
Abstract
Background
The purpose of the present work was to compare rates of postsurgical complications following thyroidectomy for multinodular goiter through a retrospective multicenter cohort study.
Methods
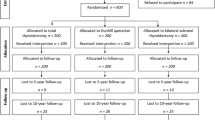
All cases of thyroidectomy (total—TT; near total—NT; and bilateral subtotal—ST) performed in two hospitals from 1990 to 2005 were studied to determine the incidence of complications after each procedure. Follow-up checked injury of laryngeal nerves, hypoparathyroidism, hypothyroidism, pathology recurrence, and appearance of neoplasm.
Results
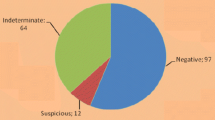
There were 6,223 cases: TT, n = 3,834 (61.6%); ST, n = 2,238 (36%); and NT, n = 151 (2.4%) NT). Of this total, 2,758 (44.3%) patients were men and 3,465 (55.7%) were women with a mean age of 48.7. Postoperative mean follow-up was 7 years, 2 months. Permanent recurrent laryngeal nerve (RLN) injury was observed in 1.4% in the TT group, 1.2% in the ST group, and 1.1% in the NT group (p > 0.1). Permanent hypocalcemia was observed in 2% in TT group, 1.9% in the ST group, and 2% in the NT group (p > 0.1). Permanent hypothyroidism occurred in all patients in the TT and NT groups, compared to 91% of the patients in the ST group (p > 0.1). Recurrence of benign disease was noted in 491 patients (20.5% of ST and NT cases combined; p < 0.05), n = 482 (21.5%) after ST and n = 9 (5.9%) after NT. Of the patients with recurrence, 173 needed a completion thyroidectomy. Malignant transformation was observed in 28 cases.
Conclusions
There is no statistically significant difference in complications among TT, NT, and ST groups. Partial thyroidectomies provide no decisive advantage over total thyroidectomies in terms of subsequent requirements of supplemental hormone therapy. The rate of reoperation in cases of recurrent pathology and incidental carcinoma was high.
Similar content being viewed by others

References
Michler M, Benadum J (1970) The letters from Jacques-Louis Reverdin and Theodore Kocher to Anton v. Eiselberg. A study on the discovery of deficiency symptoms following total extirpation of the thyroid gland. Gesnerus 27:169–184
Macdonald I (1953) The importance of total thyroidectomy for papillary carcinoma of the thyroid gland. Am Surg 19:1189–1190
Bustos FM (1951) Total thyroidectomy; results in Graves’ thyrotoxicosis. Bol Trab Acad Argent Cir 35:38–92
Caeiro JA (1951) Total thyroidectomy in the treatment of hyperthyroidism. Bol Soc Cir Urug 22:304–316
Caeiro JA (1951) Total thyroidectomy in the treatment of grave hyperthyroidism: indications. Bol Trab Acad Argent Cir 35:358–366
Block MA, Horn RC, Brush BE (1960) The place of total thyroidectomy in surgery for thyroid carcinoma. Arch Surg 81:236–243
Attie JN, Khafif RA (1975) Preservation of parathyroid glands during total thyroidectomy. Improved technic utilizing microsurgery. Am J Surg 130:399–404
Akin JT Jr, Skandaliakis JE (1976) Technique of total thyroid lobectomy. Am Surg 42:648–652
Hedley AJ, Flemming CJ, Chester MI et al (1970) Surgical treatment of thyrotoxicosis. Br Med J 1:519–523
Beahrs OH, Sakulsky SB (1968) Surgical thyroidectomy in the management of exophthalmic goiter. Arch Surg 96:512–516
Di Matteo G, Lucci S, Marchegiani C (1984) Indications, procedures and results in the surgical treatment of hyperthyroidism: a follow-up of 336 cases. Ital J Surg Sci 14:211–216
Deaconson TF, Wilson SD, Cerletty JM et al (1986) Total or near total thyroidectomy versus limited resection for radiation-associated thyroid nodules: a twelve-year follow-up of patients in a thyroid screening program. Surgery 100:1116–1120
Peix JL, Van Box Som P (1996) Role of total thyroidectomy in the treatment of benign thyroid disease. Ann Endocrinol (Paris) 57:502–507
Aytac B, Karamercan A (2005) Recurrent laryngeal nerve injury and preservation in thyroidectomy. Saudi Med J 26:1746–1749
Osmolski A, Frenkiel Z, Osmolski R (2006) Complications in surgical treatment of thyroid diseases. Otolaryngol Pol 60:165–170
Aluffi P, Policarpo M, Cherovac C et al (2001) Post-thyroidectomy superior laryngeal nerve injury. Eur Arch Otorhinolaryngol 258:451–454
Zambudio AR, Rodriguez J, Riquelme J et al (2004) Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. Ann Surg 240:18–25
Robert J, Mariethoz S, Pache JC et al (2001) Short- and long-term results of total vs subtotal thyroidectomies in the surgical treatment of Graves’ disease. Swiss Surg 7:20–24
Pelizzo MR, Toniato A, Piotto A et al (2001) Prevention and treatment of intra- and post-operative complications in thyroid surgery. Ann Ital Surg 72:273–276
Ku CF, Lo CY, Chan WF et al (2005) Total thyroidectomy replaces subtotal thyroidectomy as the preferred surgical treatment for Graves’ disease. Aust N Z J Surg 75:528–531
Pappalardo G, Guadalaxara A, Frattaroli FM et al (2998) Total compared with subtotal thyroidectomy in benign nodular disease: personal series and review of published reports. Eur J Surg 164:501–506
Dener C (2002) Complication rates after operations for benign thyroid disease. Acta Otolaryngol 122:679–683
Muller PE, Kabus S, Robens E et al (2001) Indications, risks, and acceptance of total thyroidectomy for multinodular benign goiter. Surg Today 31:958–962
Liu Q, Djuricin G, Prinz RA (1998) Total thyroidectomy for benign thyroid disease. Surgery 123:2–7
Palestini N, Grivon M, Carbonaro G et al (2005) Surgical treatment of Graves’ disease: results in 108 patients. Ann Ital Chir 76:13–18
Mattioli FP, Torre GC, Borgonovo G et al (1996) Surgical treatment of multinodular goiter. Ann Ital Chir 67:341–345
Marchesi M, Biffoni M, Tartaglia F et al (1998) Total versus subtotal thyroidectomy in the management of multinodular goiter. Int Surg 83:202–204
Colak T, Akca T, Kanik A et al (2004) Total versus subtotal thyroidectomy for the management of benign mutlinodular goiter in an endemic region. Aust N Z J Surg 74:974–978
Ponomarenko AI, Sobko EG, Piven’ NA (1973) Postoperative hypothyreosis. Klin Khir 5:34–36
Basili G, Biagini C, Manetti A et al (2003) Risk of recurrence following partial thyroidectomy for benign lesions. Report of 58 patients 15–25 years after surgery. Minerva Chir 58:321–329
Scazziga BR (1978) Long term follow-up after thyroidectomy. Helv Chir Acta 44:741–745
Koyuncu A, Dökmetas HS, Turan M et al (2003) Comparison of different thyroidectomy techniques for benign thyroid disease. Endocrine J 50:723–727
Werga-Kjellman P, Zedenius J, Tallstedt L et al (2001) Surgical treatment of hyperthyroidism: a ten-year experience. Thyroid 11:187–192
Ozbas S, Kocak S, Aydintug S et al (2005) Comparison of the complications of subtotal, near total and total thyroidectomy in the surgical management of multinodular goitre. Endocrine J 52:199–20541
Andaker L, Johansson K, Smeds et al (1992) Surgery for hyperthyroidism: hemithyroidectomy plus contralateral resection or bilateral resection? A prospective randomized study of postoperative complications and long-term results. World J Surg 16:765–769
Nonchev BI, Terzieva DD, Dimov RS et al (2005) Early hypothyroidism after subtotal thyroidectomy in patients with Graves’ disease—the role of the preoperative conservative treatment and hormonal status. Folia Med (Plovdiv) 47:40–45
Sivanandan R, Ng LG, Khin LW et al (2004) Postoperative endocrine function in patients with surgically treated thyrotoxicosis. Head Neck 26:331–337
Alimoglu O, Akdag M, Sahin M et al (2005) Comparison of surgical techniques for treatment of benign toxic multinodular goiter. World J Surg 29:921–924
Prades J-M, Dumollard J-M, Timoshenko A et al (2002) Multinodular goiter: surgical management and histopathological findings. Eur Arch Otolaryngol 259:217–221
Candela G, Varriale S, Di Libero L et al (2006) Nearly total thyroidectomy: versus total thyroidectomy: our experience. Minerva Chir 61:17–24
Perzik SL (1976) Total thyroidectomy in the management of Graves’ disease. A review of 286 cases. Am J Surg 131:284–287
Perzik S (1976) The place of total thyroidectomy in the management of 909 patients with thyroid disease. Am J Surg 132:480–483
Perzik SL (1976) Surgery in Thyroid Disease: The Place of Total Thyroidectomy, New York, Stratton Intercontinental Medical Book Corp
Berchtold R, Studer H, Teuscher J (1983) Modern surgery for goiter. Chirurg 109:187–199
Foster Jr RS (1978) Morbidity and mortality after thyroidectomy. Surg Gynecol Obstet 146:413–429
Lasagna B, Resegotti A, De Paolis P et al (1993) Estensione della tiroidectomia nel trattamento delle tireopatie nodulari benigne. Minerva Chir 48:1421–1424
Campana FP, Marchesi M, Tartaglia F et al (1992) La tiroidectomia totale per gozzo. Chirurgia 5:102–105
Jacobs J, Aland J, Ballinger J (1983) Total thyroidectomy: a review of 213 patients. Ann Surg 197:542–549
Karlan M, Katz B, Dunkelman D et al (1984) A safe technique for thyroidectomy with complete nerve dissection and parathyroid preservation. Head Neck Surg 6:1014–1021
Levin KE, Clark AH, Duh QY et al (1992) Reoperative thyroid surgery. Surgery 111:604–609
Thomusch O, Sekulla C, Dralle H (2003) Is primary total thyroidectomy justified in benign multinodular goiter? Results of a prospective quality assurance study of 45 hospitals offering different levels of care. Chirurg 74:437–443
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vaiman, M., Nagibin, A., Hagag, P. et al. Subtotal and Near Total Versus Total Thyroidectomy for the Management of Multinodular Goiter. World J Surg 32, 1546–1551 (2008). https://doi.org/10.1007/s00268-008-9541-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-008-9541-9