
Abstract
Background
Human anelloviruses (TTV, TTMDV and TTMV) are at high prevalence all across the globe, having also a controversial disease-inducing potential. This study aimed to estimate the prevalence of anelloviral DNA in the Romanian human population and to investigate the association of infections with common pathologies in Romanian population.
Methods
After informed consent, blood samples were collected from 2000 subjects represented by: clinically healthy individuals (n = 701) and a group of patients with pathologies linked to low grade inflammation or alteration of carbohydrate metabolism (n = 1299). All samples were analysed for the presence of TTV, TTMDV and TTMV DNA by hemi-nested PCR.
Results
The prevalence of TTV, TTMDV and TTMV in the studied population was 68.2, 54.4%, respectively 40.1%, lower than the recent reports from other geographic regions. The three viral species were significantly more frequent in the group of patients compared to the healthy subjects and were associated with type 2 diabetes mellitus. The presence of anelloviral DNA was also associated with medical procedures (e.g. haemodialysis/transfusions, surgical procedures) and previous hepatitis A virus infection. Lifestyle choices related to alcohol consumption, smoking, physical activity and living environment were not associated with differences in distribution of the three viruses.
Conclusion
Further evidence is needed to establish a correlation between infection with human anelloviruses and a pathology or group of pathologies.
Similar content being viewed by others


Background
Human anelloviruses, namely Torque teno virus (TTV), Torque teno mini virus (TTMV) and Torque teno midi virus (TTMDV) species are characterized by their staggering prevalence world-wide, generating conflicting views on their pathogenic potential.
The prevalence of TTV DNA in the blood of the general population reaches to 94–95% by the latest reports (Taiwan 95%, Russia 94%) [1, 2]. Reports of TTMDV and TTMV prevalence are heterogeneous and data regarding prevalence in the blood of healthy individuals are scarce. For TTMDV, the prevalence ranges between 14.5% in Iran [3] and 75% in Japan [4], while the prevalence of TTMV varies between 29% in Korea [5] and 84.8% in Japan [4].
Infection with TTV has been tested in order to link it with a wide range of human pathologies (e.g. hepatitis, cancer, haematological and autoimmune disorders - reviewed in [6]). In some studies only some subtypes of torque teno viruses were reported to be associated with human pathology were reported (e.g. TTMDV and TTMV were associated with respiratory diseases [4] and periodontitis [7]). Although the pathological mechanisms of anelloviruses are not fully understood, the latest studies have pointed out several mechanisms by which these viruses could evade and shape the immune response (activation of pro-inflammatory cytokine production TLR-9 [8], rendering infected lymphocytes resistant to immunomodulation by interferon [9]), thus leading to the worsening of pre-existent conditions. Nevertheless, human anelloviruses seem to be acquired early in childhood [4] being associated with respiratory diseases in children [10, 11].
The altered glucose metabolism and modified expression of interleukins were associated with developing a low grade chronic inflammation. Chronic inflammation appears to be a pathophysiological link between a number of common human diseases such as obesity, type 2 diabetes mellitus (T2DM), chronic periodontitis, hypertension and breast cancer [12,13,14]. Moreover, chronic periodontitis was strongly linked to obesity [15] and diabetes, being previously considered “the sixth complication of diabetes” [16]. Although the association of periodontitis with obesity is not well understood, it is believed that both are related to high levels of pro-inflammatory molecules (e.g. in the gingival crevicular fluids [17, 18]).
Whilst many studies assessed the association between anelloviruses and inflammation, as far as we are aware, there are few studies aiming to identify an association between the presence of human anelloviruses and breast cancer, as well as diabetes and its comorbidities (i.e. hypertension, obesity, and chronic periodontitis). Also, no studies have been conducted to evaluate aspects of lifestyle choices (e.g. smoking, alcohol consumption, physical activity) as potential factors involved in the epidemiology of anelloviral infections. Also, as far as we know, the human anelloviruses prevalence evaluation has not been attempted at a high scale in Romania before.
The aim of this study was to estimate the prevalence of anelloviral DNA in the Romanian human population and to establish an association with a group of pathologies which can exhibit chronic inflammation and/or alteration of carbohydrate metabolism.
Methods
A total number of 2000 subjects (701 clinically healthy individuals and 1299 patients with pathologies linked to a low grade inflammation or alteration of carbohydrate metabolism; male: female sex ratio 0.80; average age 45 ± 15.2 years) were selected and described in Table 1.
All participants gave their informed consent according to the Helsinki Declaration on ethical principles for medical research involving human subjects.
Clinical and paraclinical data and blood samples were collected from all subjects. Subjects were asked to estimate the frequency of physical exercise (no exercise, occasional exercise and regular exercise), smoking and alcohol consumption habits (non-smoker, former smoker, occasional smoker and smoker, respectively, non-drinker, former drinker, occasional drinker and drinker), number of births and surgical procedures.
Genomic DNA was isolated and purified according to the manufacturer’s recommendations from 250 μL of whole blood using a commercial kit (Wizard® Genomic DNA Purification Kit, Promega, WI, USA). TTV, TTMV and TTMDV DNA was identified using a hemi-nested PCR protocol described by Ninomiya et al. (2008) which amplifies a conserved sequence in the 5' UTR of the viral genome.
The first reaction of the hemi-nested PCR was carried out with GoTaq® Green Master Mix (Promega, WI, USA) in a total volume of 15 μL containing: 1X PCR buffer solution, 1.5 mM MgCl2, 0.2 mM dNTP mix, 0.5 μM of each primer (NG779, NG780, NG781 and NG782), 0.6 units of GoTaq® DNA-polymerase and 1.5 μL of genomic DNA. The second round of PCR consisted of three individual reactions using sets of primers specific for TTV (NG779, NG780 and NG785), TTMDV (NG795 and NG796) and, respectively TTMV (NG791, NG792, NG793 and NG794). One μL of PCR product from the first reaction was used as a template. The amplification programs and primer sequences were described by Ninomiya et al. (2008).
The amplification products of the second PCR reactions were resolved by agarose gel electrophoresis (2% w/v, 5 V/cm for 30 min) and visualized under UV light after ethidium bromide staining.
Negative and positive controls were used to validate PCRs. Samples were considered positive when an expected-size amplicon was generated.
Chi squared and Fisher exact test were used to examine possible differences in the incidence of infection among groups of subjects, while independent samples T-test and Kruskal-Wallis test were used to compare means. Odds Ratio was calculated using SPSS Statistics software v 20.0.0 (IBM). Bonferroni corrected alpha of 0.05 / 150 or ∼0.0003 was considered statistically significant. R version 3.3.3 [19] with the “ggplot2” package [20] was used to generate graphics.
MDR (Multifactor Dimensionality Reduction) software (v.2.0.beta 8.4) was used to perform the investigation of statistical epistasis between investigated variables. Best models implying combination of variables were considered based on 10-fold cross-validation and maximum testing accuracy.
Results
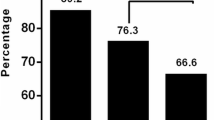
This study revealed the fact that the DNA of torque teno viruses was present in 71.5% of blood samples investigated, the prevalence of TTV, TTMDV and TTMV being 68.2, 54.4%, respectively 40.1%.
The distribution of all three viral species considered individually was significantly higher in patients compared to healthy individuals (p < 0.0003, Fig. 1).

Prevalence of TTV, TTMDV and TTMV DNA in the study group
No difference was noticed in the distribution of the three viruses in men and women participating in this study.
All three anelloviruses were similarly distributed in subjects stratified according to living areas, routine physical activity or alcohol consumption status, both in patients and in controls or also in subjects stratified according to gender.
The risk of achieving an anelloviral infection increases up to 2-fold (ORTTV = 1.8, 95% CI: 1.5–2.3; ORTTMDV = 2, 95% CI: 1.7–2.5; ORTTMV = 1.8, 95% CI: 1.5–2.2) by undergoing at least one surgery and it was higher among men in this group. Of subjects positive for TTV, TTMDV and TTMV DNA, a proportion of 76, 65.2% and, respectively, 47.8%, have undergone at least one surgical procedure (p < 0.0003, Table 2).
Human anelloviruses DNA was more frequently found in healthy women who have had at least one surgical abortion or caesarean section/vaginal birth (p < 0.0003). Also, the average number of such procedures was higher in women positive for TTV, TTMDV or TTMV DNA compared to those negative for such infections (independent samples T-Test p < 0.0003).
Higher prevalence of TTV, TTMDV or TTMV in overall patients and particularly in men (ORTTV = 2.1, 95% CI: 1.4–3.1; ORTTMDV = 2.4, 95% CI: 1.7–3.3; ORTTMV = 3.5, 95% CI: 2.5–4.8) was associated with a history of hepatitis A virus (HAV) infection (Table 2). Bivariate analysis performed with MDR also indicated an association between TTMV, history of HAV infection and haemodialysis (Table 3).
Regarding the association of human anelloviruses with pathology, no significant result was found linking the presence of anelloviral DNA with obesity and chronic periodontitis neither compared with controls, nor compared with normal weight subjects, respectively with periodontally healthy subjects. Likewise, there was no association between the BMI (independent samples T-test > 0.05) and the presence or absence of TTMDV, TTMV or TTV DNA.
The prevalence of anelloviral DNA was significantly higher in patients with hypertension compared with controls (TTV – 74.2% vs. 58.4%; TTMDV – 59.6% vs. 46.3%; TTMV – 46.4% vs. 32.1%).
The distributions of TTV, TTMDV and TTMV presented significant differences between T2DM group compared to healthy subjects (OR = 1.8 - to 2.1, p < 0.0003) (Table 4).
The analysis of co-infection patterns showed that triple co-infection was more frequent in patients with diabetes (both T1DM and T2DM) compared to healthy subjects (p < 0.0003). The presence of only TTV and TTMDV DNA was significantly more frequent in patients with breast cancer (p < 0.0003) compared with healthy women (Fig. 2).

Co-infection pattern distribution of human anelloviruses in overall patients grouped by pathology. *p < Bonferroni corrected alpha = 0.0003
The analysis of viral DNA distribution among age groups revealed similar patterns for all the three viruses. Human anelloviruses’ prevalence appears to increase with age with a lower point in the 41–50 years group and the highest peak in the over 61 year group (Fig. 3). Nevertheless, there was no significant difference in the frequency of TTV, TTMDV or TTMV DNA between other decades of age.

Age group distribution of TTV (a, a’), TTMDV (b, b’) and TTMV DNA (c, c’) stratified by status (top row) and by gender (bottom row) in the overall study group
A significantly higher number of patients within the 21–30 years age group were found positive for TTMV DNA compared to the same age healthy controls (p = 0.000031). The significance of this difference is to be further investigated.
The univariate MDR analysis confirmed the obtained results. The bivariate MDR analysis (Table 3) showed that the presence of TTV, TTMDV, TTMV, or at least of one of the viruses is associated with the combination of disease states or particular states (e.g. the presence of at least one anellovirus was associated with the number of surgical procedures and the presence of comorbidities in women).
Discussion
The prevalence of anelloviral DNA in the overall studied population was 71.5%. Results of this study showed lower values of anelloviruses DNA presence compared to a recent study from Qatar enrolling patients co-infected with HBV and HCV and healthy individuals [21]. Moreover, prevalence values found in the healthy group observed in this study were lower than values reported for only the control group in the study from Qatar (TTV 83.4% vs. 58.5%; TTMDV 74.6% vs. 46.4%; TTMV 62.1% vs. 32.1%). Also, our results are different from those reported for TTV DNA prevalence in healthy individuals of eastern Taiwanese indigenes (95% vs. 58.5%) [1]. Prevalence of viral DNA observed in this study is similar to previous data reported in the saliva of healthy individuals from Romania in 2013 [22]. These results may indicate a possible geographical stratification of anellovirus frequency.
Human anelloviruses have several routes of transmission, including blood [6]. Childbirth or medical procedures that imply open wounds (i.e. various surgical procedures) represent potential gateways for anelloviral particles access into the blood stream; whilst there are no studies to support this theory, in our study significantly higher rates of anelloviral DNA (Table 2) were found in subjects that underwent these procedures. The incidence of TTV DNA in patients undergoing haemodialysis reported by this study (90.6%), all part of the T2DM group, was higher compared to dialyzed patients from Brazil (17–36%) [23] and France (54%) [24]; however the discrepancy can be explained also by the different protocols used for molecular detection of viral DNA. For the patients undergoing haemodialysis (T2DM with chronic renal failure) the significantly higher prevalence of anelloviral DNA can be partially explained by this medical procedure. In addition, another study found that transgenic mice expressing the capsid protein of TTV (encoded by ORF1) showed renal failure resembling nephrotic syndrome [25]. Our data showed TTV, TTVD and TTMV DNA presence in T2DM patients increased up to 4-fold (ORTTV = 4.2, 95% CI: 2.4–7.7; ORTTMDV = 3.6, 95% CI: 2.4–5.4; ORTTMV = 4.1, 95% CI: 2.9–5.9) the association with chronic renal failure compared to T2DM patients negative for viral DNA (p < 0.0003); considering these results and previous reports, anellovirus infections may be one of the factors associated with the progression of diabetic nephropathy or with the medical procedures that these patients have undergone.
Evidence showed that TTV has the ability to modulate the response to interferon and to alter the expression of several cytokines [8, 9], thus changing the immune reactivity of the host. Altered expression of pro-inflammatory cytokines predispose to chronic inflammation (which sometimes is represented by persistent, low grade inflammation) which predispose to metabolic dysfunction and may increase the mutation rate [26]. Thus, chronic low grade inflammation was strongly linked to obesity, metabolic syndrome, insulin resistance, hypertension, T2DM [12], chronic periodontitis [17, 18] and some types of breast cancer [14].
TTV DNA was more prevalent among obese women without other comorbidities (Pearson’s Chi squared p = 0.024); also BMI of individuals positive for TTV DNA was overall higher than the BMI of TTV DNA-negative individuals (independent sample T-test p = 0.03), nevertheless both observations failed to reach statistical significance following Bonferroni correction. These findings could support and come in addition to previous reports of TTV DNA being more frequent with borderline statistical significance (p = 0.046) in obese women compared to matched controls [27].
Human anelloviruses exhibit an apparent pan-tropism [6] and its main multiplication cellular component occurs in the T lymphocyte [28]. Findings revealed that the presence of TTV DNA in the gingival tissue is associated with periodontitis [29]. Also, a recent study showed novel species of TTMV associated with periodontitis (p = 0.032) [7]. Our results revealed rather the percentage of TTV DNA being higher only in female subjects with periodontitis (pTTV = 0.028). Part of the result may be explained by the fact that women with periodontitis may have several confounding factors [e.g. they have had more surgeries (p < 0.001), at least a birth (p = 0.005) or haemodialysis or transfusions (p = 0.002)]; these attributes were associated with higher prevalence of human anelloviruses in this study. Also, the age of women with periodontitis was higher than periodontally healthy women (average 51.2 vs. 43.5; independent samples T-test p < 0.001).
TTV, TTMDV or TTMV DNA was significantly more prevalent in T2DM patients with frequencies of 75, 61.8% respectively 50.3%, while only TTMDV and TTMV DNA was more prevalent in T1DM compared with healthy subjects (Table 4). Anelloviral DNA was more common in patients with hypertension; however, 64.2% of these also had T2DM.
Information regarding the prevalence of human anelloviruses in diabetic patients is limited. Earlier studies reported lower prevalence for TTV DNA in T2DM patients, of 26% (16/60) [30] and 54.7% [24]. Only the second study observed a different distribution of TTV DNA in diabetics vs. control group. Given the complexity of the T2DM group, statistical analysis was performed considering all possible attributes (comorbidities); the prevalence of the three anelloviruses considered individually, as well as triple co-infections were significantly higher in diabetic patients compared to healthy individuals. However, compared with diabetic patients without comorbidities, no significant result was found. This result suggests that comorbidities such as hypertension, obesity or periodontitis do not influence the frequency of human anellovirus infections in T2DM patients. Interestingly, the age of T2DM patients with infections was higher than that of uninfected patients (average age 57.2 vs. 55.7, T-test p = 0.004), supporting the observation that incidence of anelloviral infections increases with age.
De Villieres et al. [31] suggested that active infection with TTV promotes a state of chronic inflammation that may contribute as a risk factor for cancer evolution; moreover, the microenvironment of the host cell may impact the viral genome by replication rates or mutation that could lead to the expression of viral proteins with impact on the oncogenic potential. Breast cancer patients from the present study had higher prevalence of TTV and TTMDV DNA compared to healthy women (p < 0.0033), as well as the highest rate of TTV and TTMDV co-infection, thus supporting the association between infection with TTV and breast cancer.
The association of different pathologies taken into study with a higher prevalence of TTV, TTMDV, TTMV or different combinations of anelloviruses support the theory that human anelloviruses have different biological behaviour and play distinct roles in pathogenesis and disease, as stated in another study [32].
Further investigation is needed to establish a correlation between prevalence of human anelloviruses and a pathology or group of pathologies.
The distribution of TTV, TTMDV and TTMV DNA in both clinically healthy individuals and patients, men and women, was similarly distributed among age groups and followed almost a tangential curve with the lowest point in the 18–20 age group, an inflection point in the 41–50 year age group and the highest point in the over 61 year age group (Fig. 3). Overall, the number of subjects positive for viral DNA increased with age. This observation comes in support for other studies that reported higher rates of TTV DNA with age [33, 34].
Conclusions
The prevalence of overall human anelloviruses in the Romanian population was 71.5%, lower than data reported for other regions, thus supporting the geographic stratification of infections with torque teno viruses. TTV was the most prevalent (68.2%) of the three anelloviral species, as reported in most studies.
The distribution of the three viral species was significantly higher in the overall group of patients compared to healthy subjects. The presence of TTV, TTMDV and TTMV was associated with diabetes mellitus and breast cancer.
Current data indicate that torque teno viruses act more likely like an aggravating factor in the evolution of diseases with an inflammatory background, or as an opportunistic agent in people with different medical conditions.
Abbreviations
- HAV:
-
hepatitis A virus
- MDR:
-
Multifactor Dimensionality Reduction
- OR:
-
Odds Ratio
- T1DM:
-
Type 1 Diabetes Mellitus
- T2DM:
-
Type 2 Diabetes Mellitus
- TTMDV:
-
Torque teno midi virus
- TTMV:
-
Torque teno mini virus
- TTV:
-
Torque teno virus
References
Hsiao KL, Wang LY, Lin CL, Liu HF. New phylogenetic groups of torque Teno virus identified in eastern Taiwan indigenes. PLoS One. 2016;11(2):e0149901.
Vasilyev EV, Trofimov DY, Tonevitsky AG, Ilinsky VV, Korostin DO, Rebrikov DV. Torque Teno virus (TTV) distribution in healthy Russian population. Virol J. 2009;6:134.
Fatholahi M, Bouzari M. Torque Teno midi virus/small Anellovirus in sera of healthy, HIV/HCV and HIV infected individuals in Lorestan Province, Iran. Jundishapur J Microbiol. 2015;8(11):e25368.
Ninomiya M, Takahashi M, Nishizawa T, Shimosegawa T, Okamoto H. Development of PCR assays with nested primers specific for differential detection of three human anelloviruses and early acquisition of dual or triple infection during infancy. J Clin Microbiol. 2008;46(2):507–14.
Han TH, Chung JY. Detection of small Anellovirus DNA from blood products. The Korean Society of Blood Transfusion. 2006;17(2):126–34.
Spandole S, Cimponeriu D, Berca LM, Mihaescu G. Human anelloviruses: an update of molecular, epidemiological and clinical aspects. Arch Virol. 2015;160(4):893–908.
Zhang Y, Li F, Shan TL, Deng X, Delwart E, Feng XP. A novel species of torque Teno mini virus (TTMV) in gingival tissue from chronic periodontitis patients. Sci Rep. 2016;6:26739.
Rocchi J, Ricci V, Albani M, Lanini L, Andreoli E, Macera L, Pistello M, Ceccherini-Nelli L, Bendinelli M, Maggi F. Torquetenovirus DNA drives proinflammatory cytokines production and secretion by immune cells via toll-like receptor 9. Virology. 2009;394(2):235–42.
Kincaid RP, Burke JM, Cox JC, de Villiers EM, Sullivan CS. A human torque Teno virus encodes a microRNA that inhibits interferon signaling. PLoS Pathog. 2013;9(12):e1003818.
Pifferi M, Maggi F, Caramella D, De Marco E, Andreoli E, Meschi S, Macchia P, Bendinelli M, Boner AL. High torquetenovirus loads are correlated with bronchiectasis and peripheral airflow limitation in children. Pediatr Infect Dis J. 2006;25(9):804–8.
Pifferi M, Maggi F, Di Cristofano C, Cangiotti AM, Nelli LC, Bevilacqua G, Macchia P, Bendinelli M, Boner AL. Torquetenovirus infection and ciliary dysmotility in children with recurrent pneumonia. Pediatr Infect Dis J. 2008;27(5):413–8.
Maldonado-Ruiz R, Montalvo-Martinez L, Fuentes-Mera L, Camacho A. Microglia activation due to obesity programs metabolic failure leading to type two diabetes. Nutrition & diabetes. 2017;7(3):e254.
Kyrgiou M, Kalliala I, Markozannes G, Gunter MJ, Paraskevaidis E, Gabra H, Martin-Hirsch P, Tsilidis KK. Adiposity and cancer at major anatomical sites: umbrella review of the literature. BMJ. 2017;356:j477.
Divella R, De Luca R, Abbate I, Naglieri E, Daniele A. Obesity and cancer: the role of adipose tissue and adipo-cytokines-induced chronic inflammation. J Cancer. 2016;7(15):2346–59.
Dalla Vecchia CF, Susin C, Rosing CK, Oppermann RV, Albandar JM. Overweight and obesity as risk indicators for periodontitis in adults. J Periodontol. 2005;76(10):1721–8.
Preshaw PM, Alba AL, Herrera D, Jepsen S, Konstantinidis A, Makrilakis K, Taylor R. Periodontitis and diabetes: a two-way relationship. Diabetologia. 2012;55(1):21–31.
Ylostalo P, Suominen-Taipale L, Reunanen A, Knuuttila M. Association between body weight and periodontal infection. J Clin Periodontol. 2008;35(4):297–304.
Akram Z, Abduljabbar T, Abu Hassan MI, Javed F, Vohra F. Cytokine profile in chronic periodontitis patients with and without obesity: a systematic review and meta-analysis. Dis Markers. 2016;2016:4801418.
Team RC. A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2013.
Wickham H. ggplot2: elegant graphics for data analysis. New York: Springer-Verlag; 2009.
Al-Qahtani AA, Alabsi ES, AbuOdeh R, Thalib L, Nasrallah GK. Prevalence of anelloviruses (TTV, TTMDV, and TTMV) in healthy blood donors and in patients infected with HBV or HCV in Qatar. Virol J. 2016;13(1):208.
Spandole S, Cimponeriu D, Toma M, Radu I, Ion D. Rapid detection of human torque Teno viruses using high-resolution melting analysis. Balkan journal of medical genetics : BJMG. 2013;16(1):55–62.
Takemoto AY, Okubo P, Saito PK, Yamakawa RH, Watanabe MA, Verissimo da Silva Junior W, Borelli SD, Bedendo J. Torque Teno virus among dialysis and renal-transplant patients. Brazilian J Microbiol : [publication of the Brazilian Society for Microbiology]. 2015;46(1):307–11.
Touinssi M, Gallian P, Biagini P, Attoui H, Vialettes B, Berland Y, Tamalet C, Dhiver C, Ravaux I, De Micco P, et al. TT virus infection: prevalence of elevated viraemia and arguments for the immune control of viral load. J Clin Virol. 2001;21(2):135–41.
Yokoyama H, Yasuda J, Okamoto H, Iwakura Y. Pathological changes of renal epithelial cells in mice transgenic for the TT virus ORF1 gene. J Gen Virol. 2002;83(Pt 1):141–50.
Yan B, Wang H, Rabbani ZN, Zhao Y, Li W, Yuan Y, Li F, Dewhirst MW, Li CY. Tumor necrosis factor-alpha is a potent endogenous mutagen that promotes cellular transformation. Cancer Res. 2006;66(24):11565–70.
Cimponeriu D, Serafinceanu C, Apostol P, Toma M, Stavarachi M, Radu I, Craciun A, Spandole S, Nicolae P, Rusu L, et al. Potential association of obesity with IL6 G-174C polymorphism and TTV infections. Central European J Biol. 2013;8(7):625–32.
Focosi D, Macera L, Boggi U, Nelli LC, Maggi F. Short-term kinetics of torque Teno virus viraemia after induction immunosuppression confirm T lymphocytes as the main replication-competent cells. The Journal of general virology. 2015;96(Pt 1):115–7.
Rotundo R, Maggi F, Nieri M, Muzzi L, Bendinelli M, Prato GP. TT virus infection of periodontal tissues: a controlled clinical and laboratory pilot study. J Periodontol. 2004;75(9):1216–20.
Guney C, Kadayifci A, Savas MC, Uygun A, Balkan A, Kubar A. Frequency of hepatitis G virus and transfusion-transmitted virus infection in type II diabetes mellitus. Int J Clin Pract. 2005;59(2):206–9.
de Villiers EM, Bulajic M, Nitsch C, Kecmanovic D, Pavlov M, Kopp-Schneider A, Lohr M. TTV infection in colorectal cancer tissues and normal mucosa. Int J Cancer. 2007;121(9):2109–12.
McElvania TeKippe E, Wylie KM, Deych E, Sodergren E, Weinstock G, Storch GA. Increased prevalence of anellovirus in pediatric patients with fever. PLoS One. 2012;7(11):e50937.
Massau A, Martins C, Nachtigal GC, Araujo AB, Rossetti ML, Niel C, da Silva CM. The high prevalence of torque Teno virus DNA in blood donors and haemodialysis patients in southern Brazil. Mem Inst Oswaldo Cruz. 2012;107(5):684–6.
Salakova M, Nemecek V, Konig J, Tachezy R. Age-specific prevalence, transmission and phylogeny of TT virus in the Czech Republic. BMC Infect Dis. 2004;4(1):56.
Funding
This research work was carried out with the support of Ministry of Research and Education, under the Core Program, project PN 16 46 05 01.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
SSD and DC wrote the paper and performed statistical analysis. AMC, RN and SN collected and processed the samples. IR, MT, OAA and CSI performed viral DNA genotyping. LMB designed the study and managed the teams of researchers. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the National Institute of Research and Development for Food Bioresources Ethics Committee with the registration number 342 in the 16th of May, 2014. All participants gave their informed consent according to the Helsinki Declaration on ethical principles for medical research involving human subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional information
Anne-Marie Crăciun, deceased.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Spandole-Dinu, S., Cimponeriu, D.G., Crăciun, AM. et al. Prevalence of human anelloviruses in Romanian healthy subjects and patients with common pathologies. BMC Infect Dis 18, 334 (2018). https://doi.org/10.1186/s12879-018-3248-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-018-3248-9