
Abstract
Background
Approximately 30% of children with idiopathic nephrotic syndrome develop a complicated course with frequent relapses or steroid dependency. Rituximab, a B cell depleting monoclonal antibody, is a safe and effective alternative to steroids or other immunosuppressants for achieving and maintaining remission in this population at short term. Despite the good initial response relapses inevitably occur after regeneration of B lymphocytes, necessitating either repeat courses of rituximab or addition of another steroid-sparing immunosuppressant.
Methods
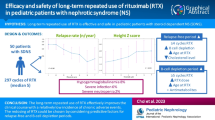
This is a prospective, single-center, open-label, two-parallel-arm randomized controlled phase III study among children with steroid dependent nephrotic syndrome who are maintained in remission with oral steroids. One hundred children will be randomized to either Rituximab and maintenance Mycophenolate mofetil (A) or repeated courses of prophylactic Rituximab only (B). In arm A, mycophenolate mofetil (1200 mg/m2 per day) will be started 3 months after Rituximab administration. In arm B, Rituximab infusions will be administered at 0, 8 and 16 months if B cell count normalize at the given time points. Prednisolone will be discontinued in both groups 2 weeks following first course of rituximab. Primary aim is to evaluate the difference in 24-month relapse-free survival. Main secondary endpoints are cumulative prednisolone dose, frequency of relapses and changes in anthropometry. Circulating B lymphocyte populations will be studied as biomarkers or predictors of rituximab responsiveness and adverse events will be analysed.
Discussion
The study will provide evidence as to the comparative safety and efficacy of two alternative steroid-sparing therapeutic options in children suffering from steroid dependent nephrotic syndrome. The two-year study design will address the long-term results obtained with the alternative treatment protocols.
Trial registration
This trial was prospectively registered to the Clinicaltrial.gov (NCT03899103 dated 02/04/2019; https://clinicaltrials.gov/) and Clinical Trials Registry of India (CTRI/2019/04/018517 dated 09/04/2019).
Similar content being viewed by others


Background
Whilst idiopathic nephrotic syndrome in children usually responds well to corticosteroid treatment, more than two thirds of patients experience relapses and 30% develop a complicated course with frequent relapses or steroid dependency (SDNS) [1,2,3,4,5,6,7]. Relapses may lead to serious complications from anasarca, infections, thrombosis and malnutrition. Repeated or even continuous steroid treatment leads to considerable medication related toxicity and morbidity [1,2,3,4,5,6].
Hence, the primary aim of treatment is to reduce the number of relapses, the cumulative dose of corticosteroids, and the incidence of serious complications. Several prospective studies have suggested that Rituximab, a B-lymphocyte depleting monoclonal antibody, could be a safe and effective alternative to steroids and conventional steroid-sparing immunosuppressants such as calcineurin inhibitors or mycophenolate-mofetil (MMF) to achieve and maintain remission in this population [7,8,9,10,11]. Single rituximab infusions reliably suppress disease relapses for 6 to 12 months with a very mild side effect profile [7,8,9,10,11]. In the RITURNS trial we demonstrated a significant and clinically relevant reduction of relapse rates by primary use of Rituximab as compared to standard CNI therapy during a 12-month observation period, accompanied by a more favourable side effect profile [7]. However, relapses inevitably occur during extended follow-up following regeneration of B-lymphocytes. Therefore, further modification of Rituximab treatment, including repeated courses of Rituximab or adjunct immunosuppressive therapies, may be necessary for maintaining long-term remission. A few case series suggested that maintenance therapy with MMF after rituximab administration was effective for maintaining long-term remission in children with complicated nephrotic syndrome, with a largely benign side effect profile [12,13,14]. The long term follow up of our RITURNS trial also revealed improved relapse free survival with maintenance MMF therapy following rituximab re-exposure [14]. Hence, repeated courses of Rituximab or sequential maintenance therapy with MMF following the initial Rituximab course have been proposed as long-term treatment options in SDNS [7,8,9,10,11]. Our study will compare the relative efficacy and safety of these protocols over a 2-year period.
Methods/design
Aim, design and setting of the study
The RITURNS II trial is a prospective, single-center, open-label, two-parallel-arm randomized controlled phase III study. The aim is to evaluate the efficacy and safety of repeat courses of Rituximab to that of maintenance MMF following a single course of Rituximab in maintaining remission over 24 months in children with SDNS (as defined in Table 1). The test hypothesis is as follows: prophylactic repeated courses of Rituximab will result in improved relapse free survival compared to maintenance Mycophenolate Mofetil following single course of Rituximab infusion in children with steroid dependent nephrotic syndrome (SDNS), i.e., testing superiority.
The trial was started on 15th May, 2019 at the Division of Pediatric Nephrology, Department of Pediatrics, NRS Medical College & Hospital, Kolkata, India. By 15th September 2020, 70 patients have been enrolled in the trial.
Characteristics of participants
Inclusion criteria: children between 3 and 16 years with SDNS; minimal change disease/FSGS/MesPGN as per kidney biopsy report; estimated glomerular filtration rate (eGFR) > 80 ml/min per 1.73 m2 at study entry; remission at study entry (urine albumin nil or trace (or proteinuria < 4 mg/m2/h or uPCR < 200 mg/g (< 20 mg/mmol)) for 3 consecutive early morning specimens); not received any steroid sparing agent (including levamisole, calcineurin inhibitors, mycophenolate mofetil, cyclophosphamide, mizoribine, chlorambucil or rituximab) previously; parents willing to give informed written and audiovisual consent; and ability to swallow tablet.
Exclusion criteria: known etiology (e.g., lupus erythematosus, IgA nephropathy, amyloidosis, malignancy, other secondary forms of NS); patients with severe leukopenia (leukocytes < 3.0× 1000 cells/mm3), severe anemia (haemoglobin < 8.9 g/dl), thrombocytopenia (platelet < 100.0 × 1000 cells/mm3) or deranged liver function tests (AST or ALT to > 50 IU/L) at enrolment; known active chronic infection (tuberculosis, HIV, hepatitis B or C); and live vaccination within 1 month prior to screening.
Processes, interventions and comparisons
Participant screening and recruitment
Consecutive cases of SDNS presenting at the study centre will be screened for eligibility. A preliminary interview for clinical and pharmacological history will be performed in order to verify the eligibility criteria. All participants undergo kidney biopsies before enrolment in the trial. A study investigator will explain the project, deliver information sheet. Children fulfilling the inclusion criteria will be recruited. The Pediatric Nephrology Division of NRS Medical College & Hospital, Kolkata is one of the largest dedicated pediatric nephrology services at Government Sector in India. An average of 140–180 children are seen per week in the nephrotic syndrome outpatient clinic; approx. 20–30% of these are new cases and about 60–80% of new cases are SDNS.
Interventions
Arm a (rituximab and mycophenolate mofetil, control treatment)
First Course Rituximab at Randomization: Two infusions will be administered intravenously at a 7-day interval at standard dose (rituximab 375 mg/m2, maximum 500 mg). Circulating B cells will be measured 24 h after second rituximab administration. If B cell count exceeds 5/mm3, it will be measured again after 1 week. If count is still > 5/mm3, one more dose of rituximab will be administered.
Co-intervention with Rituximab at Randomization: Prednisolone will be continued at alternate-day doses for 2 weeks (1.5 mg/kg (max.40 mg) per 48 h in patients on daily prednisolone at time of randomization; pre-randomization dose in those already on alternate-day dosing). At 2 weeks, prednisolone will be discontinued.
Addition of Maintenance MMF from month 4 onwards: Maintenance oral MMF 1200 mg/mt2 daily in two divided doses will be added from month 4 of follow-up and continued over the remaining study period unless an adverse event occurs.
Arm B (repeated courses of rituximab only, experimental treatment)
First Course Rituximab at Randomization: Same as Arm A.
Co-intervention with Rituximab at Randomization: Same as Arm A.
Prophylactic 2nd and 3rd Course Rituximab Re-administration at 8 Months and 16 Months of Follow-up: Prophylactic 2nd and 3rd course rituximab re-administration will be done at 8 months and 16 months of follow-up if B cell count normalize (please refer to Additional file 1: Appendix 0 for our reference range of normal age specific B cell count) and patient is in remission. Dose and route will remain as explained in Table 2.
Comparisons, randomization & blinding
Treatment arm A will be compared to treatment arm B. Randomization will be performed 1:1 using stratified block randomization with varying block sizes and including age (≤ 7 vs. > 7 years) and renal histology (MCD vs. FSGS) as stratification factors. To achieve comparable intervention groups and to minimize a potential selection bias, patients will be allocated in a concealed fashion by means of randomization after enrolment. To that end, a computer generated random list will be created according to the stratification factors and block sizes and sealed opaque envelopes will be provided by an independent data manager from the Institute of Medical Biometry and Informatics, University of Heidelberg. Enrolment and assignment of the participants to interventions will be done by investigators and resident doctors at NRS Medical College & Hospital, Kolkata, India. The trial will be open-label with no masking of patients or study staff to the treatment allocation.
Study visits & assessment
Baseline assessment at enrolment
Retrospective clinical information will be obtained from the case records and clinic files. This will include information regarding age of onset of disease, disease type, duration of total disease etc.; and treatment received, number of relapses, cumulative steroid dose, detailed anthropometry and investigations during the last 12 months prior screening. The patients shall be clinically screened for significant infection. The information will be entered into the patient data sheet (refer to Additional file 1: Appendix 1). Clinical examination shall be done and data shall be recorded.
Follow-up visit and drug compliance
Study visits will be scheduled at enrolment, then weekly for the first month, then at 4th month and then 4 monthly until the end of the study or during relapse, remission and if there is any specific need after enrolment. In Arm B (repeated courses of rituximab only), there will be 2 extra visits 1 week after the prophylactic 2nd and 3rd courses of rituximab re-administration at 8 months and 16 months, respectively.
Complete blood count, kidney function, liver enzymes, serum electrolytes, plasma proteins, serum cholesterol, serum albumin, serum immunoglobulin and B lymphocyte count as applicable will be obtained during protocol visits and in between period if needed. Circulating B-cell count (number/mm3) will be measured at enrolment, then every fortnight for the first month, then at 4 months and then 4-monthly until the end of the study or during relapse and if there is any specific need after enrolment. An overview is given in Table 3. At the 12- and 24-month visits a quality of life (QoL) assessment together with a specific questionnaire concerning the impact of the different treatment patterns on patient and family life shall be performed.
At each visit, the drug will be handed over to the parent/guardian in an amount sufficient to last the interim duration; ten extra doses would be provided to ensure compliance even if follow-up is delayed for some reason. At the follow-up visit, empty packs of drug provided in previous visit would be collected and pill count done to check compliance to intervention. At discharge from the Nephrology Unit, each patient will receive a clinical diary, to be filled with dipstick proteinuria levels and current treatment. Adherence will also be recorded in the patients’ diary.
Duration of study
The overall duration of the trial is expected to be approximately 36 months. Recruitment of the patients is planned over a time period of 12 months, and the duration of follow-up per patient (start at treatment initiation) will be 24 months (Fig. 1).

Study flow chart
Standard case management
Relapse management
Relapses will be treated by reinstitution of daily therapy with prednisolone (2 mg/kg/day, maximum 60 mg) until remission, followed by alternate-day dosing (1.5 mg/kg, maximum 40 mg) for 4 weeks, and then stopped.
Other co-interventions
Rituximab will be administered after proper premedications (administer 30 min prior to rituximab) with oral paracetamol, oral diphenhydramine and intravenous hydrocortisone as per center practice.
Hypertension, defined as blood pressure > 95th percentile (for age, height and sex) in those previously normotensive, shall be treated at the discretion of the investigator. Children shall be treated with oral calcium+vitamin D when on oral prednisolone. Other medications shall be used at the discretion of the treating physician. Trimethoprim-sulfamethoxazole shall be administered from the beginning of rituximab treatment until recovery of peripheral blood B cell for prophylaxis against Pneumocystis jirovecii infection. The investigator will record all concomitant medications taken by the subject during the study from the date of informed consent, in the appropriate section of the case report form.
Safety data
We will collect any untoward medical occurrence in the form of signs, symptoms, abnormal laboratory findings, or diseases that emerges or worsens relative to baseline (i.e. present at the initial study visit). All adverse events including any transfusion reaction following rituximab infusion will be graded according to the Common Terminology Criteria for Adverse Events, version 3 [15]. Policy and approach to define adverse events is reported in Additional file 1: Appendix 2.
Study termination
Subjects will be informed that they have the right to withdraw from the study at any time, without prejudice to their medical care, and that they are not obliged to state their reasons. The time and reason of treatment discontinuation will be documented in the CRF. Independent data-safety and monitoring board (DSMB) (or IRB) will monitor the study progress at regular interval.
Data management & quality assurance
The investigators will record study data in the case report form (CRF). The clinical and laboratory data shall be entered in electronic format. At monthly intervals, the data entries will be checked for completeness and the files reviewed for errors.
At the end of the study, the data will be transformed into different data formats for archiving and to ensure that it can be reused. It is planned to make the trial data on which scientific publications are based, as well as all the primary data, publicly available in an appropriate online data repository to allow re- and meta-analyses after completion of the trial.
Study endpoints, estimand definition, power calculation and type of statistical analysis used
Study endpoints
Primary endpoint
The primary endpoint is the time from treatment initiation to first relapse or death (whichever occurs first).
Secondary endpoints
Main secondary endpoint is 1.) the cumulative prednisolone requirement (mg/kg/yr) over the first 12 and 24 months, respectively. Further secondary endpoints are 2.) at least one relapse within the first 12 months (yes/no); 3.) at least one relapse within 24 months (yes/no); 4.) occurrence of two or more than two relapses in any period of 6 months within 24 months (yes/no); 5.) occurrence of four or more relapses in a period of any 12 months within 24 months (yes/no); 6.) at least One episode of life threatening infection or severe relapse (anasarca with hypovolemia or thrombosis) requiring hospital admission within any 12 months (within 24 months) and 24 months (yes/no), respectively; 7.) impairment of renal function (eGFR < 30 ml/min per 1.73 m2 or loss of eGFR by > = 30% with regard to baseline) within any 12 months (within 24 months) and 24 months (yes/no), respectively; 8.) treatment failure (yes/no): defined as composite endpoint consisting of the three endpoints as defined above under 5., 6. and 7. referring to month 24; 9.) number and severity of adverse events; 10.) eGFR at 4, 8, 12, 18 and 24 months, respectively; absolute change in eGFR from baseline to 4, 8, 12, 16 and 24 months, respectively; 11.) number of relapses within months 0–24, 0–12 and 12–24, respectively; 12.) number of different steroid toxicity events (new onset) within months 0–24; 13.) off steroids at month 24 (yes/no); 14.) abnormal values in biochemical tests and haematology assessments (yes/no) according to the Common Terminology Criteria for Adverse Events, version 3 [15]; 15.) height SDS at 12 and 24 months, respectively; 16.) absolute change in height SDS from baseline to 24 months; 17.) BMI SDS at 12 and 24 months, respectively; 18.) absolute change in BMI SDS from baseline to 24 months; 19.) total B Lymphocyte count (% and per mm3) over time.
Estimands
An estimand is defined through the treatment, the targeted population, the variable, a specification of how to handle intercurrent events (postrandomization events) and a population-level summary [16]. In the following, the primary estimand corresponding to the primary objective, as well as the main secondary estimands corresponding to the main secondary objective are described.
Primary Estimand
The treatment is described as above and the targeted population is defined through the in- and exclusion criteria who received at least one dose of study treatment. The intercurrent events are handled as follows. Administrative censoring at the end of study, withdrawing and loss to follow-up without prior deterioration are assumed to be uninformative and will be censored. This implies the assumption that censored patients would have behaved as the uncensored patients. Hence, this describes a scenario in which the intercurrent event would not occur (hypothetical strategy). It is assumed that the event death is worse than a first relapse, therefore it is included in the definition of the variable (composite strategy). Deviations from the treatment protocol and treatment switching will be ignored (treatment policy strategy). The population-level summary measure is the hazard ratio.
Main secondary Estimands
Treatment and population are specified as for the primary estimand. The variable is defined as the amount of cumulative prednisolone requirement (mg/kg/year) over 12 and 24 months, respectively. Intercurrent events are handled as follows. Withdrawals, lost to follow-up, death, treatment switching, deviations from the treatment protocol and AEs will be ignored (treatment policy strategy). The summary measure is the difference in variable means.
Sample size/ power calculation
The sample size calculation is based on the primary endpoint, time to first relapse or death (whichever occurs first), using log-rank test to compare the event times of arm A and B. An event rate of 25% after 24 months in arm A and 5% in arm B was assumed (hazard ratio = 0.178) [12,13,14, 17,18,19,20,21,22]. Assuming an individual follow-up time of 24 months, in total 95 patients (15 events) are required to prove efficacy with a power of 90% and a two-sided alpha level of 5% for the log-rank test. To account for major protocol violations and drop-outs an assumed drop-out rate of 10% yields a total of 100 patients to be randomized [23, 24].
Statistical analysis
The analysis will be performed on the full analysis set (FAS; according to the intention to treat principle), the per-protocol set and the safety analysis set (for details refer to Additional file 1: Appendix 3).
All documented variables will be analyzed descriptively by tabulation of empirical distribution measures accordingly to the scale level and under specification of the number of non-missing values.
The confirmatory primary analysis will be based on the FAS. The primary endpoint will be compared between the two treatment groups using a two-tailed logrank test stratified by age (≤ 7 vs. > 7 years) and renal histology (MCD vs. FSGS) at an overall type I error rate of 0.05. The survival curves will be estimated using the Kaplan-Meier product-limit method, and the corresponding confidence intervals will be calculated using Greenwood’s formula [25]. Missing values on the covariates will be imputed by a multivariate imputation model. To assess the impact of major protocol deviations, an analogous analysis of the primary endpoint will be performed on the per protocol set. In addition, the possible influence of age (continuous) and renal histology on the primary endpoint is evaluated within a multivariate Cox regression analysis including treatment group (under the assumption of proportional hazards) performed on the FAS. Furthermore, a multivariate Cox regression analysis with covariates, age (continuous), sex, renal histology (MCD vs. FSGS), duration of the nephrotic syndrome (years), number of relapses in previous year and group will be performed on the FAS. All secondary endpoints will be analyzed based on the FAS and the results will be interpreted descriptively.
The safety analysis will be based on the safety analysis set and includes calculation and comparison of frequencies and rates of adverse and serious adverse events reported in the two treatment groups. Furthermore, the relation of AEs with the cumulative dose of Rituximab, MMF and Prednisolone will be described, respectively.
More details can be found in the statistical analysis plan which will be finalized prior to database closure and before performing any analyses. All analyses will employ SAS Version 9.4 or higher.
Discussion
Existing clinical practice guidelines recommend calcineurin inhibitors (CNI) as first-line steroid sparing therapy for children with SDNS, whereas Rituximab is used as a rescue for CNI resistant cases [7,8,9,10,11]. However, the excellent efficacy and safety profile of Rituximab raised the question whether it could be used as a first-line alternative to CNI therapy. In the RITURNS trial we demonstrated a significant and clinically relevant reduction of relapse rates by primary use of Rituximab as compared to standard CNI therapy during a 12-month observation period, accompanied by a more favourable side effect profile [7]. To further assess the long-term efficacy and safety of the treatment protocols we extended the follow-up of the RITURNS trial cohorts by another 2 years [14]. In this follow-up study we noted disease recurrence in all patients of the Rituximab arm, with first relapses occurring between 6 and 24 months following Rituximab exposure. This finding supports existing literature on rituximab in children with nephrotic syndrome [26,27,28].
The transient nature of the therapeutic effect of Rituximab creates a need to develop safe and efficient longer-term treatment protocols for SDNS. Repeated prophylactic Rituximab administration is one therapeutic option. Alternatively, an oral maintenance steroid-sparing immunosuppressant can be initiated before B cells are repleted. Encouraging results have been reported for both approaches in retrospective case collections and small cohort studies [12,13,14, 17,18,19,20,21,22].
Rituximab re-treatment without any maintenance immunosuppression prolonged the relapse-free survival in previously relapsing patients [19,20,21,22]. In the RITURNS trial we demonstrated that B cell counts recovered by 12, 39 and 93% at 6 mo, 9 mo and 12 mo respectively following a single course of rituximab and all relapses occurred beyond 8 months after administration in patients who had achieved full B-cell recovery [7]. Two other trials demonstrated a similar pattern of B-cell depletion following rituximab [26,27,28]. We chose an 8-monthly re-treatment schedule as a compromise to avoid unnecessary and costly over-immunosuppression on the one hand and extended periods of fully recovered B cell activity at risk of relapses on the other hand.
MMF maintenance treatment following Rituximab re-exposure in post-Rituximab relapsers also extended the duration of remission, with two thirds of patients remaining relapse-free for 2 years [12]. The long term follow up of our RITURNS trial also revealed better relapse free survival with maintenance MMF therapy following rituximab induction, with a relatively benign side effect profile [14]. A recent retrospective multicenter study revealed that children receiving low-dose rituximab without maintenance immunosuppression had the shortest relapse-free survival, and both the cumulative rituximab dose and maintenance immunosuppression had important effects on treatment outcomes [29].
These observations and considerations motivated us to design a trial comparing these alternative treatment approaches.
RITURNS II will be the first randomised clinical trial comparing the effects of extended B cell depletion by repeated rituximab administration to that of maintenance MMF after a single course of Rituximab in maintaining extended disease remission in children with SDNS. The sample size and evaluation period will be sufficient to empower the assessment not only of differences in therapeutic efficacy but also to obtain valid safety information. The lack of the long term safety data is the main current concern of clinicians precluding extensive use of Rituximab in children with SDNS.
Another strength of this trial will be the exploration of potential markers and mediators of treatment efficacy and adverse effects. We will regularly monitor B-lymphocyte counts, as well as oral drug adherence using patient diaries and returned pill counting.
Potential limitations of our study are given by its single-centre nature, and the lack of blinding which would have required additional administration of placebo tablets and infusions, a procedure that was not deemed acceptable in this vulnerable population of children, nor required given the fact that urine protein measurement is an objective endpoint that is hardly affected by investigator expectation bias. Bias from potential confounding factors will be minimized addressed by inclusion as covariates into the statistical analysis.
In conclusion, we perform this randomized clinical trial to compare efficacy and safety of repeated courses of rituximab to that of maintenance mycophenolate mofetil following a single course of rituximab in maintaining remission over 24 months among children with SDNS, to provide an evidence base for the long-term management of children suffering from complicated nephrotic syndrome.
Availability of data and materials
The datasets generated and/or analysed during the current study will be made available in an appropriate online data repository. All investigators will have access to the final trial dataset.
Abbreviations
- AE:
-
Adverse Event
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- BSA:
-
Body surface area
- CRF:
-
Case Report Form
- DSMB:
-
Data safety and monitoring board
- EC:
-
Ethics Committee
- eGFR:
-
estimated glomerular filtration rate
- FAS:
-
Full Analysis Set
- FRNS:
-
Frequent-relapse nephrotic syndrome
- FSGS:
-
Focal segmental glomerulosclerosis
- GCP:
-
Good Clinical Practice
- ITT:
-
Intention-to-Treat
- MCD:
-
Minimal Change disease
- MesPGN:
-
Mesangioproliferative glomerulonephritis
- MMF:
-
Mycophenolate mofetil
- PI:
-
Principal Investigator
- PP:
-
Per-Protocol
- Q:
-
Quarter (time span)
- SAE:
-
Serious Adverse Event
- SSNS:
-
Steroid-sensitive nephrotic syndrome
- SDNS:
-
Steroid-dependent nephrotic syndrome
- SDS:
-
Standard deviation score
References
Hahn D, Hodson EM, Willis NS, Craig JC. Corticosteroid therapy for nephrotic syndrome in children. Cochrane Database of Systematic Reviews 2015, Issue Issue 3. Art. No.: CD001533. Art. No.: CD001533. DOI: https://doi.org/10.1002/14651858.CD001533.pub5.).
Robinson RF, Nahata MC, Mahan JD, Batisky DL. Management of nephrotic syndrome in children. Pharmacotherapy. 2003;23:1021–36.
Larkins NG, Liu ID, Willis NS, Craig JC, Hodson EM. Non-corticosteroid immunosuppressive medications for steroid-sensitive nephrotic syndrome in children. Cochrane Database of Systematic Reviews 2020, Issue 4. Art. No.: CD002290. DOI: https://doi.org/10.1002/14651858.CD002290.pub5.
Neuhaus TJ, Fay J, Dillon MJ, Trompeter RS, Barratt TM. Alternative treatment to corticosteroids in steroid sensitive idiopathic nephrotic syndrome. Arch Dis Child. 1994;71:522–6.
KDIGO. Clinical practice guideline for glomerulonephritis. Kidney Int Suppl. 2012;2:163–71.
Abeyagunawardena AS, Dillon MJ, Rees L, Hoff W, van’t Trompeter RS. The use of steroid sparing agents in steroid-sensitive nephrotic syndrome. Pediatr Nephrol. 2003;18:919–24.
Basu B, Sander A, Roy B, et al. Efficacy of rituximab vs tacrolimus in pediatric corticosteroid-dependent nephrotic syndrome: a randomized clinical trial. JAMA Pediatr. 2018 Aug;172(8):757–64.
Prytuła A, Iijima K, Kamei K, et al. Rituximab in refractory nephrotic syndrome. Pediatr Nephrol. 2010;25:461–8.
Kemper MJ, Gellermann J, Habbig S, et al. Long-term follow-up after rituximab for steroid dependent idiopathic nephrotic syndrome. Nephrol Dial Transplant. 2012;27:1910–5.
Ravani P, Magnasco A, Edefonti A, et al. Short-term effects of rituximab in children with steroid- and calcineurin-dependent nephrotic syndrome: a randomised controlled trial. Clin J Am Soc Nephrol. 2011;6:1308–15.
Ravani P, Ponticelli A, Sicialiano C, et al. Rituximab is a safe and effective long-term treatment for children with steroid and calcineurin inhibitor-dependent idiopathic nephrotic syndrome. Kidney Int. 2013;84:1025–33.
Basu B, Mahapatra TK, Mondal N. Mycophenolate Mofetil following rituximab in children with steroid-resistant nephrotic syndrome. Pediatrics. 2015 Jul;136(1):e132–9. https://doi.org/10.1542/peds.2015-0486.
Ito S, Kamei K, Ogura M, Sato M, Fujimaru T, Ishikawa T, et al. Maintenance therapy with mycophenolate mofetil after rituximab in pediatric patients with steroid-dependent nephrotic syndrome. Pediatr Nephrol. 2011;26(10):1823–8.
Basu B, Schaefer F. Rituximab and MMF maintenance therapy in children with steroid dependent nephrotic syndrome: RITURNS trial follow-up. Abstract, ASN Kidney Week, 2019.
Common Terminology Criteria for Adverse Events, Version 3.0, DCTD, NCI, NIH, DHHS March 31, 2003 (http://ctep.cancer.gov).
International Conference on Harmonization (2019), “Final ICH E9 (R1) Addendum on ‘Estimands and Sensitivity Analysis in Clinical Trials’ to the Guideline on Statistical Principles for Clinical trials”.
Sharma AP, Filler G. Role of mycophenolate mofetil in remission maintenance after a successful response to rituximab. Pediatr Nephrol. 2009;24(2):423–4.
Fujinaga S, Sakuraya K, Yamada A, Urushihara Y, Ohtomo Y. Shimizu T positive role of rituximab in switching from cyclosporine to mycophenolate mofetil for children with high-dose steroid-dependent nephrotic syndrome. Pediatr Nephrol. 2015;30:687–91.
Sellier-Leclerc AL, Macher MA, Loirat C, et al. Rituximab efficiency in children with steroid-dependent nephrotic syndrome. Pediatr Nephrol. 2010;25:1109–15. https://doi.org/10.1007/s00467-010-1465-6.
Kimata T, Hasui M, Kino J, et al. Novel use of rituximab for steroid-dependent nephrotic syndrome in children. Am J Nephrol. 2013;38:483–8. https://doi.org/10.1159/000356439.
Pendergraft WF, Cortazar FB, Wenger J, Murphy AP, Rhee EP, Laliberte KA, et al. Long-term maintenance therapy using rituximab-induced continuous B-cell depletion in patients with ANCA vasculitis. CJASN. 2014;9(4):736–44.
Cortazar FB, Rosenthal J, Laliberte K, Niles JL. Continuous B-cell depletion in frequently relapsing, steroid-dependent and steroid-resistant nephrotic syndrome. Clin Kidney J. 2018 Jul 24;12(2):224–31.
Schoenfeld D. The asymptotic properties of nonparametric tests for comparing survival distributions. Biometrika. 1981;68(1):316–9.
ADDPLAN. Adaptive Designs – Plans and Analyses. Version 6.1.1. 2014; http://www.addplan.com/ (last access Nov 29 2018).
Kalbfleisch, J. D., & Ross, L. (1980). Prentice. The statistical analysis of failure time data, 2.
Ravani P, et al. Rituximab in Children with Steroid- Dependent Nephrotic Syndrome: A Multicenter, Open-Label, Noninferiority, Randomized Controlled Trial [J]. JASN 2015, pii: ASN.2014080799(9):2259.
Iijima K, et al. Rituximab for childhood-onset, complicated, frequently relapsing nephrotic syndrome or steroid-dependent nephrotic syndrome: a multicentre, double-blind, randomised, placebo-controlled trial [J]. Lancet. 2014;384(9950):1273–81.
Kamei K, et al. Long-term outcome of childhood-onset complicated nephrotic syndrome after a multicenter, double-blind, randomized, placebo-controlled trial of rituximab. Pediatr Nephrol. 2017;32(11):2071–8.
Chan EY, Webb H, Yu E, Ghiggeri GM, et al. Both the rituximab dose and maintenance immunosuppression in steroid-dependent/frequently-relapsing nephrotic syndrome have important effects on outcomes. Kidney Int. 2020;97:393–401.
Acknowledgements
Not applicable
Funding
This research receives no specific external grant from any external funding agency in the public, commercial or not-for-profit sectors. NRS Medical College & Hospital, Kolkata, India has agreed to supply drugs and consumables related to the study, procured directly by hospital medicine store, and approved to use existing hospital infrastructure to conduct the study. There is no external manpower funding for this single-center project. As the trial is a project of the Institute, we are allowed to utilize work-time of existing staff including faculty members and postgraduate residents, the department’s data entry operator, the pediatric nephrology staff nurse, and the pediatric outpatient staff nurse. The funding source shall not be involved in collection, analysis, interpretation of data, writing of the re-port, or the decision to submit the paper for publication. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
BB: Protocol preparation, study design and preparation of manuscript. FS: Protocol preparation, study design, preparation and critical revision of manuscript. AS, SP: Protocol preparation, statistical analysis planning and preparation of manuscript. TM: study design and preparation of manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The original study protocol was approved on 13th February 2019 (NMC/586) by the Ethics Committee (Institutional Review Board) of Nil Ratan Sircar Medical College, Kolkata, India following approval of institute scientific committee.
Informed written and audiovisual consent from the parents (and assent of the child if > 7 yr old) will be obtained before enrolment by investigators and resident doctors at NRS Medical College & Hospital, Kolkata, India, after provision of detailed oral and written information concerning the context of the study, potential benefit to the child and comprehensive safety aspects. The informed consent process will be in accordance with International Council for Harmonization and Good Clinical Practice, the Declaration of Helsinki and local regulatory requirements. Parent information sheet containing background information, safety of the study and possible benefit will be provided prior to obtaining consent for the study. The investigator will ensure that the subjects’ anonymity is maintained. Any protocol amendment will be notified to all relevant parties following fresh ethics clearance. On the case report forms or other documents, participants will not be identified by their names, but by their assigned identification number. If participant names are included on copies of documents submitted to the principal investigator, the names will be obliterated and the assigned subject numbers added to the documents.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests for the overall trial and the study site.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Basu, B., Preussler, S., Sander, A. et al. Randomized clinical trial to compare efficacy and safety of repeated courses of rituximab to single-course rituximab followed by maintenance mycophenolate-mofetil in children with steroid dependent nephrotic syndrome. BMC Nephrol 21, 520 (2020). https://doi.org/10.1186/s12882-020-02153-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-020-02153-5