
Background and Purpose:
Recurrent brain metastases or new brain lesions after whole-brain radiotherapy represent a therapeutic challenge. While several treatment methods for single or few lesions have been described, options for multiple lesions are limited. This case report is intended to show an approach of whole-brain reirradiation with a simultaneous multifocal integrated boost using helical tomotherapy. Technique, feasibility, and acute side effects are presented.
Patients and Methods:
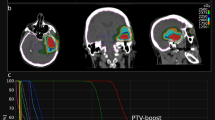
Two patients with multiple relapsed brain metastases (eight and eleven lesions) were reirradiated after previous whole-brain radiotherapy (total dose of 40 Gy 18 months before). Whole-brain reirradiation was performed using helical tomotherapy with a total dose of 15 Gy (single dose 1.5 Gy) and a multifocal simultaneous integrated boost with a total dose of 30 Gy (single dose 3 Gy) to the brain lesions. The boost planning target volume was delineated around the lesions visible on MRI plus a 2-mm margin. Follow-up of these patients was 6 and 12 months.
Results:
Radiation plans with excellent conformity and homogeneity were obtained. High dose exposure to normal brain tissue was kept minimal. Mean radiation time was 13 min. The only acute side effect observed was a mild headache over 2 days at the end of treatment. So far, no further side effects and no signs of recurrence have been observed.
Conclusion:
Helical tomotherapy offers new treatment options for the reirradiation of multiple brain metastases. The number of cases treated with the described protocol is very limited but it is considered a promising option for patients that have responded well to the initial radiotherapy and are in a good performance status.
Hintergrund und Ziel:
Rezidive von Hirnmetastasen oder neue Herde nach vorangegangener Ganzhirnbestrahlung stellen eine therapeutische Herausforderung dar. Während mehrere Techniken zur Behandlung singulärer oder weniger Läsionen beschrieben wurden, sind die Optionen bei multiplen Metastasen limitiert. Dieser Fallbericht beschreibt einen Ansatz der Ganzhirnrebestrahlung mit simultanem multifokalem integriertem Boost mittels helikaler Tomotherapie. Technik, Machbarkeit und akute Nebenwirkungen werden berichtet.
Patienten und Methodik:
Zwei Patienten mit multiplen Rezidiven von Hirnmetastasen (acht bzw. elf Herde) wurden nach vorangegangener Ganzhirnradiotherapie rebestrahlt (40 Gy 18 Monate zuvor). Mittels helikaler Tomotherapie wurden das Neurokranium mit einer Dosis von 15 Gy (Einzeldosis 1,5 Gy) und die Metastasen selbst mit einem multifokalen simultanen integrierten Boost mit einer Dosis von 30 Gy (Einzeldosis 3 Gy) rebestrahlt. Das Planungszielvolumen des Boosts wurde mit einem 2-mm-Sicherheitssaum um die Kontrastmittelaufnahme im MRT definiert. Der Nachbeobachtungszeitraum dieser Patienten betrug 6 bzw. 12 Monate.
Ergebnisse:
Es konnten Bestrahlungspläne mit hervorragender Konformität und Homogenität erreicht werden. Die Hochdosisbelastung des Hirnparenchyms konnte gering gehalten werden. Die mittlere Bestrahlungszeit betrug 13 min. Einzige Akutnebenwirkung war ein geringer Kopfschmerz zum Ende der Behandlung. Es wurden keine weiteren Toxizitäten oder Zeichen eines Rezidivs beobachtet.
Schlussfolgerung:
Die helikale Tomotherapie eröffnet neue Optionen in der Rebestrahlung multipler Hirnmetastasen. Die Anzahl der so behandelten Patienten ist sehr limitiert, dennoch erscheint diese Behandlungsmöglichkeit sehr vielversprechend für Patienten, die auf die initiale Therapie gut angesprochen haben.
Similar content being viewed by others


References
Akyurek S, Chang EL, Mahajan A, et al. Stereotactic radiosurgical treatment of cerebral metastases arising from breast cancer. Am J Clin Oncol 2007;30:310–4.
Bauman G, Yartsev S, Fisher B, et al. Simultaneous infield boost with helical tomotherapy for patients with 1 to 3 brain metastases. Am J Clin Oncol 2007;30:38–44.
Bhatnagar AK, Flickinger JC, Kondziolka D, et al. Stereotactic radiosurgery for four or more intracranial metastases. Int J Radiat Oncol Biol Phys 2006;64:898–903.
Biswas G, Bhagwat R, Khurana R, et al. Brain metastasis - evidence based management. J Cancer Res Ther 2006;2:5–13.
Chang JE, Robins HI, Mehta MP. Therapeutic advances in the treatment of brain metastases. Clin Adv Hematol Oncol 2007;5:54–64.
Cooper JS, Steinfeld AD, Lerch IA. Cerebral metastases: value of reirradiation in selected patients. Radiology 1990;174:883–5.
DiLuna ML, King JTJr, Knisely JP, et al. Prognostic factors for survival after stereotactic radiosurgery vary with the number of cerebral metastases. Cancer 2007;109:135–45.
Fahrig A, Ganslandt O, Lambrecht U, et al. Hypofractionated stereotactic radiotherapy for brain metastases. Results from three different dose concepts. Strahlenther Onkol 2007;183:625–30.
Fiorino C, Dell’Oca I, Pierelli A, et al. Significant improvement in normal tissue sparing and target coverage for head and neck cancer by means of helical tomotherapy. Radiother Oncol 2006;78:276–82.
Gutierrez AN, Westerly DC, Tome WA, et al. Whole brain radiotherapy with hippocampal avoidance and simultaneously integrated brain metastases boost: a planning study. Int J Radiat Oncol Biol Phys 2007;69:589–97.
Han C, Liu A, Schultheiss TE, et al. Dosimetric comparisons of helical tomotherapy treatment plans and step-and-shoot intensity-modulated radiosurgery treatment plans in intracranial stereotactic radiosurgery. Int J Radiat Oncol Biol Phys 2006;65:608–16.
Hazuka MB, Kinzie JJ. Brain metastases: results and effects of re-irradiation. Int J Radiat Oncol Biol Phys 1988;15:433–7.
Hocht S, Wiegel T, Hinkelbein W. Reirradiation for recurrent brain metastases: an overview. Front Radiat Ther Oncol 1999;33:327–31.
Kocher M, Maarouf M, Bendel M, et al. Linac radiosurgery versus whole brain radiotherapy for brain metastases. A survival comparison based on the RTOG recursive partitioning analysis. Strahlenther Onkol 2004;180:263–7.
Kron T, Grigorov G, Yu E, et al. Planning evaluation of radiotherapy for complex lung cancer cases using helical tomotherapy. Phys Med Biol 2004;49:3675–90.
Kurup P, Reddy S, Hendrickson FR. Results of re-irradiation for cerebral metastases. Cancer 1980;46:2587–9.
Mackie TR, Balog J, Ruchala K, et al. Tomotherapy. Semin Radiat Oncol 1999;9:108–17.
Peak S, Abrey LE. Chemotherapy and the treatment of brain metastases. Hematol Oncol Clin North Am 2006;20:1287–95.
Penagaricano JA, Papanikolaou N, Yan Y, et al. Feasibility of cranio-spinal axis radiation with the Hi-Art tomotherapy system. Radiother Oncol 2005;76:72–8.
Rades D, Bohlen G, Dunst J, et al. Comparison of short-course versus long-course whole-brain radiotherapy in the treatment of brain metastases. Strahlenther Onkol 2008;184:30–5.
Rochet N, Sterzing F, Jensen A, et al. Helical tomotherapy as a new treatment technique for whole abdominal irradiation. Strahlenther Onkol 2008;184:145–9.
Sheng K, Molloy JA, Read PW. Intensity-modulated radiation therapy (IMRT) dosimetry of the head and neck: a comparison of treatment plans using linear accelerator-based IMRT and helical tomotherapy. Int J Radiat Oncol Biol Phys 2006;65:917–23.
Soffietti R, Cornu P, Delattre JY, et al. EFNS guidelines on diagnosis and treatment of brain metastases: report of an EFNS Task Force. Eur J Neurol 2006;13:674–81.
Soisson ET, Tome WA, Richards GM, et al. Comparison of linac based fractionated stereotactic radiotherapy and tomotherapy treatment plans for skull-base tumors. Radiother Oncol 2006;78:313–21.
Sterzing F, Herfarth K, Debus J. IGRT with helical tomotherapy — effort and benefit in clinical routine. Strahlenther Onkol 2007;183:Spec No 2:35–7.
Sterzing F, Schubert K, Sroka-Perez G, et al. Helical tomotherapy. Experiences of the first 150 patients in Heidelberg. Strahlenther Onkol 2008; 184:8–14.
Wadasadawala T, Gupta S, Bagul V, et al. Brain metastases from breast cancer: management approach. J Cancer Res Ther 2007;3:157–65.
Welsh JS, Patel RR, Ritter MA, et al. Helical tomotherapy: an innovative technology and approach to radiation therapy. Technol Cancer Res Treat 2002;1:311–6.
Wong ET, Berkenblit A. The role of topotecan in the treatment of brain metastases. Oncologist 2004;9:68–79.
Wong WW, Schild SE, Sawyer TE, et al. Analysis of outcome in patients reirradiated for brain metastases. Int J Radiat Oncol Biol Phys 1996;34:585–90.
Yartsev S, Kron T, Cozzi L, et al. Tomotherapy planning of small brain tumours. Radiother Oncol 2005;74:49–52.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sterzing, F., Welzel, T., Sroka-Perez, G. et al. Reirradiation of multiple brain metastases with helical tomotherapy. Strahlenther Onkol 185, 89–93 (2009). https://doi.org/10.1007/s00066-009-1971-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-009-1971-2