
Abstract
Background
Laparoscopic surgery (LS) has been increasingly applied in perihilar cholangiocarcinoma (pCCA). In this study, we intend to compare the short-term outcomes of LS versus open operation (OP) for pCCA in a multicentric practice in China.
Methods
This real-world analysis included 645 pCCA patients receiving LS and OP at 11 participating centers in China between January 2013 and January 2019. A comparative analysis was performed before and after propensity score matching (PSM) in LS and OP groups, and within Bismuth subgroups. Univariate and multivariate models were performed to identify significant prognostic factors of adverse surgical outcomes and postoperative length of stay (LOS).
Results
Among 645 pCCAs, 256 received LS and 389 received OP. Reduced hepaticojejunostomy (30.89% vs 51.40%, P = 0.006), biliary plasty requirement (19.51% vs 40.16%, P = 0.001), shorter LOS (mean 14.32 vs 17.95 d, P < 0.001), and lower severe complication (CD ≥ III) (12.11% vs. 22.88%, P = 0.006) were observed in the LS group compared with the OP group. Major postoperative complications such as hemorrhage, biliary fistula, abdominal abscess, and hepatic insufficiency were similar between LS and OP (P > 0.05 for all). After PSM, the short-term outcomes of two surgical methods were similar, except for shorter LOS in LS compared with OP (mean 15.19 vs 18.48 d, P = 0.0007). A series subgroup analysis demonstrated that LS was safe and had advantages in shorting LOS.
Conclusion
Although the complex surgical procedures, LS generally seems to be safe and feasible for experienced surgeons.
Trial registration
NCT05402618 (date of first registration: 02/06/2022).
Similar content being viewed by others


Background
Perihilar cholangiocarcinoma (pCCA) is a devastating disease with an annual incidence of one to two cases per 100,000 individuals [1]. Radical surgery is the most important potentially curative treatment for pCCA. Meanwhile, radical surgery is also undoubtedly one of the most difficult and sophisticated skills for surgeons [2]. Recent advances in surgical techniques and perioperative management have offered increased resectability and improvement in surgical outcome; however, post-operative morbidities and mortality remain a problem [3].
Laparoscopic surgery (LS) has been increasingly used in all types of hepato-pancreato-biliary resections including pancreatectomy and hepatectomy [4,5,6]. In liver surgery, LS presented improved postoperative outcomes compared with open approach [7]. Recently, there has been increasing enthusiasm for performing laparoscopic pancreaticoduodenectomy (PD), which has been demonstrated to be feasible and safe, with outcomes that are comparable to open PD [8]. The surgical procedures for pCCA entail perihilar biliary tract resection with extended hepatectomy, which requires concomitant vascular resection and reconstruction or even combined hepatopancreatoduodenectomy. A major challenge is the complex anatomical location of the lesion, which is in close proximity to the portal vein (PV), hepatic arteries, and liver parenchyma [9, 10]. Thus, there are few reports on laparoscopic resection for pCCA due to the complexity of the surgical procedure. Till now, LS resection for pCCA was considered to be still in its infancy [11]. However, the available evidence on LS for pCCA is limited; LS cannot be considered as a dogmatic contraindication to pCCA. It thus is imperative to undertake large-scale multicenter analyses to investigate in the technical feasibility and safety of LS for pCCA [12].
Herein, we compared perioperative outcomes of LS and open operation (OP) in 654 pCCA patients in China before and after a propensity score-based analysis. To our knowledge, this is the largest series of LS compared with OP for pCCA to be investigated to date.
Methods
Patients and data collection
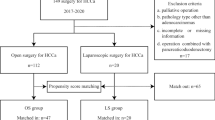
A retrospective review of institutional databases from 11 hospitals in China identified 645 pCCA patients who underwent radical surgery between January 2013 and January 2019, including 256 patients underwent LS and 389 underwent OP. An intention-to-treat design was used, such that cases converted to OP were included in the LS cohort. All cases were histologically confirmed pCCA. The exclusion criteria were as follows: (1) patients with peritoneal seeding or metastasis to the liver, para-aortic lymph nodes, or distant sites; (2) patients with non-adenocarcinoma histology; and (3) patients with incomplete clinical data. The detailed study flow was shown in Fig. 1 and Supplementary Table 1. Ethical approval was given for the study by the ethics committee/Institutional Review Board of Ethics Committee of Tongji Hospital (approval number: TJ-IRB20220531). The need for informed consent was waived by the ethics committee/Institutional Review Board of Ethics Committee of Tongji Hospital (approval number: TJ-IRB20220531) because of the retrospective nature of the study. This research was also registered at ClinicalTrials.gov (identifier: NCT05402618; date of first registration: 02/06/2022). All the work followed the ‘Sex and Gender Equity in Research-SAGER-guidelines’ and has been reported in line with the STROCSS criteria [13].

Study flow
Operative technique
LS was defined as total laparoscopic surgery (TLS), where both resection and digestive reconstruction were completed laparoscopically. The hepatectomy with en bloc resection of the caudate lobe and extrahepatic bile duct and regional lymph node dissection was applied in both laparoscopic and open surgery. Extended resections (left/right trisectionectomy), arterial vascular encasement, vascular resection/reconstruction, biliary stent in place were needed for patients based on Bismuth stage.
Variables and definitions
Data collection included demographic, clinical and oncologic data. Patients were staged according to the National Comprehensive Cancer Network (NCCN) Guideline Version 2.2019 Edition tumor node metastasis (TNM) clinical staging system for pCCA [14]. The local extension of the disease was expressed mainly according to the Bismuth–Corlette classification [15]. Operation time was defined as the time from skin incision or trocar placement to complete skin closure. Intraoperative blood loss (IBL) was carefully recorded by the anesthetist using a vacuum system. Vessel reconstruction was defined as any repair or replacement of major vessels during surgery. Main short-term outcome in this study was postoperative length of stay (LOS), which was defined as the time from surgery to normal discharge. Patients who stayed longer than 30 days or less than three days will be considered as censored. Other short-term evaluations including morbidity and mortality, defined as any complication or death, respectively, which occurred during hospitalization or within 90 days of discharge. Hospital reoperation within 30 days was recorded and postoperative morbidity was evaluated according to the Clavien-Dindo (CD) classification system [16]. Major postoperative complications such as bile leakage, postoperative hemorrhage, and liver failure were classified as previously reported [17,18,19]. Surgical failure was defined as severe complication (CD ≥ III), or received reoperation during hospitalization, or dead within 30 days after surgery.
Statistical analysis
Patients that underwent LS were matched in a 1:1 ratio to patients that underwent OP based on the propensity score model [20], with age, BMI, sex, ASA physical status, CA 19–9, preoperative Tbil, AST, ALT, albumin, Bismuth-Corlett type, hepatectomy, operative time, digestive reconstruction, IBL, vascular resection and reconstruction, positive margin, number of lymph nodes, and TMN stage being selected as the covariates. The nearest neighbor matching without replacement was performed with caliper width setting at 0.2.
Continuous data are presented as means with standard deviations (SDs) or medians with interquartile ranges (IQRs) and compared with independent-samples t-test or Mann–Whitney U test. Categorical data are presented as numbers and percentages and were compared using the Chi-square or Fisher’s exact test, as appropriate. Logistic regression analysis was used to access the risk factors of adverse postoperative complications (CD stage ≥ III). Cox regression model were used to assess the risk factors associated with postoperative LOS, with the proportional hazard assumption being tested by weighted residual score method. Furthermore, considering the postoperative complication would prolong the LOS during hospitalization, the Fine-Gray model were used to explore the prognostic factors of length of stay, with the adverse postoperative complications and death within 30 days being the competing risk events. Continuous variables will be converted into two or multiple category dummy variables according to the normal range during the regression analysis. All the statistical procedures were conducted using SAS software version 9.40 (SAS Institute, Inc., Cary, NC). Two-sided hypothesis testing with a predetermined level of P < 0.05 was considered statistically significant.
Results
Participants and baseline characteristics
Baseline characteristics of demographics and preoperative comorbidity of the included 645 resections of histologically confirmed pCCA are listed in Table 1. In raw cohort, most baseline characteristics were comparable in LS and OP group, except for more female patients (49.61% vs. 40.36%; P = 0.021), better hepatic function index (lower TBIL, AST, and ALT levels), and lower TNM stage being observed in LS group than in OP group. To overcome the bias from retrospective study, the propensity score matched analyses was conducted, in which 141 pCCA patients undergoing LS were matched with 141 patients undergoing OP. All baseline characteristics were balanced after PSM.
Perioperative outcomes
Before PSM, 19 patients (7.42%) converted to laparotomy. The mean operative time of the LS group was similar with OP group (353.4 vs. 342.1 min, P = 0.176). More patients received hepatectomy in LS compared with OP (63.67% vs 55.53%, P = 0.013), especially more left hemihepatectomy in LS (47.66% vs 36.76%). Fewer hepaticojejunostomy (39.06% vs 61.44%, P < 0.0001), biliary plasty (28.91% vs 48.84%, P < 0.001), vascular resection (8.59% vs 23.39%, P < 0.0001) and fewer hepaticojejunostomy (43.48% vs 65.48%, P < 0.0001) were performed in the LS group compared with OP group. R0 rate, IBL, transfusion rate and volume, as well as caudate lobectomy were similar between groups (Table 2).
There were no significant differences with regards to the common postoperative complications between the two groups, except lower heart failure (0.78% vs. 3.60%, P = 0.0244) and severe complications in LS group (12.11% vs. 22.88%, P = 0.0006). Patients in LS group required shorter postoperative drainage tube keep time (PDTK) (median [IQR], 8.00[5.00 ~ 11.00] vs. 9.00[6.00 ~ 14.00], P < 0.0001), and postoperative LOS (median [IQR], 13.00[10.00 ~ 18.00] vs. 15.00[12.00 ~ 23.00], P < 0.0001) than OP patients. There was no significant difference on reoperation rate or death within 30 or 90 days. The similar incidence of some most common postoperative complications between two surgical groups were still comparable in matched cohort (Table 3).
Postoperative outcomes according to Bismuth type
In the present study, 328 patients of pCCA had a low Bismuth type (Bismuth I/II) and 317 had a high Bismuth type (Bismuth III/V), with significantly different surgical characteristics and postoperative short-term outcomes. The median LOS was much shorter in the low Bismuth type (15 day; 95%CI, 14 ~ 16) than in the high Bismuth type (18 day; 95%CI, 17 ~ 20, P < 0.0001). Furthermore, shorter LOS and PDTK, as well as less transfusion during surgery were observed in patients who underwent LS compared with those who underwent OP among patients with Bismuth types I-II, with other postoperative complications being comparable between the two groups. Among patients with Bismuth types III-V, those who underwent LS showed comparable or better short-term outcomes than the OP group, such as less total postoperative complications (39(32.23)86(43.88), P = 0.0393), shorter length of stay (median days, 14 vs. 17 days), and lower rates of severe complications (10.74% vs. 26.02%), demonstrating guaranteed safety of laparoscopic resection for high Bismuth types of PHC. Besides, a significantly less vascular resection and biliary plasty were observed in the LS group (Supplementary table 2–7).
Subgroup analysis for surgical failure and LOS
Subgroup analysis about the surgical failure and LOS was performed according to age, gender, BMI level, ASA score, tumor size, hepatectomy, vascular resection, and Bismuth stage. After PSM, the rate of surgical failure was similar in LS compared to OP group in total (4.30% vs 7.20%, P = 0.131) and in all subgroups (Fig. 2). However, the subgroup analysis about LOS showed that patients would benefit from LS for rapid recovery, regardless of age, tumor size and severe postoperative complications. Other patients, such as those who were underweight, had ASA score of I or III, or underwent vascular resection, had comparable LOS in LS and OP group (Fig. 3).

Forest plot of subgroup analysis regarding to surgical failure. Surgical failure was defined as severe complication (CD ≥ III), or received reoperation during hospitalization, or dead within 30 days after surgery.

Forest plot of subgroup analysis regarding to length of stay
Risk analysis of adverse surgical outcome and length of stay
The risk analysis showed that higher ASA score, more intraoperative blood loss, and more vascular reconstruction were identified independent risk factors of postoperative complications among both matched and unmatched samples (adjusted odds ratio (AOR) > 1, P < 0.05 for all) (Table 4). Besides, we found the OP, higher level of CA19-9, as well as some common postoperative complications, and reoperation were associated with longer LOS after adjusting other covariates in matched cohort (Table 5).
Furthermore, the Fine Gray model were conducted to further investigate the association between surgical methods and the LOS, with postoperative complications, received reoperation during hospitalization, or dead within 30 days after surgery being identified as competing events when analyzing the LOS. After adjusting competing risks, the open surgery was found to be an independent risk factor of prolonged LOS in both unmatched and matched analysis (Supplemental Table 8).
Discussion
The short-term outcomes of this retrospective study showed that the LS was favored in LOS and function recovery details such as the duration of postoperative drainage tube keep than OP for pCCA patients. Moreover, the mortality rates, postoperative complication rates, and oncological outcomes were not significantly different between two surgical methods. This is the largest real-world pCCA data to date comparing LS and OP for pCCA. It showed that LS, although challenging, is feasible and safe for pCCA patients. We also performed the PSM to eliminate potential biases and found that the LS group was beneficial for postoperative functional recovery, with no differences in complications and death rate compared to the OP group. The multivariate analysis further confirmed that LS was safe for perioperative complications and could significantly shorten the postoperative LOS.
Although several cumulative evidence with meta-analysis have shown the applicability of LS in pCCA [21,22,23,24], the technique is still restricted to a minority of highly experienced surgeons and specialized institutions, and lack of large sample evidence from multicenter. LS has been used for all Bismuth-Corlette types, although it is predominantly used in patients with low stage tumors [25,26,27]. The Bismuth III-IV accounted for 47.26% in this study, and equal safety and better postoperative recover, reflected by shorter LOS and PDTK, were also found in the LS group compared to OP group in this sample. Furthermore, the feasibility of the laparoscopic approach is attested by a conversion rate (19/256 cases, 7.4% before PSM; and 11/141 cases, 7.8% after PSM), which was much lower than the generally reported surgeries for pCCA [28] and also lower for major hepatectomies [29, 30]. In fact, although the surgical management of pCCA involves most complex technical procedures, such as portal infiltration or arterial encasement, or disease infiltration along the bile ducts, the requirements of an urgent conversion are detected with relative low frequency. Since the surgical field can be easily accessible to operator’s views and thus, some operative procedures with a high degree of technical complexity were more manageable in laparoscopy.
To date, only retrospective studies with small sample size reported the perioperative outcomes of LS and OP regarding the pCCA. The efficacy and safety of LS for pCCA is largely controversial [11, 12, 31, 32]. The only comparative study conducted by Xu et al. reported the robotic resection compared unfavorably to traditional open resection in operative time. No significant difference was found in blood loss, mortality, or length of postoperative hospital stay. While the hospital expenditure was much higher in the robotic group, and the tumor recurrence-free survival was inferior in the robotic group [33]. A study summarized a series of laparoscopic procedures showed there was significantly lower blood loss, fewer intraoperative and postoperative blood transfusions, and shorter LOS in LS group. Both overall and lymphadenectomy-related morbidity were lower in the LS group [34]. In this study, there were no significant differences in operative time, IBL, postoperative complications, or death between the two groups, but shorter LOS in LS group. Besides, the surgical methods, no matter open or laparoscopic, were not associated with adverse postoperative complications in both matched and unmatched samples. Furthermore, the LS showed to be a protective factor of adverse postoperative complication than OP in the univariate analysis. These evidence demonstrated that LS is safe and feasible for pCCA patients.
The most important potential advantage of LS is the increased adoption of postoperative functional recovery pathways and shorten hospital stay [35]. The LS technique can not only allow functional recovery for simple operations, such as LC and herniorrhaphy, but also for complex surgeries, such as LPD, laparoscopic hepatectomy, or laparoscopic gastrectomy [36,37,38,39]. Our study observed a protective effect of LS in shortening the LOS with or without considering the postoperative complications being the competing risk events. Perioperative complications would potentially influence the short-term outcome evaluation with life-threatening events, and thus affect the assessment of net cumulative effect of LS in shortening the LOS. Neglecting the existence of these competing risk events will lead inaccurate calculations of the cumulative discharge rate when using the classic survival analysis methods [40, 41]. Until now, few studies considered using the Fine-Gray model to explore the postoperative benefits from LS. PSM was another statistical method to control bias in this study. It has been proposed as a method to overcome selection bias and increase the evidence level in observational and randomized studies [42, 43]. In this study, we demonstrated that fewer hepaticojejunostomy, less vascular resection, shorter LOS, and a trend towards fewer severe complication (CD stage ≥ III) in LS group compared to OP before and after PSM. The results indicated that LS could reliably shorten hospital stays and provide benefits regarding postoperative functional recovery in pCCA patients.
Furthermore, we found that high ASA score, more intraoperative blood loss and hepaticojejunostomy were consistent risk factors of adverse surgical outcome. Besides, more intraoperative blood loss was identified as a risk factor for prolonged LOS in both the common risk model and competing risk model. These results indicated that better preoperative condition and less intraoperative blood loss were associated with better short-term prognosis among pCCA patients. During surgical management of pCCA, most technical complexities are related to the management of portal infiltration, or arterial encasement, or disease infiltration along the bile ducts. Along with these conditions and related risks of vascular injury are generally more manageable in laparoscopy since the surgical field is easily accessible being close to operator’s view and bleedings can be stopped with the use of a temporary clamp if emergency situation occurred. Therefore, the LS would be better to manage intraoperative bleeding, potentially bringing benefits for short-term outcome as recently reported [28, 44]. The preoperative condition of the patient is the most concerned issue in the determination of surgery. Patient selection is a common phenomenon in clinical practice, and it is also a key challenge that still puzzled most surgical experts. In our study, we can find that the rate of vascular resection, postoperative biliary fistula, and liver hepatic insufficiency are very low, suggesting an obvious patient selection prior to surgical management. In daily practice, patients with pCCA will be asked to receive ICG test, liver function testing, and 3D imaging examination to help surgeons calculate the liver volume, assess the liver function, and present exact anatomy of the lesion before surgery. Some surgeons would be relatively conservative to perform radical surgery for pCCA when encountering complex resection and reconstruction, especially for laparoscopic surgery. Despite the difficulty, enthusiasm is growing among surgeons regarding laparoscopic radical perihilar cholangiocarcinoma surgery. The selection of suitable patients for laparoscopic radical perihilar cholangiocarcinoma to help surgeons navigate the learning curve will be the focus of our future research.
To our knowledge, this is the largest case series of pCCA comparing LS and OS techniques. However, some limitations must be noted. First, the retrospective nature of the study is at risk of selection biases and unexpected recall bias cannot be completely ruled out. Second, the multicentric nature of the study is at risk of different selection criteria applied in the participating Institutions. While, due to the complexity of the procedure, there is a paucity of laparoscopic resection available now and this large-sample analysis can provide several important information about the laparoscopic procedures of pCCA. Third, all laparoscopic resections performed by experienced hands were still in the early and exploratory stages and is performed only in select cases. In addition, the centers included in this study were all high-volume referral centers in China. The experience may be difficult to generalize to the surgeons with less intensive training. Nonetheless, given the ongoing debate regarding the complicated procedure, and the current shift toward value-based healthcare reimbursement models, our findings are relevant and timely.
Conclusions
In summary, this extensive, multi-center study demonstrated that LS does not seem to increase the intraoperative and postoperative risks of pCCA. This report thus serves as a foundation for national protocols aimed at safely implementation of LS in pCCA patients. Larger prospective cohort series and prospective randomized studies in multiple countries are warranted to further investigate this topic.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LS:
-
Laparoscopic surgery
- pCCA:
-
Perihilar cholangiocarcinoma
- OP:
-
Open operation
- PSM:
-
Propensity score matching
- LOS:
-
Length of stay portal vein
- PV:
-
Total laparoscopic surgery
- TLS:
-
Tumor node metastasis
- TNM:
-
National Comprehensive Cancer Network
- NCCN:
-
Laparoscopic pancreaticoduodenectomy
- PD:
-
Intraoperative blood loss
- IBL:
-
Clavien-Dindo
- CD:
-
Interquartile ranges
- IQR:
-
Standard deviations
- SD:
-
Body mass index
- BMI:
-
Total bilirubin
- Tbil:
-
A Lkaline Phosphatase
- ALP:
-
Aspartic acid aminotransferase
- AST:
-
Alanine aminotransferase
- ALT:
-
Acute Respiratory
- ARDS:
-
Distress Syndrome
- PDTK:
-
Postoperative drainage tube keep time
References
Groot Koerkamp B, Wiggers JK, Allen PJ, Busch OR, D’Angelica MI, DeMatteo RP, et al. American Joint Committee on Cancer staging for resected perihilar cholangiocarcinoma: a comparison of the 6th and 7th editions. HPB (Oxford). 2014;16(12):1074–82.
Kimura N, Young AL, Toyoki Y, Wyatt JI, Toogood GJ, Hidalgo E, et al. Radical operation for hilar cholangiocarcinoma in comparable Eastern and Western centers: Outcome analysis and prognostic factors. Surgery. 2017;162(3):500–14.
Tang Z, Yang Y, Zhao Z, Wei K, Meng W, Li X. The clinicopathological factors associated with prognosis of patients with resectable perihilar cholangiocarcinoma: A systematic review and meta-analysis. Medicine. 2018;97(34):e11999.
Wang Y, Ma K, Zhong A, Xiong Q, Chen J. Hepatopulmonary syndrome after radiofrequency ablation of recurrent intrahepatic cholangiocarcinoma: a case report. Onco Targets Ther. 2019;12:2431–8.
de Rooij T, van Hilst J, van Santvoort H, Boerma D, van den Boezem P, Daams F, et al. Minimally Invasive Versus Open Distal Pancreatectomy (LEOPARD): A Multicenter Patient-blinded Randomized Controlled Trial. Ann Surg. 2019;269(1):2–9.
Wang M, Peng B, Liu J, Yin X, Tan Z, Liu R, et al. Practice Patterns and Perioperative Outcomes of Laparoscopic Pancreaticoduodenectomy in China: A Retrospective Multicenter Analysis of 1029 Patients. Ann Surg. 2021;273(1):145–53.
Jin B, Chen MT, Fei YT, Du SD, Mao YL. Safety and efficacy for laparoscopic versus open hepatectomy: A meta-analysis. Surg Oncol. 2018;27(2):a26–34.
Nickel F, Haney CM, Kowalewski KF, Probst P, Limen EF, Kalkum E, et al. Laparoscopic Versus Open Pancreaticoduodenectomy: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Ann Surg. 2020;271(1):54–66.
Hosokawa I, Shimizu H, Yoshidome H, Ohtsuka M, Kato A, Yoshitomi H, et al. Surgical strategy for hilar cholangiocarcinoma of the left-side predominance: current role of left trisectionectomy. Ann Surg. 2014;259(6):1178–85.
Gumbs AA, Jarufe N, Gayet B. Minimally invasive approaches to extrapancreatic cholangiocarcinoma. Surg Endosc. 2013;27(2):406–14.
Franken LC, van der Poel MJ, Latenstein AEJ, Zwart MJ, Roos E, Busch OR, et al. Minimally invasive surgery for perihilar cholangiocarcinoma: a systematic review. J Robot Surg. 2019;13(6):717–27.
Hu HJ, Wu ZR, Jin YW, Ma WJ, Yang Q, Wang JK, et al. Minimally invasive surgery for hilar cholangiocarcinoma: state of art and future perspectives. ANZ J Surg. 2019;89(5):476–80.
Agha R, Abdall-Razak A, Crossley E, Dowlut N, Iosifidis C, Mathew G; the STROCSS Group. The STROCSS. Guideline: Strengthening the Reporting of Cohort Studies in Surgery. Int J Surg. 2019;2019(72):156–65.
Edge SBBD, Compton CC, Fritz AG, Greene FL, Trotti A. American Joint Committee on cancer. Cancer staging manual: Springer, New York; 2020.
Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar cholangiocarcinoma. Ann Surg. 1992;215(1):31–8.
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–96.
Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, et al. Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver Surgery. Surgery. 2011;149(5):680–8.
Rahbari NN, Garden OJ, Padbury R, Maddern G, Koch M, Hugh TJ, et al. Post-hepatectomy haemorrhage: a definition and grading by the International Study Group of Liver Surgery (ISGLS). HPB (Oxford). 2011;13(8):528–35.
Rahbari NN, Garden OJ, Padbury R, Brooke-Smith M, Crawford M, Adam R, et al. Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery. 2011;149(5):713–24.
Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Variable selection for propensity score models. Am J Epidemiol. 2006;163(12):1149–56.
Cipriani F, Ratti F, Fiorentini G, Reineke R, Aldrighetti L. Systematic review of perioperative and oncologic outcomes of minimally-invasive surgery for hilar cholangiocarcinoma. Updates Surg. 2021;73(2):359–77.
Rahnemai-Azar AA, Abbasi A, Tsilimigras DI, Weber SM, Pawlik TM. Current Advances in Minimally Invasive Surgical Management of Perihilar Cholangiocarcinoma. J Gastrointest Surg. 2020;24(9):2143–9.
Wang W, Fei Y, Liu J, Yu T, Tang J, Wei F. Laparoscopic surgery and robotic surgery for hilar cholangiocarcinoma: an updated systematic review. ANZ J Surg. 2021;91(1–2):42–8.
Lin E, Sarmiento JM. Laparoscopic extended right hepatectomy, portal lymphadenectomy, and hepaticojejunostomy for hilar cholangiocarcinoma. J Laparoendosc Adv Surg Tech A. 2014;24(6):411–6.
Yu H, Wu SD, Chen DX, Zhu G. Laparoscopic resection of Bismuth type I and II hilar cholangiocarcinoma: an audit of 14 cases from two institutions. Dig Surg. 2011;28(1):44–9.
Zhang CW, Liu J, Hong DF, Wang ZF, Hu ZM, Huang DS, et al. Pure laparoscopic radical resection for type IIIa hilar cholangiocarcinoma. Surg Endosc. 2018;32(3):1581–2.
Yu H, Wu SD, Tian Y, Su Y, Li YN. Single-incision laparoscopic resection of Bismuth I hilar cholangiocarcinoma. Surgical innovation. 2013;20(3):209–13.
Ratti F, Fiorentini G, Cipriani F, Catena M, Paganelli M, Aldrighetti L. Perihilar cholangiocarcinoma: are we ready to step towards minimally invasiveness? Updates Surg. 2020;72(2):423–33.
Cipriani F, Alzoubi M, Fuks D, Ratti F, Kawai T, Berardi G, et al. Pure laparoscopic versus open hemihepatectomy: a critical assessment and realistic expectations - a propensity score-based analysis of right and left hemihepatectomies from nine European tertiary referral centers. J Hepatobiliary Pancreat Sci. 2020;27(1):3–15.
Cipriani F, Ratti F, Cardella A, Catena M, Paganelli M, Aldrighetti L. Laparoscopic Versus Open Major Hepatectomy: Analysis of Clinical Outcomes and Cost Effectiveness in a High-Volume Center. J Gastrointest Surg. 2019;23(11):2163–73.
Li J, Zhao L, Zhang J, Li Z, Li A, Wei Y, et al. Application of the laparoscopic technique in perihilar cholangiocarcinoma surgery. Int J Surg. 2017;44:104–9.
Ebata T, Nagino M, Kamiya J, Uesaka K, Nagasaka T, Nimura Y, et al. Hepatectomy with portal vein resection for hilar cholangiocarcinoma: audit of 52 consecutive cases. Ann Surg. 2003;238(5):720–7.
Xu Y, Wang H, Ji W, Tang M, Li H, Leng J, et al. Robotic radical resection for hilar cholangiocarcinoma: perioperative and long-term outcomes of an initial series. Surg Endosc. 2016;30(7):3060–70.
Ratti F, Fiorentini G, Cipriani F, Paganelli M, Catena M, Aldrighetti L. Perioperative and Long-Term Outcomes of Laparoscopic Versus Open Lymphadenectomy for Biliary Tumors: A Propensity-Score-Based. Case-Matched Analysis Ann Surg Oncol. 2019;26(2):564–75.
Slim K. Laparoscopy within fast-track or within enhanced recovery after surgery? Ann Surg. 2014;259(2):e24.
Ni X, Jia D, Chen Y, Wang L, Suo J. Is the Enhanced Recovery After Surgery (ERAS) Program Effective and Safe in Laparoscopic Colorectal Cancer Surgery? A Meta-Analysis of Randomized Controlled Trials. J Gastrointest Surg. 2019;23(7):1502–12.
Morgan KA, Lancaster WP, Walters ML, Owczarski SM, Clark CA, McSwain JR, et al. Enhanced Recovery After Surgery Protocols Are Valuable in Pancreas Surgery Patients. J Am Coll Surg. 2016;222(4):658–64.
Wong-Lun-Hing EM, van Dam RM, van Breukelen GJ, Tanis PJ, Ratti F, van Hillegersberg R, et al. Randomized clinical trial of open versus laparoscopic left lateral hepatic sectionectomy within an enhanced recovery after surgery programme (ORANGE II study). Br J Surg. 2017;104(5):525–35.
Bednarski BK, Nickerson TP, You YN, Messick CA, Speer B, Gottumukkala V, et al. Randomized clinical trial of accelerated enhanced recovery after minimally invasive colorectal cancer surgery (RecoverMI trial). Br J Surg. 2019;106(10):1311–8.
Varadhan R, Weiss CO, Segal JB, Wu AW, Scharfstein D, Boyd C. Evaluating health outcomes in the presence of competing risks: a review of statistical methods and clinical applications. Med Care. 2010;48(6 Suppl):S96-105.
Koller MT, Raatz H, Steyerberg EW, Wolbers M. Competing risks and the clinical community: irrelevance or ignorance? Stat Med. 2012;31(11–12):1089–97.
Willms AG, Schaaf S, Zimmermann N, Schwab R, Güsgen C, Vilz TO, et al. The Significance of Visceral Protection in Preventing Enteroatmospheric Fistulae During Open Abdomen Treatment in Patients With Secondary Peritonitis: A Propensity Score-matched Case-control Analysis. Ann Surg. 2021;273(6):1182–8.
Bonnot PE, Piessen G, Kepenekian V, Decullier E, Pocard M, Meunier B, et al. Cytoreductive Surgery With or Without Hyperthermic Intraperitoneal Chemotherapy for Gastric Cancer With Peritoneal Metastases (CYTO-CHIP study): A Propensity Score Analysis. J Clin Oncol. 2019;37(23):2028–40.
Jingdong L, Yongfu X, Yang G, Jian X, Xujian H, Jianhua L, et al. Minimally invasive surgery for hilar cholangiocarcinoma: a multicenter retrospective analysis of 158 patients. Surg Endosc. 2021;35(12):6612–22.
Acknowledgements
We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This work was supported by grants from The National Natural Science Foundation of China (81772950 to RY Q, 81773160 to MW, 81702792 to SM X), Natural Science Foundation of Hubei Province (2017CFB467) to MW, Tongji Hospital Clinical Research Flagship Program (2019CR203) to RY Q, and Tongji Hospital Science Fund for Distinguished Young Scholars (2017) to MW, National Key Research and Development Program of China (2019YFC1315905).
Author information
Authors and Affiliations
Contributions
Min Wang: conceptualization, methodology, funding acquisition, and writing - original draft, supervision. Tingting Qin: conceptualization, methodology, data curation, investigation, and writing - original draft.Hang Zhang: data curation and investigation. Jingdong Li: conceptualization, methodology, software, and formal analysis. Xiaxing Deng: conceptualization, methodology, software, formal analysis, visualization, and writing - original draft. Yuhua Zhang: conceptualization, methodology, software, and formal analysis. Wenxing Zhao: data curation and investigation. Ying Fan: data curation and investigation. Dewei Li: data curation and investigation. Xuemin Chen: data curation, software, formal analysis, and investigation. Yecheng Feng: data curation and investigation. Siwei Zhu: data curation and investigation. Zhongqiang Xing: data curation and investigation. Guangsheng Yu: data curation and investigation. Jian Xu: data curation and investigation. Junjie Xie: data curation and investigation. Changwei Dou: data curation, funding acquisition and investigation. Hongqin Ma: data curation, funding acquisition and investigation. Gangshan Liu: data curation, funding acquisition and investigation. Yue Shao: data curation and investigation. Weibo Chen: data curation and funding acquisition. Simiao Xu: data curation and funding acquisition. Jun Liu: data curation and investigation. Jianhua Liu: writing - review & editing, project administration, resources, and supervision. Xinmin Yin: writing - review & editing, project administration, pesources, and supervision. Renyi Qin: conceptualization, writing - review & editing, project administration, funding acquisition, and supervision. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethical approval was given for the study by the ethics committee/Institutional Review Board of Ethics Committee of Tongji Hospital (approval number: TJ-IRB20220531). The need for informed consent was waived by the ethics committee/Institutional Review Board of Ethics Committee of Tongji Hospital, because the retrospective nature of the study. This research was also registered at ClinicalTrials.gov (identifier: NCT05402618; date of first registration: 02/06/2022). All methods were carried out in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, M., Qin, T., Zhang, H. et al. Laparoscopic versus open surgery for perihilar cholangiocarcinoma: a multicenter propensity score analysis of short- term outcomes. BMC Cancer 23, 394 (2023). https://doi.org/10.1186/s12885-023-10783-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-10783-9