
Abstract
Aims/hypothesis
Common genetic variants influence plasma triacylglycerol, HDL-cholesterol (HDL-C) and glucose levels in cross-sectional studies. However, the longitudinal effects of these established variants have not been studied. Our aim was to examine the longitudinal associations of four such variants in the apolipoprotein A-V (APOA5), lipoprotein lipase (LPL), and glucokinase (GCK) genes with fasting glucose or lipid levels.
Methods
The individuals analysed were participants in the Busselton Health Survey (n = 4,554). Cross-sectional analyses of family data used the total association test. Longitudinal association analyses of unrelated participant data (n = 2,864) used linear mixed-effects models.
Results
The findings of cross-sectional association analyses replicated those of previous studies. We observed associations of the G and C alleles at the APOA5 single nucleotide polymorphisms (SNPs) rs662799 and rs3135506 with raised triacylglycerol levels (p = 0.0003 and p < 0.0001, respectively), the 447X allele at the LPL SNP rs328 with reduced triacylglycerol levels (p = 0.0004) and raised HDL-C levels (p = 0.0004), and the A allele of the GCK SNP rs1799884 with raised fasting glucose level (p = 0.015). Longitudinal association analyses showed that most of these associations did not change in the same individuals over an average follow-up time of 17.4 years, though there was some evidence that the association of the 447X allele of rs328 with raised HDL-C level significantly increased with age (p = 0.01), and that the association of the C allele of rs3135506 with raised triacylglycerol level significantly increased over time (p = 0.0007).
Conclusions/interpretation
The current study suggests that the effects of established gene variants on lipid and glucose traits do not tend to alter with age during adulthood or over time.
Similar content being viewed by others

Introduction
There are an increasing number of common genetic variants that are robustly associated with common diseases and quantitative traits. These include variants associated with type 2 diabetes, height, body mass index and inflammatory diseases [1–4]. Variants associated with lipid levels also continue to be identified through ongoing genome-wide association studies [5]. Most variants have been identified through recent genome-wide association studies of cases and controls or using cross-sectional data in population-based studies.
The effects of common variants on key metabolic and cardiovascular phenotypes within individuals as they age have not been well studied. There have been many cross-sectional studies of such genotype–phenotype associations in individuals of different ages [6–10]; however, these studies do not test the possible longitudinal effects of variants in the same individuals. Like the associated risks of many diseases, measures of quantitative traits of clinical relevance often alter with age. Metabolic traits are no exception, with triacylglycerol and glucose levels, body mass index and blood pressure all tending to increase with age [11–13], and HDL-cholesterol (HDL-C) level tending to decrease with age [14]. Very few studies have tested whether variants shown to be associated with these traits in cross-sectional studies have similar associations in the same individuals over time. One study, using 3,877 individuals from the Data from an Epidemiological Study on the Insulin Resistance syndrome (DESIR) cohort, reported possible differential effects of the GCK-30 variant on fasting glucose levels at baseline and after a 9 year follow-up, but there have been few other studies [15].
In this study, we use data from the Busselton Health Survey (BHS), where individuals have been followed up for an average time of 21.2 years (95% CI 13.6–28.8 years) over the last 28 years, with an average of 3.9 measures on each individual, to assess the longitudinal associations of four common variants with metabolic and cardiovascular traits. The variants selected were the apolipoprotein A-V (APOA5) single nucleotide polymorphisms (SNPs) rs662799 and rs3135506; the lipoprotein lipase (LPL) SNP rs328; and the glucokinase (GCK) SNP rs1799884, which have been shown in multiple cross-sectional studies to be associated with triacylglycerol (APOA5 and LPL) [16–21], HDL-C (LPL) [20, 21] and fasting glucose (GCK) [9, 22] levels, traits important in the risk of diabetes and cardiovascular disease.
Methods
Participants
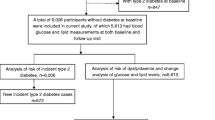
The BHS includes a series of seven cross-sectional population health surveys of adult residents of the Shire of Busselton in the south-west of Western Australia, undertaken between 1966 and 1990, and focused on respiratory and cardiovascular phenotypes [23–25]. In 1994/1995 a cross-sectional community follow-up study, which included the collection of blood for DNA extraction, was undertaken of all survivors of previous surveys. A total of 4,554 individuals participated in this follow-up, including 696 families with a median family size of three. The population is predominantly European–Australian. Population descriptives for individuals surveyed in 1994/1995 in this follow-up are presented in Table 1. A subset of this cohort, selected for longitudinal analysis, comprised 2,864 unrelated individuals who had participated in at least one of the eight cross-sectional surveys while aged between 18 and 80 years. Descriptives for individuals in this subset are presented in Table 2. These individuals had been followed up for a mean time of 21.2 years (95% CI 13.6–28.8 years) (Fig. 1) with an average of 3.9 (SEM 0.04) survey attendances. Fasting glucose, triacylglycerol and HDL-C levels were measured at 7, 6 and 4 time points respectively, with average follow-up times of 19.1, 17.2 and 15.9 years, respectively. All participants gave written informed consent and all study protocols were approved by the Human Research Ethics Committee of the University of Western Australia.

Mean follow-up times (95% CI) by age group at first survey
Clinical measurements
The clinical measurements of individuals in the BHS have been described previously [23, 24]. A self-administered questionnaire was used to record participants’ history of smoking, physician-diagnosed diabetes and use of lipid-lowering medication and insulin injections. Anthropomorphic measurements were taken according to standard clinical procedures. The presence of CHD was determined using the Rose questionnaire, electrocardiogram and self-reported history of physician-diagnosed angina or myocardial infarction. The presence of metabolic syndrome was determined according to the National Cholesterol Education Program Third Adult Panel (NCEP ATP III) criteria.
Laboratory measurements
Lipid levels (HDL-C, LDL-cholesterol (LDL-C) and triacylglycerol concentrations), and fasting plasma glucose and insulin levels were determined from fasting venous blood samples as described previously [26]. Insulin resistance was determined using model-derived estimates of the homeostatic model assessment (HOMA) scores HOMA2-%B (steady-state beta cell function), HOMA2-%S (insulin sensitivity) and HOMA2-IR (insulin resistance) [27, 28], computed by the HOMA Calculator [29].
Genes and genotyping
We selected four variants in three gene regions for analysis. These variants were the APOA5 SNPs rs662799 and rs3135506; the LPL SNP rs328; and the GCK SNP rs1799884. Genomic DNA from all 4,554 study participants was available for genotyping. The SNPs were genotyped using TaqMan probes designed and supplied by Applied Biosystems (Scoresby, VIC, Australia). All primer sequences and experimental conditions are available from the authors on request. Genotyping was performed by the PathWest Molecular Genetics Service (Nedlands, WA, Australia). Percentage call rates were at least 99.6% for all SNPs. Duplicate genotypes were run for ∼10% of participants for all SNPs, with duplicate error rates of less than 0.5% in each case.
Statistical analyses
Genotype frequencies at each SNP locus were tested for deviations from Hardy–Weinberg equilibrium using an exact test implemented in the statistical analysis package, R [30].
Cross-sectional total association analyses were performed on the whole cohort of 4,554 participants using 1994/1995 survey data. The outcome variables HDL-C, LDL-C, triacylglycerol, fasting glucose and fasting insulin levels, HOMA2-%B, HOMA2-%S, HOMA2-IR and BMI were analysed as continuous traits. All but LDL-C were natural log-transformed prior to analysis to achieve a normal distribution. Generalised linear models were used to model the effects of multiple covariates on quantitative outcomes in the unrelated sample, using the SimHap v1.0.0 program (http://www.genepi.org.au/simhap.html). Covariates associated with each outcome were identified from an initial set of relevant phenotypes through stepwise variable selection, so as to ensure that each covariate model included only covariates with independent, significant associations with the outcome, in the population under study. In addition to the full models derived using this procedure, analyses were performed using a simple covariate model including only sex and age as covariates, for comparison.
The total association test (i.e. a general variance components model to partition observed phenotypic variance into genetic and non-genetic components), as implemented in the QTDT v2.6.0 program [31], was used to model the effects of covariates and APOA5, LPL and GCK genotypes on quantitative outcomes within families. Variances between individuals were modelled with environmental, polygenic and additive major-gene-effect variance components. The evidence for population stratification was also evaluated by comparing the between- and within-family components of association in the quantitative transmission disequilibrium test orthogonal model, using the QTDT program. The absence of a significant difference between the two components was taken to indicate that the results for the SNPs analysed were not influenced by any population structure.
Genotype-specific geometric means and 95% confidence intervals were calculated for triacylglycerol and HDL-C levels in unrelated individuals, and fasting glucose levels in unrelated, non-diabetic individuals, in three consecutive age groups (18–40, 41–60 and 61–80 years) using 1994/95 survey data only, to examine whether these traits differed with genotype in different age groups. The geometric mean and geometric standard deviation of a data set can be calculated by taking the antilogarithm of the arithmetic mean and arithmetic standard deviation, respectively, of the log-transformed data values. Geometric confidence intervals are calculated from these values in the same way as arithmetic confidence intervals. Geometric statistics better describe data that, like the triacylglycerol, HDL-C and fasting glucose data, follow a log-normal distribution (i.e. a distribution for which log-transformed values are normally distributed). Therefore, the use of geometric, rather than arithmetic, mean and confidence interval values, was most appropriate for the present analysis. Differences between the geometric means of different genotype groups within each age group were tested for significance using two-tailed t tests.
Full longitudinal association analyses were performed on the sub-cohort of 2,864 unrelated participants aged 18–80 years and, for analyses of the fasting glucose outcome variable only, on the 2,665 non-diabetic participants from this sub-cohort. The longitudinal outcome variables HDL-C, triacylglycerol and fasting plasma glucose levels were natural log-transformed prior to analysis to achieve a normal distribution, and age, age2 and age3 covariates were mean-centred. Longitudinal association analyses were conducted using linear mixed-effects models [32] to incorporate correlation inherent within observations from the same individual, using the SimHap program. This involved the inclusion of time × SNP and/or age × SNP interaction terms in the models. Covariate selection was performed using stepwise elimination. In view of the low minor allele frequencies of the variants, genotypes were coded into two classes (major allele homozygote = 0, heterozygote or minor allele homozygote = 1) and analysed under a dominant genetic model.
Statistical power
All power calculations were performed using the Quanto software, version 1.2.3 [33]. It was determined that for all SNPs, analyses of quantitative phenotypes had at least 90% power at an alpha level of p = 0.05 to detect a difference of 0.07 standard deviations in the case of longitudinal analyses and 0.06 standard deviations in the case of cross-sectional analyses, under a dominant genetic model.
Results
Population characteristics
Genotype sample numbers and allele frequencies are given in Table 3. These frequencies were not different from those expected under Hardy–Weinberg equilibrium for all four SNPs in both study groups. Using the QTDT program, we found no significant evidence that population structure influenced the results for the SNPs analysed.
Cross-sectional association of SNPs with metabolic traits
The results of cross-sectional total association analyses are given in Table 4. In analyses using full covariate models, we observed that the presence of the G and C alleles at the APOA5 SNPs rs662799 and rs3135506, respectively, was associated with raised triacylglycerol levels (p = 0.0003 and p < 0.0001, respectively), that the 447X allele at the LPL SNP rs328 was associated with reduced triacylglycerol levels (p = 0.0004) and raised HDL-C levels (p = 0.0004), and that the A allele of the GCK SNP rs1799884 was associated with raised fasting glucose level (p = 0.015). Similar results were obtained using the simple covariate model, with two exceptions. While analyses using the full covariate model showed no significant association between either rs662799 or rs3135506 and HDL-C levels, analyses using the simple covariate model showed that the presence of the G and C alleles at rs662799 and rs3135506, respectively, was associated with reduced HDL-C levels (p = 0.005 and p = 0.01, respectively). Subsequent analysis indicated that this is likely the result of a correlation between HDL-C and triacylglycerol levels. In analyses of fasting glucose and lipid levels in the unrelated sample at the 1994/95 survey, we observed that rs1799884 explained 0.3% of the variation in fasting glucose level, rs662799, rs3135506 and rs328 explained 0.1%, 0.4% and 0.3% of variation in triacylglycerol level, respectively, and rs328 explained 0.2% of variation in HDL-C level. When rs662799, rs3135506 and rs328 were included together in a multivariate model for the triacylglycerol level outcome, all three remained significantly associated with triacylglycerol level (p = 0.004, p = 0.0002 and p = 0.0008, respectively) and, combined, accounted for 0.7% of the variation in this trait. No significant two-way interactions were observed between combinations of these three SNPs for the triacylglycerol level outcome. Across survey years, using simple models, the percentages of variation in glucose and lipid levels explained by each of the four individual SNPs showed no significant trends and varied by between 0.1% and 1.8%. The geometric means of glucose and lipid levels in different genotype and age groups in unrelated populations are presented in Table 5.
The results of cross-sectional total association analyses performed with additional metabolic outcomes are given in Electronic supplementary material (ESM) Table 1. The presence of the A allele at rs1799884 was found to be associated with reduced fasting insulin level, HOMA2-%B and HOMA2-IR, and raised HOMA2-%S.
Longitudinal association of SNPs with lipid and fasting glucose levels
The results of the longitudinal association analyses are summarised in Table 6. For each phenotype tested, values fitted according to the full covariate, dominant genetic model used for analysis are plotted by genotype group against age in Figs 2 and 3. There was little evidence that the effect sizes of established associations altered with either age during adult life or time over the period from 1975 to 1994/1995. An exception was an association between the age × rs328 interaction term and HDL-C level (p = 0.01), indicating that the presence of the 447X allele at rs328 increases HDL-C levels with increasing age (Fig. 3f). There was no evidence for an association between the time × rs328 interaction term and HDL-C level, indicating that the association between rs328 and HDL-C has not varied over time. A second exception was an association between the time × rs3135506, but not age × rs3135506, interaction term and triacylglycerol level (p = 0.0007). This indicated that the presence of the C allele at rs3135506 has increased triacylglycerol levels over time, without varying this effect with increasing age. Triacylglycerol level was also found to be significantly associated with the year at which it was surveyed, with levels tending to be lower at later survey times. The observed association between the time × rs3135506 interaction term and triacylglycerol level counteracts this trend over time. Similar results were obtained with both the full and simple covariate models. The results of sex-stratified longitudinal association analyses are given in ESM Table 2.

Variation with age of adjusted natural log-transformed fasting glucose values by rs1799884 genotype (black circle, homozygous wild-type; white circle, heterozygote and homozygous mutant) in unrelated, non-diabetic participants aged 18–80 years. Values were fitted using full covariate, dominant genetic models

Variation with age of adjusted natural log-transformed triacylglycerol and HDL-C values by genotype (black circle, homozygous wild-type; white circle, heterozygote and homozygous mutant), in unrelated participants aged 18–80 years, for three SNPs: a, b rs662799; c, d rs3135506; e, f rs328. Values were fitted using full covariate, dominant genetic models
Conclusion
In this study, we investigated the association of variants in the GCK, APOA5 and LPL genes with fasting glucose and lipid levels on a total of 4,554 individuals using both population- and family-based study designs and incorporating both cross-sectional and longitudinal measures. The associations of these variants with fasting glucose and lipid measures in cross-sectional studies are well established but their longitudinal effects in the same individuals followed-up for a long period of time are not known. We used data from a cohort of predominantly European–Australian individuals from the BHS to test the associations of some common variants with longitudinal measures of metabolic and cardiovascular phenotypes. The BHS is a very comprehensively phenotyped resource, with the selected cohort having been followed up on average four times over 21 years with multiple metabolic measures, and thus was well-suited to addressing the aim of this study.
Our cross-sectional association analyses confirmed previous findings of associations between the GCK rs1799884 variant and raised fasting glucose levels [9, 22], the APOA5 rs662799 and rs3135506 variants and raised triacylglycerol levels [16, 17, 34], and the LPL rs328 variant and reduced triacylglycerol levels and raised HDL-C levels [20, 21].
Our graphical presentation of the longitudinal glucose and lipid data with age (Figs 2, 3) show previously reported general trends towards higher fasting glucose and triacylglycerol levels with increasing age [11, 12], which were present for all SNP genotype groups. Though HDL-C has been reported previously to decline with age [14], no strong trend in HDL-C level was observed in this study.
When we examined the genotype–phenotype relationships in longitudinal analyses, we found that the association of the rs328 variant with raised HDL-C level increased with age. An increasing trend in the association between the rs328 mutant allele and HDL-C level is clearly visible across multiple age groups in the plot of fitted HDL-C values in Fig. 3f. This observation is also supported by the HDL-C level geometric means comparison for consecutive age groups in Table 5. Together, these results suggest that while the rs328 mutant allele does not significantly alter HDL-C levels in younger individuals in the 18–40 years age group, its association increases with age until the final 70–80 years age group at which the observation drops off. These results suggest that carriers of one or two 447X alleles are protected from decline in HDL-C, at least in middle to early old age. Further longitudinal studies are needed to confirm if and how the association between HDL-C and rs328 alters in the same individuals as they age.
We found no significant evidence of an interaction between age and rs1799884 on fasting glucose level, between age and either rs328, rs662799 or rs3135506 on triacylglycerol level, or between age and either rs662799 or rs3135506 on HDL-C level, and hence, no evidence that these SNPs are involved in age-related changes in the traits examined. These results are illustrated in the relevant plots of Figs 2 and 3, in which trait values vary with age at similar rates for the two genotype groups, irrespective of shifts related to overall variant associations. In this study, age was not a significant modifier of associations for the majority of variants.
We found no significant evidence that variant associations changed over time, independent of age-related changes, in all but one case. The triacylglycerol-raising association of the rs3135506 variant, which changes a serine residue to tryptophan (S19W), increased over time, indicating that rs3135506 may interact with environmental factors that have changed over the 20 year time period examined, to modify triacylglycerol levels. Such environmental factors could include lifestyle factors such as diet, physical activity and stress level.
Further studies are now required to assess the validity of these findings. One consideration is power. One of the strengths of this study was its ability to consider the same individuals at different ages using longitudinal data. However, with a mean follow-up time of 17.4 years, the study did not follow individuals from youth through to old age. Moreover, though power calculations showed that the dominant model used was adequately powered, there was insufficient power to detect recessive associations. A replication study in a larger cohort would have greater power to detect subtle interactions and would also enable investigation of whether a recessive model of inheritance would give the best fit.
As these findings are restricted to individuals of European ancestry, the results presented here are not necessarily generalisable to other ethnic groups. Replication in other ethnic groups may reveal how the SNPs studied here influence metabolic outcomes in other populations. Furthermore, this study considered the influence of only four variants in three genes involved in type 2 diabetes, though many common variants have been identified to influence metabolic traits and diabetes risk. Additional studies of the interactions between such variants and age would improve understanding of age-related genetic associations in metabolic disorders. However, replication studies will be limited by the available epidemiological databases, few of which contain the multiple metabolic measures collected longitudinally for the BHS.
In conclusion, the results of this study are consistent with previous reports of the effects of GCK, APOA5 and LPL variants on glucose and lipid traits. The effects of established gene variants with lipid and glucose traits do not tend to alter with age, although there is some evidence that the HDL-C-raising effect of the 447X allele of rs328 significantly increases with age.
Abbreviations
- BHS:
-
Busselton Health Survey
- HDL-C:
-
HDL-cholesterol
- HOMA:
-
homeostatic model assessment
- LDL-C:
-
LDL-cholesterol
- SNP:
-
single nucleotide polymorphism
References
Weedon MN, Lettre G, Freathy RM et al (2007) A common variant of HMGA2 is associated with adult and childhood height in the general population. Nat Genet 39:1245–1250
Frayling TM, Timpson NJ, Weedon MN et al (2007) A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 316:889–894
Zeggini E, Weedon MN, Lindgren CM et al (2007) Replication of genome-wide association signals in UK samples reveals risk loci for type 2 diabetes. Science 316:1336–1341
Wellcome Trust Case Control Consortium (2007) Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature 447:661–678
Willer CJ, Sanna S, Jackson AU et al (2008) Newly identified loci that influence lipid concentrations and risk of coronary artery disease. Nat Genet 40:161–169
Endo K, Yanagi H, Araki J, Hirano C, Yamakawa-Kobayashi K, Tomura S (2002) Association found between the promoter region polymorphism in the apolipoprotein A-V gene and the serum triglyceride level in Japanese schoolchildren. Hum Genet 111:570–572
Martin S, Nicaud V, Humphries SE, Talmud PJ (2003) Contribution of APOA5 gene variants to plasma triglyceride determination and to the response to both fat and glucose tolerance challenges. Biochim Biophys Acta 1637:217–225
Dongxia L, Qi H, Lisong L, Jincheng G (2008) Association of peroxisome proliferator-activated receptorgamma gene Pro12Ala and C161T polymorphisms with metabolic syndrome. Circ J 72:551–557
Weedon MN, Clark VJ, Qian Y et al (2006) A common haplotype of the glucokinase gene alters fasting glucose and birth weight: association in six studies and population-genetics analyses. Am J Hum Genet 79:991–1001
Melzer D, Murray A, Hurst AJ et al (2006) Effects of the diabetes linked TCF7L2 polymorphism in a representative older population. BMC Med 4:34
Folsom AR, Jacobs DR Jr, Wagenknecht LE et al (1996) Increase in fasting insulin and glucose over seven years with increasing weight and inactivity of young adults. The CARDIA Study. Coronary Artery Risk Development in Young Adults. Am J Epidemiol 144:235–246
Wilsgaard T, Arnesen E (2004) Change in serum lipids and body mass index by age, sex, and smoking status: the Tromso study 1986–1995. Ann Epidemiol 14:265–273
Auro K, Kristiansson K, Zethelius B et al (2008) USF1 gene variants contribute to metabolic traits in men in a longitudinal 32-year follow-up study. Diabetologia 51:464–472
Derby CA, Feldman HA, Bausserman LL, Parker DR, Gans KM, Carleton RA (1998) HDL cholesterol: trends in two southeastern New England communities, 1981–1993. Ann Epidemiol 8:84–91
Vaxillaire M, Veslot J, Dina C et al (2008) Impact of common type 2 diabetes risk polymorphisms in the DESIR prospective study. Diabetes 57:244–254
Dallinga-Thie GM, van Tol A, Hattori H, van Vark-van der Zee LC, Jansen H, Sijbrands EJ (2006) Plasma apolipoprotein A5 and triglycerides in type 2 diabetes. Diabetologia 49:1505–1511
Lai CQ, Demissie S, Cupples LA et al (2004) Influence of the APOA5 locus on plasma triglyceride, lipoprotein subclasses, and CVD risk in the Framingham Heart Study. J Lipid Res 45:2096–2105
Pennacchio LA, Olivier M, Hubacek JA et al (2001) An apolipoprotein influencing triglycerides in humans and mice revealed by comparative sequencing. Science 294:169–173
Talmud PJ, Hawe E, Martin S et al (2002) Relative contribution of variation within the APOC3/A4/A5 gene cluster in determining plasma triglycerides. Hum Mol Genet 11:3039–3046
Gagne SE, Larson MG, Pimstone SN et al (1999) A common truncation variant of lipoprotein lipase (Ser447X) confers protection against coronary heart disease: the Framingham Offspring Study. Clin Genet 55:450–454
Wung SF, Kulkarni MV, Pullinger CR, Malloy MJ, Kane JP, Aouizerat BE (2006) The lipoprotein lipase gene in combined hyperlipidemia: evidence of a protective allele depletion. Lipids Health Dis 5:19
Weedon MN, Frayling TM, Shields B et al (2005) Genetic regulation of birth weight and fasting glucose by a common polymorphism in the islet cell promoter of the glucokinase gene. Diabetes 54:576–581
Knuiman MW, Cullen KJ, Bulsara MK, Welborn TA, Hobbs MS (1994) Mortality trends, 1965 to 1989, in Busselton, the site of repeated health surveys and interventions. Aust J Public Health 18:129–135
Knuiman MW, Jamrozik K, Welborn TA, Bulsara MK, Divitini ML, Whittall DE (1995) Age and secular trends in risk factors for cardiovascular disease in Busselton. Aust J Public Health 19:375–382
James AL, Palmer LJ, Kicic E et al (2005) Decline in lung function in the Busselton Health Study: the effects of asthma and cigarette smoking. Am J Respir Crit Care Med 171:109–114
Chapman CM, Palmer LJ, McQuillan BM et al (2001) Polymorphisms in the angiotensinogen gene are associated with carotid intimal–medial thickening in females from a community-based population. Atherosclerosis 159:209–217
Levy JC, Matthews DR, Hermans MP (1998) Correct homeostasis model assessment (HOMA) evaluation uses the computer program. Diabetes Care 21:2191–2192
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Diabetes Trials Unit, University of Oxford (2004) HOMA Calculator, Version 2.2.2. Available from http://www.dtu.ox.ac.uk/homa, accessed February 2008
Ihaka R, Gentleman R (1996) R: A language for data analysis and graphics. J Comput Graph Stat 5:299–314
Abecasis GR, Cardon LR, Cookson WO (2000) A general test of association for quantitative traits in nuclear families. Am J Hum Genet 66:279–292
Laird NM, Ware JH (1982) Random-effects models for longitudinal data. Biometrics 38:963–974
Gauderman WJ (2002) Sample size requirements for association studies of gene–gene interaction. Am J Epidemiol 155:478–484
Pennacchio LA, Olivier M, Hubacek JA, Krauss RM, Rubin EM, Cohen JC (2002) Two independent apolipoprotein A5 haplotypes influence human plasma triglyceride levels. Hum Mol Genet 11:3031–3038
Acknowledgements
The authors thank the people of the Busselton Community for their participation in this study, the Busselton Population Medical Research Foundation and the many colleagues who assisted in the collection of these data. We also acknowledge the generous support for the 1994/95 follow-up study from Healthway, Western Australia. The Busselton population studies are supported by The Great Wine Estates of the Margaret River region of Western Australia. We also gratefully acknowledge the assistance of the Western Australian Genetic Epidemiology Resource and the Western Australian DNA Bank (National Health and Medical Research Council of Australia National Enabling Facilities), and the Australian Medical Bioinformatics Resource (a National Health and Medical Research Council of Australia Medical Bioinformatics Genomics Proteomics Program).
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Author information
Authors and Affiliations
Corresponding authors
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Table 1
Results of 1994/95 cross-sectional total association analyses of the whole study population (n = 4,554) (PDF 24 kb)
ESM Table 2
Results of longitudinal association analyses of lipid levels in unrelated men (n = 1,234) and women (n = 1,630) aged 18–80 years, and of fasting glucose level in the subset of non-diabetic participants (men n = 1,128; women n = 1,537) (PDF 38 kb)
Rights and permissions
About this article
Cite this article
Webster, R.J., Warrington, N.M., Weedon, M.N. et al. The association of common genetic variants in the APOA5, LPL and GCK genes with longitudinal changes in metabolic and cardiovascular traits. Diabetologia 52, 106–114 (2009). https://doi.org/10.1007/s00125-008-1175-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-008-1175-9