
Abstract
Background
The surgical management of multinodular goiter is the treatment of choice for the majority of cases. There is controversy between radical resection with the lifelong thyroxine substitution and function-preserving resection with the risk for recurrence, and the complications associated with total thyroidectomy.
Objective
The aim of the present study was to compare the outcome of total thyroidectomy (TT) in comparison with subtotal thyroidectomy (ST) as regards hypocalcemia, transient nerve injury, and recurrence rate.
Patients and methods
This study included published English medical articles in the last 20 years, concerning the treatment of multinodular goiter.
Results
Meta-analysis was for the evaluation of surgical outcomes after surgical management of multinodular goiter including total thyroidectomy versus subtotal thyroidectomy by comparing the TT versus ST in our study including 23 studies included of the total number of patients (4485) who underwent subtotal thyroidectomy versus the total number of patients (7116) who underwent total thyroidectomy; a comparison was done as regards postoperative complications including RLN injury (transient or permanent), rate of recurrence, need for reoperation, and incidence of postoperative hypocalcemia. The incidence of RLN injury is lower in ST compared to TT, and its recurrence is much lower in TT than in ST.
Conclusion
This meta-analysis showed that the advantages of total thyroidectomy include adequate eradication of the disease, prevention of recurrent goiter, and avoidance of the need for completion surgery in case of occult malignancy, but it is associated with higher morbidity (postoperative thyroidectomy complications: RLN palsy and hypoparathyroidism) and the need for lifelong replacement therapy (L-thyroxin supplementation).
Similar content being viewed by others


Background
Surgical management of multinodular goiter is still controversial [1], Among surgical approaches include total thyroidectomy and subtotal thyroidectomy [2].
Aim of the work
The aim of this work was to compare the outcome of total thyroidectomy in comparison with subtotal thyroidectomy as regards hypoparathyroidism, RLN injury, and recurrence rate.
Patients and methods
The study was done in the following steps:
-
Determination of the target disease.
-
Identification and location of articles.
-
Screening and evaluation of articles.
-
Data collection.
-
Data analysis.
-
Reporting and interpretation (Results).
-
Discussion and conclusion.
Target subject
The target is to compare two techniques of thyroidectomy in the treatment of multinodular goiter, total thyroidectomy, and subtotal thyroidectomy as regards postoperative complications and recurrence.
Identification and location of articles
Studies included published medical articles about the advantages and disadvantages of each total thyroidectomy and subtotal thyroidectomy through searching the MEDLINE database (www.pubmed.com) using the following keywords in different combinations:
-
Total thyroidectomy
-
Subtotal thyroidectomy
-
Multinodular goiter
-
Postoperative complication
-
Multinodular goiter recurrence
-
Incidental thyroid cancer
Over 8000 articles were found. After customizing the date, age, and language, they narrowed to about 3796 articles, and after the exclusion of non-relevant articles of 3780, about 16 relevant articles were found. By application of inclusion criteria, 6 articles were found meeting the inclusion criteria and can undergo meta-analysis.
Screening and evaluation
The screening form of articles was used by the investigators to screen the articles, which were yielded by the MEDLINE search after blinding the author name and journal name. The screen form of the articles is as follows:
-
1)
Irrelevant articles: articles that may have one of the keywords but a different purpose from our study (3780).
-
2)
Relevant articles: after the exclusion of repeated and non-relevant articles, articles that contain one or more of the above keywords (16).
-
3)
Included articles: These are 6 articles that fulfilled the following inclusion criteria and were included for further steps of data collection, analysis, and reporting (Table 1):
-
Published in the English language.
-
Since January 1996 till May 2020.
-
Conducted on human subjects.
-
Adults more than 18 years
-
All patients are euthyroid.
-
No patients with suspicion of thyroid malignancy.
-
Only randomized clinical trial, retrospective, and prospective studies.
-
No articles with different outcome measures.
Table 1 Included articles -
-
4)
Excluded articles: Articles that miss one or more of the above mentioned inclusion criteria (10).
The following table will show the excluded articles and the reason for exclusion Table 2:
Data collection
Information was gathered for each individual study on total thyroidectomy and subtotal thyroidectomy in the treatment of multinodular goiter, and we extracted data from them (postoperative complications and recurrence).
Data analysis
Statistical methods
Statistical analysis was done using Comprehensive Meta Analysis© version 2 (Biostat™, NJ, USA).
Testing for heterogeneity
Studies included in the meta-analysis were tested for heterogeneity of the estimates using the following tests:
-
1.
Cochran Q chi-square test: A statistically significant test (p value < 0.1) denoted heterogeneity among the studies.
-
2.
I-squared (I2) index which is calculated as follows: \({I}^{2}= \left(\frac{Q-df}{Q}\right)*100\mathrm{\%}\). The I-squared is interpreted as follows:
-
■ 0 to 40%: might not be important
-
■ 30 to 60%: may represent moderate heterogeneity
-
■ 50 to 90%: may represent substantial heterogeneity
-
■ 75 to 100%: considerable heterogeneity
-
Effect size estimation
The effect size for binary outcomes was expressed as relative risk (RR) with its 95% confidence limits (95% CI).
Pooling of estimates
Estimates from included studies were pooled using both the Mantel–Haenszel fixed-effects method (FEM) and the DerSimonia Laird random-effects method (REM). In the absence of significant heterogeneity, the FEM was considered; otherwise, the REM was considered.
Examination of publication bias
Publication bias was assessed by examination of funnel plots. A funnel plot is a plot of the estimated effect size (RR) on the horizontal axis versus the standard error (SE) for the effect size as a measure of study size on the vertical axis.
Large studies appear toward the top of the graph and tend to cluster near the mean effect size. Smaller studies appear toward the bottom of the graph and (since there is more sampling variation in effect size estimates in the smaller studies) will be dispersed across a range of values.
In the absence of publication bias, the studies are expected to be distributed symmetrically about the combined effect size. By contrast, in the presence of bias, it is expected that the bottom of the plot would show a higher concentration of studies on one side of the mean than the other. This would reflect the fact that smaller studies (which appear toward the bottom) are more likely to be published if they have larger-than-average effects, which makes them more likely to meet the criterion for statistical significance.
Level of significance
A two-sided p value < 0.05 denoted statistical significance.
Results
Meta-analysis of the overall incidence of RLN palsy
There is no evidence for heterogeneity among the included studies (Q = 4.887, DF = 4, P value 0.299, I2 = 18.14%) pooling of the studies using fixed effects showed a relative risk of 1.6 with 95% CI of 1.27 to 2.02 which was statistically significant (> 0.001).
Table 3 shows the results of the meta-analysis of the overall incidence of RLN palsy.
There is no evidence for heterogeneity among the included studies (Q = 4.887, DF = 4, P value 0.299, I2 = 18.14%).
Pooling of the studies using fixed effects showed a relative risk of 1.6 with a 95% CI of 1.27 to 2.02 which was statistically significant (> 0.001).
Meta-analysis of the incidence of permanent RLN palsy
No evidence for heterogeneity among the included studies (Q = 4.887, DF = 4, P value 0.2991, I2 = 18.14%) pooling of the studies using fixed effects showed a relative risk of 1.31 with 95% CI of 0.91 to 1.89 which was statistically not significant (p value 0.149).
Table 4 shows the results of the meta-analysis of the incidence of permanent RLN palsy.
There is no evidence for heterogeneity among the included studies (Q = 4.887, DF = 4, P value 0.2991, I2 = 18.14%).
Pooling of the studies using fixed effects showed a relative risk of 1.31 with a 95% CI of 0.91 to 1.89 which was statistically not significant (p value 0.149).
A funnel plot for the incidence of permanent RLN palsy was done. There is evidence for publication bias.
Meta-analysis of incidence of temporary RLN palsy
No evidence for heterogeneity among the included studies (Q = 7.060, DF = 4, P value 0.133, I2 = 43.34%) pooling of the studies using fixed effects showed a relative risk of 1.828 with 95% CI of 1.36 to 2.46 which was statistically significant (p value > 0.001).
Table 5 shows the results of the meta-analysis of the incidence of temporary RLN palsy.
No evidence for heterogeneity among the included studies (Q = 7.060, DF = 4, P value 0.133, I2 = 43.34%).
Pooling of the studies using fixed effects showed a relative risk of 1.828 with a 95% CI of 1.36 to 2.46 which was statistically significant (p value > 0.001).
A funnel plot for the incidence of temporary RLN palsy was done. There is evidence of publication bias.
Meta-analysis of the overall incidence of hypoparathyroidism
There is evidence for heterogeneity among the included studies (Q = 66.065, DF = 4, P value > 0.0001, I2 = 93.95%) pooling of the studies using random effects showed a relative risk of 1.30 with 95% CI of 1.20 to 1.41 which was statistically significant (p value 0.036).
Table 6 shows the results of the meta-analysis of the overall incidence of hypoparathyroidism.
There is evidence for heterogeneity among the included studies (Q = 66.065, DF = 4, P value > 0.0001, I2 = 93.95%).
Pooling of the studies using random effects showed a relative risk of 1.30 with a 95% CI of 1.20 to 1.41 which was statistically significant (p value 0.036).
A funnel plot for the overall incidence of hypoparathyroidism was done. There is evidence of publication bias.
Meta-analysis of the incidence of permanent hypoparathyroidism
No evidence for heterogeneity among the included studies (Q = 0.883, DF = 4, P value 0.927, I2 = 0.00%) pooling of the studies using fixed effects showed a relative risk of 1.48 with 95% CI of 1.11 to 1.96 which was statistically significant (p value 0.007).
Table 7 shows the results of a meta-analysis of the incidence of permanent hypoparathyroidism.
There is no evidence for heterogeneity among the included studies (Q = 0.883, DF = 4, P value 0.927, I2 = 0.00%).
Pooling of the studies using fixed effects showed a relative risk of 1.48 with a 95% CI of 1.11 to 1.96 which was statistically significant (p value 0.007).
A funnel plot for the incidence of permanent hypoparathyroidism was done. There is evidence of publication bias.
Meta-analysis of Incidence of temporary hypoparathyroidism
There is evidence for heterogeneity among the included studies (Q = 66.517, DF = 4, P value > 0.0001, I2 = 93.99%) pooling of the studies using random effects showed a relative risk of 2.389 with 95% CI of 1.02 to 5.61 which was statistically significant (p value 0.046).
Table 8 shows the results of the meta-analysis of the incidence of temporary hypoparathyroidism.
There is evidence for heterogeneity among the included studies (Q = 66.517, DF = 4, P value > 0.0001, I2 = 93.99%).
Pooling of the studies using random effects showed a relative risk of 2.389 with a 95% CI of 1.02 to 5.61 which was statistically significant (p value 0.046).
A funnel plot for the incidence of temporary hypoparathyroidism was done. There is evidence of publication bias.
Meta-analysis of the incidence of recurrence
There is evidence for heterogeneity among the included studies (Q = 13.484, DF = 4, P value 0.009, I2 = 70.34%) pooling of the studies using random effects showed a relative risk of 0.013 with 95% CI of 0.002 to 0.11 which was a statistically significant p value of > 0.001.
Table 9 shows the results of the meta-analysis of the incidence of recurrence.
There is evidence for heterogeneity among the included studies (Q = 13.484, DF = 4, P value 0.009, I2 = 70.34%).
Pooling of the studies using random effects showed a relative risk of 0.013 with a 95% CI of 0.002 to 0.11 which was statistically significant (p value > 0.001).
A funnel plot for the incidence of recurrence was done. There is evidence of publication bias.
Discussion
Surgical management is considered the treatment of choice for multinodular goiter [19]. Several surgical procedures for MNG, including subtotal thyroidectomy and total thyroidectomy. The postoperative complications (transient/permanent hypocalcemia and transient/permanent RLN palsy) and recurrences are regarded as the assessment of the balance between TT (total thyroidectomy) and ST (subtotal thyroidectomy) is still controversial [20, 21], and more recent studies have shown comparison of both surgical approaches regarding the postoperative complications [22].
Increasing numbers of total thyroidectomies are being performed, and the indications for this procedure include thyroid cancer, Graves’ disease, and multinodular goiter [23]. As it completely eradicates the disease process and lowers the local recurrence rate, it avoids the need for completion thyroidectomy with minimal risk of morbidity [24].
In this study, we compare the outcome of total thyroidectomy in comparison with subtotal thyroidectomy as regards hypocalcemia, hypothyroidism, recurrence rate, and RLN injury.
As regards RLN palsy, there is a higher incidence in total over subtotal in temporary and permanent RLN palsy with a P value < 0.001 which is statistically significant.
As regards postoperative hypoparathyroidism, there is a higher incidence in total over subtotal in postoperative hypoparathyroidism whether it is temporary or permanent, with a P value < 0.001 which is statistically significant.
As regards recurrence, there is a higher incidence in subtotal over the total in the overall incidence of recurrence with a P value < 0.001 which is statistically significant.
Ozbas et al. reported that the incidence rate of recurrence of MNG after bilateral subtotal thyroidectomy ranges between 1.2% [16], Delbridge reported that subtotal thyroidectomy for benign thyroid disease has been performed for more than a century and that it may reduce the associated risk of postoperative hypocalcemia and recurrent laryngeal nerve (RLN) palsy [25]. Most surgeons still argue whether the potential risk of total thyroidectomy (TT) outweighs the potential benefits [26].
Regarding the RLN injury postoperative either transient or permanent our study showed a statistically significant difference between subtotal thyroidectomy over total thyroidectomy as in subtotal thyroidectomy, we avoid dissection over RLN or using excessive diathermy also keep in mind most of them are neuropraxia, nerve traction, or edema resolving by the time.
Among included studies, the results showed that subtotal thyroidectomy has improved transient hypothyroidism and permanent hypothyroidism over total thyroidectomy with preservation of the posterolateral part to avoid postoperative hypothyroidism and the need for replacement therapy.
TT has become a preferred surgical procedure for MNG for the majority of surgeons because it eliminates the risk of recurrence, and there is no need for reoperation [26]. A lot of data has been published indicating the equal incidence of both transient/permanent RLN palsy and transient/permanent hypocalcemia for subtotal thyroidectomy and total thyroidectomy [27].
Regarding the recurrence rate, the subtotal thyroidectomy showed less significance than total thyroidectomy as total thyroidectomy ablates any remaining tissue [28].
Conclusion
This meta-analysis showed that the advantages of total thyroidectomy include adequate eradication of the disease, prevention of recurrent goiter, and avoidance of the need for completion surgery in case of occult malignancy, but it is associated with higher morbidity (postoperative thyroidectomy complications: RLN palsy and hypoparathyroidism) and the need for lifelong replacement therapy (L-thyroxin supplementation).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- TT:
-
Total thyroidectomy
- ST:
-
Subtotal thyroidectomy
- RLN:
-
Recurrent laryngeal nerve
- MNG:
-
Multinodular goiter
References
Khadra M, Delbridge L, Reeve TS, Poole AG, Crummer P (1992) Total thyroidectomy: its role in management of thyroid disease. Aust N Z J Surg 62:91–95
Duren M, Yavuz N, Bukey Y et al (2000) Impact of initial surgical treatment on survival of patients with differentiated thyroid cancer: experience of an endocrine surgery center in an iodine deficient region. World J Surg 24:1290–1294
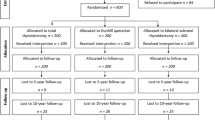
Barczyński M, Konturek A, Hubalewska-Dydejczyk A, Gołkowski F, Cichoń S, Nowak W (2010) Five-year follow-up of a randomized clinical trial of total thyroidectomy versus Dunhill operation versus bilateral subtotal thyroidectomyfor multinodular nontoxic goiter. World J Surg 34(6):1203–13
Yang W, Shao T, Ding J, Jin X, Li Q, Chu PG, Yen Y, Qiu W (2009) The feasibility of total or near-total bilateral thyroidectomy for the treatment of bilateral multinodular goiter. J Invest Surg 22(3):195–200
Pappalardo G, Guadalaxara A, Frattaroli FM, Illomei G, Falaschi P (1988) Total compared with subtotal thyroidectomy in benign nodular disease: personal series and review of published reports. Eur J Surg 164(7):501–6
Delbridge L, Guinea AI, Reeve TS (1999) Total thyroidectomy for bilateral benign multinodular goiter: effect of changing practice. Arch Surg 134(12):1389–93
Tezelman S, Borucu I, Senyurek Giles Y, Tunca F, Terzioglu T (2009) The change in surgical practice from subtotal to near-total or total thyroidectomy in the treatment of patients with benign multinodular goiter. World J Surg 33(3):400–5
Vaiman M, Nagibin A, Hagag P, Buyankin A, Olevson J, Shlamkovich N (2008) Subtotal and near total versus total thyroidectomy for the management of multinodular goiter. World J Surg 32(7):1546–51
Cirocchi R,TrastulliS, Randolph J, Guarino S, DiRocco G, Arezzo A, D’Andrea V, Santoro A, Barczyñski M, Avenia N (2015) Total or near-total thyroidectomy versus subtotal thyroidectomy for multinodular non-toxic goitre in adults. Cochrane Database Syst Rev 7;(8):CD010370.
Citgez B, Uludag M, Yetkin G, Yener F, Akgun I, Isgor A (2013) Changes in the choice of thyroidectomy for benign thyroid disease. Surg Today 43(6):625–31
Barczyński M, Konturek A, Stopa M, Cichoń S, Richter P, Nowak W (2011) Total thyroidectomy for benign thyroid disease: is it really worthwhile? Ann Surg 254(5):724–29
Albayrak Y, Demiryilmaz I, Kaya Z, Aylu B, Güzel C, Ozcan O, Aslan S, Yenisolak A, Ozturk M, Celik S (2011) Comparison of total thyroidectomy, bilateral subtotal thyroidectomy and Dunhill operations in the treatment of benign thyroid disorders. Minerva Chir 66(3):189–95
Koyuncu A, Dökmetas HS, Turan M, Aydin C, Karadayi K, Budak E, Gökgöz S, Sen M (2003) Comparison of different thyroidectomy techniques for benign thyroid disease. Endocr J 50(6):723–7
Karamanakos SN, Markou KB, Panagopoulos K, Karavias D, Vagianos CE, Scopa CD, Fotopoulou V, Liava A, Vagenas K (2010) Complications and risk factors related to the extent of surgery in thyroidectomy. Results from 2,043 procedures. Hormones (Athens) 9(4):318–25
Riju R, Jadhav S, Kanthaswamy R, Jacob P, Nair CG (2009) Is total thyroidectomy justified in multi-nodular goitre. J Indian Med Assoc 107(4):223–5
Ozbas S, Kocak S, Aydintug S et al (2005) Comparison of the complications of subtotal, near total and total thyroidectomy in the surgical management of multinodular goitre. Endocr J 52:199–205
Colak T, Akca T, Kanik A, Yapici D, Aydin S (2004) Total versus subtotal thyroidectomy for the management of benign multinodular goiter in an endemic region. ANZ J Surg 74(11):974–8
Giles Y, Boztepe H, Terzioglu T, Tezelman S (2004) The advantage of total thyroidectomy to avoid reoperation for incidental thyroid cancer in multinodular goiter. Arch Surg 139(2):179–82
Werga-Kjellman P, Zedenius J, Tallstedt L et al (2001) Surgical treatment of hyperthyroidism: a ten-year experience. Thyroid 11:187–192
Barakate MS, Agarwal G, Reeve TS et al (2002) Total thyroidectomy is now the preferred option for the surgical management of Graves’ disease. ANZ J Surg 72:321–324
Guo Z, Yu P, Liu Z et al (2013) Total thyroidectomy vs bilateral subtotal thyroidectomy in patients with Graves’ diseases: a meta-analysis of randomized clinical trials. Clin Endocrinol (Oxf) 79:739–746
Zambudio AR, Rodríguez J, Riquelme J et al (2004) Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. Ann Surg 240:18–25
Mishra A, Agarwal A, Agarwal G et al (2001) Total thyroidectomy in benign thyroid disorders in an endemic region. World J Surg 25:307–310
Delbridge L (2008) Symposium on evidence-based endocrine surgery (2): benign thyroid disease. World J Surg 32:1235–1236
Delbridge L (2003) Total thyroidectomy: the evolution of surgical technique. ANZ J Surg 73:761–768
Liu Q, Djuricin G, Prinz RA (1998) Total thyroidectomy for benign thyroid disease. Surgery 123:2–7
Bellantone R, Lombardi CP, Bossola M et al (2002) Total thyroidectomy for management of benign thyroid disease: review of 526 cases. World J Surg 26:1468–1471
Agarwal G, Aggarwal V (2008) Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based review World J Surg 32:1313–1324
Acknowledgements
Not applicable.
Funding
This research is entirely funded by the authors.
Author information
Authors and Affiliations
Contributions
Dr. Ahmed Kamel had the idea of this study, supervised the statistical analysis, and contributed to the writing of the paper (corresponding author). Dr. Mohamed Kamel put together the research plan and statistical analysis and contributed to the writing of the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kamel, A.A., Kamel, M. Total thyroidectomy versus subtotal thyroidectomy in treatment of multinodular goiter: a meta-analysis. Egypt J Otolaryngol 40, 3 (2024). https://doi.org/10.1186/s43163-023-00553-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-023-00553-6