
Abstract
Frailty is a geriatric syndrome that is an important public health problem for the older adults living in the USA. Although several methods have been developed to measure frailty in humans, we have very little understanding of its etiology. Because the molecular basis of frailty is poorly understood, mouse models would be of great value in determining which pathways contribute to the development of frailty. More importantly, mouse models would be critical in testing potential therapies to treat and possibly prevent frailty. In this article, we present data showing that Sod1KO mice, which lack the antioxidant enzyme, Cu/Zn superoxide dismutase, are an excellent model of frailty, and we compare the Sod1KO mice to the only other mouse model of frailty, mice with the deletion of the IL-10 gene. Sod1KO mice exhibit four characteristics that have been used to define human frailty: weight loss, weakness, low physical activity, and exhaustion. In addition, Sod1KO mice show increased inflammation and sarcopenia, which are strongly associated with human frailty. The Sod1KO mice also show alterations in pathways that have been proposed to play a role in the etiology of frailty: oxidative stress, mitochondrial dysfunction, and cell senescence. Using Sod1KO mice, we show that dietary restriction can delay/prevent characteristics of frailty in mice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Frailty is a clinical geriatric syndrome that is an important public health problem affecting a large proportion of older adults in the USA. Approximately 10% of older adults are frail; however, this prevalence increases markedly to 30% in those over 80 years of age (Collard et al. 2012; Mohler et al. 2014). The cost of frailty, including costs from falls and disability, was estimated to be more than $18 billion in 2000 (Janssen et al. 2004). This syndrome is recognized by geriatricians as a syndrome in which individuals show a progressive physical decline that is associated with increased medical comorbidity, disability, and mortality (Fried et al. 2001; Woods et al. 2005) even after taking common age-associated diseases and conditions into consideration (Fried and Walston 1998). As shown in Table 1, Fried et al. (2001) operationally defined and validated frailty as a medical syndrome of weight loss, weakness, slowness in walking, low physical activity, and exhaustion. Individuals with three or more of these five characteristics are categorized as frail, individuals with one or two are categorized as pre-frail, and individuals with none are classified as non-frail. These criteria were modeled in the Cardiovascular Health Study. In this cohort, individuals identified as frail were at significantly increased risk of hospitalization, falling, worsening disability, and death, after adjustment for multiple potential confounding factors, e.g., socioeconomic status, health status, subclinical and clinical disease, depressive symptoms, and disability status at baseline (Fried et al. 2001). In addition, the Cardiovascular Health Study showed that the increased risk for adverse health outcomes followed a stepwise pattern of increasing risk by frailty categorization, i.e., pre-frail conferred higher risk than non-frail and frail conferred higher risk than pre-frail, suggesting a dose–response relationship. In 2004, Studenski et al. developed a Clinical Global Impression of Change in Physical Frailty (CGIC-PF) instrument to assess physical frailty. As shown in Table 1, the CGIC-PF included six intrinsic domains (mobility, balance, strength, endurance, nutrition, and neuromotor performance) and seven consequence domains (medical complexity, healthcare utilization, appearance, self-perceived health, activities of daily living, emotional status, and social status) with each domain containing two to four clinical indicators. Changes were scored on a 7-point scale from markedly worse to markedly improved. Jones et al. (2004) developed a frailty screening tool based on items obtained from a comprehensive geriatric assessment, including impairments, disability, medical comorbidity, and quality of life. Rockwood et al. (2005) subsequently developed the 7-point clinical frailty scale in order to provide a simpler, more clinically useful tool for frailty screening. Therefore, while there is no clear consensus for frailty screening in the clinical setting, the frailty phenotype proposed by Fried et al. (2001) is the most extensively studied and has been cross-validated in several other cohorts, including the Women’s Health and Aging Studies (Bandeen-Roche et al. 2006), the Women’s Health Initiative (Woods et al. 2005), and the San Antonio Longitudinal Study of Aging (Espinoza and Hazuda 2008). One of the hallmark physical characteristics of frailty is sarcopenia, loss of muscle mass, and function. Sarcopenia is considered as a major underlying component of frailty and was included in conceptual framework, originally put forth by Fried and Walston (2003). Although the causal relationship between sarcopenia and frailty is unclear, Landi et al. (2015) argue that sarcopenia is a biological substrate of physical frailty.
Frailty is thought to represent a distinct physiologic state in which individuals are highly vulnerable to external stressors and recover poorly from these, rarely reaching their previous baseline of health and function (Fried and Walston 2003), i.e., it is characterized by loss of resilience, increased vulnerability to stress, and a lack of physiological reserve. Currently, a large amount of evidence suggests that low-grade inflammation plays an important role in the etiology of frailty. The initial studies showing an association between frailty and inflammation were obtained with serum or plasma markers of inflammation, such as interleukin-6 (IL-6) and C-reactive protein (CRP). Walston et al. (2002) found in the Cardiovascular Health Study that frail individuals had increased mean levels of CRP compared to non-frail individuals (5.5 ± 9.8 vs. 2.7 ± 4.0 mg/L). These peripheral blood markers persisted after exclusion of individuals with cardiovascular disease and diabetes, as well as after adjustment for age, sex, and race. Subsequently, Leng et al. (2002) found in community-dwelling older adults that serum IL-6 levels were elevated over 50% in frail compared to non-frail older adults. These findings have been replicated by Barzilay et al. (2007). Qu et al. (2009) found that expression of a potent inflammatory chemokine, CXCL-10, by monocytes was increased in frail compared to non-frail elderly, and there was high correlation between monocyte CXCL-10 expression and serum IL-6 levels. In addition, they found that monocytes from frail individuals had twofold increased expression of inflammatory genes compared to non-frail individuals. More recently, Collerton et al. (2012) showed an association of IL-6, TNF-α, and CRP levels with frailty in a large cross-sectional cohort in Scotland that included 845 subjects >85 years of age.
It has been argued that the increased inflammation observed in frail older adults might arise from increased oxidative stress. Oxidative stress increases with age and multiple studies report an association between oxidative stress and frailty. Protein carbonyls, which are a result of oxidative damage to proteins, were shown in a cross-sectional study to be associated with poor handgrip strength (Howard et al. 2007), and serum protein carbonyl levels were found to be an independent predictor of gait speed decline in humans (Semba et al. 2007). High levels of isoprostanes, which are produced by lipid peroxidation, have been reported to predict death in older adults (Cesari et al. 2012). In 2009, two groups reported that high oxidative stress was correlated with frailty. Serviddio et al. (2009) found increased levels of oxidized glutathione and protein adducts of malonaldehyde and 4-hydroxy-2,3-nonenal in the plasma of frail patients. Wu et al. (2009) showed an association between a marker of oxidative DNA damage (8-oxo-deoxyguanosine) in the plasma and frailty in elderly Chinese. More recently, Ingles et al. (2014) reported that markers of oxidative stress in plasma (malonaldehyde and protein carbonylation) were related to frailty but not to age or sex in a geriatric population, and in the Framingham Offspring Study, Liu et al. (2016) reported that elevated levels of plasma isoprostanes were associated with increased risk of frailty and slower gait speed.
Mitochondrial dysfunction has been proposed to play a role in frailty because mitochondria are the major source of reactive oxygen species (ROS) and energy in the cell. Therefore, changes in the function of mitochondria leading to increased ROS generation or reduced ATP generation could lead to frailty. For example, the increased oxidative stress that has been observed in frail older adults has been hypothesized to arise from mitochondrial dysfunction (Villamena and Zweier 2004). Consistent with this hypothesis is the study by Baptista et al. (2012) showing that superoxide anion production was increased in white blood cells of frail older adults. Recently, it was also shown in blood that, lower mtDNA copy number, a marker that reveals mitochondrial depletion, energy reserves, and oxidative stress is associated with frailty (Ashar et al. 2015).
More recently, it has been proposed that cell senescence may play a role in frailty (Fedarko 2011; LeBrasseur et al. 2015). It is now well accepted that senescent cells increase with age in many mammalian tissues and are found at sites of age-related pathologies (for reviews see Coppé et al. 2010 and Rodier and Campisi 2011). In addition, Campisi’s laboratory has shown that senescent cells secrete biologically active proteins (e.g., growth factors, proteases, cytokines, and other factors) that have potent autocrine and paracrine activities (Coppe et al. 2008), a phenomenon termed the senescence-associated secretory phenotype (SASP). The SASP includes several potent inflammatory cytokines including IL-6, IL-1β, and IL-8, which may serve as an important source of low-level chronic inflammation (Chung et al. 2009). Therefore, it is possible that increased cell senescence in frail older adults might contribute to increased chronic inflammation and the frailty phenotype. Baker et al. (2011) published the first direct evidence showing that cell senescence is involved in aging in mice. Using a mouse model they developed in which senescent, p16Ink4a-positive cells were eliminated upon the administration of the drug, AP20187, they were able to test the effect of reducing/eliminating senescent cells on aging/pathology. AP20187 treatment delayed/reduced the development of age-associated deficits known to accompany cell senescence, e.g., sarcopenia and the loss of adipose tissue. Of particular importance to frailty was the effect of eliminating senescent cells on muscle. Muscle fiber diameters of the AP20187-treated mice were larger than those of untreated mice and treadmill exercise tests revealed that duration of exercise, distance traveled, and overall amount of work performed were all significantly increased in the mice treated with AP20187, indicating preservation of muscle function by the elimination of senescent cells. They also showed that improvements in skeletal muscle function could also be achieved by the clearance of p16Ink4a-positive senescent cells.
Animal models of frailty
Over the past two decades, the use of genetically modified mouse models to study human diseases has become very popular, e.g., the use of ApoE or LDL receptor knockout mice to model atherosclerosis, which does not occur in normal mice, or the use of transgenic mice that produce a mutant form of a gene that has been shown to be associated with a human disease, e.g., transgenic mice that overexpress mutated amyloid precursor protein (Alzheimer’s disease), mutant Cu/Zn superoxide dismutase (amyotrophic lateral sclerosis), or mutant huntingtin (Huntington’s disease). The major advantage of mouse models that mimic a human disease is that one can use mice to identify potential targets for developing therapies as well as the biological mechanism(s) underlying the disease to be defined.
Because the molecular basis of frailty, a syndrome rather than a disease, is poorly understood, mouse models of frailty would be of great value in determining what pathways contribute to the development of frailty. More importantly, a mouse model of frailty would give the geriatric research community a model to use in testing potential therapies to treat and possibly prevent frailty. This is particularly important in treating frailty because older, frail individuals are in poor health and have limited resilience capacity.
Interleukin-10 knockout mouse
Interleukin-10 (IL-10) was identified as a cytokine produced by type 2 T helper cells in 1990 (Moore et al. 1990), and IL-10−/− (IL-10KO) mice have been generated to study the physiological role of IL-10. Kuhn et al. (1993) showed that IL-10KO mice develop a chronic enterocolitis because of an aberrant immune response. Subsequently, it was found that knocking out IL-10 resulted in an increased activation of nuclear factor-kappa B (NFκB) induced inflammatory mediators (Rennick et al. 1995; Berg et al. 1996). Because IL-10KO mice showed increased inflammation and because inflammation was believed to play a major role in frailty, Walston et al. (2008) determined whether the IL-10KO mice exhibited a frailty phenotype. As would be expected, the IL-10KO mice showed increased serum levels of IL-6. Studying mice from 10 to 18 months of age, Walston et al. (2008) found that the IL-10KO mice showed a greater decrease in grip strength with increasing age than wild-type (WT) mice and 125 genes were differentially expressed in the skeletal muscle of 50-week-old IL-10KO and WT mice. No major differences in body weight or measures of activity were found. Walston’s group (Ko et al. 2012) subsequently compared IL-10KO and WT mice from 12 to 90 weeks of age and found that the levels of circulating pro-inflammatory cytokines, e.g., IFN-γ, IL-1β, IL-6, KC, and TNF-α, were elevated across age groups in the IL-10KO mice. They also found a significant difference in the mortality between the IL-10KO and WT mice; the median survival of the IL-10KO mice was ~21 months while less than 10% of the WT mice had died at this age. IL-10KO mice also show mitochondrial dysfunction as suggested by lower rates of ATP synthesis and higher levels of damaged mitochondria in skeletal muscle (Akki et al. 2014; Ko et al. 2016).
Cu/Zn superoxide dismutase (Sod1KO) knockout mouse
Cu/Zn superoxide dismutase (Cu/ZnSOD) is the major superoxide dismutase isozyme that catalyzes the conversion of superoxide anions to hydrogen peroxide. It is found in all cells and is localized in the cytosol and the intermembrane space of the mitochondria (Okado-Matsumoto and Fridovich 2001). In 1996, Reaume et al. generated mice null for CuZnSOD (Sod1KO) and reported that they appear normal at birth. However, Sod1KO females are almost totally infertile due to ovarian dysfunction (Ho et al. 1998; Matzuk et al. 1998), and the Sod1KO mice show very high levels of oxidative stress in various tissues and plasma (Muller et al. 2006). In 2005, Huang’s laboratory reported that Sod1KO mice show a decrease in lifespan of approximately 30% (Elchuri et al. 2005). In 2013, our group confirmed that the lifespan of Sod1KO mice was reduced, e.g., median lifespan was reduced ~25% from ~30 months for WT mice to ~22 months for Sod1KO mice (Zhang et al. 2013a). Because Elchuri et al. (2005) reported that more than 70% of the Sod1KO mice developed liver hyperplasia and hepatocellular carcinoma later in life, it was initially believed that the decrease in the lifespan of the Sod1KO mice was the result of the dramatic increase in hepatocellular carcinoma, which is rare in C57BL/6 mice. In a more recent study, we found that only about 30% of the Sod1KO mice developed hepatocellular carcinoma later in life (Zhang et al. 2013a). However, data from several studies show that Sod1KO mice exhibited various accelerated aging phenotypes [e.g., hearing loss (Keithley et al. 2005), cataracts (Olofsson et al. 2007), skin thinning and delayed wound healing (Iuchi et al. 2010), and loss of muscle mass (Muller et al. 2006)] suggesting that the reduced lifespan of Sod1KO mice is largely a result of accelerated aging. We also showed that dietary restriction, which is a manipulation that retards aging in rodents, increased the lifespan of the Sod1KO mice to that of normal WT mice (Zhang et al. 2013a). Thus, the current data indicate that the Sod1KO mice show an accelerated aging phenotype.
We began considering that Sod1KO mice might be a mouse model of frailty because they exhibited many of the physiological deficits that characterize frailty in humans, e.g., weight loss, weakness, low physical activity, and exhaustion which were identified by Fried et al. (2001). Although the Sod1KO mice and WT mice are initially similar sizes, the growth of the Sod1KO mice is reduced resulting in ~20% decrease in body mass of the Sod1KO mice compared to WT mice (Muller et al. 2006). More important, as shown in Fig. 1a, the Sod1KO mice have an accelerated loss in muscle mass after 6 months of age compared to WT mice. Figure 1b shows that a significant decrease in the mass of all muscle types is observed in Sod1KO mice except for soleus. The greatest decrease in mass is observed in the gastrocnemius, which is the muscle most affected by aging in WT mice. The Sod1KO mice also show a significant decrease (~30%) in muscle strength as measured by a reduced grip strength (Fig. 2a). In addition, Larkin et al. (2011) showed that the strength of the muscle from Sod1KO mice was reduced. The lower force generating capacity was not explained entirely by the smaller muscle mass because when the force was normalized by muscle fiber cross-sectional area, the force generating capacity of the gastrocnemius muscle from the Sod1KO mice was still ~45% lower than WT mice indicating a decrease in the quality as well as in the quantity of muscle (Fig. 2b). Thus, the Sod1KO mice show marked increase in sarcopenia, which is a hallmark of frailty in humans.

Muscle mass is reduced in Sod1KO mice. a Hindlimb muscle mass of WT and Sod1KO mice over the lifespan of the Sod1KO mice. The age-dependent decrease in muscle mass in the Sod1KO mice, either absolute or relative to body mass, was statistically significant (P < 0.05) as determined by general linear model ANOVA. b Mass in milligrams for individual muscles from 20-month-old WT and Sod1KO mice. G/P gastrocnemius and plantaris, TA/EDL tibialis anterior and extensor digitorum longus, VL vastus lateralis, TB triceps brachii. Blue squares and bars represent WT and red squares and bars represent Sod1KO. Data were analyzed by general linear model ANOVA P < 0.05) with Tukey’s post hoc indicated by an asterisk. Data taken from Muller et al. (2006)

Muscle strength is reduced in Sod1KO mice. a Grip strength of 9-month-old male WT (n = 7) and Sod1KO mice (n = 8). Data are expressed as mean ± SEM. Data were analyzed by unpaired t test (*P < 0.05). b Maximum isometric specific force (specific Po) values for gastrocnemius muscle of WT and Sod1KO mice during direct muscle stimulation. Data for 1-, 8-, and 20-month-old mice were compared by two-factor (genotype × age) ANOVA. When the ANOVA showed significant differences between groups, individual differences were established by Bonferroni post hoc analyses. Significance was set at P < 0.05 (data taken from Larkin et al. 2011). Blue squares and bars represent WT and red squares and bars represent Sod1KO
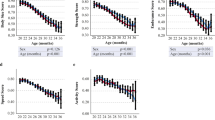
In addition to the loss of muscle mass and weakness, which are hallmarks of frailty, the Sod1KO mice also exhibit other phenotypes that are observed in humans, e.g., reduced physical activity and reduced endurance. The Sod1KO mice do not show any change in cage activity; however, spontaneous wheel running activity of the Sod1KO mice is dramatically reduced compared to the WT mice as shown in Fig. 3a (Muller et al. 2006). Although there are no data on walking speed of the Sod1KO mice, rotarod performance has been measured, which is a measure of endurance and muscle strength and has been used as a surrogate of maximal walking speed in mice (Liu et al. 2014). As shown in Fig. 3b, Sod1KO mice also show ~30% decrease in rotarod performance (Muller et al. 2006). Reduced endurance and exhaustion is also a phenotype of frailty in humans. We also measured the endurance exercise capacity of Sod1KO mice using treadmill running to exhaustion (Jang et al. 2010). Figure 3c shows that the distance that Sod1KO mice run to exhaustion is only about one third of the distance the WT mice run (e.g., 303 ± 95 vs. 859 ± 76 m). We also found that the Sod1KO mouse shows changes in pathways/processes that have been proposed to play a role in the etiology of frailty. As noted above, an increase in low-grade inflammation is believed to play an important role in frailty. We have several pieces of data indicating that inflammation is increased in the Sod1KO mice. First, we have found that the NFκB activation, which is involved in the transcription of inflammatory genes, is increased in skeletal muscle and kidney of Sod1KO mice compared to WT mice (Fig. 4a). Second, we measured a panel of pro-inflammatory cytokines in the sera of Sod1KO and WT mice (Zhang et al. 2017). As shown in Fig. 4b, four of the ten cytokines measured were significantly increased in the Sod1KO mice. If we combined the total content of the ten cytokines in the sera, we observed over a 1.8-fold increase in the level of circulating pro-inflammatory cytokines in the Sod1KO mice. Increased oxidative stress has also been correlated with frailty in humans (Serviddio et al. 2009; Wu et al. 2009; Ingles et al. 2014). As would be expected, Sod1KO mice are characterized by high levels of oxidative damage (Perez et al. 2009; Muller et al. 2006). As shown in Fig. 5a, we observed increased lipid peroxidation in plasma and muscle and increased oxidative damage to DNA in liver of the Sod1KO mice. Mitochondrial dysfunction, which has also been proposed to play a role in frailty (Walston et al. 2006; Wu et al. 2014), is also observed in Sod1KO mice. As shown in Fig. 5b, mitochondria from skeletal muscle of Sod1KO mice show increased production of reactive oxygen species and reduced ATP production. More recently, it has been argued that the accumulation of senescent cells could be involved in frailty (Tchkonia et al. 2013; Mohler et al. 2014), and as shown in Fig. 5c, we have recently found that cell senescence is increased in kidney and fat tissue of Sod1KO mice compared to WT mice.

Voluntary wheel running, rotarod performance, and treadmill endurance are reduced in Sod1KO mice. a Voluntary wheel running. WT and Sod1KO mice were individually housed in cages equipped with a zero-resistance running wheel and the average distance run each by each mouse over 16 weeks is shown. *P < 0.05 by ANOVA (data taken from Muller et al. 2006). b Rotarod performance. The average time in seconds that the mice remain on the rotating rod before falling off. *P < 0.05 by ANOVA (data taken from Muller et al. 2006). c Treadmill endurance. The time to run to exhaustion on a treadmill is shown for WT and Sod1KO mice. Significance was established using Student’s t test, ***P < 0.001 (data taken from Jang et al. 2010). Blue bars represent WT and red bars represent Sod1KO

Measures of inflammation are increased in Sod1KO mice. a NFκB binding activity of nuclear extracts from gastrocnemius muscle data was analyzed using ANOVA (data taken from Vasilaki et al. 2010) and kidney analyzed by two-tailed Student’s t test (data are taken from Zhang et al. (2017)) of WT and Sod1KO mice, *P < 0.05. b The levels of cytokines were measured in the serum collected from WT and Sod1KO mice and data were analyzed by one-tailed Student’s t test, *P < 0.05, **P < 0.01, ***P < 0.001 (data taken from Zhang et al. 2017). Blue bars represent WT and red bars represent Sod1KO

Oxidative stress, mitochondrial dysfunction, and cell senescence are increased in Sod1KO mice. a Oxidative damage. The level of lipid peroxidation (F2-isoprostanes) in plasma and whole hind limb skeletal muscle isoprostane. Data were analyzed using ANOVA and Tukey’s post hoc test, *P < 0.05) (data taken from Muller et al. 2006) and DNA oxidation (8-oxo-deoxyguanosine) in liver analyzed by the non-parametric test of ANOVA. Values that are significantly different (P < 0.05) (data taken from Perez VI et al. 2009) from WT and Sod1KO mice. b Mitochondrial dysfunction. The rate of ATP generation and hydrogen peroxide generation by isolated mitochondria from 20-month-old wild-type and Sod1KO mice is shown and the data were analyzed by Student’s t test, *P < 0.05, **P < 0.001 (data taken from Jang et al. 2010). c Cell senescence. The percent β-gal staining cells in kidney (data taken from Zhang et al. 2017) and fat tissue from Sod1KO and WT mice. Data were analyzed by Student’s t test, *P < 0.05. Blue bars represent WT and red bars represent Sod1KO
Discussion
Table 2 compares the phenotypes of frailty in humans to IL-10KO and Sod1KO mice. Both the IL-10KO and Sod1KO mice exhibit a significant decrease in lifespan, suggesting that they might physiologically age more rapidly than WT mice and therefore would be more prone to developing sarcopenia at a younger age. The IL-10KO mice, which were originally proposed by Walston et al. (2008) as a model of frailty, exhibit increased inflammation and reduced grip strength; however, there is limited information on whether the IL-10KO mice exhibit other characteristics of human frailty. In contrast, a great deal of information has been generated over the past decade on the Sod1KO mice, which indicates that Sod1KO mice would be a good model of frailty. As can be seen from Table 2, the Sod1KO mice exhibit changes in four of the five defining characteristics of human frailty proposed by Fried et al. (2001): weight loss, weakness, low physical activity, and exhaustion. In addition, the Sod1KO mice show increased circulating levels of pro-inflammatory cytokines and develop sarcopenia, which are strongly associated with frailty in humans. The Sod1KO mice also show alterations in pathways that have been proposed to play a role in the etiology of frailty: oxidative stress, mitochondrial dysfunction, and cell senescence.
Although the IL-10KO and Sod1KO mouse models are currently the best mouse models of frailty available, there is always the question of how accurately deleting IL-10 or Sod1 replicates frailty because there is no evidence that the expression of either of these genes plays a role in frailty in humans. In addition, these mice develop special pathologies normally not observed in the WT mice, e.g., chronic enterocolitis in the IL-10KO mice and hepatocellular carcinoma in about one third of the Sod1KO mice. Nevertheless, the IL-10KO and Sod1KO mouse models give investigators the first tools for studying the mechanism underlying frailty and testing interventions to delay/prevent frailty. Important information about frailty has already been gained from these models. For example, they have provided direct evidence for inflammation playing an important role in frailty. The data by Walston et al. (2008) with IL-10KO mice in which inflammation is induced demonstrates that inflammation most likely plays a causative role in frailty. Our data showing that Sod1KO mice have increased inflammation also support the concept that inflammation plays a role in the etiology of frailty. In addition, the Sod1KO mouse model provides our first insight into how frailty might be prevented/delayed. Frailty in Sod1KO mice is attenuated by dietary restriction, e.g., dietary restriction reversed the loss of muscle mass and function and improved mitochondria function (Jang et al. 2012) and attenuated the increase in oxidative damage, cell senescence, and circulating levels of IL-6 (Zhang et al. 2017). These data are supported by a recent study from Kane et al. (2016) showing that 6 months of dietary restriction improved the frailty index score of 24-month-old WT mice.
In summary, the IL-10KO and Sod1KO mouse models give investigators the first animal models that can be used to study frailty. These mouse models allow investigators to use genetic approaches to identify the pathways that can lead to frailty as well as determine which tissues are key in the development of frailty. Because these two models induce frailty through different pathways (e.g., immune dysfunction for the IL-10KO mice and increased oxidative stress in the Sod1KO mice), they are complementary and a combination of these models will give investigators a robust approach to identifying the biological processes underlying frailty. In addition, the use of conditional Sod1KO models allow the investigators to study the effect of the tissue-specific deletion of Cu/Zn superoxide dismutase on frailty. Sod1flox/flox have been generated (Zhang et al. 2013b) and used to study the role of the muscle and motor neurons in sarcopenia (Zhang et al. 2013b; Sataranatarajan et al. 2015).
References
Akki A, Yang H, Gupta A, Chacko VP, Yano T, Leppo MK, Steenbergen C, Walston J, Weiss RG (2014) Skeletal muscle ATP kinetics are impaired in frail mice. Age 36:21–30
Ashar FN, Moes A, Moore AZ, Grove ML, Chaves PH, Coresh J, Newman AB, Matteini AM, Bandeen-Roche K, Boerwinkle E, Walston JD, Arking DE (2015) Association of mitochondrial DNA levels with frailty and all-cause mortality. J Mol Med 93:177–186
Baker DJ, Wijshake T, Tchkonia T, LeBrasseur NK, Childs BG, van de Sluis B, Kirkland JL, van Deursen JM (2011) Clearance of p16Ink4a-positive senescent cells delays ageing-associated disorders. Nature 479:232–236
Bandeen-Roche K, Xue QL, Ferrucci L, Walston J, Guralnik JM, Chaves P, Zeger SL, Fried LP (2006) Phenotype of frailty: characterization in the women's health and aging studies. J Gerontol A Biol Sci Med Sci 61:262–266
Baptista G, Dupuy AM, Jaussent A, Durant R, Ventura E, Sauguet P, Picot MC, Jeandel C, Cristol JP (2012) Low-grade chronic inflammation and superoxide anion production by NADPH oxidase are the main determinants of physical frailty in older adults. Free Radic Res 46:1108–1114
Barzilay JI, Blaum C, Moore T, Xue QL, Hirsch CH, Walston JD, Fried LP (2007) Insulin resistance and inflammation as precursors of frailty: the Cardiovascular Health Study. Arch Intern Med 167:635–641
Berg DJ, Davidson N, Kuhn R, Muller W, Menon S, Holland G, Thompson-Snipes L, Leach MW, Rennick D (1996) Enterocolitis and colon cancer in interleukin-10-deficient mice are associated with aberrant cytokine production and CD4(+) TH1-like responses. J Clin Invest 98:1010–1020
Cesari M, Kritchevsky SB, Nicklas B, Kanaya AM, Patrignani P, Tacconelli S, Tranah GJ, Tognoni G, Harris TB, Incalzi RA, Newman AB, Pahor M (2012) Oxidative damage, platelet activation, and inflammation to predict mobility disability and mortality in older persons: results from the health aging and body composition study. J Gerontol A Biol Sci Med Sci 67:671–676
Chung HY, Cesari M, Anton S, Marzetti E, Giovannini S, Seo AY, Carter C, Yu BP, Leeuwenburgh C (2009) Molecular inflammation: underpinnings of aging and age-related diseases. Ageing Res Rev 8(1):18–30
Collard RM, Boter H, Schoevers RA, Oude Voshaar RC (2012) Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc 60:1487–1492
Collerton J, Martin-Ruiz C, Davies K, Hilkens CM, Isaacs J, Kolenda C, Parker C, Dunn M, Catt M, Jagger C, von Zglinicki T, Kirkwood TB (2012) Frailty and the role of inflammation, immunosenescence and cellular ageing in the very old: cross-sectional findings from the Newcastle 85+ Study. Mech Ageing Dev 133:456–466
Coppe JP, Patil CK, Rodier F, Sun Y, Munoz DP, Goldstein J, Nelson PS, Desprez PY, Campisi J (2008) Senescence-associated secretory phenotypes reveal cell-nonautonomous functions of oncogenic RAS and the p53 tumor suppressor. PLoS Biol 6:2853–2868
Coppé JP, Desprez PY, Krtolica A, Campisi J (2010) The senescence-associated secretory phenotype: the dark side of tumor suppression. Annu Rev Pathol 5:99-118
Elchuri S, Oberley TD, Qi W, Eisenstein RS, Jackson Roberts L, Van Remmen H, Epstein CJ, Huang TT (2005) CuZnSOD deficiency leads to persistent and widespread oxidative damage and hepatocarcinogenesis later in life. Oncogene 24:367–380
Espinoza SE, Hazuda HP (2008) Frailty in older Mexican-American and European-American adults: is there an ethnic disparity? J Am Geriatr Soc 56:1744–1749
Fedarko NS (2011) The biology of aging and frailty. Clin Geriatr Med 27:27–37
Fried LP, Walston J (1998) Frailty and failure to thrive. In: Hazzard WR, Blass JP, Ettinger WH Jr, Halter JB, Ouslander J (eds) Principles of geriatric medicine and gerontology. McGraw Hill Publisher, New York, pp 1387–1402
Fried LP and Walston J (2003) Frailty and failure to thrive. In: Hazzard W, Blass JP, Halter JB, et al (eds) Principles of geriatric medicine and gerontology, 5th edn, McGraw-Hill Publisher, New York, pp 1487-1502
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA (2001) Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 56:M146–M156
Ho YS, Gargano M, Cao J, Bronson RT, Heimler I, Hutz RJ (1998) Reduced fertility in female mice lacking copper-zinc superoxide dismutase. J Biol Chem 273:7765–7769
Howard C, Ferrucci L, Sun K, Fried LP, Walston J, Varadhan R, Guralnik JM, Semba RD (2007) Oxidative protein damage is associated with poor grip strength among older women living in the community. J Appl Physiol 103:17–20
Ingles M, Gambini J, Carnicero JA, Garcia-Garcia FJ, Rodriguez-Manas L, Olaso-Gonzalez G, Dromant M, Borras C, Vina J (2014) Oxidative stress is related to frailty, not to age or sex, in a geriatric population: lipid and protein oxidation as biomarkers of frailty. J Am Geriatr Soc 62:1324–1328
Iuchi Y, Roy D, Okada F, Kibe N, Tsunoda S, Suzuki S, Takahashi M, Yokoyama H, Yoshitake J, Kondo S, Fujii J (2010) Spontaneous skin damage and delayed wound healing in SOD1-deficient mice. Mol Cell Biochem 341:181–194
Jang YC, Lustgarten MS, Liu Y, Muller FL, Bhattacharya A, Liang H, Salmon AB, Brooks SV, Larkin L, Hayworth CR, Richardson A, Van Remmen H (2010) Increased superoxide in vivo accelerates age-associated muscle atrophy through mitochondrial dysfunction and neuromuscular junction degeneration. FASEB J 24:1376–1390
Jang YC, Liu Y, Hayworth CR, Bhattacharya A, Lustgarten MS, Muller FL, Chaudhuri A, Qi W, Li Y, Huang JY, Verdin E, Richardson A, Van Remmen H (2012) Dietary restriction attenuates age-associated muscle atrophy by lowering oxidative stress in mice even in complete absence of CuZnSOD. Aging Cell 11:770–782
Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R (2004) The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc 52:80–85
Jones DM, Song X, Rockwood K (2004) Operationalizing a frailty index from a standardized comprehensive geriatric assessment. J Am Geriatr Soc 52:1929–1933
Kane AE, Hilmer SN, Boyer D, Gavin K, Nines D, Howlett SE, de Cabo R, Mitchell SJ (2016) Impact of longevity interventions on a validated mouse clinical frailty index. J Gerontol A Biol Sci Med Sci 71:333–339
Keithley EM, Canto C, Zheng QY, Wang X, Fischel-Ghodsian N, Johnson KR (2005) Cu/Zn superoxide dismutase and age-related hearing loss. Hear Res 209:76–85
Ko F, Yu Q, Xue QL, Yao W, Brayton C, Yang H, Fedarko N, Walston J (2012) Inflammation and mortality in a frail mouse model. Age 34:705–715
Ko F, Abadir P, Marx R, Westbrook R, Cooke C, Yang H, Walston J (2016) Impaired mitochondrial degradation by autophagy in the skeletal muscle of the aged female interleukin 10 null mouse. Exp Gerontol 73:23–27
Kuhn R, Lohler J, Rennick D, Rajewsky K, Muller W (1993) Interleukin-10-deficient mice develop chronic enterocolitis. Cell 75:263–274
Landi F, Calvani R, Cesari M, Tosato M, Martone AM, Bernabei R, Onder G, Marzetti E (2015) Sarcopenia as the biological substrate of physical frailty. Clin Geriatr Med 31:367–374
Larkin LM, Davis CS, Sims-Robinson C, Kostrominova TY, Van Remmen H, Richardson A, Feldman EL, Brooks SV (2011) Skeletal muscle weakness due to deficiency of CuZn-superoxide dismutase is associated with loss of functional innervation. Am J Physiol Regul Integr Comp Physiol 301:R1400–R1407
LeBrasseur NK, Tchkonia T, Kirkland JL (2015) Cellular senescence and the biology of aging, disease, and frailty. Nestle Nutr Inst Workshop Ser 83:11–18
Leng S, Chaves P, Koenig K, Walston J (2002) Serum interleukin-6 and hemoglobin as physiological correlates in the geriatric syndrome of frailty: a pilot study. J Am Geriatr Soc 50:1268–1271
Liu H, Graber TG, Ferguson-Stegall L, Thompson LV (2014) Clinically relevant frailty index for mice. J Gerontol A Biol Sci Med Sci 69:1485–1491
Liu CK, Lyass A, Larson MG, Massaro JM, Wang N, D'Agostino RB Sr, Benjamin EJ, Murabito JM (2016) Biomarkers of oxidative stress are associated with frailty: the Framingham Offspring Study. Age 38:1
Matzuk MM, Dionne L, Guo Q, Kumar TR, Lebovitz RM (1998) Ovarian function in superoxide dismutase 1 and 2 knockout mice. Endocrinology 139:4008–4011
Mohler MJ, Fain MJ, Wertheimer AM, Najafi B, Nikolich-Zugich J (2014) The frailty syndrome: clinical measurements and basic underpinnings in humans and animals. Exp Gerontol 54:6–13
Moore KW, Vieira P, Fiorentino DF, Trounstine ML, Khan TA, Mosmann TR (1990) Homology of cytokine synthesis inhibitory factor (IL-10) to the Epstein-Barr virus gene BCRFI. Science 248:1230–1234
Muller FL, Song W, Liu Y, Chaudhuri A, Pieke-Dahl S, Strong R, Huang TT, Epstein CJ, Roberts LJ 2nd, Csete M, Faulkner JA, Van Remmen H (2006) Absence of CuZn superoxide dismutase leads to elevated oxidative stress and acceleration of age-dependent skeletal muscle atrophy. Free Radic Biol Med 40:1993–2004
Okado-Matsumoto A, Fridovich I (2001) Subcellular distribution of superoxide dismutases (SOD) in rat liver: Cu,Zn-SOD in mitochondria. J Biol Chem 276:38388–38393
Olofsson EM, Marklund SL, Behndig A (2007) Glucose-induced cataract in CuZn-SOD null lenses: an effect of nitric oxide? Free Radic Biol Med 42:1098–1105
Perez VI, Bokov A, Van Remmen H, Mele J, Ran Q, Ikeno Y, Richardson A (2009) Is the oxidative stress theory of aging dead? Biochim Biophys Acta 1790:1005–1014
Qu T, Yang H, Walston JD, Fedarko NS, Leng SX (2009) Upregulated monocytic expression of CXC chemokine ligand 10 (CXCL-10) and its relationship with serum interleukin-6 levels in the syndrome of frailty. Cytokine 46:319–324
Reaume AG, Elliott JL, Hoffman EK, Kowall NW, Ferrante RJ, Siwek DF, Wilcox HM, Flood DG, Beal MF, Brown RH Jr, Scott RW, Snider WD (1996) Motor neurons in Cu/Zn superoxide dismutase-deficient mice develop normally but exhibit enhanced cell death after axonal injury. Nat Genet 13:43–47
Rennick D, Davidson N, Berg D (1995) Interleukin-10 gene knock-out mice: a model of chronic inflammation. Clin Immunol Immunopathol 76:S174–S178
Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, Mitnitski A (2005) A global clinical measure of fitness and frailty in elderly people. CMAJ 173:489–495
Rodier F, Campisi J (2011) Four faces of cellular senescence. J Cell Biol 192:547–556
Sataranatarajan K, Qaisar R, Davis C, Sakellariou GK, Vasilaki A, Zhang Y, Liu Y, Bhaskaran S, McArdle A, Jackson M, Brooks SV, Richardson A, Van Remmen H (2015) Neuron specific reduction in CuZnSOD is not sufficient to initiate a full sarcopenia phenotype. Redox Biol 5:140–148
Semba RD, Ferrucci L, Sun K, Walston J, Varadhan R, Guralnik JM, Fried LP (2007) Oxidative stress is associated with greater mortality in older women living in the community. J Am Geriatr Soc 55:1421–1425
Serviddio G, Romano AD, Greco A, Rollo T, Bellanti F, Altomare E, Vendemiale G (2009) Frailty syndrome is associated with altered circulating redox balance and increased markers of oxidative stress. Int J Immunopathol Pharmacol 22:819–827
Studenski S, Hayes RP, Leibowitz RQ, Bode R, Lavery L, Walston J, Duncan P, Perera S (2004) Clinical global impression of change in physical frailty: development of a measure based on clinical judgment. J Am Geriatr Soc 52:1560–1566
Tchkonia T, Zhu Y, van Deursen J, Campisi J, Kirkland JL (2013) Cellular senescence and the senescent secretory phenotype: therapeutic opportunities. J Clin Invest 123:966–972
Vasilaki A, van der Meulen JH, Larkin L, Harrison DC, Pearson T, Van Remmen H, Richardson A, Brooks SV, Jackson MJ, McArdle A (2010) The age-related failure of adaptive responses to contractile activity in skeletal muscle is mimicked in young mice by deletion of Cu,Zn superoxide dismutase. Aging Cell 9:979–990
Villamena FA, Zweier JL (2004) Detection of reactive oxygen and nitrogen species by EPR spin trapping. Antioxid Redox Signal 6:619–629
Walston J, McBurnie MA, Newman A, Tracy RP, Kop WJ, Hirsch CH, Gottdiener J, Fried LP, Cardiovascular Health S (2002) Frailty and activation of the inflammation and coagulation systems with and without clinical comorbidities: results from the Cardiovascular Health Study. Arch Intern Med 162:2333–2341
Walston J, Hadley EC, Ferrucci L, Guralnik JM, Newman AB, Studenski SA, Ershler WB, Harris T, Fried LP (2006) Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc 54:991–1001
Walston J, Fedarko N, Yang H, Leng S, Beamer B, Espinoza S, Lipton A, Zheng H, Becker K (2008) The physical and biological characterization of a frail mouse model. J Gerontol A Biol Sci Med Sci 63:391–398
Woods NF, LaCroix AZ, Gray SL, Aragaki A, Cochrane BB, Brunner RL, Masaki K, Murray A, Newman AB, Women's Health I (2005) Frailty: emergence and consequences in women aged 65 and older in the Women's Health Initiative Observational Study. J Am Geriatr Soc 53:1321–1330
Wu IC, Shiesh SC, Kuo PH, Lin XZ (2009) High oxidative stress is correlated with frailty in elderly Chinese. J Am Geriatr Soc 57:1666–1671
Wu I, Hsiung CA, Hsu C, Lin X. (2014) Oxidative stress and frailty: a closer look at the origin of a human aging phenotype. In: Preedy VR (ed) Aging: oxidative stress and dietary antioxidants, Elsevier Inc., pp 3–13
Zhang Y, Ikeno Y, Bokov A, Gelfond J, Jaramillo C, Zhang HM, Liu Y, Qi W, Hubbard G, Richardson A, Van Remmen H (2013a) Dietary restriction attenuates the accelerated aging phenotype of Sod1(-/-) mice. Free Radic Biol Med 60:300–306
Zhang Y, Davis C, Sakellariou GK, Shi Y, Kayani AC, Pulliam D, Bhattacharya A, Richardson A, Jackson MJ, McArdle A, Brooks SV, Van Remmen H (2013b) CuZnSOD gene deletion targeted to skeletal muscle leads to loss of contractile force but does not cause muscle atrophy in adult mice. FASEB J 27:3536–3548
Zhang Y, Unnikrishnan A, Deepa SS, Liu Y, Li Y, Ikeno Y, Sosnowska D, Van Remmen H, Richardson A (2017) A new role for oxidative stress in aging: the accelerated aging phenotype in Sod1-/- mice is correlated to increased cellular senescence. Redox Biol 11:30–37
Acknowledgements
The research described above on the Sod1KO mice were generated over the past decade on program project grants from the National Institute on Aging to Drs. Brooks, Jackson, McArdle, Richardson, and Van Remmen (P01-AG020591 and P01-AG051442). Richardson and Van Remmen are supported by Senior Research Scientist Career awards from the Department of Veterans Affairs.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Deepa, S.S., Bhaskaran, S., Espinoza, S. et al. A new mouse model of frailty: the Cu/Zn superoxide dismutase knockout mouse. GeroScience 39, 187–198 (2017). https://doi.org/10.1007/s11357-017-9975-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-017-9975-9