
Abstract
Background
Although total thyroidectomy is the procedure of choice in patients with thyroid carcinoma, this surgical approach has emerged as a surgical option to treat patients with benign multinodular goiter (BMNG), especially in endemically iodine-deficient regions. The aim of this study was to review our experience with patients with BMNG in an endemically iodine-deficient region treated by either subtotal or total/near-total thyroidectomy, and to document whether total or near-total thyroidectomy decreased the rate of completion thyroidectomy for incidentally diagnosed thyroid carcinoma in comparison to the patients with BMNG treated initially by subtotal thyroidectomy.
Methods
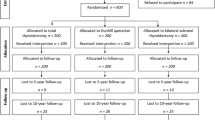
Two thousand five hundred ninety-two patients with BMNG were included. There were 1695 bilateral subtotal thyroidectomies (group 1) and 1211 total or near-total thyroidectomies (group 2) for BMNG during this period. All patients were euthyroid and had no history of hyperthyroidism, radiation exposure, or familial thyroid carcinoma. Any patient with preoperative or perioperative suspicion of malignancy or hyperthyroidism was excluded.
Results
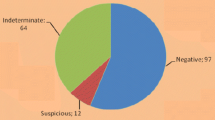
Bilateral subtotal thyroidectomy was performed in 1695 patients (58.3%) in group 1 and total or near-total thyroidectomy in 1211 patients (41.7%), in group 2, respectively. The incidence of incidental thyroid carcinoma was found to be 7.2% (n = 210/2906). Although the rate of permanent hypoparathyroidim and transient or permanent unilateral recurrent laryngeal nerve (RLN) palsy were not significantly different between the two groups, transient hypoparathyroidism was significantly higher in group 2 than in group 1 (8.4% vs. 1.42%; p < 0.001, odds ratio [OR] = 52.98). The incidence of thyroid carcinoma was significantly higher in group 2 (10.7%, n = 129/1211) than in group 1 (4.68%, n = 81/1695) (p < 0.001; OR = 39.1).Thirty-eight patients in group 1 (2.24%) underwent completion thyroidectomy, whereas completion thyroidectomy has been not indicated in group 2 (p = 0.007). Two of 38 patients (5.26%) had thyroid papillary microcarcinoma on their remnant thyroid tissue. The rate of recurrent goiter was 7.1% in group 1. The average time to recurrence in group 1 was 14.9 ± 8.7 years. Six of 121 patients with recurrent disease (4.95%) has been operated on.
Conclusions
Subtotal thyroidectomy resulted in a significantly higher rate of completion thyroidectomy for incidentally diagnosed thyroid carcinoma compared with total or near-total thyroidectomy in patients with BMNG. The extent of surgical resection had no significant effect on the rate of permanent complications. We recommend total or near-total thyroidectomy in BMNG to prevent recurrence and to eliminate the necessity for early completion thyroidectomy in case of a final diagnosis of thyroid carcinoma.


Similar content being viewed by others

References
Siragusa G, Lanzara P, Di Pace G (1998) Subtotal thyroidectomy or total thyroidectomy in the treatment of benign thyroid disease: our experience [in Italian]. Minerva Chir 53:233–238
Reeve TS, Delbribge L, Cohen A, Crummer P (1987) Total thyroidectomy: the preferred option for multinodular goiter. Ann Surg 206:782–786
Delbridge L, Guinea AI, Reeve TS (1999) Total thyroidectomy for bilateral benign multinodular goiter: effect of changing practice. Arch Surg 134:1389–1393
Jacobs JK, Aland JW Jr, Ballinger JF (1983) Total thyroidectomy: a review of 213 patients. Ann Surg 197:542–549
Pappalardo G, Guadalaxara A, Frattaroli FM, Illomei G, Falaschi P (1998) Total compared with subtotal thyroidectomy in benign nodular disease: personal series and review of published reports. Eur J Surg 164:501–506
Liu Q, Djuricin G, Prinz RA (1998) Total thyroidectomy for benign thyroid disease. Surgery 123:2–7
Mishra A, Agarwal A, Agarwal G, Mishra SK (2001) Total thyroidectomy in benign thyroid disorders in an endemic region. World J Surg 25:307–310
Gough IR, Wilkinson D (2000) Total thyroidectomy for management of thyroid disease. World J Surg 24:962–965
Wheeler MH (1998) Total thyroidectomy for benign thyroid disease. Lancet 351:1526–1527
Reeve TS, Delbridge L, Brady, Crummer P, Smyth C (1988) Secondary thyroidectomy: a twenty-year experience. World J Surg 12:449–453
Pezzullo L, Delrio P, Losito NS, Caraco C, Mozzillo N (1997) Post-operative complications after completion thyroidectomy for differentiated thyroid cancer. Eur J Surg Oncol 23:215–218
Bergamaschi R, Becouarn G, Ronceray J, Arnaud JP (1998) Morbidity of thyroid surgery. Am J Surg 176:71–75
Wilson DB, Staren ED, Prinz RA (1998) Thyroid reoperations: indications and risks. Am Surg 64:674–678
Beahrs OH, Vandertoll DJ (1963) Complications of secondary thyroidectomy. Surg Gynecol Obstet 117:535–539
McCall A, Jarosz H, Lawrence AM, Paloyan E (1986) The incidence of thyroid carcinoma in solitary cold nodules and in multinodular goiters. Surgery 100:1128–1132
Koh KBH, Chang KW (1992) Carcinoma in multinodular goitre. Br J Surg 79:266–267
Chao TC, Jeng LB, Lin JD, Chen MF (1997) Reoperative thyroid surgery. World J Surg 21:644–647
Gould EA, Hirsch E, Brecher I (1965) Complications arising in the course of thyroidectomy. Arch Surg 90:81–85
Foster RS Jr (1978) Morbidity and mortality after thyroidectomy. Surg Gynecol Obstet 146:423–429
Thomusch O, Machens A, Sekulla C et al (2000) Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: prospective multicenter study in Germany. World J Surg 24:1335–1341
Giles Y, Boztepe H, Terzioglu T, Tezelman S (2004) The advantage of total thyroidectomy to avoid reoperation for incidental thyroid cancer in multinodular goiter. Arch Surg 139:179–182
Calabro S, Auguste LJ, Attie JN (1988) Morbidity of completion thyroidectomy for initially misdiagnosed thyroid carcinoma. Head Neck Surg 10:235–238
Menegaux F, Turpin G, Dahman M, Leenhardt L, et al (1999) Secondary thyroidectomy in patients with prior thyroid surgery for benign disease: a study of 203 patients. Surgery 125:479–483
Anderson PE, Hurley PR, Rosswick P (1990) Conservative treatment and long term prophylactic thyroxine in the prevention of recurrence of multinodular goiter. Surg Gynecol Obstet 171:309–314
Kraimps JL, Marechaud R, Gineste D et al (1993) Analysis and prevention of recurrent goiter. Surg Gynecol Obstet 176:319–322
Piraneo S, Vitri P, Galimberti A, Salvaggio A, Bastagli A (1997) Ultrasonographic surveillance after surgery for euthyroid goitre in patients treated or not with thyroxine. Eur J Surg 163:21–26
Rojdmark J, Jarhult J (1995) High long term recurrence rate after subtotal thyroidectomy for nodular goitre. Eur J Surg 161:725–727
Maxon HR, Englaro RE, Thomas SR et al (1992) Radioiodine-131 therapy for well-differentiated thyroid cancer—a quantitative radiation dosimetric approach: outcome and validation. J Nucl Med 33:1132–1136
Hay ID, Bergstralh EJ, Goellner JR, Ebersold, Grant CS (1993) Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 114:1050–1058
Mazzaferri EL (1987) Papillary thyroid carcinoma: factors influencing prognosis and current therapy. Semin Oncol 14:315–322; erratum in Semin Oncol 1988; 15(3):x
Shah JP, Loree TR, Dharker D, Strong EW, Begg C, Vlamis V (1992) Prognostic factors in differentiated carcinoma of the thyroid gland. Am J Surg 164:658–661
Baudin E, Travagli JP, Ropers J et al (1998) Microcarcinoma of the thyroid gland: the Gustave-Roussy Institute experience. Cancer 83:553–559
Samaan NA, Schultz PN, Hickey RC et al (1992) The results of various modalities of treatment of well differentiated thyroid carcinoma: a retrospective review of 1599 patients. J Clin Endocrinol Metab 75:714–720
Logue JP, Tsang RW, Brierley JD, Simpson WJ (1994) Radioiodine ablation of residual tissue in thyroid cancer: relationship between administered activity, neck uptake and outcome. Br J Radiol 67:1127–1131
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tezelman, S., Borucu, I., Senyurek (Giles), Y. et al. The Change in Surgical Practice from Subtotal to Near-Total or Total Thyroidectomy in the Treatment of Patients with Benign Multinodular Goiter. World J Surg 33, 400–405 (2009). https://doi.org/10.1007/s00268-008-9808-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-008-9808-1