
Abstract
Background
Periodontal health is of great concern for periodontists and orthodontists in the inter-disciplinary management of patients with bimaxillary protrusion. The aim of present study is to investigate changes in the alveolar bone in the maxillary incisor region and to explore its relationship with displacement of root apex as well as changes in the inclination of maxillary incisors during incisor retraction.
Methods
Samples in this retrospective study consisted of 38 patients with bimaxillary protrusion. Cone-beam computed tomography (CBCT) images was taken before(T0) and after (T1) treatment. Alveolar bone thickness (ABT), height (ABH) and area (ABA) were utilized to evaluate changes in the alveolar bone, while incisor inclination and apex displacement were used to assess changes in the position of maxillary central and lateral incisors. Correlations between alveolar bone remodeling and apex displacement as well as changes in the inclination were investigated.
Results
The labial ABT of central and lateral incisors at the mid-root third was increased. In contrast, the palatal ABT at crestal, mid-root and apical third level were consistently decreased. ABH was not altered on the labial side, while significantly decreased on the palatal side. ABA was not significantly increased on the labial side, but significantly decreased on the palatal side, leading to a significantly reduced total ABA. Orthodontic treatment significantly reduced inclination of upper incisors. Changes in the amount (T1-T0) of ABA was remarkably correlated with apex displacement and changes of inclination (T1-T0); in addition, using the multivariate linear regression analysis, changes of ABA on the palatal side (T1-T0) can be described by following equation: Changes of palatal ABA (T1-T0) = − 3.258- 0.139× changes of inclination (T1-T0) + 2.533 × apex displacement (T1-T0).
Conclusions
Retraction of incisors in bimaxillary protrusion patients may compromise periodontal bone support on the palatal side. An equation that incorporated the displacement of root apex and change in the incisor inclination may enable periodontist-orthodontist interdisciplinary coordination in assessing treatment risks and developing an individualized treatment plan for adult patients with bimaxillary protrusion. Moreover, the equation in predicating area of alveolar bone may reduce the risks of placing the teeth out of the bone boundary during 3D digital setups.
Similar content being viewed by others


Background
Bimaxillary protrusion, a well-recognized malocclusion in Eastern Asian communities, is characterized by proclined incisors as well as protruded lips [1]. Negative perception of protrusive dentitions and lips is one major concern for patients to seek orthodontic care [2]. Four-premolar extraction, maximal anchorage and incisor retraction are often included in the treatment to achieve optimal improvement in the lip morphology [3]. Although dynamic remodeling of alveolar bone might ensue orthodontic tooth movement (OTM) [4,5,6], the large retraction of incisors poses a great challenge to the periodontal health in patients with bimaxillary protrusion. Precise treatment planning and risk assessment may help reduce the periodontal sequelae in patients with bimaxillary protrusion [7].
Despite the persistent controversy regarding the alveolar bone remodeling pattern during OTM, i.e. “through the bone” or “with the bone” theory [8], the 2014 American Association of Periodontal Regeneration World Workshop systematic review reports that the direction of the tooth movement and the bucco-lingual thickness of the gingiva play important roles in soft tissue alterations during orthodontic treatment [7]. Therefore, to reduce the periodontal risk in patients with bimaxillary protrusion, an inter-disciplinary approach involving the orthodontists and periodontists in the decision-making process would definitely reduce periodontal sequelae and improve orthodontic treatment outcome [9]. Anatomic features of local alveolar process, periodontal remodeling potential and orthodontic tooth movement pattern should be included in determining overall treatment plan and specific force system.
Cone-beam computed tomography (CBCT) images are being widely used in orthodontics to assess 3-dimensional (3D) spatial relationship in the diagnosis of impacted teeth [10]. In addition, 3D imaging allows for accurate detection of anatomic features of alveolus, which is superior to lateral cephalometric, intraoral periapical or panoramic radiographs [11]. Information on the alveolar bone surrounding incisors is of vital importance to determine the boundary of orthodontic tooth movement.
In addition to assessment of periodontal tissue condition and remodeling potential, accurate orthodontic treatment plan and precise tooth movement control should also be guaranteed to minimize periodontal risks. Upon application of orthodontic forces on the periodontal ligament, biological responses in the molecular and cellular level will lead to several types of OTM, including uncontrolled tipping, controlled tipping and bodily movement [12]. Such differed types of OTM may lead to varied displacement of the apex and incisor inclination although retraction of incisal edge is similar.
Orthodontic tooth movement is limited by the anatomic dentoalveolar boundaries that are set by the cortical plates of the alveolus at the level of the incisor apices [5]. Digital setup by available softwares, such as OrthoCAD (Align Technology, San Jose, Calif), SureSmile (Orametrix, Richardson, Tex), and Orchestrate (Orchestrate, Rialto, Calif), has been widely utilized to mimic tooth movement and predict final position of the dentition rather accurately [13]. However, without taking the alveolar anatomy and its remodeling capacity into consideration, digital setup-aided orthodontics as well as traditional orthodontics may possibly put the dentition out of the boundary, leading to instability, root resorption and alveolar bone loss [7].
Currently, CBCT data are focused on morphological changes during OTM [4, 14, 15]. However, few data are available regarding the correlation between incisor retraction and alveolar bone remodeling. To facilitate dentoalveolar bone risk assessment in the inter-disciplinary management of bimaxillary protrusion, we aimed to investigate changes in the alveolar bone in the incisor region before (T0) and after treatment (T1) and to explore its relationship with displacement of root apex as well as changes in the inclination of maxillary incisors. The null hypotheses of this study were that: (1) there was no changes in alveolar bone thickness (ABT), height (ABH), and area (ABA) before and after treatment; (2) the displacement of root apex and change in the inclination of maxillary incisor would not affect the alveolar bone area (ABA).
Methods
Materials
The study was designed as a retrospective cohort study. Ethical approval for the study was obtained from the Institutional Ethics Committee. The Institutional Review Board (IRB) number is 2019NL-064(KS). The study included data from 38 patients (31 females and 7 males), retrieved from the archive of medical school of university. All the patients started treatment from Jan 1st, 2014 to Dec 31st, 2017, and finished before June 30, 2019. The mean preoperative age was 19.52 years with an overall range of 15–33 years. Treatment time was 26 ± 4 months.
All patients were treated with interactive self-ligating brackets (American Orthodontics, USA). The self-ligating brackets are active in the incisors and passive in the canines, premolars, and molars with an MB prescription. The treatment protocol was briefly described as below. Alignment was achieved by sequential insertion of 0.014- and 0.018-in. nickel-titanium (NiTi) archwires, followed by levelling with 0.016 × 0.022- and 0.018 × 0.025-in. NiTi archwires, and space closure was finished with 0.019 × 0.025-in. stainless-steel (SS) archwires by en masse retraction and sliding mechanics. A retraction force of 100 g from the temporary anchorage devices (TADs) to the hook between lateral incisors and canines was utilized. The TADs were inserted at about 5 mm above the gingival margin between the 2nd premolars and 1st molars to achieve maximal anchorage. Appointment intervals were approximately 6 weeks. A lateral x-ray was used to perform the cephalometric analysis. The cephalometric data were presented in Table 1.
A sample size calculation was undertaken using the PASS software package (Version 15.0; NCSS, USA). Since no relevant data regarding the regression analysis between changes in ABA, changes in inclination of maxillary incisor, and displacement of tooth apex was reported, the sample size calculation was based on our pilot study (n = 8). The pilot study estimated that R2 was 0.63. Based on a significance level of alpha 0.05, the sample size was calculated to achieve an 80% power and the sample size calculation showed that 27 subjects were necessary.
Inclusion criteria for bimaxillary protrusion patients are:
-
(1).
With complete CBCT data before(T0) and after treatment(T1)
-
(2).
Class I canine and molar relationship;
-
(3).
Pretreatment interincisal angle less than 124° with a crowding of less than 4 mm in the maxillary arch;
-
(4).
Full permanent dentition anterior to the first molars;
-
(5).
A minimum age of 15 in girls and 18 in boys to reduce effects of growth on dental structures.
Patients with previous orthodontic treatment, cleft lip palate, impacted anterior teeth, congenital tooth loss except third molars, systemic diseases and compromised periodontium were excluded.
3D image processing and measurements
All pretreatment and posttreatment CBCT were taken by the same machine. CBCT scans (NewTomVG, Quantitative Radiology, Verona, Italy) were taken before (T0) and after treatment (T1). The following imaging acquisition parameters were used: 16 × 16 cm field of view (FOV), 5 mA, 110 kV, and 3.6 s exposure time, which generated an isotropic voxel size of 0.3 mm. The effective dose of radiation was approximately 80 μSv.
The examined subjects were positioned in the sagittal plane perpendicular to the floor, which was parallel to the Frankfort plane. All CBCT data were exported to digital imaging and communications in medicine (DICOM) format. The 3D images were reconstructed using NNT Viewer software (NewTomVG, Quantitative Radiology, Verona, Italy).
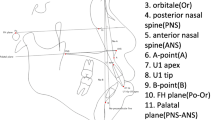
In NNT Viewer, the sagittal slices were cut through the center of apical foramen and parallel to the long axis of individual incisors. These images were imported into the software ImageJ (version 2.0, NIH, Bethesda, Md), within which the following variables were measured: (1) alveolar bone thickness (ABT) on the buccal and palatal side at 3, 6 and 9 mm from the cementoenamel junction (CEJ), which was designated as crestal, mid-root and apical third; (2) labial and palatal alveolar bone area (ABA); (3) labial and palatal alveolar bone height (ABH), defined as the distance from the CEJ to the alveolar ridge crest (Fig. 1 a and b).

Determination of alveolar bone morphology in incisors. Alveolar bone thickness was measured at the apical, mid-root and crestal level. CEJ: cementoenamel junction
Tooth movement of individual maxillary incisor was determined by apex displacement and axis inclination alteration (modified from Kyoung-Won et al.) [16]. The apical displacement was registered as the changes of the distance between the upper incisors’ apical foramen and the palatal cortical bone, with apex moving towards buccal plates defined as positive and towards palatal plates as negative. The rationale of the reference mark is that the palatal cortical plate does not undergo structural changes and remain to be stable in adult patients [17]. Moreover, this reference mark was very close to the investigated area avoiding unwanted changes of remote structures and minimizing errors of measurement. Inclination of individual incisor was determined as the lower backward angle between the long axis and Frankfort Horizontal (FH) plane.
Statistical analyses
All measurements were conducted by one trained examiner. To reduce the measurement error, we took the average value of three measurements whose time interval was one-month as the result. The inter-examiner agreement was performed by another experienced investigator. Repeated measurements were examined by the paired t-test (systematic errors) and the Dahlberg formula (casual errors) [16]. No significant systematic errors were found (P > 0.1), and the random errors were small, showing high rates of reproducibility. The normality of distribution of the variables was assessed by Shapiro-Wilks test. Interphase changes (T1–T0) were calculated, and if normally distributed, these were compared using paired t-tests; if this was not the case, the Wilcoxon test was used. Pearson’s Chi-square test was applied to determine whether different ways of teeth movement affected the measurement results before and after treatment. Regression analysis was performed to determine the relationship between changes in the alveolar bone area and apex displacement as well as changes in the inclination of incisors. All statistical analyses were performed with GraphPad Prism 8.0.1 and SPSS Statistics with a significance level of 0.05.
Results
Incisor tooth movement
Inclination of incisors related to FH plane and anatomic position of apex foramen to palatal cortical plate was determined to reflect the 3-dimensional position of the incisors. Although we selected cases with a crowding less than 4 mm, the inclination of central and lateral incisors demonstrated a rather large discrepancy, a result of crowding and irregularity in the maxillary front region. The inclination of central and lateral was significantly reduced after treatment (Table 2). In addition, the distance of apex of central and lateral incisors to palatal cortical plate was significantly reduced with an average of 1.0 mm and 1.9 respectively, showing that root apex was moved towards the palatal cortical plate (Table 2).
Alveolar bone thickness
We next explored changes of the buccal, palatal and total ABT at the crestal, mid-root and apical third. The labial ABT of both central and lateral incisors at the mid-root third was increased significantly (P < 0.05), while no significant difference was observed at the crestal and apical third. In contrast, the palatal ABT of the central and lateral incisors at all three levels were consistently decreased (P < 0.05). Regarding changes in the total ABT, significant reduction was observed in both central and lateral incisors at the crestal level, and in lateral incisors at the mid-root third level as well as apical third level (P < 0.05) (Table 3).
Alveolar bone height
In consistence with the reduced ABA, a significant decrease in the palatal ABH of both central and lateral incisors was observed between T0 and T1 (P < 0.001), indicating palatal alveolar bone resorption. However, in terms of labial ABH, no significant difference was observed (Table 4).
Alveolar bone area
Decreased palatal ABA was observed in the majority of samples (74% in central incisors and 86% in lateral incisors). In contrast, the labial ABA was decreased in 36% of central incisors and 40% of lateral incisors respectively, while it was increased in 55% of central incisors and 57% of lateral incisors. An average bone loss of 20.5 and 40.0% on the palatal side was observed in the central and lateral incisors respectively. Further statistical paired t-tests revealed that reduction in the palatal ABA of the central and lateral incisors was statistically significant (P < 0.001), while no difference was observed in the labial side (P > 0.05) (Fig. 2, Table 5).

Scatterplots showing the changes in alveolar bone area at T0 and T1

Characteristic changes in the alveolar bone during incisor retraction. a. Typical alteration in the alveolar bone at the central incisor with a massive palatal apex displacement, i.e. bodily movement; b. Typical alveolar bone remodeling at the central incisor with a large change in the inclination, i.e. tipping
Relationship between changes of labial ABA and tooth movement types
Among all 152 teeth, the apex of 38 (25%) teeth was moved toward labial side, while the remaining 114 (75%) was toward palatal side. In the meantime, the inclination of 26 (17.1%) teeth increased, whereas the remaining 126 (82.9%) decreased.
Four different ways of tooth movement were achieved through permutation and combination theory: labial apex displacement (+) & inclination increase (+), labial apex displacement (+) & inclination decrease (−), palatal apex displacement (−) & inclination increase (+), and palatal apex displacement (−) & inclination decrease (−). Among them, there was no labial apex displacement (+) & inclination increase (+) in the subjects. Pearson’s Chi-square test was applied to determine whether three ways of tooth movement affected the labial ABA before and after treatment, which showed a strong correlation between labial ABA changes and tooth movement type (P < 0.001) (Table 6). Labially-displaced apex was correlated with decreased labial ABA, while palatally-displaced apex was correlated with increased labial ABA.
Relationship between changes of palatal ABA and tooth movement types
As a reduction in palatal ABA was observed in most patients (Fig. 3), a multivariate linear regression analysis was used to further explore the relationship between alterations of palatal ABA and tooth movement type, showing that the changes (T1-T0) of palatal ABA were remarkably correlated with the apex displacement and changes of inclination (T1-T0) before and after treatment (F = 107.9, P < 0.001) (Table 7). This model can be also described by using this equation: Changes of palatal ABA (T1-T0) = − 3.3- 0.1× changes of inclination (T1-T0) + 2.5× apex displacement (T1-T0) (Table 7).
The equation can be used to predict changes of palatal ABA with certain values of the predictors. For example, the predicted changes of palatal ABA for a patient with palatal apex displacement of − 3 mm and decrease of 8° in inclination is − 3.3-0.1× (− 8) + 2.5× (− 3), which equals to − 7.5 mm2.
Discussion
Periodontal health is of great concern for the orthodontists and periodontists, especially in the inter-disciplinary management of bimaxillary protrusion patients [18]. Since protrusive lips is one chief complaint of patients seeking orthodontic treatment in the Eastern Asian community, four bicuspid extraction was commonly utilized to correct dental and lip protrusion [2]. The principal finding of the present research was that mass retraction of maxillary incisors leaded to a significant reduction in the ABA on the palatal side, and apex displacement is the major factor that contributed to decreased palatal ABA. Moreover, multiple line regression indicated an equation to potentially predicate alveolar bone resorption on the palatal side by integrating apex displacement and changes in the inclination of incisors. Therefore, the null hypotheses were rejected.
Dentists have been seeking personalized approaches to improve treatment outcome and avoid deleterious sequelae for a long time [19]. The new era of precision medicine requires a personalized, or individualized treatment plan and case management [20]. The use of digital orthodontic setups has grown quickly to aid individualized plan, mimic tooth movement and predict treatment outcome [21]. Three-dimensional CBCT imaging have exponentially enhanced the capability to evaluate regional anatomy in the alveolar process and assess periodontal risks during tooth movement [7].
Alveolar bone, which originates from the dental follicle during embryogenesis, is unique in its dynamic remodeling capacity during tooth eruption and OTM [7]. It has been long accepted that OTM is a dynamic process whereby the application of orthodontic force induces bone resorption on the pressure side and bone apposition on the tension side, which maintains structural integrity of the alveolar bone [8]. Although the alveolar bone might be dynamically remodeled to house moving teeth in growing adolescents, OTM is limited by the cortical plates of the alveolus at the level of the incisor apices, which can be regarded as “orthodontic walls”, in non-growing adults [5]. Moving teeth out of these boundaries may lead to occurrence of severe iatrogenic sequelae of alveolar bone resorption, and this is especially disastrous in adult patients [5, 22]. The width of the anterior palate at the level of the apex remained unaltered despite long-term incisor retraction in adult patients [23]. Indeed, we observed significant decrease in the height, thickness and area of alveolar bone on the palatal side.
The acumen of CBCT may help orthodontists and periodontists assess periodontal bone status and remodeling in OTM [7]. Stages of alignment, bite opening and space closing are integrated processes in extraction cases. It has been demonstrated that alignment of anterior teeth by tipping leaded to significant vertical and horizontal loss of alveolar bone in non-extraction cases [24,25,26]. In addition, Yodthong et al. investigated the effect of incisor retraction on changes of alveolar bone. CBCT was taken before retraction and after 6 months of retraction. They reported an increase of 0.4 mm in ABT at the crestal level on the labial side, 0.2 mm and 0.6 mm decrease at crestal and apical level on the palatal side respectively for the central incisors, indicating that incisor retraction is a risk of alveolar bone resorption in bimaxillary protrusion patients. However, the total thickness of the alveolar bone even increased an average of 0.6 mm at the apical level [27]. Sarikaya et al. reported that no changes in the labial side were observed, while decrease in ABT in the maxillary arch was observed in four premolar extraction cases with 0.7 mm and 1.2 mm at the crestal and mid-root level [4]. Our results were consistent with Ahn et al. that remarkable bone absorption can be found in all three levels on the palatal side, while bone thickness on the labial side increased in the middle third, by 0.27 mm for upper central incisors and by 0.65 mm for lateral incisors, with statistically significant differences [14].
In the process of assessing the periodontal risk, dentists should not only evaluate anatomic features of alveolar bone before treatment, but also the remodeling potential and 3-dimensional position of targeted teeth in the alveolus [28]. 3D imaging techniques may help orthodontic-periodontal interdisciplinary coordination in managing periodontal iatrogenic effects [29]. Consistent absorption of alveolar bone on the palatal side in our study and in Ahn et al. [14] indicates that retraction actually moves incisors “through-the-bone”. Despite the increase in alveolar bone thickness and area on the buccal side, decrease in the total thickness and area in the incisor region suggests that orthodontic treatment may lead to increased risks for periodontal sequelae.
Digital setups have been widely used for diagnosis, treatment planning, indirect bonding, simulating treatment, and designing and producing orthodontic appliances, especially in the aligner techniques [21, 30, 31]. Much emphasis has been laid on crown position rather than root position because spatial position of roots is not available until the emergence of CBCT imaging and roots are usually not directly related to esthetics and occlusal contact [32]. However, if the alveolar bone is not taken into consideration, such digital setup may push the tooth out of the bone for considerable distance. Our present data suggest that without taking the alveolar bone remodeling into consideration, 3D Digital setups, especially in aligners, may push the teeth out of the bone boundary.
Both the height and thickness of alveolar bone are critical factors to protect the teeth from plaque-induced (i.e., periodontitis) and non-plaque-induced gingival lesions [33]. Thinner alveolar wall after incisor retraction may lead to dehiscences or fenestrations that compromise alveolar bone support [17]. In order to investigate overall effect of incisor retraction on alveolar remodeling, we made a preliminary attempt to describe changes in alveolar bone area, which reflected changes in ABL and ABT; we found that apical displacement and alterations in inclination were significantly related to ABA on the palatal side; moreover, we developed an equation to describe changes in ABA, which described that changes of palatal ABA (T1-T0) is equal to (− 3.258–0.139× changes of inclination (T1-T0) + 2.533 × apex displacement (T1-T0)).
We utilized changes in the inclination of each individual incisor rather than measurements from cephalometric to generate an equation for prediction of individual palatal ABA. Such equation may customize both periodontal and orthodontic consideration in adult patients, especially determining whether bone augmentation surgery was needed to aid orthodontic therapy, commonly recognized as surgically facilitated orthodontic therapy [SFOT] [34] or periodontally accelerated osteogenic orthodontics [PAOO]) [35]. Our present equation further supports the conception that bodily retraction would lead to proximity of root apex to palatal cortical plate and extensive alveolar bone resorption [36], and this jeopardy is particularly pertinent in adults as numbers and regeneration capability of osteoblasts in the periosteum reduces with aging [37]. Therefore, clinicians should not design bodily movement of a large distance to avoid placing the teeth out of the bone boundary during treatment planning.
Many factors may influence OTM and alveolar bone remodeling in the periodontium, such as force magnitude (light or heavy), force type (intermittent, interrupted or continuous), age(adolescents or adults), distance of movement, type of OTM (tipping, controlled tipping, translation, intrusion, extrusion), speed of space closure [27]. For example, intrusion of incisors into a wider alveolus may increase alveolar bone support, thereby compensating the palatal bone resorption [38]; however, excessive intrusion may lead to remarkable root resorption [39]. Cortical plates at the root apex level did not remodel in adult patients [5]; therefore, it may be utilized as a reliable mark to reflect the position of incisors. In our present study, we did not measure the distance of retraction for individual teeth, because the distance of root apex to palatal plates and inclination of incisors actually reflected changes in the position of incisors. Another issue was that we did not include the vertical position of root apex. Only minimal intrusion of incisors can be observed during retraction of incisors in bimaxillary protrusion patients [27], and large quantities of incisor intrusion can only be observed in class II patients, especially division 2 type with reverse curve of Spee [40]. Data from the 2-dimensional changes in the lateral cephalograms were most often utilized to represent overall intrusion [27, 40, 41]; therefore, we did not further investigate influence of intrusion of incisor in 2-dimensional cephalometric on ABA.
We utilized adult patients to minimize the influence of growth on alveolar bone remodeling; therefore, interpretation of data in adolescents should be cautious. A key question critical in alveolar bone remodeling during OTM is elasticity and flexibility of alveolar bone, which undergoes rapid remodeling with low mineralization and stiffness even in adults [42]. More CBCT data, especially from growing subjects, are needed to better predict changes in the periodontium and optimize periodontal risk assessment [25]. A pre- and post-CBCT may be taken in cases who need mass incisor retraction, in order to assess potential periodontal risks such as fenestrations and dehiscence and provide individualized suggestion for long term periodontal maintenance for each subject after treatment. Clinicians should not be blinded to the periodontal sequalae induced by mass retraction, although soft tissue may hide severe bone resorption, fenestration and dehiscence on the palatal side [43]. Moreover, patients should be informed of their periodontal situation, since such severe bone loss may be disastrous once the patient lose the teeth due to trauma or periapical diseases [44].
Currently, data regarding long-term alveolar bone remodeling after retention is not available except one case report [45]. In the case report, significant alveolar bone formation was observed on the palatal side of the maxillary incisors 10 years after retention [45]. Long-term studies are needed to confirm the alveolar bone apposition on the palatal side, and to improve the predication of alveolar bone remodeling in our equation.
Although CBCT may reduce periodontal risks in OTM, ALARA (As Low As Reasonably Achievable) principle should be adhered to, especially in growing adolescents. Each subject should be evaluated individually based on their unique treatment needs and set of circumstances [7]. Digital set-up provides dentists unprecedented opportunities to predict the final position of the crowns before the treatment [46]. Our present research indicated that with the help of CBCT imaging, dentists may further predict the final root position in the alveolus in the future.
The accuracy of CBCT imaging is closely related to voxel size. A smaller voxel size such as 0.2 mm provides a superior accuracy compared to a size of 0.4 mm in assessing the alveolar bone and soft tissues [47]. However, the patients are exposed to a higher dose of ionizing radiation under the condition of a smaller voxel size [26]. Indeed, a FOV of 16 × 16 cm and a voxel size of 0.3 mm used in this study may compromise the accuracy in assessing the alveolar bone. The approximate effective dose of 80 μSv in our present study, which was similar to the study of Pauwels et al. [48], may reduce the radiation risks under a lower voxel size.
We utilized the predominant vision-based method to discriminate dental structures in the dental literatures. Such vision-based method has been widely adopted to study the alveolar bone [47], temporomandibular joint [49], and airway space [50], and it is time-efficient. However, conventional vision-based method may be less accurate and reproducible when compared to gray value–assisted method proposed [10].
We only included adult cases in the present study, which partially explain the small sample size. Further long-term prospective studies including follow-up observation and studies in adolescents may bring us more information on the periodontal remodeling during orthodontic treatment.
Conclusions
-
1.
Retraction of incisors in bimaxillary protrusion patients leaded to significant bone resorption on the palatal side, which may compromise periodontal bone support;
-
2.
Palatal displacement of root apex was highly correlated with palatal bone resorption;
-
3.
The area of bone resorption might be predicted by an equation that incorporated the displacement of root apex and changes in the incisor inclination;
-
4.
The equation in predicating area of alveolar bone may reduce the risks of placing the teeth out of the bone boundary during 3D digital setups.
Availability of data and materials
The raw data in this study are available by contacting corresponding author Dr. Lang Lei, China-Email address: leilangdental@163.com.
Abbreviations
- CBCT:
-
Cone-beam computed tomography
- ABT:
-
Alveolar bone thickness
- ABH:
-
Alveolar bone height
- ABA:
-
Alveolar bone area
- OTM:
-
Orthodontic tooth movement
- SWA:
-
Straight wire appliances
- TADs:
-
Temporary anchorage devices
- CEJ:
-
Cementoenamel junction
- FH plane:
-
Frankfort horizontal plane
References
Leonardi R, Annunziata A, Licciardello V, Barbato E. Soft tissue changes following the extraction of premolars in nongrowing patients with bimaxillary protrusion. A systematic review. Angle Orthod. 2010;80(1):211–6.
Solem RC, Marasco R, Guiterrez-Pulido L, Nielsen I, Kim SH, Nelson G. Three-dimensional soft-tissue and hard-tissue changes in the treatment of bimaxillary protrusion. Am J Orthod Dentofac Orthop. 2013;144(2):218–28.
Wang Q, Jia P, Anderson NK, Wang L, Lin J. Changes of pharyngeal airway size and hyoid bone position following orthodontic treatment of class I bimaxillary protrusion. Angle Orthod. 2012;82(1):115–21.
Sarikaya S, Haydar B, Ciğer S, Ariyürek M. Changes in alveolar bone thickness due to retraction of anterior teeth. Am J Orthod Dentofac Orthop. 2002;122(1):15–26.
Wainwright WM. Faciolingual tooth movement: its influence on the root and cortical plate. Am J Orthod. 1973;64(3):278–302.
Wehrbein H, Fuhrmann RA, Diedrich PR. Periodontal conditions after facial root tipping and palatal root torque of incisors. Am J Orthod Dentofac Orthop. 1994;106(5):455–62.
Mandelaris GA, Neiva R, Chambrone L. Cone-beam computed tomography and interdisciplinary Dentofacial therapy: an American Academy of periodontology best evidence review focusing on risk assessment of the Dentoalveolar bone changes influenced by tooth movement. J Periodontol. 2017;88(10):960–77.
Meikle MC. The tissue, cellular, and molecular regulation of orthodontic tooth movement: 100 years after Carl Sandstedt. Eur J Orthod. 2006;28(3):221–40.
Singh S, Jayan B. Comparative evaluation of Periodontally accelerated Osteogenic orthodontics (PAOO) versus conventional orthodontic tooth movement in adult patients with Bimaxillary Dentoalveolar protrusion. Int J Periodontics Restorative Dent. 2019;39(4):571–7.
Padala S, Tee BC, Beck FM, Elias K, Kim DG, Sun Z. The usefulness of cone-beam computed tomography gray values for alveolar bone linear measurements. Angle Orthod. 2018;88(2):227–32.
Damstra J, Fourie Z, Huddleston Slater JJ, Ren Y. Accuracy of linear measurements from cone-beam computed tomography-derived surface models of different voxel sizes. Am J Orthod Dentofacial Orthop. 2010; 137(1):16.e1–6; discussion 16-7.
Tominaga JY, Tanaka M, Koga Y, Gonzales C, Kobayashi M, Yoshida N. Optimal loading conditions for controlled movement of anterior teeth in sliding mechanics. Angle Orthod. 2009;79(6):1102–7.
Krieger E, Seiferth J, Saric I, Jung BA, Wehrbein H. Accuracy of Invisalign® treatments in the anterior tooth region. First results. J Orofac Orthop. 2011;72(2):141–9.
Ahn HW, Moon SC, Baek SH. Morphometric evaluation of changes in the alveolar bone and roots of the maxillary anterior teeth before and after en masse retraction using cone-beam computed tomography. Angle Orthod. 2013;83(2):212–21.
Domingo-Clérigues M, Montiel-Company JM, Almerich-Silla JM, García-Sanz V, Paredes-Gallardo V, Bellot-Arcís C. Changes in the alveolar bone thickness of maxillary incisors after orthodontic treatment involving extractions - a systematic review and meta-analysis. J Clin Exp Dent. 2019;11(1):e76–76e84.
Kim KW, Kim SJ, Lee JY, Choi YJ, Chung CJ, Lim H, et al. Apical root displacement is a critical risk factor for apical root resorption after orthodontic treatment. Angle Orthod. 2018;88(6):740–7.
Vardimon AD, Oren E, Ben-Bassat Y. Cortical bone remodeling/tooth movement ratio during maxillary incisor retraction with tip versus torque movements. Am J Orthod Dentofac Orthop. 1998;114(5):520–9.
Fuhrmann R. Three-dimensional interpretation of periodontal lesions and remodeling during orthodontic treatment. Part III. J Orofac Orthop. 1996;57(4):224–37.
Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol. 2000. 2018;78(1):7–11.
Flores M, Glusman G, Brogaard K, Price ND, Hood L. P4 medicine: how systems medicine will transform the healthcare sector and society. Per Med. 2013;10(6):565–76.
Fabels LN, Nijkamp PG. Interexaminer and intraexaminer reliabilities of 3-dimensional orthodontic digital setups. Am J Orthod Dentofac Orthop. 2014;146(6):806–11.
Matsumoto K, Sherrill-Mix S, Boucher N, Tanna N. A cone-beam computed tomographic evaluation of alveolar bone dimensional changes and the periodontal limits of mandibular incisor advancement in skeletal Class II patients. Angle Orthod. 2020.
Handelman CS. The anterior alveolus: its importance in limiting orthodontic treatment and its influence on the occurrence of iatrogenic sequelae. Angle Orthod. 1996;66(2):95–109; discussion 109-10.
Garlock DT, Buschang PH, Araujo EA, Behrents RG, Kim KB. Evaluation of marginal alveolar bone in the anterior mandible with pretreatment and posttreatment computed tomography in nonextraction patients. Am J Orthod Dentofac Orthop. 2016;149(2):192–201.
Lund H, Gröndahl K, Gröndahl HG. Cone beam computed tomography evaluations of marginal alveolar bone before and after orthodontic treatment combined with premolar extractions. Eur J Oral Sci. 2012;120(3):201–11.
Morais JF, Melsen B, de Freitas K, Castello Branco N, Garib DG, Cattaneo PM. Evaluation of maxillary buccal alveolar bone before and after orthodontic alignment without extractions: a cone beam computed tomographic study. Angle Orthod. 2018;88(6):748–56.
Yodthong N, Charoemratrote C, Leethanakul C. Factors related to alveolar bone thickness during upper incisor retraction. Angle Orthod. 2013;83(3):394–401.
Lee RJ, Weissheimer A, Pham J, Go L, de Menezes LM, Redmond WR, et al. Three-dimensional monitoring of root movement during orthodontic treatment. Am J Orthod Dentofac Orthop. 2015;147(1):132–42.
Hodges RJ, Atchison KA, White SC. Impact of cone-beam computed tomography on orthodontic diagnosis and treatment planning. Am J Orthod Dentofac Orthop. 2013;143(5):665–74.
Grauer D, Proffit WR. Accuracy in tooth positioning with a fully customized lingual orthodontic appliance. Am J Orthod Dentofac Orthop. 2011;140(3):433–43.
Im J, Cha JY, Lee KJ, Yu HS, Hwang CJ. Comparison of virtual and manual tooth setups with digital and plaster models in extraction cases. Am J Orthod Dentofac Orthop. 2014;145(4):434–42.
Germane N, Bentley BE, Isaacson RJ. Three biologic variables modifying faciolingual tooth angulation by straight-wire appliances. Am J Orthod Dentofac Orthop. 1989;96(4):312–9.
Chan HL, Garaicoa-Pazmino C, Suarez F, Monje A, Benavides E, Oh TJ, et al. Incidence of implant buccal plate fenestration in the esthetic zone: a cone beam computed tomography study. Int J Oral Maxillofac Implants. 2014;29(1):171–7.
Roblee RD, Bolding SL, Landers JM. Surgically facilitated orthodontic therapy: a new tool for optimal interdisciplinary results. Compend Contin Educ Dent. 2009; 30(5):264–275; quiz 276, 278.
Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21(1):9–19.
Meikle MC. The dentomaxillary complex and overjet correction in class II, division 1 malocclusion: objectives of skeletal and alveolar remodeling. Am J Orthod. 1980;77(2):184–97.
Ferretti C, Lucarini G, Andreoni C, Salvolini E, Bianchi N, Vozzi G, et al. Human periosteal derived stem cell potential: the impact of age. Stem Cell Rev. 2015;11(3):487–500.
Deng Y, Sun Y, Xu T. Evaluation of root resorption after comprehensive orthodontic treatment using cone beam computed tomography (CBCT): a meta-analysis. BMC Oral Health. 2018;18(1):116.
de Almeida MR, Marçal A, Fernandes T, Vasconcelos JB, de Almeida RR, Nanda R. A comparative study of the effect of the intrusion arch and straight wire mechanics on incisor root resorption: a randomized, controlled trial. Angle Orthod. 2018;88(1):20–6.
Kale Varlık S, Onur AÖ, Türköz Ç. Deepbite correction with incisor intrusion in adults: a long-term cephalometric study. Am J Orthod Dentofac Orthop. 2013;144(3):414–9.
Ng J, Major PW, Heo G, Flores-Mir C. True incisor intrusion attained during orthodontic treatment: a systematic review and meta-analysis. Am J Orthod Dentofac Orthop. 2005;128(2):212–9.
Cho MI, Garant PR. Development and general structure of the periodontium. Periodontol 2000. 2000;24:9–27.
Sheng Y, Guo HM, Bai YX, Li S. Dehiscence and fenestration in anterior teeth : comparison before and after orthodontic treatment. J Orofac Orthop. 2020;81(1):1–9.
Kher U, Tunkiwala A, Umrigar Z. Management of Fenestration Defects during Flapless Immediate Implant Placement in the esthetic zone. Int J Periodontics Restorative Dent. 2015;35(6):e90–6.
Bae SM, Kim HJ, Kyung HM. Long-term changes of the anterior palatal alveolar bone after treatment with bialveolar protrusion, evaluated with computed tomography. Am J Orthod Dentofac Orthop. 2018;153(1):108–17.
Staderini E, Guglielmi F, Cornelis MA, Cattaneo PM. Three-dimensional prediction of roots position through cone-beam computed tomography scans-digital model superimposition: a novel method. Orthod Craniofac Res. 2019;22(1):16–23.
Wood R, Sun Z, Chaudhry J, Tee BC, Kim DG, Leblebicioglu B, et al. Factors affecting the accuracy of buccal alveolar bone height measurements from cone-beam computed tomography images. Am J Orthod Dentofac Orthop. 2013;143(3):353–63.
Pauwels R, Beinsberger J, Collaert B, Theodorakou C, Rogers J, Walker A, et al. Effective dose range for dental cone beam computed tomography scanners. Eur J Radiol. 2012;81(2):267–71.
Hilgers ML, Scarfe WC, Scheetz JP, Farman AG. Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am J Orthod Dentofac Orthop. 2005;128(6):803–11.
Weissheimer A, Menezes LM, Sameshima GT, Enciso R, Pham J, Grauer D. Imaging software accuracy for 3-dimensional analysis of the upper airway. Am J Orthod Dentofac Orthop. 2012;142(6):801–13.
Acknowledgements
The authors are grateful to our dedicated colleagues, especially Dr. Jun Ji and Dr. Zitong Lin, at the Nanjing Stomatological Hospital, Medical School of Nanjing University for the support of present study.
Author details
Huimin Mao, Andi Yang, Yue Pan & Lang Lei are from Department of Orthodontics, Nanjing Stomatological Hospital, Medical School of Nanjing University, Nanjing, China; Houxuan Li is from Department of Periodontics, Nanjing Stomatological Hospital, Medical School of Nanjing University, Nanjing, China.
Funding
This research is supported by Nanjing Medical Science and technique Development Foundation (QRX17081 and QRX17025), National Natural Science Foundation of China (81670996). The funding body supported data analysis and writing the manuscript.
Author information
Authors and Affiliations
Contributions
HL and LL developed the concept and design of this study. HM conducted data collection and measurement. HL and LL supervised the data assessment. HM, AY, and YP performed statistical analyses, and all authors contributed to the interpretation of the data. HM, AY, and YP drafted the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was evaluated and approved by the local ethics committee (Nanjing Stomatological Hospital, Medical School of Nanjing University, No. 2019NL-064(KS)). Written consent was obtained from participants or their parents (for participants less than 16 years old).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mao, H., Yang, A., Pan, Y. et al. Displacement in root apex and changes in incisor inclination affect alveolar bone remodeling in adult bimaxillary protrusion patients: a retrospective study. Head Face Med 16, 29 (2020). https://doi.org/10.1186/s13005-020-00242-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13005-020-00242-2