in rats. This proves the utility of MNs in delivering therapeutic molecules against DM [9].
c) Neurological disorders: Certain drugs on oral administration cause GI abnormalities and cannot penetrate the skin on topical application due to their molecular structure. Thus, strategies on how to circumvent these disadvantages encountered by neurological drugs through formulation of MNs are been investigated [111, 135]. Alzheimer’s disease is a condition in which there is a significant reduction in cerebral neurotransmitters including acetylcholine. After discharge from the MNs, donepezil would be delivered to the bloodstream and transported to the neurons in the brain. It inhibits the hydrolysis of acetylcholine by acetylcholinesterase, resulting in improved neurotransmission [111]. L-DOPA faces similar disadvantages as donepezil during oral administration. However, like donepezil, MNs formulation loaded with L-DOPA could be a reliable option. L-DOPA-loaded MNs were formulated and various parameters such as in vitro transdermal drug permeation, in vivo drug concentration in plasma and brain of mice, and behavioral changes in mice were evaluated. Through this study, it was proven that L-DOPA MN patches could permeate through the skin layers very efficiently in a painless, noninvasive and a non-infectious manner and hence could act as a useful alternative to other transdermal delivery systems [196].
d) Ocular diseases: Like transdermal delivery, the main advantage of MNs in ocular delivery is painless administration [197]. Intraocular injections are patient non-compliant because of their invasive nature and repeated administration [198]. As discussed earlier, MN patches unlike hypodermic needles, have micron sized needles on one end which help in attachment of the patch and also help in delivery of the drug to deeper layers of eye with minimal damage. This would sustain the release of the drug; thus, repeated administration would not be required [197]. High molecular weight and lipophilic drugs tend to show very low corneal permeation. Thus, microneedle contact lens loaded with Cyclosporine A was evaluated and it showed enhanced flux and corneal retention in comparison with marketed Cyclomune® eye drops [199]. In another study, MN patch loaded with pilocarpine was investigated and it recorded superior ex vivo ocular permeation properties compared to the drug solution [129].
Diagnostic adaptation
There are various methods of disease diagnosis such as evaluation of clinical systems, evaluation of MRI-CT or PET scans. One of the major methods of diagnosis is through blood tests. Critical attributes such as level of blood components (salt, carbohydrates, vitamins, hemoglobin), level of biomarkers indicating disease (neutrophil, basophil), and pharmacokinetic characteristics of a drug could be evaluated. The traditional method of using a hypodermic needle is not patient friendly as it causes pain and tissue damage. The use of these needles also generates hazardous waste which may be lethal if accidentally reused [200]. Microneedles have been considered as a reliable alternative to the hypodermic needle due to its painless nature and ease of handling. They also occupy a larger sampling area, giving the physician better accuracy during diagnosis [200]. MNs can be used for the detection of cancer. During the early stages, specific biomarkers could be detected in the blood or interstitial fluid of the patient which would in turn, help in early diagnosis [201]. In a study, breast cancer was successfully detected through microneedle sampling of the interstitial fluid. The immunoassay and detection were performed by colorimetry. This method of detection of breast cancer is faster, cost effective and painless compared to the conventional method of detection [201].
Commercialization of microneedles
The global microneedle market is anticipated to grow in the future years due to its advantage of posing much lesser safety issues compared to other transdermal formulations. In the year 2000, the market share of MN devices was $5 billion, but this increased to $24 billion in 2013. By the year 2030, it is expected to rise to $95 billion [10]. Figure 5 shows the global market volume of microneedles based on their various applications.

Chart indicating the global market volume of microneedles based on their various applications
There are a number of MNs products under clinical trials for various applications, i.e., either diagnostic, prophylactic or therapeutic, and some have been commercialized. Few of these MN formulations are listed in Tables 3 and 4, while the top five manufacturers of MNs are listed in Table 5.
Safety and toxicology of microneedles-based delivery system
The safety assessment of MNs is an ongoing process, and regulatory bodies play crucial roles in establishing guidelines and standards for their safe use [186]. Manufacturers typically conduct comprehensive preclinical and clinical studies to assess the safety and efficacy of microneedles before they are approved for biomedical or cosmetic applications. MNs have gained popularity in various fields, including skincare, protein, vaccine and drug delivery, and medical diagnostics. When it comes to safety, microneedles have several advantages over traditional hypodermic needles. Here are some key points regarding the safety of microneedles:
-
(a)
Reduced risk of injury MNs are typically shorter and thinner than hypodermic needles, reducing the risk of accidental punctures and injuries. They are designed to penetrate the outermost layer of the skin without reaching blood vessels or nerves.
-
(b)
Minimized pain and discomfort The microneedle design, which often incorporates multiple tiny needles or even dissolvable MNs, aims to minimize pain and discomfort during skin penetration. The small size and high density of microneedles can distribute the applied force over a larger area, reducing pain perception.
-
(c)
Lower risk of infection MNs create microchannels in the skin, which allows for targeted drug delivery or sampling. These microchannels typically heal quickly, reducing the risk of infection compared to larger needle punctures. However, it is still essential to follow proper hygiene practices during microneedle use.
-
(d)
Potential for controlled drug delivery MNs offer the advantage of delivering medications or vaccines directly into the epidermis or dermis of the skin, bypassing the need for injections into muscle or subcutaneous tissue. This targeted drug delivery can enhance therapeutic efficacy and potentially reduce side effects.
-
(e)
Noninvasive monitoring and diagnostics Microneedles can also be utilized for noninvasive monitoring and diagnostics by extracting interstitial fluid or sensing biomarkers present in the skin. These applications offer the potential for continuous monitoring without the need for frequent blood sampling [205].
Despite their advantages, it is important to note that the safety of microneedles can vary depending on their design, material, and application. Proper training and adherence to usage guidelines are crucial to ensure safe and effective use [186]. Before deploying microneedles for any purpose, it is advisable to consult with a healthcare professional or expert in the specific field to ensure proper usage and safety precautions [206].
Key aspects considered in the safety assessment of microneedles:
-
(a)
Biocompatibility One of the primary concerns in safety assessment is the biocompatibility of the materials used in microneedles. The materials should be nontoxic, non-irritating, and non-allergenic. They should not elicit adverse reactions or inflammation when in contact with the skin or underlying tissues.
-
(b)
Physical properties The physical properties of microneedles such as size, shape, and mechanical strength are evaluated to determine their suitability for use. The size and shape should be optimized to minimize pain and tissue damage while ensuring efficient drug delivery or sample collection. The mechanical strength should be sufficient to avoid needle breakage or fragmentation during use [186].
-
(c)
Skin penetration MNs are designed to penetrate the outermost layer of the skin. Safety assessment involves evaluating the penetration depth and potential risks associated with deeper tissue damage, nerve injury, or blood vessel puncture. Studies are conducted to assess the optimal needle length and design to minimize these risks [207].
-
(d)
Infection risk Sterility is a crucial aspect of microneedle safety. Contamination or infection at the micropuncture sites can lead to complications. Proper manufacturing processes, packaging, and sterilization methods are evaluated to minimize the risk of infection. Additionally, studies may assess the potential for microbial growth on the microneedle surface during and after use [208].
-
(e)
Toxicity and chemical leaching MNs may contain chemicals, coatings, or drug formulations. Safety assessment includes evaluating the toxicity of these substances and their potential for leaching into the body. Studies may assess the release of substances from the microneedle and their impact on surrounding tissues or systemic circulation [209].
-
(f)
Allergic reactions Some individuals may be hypersensitive or allergic to certain materials or substances used in microneedles, such as metals or adhesives. Safety assessment involves evaluating the potential for allergic reactions through clinical testing or examining relevant patient populations [210].
-
(g)
Systemic effects In cases where microneedles are used for drug delivery, safety assessment includes evaluating the potential systemic effects of the delivered drug or its metabolites. This involves monitoring drug concentrations in the bloodstream, assessing pharmacokinetics, and evaluating any adverse systemic reactions [211].
When it comes to toxicity, microneedles present certain concerns that need to be addressed:
-
1.
Material toxicity The materials used in microneedles should be biocompatible to minimize the risk of toxicity. Common materials include silicon, metals, biodegradable polymers, and dissolvable sugar-based materials. Extensive toxicological studies should be conducted to evaluate the safety of these materials, both in vitro and in vivo to ensure they do not cause adverse effects when in contact with the skin or underlying tissues [212].
-
2.
Skin irritation Microneedles penetrate the skin and any material applied to the skin or delivered into the skin using microneedles should not cause irritation or sensitization. Toxicological studies assess the potential for local skin reactions, such as redness, swelling, or inflammation, to determine the safety profile of microneedle-based formulations [5].
-
3.
Systemic toxicity In some applications, microneedles are used for systemic drug delivery. In such cases, it is crucial to assess the potential for systemic toxicity caused by the delivered drugs or materials used in fabricating the microneedles. Toxicological studies including pharmacokinetic and toxicokinetic evaluations are performed to understand the absorption, distribution, metabolism, and elimination or excretion (ADME) of the drug or material and any potential systemic effects [213].
-
4.
Chemical interactions Microneedles may come into contact with various substances, such as drugs, cosmetics, or other chemicals. It is important to evaluate the compatibility and potential interactions between these substances and the materials used in the manufacture of the microneedles. Toxicological assessments can help identify any chemical interactions that may result in the generation of toxic by-products or compromised efficacy [212].
-
5.
Biodegradability Biodegradable microneedles are designed to dissolve or degrade over time, eliminating the need for their removal. The biodegradation process should be properly characterized to ensure that the breakdown products are nontoxic and do not pose a risk to the surrounding tissues or the environment [214].
Conclusions and future perspectives
This review article discussed the benefits, formulation techniques, characterization, applications, safety, commercialization, and regulatory guidelines in the application of MNs for drug delivery. MNs-based delivery system has opened newer opportunities for transdermal delivery of drugs, genes, vaccines, and other macromolecules. The article has shown that the benefits derived from MNs drug delivery system outweigh anticipated or known limitations. The formulation development strategies for MNs endow them with resilience during handling, adaptability, sustained release behavior, and impeccable stability. Possible side effects of MNs as drug delivery device are only rare and not life-threatening making MNs the preferred device for drug administration to the skin compared to other transdermal delivery tools. In spite of their perceived shortcomings, MNs always stand a good chance of scaling through regulatory hurdles for translation to commercialization and clinical use.
Looking ahead, it is important that any identified or imagined side effect arising from clinical application of MN be addressed at the point of design in order to maximize its benefits. The rigors and resources channeled into fabricating MNs could make affordability of the system an important issue, especially for orphan and generic drugs, and this should be addressed by adapting or modifying simple technologies that have been utilized in the manufacture of other transdermal patches as well as incorporating locally sourced pharmaceutical grade excipients. Stability of the formulation should be prioritized by ensuring that excessive sharpness of the microprojections is avoided in order to attain projected shelf life. Appropriate needle density and tip sharpness necessary to create optimum microconduits for efficient delivery of payload beyond the stratum corneum should be carefully determined before optimization of formulation. Potential variability in the drug loading capacity of MNs should be resolved to guarantee enhanced drug loading per needle. Data available to support the efficiency of MNs for gene and vaccine delivery are inadequate, and more data and further mechanisms should be provided. Where sterile MN is required, the processes should be simplified to ensure that sterility complements product efficiency and stability.
Availability of data and materials
This work is not an original research paper but a review paper. Availability of data is not applicable.
Abbreviations
- MNs:
-
Microneedles
- CPM:
-
Chemical penetrating materials
- PVP:
-
Polyvinyl pyrrolidone
- ISF:
-
Interstitial fluid
- API:
-
Active pharmaceutical ingredient
- CMC:
-
Carboxymethyl cellulose
- SARS:
-
Severe acute respiratory syndrome
- MERS:
-
Middle East respiratory syndrome
- COVID-19:
-
Corona virus disease: 19
- PDMS:
-
Polydimethylsiloxane
- HA:
-
Hyaluronic acid
- PVA:
-
Polyvinyl alcohol
- OVA:
-
Ovalbumin
- PLA:
-
Polylactic acid
- PLGA:
-
Polylactic-co-glycolic acid
- CT:
-
Computed tomography
- LNG:
-
Levonorgestrel
- FDA:
-
Food and Drug Administration
- PD1:
-
Programmed cell death protein-1
- FITC:
-
Fluorescein isothiocyanate labeling
- 3D:
-
Three-dimensional
- PEG 400:
-
Polyethylene glycol 400
- GRAS:
-
Generally regarded as safe
- TEWL:
-
Transepidermal water loss
- DOX:
-
Doxorubicin
- DLP:
-
Digital light processing
- SLA:
-
Stereolithography
- TPP:
-
Two-photon polymerization
- CLIP:
-
Continuous liquid interface production
- CAD:
-
Computer-aided design
- µSL:
-
Microstereolithography
- KOH:
-
Potassium hydroxide
- AFM:
-
Atomic force microscopy
- XPS:
-
X-ray photoelectron spectroscopy
- FTIR:
-
Fourier transform infrared spectroscopy
- SEM:
-
Scanning electron microscopy
- TEM:
-
Transmission electron microscope
- HPLC:
-
High-performance liquid chromatography
- DT:
-
Diphtheria toxoid
- TMC:
-
N-Trimethylchitosan
- IgG:
-
Immunoglobulin G
- ELISA:
-
Enzyme-linked immunosorbent assay
- SC:
-
Subcutaneous
- MTX:
-
Methotrexate
- CGRP:
-
Calcitonin gene-related peptide
- IMQ:
-
Imiquimod
- LD:
-
Lethal dose
- MD:
-
Median dose
- HD:
-
Highest dose
- SCMC:
-
Sodium carboxymethyl cellulose
- GLP-1:
-
Glucagon-like protein-1
- PEGDA:
-
Polyethylene glycol diacrylate
- HPV:
-
Human papilloma virus
- SEB:
-
Staphylococcus enterotoxin B
- AD:
-
Alzheimer’s disease
- DPH:
-
Donepezil hydrochloride
- LNC:
-
Lipid nanocapsule
- DHE:
-
Dihydroergotamine mesylate
- TRM:
-
Tissue-resident memory T cells
- APC:
-
Antigen-presenting cells
- DM:
-
Diabetes mellitus
- EMA:
-
European Medicines Agency
- ICH:
-
International Conference on Harmonization
- PK:
-
Pharmacokinetic
- GIT:
-
Gastrointestinal tract
- MRI:
-
Magnetic resonance imaging
- MTD:
-
Minimum toxic dose
References
Dharadhar S, Majumdar A, Dhoble S, Patravale V (2019) Microneedles for transdermal drug delivery: a systematic review. Drug Dev Ind Pharm 45:188–201. https://doi.org/10.1080/03639045.2018.1539497
Anjani QK, Pandya AK, Demartis S, Domínguez-Robles J, Moreno-Castellanos N, Li H, Gavini E, Patravale VB, Donnelly RF (2023) Liposome-loaded polymeric microneedles for enhanced skin deposition of rifampicin. Int J Pharm 646:123446. https://doi.org/10.1016/j.ijpharm.2023.123446
Abrbekoh FN, Salimi L, Saghati S, Amini H, Karkan SF, Moharamzadeh K, Sokullu E, Rahbarghazi R (2022) Application of microneedle patches for drug delivery; doorstep to novel therapies. J Tissue Eng 13:1–25. https://doi.org/10.1177/20417314221085390
Donnelly RF, Singh TRR, Woolfson AD (2010) Microneedle-based drug delivery systems: microfabrication, drug delivery, and safety. Drug Deliv 17(4):187–207. https://doi.org/10.3109/10717541003667798
Avcil M, Çelik A (2021) Microneedles in drug delivery: progress and challenges. Micromachines 12:1321. https://doi.org/10.3390/mi12111321
Kulkarni D, Damiri F, Rojekar S, Zehravi M, Ramproshad S, Dhoke D, Musale S, Mulani AA, Modak P, Paradhi R, Vitore J, Rahman MH, Berrada M, Giram PS, Cavalu S (2022) Recent advancements in microneedle technology for multifaceted biomedical applications. Pharmaceutics 14:1097. https://doi.org/10.3390/pharmaceutics14051097
Waghule T, Singhvi G, Dubey SK, Pandey MM, Gupta G, Singh M, Dua K (2019) Microneedles: a smart approach and increasing potential for transdermal drug delivery system. Biomed Pharmacother 109:1249–1258. https://doi.org/10.1016/j.biopha.2018.10.078
Damiri F, Kommineni N, Ebhodaghe SO, Bulusu R, Jyothi VGSS, Sayed AA, Awaji AA, Germoush MO, Al-malky HS, Nasrullah MZ, Rahman MH, Abdel-Daim MM, Berrada M (2022) Microneedle-based natural polysaccharide for drug delivery systems (DDS): progress and challenges. Pharmaceuticals 15:190. https://doi.org/10.3390/ph15020190
Migdadi EM, Courtenay AJ, Tekko IA, McCrudden MTC, Kearney MC, McAlister E, McCarthy HO, Donnelly RF (2018) Hydrogel-forming microneedles enhance transdermal delivery of metformin hydrochloride. J Control Release 285:142–151. https://doi.org/10.1016/j.jconrel.2018.07.009
Aldawood FK, Andar A, Desai SA (2021) A comprehensive review of microneedles: types, materials, processes, characterizations and applications. Polymers (Basel) 13(16):2815. https://doi.org/10.3390/polym13162815
Jakka D, Matadh AV, Shivakumar HN, Maibach H, Murthy SN (2022) Polymer coated polymeric (PCP) microneedles for sampling of drugs and biomarkers from tissues. Eur J Pharm Sci 175:106203. https://doi.org/10.1016/j.ejps.2022.106203
Guillot AJ, Cordeiro AS, Donnelly RF, Montesinos MC, Garrigues TM, Melero A (2020) Microneedle-based delivery: an overview of current applications and trends. Pharmaceutics 12:1–28. https://doi.org/10.3390/pharmaceutics12060569
Tucak A, Sirbubalo M, Hindija L, Rahić O, Hadžiabdić J, Muhamedagić K, Čekić A, Vranić E (2020) Microneedles: characteristics, materials, production methods and commercial development. Micromachines 11(11):961. https://doi.org/10.3390/mi11110961
Demir YK, Akan Z, Kerimoglu O (2013) Characterization of polymeric microneedle arrays for transdermal drug delivery. PLoS ONE 8(10):e77289. https://doi.org/10.1371/journal.pone.0077289
Xu J, Xu D, Xuan X, He H (2021) Advances of microneedles in biomedical applications. Molecules 26(19):5912. https://doi.org/10.3390/molecules26195912
Olowe M, Parupelli SK, Desai S (2022) A review of 3D-printing of microneedles. Pharmaceutics 14(12):2693. https://doi.org/10.3390/pharmaceutics14122693
Raphael AP, Crichton ML, Falconer RJ, Meliga S, Chen X, Fernando GJP, Huang H, Kendall MA (2016) Formulations for microprojection/microneedle vaccine delivery: structure, strength and release profiles. J Control Release 10(225):40–52. https://doi.org/10.1016/j.jconrel.2016.01.027
Henry S, McAllister DV, Allen MG, Prausnitz MR (1998) Microfabricated microneedles: a novel approach to transdermal drug delivery. J Pharm Sci 87(8):922–925. https://doi.org/10.1021/js980042+
Hoang MT, Ita KB, Bair DA (2015) Solid microneedles for transdermal delivery of amantadine hydrochloride and pramipexole dihydrochloride. Pharmaceutics 7(4):379–396. https://doi.org/10.3390/pharmaceutics7040379
Bariya SH, Gohel MC, Mehta TA, Sharma OP (2012) Microneedles: An emerging transdermal drug delivery system. J Pharm Pharmacol 64(1):11–29. https://doi.org/10.1111/j.2042-7158.2011.01369.x
Larrañeta E, Lutton REM, Woolfson AD, Donnelly RF (2016) Microneedle arrays as transdermal and intradermal drug delivery systems: materials science, manufacture and commercial development. Mater Sci Eng R Rep 104:1–32. https://doi.org/10.1016/j.mser.2016.03.001
Prausnitz MR, Langer R (2008) Transdermal drug delivery. Nature Biotechnol 26(11):1261–1268. https://doi.org/10.1038/nbt.1504
Haj-Ahmad R, Khan H, Arshad MS, Rasekh M, Hussain A, Walsh S, Li X, Chang MW, Ahmad Z (2015) Microneedle coating techniques for transdermal drug delivery. Pharmaceutics 7(4):486–502. https://doi.org/10.3390/pharmaceutics7040486
Jiang J, Gill HS, Ghate D, McCarey BE, Patel SR, Edelhauser HF, Prausnitz MR (2007) Coated microneedles for drug delivery to the eye. Invest Ophthalmol Vis Sci 48(9):4038–4043. https://doi.org/10.1167/iovs.07-0066
Quinn HL, Bonham L, Hughes CM, Donnelly RF (2015) Design of a dissolving microneedle platform for transdermal delivery of a fixed-dose combination of cardiovascular drugs. J Pharm Sci 104(10):3490–3500. https://doi.org/10.1002/jps.24563
Kwon KM, Lim SM, Choi S, Kim DH, Jin HE, Jee G, Hong KJ, Kim JY (2017) Microneedles: quick and easy delivery methods of vaccines. Clin Exp Vaccine Res 6(2):156–159. https://doi.org/10.7774/cevr.2017.6.2.156
Bilal M, Mehmood S, Raza A, Hayat U, Rasheed T, Iqbal HMN (2021) Microneedles in smart drug delivery. Adv Wound Care (New Rochelle) 10(4):204–219. https://doi.org/10.1089/wound.2019.1122
Ye Y, Yu J, Wen D, Kahkoska AR, Gu Z (2018) Polymeric microneedles for transdermal protein delivery. Adv Drug Deliv Rev 127:106–118. https://doi.org/10.1016/j.addr.2018.01.015
Mishra R, Maiti TK, Bhattacharyya TK (2019) Feasibility studies on nafion membrane actuated micropump integrated with hollow microneedles for insulin delivery device. J Microelectromech Syst 28(6):987–996. https://doi.org/10.1109/JMEMS.2019.2939189
Zhang P, Dalton C, Jullien GA (2009) Design and fabrication of MEMS-based microneedle arrays for medical applications. Microsyst Technol 15(7):1073–1082. https://doi.org/10.1007/s00542-009-0883-5
Menon I, Bagwe P, Gomes KB, Bajaj L, Gala R, Uddin MN, D’Souza MJ, Zughaier SM (2021) Microneedles: a new generation vaccine delivery system. Micromachines (Basel) 12(4):435. https://doi.org/10.3390/mi12040435
Zhang L, Guo R, Wang S, Yang X, Ling G, Zhang P (2021) Fabrication, evaluation and applications of dissolving microneedles. Int J Pharm 604:120749. https://doi.org/10.1016/j.ijpharm.2021.120749
Rodgers AM, Cordeiro AS, Donnelly RF (2019) Technology update: dissolvable microneedle patches for vaccine delivery. Med Devices (Auckl) 12:379–398. https://doi.org/10.2147/MDER.S198220
Ling MH, Chen MC (2013) Dissolving polymer microneedle patches for rapid and efficient transdermal delivery of insulin to diabetic rats. Acta Biomater 9(11):8952–8961. https://doi.org/10.1016/j.actbio.2013.06.029
Sullivan SP, Koutsonanos DG, Del Pilar MM, Lee JW, Zarnitsyn V, Choi SO, Murthy N, Compans RW, Skountzou I, Prausnitz MR (2010) Dissolving polymer microneedle patches for influenza vaccination. Nat Med 16(8):915–920. https://doi.org/10.1038/nm.2182
Kim YC, Park JH, Prausnitz MR (2012) Microneedles for drug and vaccine delivery. Adv Drug Deliv Rev 64(14):1547–1568. https://doi.org/10.1016/j.addr.2012.04.005
Hong X, Wu Z, Chen L, Wu F, Wei L, Yuan W (2014) Hydrogel microneedle arrays for transdermal drug delivery. Nanomicro Lett 6(3):191–199. https://doi.org/10.1007/BF03353783
Al Sulaiman D, Chang JYH, Bennett NR, Topouzi H, Higgins CA, Irvine DJ, Ladame S (2019) Hydrogel-coated microneedle arrays for minimally invasive sampling and sensing of specific circulating nucleic acids from skin interstitial fluid. ACS Nano 13(8):9620–9628. https://doi.org/10.1021/acsnano.9b04783
Courtenay AJ, McAlister E, McCrudden MTC, Vora L, Steiner L, Levin G, Levy-Nissenbaum E, Shterman N, Kearny MC, McCarthy HO, Donnelly RF (2020) Hydrogel-forming microneedle arrays as a therapeutic option for transdermal esketamine delivery. J Control Release 322:177–186. https://doi.org/10.1016/j.jconrel.2020.03.026
Jun H, Ahn MH, Choi IJ, Baek SK, Park JH, Choi SO (2018) Immediate separation of microneedle tips from base array during skin insertion for instantaneous drug delivery. RSC Adv 8(32):17786–17796. https://doi.org/10.1039/c8ra02334d
Nguyen HX, Nguyen CN (2023) Microneedle-mediated transdermal delivery of biopharmaceuticals. Pharmaceutics 15(1):277. https://doi.org/10.3390/pharmaceutics15010277
Woodhouse I, Nejati S, Selvamani V, Jiang H, Chittiboyina S, Grant J, Mutlu Z, Waimin J, Abutaleb NS, Seleem MN, Rahimi R (2021) Flexible microneedle array patch for chronic wound oxygenation and biofilm eradication. ACS Appl Bio Mater 4(7):5405–5415. https://doi.org/10.1021/acsabm.1c00087
Chen Y, Xian Y, Carrier AJ, Youden B, Servos M, Cui S, Luan T, Lin S, Zhang X (2020) A simple and cost-effective approach to fabricate tunable length polymeric microneedle patches for controllable transdermal drug delivery. RSC Adv 10(26):15541–15546. https://doi.org/10.1039/d0ra01382j
Dathathri E, Lal S, Mittal M, Thakur G, De S (2020) Fabrication of low-cost composite polymer-based microneedle patch for transdermal drug delivery. Appl Nanosci 10:371–377. https://doi.org/10.1007/s13204-019-01190-3
Donnelly RF, Singh TRR, Alkilani AZ, McCrudden MTC, O’Neill S, O’Mahony C, Armstrong K, McLoone N, Kole P, Woolfson AD (2013) Hydrogel-forming microneedle arrays exhibit antimicrobial properties: potential for enhanced patient safety. Int J Pharm 451(1–2):76–91. https://doi.org/10.1016/j.ijpharm.2013.04.045
Li WZ, Huo MR, Zhou JP, Zhou YQ, Hao BH, Liu T, Zhang Y (2010) Super-short solid silicon microneedles for transdermal drug delivery applications. Int J Pharm 389(1–2):122–129. https://doi.org/10.1016/j.ijpharm.2010.01.024
Baek C, Han M, Min J, Prausnitz MR, Park JH (2011) Local transdermal delivery of phenylephrine to the anal sphincter muscle using microneedles. J Control Release 154(2):138. https://doi.org/10.1016/j.jconrel.2011.05.004
Loizidou EZ, Inoue NT, Ashton-Barnett J, Barrow DA, Allender CJ (2016) Evaluation of geometrical effects of microneedles on skin penetration by CT scan and finite element analysis. Eur J Pharm Biopharm 107:1–6. https://doi.org/10.1016/j.ejpb.2016.06.023
Li Y, Hu X, Dong Z, Chen Y, Zhao W, Wang Y, Zhang L, Chen M, Wu C, Wang Q (2020) Dissolving microneedle arrays with optimized needle geometry for transcutaneous immunization. Eur J Pharm Sci 151:105361. https://doi.org/10.1016/j.ejps.2020.105361
Zoudani EL, Soltani M (2020) A new computational method of modeling and evaluation of dissolving microneedle for drug delivery applications: Extension to theoretical modeling of a novel design of microneedle (array in array) for efficient drug delivery. Eur J Pharm Sci 150:105339. https://doi.org/10.1016/j.ejps.2020.105339
Römgens AM, Bader DL, Bouwstra JA, Baaijens FPT, Oomens CWJ (2014) Monitoring the penetration process of single microneedles with varying tip diameters. J Mech Behav Biomed Mater 40:397–405. https://doi.org/10.1016/j.jmbbm.2014.09.015
Makvandi P, Kirkby M, Hutton ARJ, Shabani M, Yiu CKY, Baghbantaraghdari Z, Jamaledin R, Carlotti M, Mazzolai B, Mattoli V, Donnelly RF (2021) Engineering microneedle patches for improved penetration: analysis, skin models and factors affecting needle insertion. Nanomicro Lett 13:1–41. https://doi.org/10.1007/s40820-021-00611-9
Lee S, Fakhraei Lahiji S, Jang J, Jang M, Jung H (2019) Micropillar integrated dissolving microneedles for enhanced transdermal drug delivery. Pharmaceutics 11(8):402. https://doi.org/10.3390/pharmaceutics11080402
Kearney MC, McKenna PE, Quinn HL, Courtenay AJ, Larrañeta E, Donnelly RF (2019) Design and development of liquid drug reservoirs for microneedle delivery of poorly soluble drug molecules. Pharmaceutics 11(11):605. https://doi.org/10.3390/pharmaceutics11110605
Choi IJ, Kang A, Ahn MH, Jun H, Baek SK, Park JH, Na W, Choi SO (2018) Insertion-responsive microneedles for rapid intradermal delivery of canine influenza vaccine. J Control Release 286:460–466. https://doi.org/10.1016/j.jconrel.2018.08.017
Li W, Terry RN, Tang J, Feng MR, Schwendeman SP, Prausnitz MR (2019) Rapidly separable microneedle patch for the sustained release of a contraceptive. Nat Biomed Eng 3(3):220–229. https://doi.org/10.1038/s41551-018-0337-4
Li W, Tang J, Terry RN, Li S, Brunie A, Callahan RL, Noel RK, Rodríguez CA, Schwendeman SP, Prausnitz MR (2019) Long-acting reversible contraception by effervescent microneedle patch. Sci Adv 5(11):eaaw8145. https://doi.org/10.1126/sciadv.aaw8145
Miyano T, Tobinaga Y, Kanno T, Matsuzaki Y, Takeda H, Wakui M, Hanada K (2005) Sugar microneedles as transdermic drug delivery system. Biomed Microdevices 7(3):185–188. https://doi.org/10.1007/s10544-005-3024-7
Li Y, Zhang H, Yang R, Laf Y, Schmill U, Hu W, Kaddoura M, Blondeel EJM, Cui B (2019) Fabrication of sharp silicon hollow microneedles by deep-reactive ion etching towards minimally invasive diagnostics. Microsyst Nanoeng 5:41. https://doi.org/10.1038/s41378-019-0077-y
Chabri F, Bouris K, Jones T, Barrow D, Hann A, Allender C, Brain K, Birchall J (2004) Microfabricated silicon microneedles for nonviral cutaneous gene delivery. Brit J Dermatol 150(5):869–877. https://doi.org/10.1111/j.1365-2133.2004.05921.x
Kaupp G (2009) Mechanochemistry: the varied applications of mechanical bond-breaking. CrystEngComm 11(3):388–403. https://doi.org/10.1039/B810822F
Martin CJ, Allender CJ, Brain KR, Morrissey A, Birchall JC (2012) Low temperature fabrication of biodegradable sugar glass microneedles for transdermal drug delivery applications. J Control Release 158(1):93–101. https://doi.org/10.1016/j.jconrel.2011.10.024
Damiri F, Kommineni N, Ebhodaghe SO, Bulusu R, Jyothi VGSS, Sayed AA, Awaji AA, Germoush MO, Al-Malky HS, Nasrullah MZ, Rahman MH, Abdel-Daim MM, Berrada M (2022) Microneedle-based natural polysaccharide for drug delivery systems (DDS): progress and challenges. Pharmaceuticals (Basel) 15(2):1–26. https://doi.org/10.3390/ph15020190
Wang C, Ye Y, Hochu GM, Sadeghifar H, Gu Z (2016) Enhanced cancer immunotherapy by microneedle patch-assisted delivery of anti-PD1 antibody. Nano Lett 16(4):2334–2340. https://doi.org/10.1021/acs.nanolett.5b05030
Jiang Y, Chen B, Liu Y, Zhufu Z, Yan X, Hou X, Dai J, Tan Q (2013) Effect of collagen scaffold with adipose-derived stromal vascular fraction cells on diabetic wound healing: a study in a diabetic porcine model. Tissue Eng Regen Med 10(4):192–199. https://doi.org/10.1007/s13770-013-0001-8
Liu S, Jin MN, Quan YS, Kamiyama F, Katsumi H, Sakane T, Yamamoto A (2012) The development and characteristics of novel microneedle arrays fabricated from hyaluronic acid, and their application in the transdermal delivery of insulin. J Control Release 161(3):933–941. https://doi.org/10.1016/j.jconrel.2012.05.030
Fakhraei Lahiji S, Seo SH, Kim S, Dangol M, Shim J, Li CG, Ma Y, Lee C, Kang G, Yang H, Choi KY, Jung H (2018) Transcutaneous implantation of valproic acid-encapsulated dissolving microneedles induces hair regrowth. Biomaterials 167:69–79. https://doi.org/10.1016/j.biomaterials.2018.03.019
Chen MC, Ling MH, Lai KY, Pramudityo E (2012) Chitosan microneedle patches for sustained transdermal delivery of macromolecules. Biomacromol 13(12):4022–4031. https://doi.org/10.1021/bm301293d
Nair SS (2019) Chitosan-based transdermal drug delivery systems to overcome skin barrier functions. J Drug Deliv Ther 9(1):266–270. https://doi.org/10.22270/jddt.v9i1.2180
Li Z, He Y, Deng L, Zhang Z, Lin Y (2020) A fast-dissolving microneedle array loaded with chitosan nanoparticles to evoke systemic immune responses in mice. J Mater Chem B 8(3):216–225. https://doi.org/10.1039/c9tb90179e
Wang M, Hu L, Xu C (2017) Recent advances in the design of polymeric microneedles for transdermal drug delivery and biosensing. Lab Chip 17:1373–1387. https://doi.org/10.1039/C7LC00016B
Donnelly RF, Majithiya R, Singh TRR, Morrow DIJ, Garland MJ, Demir YK, Migalska K, Ryan E, Gillen D, Scott CJ, Woolfson AD (2011) Design, optimization and characterisation of polymeric microneedle arrays prepared by a novel laser-based micromoulding technique. Pharm Res 28(1):41–57. https://doi.org/10.1007/s11095-010-0169-8
Azizi Machekposhti S, Nguyen AK, Vanderwal L, Stafslien S, Narayan RJ (2022) Micromolding of amphotericin-B-loaded methoxyethylene–maleic anhydride copolymer microneedles. Pharmaceutics 14(8):1551. https://doi.org/10.3390/pharmaceutics14081551
Amodwala S, Kumar P, Thakkar HP (2017) Statistically optimized fast dissolving microneedle transdermal patch of meloxicam: a patient friendly approach to manage arthritis. Eur J Pharm Sci 104:114–123. https://doi.org/10.1016/j.ejps.2017.04.001
Nguyen HX, Bozorg BD, Kim Y, Wieber A, Birk G, Lubda D, Banga AK (2018) Poly(vinylalcohol) microneedles: fabrication, characterization, and application for transdermal drug delivery of doxorubicin. Eur J Pharm Biopharm 129:88–103. https://doi.org/10.1016/j.ejpb.2018.05.017
Jung JH, Jin SG (2021) Microneedle for transdermal drug delivery: current trends and fabrication. J Pharm Investig 51(5):503–517. https://doi.org/10.1007/s40005-021-00512-4
Mahadevan G, Sheardown H, Selvaganapathy P (2013) PDMS embedded microneedles as a controlled release system for the eye. J Biomater Appl 28(1):20–27. https://doi.org/10.1177/0885328211433778
Patel S, Edelhuaser HF, Nickerson JM, Prausnitz MR (2008) Suprachoroidal drug delivery using microneedles. Invest Ophthalmol Vis Sci 49(13):5006. https://doi.org/10.1007/s11095-010-0271-y
Ita K (2018) Ceramic microneedles and hollow microneedles for transdermal drug delivery: two decades of research. J Drug Deliv Sci Technol 44:314–322. https://doi.org/10.1016/j.jddst.2018.01.004
Vos PJ, Kuijt N, Kaya M, Rol S, van der Maaden K (2020) Nanoporous microneedle arrays seamlessly connected to a drug reservoir for tunable transdermal delivery of memantine. Eur J Pharm Sci 150:105331. https://doi.org/10.1016/j.ejps.2020.105331
Gholami S, Mohebi MM, Hajizadeh-Saffar E, Ghanian MH, Zarkesh I, Baharvand H (2019) Fabrication of microporous inorganic microneedles by centrifugal casting method for transdermal extraction and delivery. Int J Pharm 558:299–310. https://doi.org/10.1016/j.ijpharm.2018.12.089
Pere CPP, Economidou SN, Lall G, Ziraud C, Boateng JS, Alexander BD, Lamprou DA, Douroumis D (2018) 3D printed microneedles for insulin skin delivery. Int J Pharm 544(2):425–432. https://doi.org/10.1016/j.ijpharm.2018.03.031
Economidou SN, Lamprou DA, Douroumis D (2018) 3D printing applications for transdermal drug delivery. Int J Pharm 544(2):415–424. https://doi.org/10.1016/j.ijpharm.2018.01.031
Johnson AR, Caudill CL, Tumbleston JR, Bloomquist CJ, Moga KA, Ermoshkin A, Shirvanyants D, Mecham SJ, Luft JC, DeSimone JM (2016) Single-step fabrication of computationally designed microneedles by continuous liquid interface production. PLoS ONE 11(9):e0162518. https://doi.org/10.1371/journal.pone.0162518
Rad ZF, Prewett PD, Davies GJ (2021) An overview of microneedle applications, materials, and fabrication methods. Beilstein J Nanotechnol 12:1034–1046. https://doi.org/10.3762/bjnano.12.77
Lee KS, Yang DY, Park SH, Kim RH (2006) Recent developments in the use of two-photon polymerization in precise 2D and 3D microfabrication. Polym Adv Technol 17(2):72–82. https://doi.org/10.1002/pat.664
Mckee S, Lutey A, Sciancalepore C, Poli F, Selleri S, Cucinotta A (2022) Microfabrication of polymer microneedle arrays using two-photon polymerization. J Photochem Photobiol B Biol 229:112424. https://doi.org/10.1016/j.jphotobiol.2022.112424
Gittard SD, Ovsianikov A, Chichkov BN, Doraiswamy A, Narayan RJ (2010) Two-photon polymerization of microneedles for transdermal drug delivery. Expert Opin Drug Deliv 7(4):513–533. https://doi.org/10.1517/17425241003628171
Lu Y, Mantha SN, Crowder DC, Chinchilla S, Shah KN, Yun YH, Wicker RB, Choi JW (2015) Microstereolithography and characterization of poly(propylene fumarate)-based drug-loaded microneedle arrays. Biofabrication 7(4):045001. https://doi.org/10.1088/1758-5090/7/4/045001
Gittard SD, Miller PR, Jin C, Martin TN, Boehm RD, Chisholm BJ, Stafslien SJ, Daniels JW, Cilz N, Monteiro-Riviere NA, Nasir A, Narayan RJ (2011) Deposition of antimicrobial coatings on microstereolithography-fabricated microneedles. JOM 63(6):59–68. https://doi.org/10.1007/s11837-011-0093-3
Dardano P, de Martino S, Battisti M, Miranda B, Rea I, de Stefano L (2021) One-shot fabrication of polymeric hollow microneedles by standard photolithography. Polymers (Basel) 13(4):520. https://doi.org/10.3390/polym13040520
Kathuria H, Kochhar JS, Fong MHM, Hashimoto M, Iliescu C, Yu H, Kang L (2015) Polymeric microneedle array fabrication by photolithography. J Vis Exp 105:52914. https://doi.org/10.3791/52914
Faraji Rad Z, Prewett PD, Davies GJ (2021) High-resolution two-photon polymerization: the most versatile technique for the fabrication of microneedle arrays. Microsyst Nanoeng 7:71. https://doi.org/10.1038/s41378-021-00298-3
Wilke N, Hibert C, O’Brien J, Morrissey A (2005) Silicon microneedle electrode array with temperature monitoring for electroporation. Sens Actuators A Phys 123–124:319–325. https://doi.org/10.1016/j.sna.2005.05.017
Birchall J, Coulman S, Pearton M, Allender C, Brain K, Anstey A, Gateley C, Wilke N, Morrissey A (2005) Cutaneous DNA delivery and gene expression in ex vivo human skin explants via wet-etch microfabricated microneedles. J Drug Target 13(7):415–421. https://doi.org/10.1080/10611860500383705
Nagarkar R, Singh M, Nguyen HX, Jonnalagadda S (2020) A review of recent advances in microneedle technology for transdermal drug delivery. J Drug Deliv Sci Technol 59:101923. https://doi.org/10.1016/j.jddst.2020.101923
Singh P, Carrier A, Chen Y, Lin S, Wang J, Cui S, Zhang X (2019) Polymeric microneedles for controlled transdermal drug delivery. J Control Release 315:97–113. https://doi.org/10.1016/j.jconrel.2019.10.022
Juster H, Aar B, Brouwer H (2019) A review on microfabrication of thermoplastic polymer-based microneedle arrays. Polym Eng Sci 59(5):877–890. https://doi.org/10.1002/pen.25078
Ahmad Z, Khan MI, Siddique MI, Sarwar HS, Shahnaz G, Hussain SZ, Bukhari NI, Hussain I, Sohail MF (2020) Fabrication and characterization of thiolated chitosan microneedle patch for transdermal delivery of tacrolimus. AAPS PharmSciTech 21(2):68. https://doi.org/10.1208/s12249-019-1611-9
Castilla-Casadiego DA, Carlton H, Gonzalez-Nino D, Miranda-Muñoz KA, Daneshpour R, Huitink D, Prinz G, Powell J, Greenlee L, Almodovar J (2021) Design, characterization, and modeling of a chitosan microneedle patch for transdermal delivery of meloxicam as a pain management strategy for use in cattle. Mater Sci Eng C Mater Biol Appl 118:111544. https://doi.org/10.1016/j.msec.2020.111544
Akhter F, Bascos GNW, Canelas M, Griffin B, Hood RL (2020) Mechanical characterization of a fiberoptic microneedle device for controlled delivery of fluids and photothermal excitation. J Mech Behav Biomed Mater 112:104042. https://doi.org/10.1016/j.jmbbm.2020.104042
Alafnan A, Seetharam AA, Hussain T, Gupta MS, Rizvi SMD, Moin A, Alamri A, Unnisa A, Awadelkareem AM, Elkhalifa AO, Jayahanumaiah P, Khalid M, Balashanmugam N (2022) Development and characterization of PEGDA microneedles for localized drug delivery of gemcitabine to treat inflammatory breast cancer. Materials (Basel) 15(21):7693. https://doi.org/10.3390/ma15217693
Kolli CS, Banga AK (2008) Characterization of solid maltose microneedles and their use for transdermal delivery. Pharm Res 25(1):104–113. https://doi.org/10.1007/s11095-007-9350-0
Lutton RE, Moore J, Larrañeta E, Ligett S, Woolfson AD, Donnelly RF (2015) Microneedle characterization: the need for universal acceptance criteria and GMP specifications when moving towards commercialization. Drug Deliv Transl Res 5(4):313–331. https://doi.org/10.1007/s13346-015-0237-z
Pineda-Álvarez RA, Bernad-Bernad MJ, Rodríguez-Cruz IM, Escobar-Chávez JJ (2022) Development and characterization of starch/gelatin microneedle arrays loaded with lecithin-gelatin nanoparticles of losartan for transdermal delivery. J Pharm Innov 17:71–84. https://doi.org/10.1007/s12247-020-09494-6
Aung NN, Ngawhirunpat T, Rojanarata T, Patrojanasophon P, Pamornpathomkul B, Opanasopit P (2020) Fabrication, characterization and comparison of α-arbutin loaded dissolving and hydrogel forming microneedles. Int J Pharm 586:119508. https://doi.org/10.1016/j.ijpharm.2020.119508
Wang PC, Paik SJ, Kim SH, Allen MG (2014) Hypodermic needle-like hollow polymer microneedle array: fabrication and characterization. J Microelectromech Syst 23(4):991–998. https://doi.org/10.1109/JMEMS.2014.2307320
Dugam S, Tade R, Dhole R, Nangare S (2021) Emerging era of microneedle array for pharmaceutical and biomedical applications : recent advances and toxicological perspectives. Future J Pharm Sci 7:19. https://doi.org/10.1186/s43094-020-00176-1
Bal SM, Ding Z, Kersten GFA, Jiskoot W, Bouwstra JA (2010) Microneedle-based transcutaneous immunisation in mice with N-trimethyl chitosan adjuvanted diphtheria toxoid formulations. Pharm Res 27(9):1837–1847. https://doi.org/10.1007/s11095-010-0182-y
Kim E, Erdos G, Huang S, Kenniston TW, Balmert SC, Carey CD, Raj VS, Epperly MW, Klimstra WB, Haagmans BL, Korkmaz E, Falo LD, Gambotto A (2020) Microneedle array delivered recombinant coronavirus vaccines: immunogenicity and rapid translational development. EBioMedicine 55:102743. https://doi.org/10.1016/j.ebiom.2020.102743
Kearney MC, Caffarel-Salvador E, Fallows SJ, McCarthy HO, Donnelly RF (2016) Microneedle-mediated delivery of donepezil: potential for improved treatment options in Alzheimer’s disease. Eur J Pharm Biopharm 103:43–50. https://doi.org/10.1016/j.ejpb.2016.03.026
Du H, Liu P, Zhu J, Lan J, Li Y, Zhang L, Zhu J, Tao J (2019) Hyaluronic acid dissolving microneedle patch loaded with methotrexate for improved treatment of psoriasis acid microneedle with methotrexate for improved treatment of psoriasis. ACS Appl Mater Interfaces 11(46):43588–43598. https://doi.org/10.1021/acsami.9b15668
Xie X, Pascual C, Lieu C, Oh S, Wang J, Zou B, Xie J, Li Z, Xie J, Yeomans DC, Wu MX, Xie XS (2017) Analgesic microneedle patch for neuropathic pain therapy. ACS Nano 11(1):395–406. https://doi.org/10.1021/acsnano.6b06104
Liu S, Yeo DC, Wiraja C, Tey HL, Mrksich M, Xu C (2017) Peptide delivery with poly(ethylene glycol) diacrylate microneedles through swelling effect. Bioeng Transl Med 2(3):258–267. https://doi.org/10.1002/btm2.10070
Zhu S, Zhang B, Wang Y, He Y, Qian G, Deng L, Zhang ZR (2021) A bilayer microneedle for therapeutic peptide delivery towards the treatment of diabetes in Db/Db mice. J Drug Deliv Sci Technol 62:102336. https://doi.org/10.1016/j.jddst.2021.102336
Patil S, Vijayanand S, Joshi D, Menon I, Gomes KB, Kale A, Bagwe P, Yacoub S, Uddin MN, D’Souza MJ (2023) Subunit microparticulate vaccine delivery using microneedles trigger significant SARS-spike-specific humoral and cellular responses in a preclinical murine model. Int J Pharm 632:122583. https://doi.org/10.1016/j.ijpharm.2023.122583
Ray S, Wirth DM, Ortega-Rivera OA, Steinmetz NF, Pokorski JK (2022) Dissolving microneedle delivery of a prophylactic HPV vaccine. Biomacromol 23(3):903–912. https://doi.org/10.1021/acs.biomac.1c01345
Koutsonanos DG, Esser ES, McMaster SR, Kalluri P, Lee JW, Prausnitz MR, Skountzou I, Denning TL, Kohlmeier JE, Compans RW (2015) Enhanced immune responses by skin vaccination with influenza subunit vaccine in young hosts. Vaccine 33(37):4675–4682. https://doi.org/10.1016/j.vaccine.2015.01.086
Liu S, Zhang S, Duan Y, Niu Y, Gu H, Zhao Z, Zhang S, Yang Y, Wang X, Gao Y, Yang P (2019) Transcutaneous immunization of recombinant staphylococcal enterotoxin B protein using a dissolving microneedle provides potent protection against lethal enterotoxin challenge. Vaccine 37(29):3810–3819. https://doi.org/10.1016/j.vaccine.2019.05.055
Li W, Terry RN, Tang J, Feng MR, Schwendeman SP, Prausnitz MR (2019) Rapidly separable microneedle patch for the sustained release of a contraceptive. Nature Biomed Eng 3(3):220–229. https://doi.org/10.1038/s41551-018-0337-4
Naito C, Katsumi H, Suzuki T, Quan YS, Kamiyama F, Sakane T, Yamamoto A (2018) Self-dissolving microneedle arrays for transdermal absorption enhancement of human parathyroid hormone (1–34). Pharmaceutics 10(4):215. https://doi.org/10.3390/pharmaceutics10040215
Yao Z, Tong X, Hao X, Chuandong C, Xudong L, Fei W, Shen L, Cunyi F (2021) Promotion of collagen deposition during skin healing through Smad3/MTOR pathway by parathyroid hormone-loaded microneedle. Mater Sci Eng C 119:111446. https://doi.org/10.1016/j.msec.2020.111446
Shim DH, Nguyen TT, Park PG, Kim MJ, Park BW, Jeong HR, Kim DS, Joo HW, Choi SO, Park JH, Lee JM (2019) Development of botulinum toxin A-coated microneedles for treating palmar hyperhidrosis. Mol Pharm 16(12):4913–4919. https://doi.org/10.1021/acs.molpharmaceut.9b00794
Zhu T, Yu X, Yi X, Guo X, Li L, Hao Y, Wang W (2022) Lidocaine-loaded hyaluronic acid adhesive microneedle patch for oral mucosal topical anesthesia. Pharmaceutics 14(4):686. https://doi.org/10.3390/pharmaceutics14040686
Huang D, Fu X, Zhang X, Zhao Y (2022) Christmas tree-shaped microneedles as FOLFIRINOX spatiotemporal delivery system for pancreatic cancer treatment. Research (Wash D C). https://doi.org/10.34133/2022/9809417
Lan X, Zhu W, Huang X, Yu Y, Xiao H, Jin L, Pu JJ, Xie X, She J, Lui VWY, Chen HJ, Su YX (2020) Microneedles-loaded with anti-PD-1-cisplatin nanoparticles for synergistic cancer immuno-chemotherapy. Nanoscale 12(36):18885–18898. https://doi.org/10.1039/D0NR04213G
Fu JJ, Li CW, Liu Y, Chen MY, Zhang Q, Yu XY, Wu B, Li JX, Du LR, Dang YY, Wu D, Wei MY, Lin ZQ, Lei XP (2020) The microneedles carrying cisplatin and IR820 to perform synergistic chemo-photodynamic therapy against breast cancer. J Nanobiotechnol 18(1):146. https://doi.org/10.1186/s12951-020-00697-0
Abd-El-Azim H, Tekko IA, Ali A, Ramadan A, Nafee N, Khalafallah N, Rahman T, Mcdaid W, Aly RG, Vora LK, Bell SJ, Furlong F, McCarthy HO, Donnelly RF (2022) Hollow microneedle assisted intradermal delivery of hypericin lipid nanocapsules with light enabled photodynamic therapy against skin cancer. J Control Release 348:849–869. https://doi.org/10.1016/j.jconrel.2022.06.027
Roy G, Galigama RD, Thorat VS, Garg P, Venuganti VVK (2020) Microneedle ocular patch: fabrication, characterization, and ex-vivo evaluation using pilocarpine as model drug. Drug Dev Ind Pharm 46(7):1114–1122. https://doi.org/10.1080/03639045.2020.1776317
Cui M, Zheng M, Wiraja C, Chew SWT, Mishra A, Mayandi V, Lakshminarayanan R, Xu C (2021) Ocular delivery of predatory bacteria with cryomicroneedles against eye infection. Adv Sci (Weinh) 8(21):e2102327. https://doi.org/10.1002/advs.202102327
Jung JH, Chiang B, Grossniklaus HE, Prausnitz MR (2018) Ocular drug delivery targeted by iontophoresis in the suprachoroidal space using a microneedle. J Control Release 277:14–22. https://doi.org/10.1016/j.jconrel.2018.03.001
Kim M, An J, Kim KS, Choi M, Humar M, Kwok SJ, Dai T, Yun SH (2016) Optical lens-microneedle array for percutaneous light delivery. Biomed Opt Express 7(10):4220–4227. https://doi.org/10.1364/BOE.7.004220
Baek SH, Shin JH, Kim YC (2017) Drug-coated microneedles for rapid and painless local anesthesia. Biomed Microdevices 19(1):2. https://doi.org/10.1007/s10544-016-0144-1
Tariot P, Salloway S, Yardley J, Mackell J, Moline M (2012) Long-term safety and tolerability of donepezil 23 mg in patients with moderate to severe Alzheimer’s disease. BMC Res Notes 5:283. https://doi.org/10.1186/1756-0500-5-283
Kim JY, Han MR, Kim YH, Shin SW, Nam SY, Park JH (2016) Tip-loaded dissolving microneedles for transdermal delivery of donepezil hydrochloride for treatment of Alzheimer’s disease. Eur J Pharm Biopharm 105:148–155. https://doi.org/10.1016/j.ejpb.2016.06.006
Tas C, Joyce JC, Nguyen HX, Eangoor P, Knaack JS, Banga AK, Prausnitz MR (2017) Dihydroergotamine mesylate-loaded dissolving microneedle patch made of polyvinylpyrrolidone for management of acute migraine therapy. J Control Release 268:159–165. https://doi.org/10.1016/j.jconrel.2017.10.021
Du G, He P, Zhao J, He C, Jiang M, Zhang Z, Zhang Z, Sun X (2021) Polymeric microneedle-mediated transdermal delivery of melittin for rheumatoid arthritis treatment. J Control Release 336:537–548. https://doi.org/10.1016/j.jconrel.2021.07.005
Noor AH, Ghareeb MM (2021) Transdermal dissolvable microneedle-mediated delivery of controlled release ondansetron hydrogen chloride nanoparticles. Int J Drug Deliv Technol 11(3):858–863
Bhadale RS, Londhe VY (2022) Inclusion complexed iloperidone loaded dissolving microneedles: characterization, in-vitro study, and dermatopharmacokinetics. J Drug Deliv Sci Technol 68:103063. https://doi.org/10.1016/j.jddst.2021.103063
He J, Zhang Z, Zheng X, Li L, Qi J, Wu W, Lu Y (2021) Design and evaluation of dissolving microneedles for enhanced dermal delivery of propranolol hydrochloride. Pharmaceutics 13(4):579. https://doi.org/10.3390/pharmaceutics13040579
Sivaraman A, Banga AK (2017) Novel in situ forming hydrogel microneedles for transdermal drug delivery. Drug Deliv Transl Res 7(1):16–26. https://doi.org/10.1007/s13346-016-0328-5
Himawan A, Vora LK, Permana AD, Sudir S, Nurdin AR, Nislawati R, Hasyim R, Scott CJ, Donnelly RF (2023) Where microneedle meets biomarkers: futuristic application for diagnosing and monitoring localized external organ diseases. Adv Healthc Mater 12(5):e2202066. https://doi.org/10.1002/adhm.202202066
Laszlo E, De Crescenzo G, Nieto-Argüello A, Banquy X, Brambilla D (2021) Superswelling microneedle arrays for dermal interstitial fluid proteomics. Adv Funct Mater 31:2106061. https://doi.org/10.1002/adfm.202106061
González-Vázquez P, Larrañeta E, McCrudden MTC, Jarrahian C, Rein-Weston A, Quintanar-Solares M, Zehrung D, McCarthy H, Courtenay AJ, Donnelly RF (2017) Transdermal delivery of gentamicin using dissolving microneedle arrays for potential treatment of neonatal sepsis. J Control Release 265:30–40. https://doi.org/10.1016/j.jconrel.2017.07.032
Zhang X, Chen G, Bian F, Cai L, Zhao Y (2019) Encoded microneedle arrays for detection of skin interstitial fluid biomarkers. Adv Mater 31(37):1902825. https://doi.org/10.1002/adma.201902825
Wang Z, Luan J, Seth A, Liu L, You M, Gupta P, Rathi P, Wang Y, Cao S, Jiang Q, Zhang X, Gupta R, Zhou Q, Morrissey JJ, Scheller EL, Rudra JS, Singamaneni S (2021) Microneedle patch for the ultrasensitive quantification of protein biomarkers in interstitial fluid. Nat Biomed Eng 5:64–76. https://doi.org/10.1038/s41551-020-00672-y
Mandal A, Boopathy AV, Lam LKW, Moynihan KD, Welch ME, Bennett NR, Turvey ME, Thai N, Van JH, Love JC, Hammond PT, Irvine DJ (2018) Cell and fluid sampling microneedle patches for monitoring skin-resident immunity. Sci Transl Med 10(467):eaar2227. https://doi.org/10.1126/scitranslmed.aar2227
Mohan AMV, Windmiller JR, Mishra RK, Wang J (2017) Continuous minimally-invasive alcohol monitoring using microneedle sensor arrays. Biosens Bioelectron 91:574–579. https://doi.org/10.1016/j.bios.2017.01.016
Ranamukhaarachchi SA, Padeste C, Dübner M, Häfeli UO, Stoeber B, Cadarso VJ (2016) Integrated hollow microneedle-optofluidic biosensor for therapeutic drug monitoring in sub-nanoliter volumes. Sci Rep 6:29075. https://doi.org/10.1038/srep29075
Yang B, Fang X, Kong J (2020) Engineered microneedles for interstitial fluid cell-free DNA capture and sensing using iontophoretic dual-extraction wearable patch. Adv Funct Mater 30:2000591. https://doi.org/10.1002/adfm.202000591
Zheng M, Wang Z, Chang H, Wang L, Chew SWT, Lio DCS, Cui M, Liu L, Tee BCK, Xu C (2020) Osmosis-powered hydrogel microneedles for microliters of skin interstitial fluid extraction within minutes. Adv Healthc Mater 9(10):1901683. https://doi.org/10.1002/adhm.201901683
Prausnitz MR (2004) Microneedles for transdermal drug delivery. Adv Drug Deliv Rev 56(5):581–587. https://doi.org/10.1016/j.addr.2003.10.023
Bhatnagar S, Dave K, Venuganti VVK (2017) Microneedles in the clinic. J Control Release 260:164–182. https://doi.org/10.1016/j.jconrel.2017.05.029
Saha I, Rai VK (2021) Hyaluronic acid-based microneedle array: recent applications in drug delivery and cosmetology. Carbohydr Polym 267:118168. https://doi.org/10.1016/j.carbpol.2021.118168
Serrano-Castañeda P, Escobar-Chavez JJ, Rodriguez-cruz IM, Melgoza LM, Martinez-Hernandez J (2018) Microneedles as enhancer of drug absorption through the skin and applications in medicine and cosmetology. J Pharm Pharm Sci 21:73–93. https://doi.org/10.18433/jpps29610
Huang Y, Yu H, Wang L, Shen D, Ni Z, Ren S, Lu Y, Chen X, Yang J, Hong Y (2022) Research progress on cosmetic microneedle systems: preparation, property and application. Eur Polym J 163:110942. https://doi.org/10.1016/j.eurpolymj.2021.110942
Iriarte C, Awosika O, Rengifo-Pardo M, Ehrlich A (2017) Review of applications of microneedling in dermatology. Clin Cosmet Investig Dermatol 10:289–298. https://doi.org/10.2147/CCID.S142450
Prausnitz MR (2017) Engineering microneedle patches for vaccination and drug delivery to skin. Annu Rev Chem Biomol Eng 8(1):177–200. https://doi.org/10.1146/annurev-chembioeng-060816-101514
Sharma S, Hatware K, Bhadane P, Sindhikar S, Mishra DK (2019) Recent advances in microneedle composites for biomedical applications: advanced drug delivery technologies. Mater Sci Eng C 103:109717. https://doi.org/10.1016/j.msec.2019.05.002
Park YH, Ha SK, Choi I, Kim KS, Park J, Choi N, Kim B, Sung JH (2016) Fabrication of degradable carboxymethyl cellulose (CMC) microneedle with laser writing and replica molding process for enhancement of transdermal drug delivery. Biotechnol Bioproc Eng 21(1):110–118. https://doi.org/10.1007/s12257-015-0634-7
Kumar A, Naguib YW, Shi YC, Cui Z (2016) A method to improve the efficacy of topical eflornithine hydrochloride cream. Drug Deliv 23(5):1495–1501. https://doi.org/10.3109/10717544.2014.951746
Pall A, Pall S (2021) An innovative approach of treating acne scars using bipolar rotational stamping and monopolar criss-cross technique with insulated microneedling radiofrequency in Asians. J Cutan Aesthet Surg 14(2):191–202. https://doi.org/10.4103/JCAS.JCAS_89_19
El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H (2015) Microneedling therapy for atrophic acne scars: an objective evaluation. J Clin Aesthet Dermatol 8(7):36–42
Aust MC, Knobloch K, Reimers K, Redeker J, Ipaktchi R, Altintas MA, Gohritz A, Schwaiger N, Vogt PM (2010) Percutaneous collagen induction therapy: an alternative treatment for burn scars. Burns 36(6):836–843. https://doi.org/10.1016/j.burns.2009.11.014
Yalcintas EP, Ackerman DS, Korkmaz E, Telmer CA, Jarvik JW, Campbell PG, Bruchez MP, Ozdoganlar OB (2020) Analysis of in vitro cytotoxicity of carbohydrate-based materials used for dissolvable microneedle arrays. Pharm Res 37(3):33. https://doi.org/10.1007/s11095-019-2748-7
US Food and Drug Administration (2021) Dermal Fillers (Soft Tissue Fillers). Available on https://www.fda.gov/medical-devices/aesthetic-cosmetic-devices/dermal-fillers-soft-tissue-fillers. Accessed on 15 Apr 2023
Liu S, Jin MN, Quan YS, Kamiyama F, Kusamori K, Katsumi H, Sakane T, Yamamoto A (2014) Transdermal delivery of relatively high molecular weight drugs using novel self-dissolving microneedle arrays fabricated from hyaluronic acid and their characteristics and safety after application to the skin. Eur J Pharm Biopharm 86(2):267–276. https://doi.org/10.1016/j.ejpb.2013.10.001
Zhu J, Dong L, Du H, Mao J, Xie Y, Wang H, Lan J, Lou Y, Fu Y, Wen J, Jiang B, Li Y, Zhu J, Tao J (2019) 5-aminolevulinic acid-loaded hyaluronic acid dissolving microneedles for effective photodynamic therapy of superficial tumors with enhanced long-term stability. Adv Healthcare Mater 8:1900896. https://doi.org/10.1002/adhm.201900896
Xu Q, Li X, Zhang P, Wang Y (2020) Rapidly dissolving microneedle patch for synergistic gene and photothermal therapy of subcutaneous tumor. J Mater Chem B 8:4331–4339. https://doi.org/10.1039/D0TB00105H
Moreira AF, Rodrigues CF, Jacinto TA, Miguel SP, Costa EC, Correia IJ (2020) Poly(vinyl alcohol)/chitosan layer-by-layer microneedles for cancer chemo-photothermal therapy. Int J Pharm 576:118907. https://doi.org/10.1016/j.ijpharm.2019.118907
Falo L, Erdos G, Ozdoganlar B (2016) Microneedle arrays for cancer therapy applications. WO/2016/073905, 15 April, 2023
Chun Y, Rong Z (2016) Semiconductor microneedle assembly based on gene therapy, manufacturing method and manufacturing mold. CN106426729A, 15 April, 2023
Fonseca DFS, Vilela C, Pinto RJB, Bastos V, Oliveira H, Catarino J, Faísca P, Rosado C, Silvestre AJD, Freire CSR (2021) Bacterial nanocellulose-hyaluronic acid microneedle patches for skin applications: in vitro and in vivo evaluation. Mater Sci Eng C Mater Biol Appl 118:111350. https://doi.org/10.1016/j.msec.2020.111350
Demir YK, Akan Z, Kerimoglu O (2013) Sodium alginate microneedle arrays mediate the transdermal delivery of bovine serum albumin. PLoS ONE 8:e63819. https://doi.org/10.1371/journal.pone.0063819
Zhang Y, Jiang G, Yu W, Liu D, Xu B (2018) Microneedles fabricated from alginate and maltose for transdermal delivery of insulin on diabetic rats. Mater Sci Eng C 85:18–26. https://doi.org/10.1016/j.msec.2017.12.006
Choi HJ, Song JM, Bondy BJ, Compans RW, Kang SM, Prausnitz MR (2015) Effect of osmotic pressure on the stability of whole inactivated influenza vaccine for coating on microneedles. PLoS ONE 10:e0134431. https://doi.org/10.1371/journal.pone.0134431
Kim YC, Quan FS, Compans RW, Kang SM, Prausnitz MR (2010) Formulation of microneedles coated with influenza virus-like particle vaccine. AAPS PharmSciTech 11:1193–2010. https://doi.org/10.1208/s12249-010-9471-3
Fonseca DFS, Costa PC, Almeida IF, Dias-Pereira P, Correia-Sá I, Bastos V, Oliveira H, Duarte-Araújo M, Morato M, Vilela C, Silvestre AJD, Freire CSR (2020) Pullulan microneedle patches for the efficient transdermal administration of insulin envisioning diabetes treatment. Carbohydr Polym 241:116314. https://doi.org/10.1016/j.carbpol.2020.116314
Salwa NTC, Jitta SR, Marques SM, Vaz VM, Kumar L (2021) Polymeric microneedles for transdermal delivery of nanoparticles: frontiers of formulation, sterility and stability aspects. J Drug Deliv Sci Technol 65:102711. https://doi.org/10.1016/j.jddst.2021.102711
McCrudden MT, Alkilani AZ, Courtenay AJ, McCrudden CM, McCloskey B, Walker C, Alshraiedeh N, Lutton RE, Gilmore BF, Woolfson AD, Donnelly RF (2015) Considerations in the sterile manufacture of polymeric microneedle arrays. Drug Deliv Transl Res 5(1):3–14. https://doi.org/10.1007/s13346-014-0211-1
Tipnis NP, Burgess DJ (2018) Sterilization of implantable polymer-based medical devices: a review. Int J Pharm 544(2):455–460. https://doi.org/10.1016/j.ijpharm.2017.12.003
International Conference on Harmonisation Of technical requirements for registration of pharmaceuticals for human use ICH harmonised tripartite guideline stability testing of new drug substances and products Q1A(R2) (2003)
Arya JM, Dewitt K, Scott-Garrard M, Chiang YW, Prausnitz MR (2016) Rabies vaccination in dogs using a dissolving microneedle patch. J Control Release 239:19–26. https://doi.org/10.1016/j.jconrel.2016.08.012
Choi HJ, Yoo DG, Bondy BJ, Quan FS, Compans RW, Kang SM, Prausnitz MR (2012) Stability of influenza vaccine coated onto microneedles. Biomaterials 33(14):3756–3769. https://doi.org/10.1016/j.biomaterials.2012.01.054
Bhadale RS, Londhe VY (2021) A systematic review of carbohydrate-based microneedles: current status and future prospects. J Mater Sci Mater Med 32:89. https://doi.org/10.1007/s10856-021-06559-x
US Food and Drug Administration (2020) Regulatory considerations for microneedling products guidance for industry and food and drug administration staff. Available on https://www.fda.gov/regulatory-information/search-fda-guidance-documents/regulatory-considerations-microneedling-products Accessed 5 Mar 2023
Pawar K (2017) Microneedles-based devices: regulatory insights. J Pharm Drug Deliv Res 6:1. https://doi.org/10.4172/2325-9604.1000e102
Amarnani R, Shende P (2021) Microneedles in diagnostic, treatment and theranostics: an advancement in minimally-invasive delivery system. Biomed Microdevices 24(1):4. https://doi.org/10.1007/s10544-021-00604-w
Vassilieva EV, Kalluri H, McAllister D, Taherbhai MT, Esser ES, Pewin WP, Pulit-Penaloza JA, Prausnitz MR, Compans RW, Skountzou I (2015) Improved immunogenicity of individual influenza vaccine components delivered with a novel dissolving microneedle patch stable at room temperature. Drug Deliv Transl Res 5(4):360–371. https://doi.org/10.1007/s13346-015-0228-0
Mistilis MJ, Joyce JC, Esser ES, Skountzou I, Compans RW, Bommarius AS, Prausnitz MR (2017) Long-term stability of influenza vaccine in a dissolving microneedle patch. Drug Deliv Transl Res 7(2):195–205. https://doi.org/10.1007/s13346-016-0282-2
Donadei A, Kraan H, Ophorst O, Flynn O, O’Mahony C, Soema PC, Moore AC (2019) Skin delivery of trivalent Sabin inactivated poliovirus vaccine using dissolvable microneedle patches induces neutralizing antibodies. J Control Release 311–312:96–103. https://doi.org/10.1016/j.jconrel.2019.08.039
Choi IJ, Cha HR, Hwang SJ, Baek SK, Lee JM, Choi SO (2021) Live vaccinia virus-coated microneedle array patches for smallpox vaccination and stockpiling. Pharmaceutics 13(2):1–12. https://doi.org/10.3390/pharmaceutics13020209
van der Straeten A, Sarmadi M, Daristotle JL, Kanelli M, Tostanoski LH, Collins J, Pardeshi A, Han J, Varshney D, Eshaghi B, Garcia J, Forster TA, Li G, Menon N, Pyon SL, Zhang L, Jacob-Dolan C, Powers OC, Hall K, Alsaiari SK, Wolf M, Tibbitt MW, Farra R, Barouch DH, Langer R, Jaklenec A (2023) A microneedle vaccine printer for thermostable COVID-19 mRNA vaccines. Nat Biotechnol. https://doi.org/10.1038/s41587-023-01774-z
Bhatnagar S, Bankar NG, Kulkarni MV, Venuganti VVK (2019) Dissolvable microneedle patch containing doxorubicin and docetaxel is effective in 4T1 xenografted breast cancer mouse model. Int J Pharm 556:263–275. https://doi.org/10.1016/j.ijpharm.2018.12.022
Zong Q, Guo R, Dong N, Ling G, Zhang P (2022) Design and development of insulin microneedles for diabetes treatment. Drug Deliv Transl Res 12:973–980. https://doi.org/10.1007/s13346-021-00981-y
Zhou X, Li B, Guo M, Peng W, Wang D, Guo Q, Wang S, Ming D, Zheng B (2022) Microneedle patch based on molecular motor as a spatio-temporal controllable dosing strategy of L-DOPA for Parkinson’s disease. Chem Eng J 427:131555. https://doi.org/10.1016/j.cej.2021.131555
Gupta P, Yadav KS (2019) Applications of microneedles in delivering drugs for various ocular diseases. Life Sci 237:116907. https://doi.org/10.1016/j.lfs.2019.116907
Thakur SRR, Tekko I, McAvoy K, McMillan H, Jones D, Donnelly RF (2017) Minimally invasive microneedles for ocular drug delivery. Expert Opin Drug Deliv 14(4):525–537. https://doi.org/10.1080/17425247.2016.1218460
Datta D, Roy G, Garg P, Venuganti VVK (2022) Ocular delivery of cyclosporine A using dissolvable microneedle contact lens. J Drug Deliv Sci Technol 70:103211. https://doi.org/10.1016/j.jddst.2022.103211
Xue P, Zhang L, Xu Z, Yan J, Gu Z, Kang Y (2018) Blood sampling using microneedles as a minimally invasive platform for biomedical diagnostics. Appl Mater Today 13:144–157. https://doi.org/10.1016/j.apmt.2018.08.013
Singh V, Kesharwani P (2021) Recent advances in microneedles-based drug delivery device in the diagnosis and treatment of cancer. J Control Release 338:394–409. https://doi.org/10.1016/j.jconrel.2021.08.054
Chen Y, Alba M, Tieu T, Tong Z, Minhas RS, Rudd D, Voelcker NH, Cifuentes-Rius A, Elnathan R (2021) Engineering micro–nanomaterials for biomedical translation. Adv Nanobiomed Res 1(9):2100002. https://doi.org/10.1002/anbr.202100002
Halder J, Gupta S, Kumari R, Gupta GD, Rai VK (2021) Microneedle array: applications, recent advances, and clinical pertinence in transdermal drug delivery. J Pharm Innov 16:558–565. https://doi.org/10.1007/s12247-020-09460-2
Future market insights (2023) Microneedle drug delivery systems market (2023 to 2033), Available on https://www.futuremarketinsights.com/reports/microneedle-drug-delivery-systems-market Accessed 5 Mar 2023
Bariya SH, Gohel MC, Mehta TA, Sharma OP (2011) Microneedles: an emerging transdermal drug delivery system. J Pharm Pharmacol 64(1):11–29. https://doi.org/10.1111/j.2042-7158.2011.01369.x
Cleveland Clinic (2022) Microneedling: overview. Available on https://my.clevelandclinic.org/health/treatments/23113-microneedling. Accessed 13 May 2023
Zhu DD, Zhang XP, Zhang BL, Hao YY, Guo XD (2020) Safety assessment of microneedle technology for transdermal drug delivery: a review. Adv Ther 3(8):2000033. https://doi.org/10.1002/adtp.202000033
Swathi HP, Anusha MV, Paul GJ, Narasimha MS, Kanni P, Varshney L, Suresh S, Shivakumar HN (2020) Effect of gamma sterilization on the properties of microneedle array transdermal patch system. Drug Dev Ind Pharm 46(4):606–620. https://doi.org/10.1080/03639045.2020.1742144
Miller P, Moorman M, Manginell R, Ashlee C, Brener I, Wheeler D, Narayan R, Polsky R (2016) Towards an integrated microneedle total analysis chip for protein detection. Electroanalysis 28(6):1305–1310. https://doi.org/10.1002/elan.201600063
Yadav S, Dogra S (2016) A cutaneous reaction to microneedling for postacne scarring caused by nickel hypersensitivity. Aesthet Surg J 36(4):NP168-170. https://doi.org/10.1093/asj/sjv229
Gowda A, Healey B, Ezaldein H, Merati M (2021) A systematic review examining the potential adverse effects of microneedling. J Clin Aesthet Dermatol 14(1):45–54
Visan AI, Popescu-Pelin G, Socol G (2021) Degradation behaviour of polymers used as coating materials for drug delivery—a basic review. Polymers 13(8):1272. https://doi.org/10.3390/polym13081272
Bal SM, Caussin J, Pavel S, Bouwstra JA (2008) In vivo assessment of safety of microneedle arrays in human skin. Eur J Pharm Sci 35(3):193–202. https://doi.org/10.1016/j.ejps.2008.06.016
So JW, Park HH, Lee SS, Kim DC, Shin SC, Cho CW (2009) Effect of microneedle on the pharmacokinetics of ketoprofen from its transdermal formulations. Drug Deliv 16(1):52–56. https://doi.org/10.1080/10717540802518082
Acknowledgements
The authors would like to thank the Department of Biotechnology (DBT), Ministry of Science & Technology, Government of India, and The World Academy of Sciences (TWAS), Italy, for providing postdoctoral fellowship to Chukwuebuka Emmanuel Umeyor to the Institute of Chemical Technology, Mumbai.
Funding
This work was not funded or supported by any persons or group.
Author information
Authors and Affiliations
Contributions
CEU conceptualized, designed, drafted, reviewed and edited the manuscript; VS, AP, PK, SJ, NT, AA, AN, GB, AA, VR, SB, AC collated literature data, interpreted the information, and drafted the manuscript; VBP coordinated, provided access to databases and supervised the work; all authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No animal or human tissue was used in this work, and ethics approval and consent were not applicable.
Consent for publication
All authors gave their full consent for publication of this work.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Umeyor, C.E., Shelke, V., Pol, A. et al. Biomimetic microneedles: exploring the recent advances on a microfabricated system for precision delivery of drugs, peptides, and proteins. Futur J Pharm Sci 9, 103 (2023). https://doi.org/10.1186/s43094-023-00553-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-023-00553-6