
Abstract
Background
While acknowledgement of emotions’ importance in simulation-based education is emerging, there are concerns regarding how education researchers understand the concept of emotions for them to deliberately incorporate emotionally charged scenarios into simulation-based education. This concern is highlighted especially in the context of medical education often lacking strong theoretical integration. To map out how current simulation-based education literature conceptualises emotion, we conducted a scoping review on how emotions and closely related constructs (e.g. stress, and emotional intelligence) are conceptualised in simulation-based education articles that feature medical students, residents, and fellows.
Methods
The scoping review was based on articles published in the last decade identified through database searches (EMBASE and Medline) and hand-searched articles. Data extraction included the constructs featured in the articles, their definitions, instruments used, and the types of emotions captured. Only empirical articles were included (e.g. no review or opinion articles). Data were charted via descriptive analyses.
Results
A total of 141 articles were reviewed. Stress was featured in 88 of the articles, while emotions and emotional intelligence were highlighted in 45 and 34 articles respectively. Conceptualisations of emotions lacked integration of theory. Measurements of emotions mostly relied on self-reports while stress was often measured via physiological and self-report measurements. Negative emotions such as anxiety were sometimes seen as interchangeable with the term stress. No inferences were made about specific emotions of participants from their emotional intelligence.
Conclusions
Our scoping review illustrates that learners in simulation-based education are most often anxious and fearful. However, this is partially due to medical education prioritising measuring negative emotions. Further theoretical integration when examining emotions and stress may help broaden the scope towards other kinds of emotions and better conceptualisations of their impact. We call for simulation education researchers to reflect on how they understand emotions, and whether their understanding may neglect any specific aspect of affective experiences their simulation participants may have.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Training for delivering better patient outcomes requires understanding emotions—they are pervasive throughout healthcare environments for both physicians and trainees [1]. Moreover, recent medical education research has highlighted the roles and potential impact of emotions in training future doctors [2, 3]. Not only can emotionally charged scenarios sway clinical decisions [4], but being able to understand, monitor, and manage one’s own and others’ emotions (i.e. emotional intelligence) is deemed crucial for developing core competencies physicians require [5] as it relates to desirable aptitudes such as resiliency against burnout [6], leadership [7], and communication [8, 9]. In sum, medical education can help prepare learners to be emotionally resilient and better emotionally attuned to one another and their patients. Therefore, advancing these goals and informing practice requires a better understanding of medical trainees’ emotions during medical education, including simulations.
Simulation-based education (SBE) is no exception to emotions’ pervasiveness: a recent conceptual review by LeBlanc and Posner highlighted how SBE can be “rife with emotional situations” [10], (p.6). Indeed, the ubiquitous nature of emotions in medicine, including in SBE has been echoed previously [1, 11] and its potential impact on healthcare practice and education has been empirically documented in various domains, including diagnostic reasoning [12], patient-physician communication [13], and patient safety issues related to medical errors [14, 15].
LeBlanc and Posner’s review [10] also underscored how simulation educators’ various beliefs regarding the role of emotions are often based on personal experiences—one concern regarding this is whether educators can consistently be “thoughtful and deliberate” [10], (p.5) when incorporating emotional experiences into SBE scenarios. This can be especially so when simulation educators conceptualise and use the term emotions in everyday and professional discourse. For example, McNaughton’s discourse analysis shows how educators can view emotions not only as a “series of biological and neurochemical responses”, but also as “skills that can be learned” (i.e. emotional intelligence; EI), and “a set of practices that are constructed by social, cultural, and political arrangements” [11], (p.73). To put the concern another way: are medical educators understanding emotions as something interchangeable to EI? Will they distinguish something like stress (also a product of “series of biological and neurochemical responses”) from emotions? To truly be purposeful in incorporating emotions in SBE, educators should be aware of how they conceptualise emotions, and why they subscribe to their understanding.
Integrating a theoretical framework into research is a straightforward way of advancing understanding of emotions (e.g. see Coppin & Sander [16]). While medical education research often lacks strong theoretical integration [17, 18], there have been calls for integrating frameworks such as the Control Value Theory of Achievement Emotions (CVT) [1, 2, 19], a prominent theoretical framework in educational psychology [20, 21]. CVT’s definition of emotion aligns with the consensus mainstream emotion theories and its definition can help educators distinguish emotions from other affective phenomena including moods and stress [19, 22]. CVT defines emotions as multi-componential psychological responses produced by coordinated affective, cognitive, motivational, and expressive processes. Emotions are described based on a three-dimensional taxonomy: valence (negative or positive), activation (deactivating or activating, also known as arousal), and object focus (retrospective outcome, concurrent activity, or prospective outcome). Research indicates that positive-activating emotions (e.g. enjoyment) should favour learning outcomes, while other types of emotions tend to hinder learning outcomes, especially negative-deactivating emotions such as hopelessness [23]. While CVT has been utilised in contemporary research in medical education [12, 24], it is unclear how widespread incorporating such frameworks into SBE research and simulation design is.
To help address the concern of whether simulation educators can consistently be deliberate in incorporating emotional experiences into SBE scenarios, a scoping review aiming to distill how simulation educators understand and study emotions was conducted. The review examined not only emotions but also closely related constructs: mood, EI, and stress.
The peripheral constructs to emotions: mood, stress, and emotional intelligence
Previous research reports that terms such as mood and stress are closely related constructs to emotions, although they are not interchangeable terms and can be differentiated [22, 25]. EI, while not used interchangeably with emotions in the psychology or educational psychology literature, is often viewed by medical educators as one way of conceptualising emotions [11].We first identified mood as a construct of interest for our review, as we thought it may be possible for researchers to mistakenly use the term interchangeably with emotions, despite the general consensus from emotion researchers [22].
We identified stress as another construct of interest. Stress is “inextricably linked to anxiety” [26] (p.4), where such discrete negative emotions are the consequence of a stress response [25, 26]. In other words, where there is stress response, one would expect negative emotions [25]. In addition, like emotions, stress has traditionally been hard to define [27], and there was concern regarding what approach recent SBE research would take. Given the uncertainty of how stress would be conceptualised, and with stress having a close relationship with negative emotions, we reasoned that studies that examined stress held potential to infer or directly measure emotions.
We lastly considered EI. EI is deemed a highly desirable trait in medical trainees; often measured as emotional quotient (EQ) through instruments such as Bar-On’s Emotional Quotient Inventory (EQ-i) [28]. EI is associated with leadership skills, non-technical skills, reduced stress/burnout, higher job satisfaction, and better relationships with patients [29]. While EI is not an affective phenomena and moreover a trait rather than a state, it directly concerns recognising and regulating emotions [30]. Therefore, with the popularity of examining EI in SBE literature, coupled with its relationship recognising and managing emotions, we were interested in how the literature approached EI. Our interest included whether any emotional experiences would be inferred from EI measurements.
Objectives and research questions
The objective of this scoping review was to map out how recent SBE research approached studying emotions. Our primary research question was the following: How are emotions and closely related constructs (i.e. stress, emotional intelligence, and mood) conceptualised in articles that focus on simulation environments, with medical students and trainees as the population of interest?
We formulated sets of complementary secondary questions (SQ) that align with our objective:
-
(SQ1): What is known about how emotions are conceptualised?
-
◦ (SQ1-A) Are emotions defined?
-
◦ (SQ1-B) Do the articles cite a theory?
-
◦ (SQ1-C) How are closely related constructs conceptualised?
-
-
(SQ2): What is known about how emotions are measured?
-
◦ (SQ2-A) How are other closely related constructs measured?
-
-
(SQ3): What are the emotions medical students and trainees experienced?
-
(SQ4): What kinds of emotions did medical students and trainees experience in studies that measured their stress levels?
-
(SQ5): Can we infer the kinds of emotions medical trainees and students experienced in studies that measured their emotional intelligence?
Methods
Design
We designed and conducted our scoping review based on Arksey and O’Malley’s [31] methodological framework. We further consulted guidelines that elaborate on this framework [32], and a librarian with expertise in scoping reviews and health sciences education. Lastly, we referred to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [33]. See Appendix A for review protocol details, and Appendix B for the completed PRISMA-ScR checklist. A scoping review was chosen over a systematic review as we set out to identify the types of knowledge and research the current literature offers, and clarify key concepts—a systematic review would be better suited to assess the quality of current practices and can be a natural progression after a scoping review is conducted first [31, 34]. Our review of the literature indicates that there has yet to be a scoping review for this topic. Therefore, this knowledge synthesis work appropriately takes place before any systematic reviews.
Stage 1: Identifying the research questions
We formulated our primary question based on our primary research objective: to map out how recent SBE research approached studying emotions. We also considered which specific aspects our review should focus on [31], namely which additional constructs related to emotions our scope would cover. There are numerous constructs that are closely related to emotions, and while they can be differentiated from emotions, they have components and features that overlap with emotions [22, 35]. Therefore, we believed there may be a range of how these terms are used and applied in research settings, warranting their inclusion.
As per our methodological framework, we refined our research question through an iterative process to balance out the vastness of our scope and the relevancy that our identified articles would yield. This included consulting our librarian and deciding to focus on SBE (versus general medical education) to enhance the review’s focus and quality. We iterated through the guidelines from Arksey and O’Malley [31] and ensured our adjusted scope aligned with our research questions and search strategy.
Eligibility criteria for constructs related to emotions
In terms of eligibility criteria for specific constructs, we consulted a health sciences education librarian to explore related MeSH terms and the existing literature to focus on key constructs. This allowed us to exclude less relevant terms towards our research objective such as “social stress” or terms related to clinical disorders (e.g. mood disorders).
We also decided to focus on medical students and trainees, meaning we only included studies that featured medical students, interns, residents, and fellows. If a study featured other population groups (e.g. pre-med students, nurses, attending physicians), it was only included if it featured our target population. In addition, as we were interested in the context of SBE, we sought studies that had such environments. Hence, studies that asked for general life satisfaction or a survey that asked for emotions concerning day-to-day activities were excluded. When dealing with simulations, we were mindful of whether the simulation content would be related to medical knowledge, procedure, or non-technical skills. For example, simulations of war combat via a video game would not be included in our review as the simulated content is not something we would expect a medical trainee to experience (even if there were educational components featured in the simulation).
Through the above considerations and process of exploring what our scope would be, we were able to finalise the primary research question to focus on emotions, mood, stress, and EI of medical students and trainees in a SBE context. After trials identifying the number of articles we would yield, the team agreed our scope was broad enough to adhere to our research objective.
Stage 2: Identifying studies
We developed a search strategy with our librarian’s consultation. An iterative development process led to identifying a list of relevant keywords and MeSH terms (Table 1). Our search was carried out on Medline and EMBASE on June 22nd, 2020, exclusively looking at articles published from June 22nd, 2010 to June 22nd 2020. The initial yield of 29,329 articles decreased to 19,508 after deduplication.
We chose electronic databases and decided to complement them with hand-searched articles as outlined in Arksey & O’Malley’s guidelines [31]. We chose EMBASE and Medline based on our previous experience conducting scoping reviews related to research in the fields of medical education [36]. We selected Academic Medicine and Medical Education to hand-search articles because key articles were often featured there (e.g. Artino and Pekrun [2], Pottier and colleagues [37]). Hand searching is a supplementary technique in a scoping review and not intended to be comprehensive.
Stage 3: Study selection
For our database searches, there were three screening processes. Table 2 shows our inclusion and exclusion criteria for the title-abstract screening. Tables 3 and 4 show the criteria for the first and second full-text screening, respectively. While the first full-text screening included all medical education scenarios, the second full-text screening specifically filtered for simulation-based studies as per the iterated process outlined in Stage 1. Gaba’s definition of simulation was used to help screen the articles, where simulation was defined as “a technique—not a technology—to replace or amplify real experiences with guided experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner” [38] (p.i2). We referred to Gaba’s article that describes various dimensions of simulations to operationalise different criteria and types of simulators.
Each of the screening processes involved a team of reviewers (six for title-abstract screening, four for both full-text screenings), where each article was screened by a pair. A pilot preceded every screening process to ensure 75+% interrater reliability before proceeding [39]. Re-calibrations took place after 1/3 and 2/3 of the articles were screened.
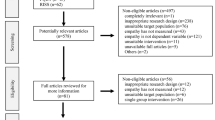
In addition to searching electronic databases, screening of hand-searched articles involved four reviewers. These articles (37) were screened for SBE content, similarly to our full-text screenings. After deduplication, two articles were added (please see Fig. 1 for the flow diagram).

Flow diagram of study selection process
Stage 4: Data charting and reporting
We finalised our data extraction sheet and strategy through consultation of multiple resources, our librarian, and pilot testing. Two reviewers were chosen in the end to extract the articles to ensure high interrater reliability. See Appendix C for details.
The final data extraction sheet included three categories of data: (1) information pertaining to the publication of the article (e.g. author, year); (2) information about the constructs of interest (e.g. whether the article focused on emotions or closely related constructs, what measurements were used); and (3) information on the simulation based on Gaba’s dimensions of simulation applications [38].
Stage 5: Collating, summarising, and reporting the results
We analysed our data descriptively; we summarised general characteristics of the papers through various charts to provide a broad overview of study characteristics. We report our summary to answer our research questions while providing context.
Results
The database search (139) combined with hand searching (2) yielded a total of 141 articles that met the inclusion criteria for review [194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296,297,298,299,300,301,302,303,304,305,306,307,308,309,310,311,312,313,314,315,316,317,318,319,320,321,322,323,324,325,326,327,328,329,330,331,332,333,334].
Study characteristics
Our results showed that research in emotions and related constructs have been increasing over the years, with most of the articles published in western countries (e.g. USA, UK). The vast majority (83.0%; 117 articles) were quantitative studies, while the bulk of the populations featured were medical students (56.7%; 80 articles) and residents (43.4%; 61 articles).
Stress was featured the most in the articles we identified (62.4%; 88 articles), followed by emotions (31.9%; 45 articles) and EI (24.1%; 34 articles). Only 1 article (0.7%) featured mood. Appendix D contains more details about study characteristics, including simulation characteristics.
Conceptualisation, measurement, and experiences of emotions
Our results indicated that most of the articles that focused on emotions did not formally define emotions: 35 (77.8%) of the 45 articles on emotions [40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73]. Seven (15.6%) articles [9, 74,75,76,77,78,79] defined a type or a discrete emotion (e.g. anxiety), 2 [80, 81] (4.4%) provided formal definitions, while 1 [82] defined both a formal definition for the term emotion, and separate definitions for discrete emotions (e.g. anxiety). For specific types of emotions, achievement emotions were the only type identified (as opposed to other types such as epistemic emotions—emotions that relate to knowledge and generation of knowledge [83]). Definitions of discrete emotions focused mainly on negatively valenced emotions such as anxiety and embarrassment. Amongst the articles that formally defined emotions, the circumplex model of emotion was referenced once and CVT was referenced four times.
Figure 2 shows that self-report measures (34 articles) were the most common method of collecting data on emotions. Besides custom self-made instruments [43, 44, 47, 50, 55, 56, 63, 69, 74, 84], the State-Trait Anxiety Inventory [40, 41, 60, 64,65,66,67, 79] (STAI; or a variation of it) was the most employed instrument (featured 8 times in emotion-focused articles). The next most common instruments were the Achievement Emotions Questionnaire [74, 77, 82] (AEQ), and a scale based on Barrett and Russel’s work on emotions [48, 53, 76] (i.e. the circumplex model [85]), each featured 3 times. See Appendix E for more details on the wide array of other instruments used in studies. Figure 3 shows that anxiety and fear (captured in 25 [9, 40, 41, 44, 46, 47, 50, 52, 55, 59, 60, 62, 64,65,66,67, 69, 73, 74, 77,78,79,80,81, 84] and 10 articles [44,45,46,47, 50, 52, 55, 57, 59, 64], respectively) were the most commonly measured emotions across the 45 articles that focused on emotions. Few positive emotions were captured in the studies, with excitement and enjoyment being the most frequently measured ones, but only being mentioned in four [50, 53, 56, 80] and five articles [53, 57, 71, 74, 77], respectively.

Number of articles by measurement types for emotions-focused articles

Number of appearances for discrete emotions
Conceptualisations and measurements of other constructs
Sixty-four of the 88 articles that focused on stress (72.4%) did not formally define stress with an explicit reference to a theoretical framework. Sixteen (18.2%) articles [37, 65, 66, 72, 79, 86,87,88,89,90,91,92,93,94,95,96] did, however, formally define what stress was, while 6 articles [59, 97,98,99,100,101] (6.8%) defined related terms to stress such as distress and stressors. Lastly, 2 articles [102, 103] (2.3%) defined both stress and related terms. For the 16 papers that formally defined stress, 8 [65, 66, 72, 79, 86, 92,93,94] relied on conceptualisation of stress stemming from a physiological-oriented (physiogenic) approach (e.g. Selhye’s General Adaptation Syndrome [104]), while 6 of the papers [37, 66, 90, 91, 95, 96] from a psychological-oriented (psychogenic) approach (i.e. Lazarus’ Transactional Model [105]). Overall, 3 papers [79, 87, 102] relied on definitions that drew from multiple approaches. It should be noted that 1 paper that explicitly defined stress did not provide any references (however took a physiological-oriented approach to defining stress) [88].
Figure 4 shows the measurements that stress articles employed. Studies using both self-reports and physiological measures were the most common (33 articles [37, 65,66,67, 72, 73, 87, 90, 91, 94, 96, 98, 101, 106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125]; 37.5%), followed by articles solely relying on either self-reports alone (30 articles [56, 60, 63, 64, 68, 70, 71, 84, 92, 95, 99, 102, 103, 126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142]; 34.1%) or physiological measures alone (19 articles [55, 62, 69, 79, 86, 88, 89, 93, 143,144,145,146,147,148,149,150,151,152,153]; 21.6%). There were two articles [100, 154] (2.3%) that used behavioural analysis in addition to self-reports and physiological measures. Heart rate or heart rate variability-related instruments were the most common (32 articles [65, 67, 69, 79, 86,87,88,89,90, 94, 96, 98, 100, 106,107,108,109,110,111, 113, 114, 117,118,119,120, 124, 143, 145, 148, 151, 152, 154]; 36.4%) for physiological measures. For self-report measures, the STAI was the most common (20 articles [37, 64, 67, 72, 90, 94, 98, 100, 103, 106, 108,109,110, 113, 114, 116, 118, 123, 124]; 22.7%).
Nine EI articles [7, 9, 98, 155,156,157,158,159,160] (26.5%) formally defined EI. Thirteen articles [57, 60, 97, 161,162,163,164,165,166,167,168,169,170] (38.2%) defined a construct directly related to, or a subordinate construct of EI (e.g. empathy, emotional skills). The most common measurement in these articles was the Jefferson Scale of Physician Empathy [171] (JSE; 6 articles [162, 166, 167, 169, 170, 172]; 17.6%), followed by The Trait Emotional Intelligence Questionnaire [173] (TEIQue; 4 articles [98, 158, 165, 174]; 11.8%) and The Mayer-Salovey-Caruso Emotional Intelligence Test [175] (MSCEIT; 3 articles [9, 159, 160]; 8.8%). The EI articles exclusively focused on EI did not infer emotions from their measures.

Number of articles by measurement types for stress-focused articles
The one article that focused on mood [176] utilised the visual analogue scales (VAS) from Bond and Lader [177] to assess “high” (positive) and “low” (negative) mood, and hence did not measure any discrete mood or emotions. It did not formally define mood or emotions.
Discussion
Primary question
Our primary research question was: “How are emotions and closely related constructs (i.e. stress, emotional intelligence, and mood) conceptualised in articles that focus on simulation environments, with medical students and trainees as the population of interest?” Based on our results, the short answer is that the SBE literature concerning emotions and related constructs tend to be light on theory, relying on previous research findings to orient their research. The literature had an affinity towards focusing on negative emotions (e.g. anxiety) and made connections between negative emotions and stress. Our review also further acknowledged the importance of these psychological constructs in education—hence acknowledging the desirability of EI in trainees (although no emotions are inferred from students’ EI levels). The more elaborate version of our answer was obtained through answering the secondary questions we proposed.
Secondary questions
Conceptualisation and measurements of emotions
SBE literature often discusses emotions informally, without explicit definitions or references. This was evident as most emotion-focused articles (35/45) did not provide a definition for emotions. We believe this may partially be due to the studies’ scopes and intentions, which are shaped by norms and trends in SBE. While a definition by itself is not a theory, it serves as an important part of a psychological theory. As these articles did not formally cite any theories either, we concluded that they lacked a theoretical-based conceptualisation of emotions. Based on our results, we believe that recent work in the SBE literature resembles the early emotion research activities in the realm of traditional education research in that it focuses on specific discrete negative-activating emotions and relies on self-report measures [178].
Many studies concentrated on negative emotions. For example, Kim’s study [74] looked at how medical students’ anxiety and boredom in class were associated to levels of anxiety in Objective Structured Clinical Examinations (OSCEs). Fraser and colleagues’ [48] focused on negative emotions elicited from simulated patient death. It was therefore not surprising that measurements towards emotions largely included self-reports (34 articles of 45 that focused on emotions) that focused on negative emotions such as anxiety (8 articles using STAI [179] to measure this) and other negative emotions such as fear (measured via the Fear of Negative Evaluation Scale [180]) and shame (measured via Experimental Shame Scale [181]). We noted that studies that did not rely on self-reports also followed the trend of identifying negative emotions in SBE [45, 52, 58, 59].
The emphasis on negative emotions is understandable. This is especially so when we consider how medical trainees face training scenarios that are meant to elicit negative emotions, due to the nature of the topic the scenarios deal with, and the pressure for achieving high performance. For example, articles such as Groot’s article [58] featured medical students taking on residency-level simulations that featured emergency room acute care cases (e.g. anaphylaxis, acute myocardial infarction). These simulations placed the students in an emotionally charged situation where negative emotions such as anxiety (i.e. stress) would be elicited, in part, due to the advanced and challenging nature of the medical issues they needed to manage. Students strived to perform well but ultimately reported stress and disappointment in themselves failing to meet their own expectations. Our other reviewed articles follow this example in terms of dealing with emotionally charged topics and scenarios likely to elicit negative emotions. Bloomfield and others’ article [51] featured students communicating with dying patients and their family members. Bauer and others’ article [79] had residents for their first time be given a high-fidelity mannikin in a scenario where the simulated patient was intubated during an intra-hospital transportation, but had oxygen desaturation, and was under mechanical ventilation. Summing up these examples, we report that the typical SBE scenario in our review featured stress-inducing, negative emotion eliciting experiences—explaining why the literature perhaps tends to focus on negative emotions.
Our results showed that four articles referenced the CVT to define emotions, with three using related measures (i.e. Achievement Emotion Questionnaire; AEQ [182]). While focusing on specific emotions such as anxiety has merit, extending the acknowledgement of emotions’ role beyond a specific discrete emotion such as anxiety, or a type of emotion would benefit the SBE literature by providing a more comprehensive picture of the potential role other emotions play. Broad examples of this include studying emotions during simulation versus after simulation (debriefing); effects of positive-activating emotions (enjoyment) versus positive-deactivating emotions (relief) and so on. We make a positive note that CVT—one of the most suitable frameworks for being applied to SBE research—was cited by several of the few articles that did rely on theory. This suggests that SBE researchers are on the right track in conceptualising emotions in academic contexts.
While we highlighted the need to look beyond negative emotions in SBE research, studies such as Butteris and colleague’s [50] illuminates the rationale for focusing on negative emotions. Unlike the rule of thumb that negative emotions are generally undesirable in education, the study’s facilitators’ consensus seemed to be that completing a simulation scenario involving a neonatal death or caring for a simulated HIV-positive toddler requires trainees to experience negative emotions so that they are motivated to reflect on their competency and preparedness [50]. We note that the study emphasised post-simulation debriefings to help trainees adaptively digest these negative emotions. Though the non-profession-specific educational (e.g. high school, higher education) emotion literature acknowledges that emotions such as anger may be beneficial in specific contexts [23, 183], the contexts featured are difficult to compare to what medical students and trainees experience.
Conceptualisations and measurements of related constructs to emotions
Like emotions, most articles focusing on stress (64/88) did not offer formal definitions. Instead, they referenced previous work and expert opinions to establish research directions. Further, papers featuring stress tended to simply conceptualise stress from a biological, physiological approach. The assumption may be that readers of medical education journals do not expect formal explanations of stress, as they are familiar with the biological components of stress responses (e.g. activation of the hypothalamic-pituitary-adrenal and the sympathetic-adrenal-medullary axes). Hence, many authors simply mention this physiological side of stress in lieu of citing a theoretical framework. We note that authors who measured constructs such as anxiety as an indicator of stress were measuring a construct that is different from stress, albeit related [184].
Measurements of stress-related articles were similar to emotion-related articles in that they often employed instruments such as the STAI [179]. In other words, articles that focused on stress, while not studying a wide variety of emotions, still often examined negative-activating emotions such as anxiety. This is supported by our findings that of the 18 articles that examined both emotions and stress, 16 featured STAI for measuring anxiety. What was different from emotion-related articles, however, was the frequent reliance on multiple channels of data: 36.4% of stress articles included both self-report and physiological measures to infer stress as opposed to just 2.1% of the emotion articles. We believe this is a symptom of the SBE literature not embracing formal definitions of emotions. Formal definitions of emotions will tend to agree that emotions are multi-componential psychological responses which include a combination of affective, cognitive, physiological, motivational, and expressive processes [22]. Therefore, measuring emotions should go beyond self-report measures and should also measure the physiological (e.g. skin conductance, heart rates) and expressive (e.g. facial expressions, speech) aspects of emotions.
The conceptualisation of EI was more formal relative to emotions and stress (26.5% of the articles with formal definitions versus 4.4% and 18.2% of the articles with formal definitions for emotions and stress respectively). Articles often cited ideas related to Goleman [185] and Mayer [186] (theories claiming EI as a type of intelligence), in addition to citing Petrides [187] in reference to the theory of trait emotional intelligence. If we consider that 13 articles that did not define EI still defined the construct they were measuring (e.g. empathy), 64.7% of EI articles featured formal definitions. This finding seems to signal a trend in SBE where constructs such as emotions are just emerging and therefore lack theoretical integration, while emotional intelligence may be a more established topic with a more matured approach.
We lastly note that we only identified one article that focused on mood. We report that the SBE literature does not seem to interchangeably use the term mood and emotions.
Emotions of medical students and trainees
We report that anxiety and fear were the most captured emotions in our reviewed articles. According to CVT’s classification, both are negative-activating emotions, indicating their similarities. The captured emotions reflected how the chosen instruments aligned with the studies’ objectives of investigating negative-activating emotions. In other words, if the study sought to investigate anxiety in medical students, the emotional profile reported will mainly be anxiety. Overall, as discussed earlier, we report that while students and trainees do experience positive emotions (e.g. excitement, enjoyment) during certain simulation scenarios, the literature in our review more often captured negative emotions (e.g. anxiety, fear, frustration, guilt) due to the intensity of the scenarios (e.g. simulated patient death [48]), and the high expectations set for learners. According to the CVT, high expectations means high appraisal of value (i.e. learners perceive their performance in a simulation to be important), which lead to emotions with high levels of intensity [188]. This is especially the case when one’s control over a situation is uncertain or low (i.e. the difficulty of the simulation is high, or there are uncontrollable factors in a simulation) [188].
Inferring emotions from stress and emotional intelligence
Studies that focused on both stress and emotions (predominantly anxiety) tended to infer anxiety from stress levels of their participants. It is also interesting to note that two of the studies [58, 61] that focused on emotion reported “stress” as a type of emotion their participants experienced. Overall, SBE articles tended to acknowledge that anxiety is an expressive component of stress. However, we think caution is warranted in using the term stress, emotions, and anxiety interchangeably. Anxiety is just one of many different stress responses [189], and hence sole reliance on measurement of anxiety may be limited as opposed to relying on multiple measures that also take into account physiological measures or behavioural coding.
Further, when examining what other discrete emotions educators could intend on introducing and measuring in SBE, considering that the CVT illustrates how interchanging stress is with the term emotion, this interchangeability may potentially lead to a narrow capture of emotions. While anxiety is a negative-activating emotion like anger and shame, they are not identical and have different implications for learning [2, 190]. Therefore, measuring stress may capture whether one is feeling anxious or not, but not adequately capture anger or shame. For other emotions that are still negative but are deactivating (e.g. boredom, hopelessness, sadness, disappointment), this issue becomes much more prominent. Finally, measuring stress would not capture positive emotions, missing emotions such as enjoyment and curiosity.
While McNaughton’s discourse analysis revealed that educators can view emotions as a skillset, we believe, from an educational psychology perspective, that there is a distinction between having the ability to understand one’s own and others’ emotions (i.e. EI) [29, 186] and the actual experience of feeling specific emotions. Aligned with this, our results showed that the researchers that focused on EI did not infer emotions from EI measurements. The closest inference would be Dohms and others [191] reporting that students with higher empathy will have better emotion regulation, leading to a calmer emotional profile in stressful situations relative to their peers. We therefore presume that SBE researchers do not confuse experiencing specific discrete emotions with levels of emotional intelligence.
Specific calls to action based on our research partially echoes Leblanc and Posner’s review [10]: simulation designers and researchers should ask what emotions they are deliberately or potentially introducing to the participants and consider the impact they may have. However, in thinking and conceptualising this, we would like to extend their call by specifying how to be deliberate and consider integrating a theoretical framework that can formally define what emotions are.
Contextual factors and future directions
When interpreting our study, certain contextual factors matter. Our results show that SBE literature is prominent in the western world, with USA, UK, Germany, Canada, and France comprising 66.6% of the articles. The role of culture may influence studies [192, 193] and increasing cultural diversity in SBE emotions research is therefore an important future direction. Specifically examining SBEs offered in institutions in various nations is one example of this direction. Further, our results indicate that certain types of simulation structures and contexts were underrepresented. For example, only 6.4% of our studies featured interprofessional teams, while certain simulators such as augmented reality or virtual reality simulators were featured much less (3.5%). Focusing the investigation of emotions in such specific SBE contexts could be valuable future directions.
We note limitations of our scoping review process, including our limited selection of electronic databases, not drawing on more than two journals for hand searching, especially from journals that are SBE-focused. Other limitations include our review focusing on just empirical articles, lacking additional screenings of identified articles’ reference lists, and the lack of consulting content experts. In addition, as our study inclusion criteria was quite broad (e.g. including individual-based, team-based simulations, and a wide range of simulators), our findings may have different applications when focused on specific types of SBE. While our results are applicable to the general landscape of the SBE literature, extrapolating our findings to specific subfields of SBE may warrant care.
Our study had some notable strengths as well. Other than the expected standards of following a scoping review framework and being consulted on our search decisions by an expert librarian, we have also conducted screenings, data extraction, and analysis via evidence-based practices. From identifying the affect-related constructs to be studied, to how we conceptualised simulations and their different features, decisions were based on prominent ideas to ensure consistent and accurate intake and analysis of data. Our appendix and body of the manuscript also offer full transparency in all the steps we have taken based on Arksey and O’Malley’s framework.
Future studies could focus on exploring more databases with additional consultation from content experts. Further, our study only extends to the middle of 2020. At the time we wrote this article, the COVID-19 pandemic had left its impact on healthcare education worldwide; it would be interesting to see whether there are any shifts in directions and activities within the SBE literature. Other future directions include this review being a basis for a systematic review on how theoretical frameworks guide emotion-focused SBE research and the interpretation of the results.
Conclusion
We presented a scoping review that aimed to describe the current state of SBE literature pertaining to the conceptualisation of emotions and related constructs: stress, emotional intelligence, and mood. Our results revealed that authors of SBE tend to omit including a theoretical framework for conceptualising emotion-related constructs in their study. We also highlight another tendency amongst SBE studies: capturing negative emotions such as anxiety, where studies that examine stress also often evaluate the levels of anxiety of learners. This tendency of capturing negative emotions reveals that, at first glance, medical trainees and students are stricken with anxiety, fear, and guilt. However, we note that this finding partially stems from studies setting out to measure negative emotions that are also identified as important in medical education. Unlike in more traditional fields of education (i.e. Kindergarden-12, Higher Ed), negative emotions seem to have a more profound and authentic role in facilitating learning in SBE. For example, Butteris and colleagues identified how negative emotions such as frustration and helplessness facilitated motivation for preparedness [50]. Future research that embraces theoretical frameworks such as CVT should equip researchers with the tools they need to critically interpret the impact of such emotions in SBE. In addition, synthesis work focusing on specific types of SBE environments in relation to emotion-related constructs (e.g. interprofessional SBE using virtual reality simulators), and the role of emotion regulation [21] supporting instructional design can serve as next steps. This line of work can illuminate the roles of emotions in SBE and how to best support students’ experiences of these influential psychological states that are associated with learning, performance, and psychological well-being.
Abbreviations
- SBE:
-
Simulation-based education
- EI:
-
Emotional intelligence
- CVT:
-
Control Value Theory of Achievement Emotions
References
Artino AR, Holmboe ES, Durning SJ. Can achievement emotions be used to better understand motivation, learning, and performance in medical education? Med Teach. 2012;34(3):240–4. https://doi.org/10.3109/0142159X.2012.643265.
Artino AR, Pekrun R. Using control-value theory to understand achievement emotions in medical education. Acad Med. 2014;89(12):1696. https://doi.org/10.1097/ACM.0000000000000536.
LeBlanc VR, McConnell MM, Monteiro SD. Predictable chaos: a review of the effects of emotions on attention, memory and decision making. Adv Health Sci Educ. 2015;20(1):265–82. https://doi.org/10.1007/s10459-014-9516-6.
Kozlowski D, Hutchinson M, Hurley J, Rowley J, Sutherland J. The role of emotion in clinical decision making: an integrative literature review. BMC Med Educ. 2017;17(1):255. https://doi.org/10.1186/s12909-017-1089-7.
Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, Sevdalis N. Emotional intelligence in medicine: a systematic review through the context of the ACGME competencies: emotional intelligence in medicine. Med Educ. 2010;44(8):749–64. https://doi.org/10.1111/j.1365-2923.2010.03709.x.
Shahid R, Stirling J, Adams W. Promoting wellness and stress management in residents through emotional intelligence training. AMEP. 2018;9:681–6. https://doi.org/10.2147/AMEP.S175299.
Cerrone SA, Adelman P, Akbar S, Yacht AC, Fornari A. Using Objective Structured Teaching Encounters (OSTEs) to prepare chief residents to be emotionally intelligent leaders. Med Educ Online. 2017;22(1):1320186. https://doi.org/10.1080/10872981.2017.1320186.
Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction: emotional intelligence and doctor and patient satisfaction. Med Educ. 2011;45(8):835–42. https://doi.org/10.1111/j.1365-2923.2011.03985.x.
Cherry MG, Fletcher I, O’Sullivan H. Validating relationships among attachment, emotional intelligence and clinical communication. Med Educ. 2014;48(10):988–97. https://doi.org/10.1111/medu.12526.
LeBlanc VR, Posner GD. Emotions in simulation-based education: friends or foes of learning? Adv Simul. 2022;7(1):3. https://doi.org/10.1186/s41077-021-00198-6.
McNaughton N. Discourse(s) of emotion within medical education: the ever-present absence: Discourses of emotion in medical education. Med Educ. 2013;47(1):71–9. https://doi.org/10.1111/j.1365-2923.2012.04329.x.
Harley JM, Jarrell A, Lajoie SP. Emotion regulation tendencies, achievement emotions, and physiological arousal in a medical diagnostic reasoning simulation. Instruct Sci. 2019;47(2):151–80. https://doi.org/10.1007/s11251-018-09480-z.
Kazemitabar M, Lajoie SP, Doleck T. Analysis of emotion regulation using posture, voice, and attention: a qualitative case study. Comput Educ Open. 2021;2:100030. https://doi.org/10.1016/j.caeo.2021.100030.
Heyhoe J, Birks Y, Harrison R, O’Hara JK, Cracknell A, Lawton R. The role of emotion in patient safety: are we brave enough to scratch beneath the surface? J R Soc Med. 2016;109(2):52–8. https://doi.org/10.1177/0141076815620614.
Ali S, Thomson D, Graham TAD, Rickard S, Stang A. High stakes and high emotions: providing safe care in Canadian emergency departments. OAEM. 2017;9:23–6. https://doi.org/10.2147/OAEM.S122646.
Coppin G, Sander D. Theoretical approaches to emotion and its measurement. In: Emotion Measurement. Elsevier; 2016:3-30. https://doi.org/10.1016/B978-0-08-100508-8.00001-1.
Cleary TJ, Durning SJ, Gruppen LD, Hemmer PA, Artino AR. Self-regulated learning in medical education. In: Walsh K, ed. Oxford Textbook of Medical Education. Oxford University Press; 2013:465-477. https://doi.org/10.1093/med/9780199652679.003.0040.
Ajjawi R, McIlhenny C. Researching in surgical education: an orientation. In: Nestel D, Dalrymple K, Paige JT, Aggarwal R, eds. Advancing Surgical Education. Vol 17. Innovation and Change in Professional Education. Springer Singapore; 2019:341-352. https://doi.org/10.1007/978-981-13-3128-2_30.
Pekrun R. The control-value theory of achievement emotions: assumptions, corollaries, and implications for educational research and practice. Educ Psychol Rev. 2006;18(4):315–41. https://doi.org/10.1007/s10648-006-9029-9.
Eliot JAR, Hirumi A. Emotion theory in education research practice: an interdisciplinary critical literature review. Educ Tech Res Dev. 2019;67(5):1065–84. https://doi.org/10.1007/s11423-018-09642-3.
Harley JM, Pekrun R, Taxer JL, Gross JJ. Emotion regulation in achievement situations: an integrated model. Educ Psychol. 2019;54(2):106–26. https://doi.org/10.1080/00461520.2019.1587297.
Jarrell A, Lajoie SP. The regulation of achievements emotions: implications for research and practice. Can Psychol/Psychologie canadienne. 2017;58(3):276–87. https://doi.org/10.1037/cap0000119.
Loderer K, Pekrun R, Lester JC. Beyond cold technology: a systematic review and meta-analysis on emotions in technology-based learning environments. Learn Instruct. 2018:S095947521730436X. https://doi.org/10.1016/j.learninstruc.2018.08.002.
Duffy MC, Lajoie SP, Pekrun R, Lachapelle K. Emotions in medical education: examining the validity of the Medical Emotion Scale (MES) across authentic medical learning environments. Learn Instruct. 2020;70:101150. https://doi.org/10.1016/j.learninstruc.2018.07.001.
Gross JJ, Thompson RA. Emotion regulation: conceptual foundations. In: Handbook of Emotion Regulation. Guilford Publications; 2007:22.
Fink G. Stress, definitions, mechanisms, and effects outlined. In: Stress: Concepts, Cognition, Emotion, and Behavior. Elsevier; 2016:3-11. https://doi.org/10.1016/B978-0-12-800951-2.00001-7.
Koolhaas JM, Bartolomucci A, Buwalda B, et al. Stress revisited: a critical evaluation of the stress concept. Neurosci Biobehav Rev. 2011;35(5):1291–301. https://doi.org/10.1016/j.neubiorev.2011.02.003.
Dawda D, Hart SD. Assessing emotional intelligence: reliability and validity of the Bar-On Emotional Quotient Inventory (EQ-i) in university students. Personal Individual Differ. 2000;28(4):797–812. https://doi.org/10.1016/S0191-8869(99)00139-7.
Sharp G, Bourke L, Rickard MJFX. Review of emotional intelligence in health care: an introduction to emotional intelligence for surgeons. ANZ J Surg. 2020;90(4):433–40. https://doi.org/10.1111/ans.15671.
Mayer JD, Caruso DR, Salovey P. The ability model of emotional intelligence: principles and updates. Emotion Rev. 2016;8(4):290–300. https://doi.org/10.1177/1754073916639667.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. https://doi.org/10.1080/1364557032000119616.
Thomas A, Lubarsky S, Durning SJ, Young ME. Knowledge syntheses in medical education: demystifying scoping reviews. Acad Med. 2017;92(2):161–6. https://doi.org/10.1097/ACM.0000000000001452.
Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/M18-0850.
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. https://doi.org/10.1186/s12874-018-0611-x.
Shuman V, Scherer KR. Concepts and structures of emotions. In: International Handbook of Emotions in Education. Routledge; 2014. https://doi.org/10.4324/9780203148211.ch2.
Maurice-Ventouris M, Muller Moran HR, Alharbi M, Ahn BT, Harley JM, Lachapelle KJ. The study of visuospatial abilities in trainees: a scoping review and proposed model. Surg Open Sci. 2021;5:25–33. https://doi.org/10.1016/j.sopen.2021.05.001.
Pottier P, Hardouin JB, Dejoie T, et al. Stress responses in medical students in ambulatory and in-hospital patient consultations: stress responses in medical students. Med Educ. 2011;45(7):678–87. https://doi.org/10.1111/j.1365-2923.2011.03935.x.
Gaba DM. The future vision of simulation in health care. Qual Saf Health Care. 2004;13(suppl_1):i2–10. https://doi.org/10.1136/qshc.2004.009878.
Peters M, Godfrey C, McInerney P, Munn Z, Trico A, Khalil H. Chapter 11: scoping reviews. In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI; 2020. https://doi.org/10.46658/JBIMES-20-12.
Yutani M, Takahashi M, Miyaoka H. Changes in communication skills of clinical residents through psychiatric training: communication skills training. Psychiatry Clin Neurosci. 2011;65(6):561–6. https://doi.org/10.1111/j.1440-1819.2011.02265.x.
Romo-Barrientos C, Criado-Álvarez JJ, González-González J, et al. Anxiety levels among health sciences students during their first visit to the dissection room. BMC Med Educ. 2020;20(1):109. https://doi.org/10.1186/s12909-020-02027-2.
Zhou Y, Collinson A, Laidlaw A, Humphris G. How do medical students respond to emotional cues and concerns expressed by simulated patients during OSCE consultations? – a multilevel study. PLoS One. 2013;8(10):e79166. https://doi.org/10.1371/journal.pone.0079166. (Houser D, ed).
Beckers SK, Biermann H, Sopka S, et al. Influence of pre-course assessment using an emotionally activating stimulus with feedback: a pilot study in teaching Basic Life Support. Resuscitation. 2012;83(2):219–26. https://doi.org/10.1016/j.resuscitation.2011.08.024.
Russa AD, Mligiliche NuruL. Inspiring Tanzanian medical students into the profession: appraisal of cadaveric dissection stress and coping strategies. Italian J Anat Embryo. 2015;19:268–76. https://doi.org/10.13128/IJAE-15560. (Pages, 276 kB).
Romotzky V, Galushko M, Düsterdiek A, et al. “It’s not that easy”—medical students’ fears and barriers in end-of-life communication. J Canc Educ. 2015;30(2):333–9. https://doi.org/10.1007/s13187-014-0712-0.
Chang HJ, Kim HJ, Rhyu IJ, Lee YM, Uhm CS. Emotional experiences of medical students during cadaver dissection and the role of memorial ceremonies: a qualitative study. BMC Med Educ. 2018;18(1):255. https://doi.org/10.1186/s12909-018-1358-0.
Bernhardt V, Rothkötter HJ, Kasten E. Psychische Belastungen durch die Dissektion am Leichnam im anatomischen Präparierkurs bei Erstsemestern des Studienfachs Medizin. GMS Zeitschrift für Medizinische Ausbildung. 2012; 29(1):Doc12; https://doi.org/10.3205/ZMA000782. ISSN 1860-3572.
Fraser K, Huffman J, Ma I, et al. The emotional and cognitive impact of unexpected simulated patient death. Chest. 2014;145(5):958–63. https://doi.org/10.1378/chest.13-0987.
Lefroy J, Brosnan C, Creavin S. Some like it hot: medical student views on choosing the emotional level of a simulation: student views on emotion in simulation. Med Educ. 2011;45(4):354–61. https://doi.org/10.1111/j.1365-2923.2010.03881.x.
Butteris SM, Gladding SP, Eppich W, Hagen SA, Pitt MB. Simulation Use for Global Away Rotations (SUGAR): preparing residents for emotional challenges abroad—a multicenter study. Acad Pediatr. 2014;14(5):533–41. https://doi.org/10.1016/j.acap.2014.05.004.
Bloomfield JG, O’Neill B, Gillett K. Enhancing student communication during end-of-life care: a pilot study. Pall Supp Care. 2015;13(6):1651–61. https://doi.org/10.1017/S147895151500022X.
Kerins J, Smith SE, Phillips EC, Clarke B, Hamilton AL, Tallentire VR. Exploring transformative learning when developing medical students’ non-technical skills. Med Educ. 2020;54(3):264–74. https://doi.org/10.1111/medu.14062.
Fraser K, Ma I, Teteris E, Baxter H, Wright B, McLaughlin K. Emotion, cognitive load and learning outcomes during simulation training: emotion and cognitive load during simulation. Med Educ. 2012;46(11):1055–62. https://doi.org/10.1111/j.1365-2923.2012.04355.x.
Noll C, von Jan U, Raap U, Albrecht UV. Mobile augmented reality as a feature for self-oriented, blended learning in medicine: randomized controlled trial. JMIR Mhealth Uhealth. 2017;5(9):e139. https://doi.org/10.2196/mhealth.7943.
Robb A, Kopper R, Ambani R, et al. Leveraging virtual humans to effectively prepare learners for stressful interpersonal experiences. IEEE Trans Visual Comput Graphics. 2013;19(4):662–70. https://doi.org/10.1109/TVCG.2013.35.
Rajeh NA, Badroun LE, Alqarni AK, et al. Cadaver dissection: a positive experience among Saudi female medical students. J Taibah Univ Med Sci. 2017;12(3):268–72. https://doi.org/10.1016/j.jtumed.2016.07.005.
Dupuy L, Micoulaud-Franchi JA, Cassoudesalle H, et al. Evaluation of a virtual agent to train medical students conducting psychiatric interviews for diagnosing major depressive disorders. J Affect Disord. 2020;263:1–8. https://doi.org/10.1016/j.jad.2019.11.117.
Groot F, Jonker G, Rinia M, ten Cate O, Hoff RG. Simulation at the frontier of the zone of proximal development: a test in acute care for inexperienced learners. Acad Med. 2020;95(7):1098–105. https://doi.org/10.1097/ACM.0000000000003265.
Lewis G, McCullough M, Maxwell AP, Gormley GJ. Ethical reasoning through simulation: a phenomenological analysis of student experience. Adv Simul. 2016;1(1):26. https://doi.org/10.1186/s41077-016-0027-9.
Meunier J, Libert Y, Merckaert I, et al. How much is residents’ distress detection performance during a clinical round related to their characteristics? Patient Educ Counsel. 2011;85(2):180–7. https://doi.org/10.1016/j.pec.2010.09.022.
Torres A, Horodeńska M, Witkowski G, Torres K. Hybrid simulation of pediatric gynecologic examination: a mix-methods study of learners’ attitudes and factors affecting learning. BMC Med Educ. 2020;20(1):164. https://doi.org/10.1186/s12909-020-02076-7.
O’Rourke SR, Branford KR, Brooks TL, Ives LT, Nagendran A, Compton SN. The emotional and behavioral impact of delivering bad news to virtual versus real standardized patients: a pilot study. Teach Learn Med. 2020;32(2):139–49. https://doi.org/10.1080/10401334.2019.1652180.
Bob MH, Popescu CA, Armean MS, Suciu SM, Buzoianu AD. Ethical views, attitudes and reactions of Romanian medical students to the dissecting room. Rev Med Chir Soc Med Nat Iasi. 2014;118(4):1078–85.
Leboulanger N. First cadaver dissection: stress, preparation, and emotional experience. Eur Ann Otorhinolaryngol Head Neck Dis. 2011;128(4):175–83. https://doi.org/10.1016/j.anorl.2011.01.007.
Hulsman RL, Pranger S, Koot S, Fabriek M, Karemaker JM, Smets EMA. How stressful is doctor–patient communication? Physiological and psychological stress of medical students in simulated history taking and bad-news consultations. Int J Psychophysiol. 2010;77(1):26–34. https://doi.org/10.1016/j.ijpsycho.2010.04.001.
Piquette D, Tarshis J, Sinuff T, Fowler RA, Pinto R, Leblanc VR. Impact of acute stress on resident performance during simulated resuscitation episodes: a prospective randomized cross-over study. Teach Learn Med. 2014;26(1):9–16. https://doi.org/10.1080/10401334.2014.859932.
Harvey A, Bandiera G, Nathens AB, LeBlanc VR. Impact of stress on resident performance in simulated trauma scenarios. J Trauma Acute Care Surg. 2012;72(2):497–503. https://doi.org/10.1097/TA.0b013e31821f84be.
McNeer RR, Bennett CL, Dudaryk R. Intraoperative noise increases perceived task load and fatigue in anesthesiology residents: a simulation-based study. Anesth Analgesia. 2016;122(2):512–25. https://doi.org/10.1213/ANE.0000000000001067.
Clarke S, Horeczko T, Cotton D, Bair A. Heart rate, anxiety and performance of residents during a simulated critical clinical encounter: a pilot study. BMC Med Educ. 2014;14(1):153. https://doi.org/10.1186/1472-6920-14-153.
Hurst SA, Baroffio A, Ummel M, Layat Burn C. Helping medical students to acquire a deeper understanding of truth-telling. Med Educ Online. 2015;20(1):28133. https://doi.org/10.3402/meo.v20.28133.
Hagemann V, Herbstreit F, Kehren C, et al. Does teaching non-technical skills to medical students improve those skills and simulated patient outcome? Int J Med Educ. 2017;8:101–13. https://doi.org/10.5116/ijme.58c1.9f0d.
Crewther BT, Shetty K, Jarchi D, et al. Skill acquisition and stress adaptations following laparoscopic surgery training and detraining in novice surgeons. Surg Endosc. 2016;30(7):2961–8. https://doi.org/10.1007/s00464-015-4584-0.
Cook CJ, Crewther BT. The impact of a competitive learning environment on hormonal and emotional stress responses and skill acquisition and expression in a medical student domain. Physiol Behav. 2019;199:252–7. https://doi.org/10.1016/j.physbeh.2018.11.027.
Kim KJ. Factors associated with medical student test anxiety in objective structured clinical examinations: a preliminary study. Int J Med Educ. 2016;7:424–7. https://doi.org/10.5116/ijme.5845.caec.
Hautz WE, Schröder T, Dannenberg KA, et al. Shame in medical education: a randomized study of the acquisition of intimate examination skills and its effect on subsequent performance. Teach Learn Med. 2017;29(2):196–206. https://doi.org/10.1080/10401334.2016.1254636.
Fraser K, McLaughlin K. Temporal pattern of emotions and cognitive load during simulation training and debriefing. Med Teach. 2019;41(2):184–9. https://doi.org/10.1080/0142159X.2018.1459531.
Behrens CC, Dolmans DH, Gormley GJ, Driessen EW. Exploring undergraduate students achievement emotions during ward round simulation: a mixed-method study. BMC Med Educ. 2019;19(1):316. https://doi.org/10.1186/s12909-019-1753-1.
Carenzo L, Braithwaite EC, Carfagna F, et al. Cognitive appraisals and team performance under stress: a simulation study. Med Educ. 2020;54(3):254–63. https://doi.org/10.1111/medu.14050.
Bauer C, Rimmelé T, Duclos A, et al. Anxiety and stress among anaesthesiology and critical care residents during high-fidelity simulation sessions. Anaesth Crit Care Pain Med. 2016;35(6):407–16. https://doi.org/10.1016/j.accpm.2016.01.004.
Rogers T, Andler C, O’brien B, van Schaik S. Self-reported emotions in simulation-based learning: active participants vs observers. Sim Healthcare. 2019;14(3):140–5. https://doi.org/10.1097/SIH.0000000000000354.
Toivonen AK, Lindblom-Ylänne S, Louhiala P, Pyörälä E. Medical students’ reflections on emotions concerning breaking bad news. Patient Educ Counsel. 2017;100(10):1903–9. https://doi.org/10.1016/j.pec.2017.05.036.
Naismith LM, Lajoie SP. Motivation and emotion predict medical students’ attention to computer-based feedback. Adv in Health Sci Educ. 2018;23(3):465–85. https://doi.org/10.1007/s10459-017-9806-x.
Vogl E, Pekrun R, Loderer K. Epistemic emotions and metacognitive feelings. In: Moraitou D, Metallidou P, eds. Trends and Prospects in Metacognition Research across the Life Span. Springer International Publishing; 2021:41-58. https://doi.org/10.1007/978-3-030-51673-4_3 .
Daly SC, Wilson NA, Rinewalt DE, Bines SD, Luu MB, Myers JA. A subjective assessment of medical student perceptions on animal models in medical education. J Surg Educ. 2014;71(1):61–4. https://doi.org/10.1016/j.jsurg.2013.06.017.
Feldman Barrett L, Russell JA. Independence and bipolarity in the structure of current affect. J Personal Soc Psychol. 1998;74(4):967–84. https://doi.org/10.1037/0022-3514.74.4.967.
Hurley AM, Kennedy PJ, O’Connor L, et al. SOS save our surgeons: Stress levels reduced by robotic surgery. Gynecol Surg. 2015;12(3):197–206. https://doi.org/10.1007/s10397-015-0891-7.
Tramèr L, Becker C, Schumacher C, et al. Association of self-esteem, personality, stress and gender with performance of a resuscitation team: a simulation-based study. PLoS One. 2020;15(5):e0233155. https://doi.org/10.1371/journal.pone.0233155. (Roma PG, ed).
Tramèr L, Becker C, Hochstrasser S, Marsch S, Hunziker S. Association of electrocardiogram alterations of rescuers and performance during a simulated cardiac arrest: a prospective simulation study. PLoS One. 2018;13(6):e0198661. https://doi.org/10.1371/journal.pone.0198661. (Lazzeri C, ed).
Bensouda B, Mandel R, Mejri A, Lachapelle J, St-Hilaire M, Ali N. Effect of an audience on trainee stress and performance during simulated neonatal intubation: a randomized crossover trial. BMC Med Educ. 2018;18(1):230. https://doi.org/10.1186/s12909-018-1338-4.
Bajunaid K, Mullah MAS, Winkler-Schwartz A, et al. Impact of acute stress on psychomotor bimanual performance during a simulated tumor resection task. JNS. 2017;126(1):71–80. https://doi.org/10.3171/2015.5.JNS15558.
Pottier P, Dejoie T, Hardouin JB, et al. Effect of stress on clinical reasoning during simulated ambulatory consultations. Med Teach. 2013;35(6):472–80. https://doi.org/10.3109/0142159X.2013.774336.
Oriot D, Trigolet M, Kessler DO, Auerbach MA, Ghazali DA. Stress: a factor explaining the gap between simulated and clinical procedure success. Pediatr Emer Care. 2021;37(12):e1192–6. https://doi.org/10.1097/PEC.0000000000001962.
Phitayakorn R, Minehart RD, Pian-Smith MCM, Hemingway MW, Petrusa ER. Practicality of using galvanic skin response to measure intraoperative physiologic autonomic activation in operating room team members. Surgery. 2015;158(5):1415–20. https://doi.org/10.1016/j.surg.2015.04.009.
Baker BG, Bhalla A, Doleman B, et al. Simulation fails to replicate stress in trainees performing a technical procedure in the clinical environment. Med Teach. 2017;39(1):53–7. https://doi.org/10.1080/0142159X.2016.1230188.
Chia TI, Oyeniran OI, Ajagbe AO, Onigbinde OA, Oraebosi MI. The symptoms and stress experienced by medical students in anatomy dissection halls. J Taibah Univ Med Sci. 2020;15(1):8–13. https://doi.org/10.1016/j.jtumed.2020.01.001.
Hunziker S, Semmer NK, Tschan F, Schuetz P, Mueller B, Marsch S. Dynamics and association of different acute stress markers with performance during a simulated resuscitation. Resuscitation. 2012;83(5):572–8. https://doi.org/10.1016/j.resuscitation.2011.11.013.
Harendza S, Soll H, Prediger S, Kadmon M, Berberat PO, Oubaid V. Assessing core competences of medical students with a test for flight school applicants. BMC Med Educ. 2019;19(1):9. https://doi.org/10.1186/s12909-018-1438-1.
Arora S, Russ S, Petrides KV, et al. Emotional intelligence and stress in medical students performing surgical tasks. Acad Med. 2011;86(10):1311–7. https://doi.org/10.1097/ACM.0b013e31822bd7aa.
Böckers A, Baader C, Fassnacht UK, Öchsner W, Böckers TM. Reduction of mental distress in the dissection course by introducing the body donor experience through anatomical demonstrations of organ systems. Anat Sci Ed. 2012;5(6):321–9. https://doi.org/10.1002/ase.1292.
Andreatta PB, Hillard M, Krain LP. The impact of stress factors in simulation-based laparoscopic training. Surgery. 2010;147(5):631–9. https://doi.org/10.1016/j.surg.2009.10.071.
Ontrup G, Vogel M, Wolf OT, Zahn PK, Kluge A, Hagemann V. Does simulation-based training in medical education need additional stressors? An experimental study. Ergonomics. 2020;63(1):80–90. https://doi.org/10.1080/00140139.2019.1677948.
Boyle E, Kennedy AM, Doherty E, O’Keeffe D, Traynor O. Coping with stress in surgery: the difficulty of measuring non-technical skills. Ir J Med Sci. 2011;180(1):215–20. https://doi.org/10.1007/s11845-010-0578-z.
Pottier P, Hardouin JB, Dejoie T, et al. Effect of extrinsic and intrinsic stressors on clinical skills performance in third-year medical students. J Gen Intern Med. 2015;30(9):1259–69. https://doi.org/10.1007/s11606-015-3314-6.
Selye H. Stress and the general adaptation syndrome. Br Med J. 1950;1(4667):1383–92. https://doi.org/10.1136/bmj.1.4667.1383.
Biggs A, Brough P, Drummond S. Lazarus and Folkman’s Psychological Stress and Coping Theory. In: Cooper CL, Quick JC, eds. The Handbook of Stress and Health. John Wiley & Sons, Ltd; 2017:349-364. https://doi.org/10.1002/9781118993811.ch21.
Maher Z, Milner R, Cripe J, Gaughan J, Fish J, Goldberg AJ. Stress training for the surgical resident. Am J Surg. 2013;205(2):169–74. https://doi.org/10.1016/j.amjsurg.2012.10.007.
Bong CL, Lee S, Ng ASB, Allen JC, Lim EHL, Vidyarthi A. The effects of active (hot-seat) versus observer roles during simulation-based training on stress levels and non-technical performance: a randomized trial. Adv Simul. 2017;2(1):7. https://doi.org/10.1186/s41077-017-0040-7.
Poolton JM, Wilson MR, Malhotra N, Ngo K, Masters RSW. A comparison of evaluation, time pressure, and multitasking as stressors of psychomotor operative performance. Surgery. 2011;149(6):776–82. https://doi.org/10.1016/j.surg.2010.12.005.
Malhotra N, Poolton JM, Wilson MR, Ngo K, Masters RSW. Conscious monitoring and control (reinvestment) in surgical performance under pressure. Surg Endosc. 2012;26(9):2423–9. https://doi.org/10.1007/s00464-012-2193-8.
Dias RD, Scalabrini-Neto A. Acute stress in residents playing different roles during emergency simulations: a preliminary study. Int J Med Educ. 2017;8:239–43. https://doi.org/10.5116/ijme.5929.60f1.
Bakhsh A, Martin GFJ, Bicknell CD, Pettengell C, Riga C. An evaluation of the impact of high-fidelity endovascular simulation on surgeon stress and technical performance. J Surg Educ. 2019;76(3):864–71. https://doi.org/10.1016/j.jsurg.2018.10.015.
Finan E, Bismilla Z, Whyte HE, LeBlanc V, McNamara PJ. High-fidelity simulator technology may not be superior to traditional low-fidelity equipment for neonatal resuscitation training. J Perinatol. 2012;32(4):287–92. https://doi.org/10.1038/jp.2011.96.
Daglius Dias R, Scalabrini Neto A. Stress levels during emergency care: a comparison between reality and simulated scenarios. J Crit Care. 2016;33:8–13. https://doi.org/10.1016/j.jcrc.2016.02.010.
Flinn JT, Miller A, Pyatka N, Brewer J, Schneider T, Cao CGL. The effect of stress on learning in surgical skill acquisition. Med Teach. 2016;38(9):897–903. https://doi.org/10.3109/0142159X.2015.1114597.
DeMaria S, Silverman ER, Lapidus KAB, et al. The impact of simulated patient death on medical students’ stress response and learning of ACLS. Med Teach. 2016;38(7):730–7. https://doi.org/10.3109/0142159X.2016.1150986.
Harvey A, Nathens AB, Bandiera G, LeBlanc VR. Threat and challenge: cognitive appraisal and stress responses in simulated trauma resuscitations: appraisal and stress in simulated trauma resuscitations. Med Educ. 2010;44(6):587–94. https://doi.org/10.1111/j.1365-2923.2010.03634.x.
Łoś K, Chmielewski J, Łuczyński W. Relationship between executive functions, mindfulness, stress, and performance in pediatric emergency simulations. IJERPH. 2020;17(6):2040. https://doi.org/10.3390/ijerph17062040.
Waterland P, Khan FS, Ismaili E, Cheruvu C. Environmental noise as an operative stressor during simulated laparoscopic surgery. Surg Laparoscopy Endosc Percutaneous Techniques. 2016;26(2):133–6. https://doi.org/10.1097/SLE.0000000000000250.
Modi HN, Singh H, Fiorentino F, et al. Association of residents’ neural signatures with stress resilience during surgery. JAMA Surg. 2019;154(10):e192552. https://doi.org/10.1001/jamasurg.2019.2552.
Modi HN, Singh H, Orihuela-Espina F, et al. Temporal stress in the operating room: brain engagement promotes “coping” and disengagement prompts “choking.” Ann Surg. 2018;267(4):683–91. https://doi.org/10.1097/SLA.0000000000002289.
Lizotte MH, Janvier A, Latraverse V, et al. The impact of neonatal simulations on trainees’ stress and performance: a parallel-group randomized trial*. Pediatr Crit Care Med. 2017;18(5):434–41. https://doi.org/10.1097/PCC.0000000000001119.
Deinzer R, Kiupel S, Weik U. Endocrine and psychological stress response in simulated doctor-patient interactions in medical education. Psychoneuroendocrinology. 2019;105:172–7. https://doi.org/10.1016/j.psyneuen.2018.09.028.
Keitel A, Ringleb M, Schwartges I, et al. Endocrine and psychological stress responses in a simulated emergency situation. Psychoneuroendocrinology. 2011;36(1):98–108. https://doi.org/10.1016/j.psyneuen.2010.06.011.
Goldberg MB, Mazzei M, Maher Z, et al. Optimizing performance through stress training — an educational strategy for surgical residents. Am J Surg. 2018;216(3):618–23. https://doi.org/10.1016/j.amjsurg.2017.11.040.
Geeraerts T, Roulleau P, Cheisson G, et al. Physiological and self-assessed psychological stress induced by a high fidelity simulation course among third year anesthesia and critical care residents: an observational study. Anaesth Crit Care Pain Med. 2017;36(6):403–6. https://doi.org/10.1016/j.accpm.2017.06.002.
Hochberg MS, Berman RS, Kalet AL, Zabar SR, Gillespie C, Pachter HL. The stress of residency: recognizing the signs of depression and suicide in you and your fellow residents. Am J Surg. 2013;205(2):141–6. https://doi.org/10.1016/j.amjsurg.2012.08.003.
Ishiyama Y, Inaki N, Bando H, Yamada T. Assessment of intracorporeal suturing in single-port surgery using an experimental suturing model. Indian J Surg. 2017;79(2):137–42. https://doi.org/10.1007/s12262-016-1445-6.
Maschuw K, Schlosser K, Kupietz E, Slater EP, Weyers P, Hassan I. Do soft skills predict surgical performance?: a single-center randomized controlled trial evaluating predictors of skill acquisition in virtual reality laparoscopy. World J Surg. 2011;35(3):480–6. https://doi.org/10.1007/s00268-010-0933-2.
Larkin AC, Cahan MA, Whalen G, et al. Human Emotion and Response in Surgery (HEARS): a simulation-based curriculum for communication skills, systems-based practice, and professionalism in surgical residency training. J Am Coll Surg. 2010;211(2):285–92. https://doi.org/10.1016/j.jamcollsurg.2010.04.004.
Hunziker S, Pagani S, Fasler K, Tschan F, Semmer NK, Marsch S. Impact of a stress coping strategy on perceived stress levels and performance during a simulated cardiopulmonary resuscitation: a randomized controlled trial. BMC Emerg Med. 2013;13(1):8. https://doi.org/10.1186/1471-227X-13-8.
Pai DR, Ram S, Madan SS, Soe HHK, Barua A. Causes of stress and their change with repeated sessions as perceived by undergraduate medical students during high-fidelity trauma simulation. The Natl Med J India. 2014;27(4):7.
Nicolaides M, Theodorou E, Emin EI, et al. Team performance training for medical students: Low vs. high fidelity simulation. Ann Med Surg. 2020;55:308–15. https://doi.org/10.1016/j.amsu.2020.05.042.
Bragard I, Etienne AM, Merckaert I, Libert Y, Razavi D. Efficacy of a Communication and stress management training on medical residents’ self-efficacy, stress to communicate and burnout: a randomized controlled study. J Health Psychol. 2010;15(7):1075–81. https://doi.org/10.1177/1359105310361992.
Murugavadigal N. The impact of stressors on the learning outcome of high-fidelity patient simulation in undergraduate medical students. 2020;75(3):7
Schwill S, Fahrbach-Veeser J, Moeltner A, et al. Peers as OSCE assessors for junior medical students – a review of routine use: a mixed methods study. BMC Med Educ. 2020;20(1):17. https://doi.org/10.1186/s12909-019-1898-y.
Bragard I, Seghaye MC, Farhat N, et al. Implementation of a 2-day simulation-based course to prepare medical graduates on their first year of residency. Pediatric Emerg Care. 2018;34(12):857–61. https://doi.org/10.1097/PEC.0000000000000930.
Klein MI, Mouraviev V, Craig C, et al. Mental stress experienced by first-year residents and expert surgeons with robotic and laparoscopic surgery interfaces. J Robotic Surg. 2014;8(2):149–55. https://doi.org/10.1007/s11701-013-0446-8.
Klein MI, Warm JS, Riley MA, et al. Mental workload and stress perceived by novice operators in the laparoscopic and robotic minimally invasive surgical interfaces. J Endourol. 2012;26(8):1089–94. https://doi.org/10.1089/end.2011.0641.
Anyanwu GE, Nto JN, Agu AU, Ekezie J, Esom EA. Musical preferences and learning outcome of medical students in cadaver dissection laboratory: a Nigerian survey. Ann Anat - Anatomischer Anzeiger. 2016;208:228–33. https://doi.org/10.1016/j.aanat.2016.07.010.
Alt-Epping B, Lohse C, Viebahn C, von Steinbüchel N, Benze G, Nauck F. On death and dying – an exploratory and evaluative study of a reflective, interdisciplinary course element in undergraduate anatomy teaching. BMC Med Educ. 2014;14(1):15. https://doi.org/10.1186/1472-6920-14-15.
Anton NE, Bean EA, Myers E, Stefanidis D. Optimizing learner engagement during mental skills training: a pilot study of small group vs. individualized training. Am J Surg. 2020;219(2):335–9. https://doi.org/10.1016/j.amjsurg.2019.12.022.
Khairat S, Coleman C, Ottmar P, Bice T, Koppel R, Carson SS. Physicians’ gender and their use of electronic health records: findings from a mixed-methods usability study. J Am Med Informatics Assoc. 2019;26(12):1505–14. https://doi.org/10.1093/jamia/ocz126.
Feng X, Morandi A, Boehne M, et al. 3-Dimensional (3D) laparoscopy improves operating time in small spaces without impact on hemodynamics and psychomental stress parameters of the surgeon. Surg Endosc. 2015;29(5):1231–9. https://doi.org/10.1007/s00464-015-4083-3.
Pavlidis I, Zavlin D, Khatri AR, Wesley A, Panagopoulos G, Echo A. Absence of stressful conditions accelerates dexterous skill acquisition in surgery. Sci Rep. 2019;9(1):1747. https://doi.org/10.1038/s41598-019-38727-z.
Cleary DR, Siler DA, Whitney N, Selden NR. A microcontroller-based simulation of dural venous sinus injury for neurosurgical training. J Neurosurg. 2018;128(5):1553–9. https://doi.org/10.3171/2016.12.JNS162165.
Maddox MM, Lopez A, Mandava SH, et al. Electroencephalographic monitoring of brain wave activity during laparoscopic surgical simulation to measure surgeon concentration and stress: can the student become the master? J Endourol. 2015;29(12):1329–33. https://doi.org/10.1089/end.2015.0239.
Le Lous M, De Chanaud N, Bourret A, et al. Improving the quality of transvaginal ultrasound scan by simulation training for general practice residents. Adv Simul. 2017;2(1):24. https://doi.org/10.1186/s41077-017-0056-z.
Fukushima Y, Yamada A, Imoto N, Iba T. Does TeamSTEPPS affect psychological status? IJHCQA. 2019;32(1):11–20. https://doi.org/10.1108/IJHCQA-08-2017-0156.
Marvin RK, Saepoo MB, Ye S, et al. Salivary protein changes in response to acute stress in medical residents performing advanced clinical simulations: a pilot proteomics study. Biomarkers. 2017;22(3–4):372–82. https://doi.org/10.1080/1354750X.2017.1279215.
LaPorta AJ, McKee J, Hoang T, et al. Stress inoculation: preparing outside the box in surgical resuscitation and education. Curr Trauma Rep. 2017;3(2):135–43. https://doi.org/10.1007/s40719-017-0090-2.
Timberlake MD, Stefanidis D, Gardner AK. Examining the impact of surgical coaching on trainee physiologic response and basic skill acquisition. Surg Endosc. 2018;32(10):4183–90. https://doi.org/10.1007/s00464-018-6163-7.
Dedmon MM, O’Connell BP, Yawn RJ, et al. Measuring mental stress during otologic surgery using heart rate variability analysis. Otol Neurotol. 2019;40(4):529–34. https://doi.org/10.1097/MAO.0000000000002187.
Kromann CB, Jensen ML, Ringsted C. Test-enhanced learning may be a gender-related phenomenon explained by changes in cortisol level: Test-enhanced learning, gender and cortisol. Med Educ. 2011;45(2):192–9. https://doi.org/10.1111/j.1365-2923.2010.03790.x.
Cheung EO, Barsuk JH, Mitra D, et al. Preliminary efficacy of a brief mindfulness intervention for procedural stress in medical intern simulated performance: a randomized controlled pilot trial. J Altern Complement Med. 2020;26(4):282–90. https://doi.org/10.1089/acm.2019.0209.
Johnson JM, Stern TA. Teaching residents about emotional intelligence and its impact on leadership. Acad Psychiatry. 2014;38(4):510–3. https://doi.org/10.1007/s40596-014-0048-4.
Reed S, Kassis K, Nagel R, Verbeck N, Mahan JD, Shell R. Does emotional intelligence predict breaking bad news skills in pediatric interns? A pilot study. Med Educ Online. 2015;20(1):24245. https://doi.org/10.3402/meo.v20.24245.
Dugan JW, Weatherly RA, Girod DA, Barber CE, Tsue TT. A longitudinal study of emotional intelligence training for otolaryngology residents and faculty. JAMA Otolaryngol Head Neck Surg. 2014;140(8):720. https://doi.org/10.1001/jamaoto.2014.1169.
Nayar SK, Musto L, Fernandes R, Bharathan R. Emotional intelligence predicts accurate self-assessment of surgical quality: a pilot study. J Surg Res. 2020;245:383–9. https://doi.org/10.1016/j.jss.2019.07.051.
Cherry MG, Fletcher I, O’Sullivan H. Exploring the relationships among attachment, emotional intelligence and communication: emotional intelligence and clinical communication. Med Educ. 2013;47(3):317–25. https://doi.org/10.1111/medu.12115.
Lim G, Gardner AK. Emotional intelligence and delivering bad news: the jury is still out. J Surg Educ. 2019;76(3):779–84. https://doi.org/10.1016/j.jsurg.2018.09.017.
Kanter JW, Rosen DC, Manbeck KE, et al. Addressing microaggressions in racially charged patient-provider interactions: a pilot randomized trial. BMC Med Educ. 2020;20(1):88. https://doi.org/10.1186/s12909-020-02004-9.
Graupe T, Fischer MR, Strijbos JW, Kiessling C. Development and piloting of a situational judgement test for emotion-handling skills using the Verona Coding Definitions of Emotional Sequences (VR-CoDES). Patient Educ Counsel. 2020;103(9):1839–45. https://doi.org/10.1016/j.pec.2020.04.001.
Farrell MH. Child health providers’ precautionary discussion of emotions during communication about results of newborn genetic screening. Arch Pediatr Adolesc Med. 2012;166(1):62. https://doi.org/10.1001/archpediatrics.2011.696.
Ruiz-Moral R, Pérula de Torres L, Monge D, García Leonardo C, Caballero F. Teaching medical students to express empathy by exploring patient emotions and experiences in standardized medical encounters. Patient Educ Counsel. 2017;100(9):1694–700. https://doi.org/10.1016/j.pec.2017.04.018.
Bourgeon L, Bensalah M, Vacher A, Ardouin JC, Debien B. Role of emotional competence in residents’ simulated emergency care performance: a mixed-methods study. BMJ Qual Saf. 2016;25(5):364–71. https://doi.org/10.1136/bmjqs-2015-004032.
Schweller M, Costa FO, Antônio MÂRGM, Amaral EM, de Carvalho-Filho MA. The impact of simulated medical consultations on the empathy levels of students at one medical school. Acad Med. 2014;89(4):632–7. https://doi.org/10.1097/ACM.0000000000000175.
Sevrain-Goideau M, Gohier B, Bellanger W, Annweiler C, Campone M, Coutant R. Forum theater staging of difficult encounters with patients to increase empathy in students: evaluation of efficacy at The University of Angers Medical School. BMC Med Educ. 2020;20(1):58. https://doi.org/10.1186/s12909-020-1965-4.
Nelson S, Germann C, MacVane C, Bloch R, Fallon T, Strout T. Intern as patient: a patient experience simulation to cultivate empathy in emergency medicine residents. WestJEM. 2018:41-48. https://doi.org/10.5811/westjem.2017.11.35198.
Ogle J, Bushnell JA, Caputi P. Empathy is related to clinical competence in medical care. Med Educ. 2013;47(8):824–31. https://doi.org/10.1111/medu.12232.
Berg K, Majdan JF, Berg D, Veloski J, Hojat M. Medical studentsʼ self-reported empathy and simulated patientsʼ assessments of student empathy: an analysis by gender and ethnicity. Acad Med. 2011;86(8):984–8. https://doi.org/10.1097/ACM.0b013e3182224f1f.
Hojat M, Mangione S, Nasca TJ, et al. The Jefferson Scale of Physician Empathy: development and preliminary psychometric data. Educ Psychol Measure. 2001;61(2):349–65. https://doi.org/10.1177/00131640121971158.
LaNoue MD, Roter DL. Exploring patient-centeredness: the relationship between self-reported empathy and patient-centered communication in medical trainees. Patient Educ Counsel. 2018;101(6):1143–6. https://doi.org/10.1016/j.pec.2018.01.016.
Andrei F, Smith MM, Surcinelli P, Baldaro B, Saklofske DH. The Trait Emotional Intelligence Questionnaire: internal structure, convergent, criterion, and incremental validity in an Italian sample. Measure Eval Counsel Dev. 2016;49(1):34–45. https://doi.org/10.1177/0748175615596786.
Trickey AW, Newcomb AB, Porrey M, et al. Assessment of surgery residents’ interpersonal communication skills: validation evidence for the communication assessment tool in a simulation environment. J Surg Educ. 2016;73(6):e19–27. https://doi.org/10.1016/j.jsurg.2016.04.016.
Mayer JD, Salovey P, Caruso DR. Mayer-Salovey-Caruso Emotional Intelligence Test. Published online May 7, 2012. https://doi.org/10.1037/t05047-000.
Huizinga CRH, de Kam ML, Stockmann HBAC, van Gerven JMA, Cohen AF, van der Bogt KEA. Evaluating fitness to perform in surgical residents after night shifts and alcohol intoxication: the development of a “fit-to-perform” test. J Surg Educ. 2018;75(4):968–77. https://doi.org/10.1016/j.jsurg.2018.01.010.
Bond A, Lader M. The use of analogue scales in rating subjective feelings. Br J Med Psychol. 1974;47(3):211–8. https://doi.org/10.1111/j.2044-8341.1974.tb02285.x.
Pekrun R, Perry RP. Control-value theory of achievement emotions. In: International Handbook of Emotions in Education. Routledge; 2014. https://doi.org/10.4324/9780203148211.ch7.
Spielberger CD, Gonzalez-Reigosa F, Martinez-Urrutia A, Natalicio LF, Natalicio DS. The state-trait anxiety inventory. Revista Interamericana de Psicologia/Interamerican J Psychology. 1971;5(3 & 4).
Watson D, Friend R. Measurement of social-evaluative anxiety. J Consult Clin Psychol. 1969;33(4):448–57. https://doi.org/10.1037/h0027806.
Turner JE. Researching state shame with the Experiential Shame Scale. J Psychol. 2014;148(5):577–601. https://doi.org/10.1080/00223980.2013.818927.
Pekrun R, Goetz T, Frenzel AC, Barchfeld P, Perry RP. Measuring emotions in students’ learning and performance: the Achievement Emotions Questionnaire (AEQ). Contemp Educ Psychol. 2011;36(1):36–48. https://doi.org/10.1016/j.cedpsych.2010.10.002.
Rowe A, Fitness J. Understanding the role of negative emotions in adult learning and achievement: a social functional perspective. Behav Sci. 2018;8(2):27. https://doi.org/10.3390/bs8020027.
Gross JJ. The extended process model of emotion regulation: elaborations, applications, and future directions. Psychol Inquiry. 2015;26(1):130–7. https://doi.org/10.1080/1047840X.2015.989751.
Goleman D. Emotional Intelligence. 25th anniversary edition. Bantam Books; 2020.
Salovey P, Mayer JD. Emotional intelligence. Imagination Cogn Personal. 1990;9(3):185–211. https://doi.org/10.2190/DUGG-P24E-52WK-6CDG.
Petrides KV, Pita R, Kokkinaki F. The location of trait emotional intelligence in personality factor space. Bri J Psychol. 2007;98(2):273–89. https://doi.org/10.1348/000712606X120618.
Pekrun R. Achievement emotions: a control-value theory perspective. In: Emotions in Late Modernity. Routledge; 2019:142-157.
Crosswell AD, Lockwood KG. Best practices for stress measurement: how to measure psychological stress in health research. Health Psychol Open. 2020;7(2):205510292093307. https://doi.org/10.1177/2055102920933072.
Camacho-Morles J, Slemp GR, Pekrun R, Loderer K, Hou H, Oades LG. Activity achievement emotions and academic performance: a meta-analysis. Educ Psychol Rev. 2021;33(3):1051–95. https://doi.org/10.1007/s10648-020-09585-3.
Dohms MC. Video-based feedback using real consultations for a formative assessment in communication skills. Published online 2020:9.
Ogarkova A. Cross-lingual translatability of emotion terms. In: Emotion Measurement. Elsevier; 2021:909-935. https://doi.org/10.1016/B978-0-12-821124-3.00028-4.
Chentsova Dutton YE, Lyons SH. Different ways of measuring emotions cross-culturally. In: Emotion Measurement. Elsevier; 2021:937-974. https://doi.org/10.1016/B978-0-12-821124-3.00029-6.
Romotzky V, Galushko M, Düsterdiek A, et al. “It’s Not that Easy”—Medical Students’ Fears and Barriers in End-of-Life Communication. J Canc Educ. 2015;30(2):333–9. https://doi.org/10.1007/s13187-014-0712-0.
Feng X, Morandi A, Boehne M, et al. 3-Dimensional (3D) laparoscopy improves operating time in small spaces without impact on hemodynamics and psychomental stress parameters of the surgeon. Surg Endosc. 2015;29(5):1231–9. https://doi.org/10.1007/s00464-015-4083-3.
Poolton JM, Wilson MR, Malhotra N, Ngo K, Masters RSW. A comparison of evaluation, time pressure, and multitasking as stressors of psychomotor operative performance. Surgery. 2011;149(6):776–82. https://doi.org/10.1016/j.surg.2010.12.005.
Dugan JW, Weatherly RA, Girod DA, Barber CE, Tsue TT. A Longitudinal Study of Emotional Intelligence Training for Otolaryngology Residents and Faculty. JAMA Otolaryngol Head Neck Surg. 2014;140(8):720. https://doi.org/10.1001/jamaoto.2014.1169.
Cleary DR, Siler DA, Whitney N, Selden NR. A microcontroller-based simulation of dural venous sinus injury for neurosurgical training. J Neurosurg. 2018;128(5):1553–9. https://doi.org/10.3171/2016.12.JNS162165.
Grayson-Sneed KA, Smith RC. A research coding method to evaluate a smoking cessation model for training residents—A preliminary report. Patient Educ Counsel. 2018;101(3):541–5. https://doi.org/10.1016/j.pec.2017.09.010.
Grayson-Sneed KA, Smith RC. A research coding method to evaluate medical clinicians conduct of behavioral health care in patients with unexplained symptoms. Patient Educ Counsel. 2018;101(4):743–9. https://doi.org/10.1016/j.pec.2017.10.006.
Daly SC, Wilson NA, Rinewalt DE, Bines SD, Luu MB, Myers JA. A Subjective Assessment of Medical Student Perceptions on Animal Models in Medical Education. J Surg Educ. 2014;71(1):61–4. https://doi.org/10.1016/j.jsurg.2013.06.017.
Pavlidis I, Zavlin D, Khatri AR, Wesley A, Panagopoulos G, Echo A. Absence of Stressful Conditions Accelerates Dexterous Skill Acquisition in Surgery. Sci Rep. 2019;9(1):1747. https://doi.org/10.1038/s41598-019-38727-z.
Dias RD, Scalabrini-Neto A. Acute stress in residents playing different roles during emergency simulations: a preliminary study. Int J Med Educ. 2017;8:239–43. https://doi.org/10.5116/ijme.5929.60f1.
Kanter JW, Rosen DC, Manbeck KE, et al. Addressing microaggressions in racially charged patient-provider interactions: a pilot randomized trial. BMC Med Educ. 2020;20(1):88. https://doi.org/10.1186/s12909-020-02004-9.
Bakhsh A, Martin GFJ, Bicknell CD, Pettengell 1186 C, Riga C. An Evaluation of the Impact of High-Fidelity Endovascular Simulation on Surgeon Stress and Technical Performance. J Surg Educ. 2019;76(3):864–71. https://doi.org/10.1016/j.jsurg.2018.10.015.
Bauer C, Rimmelé T, Duclos A, et al. Anxiety and stress among anaesthesiology and critical care residents during high-fidelity simulation sessions. Anaesth Crit Care Pain Med. 2016;35(6):407–16. https://doi.org/10.1016/j.accpm.2016.01.004.
Romo-Barrientos C, Criado-Álvarez JJ, González-González J, et al. Anxiety levels among health sciences students during their first visit to the dissection room. BMC Med Educ. 2020;20(1):109. https://doi.org/10.1186/s12909-020-02027-2.
Harendza S, Soll H, Prediger S, Kadmon M, Berberat PO, Oubaid V. Assessing core competences of medical students with a test for flight school applicants. BMC Med Educ. 2019;19(1):9. https://doi.org/10.1186/s12909-018-1438-1.
Posner G, Naik V, Bidlake E, et al. Assessing Residents’ Disclosure of Adverse Events: Traditional Objective Structured Clinical Examinations Versus Mixed Reality. J Obstet Gynaecol Can. 2012;34(4):367–73. https://doi.org/10.1016/S1701-2163(16)35219-7.
Ishiyama Y, Inaki N, Bando H, Yamada T. Assessment of Intracorporeal Suturing in Single-Port Surgery Using an Experimental Suturing Model. Indian J Surg. 2017;79(2):137–42. https://doi.org/10.1007/s12262-016-1445-6.
Trickey AW, Newcomb AB, Porrey M, et al. Assessment of Surgery Residents’ Interpersonal Communication Skills: Validation Evidence for the Communication Assessment Tool in a Simulation Environment. J Surg Educ. 2016;73(6):e19–27. https://doi.org/10.1016/j.jsurg.2016.04.016.
Tramèr L, Becker C, Hochstrasser S, Marsch S, Hunziker S. Association of electrocardiogram alterations of rescuers and performance during a simulated cardiac arrest: A prospective simulation study. Lazzeri C, ed. PLoS ONE. 2018;13(6):e0198661. https://doi.org/10.1371/journal.pone.0198661.
Modi HN, Singh H, Fiorentino F, et al. Association of Residents’ Neural Signatures With Stress Resilience During Surgery. JAMA Surg. 2019;154(10):e192552. https://doi.org/10.1001/jamasurg.2019.2552.
Tramèr L, Becker C, Schumacher C, et al. Association of self-esteem, personality, stress and gender with performance of a resuscitation team: A simulation-based study. Roma PG, ed. PLoS ONE. 2020;15(5):e0233155. https://doi.org/10.1371/journal.pone.0233155.
Rajeh NA, Badroun LE, Alqarni AK, et al. Cadaver dissection: A positive experience among Saudi female medical students. J Taibah Univ Med Sci. 2017;12(3):268–72. https://doi.org/10.1016/j.jtumed.2016.07.005.
Pai DR, Ram S, Madan SS, Soe 1220 HHK, Barua A. Causes of stress and their change with repeated sessions as perceived by undergraduate medical students during high-fidelity trauma simulation. Natl Med J India. 2014;27(4):7.
Yutani M, Takahashi M, Miyaoka H. Changes in communication skills of clinical residents through psychiatric training: Communication skills training. Psychiatry Clin Neurosci. 2011;65(6):561–6. https://doi.org/10.1111/j.1440-1819.2011.02265.x.
Farrell MH. Child Health Providers’ Precautionary Discussion of Emotions During Communication About Results of Newborn Genetic Screening. Arch Pediatr Adolesc Med. 2012;166(1):62. https://doi.org/10.1001/archpediatrics.2011.696.
Carenzo L, Braithwaite EC, Carfagna F, et al. Cognitive appraisals and team performance under stress: A simulation study. Med Educ. 2020;54(3):254–63. https://doi.org/10.1111/medu.14050.
Malhotra N, Poolton JM, Wilson MR, Ngo K, Masters RSW. Conscious monitoring and control (reinvestment) in surgical performance under pressure. Surg Endosc. 2012;26(9):2423–9. https://doi.org/10.1007/s00464-012-2193-8.
Boyle E, Kennedy AM, Doherty E, O’Keeffe D, Traynor O. Coping with stress in surgery: the difficulty of measuring non-technical skills. Ir J Med Sci. 2011;180(1):215–20. https://doi.org/10.1007/s11845-010-0578-z.
Graupe T, Fischer MR, Strijbos JW, Kiessling C. Development and piloting of a Situational Judgement Test for emotion-handling skills using the Verona Coding Definitions of Emotional Sequences (VR-CoDES). Patient Educ Couns. 2020;103(9):1839–45. https://doi.org/10.1016/j.pec.2020.04.001.
Maschuw K, Schlosser K, Kupietz E, Slater EP, Weyers P, Hassan I. Do Soft Skills Predict Surgical Performance?: A Single-Center Randomized Controlled Trial Evaluating Predictors of Skill Acquisition in Virtual Reality Laparoscopy. World J Surg. 2011;35(3):480–6. https://doi.org/10.1007/s00268-010-0933-2.
Reed S, Kassis K, Nagel R, Verbeck N, Mahan JD, Shell R. Does emotional intelligence predict breaking bad news skills in pediatric interns? A pilot study. Med Educ Online. 2015;20(1):24245. https://doi.org/10.3402/meo.v20.24245.
Ontrup G, Vogel M, Wolf OT, Zahn PK, Kluge A, Hagemann V. Does simulation-based training in medical education need additional stressors? An experimental study Ergonomics. 2020;63(1):80–90. https://doi.org/10.1080/00140139.2019.1677948.
Hagemann V, Herbstreit F, Kehren C, et al. Does teaching non-technical skills to medical students improve those skills and simulated patient outcome? Int J Med Educ. 2017;8:101–13. https://doi.org/10.5116/ijme.58c1.9f0d.
Fukushima Y, Yamada A, Imoto N, Iba T. Does TeamSTEPPS affect psychological status? IJHCQA. 2019;32(1):11–20. https://doi.org/10.1108/IJHCQA-08-2017-0156.
Hunziker S, Semmer NK, Tschan F, Schuetz P, Mueller B, Marsch S. Dynamics and association of different acute stress markers with performance during a simulated resuscitation. Resuscitation. 2012;83(5):572–8. https://doi.org/10.1016/j.resuscitation.2011.11.013.
Pottier P, Hardouin JB, Dejoie T, et al. Effect of Extrinsic and Intrinsic Stressors on Clinical Skills Performance in Third-Year Medical Students. J Gen Intern Med. 2015;30(9):1259–69. https://doi.org/10.1007/s11606-015-3314-6.
Pottier P, Dejoie T, Hardouin JB, et al. Effect of stress on clinical reasoning during simulated ambulatory consultations. Medical Teacher. 2013;35(6):472–80. https://doi.org/10.3109/0142159X.2013.774336.
Bragard I, Etienne AM, Merckaert I, Libert Y, Razavi D. Efficacy of a Communication and Stress Management Training on Medical Residents’ Self-efficacy, Stress to Communicate and Burnout: A Randomized Controlled Study. J Health Psychol. 2010;15(7):1075–81. https://doi.org/10.1177/1359105310361992.
Maddox MM, Lopez A, Mandava SH, et al. Electroencephalographic Monitoring of Brain Wave Activity During Laparoscopic Surgical Simulation to Measure Surgeon Concentration and Stress: Can the Student Become the Master? J Endourol. 2015;29(12):1329–33. https://doi.org/10.1089/end.2015.0239.
Fraser K, Ma I, Teteris E, Baxter H, Wright B, McLaughlin K. Emotion, cognitive load and learning outcomes during simulation training: Emotion and cognitive load during simulation. Med Educ. 2012;46(11):1055–62. https://doi.org/10.1111/j.1365-2923.2012.04355.x.
Chang HJ, Kim HJ, Rhyu IJ, Lee YM, Uhm CS. Emotional experiences of medical students during cadaver dissection and the role of memorial ceremonies: a qualitative study. BMC Med Educ. 2018;18(1):255. https://doi.org/10.1186/s12909-018-1358-0.
Lim G, Gardner AK. Emotional Intelligence and Delivering Bad News: The Jury is Still Out. J Surg Educ. 2019;76(3):779–84. https://doi.org/10.1016/j.jsurg.2018.09.017.
Arora S, Russ S, Petrides KV, et al. Emotional Intelligence and Stress in Medical Students Performing Surgical Tasks: Acad Med. 2011;86(10):1311–7. https://doi.org/10.1097/ACM.0b013e31822bd7aa.
Nayar SK, Musto L, Fernandes R, Bharathan R. Emotional Intelligence Predicts Accurate Self-Assessment of Surgical Quality: A Pilot Study. J Surg Res. 2020;245:383–9. https://doi.org/10.1016/j.jss.2019.07.051.
Ogle J, Bushnell JA, Caputi P. Empathy is related to clinical competence in medical care. Med Educ. 2013;47(8):824–31. https://doi.org/10.1111/medu.12232.
Deinzer R, Kiupel S, Weik U. Endocrine and psychological stress response in simulated doctor-patient interactions in medical education. Psychoneuroendocrinology. 2019;105:172–7. https://doi.org/10.1016/j.psyneuen.2018.09.028.
Keitel A, Ringleb M, Schwartges I, et al. Endocrine and psychological stress responses in a simulated emergency situation. Psychoneuroendocrinology. 2011;36(1):98–108. https://doi.org/10.1016/j.psyneuen.2010.06.011.
Bloomfield JG, O’Neill B, Gillett K. Enhancing student communication during end-of-life care: A pilot study. Pall Supp Care. 2015;13(6):1651–61. https://doi.org/10.1017/S147895151500022X.
Waterland P, Khan FS, Ismaili E, Cheruvu C. Environmental Noise as an Operative Stressor During Simulated Laparoscopic Surgery. Surg Laparosc Endosc Percutan Tech. 2016;26(2):133–6. https://doi.org/10.1097/SLE.0000000000000250.
Lewis G, McCullough M, Maxwell AP, Gormley GJ. Ethical reasoning through simulation: a phenomenological analysis of student experience. Adv Simul. 2016;1(1):26. https://doi.org/10.1186/s41077-016-0027-9.
Bob MH, Popescu CA, Armean MS, Suciu SM, Buzoianu AD. Ethical views, attitudes and reactions of Romanian medical students to the dissecting room. Rev Med Chir Soc Med Nat Iasi. 2014;118(4):1078–85.
Huizinga CRH, de Kam ML, Stockmann HBAC, van Gerven JMA, Cohen AF, van der Bogt KEA. Evaluating Fitness to Perform in Surgical Residents after Night Shifts and Alcohol Intoxication: The development of a “Fit-to-Perform” test. J Surg Educ. 2018;75(4):968–77. https://doi.org/10.1016/j.jsurg.2018.01.010.
Dupuy L, Micoulaud-Franchi JA, Cassoudesalle H, et al. Evaluation of a virtual agent to train medical students conducting psychiatric interviews for diagnosing major depressive disorders. J Affect Disord. 2020;263:1–8. https://doi.org/10.1016/j.jad.2019.11.117.
Timberlake MD, Stefanidis D, Gardner AK. Examining the impact of surgical coaching on trainee physiologic response and basic skill acquisition. Surg Endosc. 2018;32(10):4183–90. https://doi.org/10.1007/s00464-018-6163-7.
LaNoue MD, Roter DL. Exploring patient-centeredness: The relationship between self-reported empathy and patient-centered communication in medical trainees. Patient Educ Couns. 2018;101(6):1143–6. https://doi.org/10.1016/j.pec.2018.01.016.
Cherry MG, Fletcher I, O’Sullivan H. Exploring the relationships among attachment, emotional intelligence and communication: Emotional intelligence and clinical communication. Med Educ. 2013;47(3):317–25. https://doi.org/10.1111/medu.12115.
Kerins J, Smith SE, Phillips EC, Clarke B, Hamilton AL, Tallentire VR. Exploring transformative learning when developing medical students’ non-technical skills. Med Educ. 2020;54(3):264–74. https://doi.org/10.1111/medu.14062.
Behrens CC, Dolmans DH, Gormley GJ, Driessen EW. Exploring undergraduate students achievement emotions during ward round simulation: a mixed-method study. BMC Med Educ. 2019;19(1):316. https://doi.org/10.1186/s12909-019-1753-1.
Kim KJ. Factors associated with medical st 1328 udent test anxiety in objective structured clinical examinations: a preliminary study. Int J Med Educ. 2016;7:424–7. https://doi.org/10.5116/ijme.5845.caec.
Leboulanger N. First cadaver dissection: Stress, preparation, and emotional experience. Eur Ann Otorhinolaryngol Head Neck Dis. 2011;128(4):175–83. https://doi.org/10.1016/j.anorl.2011.01.007.
Sevrain-Goideau M, Gohier B, Bellanger W, Annweiler C, Campone M, Coutant R. Forum theater staging of difficult encounters with patients to increase empathy in students: evaluation of efficacy at The University of Angers Medical School. BMC Med Educ. 2020;20(1):58. https://doi.org/10.1186/s12909-020-1965-4.
Clarke S, Horeczko T, Cotton D, Bair A. Heart rate, anxiety and performance of residents during a simulated critical clinical encounter: a pilot study. BMC Med Educ. 2014;14(1):153. https://doi.org/10.1186/1472-6920-14-153.
Hurst SA, Baroffio A, Ummel M, Layat Burn C. Helping medical students to acquire a deeper understanding of truth-telling. Medical Education Online. 2015;20(1):28133. https://doi.org/10.3402/meo.v20.28133.
Finan E, Bismilla Z, Whyte HE, LeBlanc V, McNamara PJ. High-fidelity simulator technology may not be superior to traditional low-fidelity equipment for neonatal resuscitation training. J Perinatol. 2012;32(4):287–92. https://doi.org/10.1038/jp.2011.96.
Zhou Y, Collinson A, Laidlaw A, Humphris G. How Do Medical Students Respond to Emotional Cues and Concerns Expressed by Simulated Patients during OSCE Consultations? – A Multilevel Study. Houser D, ed. PLoS ONE. 2013;8(10):e79166. https://doi.org/10.1371/journal.pone.0079166.
Meunier J, Libert Y, Merckaert I, et al. How much is residents’ distress detection performance during a clinical round related to their characteristics? Patient Educ Couns. 2011;85(2):180–7. https://doi.org/10.1016/j.pec.2010.09.022.
Hulsman RL, Pranger S, Koot S, Fabriek M, Karemaker JM, Smets EMA. How stressful is doctor–patient communication? Physiological and psychological stress of medical students in simulated history taking and bad-news consultations. Int J Psychophysiol. 2010;77(1):26–34. https://doi.org/10.1016/j.ijpsycho.2010.04.001.
Larkin AC, Cahan MA, Whalen G, et al. Human Emotion and Response in Surgery (HEARS): A Simulation-Based Curriculum for Communication Skills, Systems-Based Practice, and Professionalism in Surgical Residency Training. J Am College of Surgeons. 2010;211(2):285–92. https://doi.org/10.1016/j.jamcollsurg.2010.04.004.
Torres A, Horodeńska M, Witkowski G, Torres K. Hybrid simulation of pediatric gynecologic examination: a mix-methods study of learners’ attitudes and factors affecting learning. BMC Med Educ. 2020;20(1):164. https://doi.org/10.1186/s12909-020-02076-7.
Hunziker S, Pagani S, Fasler K, Tschan F, Semmer NK, Marsch S. Impact of a stress coping strategy on perceived stress levels and performance during a simulated cardiopulmonary resuscitation: a randomized controlled trial. BMC Emerg Med. 2013;13(1):8. https://doi.org/10.1186/1471-227X-13-8.
Bajunaid K, Mullah MAS, Winkler-Schwartz A, et al. Impact of acute stress on psychomotor bimanual performance during a simulated tumor resection task. JNS. 2017;126(1):71–80. https://doi.org/10.3171/2015.5.JNS15558.
Piquette D, Tarshis J, Sinuff T, Fowler RA, Pinto R, Leblanc VR. Impact of Acute Stress on Resident Performance During Simulated Resuscitation Episodes: A Prospective Randomized Cross-Over Study. Teach Learn Med. 2014;26(1):9–16. https://doi.org/10.1080/10401334.2014.859932.
Harvey A, Bandiera G, Nathens AB, LeBlanc VR. Impact of stress on resident performance in simulated trauma scenarios. J Trauma Acute Care Surg. 2012;72(2):497–503. https://doi.org/10.1097/TA.0b013e31821f84be.
Wasp GT, Cullinan AM, Chamberlin MD, Hayes C, Barnato AE, Vergo MT. Implementation and Impact of a Serious Illness Communication Training for Hematology-Oncology Fellows. J Canc Educ. 2021;36(6):1325–32. https://doi.org/10.1007/s13187-020-01772-8.
Bragard I, Seghaye MC, Farhat N, et al. Implementation of a 2-Day Simulation-Based Course to Prepare Medical Graduates on Their First Year of Residency: Pediatr Emerg Care. 2018;34(12):857–61. https://doi.org/10.1097/PEC.0000000000000930.
Le Lous M, De Chanaud N, Bourret A, et al. Improving the quality of transvaginal ultrasound scan by simulation training for general practice residents. Adv Simul. 2017;2(1):24. https://doi.org/10.1186/s41077-017-0056-z.
Beckers SK, Biermann H, Sopka S, et al. Influence of pre-course assessment using an emotionally activating stimulus with feedback: A pilot study in teaching Basic Life Support. Resuscitation. 2012;83(2):219–26. https://doi.org/10.1016/j.resuscitation.2011.08.024.
Russa AD, Mligiliche NuruL. Inspiring Tanzanian medical students into the profession: appraisal of cadaveric dissection stress and coping strategies. Italian J Anat Embryol. 2015;119:268–76. 276 kB. https://doi.org/10.13128/IJAE-15560.
Nelson S, Germann C, MacVane C, Bloch R, Fallon T, Strout T. Intern as Patient: A Patient Experience Simulation to Cultivate Empathy in Emergency Medicine Residents. WestJEM. Published online January 18 2018:41–8. https://doi.org/10.5811/westjem.2017.11.35198.
McNeer RR, Bennett CL, Dudaryk R. Intraoperative Noise Increases Perceived Task Load and Fatigue in Anesthesiology Residents: A Simulation-Based Study. Anesth Analg. 2016;122(2):512–25. https://doi.org/10.1213/ANE.0000000000001067.
Robb A, Kopper R, Ambani R, et al. Leveraging Virtual Humans to Effectively Prepare Learners for Stressful Interpersonal Experiences. IEEE Trans Visual Comput Graphics. 2013;19(4):662–70. https://doi.org/10.1109/TVCG.2013.35.
Singh S, Modi C, Patel C, Pathak A. Low-fidelity simulation to enhance understanding of infection control among undergraduate medical students. Natl Med J India. 2017;30(4):215. https://doi.org/10.4103/0970-258X.218677.
Dedmon MM, O’Connell BP, Yawn RJ, et al. Measuring Mental Stress During Otologic Surgery Using Heart Rate Variability Analysis. Otol Neurotol. 2019;40(4):529–34. https://doi.org/10.1097/MAO.0000000000002187.
Tiuraniemi J, Läärä R, Kyrö T, Lindeman S. Medical and psychology students’ self-assessed communication skills: A pilot study. Patient Educ Couns. 2011;83(2):152–7. https://doi.org/10.1016/j.pec.2010.05.013.
Toivonen AK, Lindblom-Ylänne S, Louhiala P, Pyörälä E. Medical students’ reflections on emotions concerning breaking bad news. Patient Educ Couns. 2017;100(10):1903–9. https://doi.org/10.1016/j.pec.2017.05.036.
Berg K, Majdan JF, Berg D, Veloski J, Hojat M. Medical Studentsʼ Self-Reported Empathy and Simulated Patientsʼ Assessments of Student Empathy: An Analysis by Gender and Ethnicity: Acad Med. 2011;86(8):984–8. https://doi.org/10.1097/ACM.0b013e3182224f1f.
Klein MI, Mouraviev V, Craig C, et al. Mental stress experienced by first-year residents and expert surgeons with robotic and laparoscopic surgery interfaces. J Robotic Surg. 2014;8(2):149–55. https://doi.org/10.1007/s11701-013-0446-8.
Klein MI, Warm JS, Riley MA, et al. Mental Workload and Stress Perceived by Novice Operators in the Laparoscopic and Robotic Minimally Invasive Surgical Interfaces. J Endourol. 2012;26(8):1089–94. https://doi.org/10.1089/end.2011.0641.
Noll C, von Jan U, Raap U, Albrecht UV. Mobile Augmented Reality as a Feature for Self-Oriented, Blended Learning in Medicine: Randomized Controlled Trial. JMIR Mhealth Uhealth. 2017;5(9):e139. https://doi.org/10.2196/mhealth.7943.
Naismith LM, Lajoie SP. Motivation and emotion predict medical students’ attention to computer-based feedback. Adv in Health Sci Educ. 2018;23(3):465–85. https://doi.org/10.1007/s10459-017-9806-x.
Anyanwu GE, Nto JN, Agu AU, Ekezie J, Esom EA. Musical preferences and learning outcome of medical students in cadaver dissection laboratory: A Nigerian survey. Annal Anat Anat Anz. 2016;208:228–33. https://doi.org/10.1016/j.aanat.2016.07.010.
Alt-Epping B, Lohse C, Viebahn C, von Steinbüchel N, Benze G, Nauck F. On death and dying – an exploratory and evaluative study of a reflective, interdisciplinary course element in undergraduate anatomy teaching. BMC Med Educ. 2014;14(1):15. https://doi.org/10.1186/1472-6920-14-15.
Anton NE, Bean EA, Myers E, Stefanidis D. Optimizing learner engagement during mental skills training: A pilot study of small group vs. individualized training. Am J Surg. 2020;219(2):335–9. https://doi.org/10.1016/j.amjsurg.2019.12.022.
Goldberg MB, Mazzei M, Maher Z, et al. Optimizing performance through stress training — An educational strategy for surgical residents. Am J Surg. 2018;216(3):618–23. https://doi.org/10.1016/j.amjsurg.2017.11.040.
Smink GM, Jeffe DB, Hayashi RJ, Al-Hammadi N, Fehr JJ. Paediatric oncology simulation training for resident education. BMJ STEL. 2019;5(3):155–60. https://doi.org/10.1136/bmjstel-2018-000347.
Schwill S, Fahrbach-Veeser J, Moeltner A, et al. Peers as OSCE assessors for junior medical students – a review of routine use: a mixed methods study. BMC Med Educ. 2020;20(1):17. https://doi.org/10.1186/s12909-019-1898-y.
Khairat S, Coleman C, Ottmar P, Bice T, Koppel R, Carson SS. Physicians’ gender and their use of electronic health records: findings from a mixed-methods usability study. J Am Med Inform Assoc. 2019;26(12):1505–14. https://doi.org/10.1093/jamia/ocz126.
Geeraerts T, Roulleau P, Cheisson G, et al. Physiological and self-assessed psychological stress induced by a high fidelity simulation course among third year anesthesia and critical care residents: An observational study. Anaesth Crit Care Pain Med. 2017;36(6):403–6. https://doi.org/10.1016/j.accpm.2017.06.002.
Phitayakorn R, Minehart RD, Pian-Smith MCM, Hemingway MW, Petrusa ER. Practicality of using galvanic skin response to measure intraoperative physiologic autonomic activation in operating room team members. Surgery. 2015;158(5):1415–20. https://doi.org/10.1016/j.surg.2015.04.009.
Cheung EO, Barsuk JH, Mitra D, et al. Preliminary Efficacy of a Brief Mindfulness Intervention for Procedural Stress in Medical Intern Simulated Performance: A Randomized Controlled Pilot Trial. J Altern Complement Med. 2020;26(4):282–90. https://doi.org/10.1089/acm.2019.0209.
Bernhardt V, Rothkötter HJ, Kasten E. Psychische Belastungen durch die Dissektion am Leichnam im anatomischen Präparierkurs bei Erstsemestern des Studienfachs Medizin. GMS Z Med Ausbildung; 29(1):Doc12; ISSN 1860-3572. Published online 2012. https://doi.org/10.3205/ZMA000782.
Böckers A, Baader C, Fassnacht UK, Öchsner W, Böckers TM. Reduction of mental distress in the dissection course by introducing the body donor experience through anatomical demonstrations of organ systems. Anat Sci Ed. 2012;5(6):321–9. https://doi.org/10.1002/ase.1292.
Łoś K, Chmielewski J, Łuczyński W. Relationship between Executive Functions, Mindfulness, Stress, and Performance in Pediatric Emergency Simulations. IJERPH. 2020;17(6):2040. https://doi.org/10.3390/ijerph17062040.
Bourgeon L, Bensalah M, Vacher A, Ardouin JC, Debien B. Role of emotional competence in residents’ simulated emergency care performance: a mixed-methods study. BMJ Qual Saf. 2016;25(5):364–71. https://doi.org/10.1136/bmjqs-2015-004032.
Marvin RK, Saepoo MB, Ye S, et al. Salivary protein changes in response to acute stress in medical residents performing advanced clinical simulations: a pilot proteomics study. Biomarkers. 2017;22(3–4):372–82. https://doi.org/10.1080/1354750X.2017.1279215.
Rogers T, Andler C, O’Brien B, van Schaik S. Self-Reported Emotions in Simulation-Based Learning: Active Participants vs. Observers. Sim Healthcare. 2019;14(3):140–5. https://doi.org/10.1097/SIH.0000000000000354.
Hautz WE, Schröder T, Dannenberg KA, et al. Shame in Medical Education: A Randomized Study of the Acquisition of Intimate Examination Skills and Its Effect on Subsequent Performance. Teach Learn Med. 2017;29(2):196–206. https://doi.org/10.1080/10401334.2016.1254636.
Groot F, Jonker G, Rinia M, ten Cate O, Hoff RG. Simulation at the Frontier of the Zone of Proximal Development: A Test in Acute Care for Inexperienced Learners. Acad Med. 2020;95(7):1098–105. https://doi.org/10.1097/ACM.0000000000003265.
Baker BG, Bhalla A, Doleman B, et al. Simulation fails to replicate stress in trainees performing a technical procedure in the clinical environment. Med Teach. 2017;39(1):53–7. https://doi.org/10.1080/0142159X.2016.1230188.
Butteris SM, Gladding SP, Eppich W, Hagen SA, Pitt MB. Simulation Use for Global Away Rotations (SUGAR): Preparing Residents for Emotional Challenges Abroad—A Multicenter Study. Acad Pediatr. 2014;14(5):533–41. https://doi.org/10.1016/j.acap.2014.05.004.
Crewther BT, Shetty K, Jarchi D, et al. Skill acquisition and stress adaptations following laparoscopic surgery training and detraining in novice surgeons. Surg Endosc. 2016;30(7):2961–8. https://doi.org/10.1007/s00464-015-4584-0.
Lefroy J, Brosnan C, Creavin S. Some like it hot: medical student views on choosing the emotional level of a simulation: Student views on emotion in simulation. Med Educ. 2011;45(4):354–61. https://doi.org/10.1111/j.1365-2923.2010.03881.x.
Hurley AM, Kennedy PJ, O’Connor L, et al. SOS save our surgeons: Stress levels reduced by robotic surgery. Gynecol Surg. 2015;12(3):197–206. https://doi.org/10.1007/s10397-015-0891-7.
LaPorta AJ, McKee J, Hoang T, et al. Stress Inoculation: Preparing Outside the Box in Surgical Resuscitation and Education. Curr Trauma Rep. 2017;3(2):135–43. https://doi.org/10.1007/s40719-017-0090-2.
Daglius Dias R, Scalabrini Neto A. Stress levels during emergency care: A comparison between reality and simulated scenarios. J Crit Care. 2016;33:8–13. https://doi.org/10.1016/j.jcrc.2016.02.010.
Pottier P, Hardouin JB, Dejoie T, et al. Stress responses in medical students in ambulatory and in hospital patient consultations: Stress responses in medical students. Med Educ. 2011;45(7):678–87. https://doi.org/10.1111/j.1365-2923.2011.03935.x.
Maher Z, Milner R, Cripe J, Gaughan J, Fish J, Goldberg AJ. Stress training for the surgical resident. Am J Surg. 2013;205(2):169–74. https://doi.org/10.1016/j.amjsurg.2012.10.007.
Oriot D, Trigolet M, Kessler DO, Auerbach MA, Ghazali DA. Stress: A Factor Explaining the Gap Between Simulated and Clinical Procedure Success. Pediatr Emer Care. 2021;37(12):e1192–6. https://doi.org/10.1097/PEC.0000000000001962.
Brouwers MH, Bor H, Laan R, van Weel C, van Weel-Baumgarten E. Students’ experiences with a longitudinal skills training program on breaking bad news: A follow-up study. Patient Educ Couns. 2018;101(9):1639–44. https://doi.org/10.1016/j.pec.2018.05.008.
Ruiz-Moral R, Pérula de Torres L, Monge D, García Leonardo C, Caballero F. Teaching medical students to express empathy by exploring patient emotions and experiences in standardized medical encounters. Patient Educ Couns. 2017;100(9):1694–700. https://doi.org/10.1016/j.pec.2017.04.018.
Johnson JM, Stern TA. Teaching Residents About Emotional Intelligence and Its Impact on Leadership. Acad Psychiatry. 2014;38(4):510–3. https://doi.org/10.1007/s40596-014-0048-4.
Nicolaides M, Theodorou E, Emin EI, et al. Team performance training for medical students: Low vs high fidelity simulation. Ann Med Surg. 2020;55:308–15. https://doi.org/10.1016/j.amsu.2020.05.042.
Fraser K, McLaughlin K. Temporal pattern of emotions and cognitive load during simulation training and debriefing. Med Teach. 2019;41(2):184–9. https://doi.org/10.1080/0142159X.2018.1459531.
Modi HN, Singh H, Orihuela-Espina F, et al. Temporal Stress in the Operating Room: Brain Engagement Promotes “Coping” and Disengagement Prompts “Choking.” Ann Surg. 2018;267(4):683–91. https://doi.org/10.1097/SLA.0000000000002289.
Kromann CB, Jensen ML, Ringsted C. Test-enhanced learning may be a gender-related phenomenon explained by changes in cortisol level: Test-enhanced learning, gender and cortisol. Med Educ. 2011;45(2):192–9. https://doi.org/10.1111/j.1365-2923.2010.03790.x.
Flinn JT, Miller A, Pyatka N, Brewer J, Schneider T, Cao CGL. The effect of stress on learning in surgical skill acquisition. Med Teach. 2016;38(9):897–903. https://doi.org/10.3109/0142159X.2015.1114597.
Bong CL, Lee S, Ng ASB, Allen JC, Lim EHL, Vidyarthi A. The effects of active (hot-seat) versus observer roles during simulation-based training on stress levels and non-technical performance: a randomized trial. Adv Simul. 2017;2(1):7. https://doi.org/10.1186/s41077-017-0040-7.
O’Rourke SR, Branford KR, Brooks TL, Ives LT, Nagendran A, Compton SN. The Emotional and Behavioral Impact of Delivering Bad News to Virtual versus Real Standardized Patients: A Pilot Study. Teach Learn Med. 2020;32(2):139–49. https://doi.org/10.1080/10401334.2019.1652180.
Fraser K, Huffman J, Ma I, et al. The Emotional and Cognitive Impact of Unexpected Simulated Patient Death. Chest. 2014;145(5):958–63. https://doi.org/10.1378/chest.13-0987.
Cook CJ, Crewther BT. The impact of a competitive learning environment on hormonal and emotional stress responses and skill acquisition and expression in a medical student domain. Physiol Behav. 2019;199:252–7. https://doi.org/10.1016/j.physbeh.2018.11.027.
Lizotte MH, Janvier A, Latraverse V, et al. The Impact of Neonatal Simulations on Trainees’ Stress and Performance: A Parallel-Group Randomized Trial*. Pediatr Crit Care Med. 2017;18(5):434–41. https://doi.org/10.1097/PCC.0000000000001119.
Schweller M, Costa FO. Antônio MÂRGM, Amaral EM, de Carvalho-Filho MA. The Impact of Simulated Medical Consultations on the Empathy Levels of Students at One Medical School: Acad Med. 2014;89(4):632–7. https://doi.org/10.1097/ACM.0000000000000175.
DeMaria S, Silverman ER, Lapidus KAB, et al. The impact of simulated patient death on medical students’ stress response and learning of ACLS. Med Teach. 2016;38(7):730–7. https://doi.org/10.3109/0142159X.2016.1150986.
Andreatta PB, Hillard M, Krain LP. The impact of stress factors in simulation-based laparoscopic training. Surgery. 2010;147(5):631–9. https://doi.org/10.1016/j.surg.2009.10.071.
Nachiappan M, Bikramjit P, Aung WT, Htoo HKS, Sudipta P. The impact of stressors on the learning outcome of high-fidelity patient simulation in undergraduate medical students. Med J Malaysia. 2020;75(3):209–15.
Hochberg MS, Berman RS, Kalet AL, Zabar SR, Gillespie C, Pachter HL. The stress of residency: recognizing the signs of depression and suicide in you and your fellow residents. Am J Surg. 2013;205(2):141–6. https://doi.org/10.1016/j.amjsurg.2012.08.003.
Chia TI, Oyeniran OI, Ajagbe AO, Onigbinde OA, Oraebosi MI. The symptoms and stress experienced by medical students in anatomy dissection halls. J Taibah Univ Med Sci. 2020;15(1):8–13. https://doi.org/10.1016/j.jtumed.2020.01.001.
Harvey A, Nathens AB, Bandiera G, LeBlanc VR. Threat and challenge: cognitive appraisal and stress responses in simulated trauma resuscitations: Appraisal and stress in simulated trauma resuscitations. Med Educ. 2010;44(6):587–94. https://doi.org/10.1111/j.1365-2923.2010.03634.x.
Cerrone SA, Adelman P, Akbar S, Yacht AC, Fornari A. Using Objective Structured Teaching Encounters (OSTEs) to prepare chief residents to be emotionally intelligent leaders. Med Educ Online. 2017;22(1):1320186. https://doi.org/10.1080/10872981.2017.1320186.
Cherry MG, Fletcher I, O’Sullivan H. V 1575 alidating relationships among attachment, emotional intelligence and clinical communication. Med Educ. 2014;48(10):988–97. https://doi.org/10.1111/medu.12526.
Dohms MC, Collares CF, Tibério IC. Video-based feedback using real consultations for a formative assessment in communication skills. BMC Med Educ. 2020;20(1):57. https://doi.org/10.1186/s12909-020-1955-6.
Acknowledgements
We would like to acknowledge Andrea Quaiattini for her expert consultations on our methodology. We would also like to thank Naz Alpdogan for helping with the deduplication and the article screening process.
Funding
This research was supported by start-up funding from the Research Institute of the McGill University Health Centre (RI-MUHC) awarded to the senior author, J.M. Harley, and a Social Sciences and Humanities Research Council of Canada (SSHRC) doctoral fellowship awarded to the first author, B.T. Ahn.
Author information
Authors and Affiliations
Contributions
B.T.A contributed to conceptualisation and design of the research project, development of search strategy, development of task protocols and data extraction sheet, documentations, article screening, data extraction, data analysis and visualisation, literature review, manuscript writing, hand searching for articles, revisions, and approval for submission. M.M.V contributed to conceptualisation and design of the research project, development of search strategy, development of the data extraction sheet, development of task protocols, article screening, data extraction, file management, and approval for submission. E.B. contributed to the development of data extraction sheet, article screening, hand searching, and approval for submission. A.Y contributed to the development of search strategy, development of the data extraction sheet, article screening, hand searching for articles, and approval for submission. C.H.L contributed to the development of the data extraction sheet, article screening, and approval for submission. H.P contributed to the development of the data extraction sheet, article screening, and approval for submission. K.L. contributed to the development of search strategy, development of the data extraction sheet, article screening, hand searching for articles, file management, and approval for submission. D.C contributed to the development of search strategy, development of the data extraction sheet, article screening, hand searching for articles, file management, and approval for submission. J.M.H contributed to the conceptualisation and design of the research project, development of search strategy, development of task protocols, and data extraction sheet, providing guidance on data analysis, visualisation, literature review, manuscript writing, revision, and submission of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study does not involve human participants or human data, and hence this is not applicable.
Consent for publication
This study does not involve human participants or human data, and hence this is not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix A.
Review Protocol. Appendix B. PRISMA Extension for Scoping Reviews (PRISMA-ScR) Checklist. Appendix C. Data Charting Process. Appendix D. Study characteristics. Figure D1. Articles published by year. Figure D2. Percentage of first (or corresponding) authors’ affiliated institution’s country. Figure D3. Number of articles by specific study design. Figure D4. Number of articles featuring population type. Figure D5. Number of times mood, EI, stress, or emotions featured in the articles. Figure D6. Percentage of articles by combination of constructs featured. Table D1. Types of simulators featured. Appendix E. List of scales featured for measuring emotions.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ahn, B., Maurice-Ventouris, M., Bilgic, E. et al. A scoping review of emotions and related constructs in simulation-based education research articles. Adv Simul 8, 22 (2023). https://doi.org/10.1186/s41077-023-00258-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41077-023-00258-z