
Abstract
Background
The unsatisfied clinical need has encouraged the development and validation of bioanalytical procedures for the quantification of drugs in biological samples because the monitoring of drug concentrations helps in personalizing the patient’s pharmacotherapy, assessing the adherence to therapy, and is also extensively useful for pharmacokinetics and drug-drug interactions studies.
Main Body
The present review aimed to provide insightful information about the various liquid chromatographic methods developed till 2019 for the analysis and quantification of atorvastatin, its metabolites, and co-administered drugs in the various biological matrices like the serum, plasma, and urine with special emphasis on sample preparation techniques applied before chromatographic analysis along with different chromatographic conditions and their validation data. A total of 88 published papers that have used liquid chromatography techniques to quantify atorvastatin in biological fluids are included in the study. Out of the total reported liquid chromatographic methods, 34% used UV spectrophotometer as a detector, and 55% used MS/MS as a detector. Whereas 38% of them used protein precipitation procedure, 33% applied liquid-liquid extraction approach, and 12% employed solid-phase extraction technique for sample preparation.
Conclusion
In the last decade, numerous bioanalytical procedures have been developed for the quantification of atorvastatin in different biological samples using liquid chromatographic techniques. Moreover, advancement in technology developed several new and advanced sample preparation approaches like dispersive liquid-liquid extraction, microextraction by packed sorbent, which have high recovery rates than conventional procedures. Thus, the summarized review may be consulted as an informative tool to support the optimization of new bioanalytical methods for the quantification of atorvastatin.
Similar content being viewed by others

Background
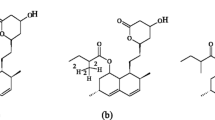
Statins (HMG CoA reductase inhibitors) are considered as the drug of choice for the treatment of hypercholesterolemia because of their extremely beneficial effect in reducing total cholesterol and low-density lipoprotein cholesterol levels in the human body [1]. Statins competitively inhibit the HMG-CoA reductase which further depletes the intracellular supply of cholesterol [2]. Atorvastatin (AT) (Fig. 1) is one of the oldest and major drug under the class of statins, which is chemically (3R,5R)-7-2-(4-Fluorophenyl)-3-phenyl-4-(phenyl arbamoyl)-5-propan-2-ylpyrrol-1-yl-3,5-dihydroxyheptanoic acid [3] and shows the highest low-density lipoprotein-cholesterol lowering efficacy in human at a maximum daily dose of 80 mg. With a molecular formula of C33H15FN2O5 and a molecular weight of 558.064 g mol−1, AT exists in two different forms, one is open-structured hydroxyl acid while another one is ring-structural lactone which degrades in both high alkaline and low acidic conditions [4]. AT has a significantly longer plasma half-life of 18–24 h compared to other statins [5]. AT is administered in its active acid form which afterward metabolized in its two active hydroxyl metabolites, i.e., ortho-hydroxy atorvastatin (o-OH AT) and para-hydroxy atorvastatin (p-OH AT) and three inactive lactone metabolites [6]. Runny nose, sneezing, and coughing are the most common side effects of AT whereas muscle problems, liver problems, loss of appetite, and upper stomach pain are certain serious side effects of AT [7]. AT is also clinically used to reduce the risk of stroke [8]; myocardial infarction [9], which further reduces the risk for angina [10]; and revascularization procedures [11].

Chemical structure of AT
Although plasma drug monitoring is not crucial for the AT, an increasing number of patients taking AT have drawn the attention of healthcare professionals for mandatory monitoring of plasma concentration in various conditions. Moreover, monitoring the plasma concentrations of AT helps personalize the patient’s pharmacotherapy and to assess the adherence to therapy. Since AT is also co-administered with many other drugs as polypharmacy therapy, the bioanalytical assays are also extensively used for its pharmacokinetics and drug-drug interactions’ studies. Thus, the unsatisfied clinical need has encouraged the development and validation of several liquid chromatography methods as bioanalytical procedures for the determination of AT in body fluids with high accuracy, precision, and better reproducibility. The present review encapsulates all reported liquid chromatography-based bioanalytical procedures available in the literature that are used for the quantification of AT alone, with its metabolites and with co-administered drugs in different biological samples. Also, a succinct tabular outline of the bioanalytical procedures has been included in the review which consists of chromatographic conditions, sample preparation strategies, validation data, etc.
Main text
Indeed, the best approach for the accurate analysis of drug concentration in biological samples is the use of high-resolution liquid chromatographic techniques such as HPLC and UPLC coupled with UV spectrophotometer or MS/MS detectors. Liquid chromatography techniques are not only considered as an important tool to support the therapeutic drug monitoring of drugs in the biological fluids but also during quality control of pharmaceutical formulations as well as during non-clinical and clinical drug development. From 1998 to 2019, different liquid chromatographic procedures to analyze AT in biological fluids were developed, validated, and applied in pharmacokinetic studies and therapeutic drug monitoring. Out of the total reported liquid chromatographic methods, 34% used UV spectrophotometer as a detector, and 55% used MS/MS as a detector.
Analysis using HPLC
HPLC is the preferable method for the analysis of drugs and currently the widest accepted method for separation technique. Table 1 [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] enlist the various HPLC methods coupled with UV, DAD, and PDA detectors used to detect AT and co-administered drugs in biological fluids. Usually, the reverse phase HPLC method has been used to quantify AT using C18 analytical columns because of the presence of pyrrole and phenyl as aromatic functional groups that make analysis suitable by the reverse phase method [52]. However, some published work has used the C8 column as the stationary phase. The mobile phase that has been used in the quantification of AT in biological matrices, primarily comprised of acetonitrile (ACN), methanol (MeOH), water, and different buffer solutions that have either isocratic or gradient elution with a flow rate of 1 mL min−1. Retention of analyte in the analytical column hinge upon the pH of elution, so in reported bioanalytical assays, pH of the mobile phase has been maintained between 2 and 4 to make better retention of analyte in the analytical column and enhanced the resolution of the peak because these pH values are lesser than pKa value of AT and AT remain in unionized form for a longer time and interact more with the stationary phase [52]. The retention time (Rt) of AT reported in Table 1 variegates from 1.7 to 19.8 min, but in most of the developed HPLC methods, Rt has ranged 2 to 5 min. The wavelength of UV detector used to detect AT has ranged from 210 to 270 nm, but commonly, 247 nm has been used as detection wavelength. Conversely, Tekkeli et al. quantify AT in human plasma using fluorimetric detection at excitation and an emission wavelength of 282 and 400 nm, respectively [37]. For the accuracy in quantification, diclofenac [20, 26, 31, 34] and ibuprofen [29, 39] have been often employed as internal standards in various developed HPLC methods to determine AT. Considering the validation of developed methods, all the developed methods have been validated as per ICH Q2 (R1) guidelines for system suitability, sensitivity, selectivity, linearity, limit of detection (LOD), limit of quantification (LOQ), and inter-day and intra-day accuracy and precision. LOD of the AT has been determined based using signal intensity to baseline noise ratio (S/N) of 3:1 by comparing test results from samples of a known concentration of analyte with the blank sample while LOQ determination has been based on signal intensity ten times more than baseline noise, i.e., S/N = 10. Least LOQ and LOD value of 0.2033 ng mL−1 and 0.0608 ng mL−1 respectively were observed in the method proposed by Dastkhhon et al. [43]. whereas the method developed by Gholami and Ahmadi was highly sensitive with LOQ value of 0.38 ng mL−1 and LOD value of 0.10 ng mL−1 with linearity in concentration calibration range of 1 to 1000 ng mL−1 and %RSD less than 4.2% [49].
Analysis using LC-MS/MS and UPLC-MS/MS
The liquid chromatography-based bioanalytical procedures using MS/MS detectors are listed in Table 2 [53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,53,100]. On the other hand, few studies used UPLC MS/MS method for the estimation of AT in the biological fluids and are also indexed in Table 2 [55, 56, 65, 71, 74, 81, 87, 91, 94, 95, 100]. Similar to HPLV-UV methods, C18 analytical columns have been extensively used in LC-MS/MS assay as a stationary phase because their long alkyl chain provides more efficient separation of nonpolar compounds in MS/MS detection [101], whereas a column packed with bridge ethyl hybrid (BEH) has been used in UPLC method as a stationary phase [71, 81, 87, 95] because of their high mechanical resistance [102]. Although MeOH, ACN, and water are used as mobile phases for quantification in LC-MS/MS, certain additives like formic acid (FA), ammonium acetate (AA), and acetic acid (AcA) have been added in the mobile phase to enhance ionization which further increases the sensitivity of the method. Isocratic elution has been predominantly preferred over gradient elution in the analysis of AT with an elution rate of 0.2–0.5 mL min−1. Rt has found to be quite small, ranged between 0.66 and 6.3 min. AT and its metabolites can be detected in both positive and negative ionization modes of MS, yet most of the published work has performed LC-MS/MS analyses of AT in positive ionization mode using electrospray ionization (ESI), but few reported studies used negative ions [54, 56, 58, 67, 80, 94] of AT for the analysis even though, polarity switching within run is required in ESI− mode [89]. On the other hand, the atomic pressure chemical ionization (APCI) technique has been used by Tahboub for ionization of AT in positive mode [64]. Figures 2 and 3 represent the product ion spectra of AT and metabolites in both ESI+ and ESI− modes respectively. Interestingly, a study by Partani et al. concluded that analysis in ESI− mode gives quite low LOQ value because the negative ions enhance the selective detection and also improve the sensitivity of the method [67]. Principally, quantification of AT has been carried out using multiple reaction monitoring (MRM) transition with the precursor ion M+H+ at m/z 559 Da and product ion at m/z 440 Da, while SRM transition has also been employed in numerous ESI+ methods with transitions at m/z 559 → 440 [52, 65, 70, 81, 88, 89]. Importantly, Jang et al. utilized the MRM transition of m/z 559.3 → 250.2 for the detection of AT in the human urine samples [92]. Negative ions of AT have been analyzed at m/z 557.4 → 278.1 in the MRM transition [56, 58, 67] but in some ESI− mode quantification of AT has been carried out with product ion at m/z 397 [56, 60, 80] while AT was detected using MRM transition 557.0 → 453.0 in the bioanalytical method proposed by Xia et al. [94]. Interestingly, Varghese and Kochupappy Ravi [53] and Ma et al. [84] performed the analysis of AT using LC–ESI–MS in selected ion monitoring (SIM) mode at m/z 559. In most of the LC-MS/MS assays, either deuterium-labeled analogs of AT (d5-AT) or structural analogs of AT such as rosuvastatin [53, 55, 58, 66, 86, 94], pitavastatin [66, 84], and pravastatin [70, 80] have been selected as internal standards to get most accurate results.

Product ion spectra of a AT, b o-OH AT, and c p-OH AT in ESI+ mode [61]

Product ion spectra of a AT, b o-OH AT, and c p-OH AT in ESI− mode [66]
LOD and LOQ in the reported methods have been calculated based on their signal to noise ratio, as discussed earlier; nevertheless, in some developed methods, lowest concentration of their linear calibration curve has been chosen as LOQ for analysis. The bioanalytical method developed by Zhou et al. is most sensitive than all other reported LC-MS/MS methods with the lowest LOQ of 0.036 ng mL−1 and the calibration curve in the range of 0.03–25 ng mL−1 along with intra-day and inter-day RSD of 4.02% and 5.23% respectively [69]. In more than 50% of total reported LC-MS/MS methods, LOQ is equal to or less than 0.5 ng mL−1 which indicates the developed LC-MS/MS methods are highly sensitive. Importantly, Novakova and co-workers have demonstrated the role of the two variables, i.e., concentration and pH of buffer solution in the mobile phase that affects the signal to noise ratio of MS/MS detector, and observed that an increase in a concentration above 5 mM significantly reduces the response of mass spectrometer and the concentrations lower than 0.5 mM were not enough to keep buffering capacity and thus had a negative impact to the response of the MS/MS detector; thus, the best response of AT and simvastatin was observed at 0.5 mM concentration of buffers. Also, AA gave better peak shapes as compared to ammonium formate (AF), and finally, AA buffer (pH 4.0; 0.5 mM) was selected as an optimized buffer for mobile phase composition [81].
Analysis of metabolites and co-administered drugs
Most of the references cited in Tables 1 and 2 also describe the simultaneous determination of AT with certain other statins [13, 20, 24, 27,28,29, 50, 51, 54, 56, 61, 65, 81, 87] and other co-administered drugs such as amlodipine [35, 40, 59, 64, 65, 69, 70, 77, 78, 95], ezetimibe [42, 66, 71], gemfibrozil [13, 30, 51], clopidogrel [14, 15, 41, 93], fenofibrate [26], aspirin [15, 23, 72], ramipril [64, 78], pioglitazone [17, 22], glimepiride [64, 68, 73], olmesartan [62, 98], and many other. Various methods have also been developed and validated using LC-MS/MS to quantify the metabolites of AT and are enlisted in Table 2 [54, 56,57,58, 60,61,62, 65, 67, 69, 70, 74,75,76, 79, 80, 82, 83, 85,86,87,88,89,90,91, 96, 100].
In 1999, Bullen et al. were the first to propose an LC-MS/MS method for the determination of AT and 2 of its metabolites, o-OH AT and p-OH AT in rat, dog and human plasma using a C18 column with isocratic elution of ACN and AcA (70:30, v/v) and detection in ESI+ MRM mode with transitions 559.3 → 440.2 for AT, 575.3 → 440.2 for p-OH AT, and 575.3 → 440.2 for o-OH AT [90]. Correspondingly, both the acid and lactone form of AT were simultaneously analyzed by Jemal et al. along with their 4 metabolites, i.e., o-OH AT, p-OH AT, o-OH AT-lactone, and p-OH AT-lactone in human serum in ESI+ mode with eight SRM channels using a highly sensitive and selective LC-MS/MS method [89]. However, MacWan et al. also proposed a method for quantification of AT and its 5 metabolites in human plasma using phenyl column [75]. Interestingly, Van pelt et al. modified the conventional LC-MS system by incorporating three valves and four columns into it for the analysis of AT and acid and lactone metabolites in human plasma to reduce the overall run time from 4.5 to 1.65 min [96].
Courlet et al. developed a UHPLC-MS/MS method for the simultaneous quantification of amlodipine, metoprolol, pravastatin, rosuvastatin, AT, o-OH AT, and p-OH AT in human plasma using their stable isotopically labeled analogs as IS. All the compounds were analyzed using ESI+ mode, except for pravastatin which was detected using ESI− mode [65]. Vlčková et al. optimized a UHPLC–MS/MS method for selective quantification of seven statins along with their inter-converted products and metabolites in biological samples by comparing the three MS/MS detector with different specifications [55]. Likewise, Wagmann et al. proposed a highly selective method to detect seven statins and their metabolites in human blood plasma using LC-high-resolution MS/MS and applied in the therapeutic drug monitoring of these statins on 14 human plasma samples [53]. Also in 2014, eight different cardiovascular drugs were simultaneously quantified in human plasma using an APCI LC-MS/MS method by Tahboub [64]. However, an RP-HPLC-UV method was designed by Bhatia et al. for the simultaneous estimation of four cardiovascular drugs, i.e., AT, aspirin, atenolol, and losartan in tablet dosage form and plasma [23].
Analysis in biological fluids other than blood
Instead of analysis in common biological fluids such as plasma and serum from humans or animals, certain researchers have successfully developed liquid chromatography-based bioanalytical procedures for the quantification of AT in various other biological fluids. Silva et al. determined AT and curcumin in mouse plasma and also in the lung, brain, liver, and spleen homogenate supernatants using an HPLC-DAD assay [12]. Identically, AlKhani et al. designed a precise HPLC-UV method to quantify AT in both rat plasma and rat intestinal perfusion solution for its further application in pharmacokinetic studies [39]. The development of analytical methods for the detection of drugs and its metabolites in the urine samples generally helps to understand in vivo metabolism and clearance process, so, various methods have been developed to analyze AT in the urine samples [13, 43, 44, 47, 92]. In the year 2017, Beydokhti et al. proposed a method to simultaneously determine AT, rosuvastatin, and gemfibrozil in deionized water, wastewater, human plasma, and urine using HPLC-UV method and urine samples were prepared for analysis by diluting with 10 mL of deionized water [13]. Likewise, eight statins were simultaneous determined in human urine using a highly selective and sensitive LC-MS/MS method developed by Jang et al. in which dilute and shot approach was used for urine sample preparation [92].
Sample preparation or extraction of drug from the biological matrix
Traditionally, sample preparation is carried out by diverse techniques such as precipitation of the plasma proteins (PP), liquid-liquid extraction (LLE), and solid-phase extraction (SPE), before the final bioanalysis using liquid chromatography interfaced with UV or MS or MS/MS or capillary gas chromatography to prevent the interference of endogenous substances such as lipids, proteins, salts, acids, bases, and cells present in biological fluid with the chromatographic detection. Out of the total methods cited in Tables 1 and 2, 38% used PP for sample preparation, 33% applied LLE techniques, and 12% employed SPE technique.
Protein precipitation (PP) is the most commonly applied sample preparation technique used for the extraction of AT from biological matrix because of its rapidity, simplicity, and suitability to both hydrophilic and lipophilic analytes. PP process generally involves the addition of ACN or MeOH as precipitating agents followed by subsequent vortex and centrifugation. The % mean recoveries obtain from PP are quite significant. Acidification of the solvent has been generally employed in many PP methodologies to extract AT because the addition of acids such as trichloroacetic acid (TCA) or formic acid (FA) or AcA in the organic solvent enhanced the precipitation process due to changes in the pH [15, 25, 33, 35, 40, 65, 75, 77, 93]. Also, ice-cold extraction solvents have been used in many procedures to prevent degradation and achieve high purification of samples [15, 25, 34, 40, 46, 99]. Mathur and Devi used 10% perchloric acid as a precipitating agent along with a mixture of K2CO3 (2.5 M) and KOH (6 M) to maintain pH between 6.0 and 6.5 [48].
Various bioanalytical methods used LLE strategy for the sample pre-treatment of AT before the final analysis by using ethyl acetate, methyl-tertiary butyl ether, dichloromethane, or diethyl ether as organic extraction solvents. Instead of the single solvent procedure, various methods have also used a combination of different solvents [17, 27, 53, 54, 69, 85, 86] or various buffering agents such as FA [17, 60]. AA [20] and phosphate buffer [33, 70,71,72, 85] for the extraction of AT using LLE method. Also, the addition of buffering agents to the extraction solvent has improved the recovery of analyte from biological matrices. Bullen et al. used NaOH as a buffering agent to boost the extraction of AT from the rat, dog, and human plasma [90]. Despite its few disadvantages such as time-consuming, use of toxic, expensive, and environmentally unfriendly organic solvents [18] and less selectivity toward hydrophilic drugs and metabolites [103], LLE is still extensively employed as a sample preparation technique.
Because of its laborious multistep procedure including column conditioning, sample loading, washing, and elution, followed by evaporation of the eluent, only 12% of the total reported methods adopted SPE approaches for the extraction of AT from biological matrices. Different types of reverse phase SPE cartridges or columns such as HLB or C18 SPE cartridges have been used in SPE as a stationary phase. Moreover, ACN and MeOH have been commonly employed as a solvent for column conditioning, washing, and elution along with some acid, base, or buffers to facilitate elution. SPE isolates analyte more effectively than LLE but not widely employed. Apart from its tedious procedures, cartridges used in SPE are also too expensive, and the plugging of the cartridge is also a major concern in this extraction procedure. Interestingly, Partani et al. carried out their whole SPE sample preparation process in an ice-cold water bath (excluding vortex mixing, SPE, and drying) and under low light conditions to prevent the degradation of the analyte by the temperature and light [67].
Besides conventional sample preparation approaches, many researchers used modified and novel extraction procedures to isolate AT from biological matrices. Both Hassan et al. and Yang et al. employed a novel Salting-out assisted liquid-liquid extraction (SALLE) technique for the extraction of AT from human serum and human plasma respectively using ACN salted with AA and magnesium chloride as a water-miscible solvent [18, 62]. Interestingly, this fast sample pre-treatment procedure shortens the chromatographic run time of AT. Martins et al. utilized dispersive liquid-liquid micro-extraction (DLLME) as a novel extraction method for the isolation of AT from biological matrices and compare it with the conventional SPE method [24]. A further modification in the DLLME technique with solidification in the prepared floating organic droplets has been made by Taheri et al. using a low-density solvent (Undecanol), which floats and solidifies at the top of the extraction vial during the extracted phase and separates the analyte easily [16]. Furthermore, Farajzadeh et al. used sugar cubes as a disperser base instead of a disperser solvent in the DLLME procedure to extract AT from human serum [38]. Notably, Beydokiti et al. resolved the problem of lack of sample clean-up by using tandem air-agitated LLE based on solidification of floating organic droplets (TAALLME-SFO) technique for the extraction of AT from a biological matrix. However, the use of chlorinated solvents is also a major drawback of this method [50]. Interestingly, instead of two-phase liquid microextraction, in 2009, Farahani et al. designed a novel three-phase liquid microextraction process (LLLME) in droplet-based mode to separate the analyte from complex biological matrix before HPLC assay [31].
Rukthong et al. utilized a simple, sensitive, and rapid solid-phase microextraction (SPME) technique to extract AT from human plasma using an RP-C18 SPE sorbent material which is packed in a 100-μL pipette tip to eliminates the clogging problem [97]. Because of comparative high sorption capacity and high selectivity for analytes, many researchers employed magnetic nanoparticles (MNPs) as sorbents instead of conventional SPE sorbent in the extraction of AT from biological matrices and the extraction technique involving MNP is termed as magnetic solid-phase extraction (MSPE). Tekkeli et al. used graphene nanosheets decorated with Fe3O4 nanoparticles as a magnetic sorbent for the extraction of AT from human plasma along with ACN as an extraction solvent [37]. Similarly in another study, Khoshhesab et al. used an ultrasound-assisted MSPE technique using sodium dodecyl sulfate-coated Fe3O4 MNP as a sorbent for the extraction and found it comparatively easy and fast while comparing with conventional LLE and LLLME methods [44]. Dastkhoon et al. in 2017 developed dispersive micro solid-phase extraction (Dμ-SPE) approach as a novel modification in the SPE technique for extraction of AT from human plasma and urine using Cu@SnS/SnO2 nanoparticles loaded on activated carbon as a sorbent for separation of AT from matrices [43]. Interestingly, a combined magnetic-dispersive SPE (MD-SPE) approach was designed by Gholami and Ahmadi for the extraction of AT from human serum using polypyrrole-Fe3O4 MNP as sorbent [49]. Notably, Azadi and Ahmadi further used magnetic dispersive micro solid-phase extraction (MDμ-SPE) technique for the extraction of AT and valsartan from human serum and urine using CMC-coated Fe3O4 MNP [47]. In the same way, Beydokhti et al. developed a novel extraction technique by the combining magnetic dispersive micro SPE process and supra-molecular solvent-based microextraction process (Mdμ-SPE–SSME) to extract AT, rosuvastatin, and gemfibrozil from human plasma and urine sample with the help of layered double hydroxide-coated Fe3O4. Also, in comparison with the conventional SPE technique, Mdμ-SPE–SSME reduces the overall extraction time and eliminates the elution step [13]. Interestingly, Vlčková et al. developed microextraction by packed sorbent (MEPS) technique to extract AT and its metabolites from biological samples using a gas-tight syringe as an extraction device [56, 74]. Briefly, MEPS is a novel and miniature version SPE technique, and in comparison with the conventional SPE methods, the MEPS technique is quite simpler and time-saving and requires a lesser amount of sample. Moreover, the MEPS technique has good recovery in a short time with a lesser volume of samples.
Conclusion
Analysis of AT in the biological fluid is quite useful for pharmacokinetic studies, therapeutic drug monitoring, and drug-drug interaction studies. Numerous developed bio-analytical methods that are useful for quantitation of AT either alone or with its metabolites or co-administered drugs in plasma, serum, or urine are herein summarized and discussed. Due to advancement in technology, many new LC methods have been developed in the last decade with high sensitivity and accuracy. However, LC-MS/MS technique is more sensitive, selective, and precise as compared to the HPLC-UV technique for the quantification of AT. Also, various extraction techniques used to extract AT from biological matrices are discussed herein. Indeed, PP is the most commonly applied technique for sample preparation, followed by LLE and SPE, yet numerous advance methods have been developed such as SALLE, DLLME, and MEPS for the extraction of AT from biological fluids, to get high recovery. Thus, this review can be used as an informative tool to develop and optimize certain new LC methods for quantification of AT in biological matrices.
Availability of data and materials
Data and materials are available upon request
Abbreviations
- AA:
-
Ammonium acetate
- AcA:
-
Acetic acid
- ACN:
-
Acetonitrile
- AF:
-
Ammonium formate
- APCI:
-
Atmospheric pressure chemical ionization
- AT:
-
Atorvastatin
- Dμ-SPE:
-
Dispersive micro solid-phase extraction
- DAD:
-
Diode array detector
- DLLME:
-
Dispersive liquid-liquid micro-extraction
- ESI− :
-
Negative electrospray ionization
- ESI+ :
-
Positive electrospray ionization
- FA:
-
Formic acid
- LLE:
-
Liquid-liquid extraction
- LLLME:
-
Liquid-liquid-liquid microextraction
- LLME:
-
Liquid-liquid microextraction
- LOD:
-
Limit of detection
- LOQ:
-
Limit of quantification
- MSPE:
-
Magnetic solid-phase extraction
- MDμ-SPE:
-
Magnetic dispersive micro solid-phase extraction
- MeOH:
-
Methanol
- MEPS:
-
Microextraction by packed sorbent
- MRM:
-
Multiple reaction monitoring
- o-OH AT:
-
Ortho-hydroxy Atorvastatin
- PDA:
-
Photodiode array detector
- p-OH AT:
-
Para-hydroxy Atorvastatin
- PP:
-
Protein precipitation
- Rt :
-
Retention time
- r 2 :
-
Regression coefficient
- SALLE:
-
Salting-out assisted liquid-liquid extraction
- SIM:
-
Selected ion monitoring
- SPE:
-
Solid-phase extraction
- SPME:
-
Solid-phase microextraction
- SRM:
-
Selected reaction monitoring
- TCA:
-
Trichloroacetic acid
- UPLC:
-
Ultra performance liquid chromatography
References
Mager DR (2016) Statins: and the unexpected. Home Healthc Now 34:388–393
Kokilambigai KS, Seetharaman R, Lakshmi KS (2017) Critical review on the analytical techniques for the determination of the oldest statin—Atorvastatin—in bulk, pharmaceutical formulations and biological fluids. Crit Rev Anal Chem 47:538–555
O’Rourke A (2010) Martindale: the complete drug reference, 39th edn. The Pharmaceutical Press
Sirén H (2018) Atorvastatin and related compounds: review on analyses of pharmaceutical, blood and environmental samples. J Biomed Res Pract 1:1–31
Tripathi K (2018) Essentials of Medical Pharmacology, 8th ed, Jaypee Brothers Medical Publishers (P) Ltd
Lemke TL, Williams DA, Victoria PFR, Zito SW (2013) Foye’s Principles of Medicinal Chemistry, 7th edn. Lippincott Williams & Wilkins Publication
Ritter J, Flower R, Graeme H, Loke YK, MacEwan D, Rang H (2019) Rang & Dale’s Pharmacology, 9th edn. Elsevier Ltd
Sever PS, Poulter NR, Dahlöf B, Wedel H (2005) Different time course for prevention of coronary and stroke events by atorvastatin in the Anglo-Scandinavian cardiac outcomes trial–lipid-lowering arm (ASCOT-LLA). Am J Cardiol 96:39–44
Cheng X, Liao YH, Zhang J, Li B, Ge H, Yuan J, Wang M, Lu B, Liu Y, Cheng Y (2005) Effects of atorvastatin on Th polarization in patients with acute myocardial infarction. Eur J Heart Fail 7:1099–1104
Tousoulis D, Antoniades C, Katsi V, Bosinakou E, Kotsopoulou M, Tsioufis C, Stefanadis C (2006) The impact of early administration of low-dose atorvastatin treatment on inflammatory process, in patients with unstable angina and low cholesterol level. Int J Cardiol 109:48–52
Newman C, Tsai J, Szarek M, Luo D, Gibson E (2006) Comparative safety of atorvastatin 80 mg versus 10 mg derived from analysis of 49 completed trials in 14,236 patients. Am J Cardiol 97:61–67
Silva J, Basso J, Sousa J, Fortuna A, Vitorino C (2019) Development and full validation of an HPLC methodology to quantify atorvastatin and curcumin after their intranasal co delivery to mice. Biomed Chromatogr 33:1–11
Arghavani-Beydokhti S, Rajabi M, Asghari A (2017) Combination of magnetic dispersive micro solid-phase extraction and supramolecular solvent-based microextraction followed by high-performance liquid chromatography for determination of trace amounts of cholesterol-lowering drugs in complicated matrices. Anal Bioanal Chem 409:4395–4407
Nagavi JB, Gurupadayya B (2015) Development and validation of bio-analytical RP-ultra fast liquid chromatographic method for simultaneous estimation of clopidogrel and rosuvastatin in human plasma. Int J Curr Pharm Res 6:219–225
Porwal PK, Akhalaque ARA, Chhajed SS, Chatpalliwar VA (2015) Liquid chromatographic method for simultaneous quantitation of clopidogrel, aspirin and atorvastatin in rat plasma and its application to the pharmacokinetic study. J Chromatogr Sci 53:1155–1162
Taheri S, Jalali F, Fattahi N, Bahrami G (2015) Sensitive determination of atorvastatin in human plasma by dispersive liquid–liquid microextraction and solidification of floating organic drop followed by high-performance liquid chromatography. J Sep Sci 38:309–315
Sharma RN, Pancholi SS (2014) HPLC-DAD method for the pharmacokinetic interaction study of atorvastatin with pioglitazone and cholestyramine in wistar rats. Sci Pharm 82:555–570
Hassan J, Bahrani SH (2014) Determination of atorvastatin in human serum by salting out assisted solvent extraction and reversed-phase high-performance liquid chromatography-UV detection. Arab J Chem 7:87–90
Hu L, Song W, Zhang H, Gu D (2013) HPLC-UV method development for atorvastatin calcium micro-emulsion determination in rat plasma and its application to elucidate pharmacokinetic behaviour after oral administration to rats. Int J Pharm Sci Res 4:3839–3844
Al-Akkam J, Rasool AAA, Badwan AA, Jbour NDA, Qinna NA (2013) Development and validation of a sensitive and accurate method for determination of atorvastatin and rosuvastatin in rat plasma by reversed- phase high performance liquid chromatography with UV detection. Int J Pharm Pharm Sci 5:211–219
Chou YC, Wang YK, Charng MJ, Ueng YF (2013) Determination of serum atorvastatin concentrations in lipid-controlling patients with and without myalgia syndrome. J Food Drug Anal 21:147–153
Mirza AZ, Arayne MS, Sultana N (2013) RP-LC method for the simultaneous determination of gliquidone, pioglitazone hydrochloride, and atorvastatin in formulations and human serum. J AOAC Int 96:56–59
Bhatia NM, Gurav SB, Jadhav SD, Bhatia MS (2012) RP-HPLC method for simultaneous estimation of atorvastatin calcium, losartan potassium, atenolol, and aspirin from tablet dosage form and plasma. J Liq Chromatogr Relat Technol 35:428–443
Martins AF, C da s F, Altissimo J, de Oliveira JA, da Silva DS, Reichert JF, Souza DM (2017) Determination of statin drugs in hospital effluent with dispersive liquid–liquid microextraction and quantification by liquid chromatography. J Environ Sci Heal - Part A Toxic/Hazardous Subst Environ Eng 52:939–945
Sher M (2012) Development and validation of high-performance liquid chromatographic- ultraviolet (HPLC-UV) method for the bioequivalence study of atorvastatin. Afr J Pharm Pharmacol 6:2424–2428
Bhinge SD, Malipatil SM, Jondhale A, Savali AS (2013) Simultaneous estimation of atorvastatin calcium and fenofibrate in rabbit plasma by RP-HPLC. Asian J Chem 25:981–985
Shah Y, Iqbal Z, Ahmad L, Khan A, Khan MI, Nazir S, Nasir F (2011) Simultaneous determination of rosuvastatin and atorvastatin in human serum using RP-HPLC/UV detection: Method development, validation and optimization of various experimental parameters. J Chromatogr B 879:557–563
Sultana N, Arayne MS, Naveed S (2011) Validated method for the simultaneous determination of lisinopril, pravastatin, atorvastatin and rosuvastatin in API, formulations and human serum by RP-HPLC. Chin J Chem 29:1216–1220
Abdallah OM (2011) RP-HPLC determination of three anti-hyperlipidemic drugs in spiked human plasma and in dosage forms. E-Journal Chem 8:753–761
Khan IU, Jillani SMS, Ashfaq M (2010) Determination of atorvastatin and gemfibrozil in human plasma by reversed-phase liquid chromatography. Lat Am J Pharm 29:1383–1388
Farahani H, Norouzi P, Beheshti A, Sobhi HR, Dinarvand R, Ganjali MR (2009) Quantitation of atorvastatin in human plasma using directly suspended acceptor droplet in liquid–liquid–liquid microextraction and high-performance liquid chromatography-ultraviolet detection. Talanta 80:1001–1006
Shen HR, Li ZD, Zhong MK (2006) HPLC assay and pharmacokinetic study of atorvastatin in beagle dogs after oral administration of atorvastatin self-microemulsifying drug delivery system. Pharmazie 61:18–20
Zarghi A, Shafaati A, Foroutan SM, Khoddam A (2005) A simple and rapid HPLC method for the determination of atorvastatin in human plasma with UV detection and its application to pharmacokinetic studies. Arzneimittel Forschung Drug Res 55:451–454
Bahrami G, Mohammadi B, Mirzaeei S, Kiani A (2005) Determination of atorvastatin in human serum by reversed-phase high-performance liquid chromatography with UV detection. J Chromatogr B 826:41–45
Porwal PK, Talele GS (2017) Development of validated HPLC-UV method for simultaneous determination of meformin, amlodipine, glibenclamide and atorvastatin in human plasma and application to protein binding studies. Bull Fac Pharmacy, Cairo Univ 55:129–139
Altuntas TG, Erk N (2004) Liquid chromatographic determination of atorvastatin in bulk drug, tablet and human plasma. J Liq Chromatogr Relat Technol 27:83–93
Kepekci Tekkeli SE, Durmus Z, Onal A (2016) Determination of atorvastatin in human plasma by magnetic solid-phase extraction combined with HPLC and application to a pharmacokinetic study. J Liq Chromatogr Relat Technol 39:852–860
Farajzadeh MA, Khorram P, Pazhohan A (2016) Simultaneous determination of atorvastatin and valsartan in human plasma by solid-based disperser liquid-liquid microextraction followed by high-performance liquid chromatography-diode array detection. J Chromatogr B Anal Technol Biomed Life Sci 1017–1018:62–69
AlKhani M, Al-Laham A, Al-Mardini MA (2016) Simultaneous and precise HPLC method for quantification of atorvastatin in rat plasma and intestinal perfusion solution. Int J Pharm Sci Rev Res 38:70–74
Talele GS, Porwal PK (2015) Development of validated bioanalytical HPLC-UV method for simultaneous estimation of amlodipine and atorvastatin in rat plasma. Indian J Pharm Sci 77:742–750
Croitoru O, Spiridon A-M, Belu I, Turcu-Ftiolics A, Neamuu J (2015) Development and validation of an HPLC method for simultaneous quantification of clopidogrel bisulfate, its carboxylic acid metabolite and atorvastatin in human plasma: application to a pharmacokinetic study. J Anal Methods Chem 2015:1–12
Ashutosh Kumar S, Debnath M, Seshagiri Rao JVLN, Gowri Sankar D (2015) New validated stability-indicating RP-HPLC method for simultaneous estimation of atorvastatin and ezetimibe in human plasma by using PDA detector. Adv Pharm Bull 5:385–391
Dastkhoon M, Ghaedi M, Asfaram A, Arabi M, Ostovan A, Goudarzi A (2017) Cu@SnS/SnO2 nanoparticles as novel sorbent for dispersive micro solid phase extraction of atorvastatin in human plasma and urine samples by high-performance liquid chromatography with UV detection: application of central composite design (CCD). Ultrason Sonochem 36:42–49
Khoshhesab ZM, Ayazi Z, Farrokhrouz Z (2016) Ultrasound-assisted mixed hemimicelle magnetic solid phase extraction followed by high performance liquid chromatography for the quantification of atorvastatin in biological and aquatic samples. Anal Methods 8:4934–4940
Kotagiri H, Gannu R, Palem CR, Yamsani SK, Yamsani VV, Yamsani MR (2011) Simultaneous determination of glimepiride and atorvastatin in human serum by high-performance liquid chromatography: Application to pharmacokinetic study. J Liq Chromatogr Relat Technol 34:2420–2432
Kumar K, Reddy A, Anbu J, Reddy Y (2008) Simultaneous determination of atorvastatin and lercanidipine in rat plasma by HPLC and pharmacokinetic studies. Asian J Pharmacodymanics Pharmacokinet 8:299–304
Azadi A, Ahmadi S (2019) Simultaneous magnetic dispersive micro solid phase extraction of valsartan and atorvastatin using a CMC-coated Fe3O4 nanocomposite prior to HPLC-UV detection: multivariate optimization. New J Chem 43:16950–16959
Mathur M, Devi VK (2017) Design of experiment utilization to develop and validate high performance liquid chromatography technique for estimation of pure drug and marketed formulations of atorvastatin in spiked rat plasma samples. Int J Pharm Sci Res 8:1708–1716
Gholami SG, Ahmadi S (2018) Polypyrrole-modified magnetic nanoparticles for preconcentration of atorvastatin in human serum prior to its determination using high-performance liquid chromatography. Micro Nano Lett 13:1425–1430
Sultana N, Arayne MS, Naveed S (2011) Simultaneous determination of captopril and statin’s in API, pharmaceutical formulations by RP-HPLC. J Chin Chem Soc 57:378–383
Arghavani-Beydokhti S, Asghari A, Bazregar M, Rajabi M (2016) Application of a tandem air-agitated liquid–liquid microextraction technique based on solidification of floating organic droplets as an efficient extraction method for determination of cholesterol-lowering drugs in complicated matrices. RSC Adv 6:93582–93589
Crevar-Sakač M, Vujić Z, Brborić J, Kuntić V, Uskoković-Marković S (2013) An Improved HPLC Method with the aid of a chemometric protocol: simultaneous determination of atorvastatin and its metabolites in plasma. Molecules 18:2469–2482
Varghese SJ, Kochupappy Ravi T (2019) Liquid chromatography/mass spectrometry method for the simultaneous determination of atorvastatin and telmisartan in human plasma. Anal Chem Lett 9:552–563
Wagmann L, Hemmer S, Caspar AT, Meyer MR (2020) Method development for quantitative determination of seven statins including four active metabolites by means of high-resolution tandem mass spectrometry applicable for adherence testing and therapeutic drug monitoring. Clin Chem Lab Med 58:664–672
Harahap Y, Purnasari S, Harmita RR, Dian K, Pratami SW, Fatriyah S (2016) Quantification of atorvastatin in human plasma by liquid chromatography tandem mass spectrometry and its application for bioequivalence study of three formulations. Asian J Pharm Sci 11:66–67
Vlčková H, Svoboda P, Novák O, Solich P, Nováková L (2016) Development of MEPS-UHPLC-MS/MS multistatin methods for clinical analysis. Bioanalysis 8:333–349
Crevar-Sakač M, Vujić Z, Vujčić Z, Marković B, Vasiljević D (2016) LC-MS/MS method for quantification of atorvastatin, o-hydroxyatorvastatin, p-hydroxyatorvastatin, and atorvastatin lactone in rat plasma. Acta Chromatogr 28:281–298
Dhiman R, Kumar D, Kumar B, Pandey BL (2016) Quantitative determination of atorvastatin , ortho-hydroxy atorvastatin, para-hydroxy atorvastatin in human plasma using rosuvastatin as internal standard by LC-MS / MS. Int J Pharm Chem Sci 4:487–500
Danafar H, Hamidi M (2015) Pharmacokinetics and bioequivalence study of amlodipine and atorvastatin in healthy male volunteers by LC-MS. Pharm Sci 21:167–174
Bayya V, Makula A, Sanka K, Borra NS, Chaganty S (2015) Rapid, selective, and rugged method development and validation of atorvastatin and its active metabolites, o-hydroxy atorvastatin and p-hydroxy atorvastatin, in stabilized plasma using liquid chromatography coupled with tandem mass spectrometry. J Liq Chromatogr Relat Technol 38:1585–1592
Wang J, Luzum JA, Phelps MA, Kitzmiller JP (2015) Liquid chromatography-tandem mass spectrometry assay for the simultaneous quantification of simvastatin, lovastatin, atorvastatin, and their major metabolites in human plasma. J Chromatogr B 983–984:18–25
Yang Y, Xu Q, Zhou L, Zhong D, Chen X (2015) High-throughput salting-out-assisted liquid-liquid extraction for the simultaneous determination of atorvastatin, ortho-hydroxyatorvastatin, and para-hydroxyatorvastatin in human plasma using ultrafast liquid chromatography with tandem mass spectrometry. J Sep Sci 38:1026–1034
Das R, Pal TK (2014) Method development & validation of LCMS/MS for atorvastatin and olmesartan in human plasma to trace drug interaction of formulation. Curr Pharm Anal 11:43–52
Tahboub YR (2014) Chromatographic behavior of co-eluted plasma compounds and effect on screening of drugs by APCI-LC-MS(/MS): applications to selected cardiovascular drugs. J Pharm Anal 4:384–391
Courlet P, Spaggiari D, Desfontaine V, Cavassini M, Alves Saldanha S, Buclin T, Marzolini C, Csajka C, Decosterd LA (2019) UHPLC-MS/MS assay for simultaneous determination of amlodipine, metoprolol, pravastatin, rosuvastatin, atorvastatin with its active metabolites in human plasma, for population-scale drug-drug interactions studies in people living with HIV. J Chromatogr B 1125:121733
El-Bagary RI, Elkady EF, El-Sherif ZA, Kadry AM (2014) LC-MS-MS simultaneous determination of atorvastatin and ezetimibe in human plasma. J Chromatogr Sci 52:773–780
Partani P, Verma SM, Gurule S, Khuroo A, Monif T (2014) Simultaneous quantitation of atorvastatin and its two active metabolites in human plasma by liquid chromatography/(-) electrospray tandem mass spectrometry. J Pharm Anal 4:26–36
Polagani SR, Pilli NR, Gajula R, Gandu V (2013) Simultaneous determination of atorvastatin, metformin and glimepiride in human plasma by LC-MS/MS and its application to a human pharmacokinetic study. J Pharm Anal 3:9–19
Zhou Y, Li J, He X, Jia M, Liu M, Li H, Xiong Z, Fan Y, Li W (2013) Development and validation of a liquid chromatography-tandem mass spectrometry method for simultaneous determination of amlodipine, atorvastatin and its metabolites ortho-hydroxy atorvastatin and para-hydroxy atorvastatin in human plasma and its application in a bioequivalence study. J Pharm Biomed Anal 83:101–107
Yacoub M, Awwad AA, Alawi M, Arafat T (2013) Simultaneous determination of amlodipine and atorvastatin with its metabolites; ortho and para hydroxy atorvastatin; in human plasma by LC-MS/MS. J Chromatogr B 917–918:36–47
Abdelbary G, Nebsen M (2013) Application of a novel UPLC–MS/MS method for the pharmacokinetic/bioequivalence determination of atorvastatin and ezetimibe in human plasma. J Pharm Res 7:24–32
Gajula R, Pilli NR, Ravi VB, Maddela R, Inamadugu JK, Polagani SR, Busa S (2012) Simultaneous determination of atorvastatin and aspirin in human plasma by LC-MS/MS: Its pharmacokinetic application. Sci Pharm 80:923–940
Hotha KK, Yarramu NR, Kandibedala T, Dasari VB, Vobalaboina V (2012) Simultaneous determination of atorvastatin and glimepiride by LC-MS/MS in human plasma and its application to a pharmacokinetic study. Am J Anal Chem 3:559–569
Vlčková H, Solichová D, Bláha M, Solich P, Nováková L (2011) Microextraction by packed sorbent as sample preparation step for atorvastatin and its metabolites in biological samples-Critical evaluation. J Pharm Biomed Anal 55:301–308
MacWan JS, Ionita IA, Dostalek M, Akhlaghi F (2011) Development and validation of a sensitive, simple, and rapid method for simultaneous quantitation of atorvastatin and its acid and lactone metabolites by liquid chromatography-tandem mass spectrometry (LC-MS/MS). Anal Bioanal Chem 400:423–433
Vethe NT, Munkhaugen J, Andersen AM, Husebye E, Bergan S (2019) A method for direct monitoring of atorvastatin adherence in cardiovascular disease prevention: Quantification of the total exposure to parent drug and major metabolites using 2-channel chromatography and tandem mass spectrometry. Ther Drug Monit 41:19–28
Yu Q, Hu Z-Y, Zhu F-Y, Zhu J-H, Wan L-L, Li Y, Guo C (2011) HPLC–MS–MS for the simultaneous determination of atorvastatin and amlodipine in plasma of hypertensive patients. Chromatographia 73:257–262
Pilli NR, Inamadugu JK, Mullangi R, Karra VK, Vaidya JR, Seshagiri Rao JVLN (2011) Simultaneous determination of atorvastatin, amlodipine, ramipril and benazepril in human plasma by LC-MS/MS and its application to a human pharmacokinetic study. Biomed Chromatogr 25:439–449
Ghosh C, Jain I, Gaur S, Patel N, Upadhyay A, Chakraborty BS (2011) Simultaneous estimation of atorvastatin and its two metabolites from human plasma by ESI-LC-MS/MS. Drug Test Anal 3:352–362
Jani AJ, Dasandi B, Rathnam S, Mehta AA (2010) Liquid chromatographic-MS/ MS determination of atorvastatin and metabolites in human plasma. Eurasian J Anal Chem 5:46–52
Nováková L, Vlčková H, Šatínský D, Sadílek P, Solichová D, Bláha M, Bláha V, Solich P (2009) Ultra high performance liquid chromatography tandem mass spectrometric detection in clinical analysis of simvastatin and atorvastatin. J Chromatogr B 877:2093–2103
Guillén D, Cofán F, Ros E, Millán O, Cofán M, Rimola A, Brunet M (2009) Determination of atorvastatin and its metabolite ortho-hydroxyatorvastatin in human plasma by on-line anion-exchange solid-phase extraction and liquid chromatography tandem mass spectrometry. Anal Bioanal Chem 394:1687–1696
Liu D, Jiang J, Zhou H, Hu P (2008) Quantitative determination of atorvastatin and para-hydroxy atorvastatin in human plasma by LC-MS-MS. J Chromatogr Sci 46:862–866
Ma L, Dong J, Chen XJ, Wang GJ (2007) Development and validation of atorvastatin by LC–ESI–MS and application in bioequivalence research in healthy chinese volunteers. Chromatographia 65:737–741
Bořek-Dohalský V, Huclová J, Barrett B, Němec B, Ulč I, Jelínek I (2006) Validated HPLC-MS-MS method for simultaneous determination of atorvastatin and 2-hydroxyatorvastatin in human plasma - Pharmacokinetic study. Anal Bioanal Chem 386:275–285
Nirogi RVS, Kandikere VN, Shukla M, Mudigonda K, Maurya S, Boosi R, Anjaneyulu Y (2006) Simultaneous quantification of atorvastatin and active metabolites in human plasma by liquid chromatography-tandem mass spectrometry using rosuvastatin as internal standard. Biomed Chromatogr 20:924–936
El-Zailik A, Cheung LK, Wang Y, Sherman V, Chow DSL (2019) Simultaneous LC–MS/MS analysis of simvastatin, atorvastatin, rosuvastatin and their active metabolites for plasma samples of obese patients underwent gastric bypass surgery. J Pharm Biomed Anal 164:258–267
Hermann M, Christensen H, Reubsaet JLE (2005) Determination of atorvastatin and metabolites in human plasma with solid-phase extraction followed by LC-tandem MS. Anal Bioanal Chem 382:1242–1249
Jemal M, Ouyang Z, Chen BC, Teitz D (1999) Quantitation of the acid and lactone forms of atorvastatin and its biotransformation products in human serum by high-performance liquid chromatography with electrospray tandem mass spectrometry. Rapid Commun Mass Spectrom 13:1003–1015
Bullen WW, Miller RA, Hayes RN (1999) Development and validation of a high-performance liquid chromatography tandem mass spectrometry assay for atorvastatin, ortho-hydroxy atorvastatin, and para-hydroxy atorvastatin in human, dog, and rat plasma. J Am Soc Mass Spectrom 10:55–66
Cestari RN, Rocha A, Marques MP, de Oliveira RDR, Lanchote VL (2019) Simultaneous analysis of the total plasma concentration of atorvastatin and its five metabolites and the unbound plasma concentration of atorvastatin: Application in a clinical pharmacokinetic study of single oral dose. J Chromatogr B 1126–1127:121766
Jang H, Mai XL, Lee G, Ahn JH, Rhee J, Truong QK, Vinh D, Hong J, Kim KH (2018) Simultaneous determination of statins in human urine by dilute-and-shoot-liquid chromatography-mass spectrometry. Mass Spectrom Lett 9:95–99
Turner RM, Fontana V, Bayliss M, Whalley S, Santoyo Castelazo A, Pirmohamed M (2018) Development, validation and application of a novel HPLC-MS/MS method for the quantification of atorvastatin, bisoprolol and clopidogrel in a large cardiovascular patient cohort. J Pharm Biomed Anal 159:272–281
Xia B, Li Y, Zhang Y, Xue M, Li X, Xu P, Xia T, Chen S (2018) UHPLC-MS/MS method for determination of atorvastatin calcium in human plasma: Application to a pharmacokinetic study based on healthy volunteers with specific genotype. J Pharm Biomed Anal 160:428–435
Rezk MR, Badr KA (2018) Quantification of amlodipine and atorvastatin in human plasma by UPLC-MS/MS method and its application to a bioequivalence study. Biomed Chromatogr 32:e4224
Van Pelt CK, Corso TN, Schultz GA, Lowes S, Henion J (2001) A four-column parallel chromatography system for isocratic or gradient LC/MS analyses. Anal Chem 73:582–588
Rukthong P, Sangvanich P, Kitchaiya S, Jantratid E, Sathirakul K (2013) The quantitation of atorvastatin in human plasma by solid phase micro-extraction followed by LC-MS/MS and its application to pharmacokinetics study. Songklanakarin J Sci Technol 35:41–50
Ravi VB, Mullangi R, Inamadugu JK, Pilli NR, Gajula R, Ponneri V (2012) Simultaneous determination of atorvastatin and niacin in human plasma by LC-MS/MS and its application to a human pharmacokinetic study. Biomed Chromatogr 26:1436–1443
Shankar Ganesh G, Deme P, Sistla R (2014) Simultaneous determination of atorvastatin calcium and olmesartan medoxomil in rat plasma by liquid chromatography electrospray ionization tandem mass spectrometry and its application to pharmacokinetics in rats. Int J Pharm Pharm Sci 6:464–468
Cai L, Zheng Z, Wang X, Tang L, Mai L, He G, Lei H, Zhong S (2017) Simultaneous determination of atorvastatin and its metabolites in human plasma by UPLC-MS/MS. Anal Methods 9:1038–1045
Braithwaite A, Smith JF (1999) Chromatographic Methods, 5th edn. Kluwer Academic Publishers
Guillarme D, Nguyen DTT, Rudaz S, Veuthey JL (2007) Recent developments in liquid chromatography-Impact on qualitative and quantitative performance. J Chromatogr A 1149:20–29
Wong A, Xiang X, Ong P, Mitchell E, Syn N, Wee I, Kumar A, Yong W, Sethi G, Goh B, Ho P, Wang L (2018) A review on liquid chromatography-tandem mass spectrometry methods for rapid quantification of oncology drugs. Pharmaceutics 10:221
Acknowledgements
Not applicable
Funding
This work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KW: Investigation, Methodology, Writing-Original Draft, Conceptualization. ACR: Validation, Supervision. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wadhwa, K., Rana, A.C. A review on liquid chromatographic methods for the bioanalysis of atorvastatin. Futur J Pharm Sci 7, 4 (2021). https://doi.org/10.1186/s43094-020-00146-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-020-00146-7