
Abstract
Purpose
An understanding of the behavior of a new ACL graft in the femoral tunnel during knee motion and external loading can provide information pertinent to graft healing, tunnel enlargement, and graft failure. The purpose of the study was to measure the percentage of the tunnel filled by the graft and determine the amount and location of the graft–tunnel contact with knee motion and under external knee loads.
Methods
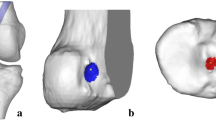
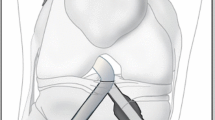
Single bundle anatomical ACL reconstruction was performed on six cadaveric knees. Specimens were positioned with a robotic testing system under: (1) passive flexion–extension, (2) 89-N anterior and posterior tibial loads, (3) 5-N m internal and external torques, and (4) 7-N m valgus moment. The knees were then dissected, repositioned by the robot and the geometry of the femoral tunnel and graft were digitized by laser scanning. The percentage of tunnel filled and the contact region between graft and tunnel at the femoral tunnel aperture were calculated.
Results
The graft occupies approximately 70% of the femoral tunnel aperture and anterior tibial loading tended to reduce this value. The graft contacted about 60% of the tunnel circumference and the location of the graft–tunnel contact changed significantly with knee flexion.
Conclusion
This study found that the graft tends to rotate around the tunnel circumference during knee flexion–extension and contract under knee loading. The “windshield–wiper” and “bungee cord” effect may contribute to femoral tunnel enlargement, affect graft healing, and lead to graft failure. There can be a considerable motion of the graft in the tunnel after surgery and appropriate rehabilitation time should be allowed for graft–tunnel healing to occur. To reduce graft motion, consideration should be given to interference screw fixation or a graft with bone blocks, which may allow an earlier return to activity.







Similar content being viewed by others

References
Amano H, Tanaka Y, Kita K, Uchida R, Tachibana Y, Yonetani Y et al (2019) Significant anterior enlargement of femoral tunnel aperture after hamstring ACL reconstruction, compared to bone-patellar tendon-bone graft. Knee Surg Sports Traumatol Arthrosc 27:461–470
Araki D, Thorhauer E, Tashman S (2018) Three-dimensional isotropic magnetic resonance imaging can provide a reliable estimate of the native anterior cruciate ligament insertion site anatomy. Knee Surg Sports Traumatol Arthrosc 26:1311–1318
Ballmer PM, Jakob RP (1988) The non operative treatment of isolated complete tears of the medial collateral ligament of the knee. A prospective study. Arch Orthop Trauma Surg 107:273–276
Barber FA, Spruill B, Sheluga M (2003) The effect of outlet fixation on tunnel widening. Arthroscopy 19:485–492
Celik H, Kim JH, Lee SH, Lee DH (2021) Femoral tunnel widening via transcondylar cross-pin fixation versus extracortical suspensory fixation after single-bundle ACLR: a systematic review and meta-analysis. Orthop J Sports Med 9:2325967121993811
Cheung P, Chan WL, Yen CH, Cheng SC, Woo SB, Wong TK et al (2010) Femoral tunnel widening after quadrupled hamstring anterior cruciate ligament reconstruction. J Orthop Surg (Hong Kong) 18:198–202
Choi SH, Ha JK, Jun DJ, Seo JG, Park JH (2017) Additional post-tie for unstable femoral suspensory fixation during anterior cruciate ligament reconstruction using TightRope ® RT : clinical reports on 3 cases. Arthrosc Orthop Sports Med 4:34–38
Clatworthy MG, Annear P, Bulow JU, Bartlett RJ (1999) Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc 7:138–145
Cohen SB, Fu FH (2007) Three-portal technique for anterior cruciate ligament reconstruction: use of a central medial portal. Arthroscopy 23(325):e321-325
Daniel DM, Stone ML, Sachs R, Malcom L (1985) Instrumented measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption. Am J Sports Med 13:401–407
Desai VS, Anderson GR, Wu IT, Levy BA, Dahm DL, Camp CL et al (2019) Anterior cruciate ligament reconstruction with hamstring autograft: a matched cohort comparison of the all-inside and complete tibial tunnel techniques. Orthop J Sports Med 7:2325967118820297
Fahey M, Indelicato PA (1994) Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 22:410–414
Fujii M, Sasaki Y, Araki D, Furumatsu T, Miyazawa S, Ozaki T et al (2016) Evaluation of the semitendinosus tendon graft shift in the bone tunnel: an experiemental study. Knee Surg Sports Traumatol Arthrosc 24:2773–2777
Fujimaki Y, Thorhauer E, Sasaki Y, Smolinski P, Tashman S, Fu FH (2016) Quantitative in situ analysis of the anterior cruciate ligament: length, midsubstance cross-sectional area, and insertion site areas. Am J Sports Med 44:118–125
Hoher J, Moller HD, Fu FH (1998) Bone tunnel enlargement after anterior cruciate ligament reconstruction: fact or fiction? Knee Surg Sports Traumatol Arthrosc 6:231–240
Ioria R, Di Sanzo V, Vadala A, Conteduca J, Mazza D, Redler A et al (2013) ACL reconstructions with hamstrings: how different technique and fixation devices influence bone tunnel enlargement. Eur Rev Med Pharmacol Sci 17:2956–2961
Iorio R, Vadala A, Argento G, Di Sanzo V, Ferretti A (2007) Bone tunnel enlargement after ACL reconstruction using autologous hamstring tendons: a CT study. Int Orthop 31:49–55
Jagodzinski M, Foerstemann T, Mall G, Krettek C, Borsch U, Paessler HH (2005) Analysis of forces of ACL reconstructon at the tunnel entrance; is tunnel enlargement a biomechanical problem? J Biomech 38:23–31
Jorgensen U, Thomsen H (2000) Behavior of the graft within the bone tunnels following anterior cruciate ligament reconstruction, studied by cinematic magentic resonance imaging. Knee Surg Sports Traumatol Arthrosc 8:32–35
Kato Y, Ingham SJM, Kramer S, Smolinski P, Saito A, Fu FH (2009) Effect of tunnel position for anatomical single-bundle ACL reconstruction on knee biomechanics in a porcine model. Knee Surg Sports Traumatol Arthrosc 18:2–10
L’Insalata JC, Klatt B, Fu FH, Harner CD (1997) Tunnel expansion following anterior cruciate ligament reconstruction: a comparison of hamstring and patellar tendon autographs. Knee Surg Sports Traumatol Arthrosc 5:234–238
Lanzetti RM, Lupariello D, De Carli A, Monaco E, Guzzini M, Fabbri M et al (2017) Can the outside-in half-tunnel technique reduce femoral tunnel widening in anterior cruciate ligament reconstruction? A CT study. Eur J Orthop Surg Traumatol 27:659–664
Lee BH, Bansal S, Park SH, Wang JH (2015) Eccentric graft positioning within the femoral tunnel aperature in anatomic double-bundle anterior cruciate ligament reconstruction using the transportal and outside-in techniques. Am J Sports Med 43:1180–1188
Lee BH, Seo DY, Bansal S, Kim JH, Ahn JH, Wang JH (2016) Comparative magnetic resonance imaging study of the cross-sectional area of anatomic double bundle ligament reconstruction grafts and the contralateral uninjured KNN. Arthroscopy 32:321–329
Mutsuzaki H, Kinugasa T, Ikeda K, Sakane M (2019) Morphological changes in the femoral and tibial bone tunnels after anatomic single-bundle anterior cruciate ligament reconstruction using a calcium phosphate-hybridized tendon graft in 2 years of follow-up. Orthop Traumatol Surg Res 105:653–660
Nebelung W, Becker R, Merkel M, Ropke M (1998) Bone tunnel enlargement after anterior cruciate ligament reconstruction with semitendinosus tendon using endobutton fixation on the femoral side. Arthroscopy 14:810–815
Onodera J, Yasuda K, Masuda T, Tanabe Y, Kitamura N, Yagi T et al (2017) Is the grafted tendon shifted anteriorly in the femoral tunnel at the postremodeling phase after anterior cruciate ligament reconstruction? A clinical MRI study. Orthop J Sports Med 5:2325967117711120
Rahnemai-Azar AA, Sabzevari S, Irarrazaval S, Chao T, Fu FH (2016) Anatomical individualized ACL reconstruction. Arch Bone Jt Surg 4:291–297
Rangger C, Daniel DM, Stone ML, Kaufman K (1993) Diagnosis of an ACL disruption with KT-1000 arthrometer measurements. Knee Surg Sports Traumatol Arthrosc 1:60–66
Sasaki Y, Chang SS, Fujii M, Araki D, Zhu J, Marshall B et al (2016) Effect of fixation angle and graft tension in double-bundle anterior cruciate ligament reconstruction on knee biomechanics. Knee Surg Sports Traumatol Arthrosc 24:2892–2898
Schiavone Panni A, Denti M, Franzese S, Monteleone M (1993) The bone-ligament junction: a comparison between biological and artificial ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 1:9–12
Silva A, Sampaio R, Pinto E (2010) Femoral tunnel enlargement after anatomic ACL reconstruction: a biological problem? Knee Surg Sports Traumatol Arthrosc 18:1189–1194
Surer L, Michail K, Koken M, Yapici C, Zhu J, Marshall BD et al (2017) The effect of anterior cruciate ligament graft rotation on knee biomechanics. Knee Surg Sports Traumatol Arthrosc 25:1093–1100
Suzuki T, Shino K, Otsubo H, Suzuki D, Mae T, Fujimiya M et al (2014) Biomechanical comparison between the rectangular-tunnel and the round-tunnel anterior crucciate ligament reconstruction procedures with a bone-patellar tendon-bone graft. Arthroscopy 30:1294–1302
Tachibana Y, Mae T, Shino K, Ohori T, Amano H, Yoshikawa H et al (2018) Femoral tunnel enlargement after anatomic anterior cruciate ligament reconstruction: bone-patellar tendon-bone/single rectangular tunnel versus hamstring tendon/double tunnels. J Orthop Sci 23:1011–1018
Tang X, Marshall B, Wang JH, Zhu J, Li J, Smolinski P et al (2019) Lateral meniscal posterior root repair with anterior cruciate ligament reconstruction better restores knee stability. Am J Sports Med 47:59–65
Tsuda E, Fukuda Y, Loh JC, Debski R, Fu FH, Woo SL (2002) The effect of soft-tissue graft fixation in anterior cruciate ligament recontruction on graft-tunnel motion under anterior tibial loading. Arthroscopy 18:960–967
Vignos MF, Smith CR, Roth JD, Kaiser JM, Baer GS, Kijowski R et al (2020) Anterior cruciate ligament graft tunnel placement and graft angle are primary determinants of internal knee mechanics after reconstructive surgery. Am J Sports Med 48:3503–3514
Wilson TC, Kantaras A, Atay A, Johnson DL (2004) Tunnel enlargement after anterior cruciate ligament surgery. Am J Sports Med 32:543–549
Woo SL, Debski RE, Withrow JD, Janaushek MA (1999) Biomechanics of knee ligaments. Am J Sports Med 27:533–543
Woo SL, Fisher MB (2009) Evaluation of knee stability with use of a robotic system. J Bone Joint Surg Am 91(Suppl 1):78–84
Funding
No external funding was received for this study.
Author information
Authors and Affiliations
Contributions
JZ and BM carried out the study and participated in data collection and interpretation. XT provided technical support and design. ML participated in study conception and design, provided critical revision of the manuscript. FF and PS helped in the analysis and interpretation of data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
Institutional approval (Committee for Oversight of Research and Clinical Training Involving Decedents #453) was obtained.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhu, J., Marshall, B., Tang, X. et al. ACL graft with extra-cortical fixation rotates around the femoral tunnel aperture during knee flexion. Knee Surg Sports Traumatol Arthrosc 30, 116–123 (2022). https://doi.org/10.1007/s00167-021-06703-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06703-8