
Objective:
To verify whether the treatment of brain oligometastases with whole-brain radiotherapy (WBRT) plus stereotactic radiotherapy (SRT) or surgical resection results in different outcomes.
Methods:
Files of patients affected by brain metastases submitted to surgical resection followed by WBRT (group A) or WBRT + SRT (group B) were retrospectively selected for this study. The two treatment groups were matched for the following potential prognostic factors: WBRT schedule, age, gender, performance status, tumor type, number of brain metastases, extra-cerebral metastases, and recursive partitioning analysis class (RPA). The outcomes of patients in both groups were evaluated in terms of toxicity, local control, and overall survival.
Results:
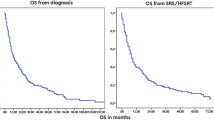
Total of 97 patients were selected (56 male; 42 female) who were respectively submitted to surgical resection followed by WBRT (group A, n = 50 patients) or WBRT + SRT (Group B, n = 47 patients). Median follow-up was 95 months (range, 8–171 months). The 1-year local control rates were 46.0% and 69.0% respectively. No significant difference in local tumor control was observed between group A and B (p = 0.10). Median overall survival was 15 and 19 months in group A and B, respectively. One-year survival was 56.0% and 62%, respectively. No difference was observed in the two groups (p = 0.40).
Conclusion:
Surgery remains the main therapeutic approach in symptomatic patients; nevertheless, our data support the use of WBRT plus SRT in one or two brain metastases smaller than 3 cm.
Zielsetzung:
Zu untersuchen, ob die Behandlung von Oligohirnmetastasen mit Ganzhirnbestrahlung (whole-brain radiotherapy, WBRT) plus stereotaktischer Radiotherapie (SRT) oder chirurgischer Resektion unterschiedliche Ergebnisse bringt.
Methoden:
Krankenakten von Patienten mit operativ entfernten Hirnmetastasen und anschließender WBRT (Gruppe A) oder WBRT + SRT (Gruppe B) wurden retrospektiv für diese Studie ausgewählt. Die zwei Beghandlungsarme wurden für folgende prognostische Parameter gematcht: WBRT-Schema. Alter, Geschlecht, Allgemeinzustand, Art des Primärtumors, Anzahl der Hirnmetastasen, extrazerebrale Metastasen, Recursive-Partioning-Analysis-(RPA-)Klasse. Das Behandlungsergebnis für beide Patientengruppen wurde im Hinblick auf Toxizität, lokale Tumorkontrolle und Gesamtüberleben bewertet.
Ergebnisse:
Insgesamt wurden 97 Patienten ausgewählt (56 m; 42 w), die entweder mit operativer Entfernung und anschließender WBRT (Gruppe A, n = 50 Pat.) oder mit WBRT + SRT (Gruppe B, n = 47 Pat.) behandelt wurden. Die mediane Beobachtungszeit betrug 95 Monate (Spanne 8–171). Die lokale Tumorkontrolle nach 1 Jahr betrug 46,0% (Gruppe A) und 69,0% (Gruppe B), ohne dass dieser Unterschied statistisch signifikant wäre (p = 0,10). Das mediane Gesamtüberleben betrug jeweils 15 und 19 Monate in Gruppe A and B. Die 1-Jahres-Überlebensrate betrug jeweils 56,0% and 62%. Es wurde kein Unterschied zwischen den beiden Gruppen gefunden (p = 0,40).
Schlussfolgerung:
Die chirurgische Entfernung bleibt die Behandlungsoption bei symptomatischen Patienten. Unsere Daten sprechen für eine Behandlung mit WBRT plus SRT bei Vorliegen von ein oder zwei Hirnmetastasen, die kleiner als 3 cm sind.
Similar content being viewed by others


References
Buhmann Kirchhoff S, Becker C, Duerr HR et al. Detection of osseous metastases of the spine: comparison of high resolution multi-detector-CT with MRI. Eur J Radiol 2009;69:567–573.
Catton C, O’sullivan B, Bell R et al. Chordoma: long-term follow-up after radical photon irradiation. Radiother Oncol 1996;41:67–72.
Cummings BJ, Hodson DI, Bush RS. Chordoma: the results of megavoltage radiation therapy. Int J Radiat Oncol Biol Phys 1983;9:633–642.
Emami B, Lyman J, Brown A et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys 1991;21:109–122.
Freundt K, Meyners T, Bajrovic A et al. Radiotherapy for oligometastatic disease in patients with spinal cord compression (MSCC) from relatively radioresistant tumors. Strahlenther Onkol 2010;186:218–223.
Gabriele P, Macias V, Stasi M et al. Feasibility of intensity-modulated radiation therapy in the treatment of advanced cervical chordoma. Tumori 2003;89:298–304.
Kim B, Soisson ET, Duma C et al. Image-guided helical tomotherapy for treatment of spine tumors. Clin Neurol Neurosurg 2008;110:357–362.
Mahan SL, Ramsey CR, Scaperoth DD et al. Evaluation of image-guided helical tomotherapy for the retreatment of spinal metastasis. Int J Radiat Oncol Biol Phys 2005;63:1576–1583.
Mamitz S, Stromberger C, Kawgan-Kagan M et al. Helical tomotherapy in cervical cancer patients: simultaneous integrated boost concept: technique and acute toxicity. Strahlenther Onkol 2010;186:572–579.
Marcus RB, Jr., Million RR. The incidence of myelitis after irradiation of the cervical spinal cord. Int J Radiat Oncol Biol Phys 1990;19:3–8.
Pirzkall A, Carol M, Lohr F et al. Comparison of intensity-modulated radiotherapy with conventional conformal radiotherapy for complex-shaped tumors. Int J Radiat Oncol Biol Phys 2000;48:1371–1380.
Rochet N, Sterzing F, Jensen A et al. Helical tomotherapy as a new treatment technique for whole abdominal irradiation. Strahlenther Onkol 2008;184:145–149.
Scarabino T, Perfetto F, Giannatempo GM et al. [Imaging with magnetic resonance imaging of the operated cervical spine]. Radiol Med 1996;92:671–676.
Schultheiss TE, Kun LE, Ang KK et al. Radiation response of the central nervous system. Int J Radiat Oncol Biol Phys 1995;31:1093–1112.
Schulz-Ertner D, Karger CP, Feuerhake A et al. Effectiveness of carbon ion radiotherapy in the treatment of skull-base chordomas. Int J Radiat Oncol Biol Phys 2007;68:449–457.
Sterzing F, Herfarth K, Debus J. IGRT with helical tomotherapy-effort and benefit in clinical routine. Strahlenther Onkol 2007;183(Spec No 2):35–37.
Sterzing F, Sroka-Perez G, Schubert K et al. Evaluating target coverage and normal tissue sparing in the adjuvant radiotherapy of malignant pleural mesothelioma: helical tomotherapy compared with step-and-shoot IMRT. Radiother Oncol 2008;86:251–257.
Sterzing F, Welzel T, Sroka-Perez G et al. Reirradiation of multiple brain metastases with helical tomotherapy. A multifocal simultaneous integrated boost for eight or more lesions. Strahlenther Onkol 2009;185:89–93.
Sterzing F, Hauswald H, Uhl M et al. Spinal cord sparing reirradiation with helical tomotherapy. Cancer 2010;116:3961–3968.
Stoiber EM, Lechsel G, Giske K et al. Quantitative assessment of image-guided radiotherapy for paraspinal tumors. Int J Radiat oncol Biol Phys 2009:45:933–940.
Terezakis SA, Lovelock DM, Bilsky MH et al. Image-guided intensity-modulated photon radiotherapy using multifractionated regimen to paraspinal chordomas and rare sarcomas. Int J Radiat Oncol Biol Phys 2007;69:1502–1508.
Thariat J, Castelli J, Chanalet S, et al. CyberKnife stereotactic radiotherapy for spinal tumors: value of computed tomographic myelography in spinal cord delineation. Neurosurgery 2009;64:A60–A66.
Verhey LJ. Comparison of three-dimensional conformal radiation therapy and intensity-modulated radiation therapy systems. Semin Radiat Oncol 1999;9:78–98.
Yamada Y, Lovelock DM, Bilsky MH. A review of image-guided intensity-modulated radiotherapy for spinal tumors. Neurosurgery 2007;61:226–235; discussion 235.
Zibold F, Sterzing F, Sroka-Perez G et al. Surface dose in the treatment of breast cancer with helical tomotherapy. Strahlenther Onkol 2009;185:574–581.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
D’Agostino, G.R., Autorino, R., Pompucci, A. et al. Whole-Brain Radiotherapy Combined with Surgery or Stereotactic Radiotherapy in Patients with Brain Oligometastases. Strahlenther Onkol 187, 421–425 (2011). https://doi.org/10.1007/s00066-011-2228-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2228-4