
Abstract
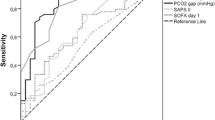
This study aimed to compare the prognostic performance of the ratio of mixed and central venous–arterial CO2 tension difference to arterial–venous O2 content difference (Pv-aCO2/Ca-vO2 and Pcv-aCO2/Ca-cvO2, respectively) with that of the mixed and central venous-to-arterial carbon dioxide gradient (Pv-aCO2 and Pcv-aCO2, respectively) for adverse events after cardiac surgery. One hundred and ten patients undergoing cardiac surgery with cardiopulmonary bypass were enrolled. After catheter insertion, three blood samples were withdrawn simultaneously through arterial pressure, central venous, and pulmonary artery catheters, before and at the end of the operation, and preoperative and postoperative values were determined. The primary end-point was set as the incidence of postoperative major organ morbidity and mortality (MOMM). Receiver operating characteristic (ROC) curve and multivariate logistic regression analyses were performed to evaluate the prognostic reliability of Pv-aCO2, Pcv-aCO2, Pv-aCO2/Ca-vO2, and Pcv-aCO2/Ca-cvO2 for MOMM. MOMM events occurred in 25 patients (22.7%). ROC curve analysis revealed that both postoperative Pv-aCO2/Ca-vO2 and Pcv-aCO2/Ca-cvO2 were significant predictors of MOMM. However, postoperative Pv-aCO2 was the best predictor of MOMM (area under the curve [AUC]: 0.804; 95% confidence interval [CI] 0.688–0.921), at a 5.1-mmHg cut-off, sensitivity was 76.0%, and specificity was 74.1%. Multivariate analysis revealed that postoperative Pv-aCO2 was an independent predictor of MOMM (odds ratio [OR]: 1.42, 95% CI 1.01–2.00, p = 0.046) and prolonged ICU stay (OR: 1.45, 95% CI 1.05–2.01, p = 0.024). Pv-aCO2 at the end of cardiac surgery was a better predictor of postoperative complications than Pv-aCO2/Ca-vO2 and Pcv-aCO2/Ca-cvO2.

Similar content being viewed by others
References
Etzioni DA, Liu JH, Maggard MA, Ko CY. The aging population and its impact on the surgery workforce. Ann Surg. 2003;238:170–7.
Hallqvist L, Martensson J, Granath F, Sahlen A, Bell M. Intraoperative hypotension is associated with myocardial damage in noncardiac surgery: an observational study. Eur J Anaesthesiol. 2016;33:450–6.
Shoemaker WC, Appel PL, Kram HB. Role of oxygen debt in the development of organ failure sepsis, and death in high-risk surgical patients. Chest. 1992;102:208–15.
Aya HD, Cecconi M, Hamilton M, Rhodes A. Goal-directed therapy in cardiac surgery: a systematic review and meta-analysis. Br J Anaesth. 2013;110:510–7.
Holm J, Hakanson E, Vanky F, Svedjeholm R. Mixed venous oxygen saturation predicts short- and long-term outcome after coronary artery bypass grafting surgery: a retrospective cohort analysis. Br J Anaesth. 2011;107:344–50.
Reinhart K, Kuhn HJ, Hartog C, Bredle DL. Continuous central venous and pulmonary artery oxygen saturation monitoring in the critically ill. Intensive Care Med. 2004;30:1572–8.
Perz S, Uhlig T, Kohl M, Bredle DL, Reinhart K, Bauer M, Kortgen A. Low and “supranormal” central venous oxygen saturation and markers of tissue hypoxia in cardiac surgery patients: a prospective observational study. Intensive Care Med. 2011;37:52–9.
Puskarich MA, Trzeciak S, Shapiro NI, Heffner AC, Kline JA, Jones AE. Outcomes of patients undergoing early sepsis resuscitation for cryptic shock compared with overt shock. Resuscitation. 2011;82:1289–93.
van Beest PA, Lont MC, Holman ND, Loef B, Kuiper MA, Boerma EC. Central venous-arterial pCO(2) difference as a tool in resuscitation of septic patients. Intensive Care Med. 2013;39:1034–9.
Vallet B, Pinsky MR, Cecconi M. Resuscitation of patients with septic shock: please “mind the gap”! Intensive Care Med. 2013;39:1653–5.
Futier E, Robin E, Jabaudon M, Guerin R, Petit A, Bazin JE, Constantin JM, Vallet B. Central venous O(2) saturation and venous-to-arterial CO(2) difference as complementary tools for goal-directed therapy during high-risk surgery. Crit Care. 2010;14:R193.
Jakob SM, Kosonen P, Ruokonen E, Parviainen I, Takala J. The Haldane effect—an alternative explanation for increasing gastric mucosal PCO2 gradients? Br J Anaesth. 1999;83:740–6.
Mekontso-Dessap A, Castelain V, Anguel N, Bahloul M, Schauvliege F, Richard C, Teboul JL. Combination of venoarterial PCO2 difference with arteriovenous O2 content difference to detect anaerobic metabolism in patients. Intensive Care Med. 2002;28:272–7.
Ospina-Tascon GA, Hernandez G, Cecconi M. Understanding the venous-arterial CO2 to arterial-venous O2 content difference ratio. Intensive Care Med. 2016;42:1801–4.
Ospina-Tascon GA, Umana M, Bermudez W, Bautista-Rincon DF, Hernandez G, Bruhn A, Granados M, Salazar B, Arango-Davila C, De Backer D. Combination of arterial lactate levels and venous-arterial CO2 to arterial-venous O2 content difference ratio as markers of resuscitation in patients with septic shock. Intensive Care Med. 2015;41:796–805.
Mallat J, Lemyze M, Meddour M, Pepy F, Gasan G, Barrailler S, Durville E, Temime J, Vangrunderbeeck N, Tronchon L, Vallet B, Thevenin D. Ratios of central venous-to-arterial carbon dioxide content or tension to arteriovenous oxygen content are better markers of global anaerobic metabolism than lactate in septic shock patients. Ann Intensive Care. 2016;6:10.
Shroyer AL, Coombs LP, Peterson ED, Eiken MC, DeLong ER, Chen A, Ferguson TB Jr, Grover FL, Edwards FH. The Society of Thoracic Surgeons: 30-day operative mortality and morbidity risk models. Ann Thorac Surg. 2003;75:1856–64. discussion 1864 – 1855.
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148:839–43.
Ospina-Tascon GA, Bautista-Rincon DF, Umana M, Tafur JD, Gutierrez A, Garcia AF, Bermudez W, Granados M, Arango-Davila C, Hernandez G. Persistently high venous-to-arterial carbon dioxide differences during early resuscitation are associated with poor outcomes in septic shock. Crit Care. 2013;17:R294.
Monnet X, Julien F, Ait-Hamou N, Lequoy M, Gosset C, Jozwiak M, Persichini R, Anguel N, Richard C, Teboul JL. Lactate and venoarterial carbon dioxide difference/arterial-venous oxygen difference ratio, but not central venous oxygen saturation, predict increase in oxygen consumption in fluid responders. Crit Care Med. 2013;41:1412–20.
He HW, Liu DW, Long Y, Wang XT. High central venous-to-arterial CO2 difference/arterial-central venous O2 difference ratio is associated with poor lactate clearance in septic patients after resuscitation. J Crit Care. 2016;31:76–81.
Mesquida J, Saludes P, Gruartmoner G, Espinal C, Torrents E, Baigorri F, Artigas A. Central venous-to-arterial carbon dioxide difference combined with arterial-to-venous oxygen content difference is associated with lactate evolution in the hemodynamic resuscitation process in early septic shock. Crit Care. 2015;19:126.
Ospina-Tascon GA, Umana M, Bermudez WF, Bautista-Rincon DF, Valencia JD, Madrinan HJ, Hernandez G, Bruhn A, Arango-Davila C, De Backer D. Can venous-to-arterial carbon dioxide differences reflect microcirculatory alterations in patients with septic shock? Intensive Care Med. 2016;42:211–21.
Teboul JL, Scheeren T. Understanding the Haldane effect. Intensive Care Med. 2017;43:91–3.
Ospina-Tascon GA, Hernandez G, Cecconi M. Understanding the venous-arterial CO to arterial-venous O content difference ratio. Intensive Care Med. 2016;42:1801–4
He H, Liu D. The pseudo-normalization of the ratio index of the venous-to-arterial CO2 tension difference to the arterial-central venous O2 difference in hypoxemia combined with a high oxygen consumption condition. J Crit Care. 2017;40:305–6.
Cuschieri J, Rivers EP, Donnino MW, Katilius M, Jacobsen G, Nguyen HB, Pamukov N, Horst HM. Central venous-arterial carbon dioxide difference as an indicator of cardiac index. Intensive Care Med. 2005;31:818–22.
Suehiro K, Tanaka K, Matsuura T, Funao T, Yamada T, Mori T, Nishikawa K. Discrepancy between superior vena cava oxygen saturation and mixed venous oxygen saturation can predict postoperative complications in cardiac surgery patients. J Cardiothorac Vasc Anesth. 2014;28:528–33.
Morel J, Grand N, Axiotis G, Bouchet JB, Faure M, Auboyer C, Vola M, Molliex S. High veno-arterial carbon dioxide gradient is not predictive of worst outcome after an elective cardiac surgery: a retrospective cohort study. J Clin Monit Comput. 2016;30:783–9.
Guinot PG, Badoux L, Bernard E, Abou-Arab O, Lorne E, Dupont H. Central venous-to-arterial carbon dioxide partial pressure difference in patients undergoing cardiac surgery is not related to postoperative outcomes. J Cardiothorac Vasc Anesth. 2017;31:1190–6.
Funding
Only departmental funds were used for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mukai, A., Suehiro, K., Kimura, A. et al. Comparison of the venous–arterial CO2 to arterial–venous O2 content difference ratio with the venous–arterial CO2 gradient for the predictability of adverse outcomes after cardiac surgery. J Clin Monit Comput 34, 41–53 (2020). https://doi.org/10.1007/s10877-019-00286-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-019-00286-z