
Abstract
Background
To evaluate the feasibility of two-colour index maps containing combined diffusion and perfusion information from simplified intravoxel incoherent motion (IVIM) for liver lesion malignancy assessment.
Methods
Diffusion-weighted data from a respiratory-gated 1.5-T magnetic resonance sequence were analysed in 109 patients with liver lesions. With three b values (0, 50, 800 s/mm2) estimated diffusion coefficient D′, perfusion fraction f′, and apparent diffusion coefficient (ADC) maps were calculated and analysed for regions of interest (ROIs). D′ and f′ cutoff values were determined by differentiating haemangiomas from other lesions and focal nodular hyperplasias from other lesions, respectively. Combined IDf index maps were generated with a voxel value set to 100, if both D′ and f′ voxel values were lower than their cutoff values (1,529.4 × 10-6 mm2/s and 114.4 × 10-3, respectively), otherwise to 0. Moreover, IADC index maps were generated from ADC cutoff value (1,338.5 × 10-6 mm2/s) obtained by differentiating benign from malignant lesions. Discriminatory power was assessed for both IDf and IADC. Index maps were displayed as two-colour overlays to b-800 images and visually assessed within the translucent hyperintense areas.
Results
For IDf, the same diagnostic accuracy was achieved as for the combined use of parameters D′ and f′ (93.6%). Compared to IADC, IDf showed a higher diagnostic accuracy. Visual judgment of IDf yielded an accuracy (95.4%) similar to that of quantitative analysis (93.6%).
Conclusion
Voxel-wise combined two-colour index maps IDf provide similar diagnostic accuracy as ROI-based combination of estimated IVIM parameters D′ and f′ and are suitable for visual assessment of liver lesion malignancy.
Similar content being viewed by others
Key points
-
Index map IDf can replace the combined use of D and f parameters.
-
Two-colour b-800 overlay IDf enables a visual assessment of liver lesion malignancy.
-
Visual judgment and quantitative analysis of IDf showed comparable diagnostic accuracy.
Background
Diffusion-weighted imaging (DWI) is an important magnetic resonance imaging (MRI) technique for detection and differentiation of liver lesions not needing contrast agent administration and should be implemented in standard liver examination in routine clinical practice [1].
While DWI acquired with a low b value (“black blood” images) provides high sensitivity for lesion detection [2, 3], the apparent diffusion coefficient (ADC) determined from at least two b values between 0 and 500–1000 s/mm2 is usually used for lesion characterisation [4, 5]. The intravoxel incoherent motion (IVIM) concept enables the separation of diffusion and perfusion effects on the DWI signal by assuming a biexponential behaviour of signal intensity [6,7,8]. The true diffusion coefficient D, the pseudodiffusion coefficient D*, and the perfusion fraction f, reflecting the relative contribution of perfusion to the DWI signal, are often determined by fit algorithms [9]. These require a high number of b values and thus relatively long acquisition times. Limited data quality due to signal variations caused by respiratory and cardiac motion and due to low signal-to-noise ratio may lead to unstable fitting results, measurement errors, and poor reproducibility [10,11,12,13]. Improved stability and lower acquisition times can be achieved by so-called “simplified IVIM”, which uses explicit computation of IVIM numerically stable parameter estimations in combination with a small number of b values. Simplified IVIM turned out to be valuable for liver lesion characterisation and assessment of therapy in clinical routine [3, 14,15,16,17,18,19,20].
For lesion assessment, voxel-wise evaluation and the creation of parameter maps are important. Still somewhat inconvenient for clinical use is the quantitative analysis of regions of interests (ROI) in the IVIM parameter maps. The use of colour-coded maps [21, 22] as overlay over b0 DWI images [14,15,16, 23] enables visual lesion assessment. For the assessment of malignancy, knowledge of the cutoff values of each IVIM parameter is necessary. From ischemic stroke diagnostic using computed tomography perfusion, the use of two-colour index maps is known allowing a rapid and easy image interpretation [24, 25]. Suitable two-colour index maps obtained from IVIM parameters could allow a rapid and easy image interpretation with respect to malignancy.
The purpose of this study was to create and evaluate two-colour index maps, which combines diffusion and perfusion information obtained by simplified IVIM for convenient visual assessment of liver lesion malignancy.
Methods
Study cohort
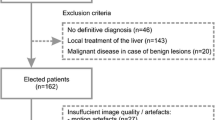
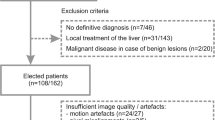
This retrospective study was approved by the local institutional review board of the University Hospital Bonn, Germany, with waiver for written informed patient consent. Data of 1,721 consecutive examinations (from February 2013 to September 2016) of patients, who received a 4 b value DWI sequence at 1.5 T, were reviewed. Data of 1350 examinations were not used because the patients had no liver lesions, only cysts, or lesions < 1 cm, or because it was not the first examination in the study time frame, so that data of 371 different patients with at least one focal liver lesion ≥ 1 cm other than cysts were included. Of these 371 patients, 262 (70.6%) were excluded due to lack of a definitive diagnosis based on histology or typical imaging characteristics (n = 46), local treatment of the liver (n = 143), insufficient image quality caused by motion artifacts (n = 27) or pixel misalignments (n = 5), unfavourable lesion location as close to prior biopsy or drainage tracts or at the edge of the liver (n = 6), partial volume of an adjacent slice (n = 10), or difficulties to identify the lesions on DWI (n = 5). In the presence of a combination of (non-cystic) benign lesions and malignant disease, patients were excluded because malignant disease may affect the appearance of benign liver lesions, e.g., due to thrombosis (n = 20). Finally, data of 109 patients were analysed (Table 1).
These patients had already been examined in an upcoming study by Mesropyan et al and in a previous study [15], where basic investigations concerning simplified IVIM for liver lesion characterisation [15] and different ROI placement and analysis methods had been performed in an upcoming study by Mesropyan et al. In the present study, the data were used to evaluate two-colour index maps constructed with the help of IVIM parameter analysis results.
Cholangiocellular carcinomas (CCCs) were histologically proven. Hepatocellular carcinomas (HCCs) were either histologically proven or diagnosed according to the American Association for the Study for Liver Disease MRI criteria [26]. Diagnosis of metastasis was histologically proven or based on typical imaging features in combination with histologically proven primary cancer. Diagnosis of focal nodular hyperplasia (FNH) or haemangioma was established based on typical radiological findings on contrast-enhanced MRI and was confirmed by at least one follow-up examination.
Magnetic resonance imaging
Imaging was performed on a clinical whole-body 1.5-T MRI system (Ingenia, Philips Healthcare, Eindhoven, The Netherlands) equipped with powerful gradient system (45 mT/m maximum amplitude, 200 T/m/s maximum slew rate) and 32-channel abdominal coil with digital interface for signal reception. DWI with a respiratory-triggered single-shot spin-echo echo-planar imaging variant (Table 2) with four b values (0, 50, 250, 800 s/mm2) was applied before contrast agent administration. Isotropic diffusion-weighted images were reconstructed by from the images with diffusion-sensitised gradients in three orthogonal directions on the MRI system.
Postprocessing
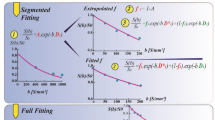
IVIM parameters D and f as well as conventional ADC were calculated voxel-wise from b = 0, 50, and 800 s/mm2 by using the following approximations:
Parameter maps and two-colour index maps (see below) were calculated offline using custom written software in MATLAB (MathWorks, Natick, Massachusetts, USA).
Image analysis
Image analysis by ROIs was performed by a radiologist (N.M.) with 3 years of experience and checked by a radiologist (C.C.P.) with 10 years of experience in abdominal imaging and a physicist (P.M.) with more than 20 years of experience in DWI. All were blinded to clinical information. One reference lesion per lesion type was analysed. A two-dimensional ROI was placed centrally in each lesion on a single representative slice. This slice was largely unaffected by motion and susceptibility artifacts and pixel misalignments and not at the rim of the lesion to avoid partial volume effects. ROIs were drawn as large as possible using DWI with the highest contrast between lesion and normal tissue. Central necrosis, cystic components, and scars as found by hyperintensities on b0 images and/or hypointensities on b-800 images were excluded in an upcoming study by Mesropyan et al. After visually cross-checking for pixel misalignments between images with different b values, the ROI was analysed in the related parameter maps ADC, D′, and f′ and saved for later use (see below).
Construction of two-colour index maps
Two-colour index maps IADC, ID, and If were constructed from suitable cutoff values for ADC, D′, and f′, respectively. The cutoff values were determined as previously introduced [14, 15]: the ADC cutoff value was determined by receiver operating characteristic (ROC) analysis of malignant and benign lesion groups; for the combined use of D′ and f′, the D’ cutoff value was determined by differentiation between haemangiomas and all other lesions and the f′ cutoff value by differentiation between FNHs and all other lesions. Motivated by the high diffusion coefficient of haemangiomas [14, 15, 27, 28] and the high perfusion fraction of FNHs [14, 15, 29], lesions were assigned as malignant if ROI-wise mean values of D′ and f′ were both below their cutoff values, and otherwise as benign. In the index maps, a voxel value was set to 100 if the corresponding parameter voxel value was lower than the determined cutoff value; otherwise, the voxel value was set to 0. By combining ID and If, the index map IDf was generated. For IDf, a voxel value was set to 100 if the corresponding voxel values of ID and If were both 100; otherwise, the voxel value was set to 0. Voxel values 0 and 100 were displayed in green and red, respectively, indicating benign and malignant structures. These index maps were displayed as overlay over the DWI b-800 images.
Evaluation of the two-colour index maps
First, to ensure that the voxel-wise consideration of the cutoff values does not worsen diagnostic performance compared to ROI-wise, for IADC, ID, and If, the same ROC analysis was performed as for the related original parameter (see the "Construction of two-colour index maps" section). AUC values were compared pairwise. Second, to compare the diagnostic performance of ADC, D′, and f′ as well as of IDf, IADC, and ADC, all maps were quantitatively analysed using ROIs (see the “Image analysis” section). ROC analyses of the benign and malignant lesion groups were then performed. AUC values were compared with each other.
Third, the IADC and IDf index maps were evaluated visually by one investigator (P.M.). The visual assessment was restricted to areas of translucent hyperintensity from DWI b-800 images, whereby necrosis, cystic components, and scars identified as hyperintense areas on b-0 images and/or hypointense areas on b-800 images were excluded. A four-point scale was used, as follows: (1) definitely malignant, if the red voxels dominated definitely; (2) probably malignant, if red voxels dominated only slightly; (3) probably benign, if green voxels dominated only slightly; and (4) definitely benign, if green voxels dominated definitely.
The accuracy of IADC and IDf for lesion differentiation by visual assessment was determined and compared with each other and with ADC.
The assessment was repeated after 4 months by the same investigator (P.M.) and by a second independent investigator (C.C.P.).
Statistical analysis
Statistically significant differences (p < 0.05) between groups (independent samples) were tested in SPSS (version 24.0, IBM, Armonk, New York , USA) by using Student t test or non-parametric Mann–Whitney U test, depending on whether the data were normally distributed or not. In order to differentiate between two groups, ROC analysis was performed using pROC package in R (version 1.17.0.1, open source package, accessible at http://expasy.org/tools/pROC/ under the GNU General Public License) [30]. Youden’s index was used to determine the optimal cutoff value of the ROC curve providing the highest combination of sensitivity and specificity. DeLong method was used to compare the area under the curve (AUC) of dependent and independent ROC curves [31]. The intraclass correlation coefficients (ICCs) were calculated for the visual assessment results of the same investigators (ICCintra) and of the two different investigators (ICCinter).
Results
Examples of DWI and two-colour index maps are given in Figs. 1 and 2.

Typical examples of two-colour index maps. Combined index maps IDf are given in comparison to index maps IADC together with ID and If, overlaid to b-800 images, for (a) FNH together with two haemangiomas (blue x), (b) HCC, (c) CCC together with bilioma (red x), and (d) metastasis from colorectal carcinoma (CRC). The FNH reveals almost everywhere voxels with perfusion fraction above cutoff (If green) so that IDf shows clear benignity despite diffusion coefficient below cutoff (ID red), IADC showed slightly less green voxels compared to IDf (79% versus 92%). The haemangiomas shows almost everywhere voxels with diffusion coefficient above cutoff (ID green), so that IDf shows clear benignity despite the low perfusion fraction (If red), the same is valid for IADC. The HCC shows area-wide diffusion coefficient below cutoff (red ID), and mainly perfusion fraction below cutoff with heterogeneous distribution (If scattered red) and thus also IDf showing clear malignancy, IADC shows less red voxels compared to IDf (41% versus 69%) showing benignity, the visual assessment was “probably” benign. The CCC appears on all maps mainly red showing clear malignancy on IDf and IADC maps. The bilioma looks identical to the haemangiomas. The CRC reveals mainly red voxels within the selected region of interest, which excluded hypointense region on b-800 image (necrosis). CCC Cholangiocellular carcinoma, CRC Metastasis from colorectal carcinoma, FNH Focal nodular hyperplasia, HCC Hepatocellular carcinoma

Further examples of combined two-colour index maps. Combined index maps IDf are given in comparison to index maps IADC together with ID and If, overlaid to b-800 images, for (a) FNH, (b) HCC, (c) metastasis of breast cancer, and (d) HCC. The FNH with central scar (a) and the HCC with central necrosis (b) show similar behaviour on all index maps with nearly all voxels being red on ID and about half of the voxels being red with scattered distribution on If and also on IADC and IDf. On IADC, visual assessment of FNH is “probable malignant” and of HCC “probably benign,” which is wrong in both cases. Quantitative values are both (50% and 45%, respectively) just below the threshold to malignancy (at 53%) leading to correct assignment for FNH and wrong for HCC. On IDf, visual assessment of FNH is “probable benign” and of HCC “probably malignant,” which is correct in both cases. Quantitative values (38% and 55%, respectively) were below and above threshold (50%), respectively, leading also to correct assignments. The metastasis with central necrosis (c) shows only a small margin of vital tumour, which can be easier captured by visible judgment than by ROI analysis with unclear tissue boundary. The HCC (d) shows the typical behaviour of a haemangioma (see Fig. 1a) and the assignment is false negative. However, the hypointense area of the left liver lobe adjacent to the lesion on b-800 indicates motion influences, which raise the diffusion coefficient of the liver tissue and lesion artificially as can be seen on ID, IADC, and IDf index maps. CCC Cholangiocellular carcinoma, FNH Focal nodular hyperplasia, HCC Hepatocellular carcinoma
Verification of voxel-wise cutoff value applicability
ROC analysis of ROI-based analysed index maps and related original parameter maps revealed similar AUC values (Table 3). The comparison of AUC values revealed no significant differences, as expected, neither between IADC and ADC in discriminating benign from malignant lesions (0.958 versus 0.945, p = 0.196), nor between ID and D′ in discriminating haemangiomas from all other lesions (0.985 versus 0.985, p = 1.000), nor between If and f′ in discriminating FNHs and all other lesions (0.968 versus 0.974, p = 0.294).
Quantitative evaluation of index maps IADC and IDf
All parameter values were significantly lower for malignant lesions than for benign (Table 4), e.g., for ADC 1,124 ± 180 × 10-6 mm2/s (mean ± standard deviation) versus 1,692 ± 313 × 10-6 mm2/s (p < 0.001). Accordingly, for all index values, the numbers of red voxels were significantly higher for malignant than for benign lesions, e.g., for IADC 80% ± 21% versus 17% ± 25% (p < 0.001) and for IDf 76% ± 17% versus 20% ± 18% (p < 0.001).
As can be seen in Table 4, among the single parameters ADC, D’, and f′, the ADC was best suited to discriminate benign and malignant lesions. The AUC value of ADC was significantly higher than that of D′ (0.958 versus 0.902, p = 0.001) and f′ (0.958 versus 0.622, p < 0.001), AUC of D′ was significantly higher than that of f’ (0.902 versus 0.622, p = 0.001). By ADC, 89.9% of the lesions were correctly identified as malignant and benign (cutoff value 1,338.5 × 10-6 mm2/s). By using the combination of D′ and f′, 93.6% of the lesions were correctly identified (cutoff values 1,529.4 × 10-6 mm2/s and 114.4 × 10-3, respectively), which was an improvement compared to ADC.
Comparing the AUC values of IDf and IADC, larger values were found for IDf than for IADC (0.975 versus 0.945), but differences were not significant (p = 0.168). The diagnostic accuracy was higher for IDf than for IADC. With IDf 93.6% of the lesions (cutoff value 50.2%) were correctly identified as benign and malignant, with IADC 88.1% (cutoff value 53.4%). Falsely identified cases by IDf versus IADC were 1 versus 2 FNHs, 1 versus 1 haemangiomas, 4 versus 3 HCCs, 0 versus 1 CCCs, and 1 versus 6 metastases. IDf was superior to IADC especially in case of metastases identifying 5 cases correctly as malignant, which were falsely assigned as benign by IADC.
Visual evaluation of index maps IADC and IDf
By visual judgment of IDf and IADC maps within translucent hyperintensity from DWI b-800 images (Table 5), a similar number of lesions were correctly identified as by quantitative analysis using ROIs excluding central necrosis, cystic components, and scars (95.4% instead of 93.6% for IDf and 90.8% instead of 88.1% for IADC). As in the quantitative analysis, the reached diagnostic accuracy was higher for IDf than for IADC. With IDf 95.4% of the lesions were correctly identified, with IADC 90.8%. The assignment was “definite” in 87.2% for IDf and in 89.9% for IADC and “probable” in 12.8% for IDf and in 10.1% for IADC. “Probable” assignment by IDf and IADC was mainly found for FNHs (4 and 7, respectively) and HCCs (4 and 6, respectively) and only rarely for haemangiomas (0 and 1, respectively), CCCs (1 and 0, respectively), and metastases (2 and 0, respectively). Falsely identified cases by IDf versus IADC were 2 versus 5 FNHs, 1 versus 1 haemangiomas, 1 versus 3 HCCs, 0 versus 0 CCCs, and 1 versus 1 metastasis. IDf was superior to IADC especially in case of FNHs and HCCs identifying 3 FNHs and 2 HCCs correctly, which were falsely assigned by IADC. Examples are given in Fig. 1b, Fig. 2a, and Fig. 2b. Visual judgment of IDf was superior especially in case of HCCs identifying 4 HCCs correctly, which were falsely assigned by quantitative analysis. Visual judgment of IADC was superior especially in case of metastases but inferior in case of FNHs identifying 5 metastases correctly, which were falsely assigned by quantitative analysis, and 3 FNHs falsely (as “probable malignant”), which were correctly identified by quantitative analysis.
The repeated analysis by the same investigator and by the independent investigator (see Table 5) revealed excellent intraobserver and interobserver reliability (ICCintra 0.992 for IADC and 0.989 for IDf; ICCinter 0.986 for IADC and 0.977 for IDf).
Discussion
In this study, simplified IVIM was used to create combined two-colour index maps IDf from parameters D′ and f′ as overlay to b-800 images in order to facilitate visual assessment of liver lesions. Red voxels show diffusion and perfusion restrictions and indicate malignancy in combination with translucent b-800 hyperintensity. The main result was that the voxel-wise combination of D′ and f′ thresholds in the form of the IDf index map provides identical diagnostic accuracy as the ROI-based combined analysis of the D′ and f′ parameter maps. A higher diagnostic accuracy was found for IDf than for IADC (created from ADC). Visual judgment of the IDf index map as two-colour overlay to b-800 images showed comparable diagnostic accuracy than quantitative analysis of IDf.
In previous simplified IVIM studies on liver lesions at 1.5 and 3.0 T it was found that ADC is the best single parameter to discriminate between malignant and benign liver lesions but that improved discriminatory power could be reached by combined use of D′ and f′ [14, 15]. This result was confirmed in the present study. Compared to the previous 1.5-T study [15], which was performed on the same patient group than the present study but with new ROI analysis, higher diagnostic accuracy was reached, for ADC (89.9% versus 82.1%) and for combined D′ and f′ (93.6% versus 85.6%). In the present study, one reference ROI per lesion type and patient was included, in the previous study up to 5 lesions per lesion type and patient were included and averaged for analysis (clustered analysis). Necrotic areas, liquids, and scares were excluded from ROIs in both studies, but can also be excluded retrospectively by automatically selecting voxels with low diffusion coefficients with the help of histogram analysis of D′ (upcoming study by Mesropyan et al).
New in the present work is the creation and evaluation of the index maps IDf, which combine the information from D′ and f′, use only two colours, and are presented as overlay to b-800 in order to be able to assess only the vital tumour areas by translucent hyperintensity and to exclude necrosis, cystic components, and scars from assessment. Up to now, colour-coded maps with more than two colours have been used for the different IVIM parameters [13, 21, 22, 32], sometimes presented as overlays to b0 images [14, 15]. Whether the ROI-wise obtained and combined cutoff values of D′ and f′ would also work voxel-wise in IDf was not clear in advance. Perfusion and diffusion restrictions do not necessarily have to occur in the same voxels. But the fact that IDf provided identical diagnostic accuracy than combined use of D′ and f′ (93.6% versus 93.6%) means that the ROI-wise obtained cutoff values of the parameters can be applied voxel-wise in the index maps.
For IDf higher accuracy was reached than for IADC, by quantitative analysis (93.6% versus 88.1%) and by visual judgment (95.4% versus 90.8%). The relative good performance of IADC is due to the fact that for liver lesion differentiation diffusion and perfusion influences act in the same direction.
When visually assessing two-colour index maps, it is only necessary to distinguish whether more or less than half of the voxels in the tumour areas of interest are red. This allows a rapid and easy image interpretation also for less skilled operators. Excellent intraobserver and interobserver reliability was achieved. By visual judgment comparable diagnostic accuracy was reached than by ROI-based quantitative analysis, for IDf (95.4% versus 93.6%) and IADC (90.8% versus 88.1%). The assignment malignant/benign was “definite” in about 90% of the cases and “probable” in about 10%, for IDf and IADC. Some of the FNHs showed relatively high numbers of red voxels on IDf with scattered distribution caused by heterogeneous perfusion as can be seen on If index map. Those FNHs looked similar to typical HCCs (Fig. 2a, b). Visual assessment of those lesions was less accurate than ROI-based quantitative analysis. Metastases, on the other hand, often have only a narrow margin of vital tumour tissue, so that an exact ROI positioning is difficult leading to less accurate results in case of quantitative analysis compared to visual assessment (Fig. 2c).
General concerns regarding the simplified IVIM approach as for example the b value choice have already been addressed in the previous studies [14, 15]. Only three of the four acquired b values were used, because no diagnostic added value was found for the fourth b value (250 s/mm2) and the determination of D* [14, 15]. Simplified IVIM parameter calculations by using approximations and explicit formulas instead of fitting procedures are simple and stable and lead to reliable information. Exceptions are as generally low signal-to-noise ratios (e.g., patients with hemochromatosis or fatty liver), small lesions (partial volume effects), or presence of artifacts. Due to motion influences artificially enlarged D′ and reduced f′ values may be measured, especially for the left liver lobe and on slices close to the heart. It is important to check the surrounding liver in the b-800 image for signal loss (Fig. 2d). Since the IVIM parameter f depends on the relaxation times, f may vary with field strength and sequence parameters used (especially b values, echo times, and repetition times) [33, 34], this also applies to the cutoff points used for the index maps. The new combined two-colour index maps IDf were checked on the same patients who provided the cutoff points for generation in order to enable a direct comparison with the combined use of the parameter maps D′ and f′. A validation study is planned on a larger patient cohort, which also includes rarer and atypical lesions as well as lesions difficult to identify in DWI. It is interesting to compare the use of the two-colour index maps IDf with full set of conventional protocol in terms of reading time and reader confidence.
In conclusion, the voxel-wise combined index maps IDf and the ROI-based combination of D′ and f′ parameters provide concordant diagnostic accuracy for the differentiation of malignant and benign liver lesions. The IDf index map used as two-colour overlay to b-800 images can be considered as a new tool for visual assessment of liver lesion malignancy.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ADC:
-
Apparent diffusion coefficient
- AUC:
-
Area under the curve
- CCC:
-
Cholangiocellular carcinoma
- CRC:
-
Metastasis from colorectal carcinoma
- D′:
-
Estimated diffusion coefficient
- DWI:
-
Diffusion-weighted imaging
- f′:
-
Estimated perfusion fraction
- FNH:
-
Focal nodular hyperplasia
- HCC:
-
Hepatocellular carcinoma
- IADC :
-
ADC index maps
- ICC:
-
Intraclass correlation coefficient
- ID :
-
D′ index maps
- IDf :
-
D′ and f′ combined index maps
- If :
-
f′ index maps
- IVIM:
-
Intravoxel incoherent motion
- MRI:
-
Magnetic resonance imaging
- ROC:
-
Receiver operating characteristic
- ROI:
-
Region of interest
References
Taouli B (2012) Diffusion-weighted MR imaging for liver lesion characterization: a critical look. Radiology 262:378–380. https://doi.org/10.1148/radiol.11112417
Takahara T, Kwee TC (2012) Low b-value diffusion-weighted imaging: emerging applications in the body. J Magn Reson Imaging 35:1266–1273. https://doi.org/10.1002/jmri.22857
Coenegrachts K, Delanote J, Ter Beek L et al (2009) Evaluation of true diffusion, perfusion factor, and apparent diffusion coefficient in non-necrotic liver metastases and uncomplicated liver hemangiomas using black-blood echo planar imaging. Eur J Radiol 69:131–138. https://doi.org/10.1016/j.ejrad.2007.09.013
Miller FH, Hammond N, Siddiqi AJ, et al (2010) Utility of diffusion-weighted MRI in distinguishing benign and malignant hepatic lesions. J Magn Reson Imaging 32:138–147. https://doi.org/10.1002/jmri.22235
Parikh T, Drew SJ, Lee VS, et al (2008) Focal liver lesion detection and characterization with diffusion-weighted MR imaging: comparison with standard breath-hold T2-weighted imaging. Radiology 246:812–822. https://doi.org/10.1148/radiol.2463070432
Padhani AR, Liu G, Koh DM et al (2009) Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia 11:102–125. https://doi.org/10.1593/neo.81328
Koh DM, Collins DJ, Orton MR (2011) Intravoxel incoherent motion in body diffusion-weighted MRI: reality and challenges. AJR Am J Roentgenol 196:1351–1361. https://doi.org/10.2214/AJR.10.5515
Guiu B, Cercueil JP (2011) Liver diffusion-weighted MR imaging: the tower of Babel? Eur Radiol 21:463–467. https://doi.org/10.1007/s00330-010-2017-y
Le Bihan D, Breton E, Lallemand D et al (1988) Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 168:497–505. https://doi.org/10.1148/radiology.168.2.3393671
Andreou A, Koh DM, Collins DJ, et al (2013) Measurement reproducibility of perfusion fraction and pseudodiffusion coefficient derived by intravoxel incoherent motion diffusion-weighted MR imaging in normal liver and metastases. Eur Radiol 23:428–434. https://doi.org/10.1007/s00330-012-2604-1
Kakite S, Dyvorne H, Besa C, et al (2015) Hepatocellular carcinoma: short-term reproducibility of apparent diffusion coefficient and intravoxel incoherent motion parameters at 3.0T. J Magn Reson Imaging 41:149–156. https://doi.org/10.1002/jmri.24538
Cho GY, Kim S, Jensen JH, Storey P, Sodickson DK, Sigmund EE (2012) A versatile flow phantom for intravoxel incoherent motion MRI. Magn Reson 67:1710–1720. https://doi.org/10.1002/mrm.23193
Lee Y, Lee SS, Kim N, et al (2015) Intravoxel incoherent motion diffusion-weighted MR imaging of the liver: effect of triggering methods on regional variability and measurement repeatability of quantitative parameters. Radiology 274:405–415. https://doi.org/10.1148/radiol.14140759
Mürtz P, Pieper CC, Reick M, et al (2019) Is liver lesion characterisation by simplified IVIM DWI also feasible at 3.0 T? Eur Radiol 29:5889–5900. https://doi.org/10.1007/s00330-019-06192-x
Mürtz P, Sprinkart AM, Reick M, et al (2018) Accurate IVIM model-based liver lesion characterisation can be achieved with only three b-value DWI. Eur Radiol 28:4418–4428. https://doi.org/10.1007/s00330-018-5401-7
Penner A-H, Sprinkart AM, Kukuk GM, et al (2013) Intravoxel incoherent motion model-based liver lesion characterisation from three b-value diffusion-weighted MRI. Eur Radiol 23:2773–2783. https://doi.org/10.1007/s00330-013-2869-z
Pieper C, Meyer C, Sprinkart AM, et al (2016) The value of intravoxel incoherent motion model-based diffusion-weighted imaging for outcome prediction in resin-based radioembolization of breast cancer liver metastases. Onco Targets Ther 9:4089–4098. https://doi.org/10.2147/OTT.S104770
Mürtz P, Penner A-H, Pfeiffer A-K, et al (2016) Intravoxel incoherent motion model-based analysis of diffusion-weighted magnetic resonance imaging with 3 b-values for response assessment in locoregional therapy of hepatocellular carcinoma. Onco Targets Ther 9:6425–6433. https://doi.org/10.2147/OTT.S113909
Pieper CC, Sprinkart AM, Meyer C, et al (2016) Evaluation of a simplified intravoxel incoherent motion (IVIM) analysis of diffusion-weighted imaging for prediction of tumor size changes and imaging response in breast cancer liver metastases undergoing radioembolization: a retrospective single center analysis. Medicine (Baltimore) 95:e3275. https://doi.org/10.1097/MD.0000000000003275
Pieper CC, Willinek WA, Meyer C, et al (2016) Intravoxel incoherent motion diffusion-weighted MR imaging for prediction of early arterial blood flow stasis in radioembolization of breast cancer liver metastases. J Vasc Interv Radiol 27:1320–1328. https://doi.org/10.1016/j.jvir.2016.04.018
Wang M, Li X, Zou J, Chen X, Chen S, Xiang W (2016) Evaluation of hepatic tumors using intravoxel incoherent motion diffusion-weighted MRI. Med Sci Monit 22:702–709. https://doi.org/10.12659/MSM.895909
Luo M, Zhang L, Jiang X, Zhang W (2017) Intravoxel incoherent motion diffusion-weighted imaging: evaluation of the differentiation of solid hepatic lesions. Transl Oncol 10:831–838. https://doi.org/10.1016/j.tranon.2017.08.003
Concia M, Sprinkart AM, Penner A-H, et al (2014) Diffusion-weighted magnetic resonance imaging of the pancreas: diagnostic benefit from an intravoxel incoherent motion model-based 3 b-value analysis. Invest Radiol 49:93–100. https://doi.org/10.1097/RLI.0b013e3182a71cc3
Ukmar M, Degrassi F, Pozzi Mucelli RA, Neri F, Mucelli FP, Cova MA (2017) Perfusion CT in acute stroke: effectiveness of automatically-generated colour maps. Br J Radiol 90:1–10. https://doi.org/10.1259/bjr.20150472
Lin L, Bivard A, Parsons MW (2013) Perfusion patterns of ischemic stroke on computed tomography perfusion. J Stroke 15:164–173. https://doi.org/10.5853/jos.2013.15.3.164
Bruix J, Sherman M, Llovet JM, et al (2001) Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol 35:421–430. https://doi.org/10.1016/s0168-8278(01)00130-1
Choi IY, Lee SS, Sung YS, et al (2017) Intravoxel incoherent motion diffusion-weighted imaging for characterizing focal hepatic lesions: correlation with lesion enhancement. J Magn Reson Imaging 45:1589–1598. https://doi.org/10.1002/jmri.25492
Zhu L, Cheng Q, Luo W, Bao L, Guo G (2015) A comparative study of apparent diffusion coefficient and intravoxel incoherent motion-derived parameters for the characterization of common solid hepatic tumors. Acta Radiol 56:1411–1418. https://doi.org/10.1177/0284185114559426
Luo M, Zhang L, Jiang X-H, Zhang W-D (2017) Intravoxel incoherent motion: application in differentiation of hepatocellular carcinoma and focal nodular hyperplasia. Diagn Interv Radiol 23:263–271. https://doi.org/10.5152/dir.2017.16595
Robin X, Turck N, Hainard A, et al (2011) pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics 12:1–8. https://doi.org/10.1186/1471-2105-12-77
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:837–845. https://doi.org/10.2307/2531595
Ter Voert EEGW, Delso G, Porto M et al (2016) Intravoxel incoherent motion protocol evaluation and data quality in normal and malignant liver tissue and comparison to the literature. Invest Radiol 51:90–99. https://doi.org/10.1097/RLI.0000000000000207
Grech-Sollars M, Hales PW, Miyazaki K, et al (2015) Multi-centre reproducibility of diffusion MRI parameters for clinical sequences in the brain. NMR Biomed 28:468–485. https://doi.org/10.1002/nbm.3269
Lemke A, Laun FB, Simon D, Stieltjes B, Schad LR (2010) An in vivo verification of the intravoxel incoherent motion effect in diffusion-weighted imaging of the abdomen. Magn Reson Med 64:1580–1585. https://doi.org/10.1002/mrm.22565
Funding
The authors state that this work has not received any funding. Open Access funding enabled and organised by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Study concept: PM and CP; manuscript preparation and editing: PM, CP, NM, AS, and UA; data acquisition and analysis: NM, PM, CP, AS, WB, and JL. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The local institutional review board of the University Hospital Bonn, Germany, approved the retrospectively performed IVIM analysis of DWI MRI data from clinical routine examinations (reference number 303/16).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mürtz, P., Mesropyan, N., Sprinkart, A.M. et al. Simplified intravoxel incoherent motion diffusion-weighted MRI of liver lesions: feasibility of combined two-colour index maps. Eur Radiol Exp 5, 33 (2021). https://doi.org/10.1186/s41747-021-00233-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41747-021-00233-1