
Abstract
Background
Autoregulation has emerged as a potentially beneficial resistance training paradigm to individualize and optimize programming; however, compared to standardized prescription, the effects of autoregulated load and volume prescription on muscular strength and hypertrophy adaptations are unclear. Our objective was to compare the effect of autoregulated load prescription (repetitions in reserve-based rating of perceived exertion and velocity-based training) to standardized load prescription (percentage-based training) on chronic one-repetition maximum (1RM) strength and cross-sectional area (CSA) hypertrophy adaptations in resistance-trained individuals. We also aimed to investigate the effect of volume autoregulation with velocity loss thresholds ≤ 25% compared to > 25% on 1RM strength and CSA hypertrophy.
Methods
This review was performed in accordance with the PRISMA guidelines. A systematic search of MEDLINE, Embase, Scopus, and SPORTDiscus was conducted. Mean differences (MD), 95% confidence intervals (CI), and standardized mean differences (SMD) were calculated. Sub-analyses were performed as applicable.
Results
Fifteen studies were included in the meta-analysis: six studies on load autoregulation and nine studies on volume autoregulation. No significant differences between autoregulated and standardized load prescription were demonstrated for 1RM strength (MD = 2.07, 95% CI – 0.32 to 4.46 kg, p = 0.09, SMD = 0.21). Velocity loss thresholds ≤ 25% demonstrated significantly greater 1RM strength (MD = 2.32, 95% CI 0.33 to 4.31 kg, p = 0.02, SMD = 0.23) and significantly lower CSA hypertrophy (MD = 0.61, 95% CI 0.05 to 1.16 cm2, p = 0.03, SMD = 0.28) than velocity loss thresholds > 25%. No significant differences between velocity loss thresholds > 25% and 20–25% were demonstrated for hypertrophy (MD = 0.36, 95% CI – 0.29 to 1.00 cm2, p = 0.28, SMD = 0.13); however, velocity loss thresholds > 25% demonstrated significantly greater hypertrophy compared to thresholds ≤ 20% (MD = 0.64, 95% CI 0.07 to 1.20 cm2, p = 0.03, SMD = 0.34).
Conclusions
Collectively, autoregulated and standardized load prescription produced similar improvements in strength. When sets and relative intensity were equated, velocity loss thresholds ≤ 25% were superior for promoting strength possibly by minimizing acute neuromuscular fatigue while maximizing chronic neuromuscular adaptations, whereas velocity loss thresholds > 20–25% were superior for promoting hypertrophy by accumulating greater relative volume.
Protocol Registration The original protocol was prospectively registered (CRD42021240506) with the PROSPERO (International Prospective Register of Systematic Reviews).
Similar content being viewed by others


Key Points
-
Autoregulated and standardized load prescription resulted in similar improvements in muscular strength. Subjective (repetitions in reserve-based rating of perceived exertion) and objective (velocity-based training) autoregulated load prescription also demonstrated similar improvements in muscular strength.
-
Velocity loss thresholds ≤ 25% demonstrated significantly greater improvements in muscular strength compared to velocity loss thresholds > 25%; however, this was only evident when exercises in addition to the main resistance training intervention were performed. Velocity loss thresholds > 25% demonstrated significantly greater improvements in muscular hypertrophy compared to velocity loss thresholds ≤ 25%. No significant differences in hypertrophy were demonstrated between velocity loss thresholds of 20–25% and > 25%; however, velocity loss thresholds > 25% demonstrated significantly greater improvements in hypertrophy compared to velocity loss thresholds ≤ 20%.
-
Future research is warranted investigating the chronic effects of autoregulated load and volume prescription with a more precise quantification of proximity to failure and in clinical populations when acute fluctuations in performance and chronic changes in adaptation are most apparent.
Introduction
Background
Resistance training (RT) is the principal modality to increase strength and hypertrophy for improving athletic performance and clinical health [1]. Traditionally, RT has been prescribed based on a pre-determined percentage of one-repetition maximum (1RM), which has been referred to in the scientific literature as standardized percentage-based training (PBT) [2]. There are, however, numerous limitations evident with PBT, the primary being that daily fluctuations [3] and short-term changes [4] in 1RM have been consistently observed [5]; therefore, PBT does not match the acute performance fluctuations and chronic physiological adaptations of each individual [6]. PBT also involves prescribing load based on a single 1RM testing session; thus, if abnormal performance or improper administration were present, the training stimulus applied for the study intervention or successive training cycle may be inappropriate for the intended outcome and may impact other variables (i.e., fatigue, load, volume) in the prescription [5]. Finally, repetitions performed at given intensities are largely lift-specific [7] and highly variable between individuals [8]; therefore, PBT fails to accurately quantify proximity to failure and the degree of neuromuscular fatigue for each individual and lift.
As an alternative approach to PBT, autoregulated RT has gained considerable popularity in recent years due to its theoretical ability to account for an individual’s changes in physiological adaptations and performance parameters [6]. Autoregulation may be defined as a two-step process of measurement and adjustment based on an individual’s acute and chronic fluctuations in performance (i.e., strength), in which performance is comprised of the sum of training (fitness and fatigue) and non-training (readiness) related factors [6]. The two predominant autoregulatory methods involve the systematic manipulation of load and volume via subjective and/or objective strategies [9]. Specifically, subjective load autoregulation involves implementing the repetitions in reserve-based rating of perceived exertion scale (RIR-based RPE scale) in an attempt to quantify proximity to failure, which is commonly referred to as RPE-based training [10]. However, due to the inaccuracy in intra-set RPE predictions [11], objective velocity-based training (VBT) [12] has emerged as a novel load autoregulatory strategy to rectify the limitations of subjective RPE-based training [13] and standardized PBT [14]. VBT load autoregulation involves either prescribing an average concentric velocity (ACV) zone corresponding to the force–velocity continuum [15, 16] or an individualized first repetition average concentric velocity (FRV) corresponding to a specific percentage of 1RM via an individualized load-velocity profile [17,18,19]. Despite the theoretical basis for autoregulated load prescription, the available evidence is conflicting whether it indeed provides an advantage over standardized load prescription for chronic muscular strength and hypertrophy adaptations. Although some studies have demonstrated that autoregulated load prescription may be superior to standardized load prescription for 1RM strength adaptations [15, 20] by enabling load to match the adaptation of the individual throughout a training study (i.e., enable higher relative intensities to be achieved) others have revealed no significant differences [19, 21,22,23].
Similar to subjective load autoregulation, subjective volume autoregulation involves implementing the RPE stop strategy, in which a particular number of sets are prescribed and each set is terminated at a pre-determined subjective RPE [24]. To date, no study has investigated the chronic effects of the RPE stop strategy on muscular strength and hypertrophy. Rather, objective velocity loss has emerged as the predominant strategy of volume autoregulation due to its inherent ability to accurately quantify acute intra-set neuromuscular fatigue [25]. Lower intra-set neuromuscular fatigue (i.e., lower velocity loss thresholds) may be superior for optimizing neuromuscular adaptations such as power output and shifts towards velocity-oriented force–velocity profiles; whereas higher intra-set neuromuscular fatigue (i.e., higher velocity loss thresholds) may be superior for optimizing muscular endurance [26]. The available evidence remains unclear which velocity loss thresholds optimize chronic strength and hypertrophy adaptations [27,28,29,30,31,32,33,34,35,36].
Proximity to failure and neuromuscular fatigue is of paramount importance when considering the design of RT programs [37]. Although training to failure has traditionally been promoted for overload [38, 39], this practice elevates muscle damage and elongates recovery time considerably compared to not training to failure [40]. Importantly, two recent systematic reviews and meta-analyses demonstrated no difference in hypertrophy between training to failure compared to not training to failure when volume was equalized [41, 42]. Similarly, two separate systematic reviews and meta-analyses also demonstrated no difference in hypertrophy between traditional sets compared to alternative set structures when relative intensity and relative volume were equated, which further demonstrates that considerable magnitudes of intra-set fatigue are unnecessary to promote hypertrophy [26, 37]. Despite this, all four systematic reviews and meta-analyses demonstrated no difference in strength adaptations between comparisons [26, 37, 41, 42]; however, appropriately managing the dynamic inter-play amidst proximity to failure and neuromuscular fatigue by integrating load and volume autoregulation strategies may have important practical implications [6, 43]. To illustrate, when sets and repetitions per set are matched, autoregulating set-to-set load to match the individual’s performance by training at closer proximities to failure (i.e., at higher relative intensities) results in significantly greater 1RM strength adaptations [20]. Alternatively, when sets and percentage of 1RM are matched, autoregulating intra-set volume with velocity loss thresholds (i.e., reducing neuromuscular fatigue) also results in significantly greater 1RM strength adaptations [28]. When equated for intra-set fatigue, the time course of recovery is similar regardless of the proximity to failure and relative intensity; however, when proximity to failure is equated, training with greater intra-set fatigue results in greater elevations in indirect measures of muscle damage compared to lower intra-set fatigue [44]. Crucially, excessive acute muscle damage attenuates high-threshold motor unit recruitment and motor skill learning; thus, impairing overall performance, training quality, and skill practice [45]. Chronic neuromuscular fatigue may reduce training frequency, an imperative variable implemented to increase volume and enhance hypertrophy to augment strength adaptations [46]. Overall, the potential practical implications but unclear efficacy of load and volume autoregulation justify the requirement to collate the existing literature and provide a comprehensive synthesis of the evidence.
Objectives
The primary purpose of this review was to determine the chronic effects of load and volume autoregulation on 1RM strength adaptations, with cross-sectional area (CSA) muscle hypertrophy as a secondary outcome. Specifically, systematic and meta-analytic approaches were conducted to investigate the chronic effects of autoregulated compared to standardized load prescription and to investigate the chronic effects of autoregulated volume prescription via velocity loss thresholds ≤ 25% compared to velocity loss thresholds > 25%. It was hypothesized that autoregulated load prescription would result in significantly greater strength adaptations than standardized load prescription; however, no differences in hypertrophy would be observed. It was also hypothesized that velocity loss thresholds ≤ 25% would result in significantly greater strength adaptations, whereas velocity loss thresholds > 25% would result in significantly greater hypertrophy. Moreover, a quality assessment of the studies and limitations of the present autoregulatory methods were identified to suggest avenues for future research. The goal is that this review will provide comprehensive evidence regarding the efficacy of load and volume autoregulation for 1RM strength and CSA hypertrophy adaptations. Ultimately, the dissemination of this information may assist exercise professionals in the systematic individualization of resistance training programming.
Methods
Research Question
A systematic review and meta-analysis were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [47]. The original protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) on April 8, 2021 (Registration number: CRD42021240506). A study intervention length of ≥ 5 weeks was selected because this corresponds to the approximate minimal amount of time required to observe significant hypertrophy with resistance training [48]. For volume autoregulation, a velocity loss threshold of ≤ 25% to > 25% was compared as ~ 20–30% velocity loss corresponds to ~ 50% of the maximal number of repetitions within a set [25] and ~ 25% velocity loss has typically been suggested to optimize 1RM strength adaptations [25, 30,31,32, 36]. The research question was defined using the participants, interventions, comparisons, outcomes, and study design (PICOS) framework:
-
1.
Participants: Apparently healthy individuals with RT experience and no injury or health condition.
-
2.
Interventions: RT interventions (≥ 5 weeks) that employed an autoregulated load prescription or volume autoregulation (≤ 25% velocity loss) protocol.
-
3.
Comparator: RT interventions (≥ 5 weeks) that employed a standardized load prescription or volume autoregulation (> 25% velocity loss) protocol.
-
4.
Outcomes: Muscular strength and/or muscular hypertrophy.
-
5.
Study design: Prospective randomized or non-randomized comparative studies.
Literature Search Strategy
A systematic search of the electronic databases MEDLINE, Embase, Scopus, and SPORTDiscus was performed to identify original research articles up to and including May 25, 2021. The searches had no language or date restrictions. The search strategy involved the following Boolean phrase of combined MeSH terms and keywords; ‘autoregulation’ OR ‘auto-regulation’ OR ‘load autoregulation’ OR ‘volume autoregulation’ OR ‘load prescription’ OR ‘volume prescription’ OR ‘rating of perceived exertion’ OR ‘repetitions in reserve’ OR ‘velocity-based training’ OR ‘velocity based training’ OR ‘velocity loss’ OR ‘absolute velocity’ OR ‘load-velocity profile’ OR ‘load velocity profile’ AND ‘powerlifting’ OR ‘power-lifting’ OR ‘power lifting’ OR ‘weightlifting’ OR ‘weight-lifting’ OR ‘weight lifting’ OR ‘weight-training’ OR ‘weight training’ OR ‘resistance-training’ OR ‘resistance training’ OR ‘resistance-exercise’ OR ‘resistance exercise’ OR ‘strength-training’ OR ‘strength training’ AND ‘one-repetition maximum’ OR ‘one repetition maximum’ OR ‘strength’ OR ‘musc* strength’ OR ‘hypertrophy’ OR ‘musc* hypertrophy’ OR ‘musc* size’ OR ‘musc* thickness’ OR ‘musc* cross-sectional area’.
Study Selection
The Covidence systematic review software (Veritas Health Innovations, Melbourne, Australia) was used to screen titles and abstracts for full-text inclusion. Articles were deduplicated by Covidence and manually screened independently by LMH and KAS. Disagreements were resolved by consensus.
Inclusion Criteria
The inclusion criteria for this review consisted of: (1) randomized or non-randomized comparative studies; (2) training intervention group that employed load or volume autoregulation; (3) strength and/or hypertrophy assessment pre- and post-intervention; (4) apparently healthy individuals with resistance training experience and no injury nor health condition; (5) ≥ 5 week resistance training intervention; (6) ≥ 2 times per week training frequency; (7) detailed description of training intervention including training intensity and training volume; (8) a validated device to measure and monitor velocity (for studies incorporating VBT). All grey literature (i.e., conferences, theses, reports, etc.) were excluded from the review.
Data Extraction
The full texts of all articles that met the inclusion criteria for review were obtained for data extraction. The pre- and post-intervention data were extracted as mean differences (MD) ± standard deviations (SD). LMH extracted the relevant data of interest: (1) study information (study author and publication year); (2) participant characteristics (sample size, sex, age, height, weight, and training status); (3) training characteristics (prescription description, intervention length, training frequency, sets difference, repetitions difference, training volume, and training intensity). The authors of the selected articles were contacted to request any missing relevant information.
Risk of Bias Assessment
The evaluation of risk of bias was performed using the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). LMH and KAS performed the methodological quality assessment independently. Disagreements were resolved by consensus.
Statistical Analysis
All statistical analyses were conducted using RevMan (Version 5.3, Copenhagen, The Nordic Cochrane Centre, The Cochrane Collaboration). A fixed effects model was implemented to analyze the data. The data are reported as MD and 95% confidence intervals (CI). Standardized mean differences (SMD) were also determined to estimate effect sizes. An SMD of 0.20–0.49, 0.50–0.79, and ≥ 0.80 was considered a small, medium, and large effect, respectively. For load autoregulation with respect to 1RM strength outcomes, a positive and negative MD favored autoregulated and standardized load prescription, respectively. For volume autoregulation with respect to 1RM strength outcomes, a positive and negative MD favored velocity loss thresholds ≤ 25% and > 25%, respectively. For volume autoregulation with respect to CSA hypertrophy outcomes, a positive and negative MD favored velocity loss thresholds > 25% and ≤ 25%, respectively. Sub-analyses (i.e., intervention length, training frequency, etc.) and sub-group analyses (i.e., additional vs no additional exercise, etc.) were also performed. Results were considered statistically significant at p ≤ 0.05. The I2 and Chi2 statistics were used to assess heterogeneity. Funnel plots were used to assess publication bias.
Results
Study Selection
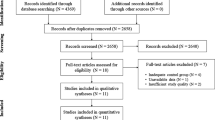
The PRISMA flow diagram outlining the literature search strategy is illustrated in Fig. 1. A total of 1336 studies were identified in the search, 18 of which were included in the systematic review: eight studies on load autoregulation and 10 studies on volume autoregulation. Of those 18 studies, 15 studies were included in the meta-analysis: six studies on load autoregulation and nine studies on volume autoregulation. Specifically, two studies on load autoregulation included in the systematic review were excluded from the meta-analysis; one study compared subjective load autoregulation via RPE-based training to objective load autoregulation via ACV zones [16], while the other study compared objective load autoregulation via group load-velocity profiles to objective load autoregulation via individualized load-velocity profiles [18]. One study on volume autoregulation included in the systematic review was excluded from the meta-analysis as the velocity loss thresholds in the two groups compared were both below 25% velocity loss (5% and 20% velocity loss) [27]. The authors of four studies were contacted to obtain relevant data of interest required to conduct the meta-analysis that were not presented in the published manuscripts. The author of two studies was contacted to obtain the pre- and post-test mean and SD for CSA of the vastus lateralis [31] and pectoralis major [32]. One author was contacted to verify the velocity loss threshold of the training to-repetition-failure group [28]. A final author was contacted to clarify the post-test mean and SD for 1RM of the bench press in the PBT group [21]. All authors responded and supplied the relevant data.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of literature search strategy. n number of studies
Risk of Bias Assessment and Methodological Quality
Detailed summaries outlining the methodological quality of the included studies on autoregulated load and volume prescription are illustrated in Additional file 1: Table S1 and Additional file 2: Table S2, respectively. All studies had some risk of bias. Funnel plots for detecting publication bias of the included studies on load autoregulation for strength, volume autoregulation for strength, and volume autoregulation for hypertrophy are illustrated in Additional file 3: Fig. S1, Additional file 4: Fig. S2, and Additional file 5: Fig. S3, respectively. Visual inspection of the funnel plots indicated no obvious publication bias.
Effect of Autoregulated Versus Standardized Load Prescription on Muscular Strength
Participant Characteristics
A detailed summary outlining the participant characteristics of the included studies on load autoregulation is illustrated in Table 1. A total of 133 participants (autoregulated: n = 64; standardized: n = 69) and 247 comparisons (autoregulated: n = 120; standardized: n = 127) were included in the meta-analysis. Five of the six studies included in the meta-analysis involved exclusively male participants aged 17 ± 1 to 28.3 ± 5.6 years old with ≥ 2 years of resistance-training experience [15, 19,20,21,22], and one study involved exclusively female participants aged 15.8 ± 1.3 years old with ≥ 1 year of resistance-training experience [23].
Training Characteristics
A detailed summary outlining the training characteristics of the included studies on load autoregulation is illustrated in Table 2. The length of the studies ranged from six to 12 weeks with a training frequency of two to three times per week. In all six studies that were included in the meta-analysis, the number of sets were matched, and in four studies, the repetitions were also matched. Outcome measures of interest for strength included 1RM of the back squat (six), bench press (three), deadlift (one), front squat (one), and overhead press (one). Outcome measures of interest for hypertrophy included muscle thickness of the vastus lateralis at 50% (one), vastus lateralis at 70% (one), and pectoralis major (one). A meta-analysis comparing the effect of autoregulated to standardized load prescription on muscular hypertrophy was unable to be conducted as only a single study measured and reported hypertrophy outcomes [21].
Strength Outcomes
Five of the six studies measured muscular strength with a 1RM test [15, 19,20,21,22], while the remaining study estimated 1RM in accordance with the Brzycki [49] prediction equation using a 10RM test [23]. The overall pooled analysis revealed no significant difference for 1RM strength adaptations between autoregulated and standardized load prescription (MD = 2.07, 95% CI – 0.32 to 4.46 kg, p = 0.09, SMD = 0.21) as illustrated in Fig. 2. Specifically, three studies employed subjective load autoregulation [20, 21, 23] and three studies employed objective load autoregulation [15, 19, 22], comprising a total of six outcome measures for each autoregulation type. The sub-analysis revealed near-significance with a small effect favoring autoregulated over standardized load prescription when subjective autoregulation was employed (MD = 3.15, 95% CI – 0.14 to 6.45 kg, p = 0.06, SMD = 0.30), but no meaningful difference when objective autoregulation was employed (MD = 0.88, 95% CI – 2.59 to 4.34 kg, p = 0.62, SMD = 0.10). Despite this finding, the pooled subgroup analysis comparing subjective to objective load autoregulation revealed no significant difference (p = 0.35).

Forest plot for fixed effects meta-analysis of the mean differences in one-repetition maximum strength adaptations comparing autoregulated to standardized load prescription with subgroup analysis comparing subjective to objective autoregulation. CI confidence interval, df degrees of freedom, kg kilograms, SD standard deviation
Sub-analyses are presented in Additional file 6: Table S3. The sub-analysis revealed near-significance with a small effect favoring autoregulated over standardized load prescription when the training intervention was ≥ 8 weeks (p = 0.06, SMD = 0.30), but no significant differences for all other sub-analyses (i.e., when the training intervention was < 8 weeks, when the training frequency was 3 times per week or < 3 times per week, when training volume was controlled or uncontrolled, when relative intensity was greater for autoregulated or the same as standardized load prescription, when lower or upper body exercises were assessed separately, when squat or bench press were assessed separately, or when exercises additional to the resistance training were performed or not performed).
Effect of Volume Autoregulation on Muscular Strength and Hypertrophy
Participant Characteristics
A detailed summary outlining the participant characteristics of the included studies on volume autoregulation is illustrated in Table 3. A total of 308 participants (≤ 25% velocity loss: n = 171; > 25% velocity loss: n = 137) and 457 comparisons (≤ 25% velocity loss: n = 230; > 25% velocity loss: n = 227) were included in the meta-analysis. All studies involved male participants, while one study also involved four female participants. All participants possessed resistance-training experience and the age ranged from 19.4 ± 1.7 to 26.7 ± 5.5 years old.
Training Characteristics
A detailed summary outlining the training characteristics of the included studies on volume autoregulation is illustrated in Table 4. The length of the studies ranged from five to eight weeks with a training frequency of two to three times per week. In all nine studies, the number of sets were matched; however, the total number of repetitions performed varied and increased concomitantly with an increasing velocity loss threshold employed. Outcome measures of interest for strength included 1RM of the back squat (one), bench press (one), deadlift (one), bench row (one), smith machine back squat (five), smith machine bench press (one), weight stack bench press (one), and body mass prone-grip pullup (one). Outcome measures of interest for hypertrophy included CSA of the rectus femoris (one), vastus lateralis (one), vastus lateralis + vastus intermedius (one), vastus medialis (one), and pectoralis major (one).
Strength Outcomes
All nine studies reported our primary outcome measure of muscular strength and employed a 1RM test [28,29,30,31,32,33,34,35,36]. In studies comparing ≥ 3 velocity loss threshold groups, the velocity loss thresholds were separated into their respective groups for comparisons (i.e., ≤ 25% or > 25% velocity loss). Therefore, our overall meta-analysis for strength was comprised of 230 and 227 comparisons for velocity loss thresholds ≤ 25% and > 25%, respectively. The overall pooled analysis revealed a significant difference for 1RM strength adaptations favoring velocity loss thresholds ≤ 25% over velocity loss thresholds > 25% (Fig. 3; p = 0.02, SMD = 0.23). The sub-analysis revealed a significant difference for 1RM strength adaptations favoring velocity loss thresholds ≤ 25% over velocity loss thresholds > 25% when exercise in addition to the resistance training protocol was performed (p = 0.002, SMD = 0.62), but not for when no additional exercise was performed (p = 0.25, SMD = 0.13). Importantly, the pooled subgroup analysis comparing additional exercise to no additional exercise also revealed a significant difference (p = 0.02).

Forest plot for fixed effects meta-analysis of the mean differences in one-repetition maximum strength adaptations comparing ≤ 25% to > 25% velocity loss with subgroup analysis comparing additional to no additional exercise apart from the main comparator resistance training protocol. BMPGP body mass prone-grip pullup, CI confidence interval, df degrees of freedom, kg kilograms, SD standard deviation, SMBP smith machine bench press, SMBS smith machine back squat, TRF to-repetition-failure, VL percentage velocity loss, WSBP weight stack bench press
Sub-analyses are presented in Additional file 7: Table S4. The sub-analysis revealed a significant difference for 1RM strength favoring velocity loss thresholds ≤ 25% over velocity loss thresholds > 25% when the training intervention was 8 weeks (p = 0.009), when training frequency was < 3 times per week (p = 0.009), in lower body exercises (p = 0.007), in the smith machine back squat (p = 0.05), and in free-weight exercises (p = 0.0007), but no meaningful difference when the training intervention was < 8 weeks, when training frequency was 3 times per week, in upper body exercises, in the smith machine / weight stack bench press, or in machine-based exercises. The results from all additional sub-analyses for 1RM strength adaptations comparing each velocity loss threshold and every range iteration from 0–25% compared to > 25% are presented in Additional file 8: Table S5. Significantly greater 1RM strength adaptations were demonstrated for velocity loss thresholds of 10%, 10–25%, 10–20%, 0–20%, and 10–15% compared to velocity loss thresholds > 25%.
Hypertrophy Outcomes
A total of three studies [30,31,32] reported our secondary outcome measure of muscular hypertrophy measured as muscle CSA. Similar to strength outcomes, in studies comparing ≥ 3 velocity loss threshold groups, the velocity loss thresholds were separated into their respective groups for comparisons (i.e., > 25% or ≤ 25% velocity loss). Therefore, our overall meta-analysis for hypertrophy was comprised of 120 and 123 comparisons for velocity loss thresholds > 25% and ≤ 25%, respectively. The overall pooled analysis revealed a significant difference for CSA hypertrophy adaptations favoring velocity loss thresholds > 25% over velocity loss thresholds ≤ 25% (MD = 0.61, 95% CI 0.05 to 1.16 cm2, p = 0.03, SMD = 0.28) as illustrated in Fig. 4. The results from all sub-analyses for CSA hypertrophy adaptations comparing velocity loss thresholds > 25% to each velocity loss threshold and every range iteration from 0–25% are presented in Additional file 9: Table S6. The sub-analysis revealed no significant difference and negligible effects for CSA hypertrophy when comparing velocity loss thresholds > 25% to velocity loss thresholds of 20–25%; however, all additional sub-analyses revealed small-to-moderate effects in favor of > 25%. Significantly greater CSA hypertrophy adaptations were demonstrated for velocity loss thresholds > 25% compared to velocity loss thresholds of 0–20%, 0–15%, 0–10%, and 0%.

Forest plot for fixed effects meta-analysis of the mean differences in cross-sectional area hypertrophy adaptations comparing > 25% to ≤ 25% velocity loss. CI confidence interval, cm centimetres, df degrees of freedom, PM pectoralis major, RF rectus femoris, SD standard deviation, VA vastus lateralis, VI vastus intermedius, VL percentage velocity loss, VM vastus medialis
Discussion
To the authors’ knowledge, this is the first systematic review and meta-analysis to directly investigate the effect of load and volume autoregulation on muscular strength and hypertrophy adaptations. There were similar improvements in 1RM strength between autoregulated and standardized load prescription. Moreover, the subgroup analysis demonstrated no difference in 1RM strength whether subjective or objective autoregulated load prescription was employed. For volume autoregulation, low-moderate velocity loss thresholds (≤ 25%) were optimal for 1RM strength, which was only apparent when studies included exercise outside of the main comparator training protocol. Conversely, moderate-high velocity loss thresholds (> 25%) were optimal for muscle hypertrophy; however, velocity loss thresholds of 20 and 25% stimulate similar improvements in hypertrophy. Collectively, velocity loss thresholds of ~ 20–25% may be optimal for 1RM strength adaptations plausibly by promoting type II phenotype muscle hypertrophy [30], and potentially by maximizing chronic neuromuscular adaptations (i.e., late rate of force development) [32] while minimizing excessive and unnecessary acute neuromuscular fatigue [44]. Appropriate prescription of load and volume autoregulation strategies may enable the stimulus to parallel an individual’s performance and overarching goals of a resistance training program.
Load Autoregulation
Muscular Strength
Overall, there was no significant difference in 1RM strength adaptations between autoregulated and standardized load prescription. Although non-significant, the sub-analysis demonstrated a small effect (SMD = 0.28) for greater 1RM strength when autoregulated load prescription employed a significantly higher relative intensity compared to standardized load prescription. It has been consistently supported that 1RM strength adaptations are primarily driven by high relative intensity training [50, 51], which agrees with the well documented force–velocity relationship (strength-speed continuum) [52, 53]. To illustrate, Graham and Cleather [20] demonstrated that when volume load, sets, and repetitions per set were matched, autoregulating load using RIR-based RPE to utilize a significantly higher relative intensity (percentage of 1RM) than the standardized PBT group resulted in significantly greater 1RM strength in both the back squat and front squat. Therefore, it appears that autoregulated load prescription has the potential to be slightly superior to standardized load prescription for 1RM strength if it enables a greater load (percentage of 1RM) to be utilized while accounting for an individual’s fluctuations and changes in 1RM.
The pooled analysis revealed near-significance (p = 0.06) with a small effect (SMD = 0.30) favoring subjective autoregulated over standardized load prescription; however, objective autoregulated load prescription failed to reveal any differences (p = 0.62; SMD = 0.10). The underlying rationale for these results is plausibly due to the objective autoregulated load prescription groups training at similar relative intensities as the standardized load prescription groups in all three of the objective load autoregulation studies [15, 19, 22]. In contrast, subjective autoregulated load prescription employed a significantly higher relative intensity than standardized load prescription for 50% of the total exercises in the subjective load autoregulation studies [20, 21, 23]. Moreover, an important consideration is that the studies employing subjective load autoregulation [20, 21, 23] were notably longer in duration than the studies employing objective load autoregulation [15, 19, 22]. Therefore, the reason for the marginally greater 1RM strength adaptations observed with subjective load autoregulation is likely twofold: (1) enabling a higher average RPE to be achieved; thus, resulting in a higher relative intensity being employed; and (2) longer training interventions; thus, providing a longer duration for strength adaptations to ensue. Interestingly, the results from this meta-analysis are conflicting with the sole study to date to directly compare subjective versus objective load autoregulation: a 12-week randomized cross-over design by Shattock and Tee [16] revealed that the 1RM strength improvements for objective load autoregulation (VBT) were significantly greater than subjective load autoregulation (RPE) in both the back squat (p = 0.00001; ES: 1.37) and bench press (p = 0.003; ES: 0.98). As the numbers of sets and repetitions per set were matched between groups, the significantly greater 1RM strength improvements following objective load autoregulation were postulated to be due to training at a higher average RPE (higher relative intensity) than the subjective load autoregulation protocol since it has been supported that subjective intra-set RPE ratings tend to be overestimated [11]. Furthermore, evidence has supported that velocity feedback improves competitiveness and motivation to train [54]; ensuring maximal intended concentric velocity, which results in significantly greater 1RM strength compared to half-maximal intended concentric velocity training [55].
Finally, no noteworthy differences in 1RM strength were demonstrated between autoregulated and standardized load prescription when sub-analyses on training frequency, volume differences, exercise type, and additional exercises were conducted. Based on the meta-analytic findings from the present review it appears that autoregulated and standardized load prescription are similarly effective at eliciting considerable improvements in 1RM strength adaptations. These findings may be attributable to the limitations and lack of optimization in the presently employed autoregulatory strategies.
Primary Limitations
RPE-based training often autoregulates load prescription by attempting to standardize the inter-individual proximity to failure [20, 21, 23]; however, it contains a limitation: subjectivity [7, 11]. To illustrate, when participants performed a set to failure at 70% of 1RM in the back squat and verbally indicated when they believed that they were at a 5, 7, and 9 RPE, their actual RPE values were ~ 5, 4, and 2 repetitions below the predicted RPE, respectively [11]. Despite the limitations of RPE-based training, the ability to accurately predict RPE improves from set-to-set and when performed closer to failure [7]; therefore, it may serve as a suitable autoregulatory strategy in certain settings (i.e., clinical).
Banyard et al. [22] and Orange et al. [19] employed individualized load-velocity profiles to prescribe and autoregulate load from set-to-set. Average concentric velocity (ACV) is reliable from session-to-session in the back squat at 20–90% of 1RM [56]; therefore, prescribing an individualized first repetition average concentric velocity (FRV) corresponding to a particular percentage of 1RM from an individualized load-velocity profile is a feasible strategy to dictate and autoregulate relative training load. Specifically, in the study conducted by Banyard et al. [22], if the ACV of all repetitions within a set was ± 0.06 m per second (m.s−1) outside the target ACV corresponding to a particular percentage of 1RM, the load was adjusted by a universal ± 5% of 1RM. However, ACV decreases linearly from repetition-to-repetition as one approaches failure [25]; Morán-Navarro et al. [13] reported that changes in ACV of 0.03 m.s−1 can produce a difference of two RPE in the back squat. As a result, load was seemingly reduced prematurely as evidenced by the VBT group training at similar relative intensities as the PBT group (~ 69 and ~ 71% of 1RM, respectively) [22]. Although a universal load adjustment of ± 5% of 1RM was still prescribed in Orange et al. [19], the load was appropriately adjusted from the FRV (rather than the ACV of all repetitions). Despite this, the intervention simply did not enable adequate progressive overload to observe any significant differences in 1RM strength improvements between the VBT and PBT groups [19]. In one of the most recent load autoregulation studies, individualized set-to-set load adjustments based off the actual percentage of 1RM from the previous set were performed; however, no differences in 1RM strength were reported between individualized and group load-velocity profiles following the 6-week training protocol [18].
An additional velocity-based load autoregulation strategy is the use of ACV zones [15, 16]. Although ACV zones account for specific zones on the force–velocity continuum [52, 53], they can correspond to considerably large ranges of relative intensities and proximities to failure. For example, if 3 sets of 8 repetitions in an ACV zone of 0.60–0.40 m.s−1 are prescribed, some individuals may commence the set at 0.60 m.s−1 and terminate the set at 0.45 m.s−1, while other individuals may commence the set at 0.50 m.s−1 and terminate the set at 0.40 m.s−1. However, Morán-Navarro et al. [13] reported group ACVs of ~ 0.49, 0.45, and 0.40 m.s−1 at a 4, 6, and 8 RPE, respectively during a single set to failure in the back squat. Therefore, terminating the set at an ACV of ~ 0.45 and 0.40 m.s−1 in the back squat is associated with ~ 6 and 8 RPE, respectively [13]; thus, ACV zones also fail to equate for proximity to failure and intra-set neuromuscular fatigue.
Finally, 1RM prediction from individualized regression equations of submaximal ACV may be inaccurate for determining sessional 1RM to prescribe load and autoregulate volume within a training session, or for tracking estimated 1RM to monitor chronic strength improvements across a training intervention [57,58,59]. In theory, the efficacy of 1RM prediction from individualized regression equations of submaximal ACV is predicated upon its ability to accurately predict 1RM, which has lacked consistent support [60,61,62,63,64,65,66,67,68]. These 1RM prediction methods have been purported to accurately predict the actual 1RM for most machine-based exercises [67, 68]; however, they over-predict the actual 1RM for barbell exercises in all [60,61,62,63, 65] but two [64, 66] studies. To summarize, the present load autoregulation strategies likely require further optimization encompassing individualized load adjustments and accurate quantifications of proximity to failure.
Volume Autoregulation
Muscular Strength
Velocity loss thresholds ≤ 25% were superior for increasing 1RM strength over velocity loss thresholds > 25%, which is plausibly attributable to more favorable neuromuscular adaptations [31, 32] and lower neuromuscular fatigue [25, 44]. To better contextualize the overall meta-analytic findings for neuromuscular adaptations contributing to 1RM strength, a recent study conducted by Pareja-Blanco et al. [32] comparing 0, 15, 25, and 50% velocity loss demonstrated that 25% velocity loss resulted in the greatest 1RM strength improvements and was the velocity loss threshold that significantly increased late rate of force development. Crucially, maximizing late rate of force development is the paramount component of the force–time curve to optimize 1RM strength as shifting the force–time curve towards late rate of force development-oriented profiles optimizes the peak absolute force (absolute load) that can be produced [69, 70]. It is important to recognize that when percentage of 1RM and total repetitions are matched, maximizing intra-set force production with alternative set structures does not result in meaningfully different chronic strength adaptations compared to traditional sets as supported in two recent systematic reviews and meta-analyses [26, 37]. Rather, increases in the force component of the force–velocity curve for 1RM strength adaptations are largely contingent upon the load (i.e., percentage of 1RM) employed [50, 51, 71, 72]. Our meta-analytic data suggest that there may be a non-significant dose–response relationship between autoregulated velocity loss and 1RM strength adaptations from zero to ~ 25% velocity loss when training up to ~ 85% of 1RM possibly due to adaptation shifts from early to late rate of force development-oriented profiles [31, 32]. Moreover, velocity loss thresholds exceeding 25% typically result in meaningfully lower 1RM strength adaptations caused by unfavorable neuromuscular adaptations concomitant with counterproductive neuromuscular fatigue.
Velocity loss thresholds ≤ 25% were superior to velocity loss thresholds > 25% for increasing strength when the training intervention was 8 weeks in length, but not when it was < 8 weeks. This supports the contention that the advantages of lower intra-set fatigue for strength development are predominantly a result of chronic neuromuscular adaptations. A recent investigation by Pareja-Blanco et al. [31] demonstrated that 0 and 10% velocity loss significantly decreased vastus medialis muscle displacement, which is an indication of increased muscle stiffness [73, 74]; a property that mediates the force capabilities of skeletal muscle’s contractile elements [75]. Training at 0% velocity loss significantly increased early rate of force development [32], while 40% velocity loss significantly decreased early rate of force development [31]. Moreover, 40% velocity loss significantly increases vastus lateralis delay time [31], which has a positive relationship with myosin heavy chain I adaptations [76]. Rate of force development is a vital component for overcoming the sticking point in compound barbell lifts [77] and the decrease in rate of force development correlates with a decrease in the percentage of type IIX fibers [78, 79]. Importantly, type IIX fibers possess greater cross-bridge cycling rates compared to type I fibers [80] and are essential for enhancing muscle fiber conduction velocity [81]. Although 15% velocity loss elicits high peak muscle excitation [32], which is related to increased neural drive, rate coding, and sarcoplasmic reticulum calcium kinetics [82,83,84,85], training with 15% velocity loss does not change early or late rate of force development [32].
Compared to training with > 25% velocity loss, training with 25, 20, and 10% velocity loss all revealed small effects for increasing 1RM; however, both 15 and 0% velocity loss failed to reveal greater benefits for 1RM strength adaptations. For optimizing 1RM strength, it appears that the velocity loss thresholds may be polarized at 10% and 20–25% up to ~ 85% of 1RM as a viable strategy to minimize neuromuscular fatigue and maximize late rate of force development, respectively [28, 32]. However, upon further inspection of the included studies, it must be noted that the investigation conducted by Held et al. [28] comparing velocity loss thresholds of 10% at ~ 8 RPE to- repetition-failure training at 80% of 1RM in the barbell back squat, bench press, deadlift, bench row, and power clean also involved a high volume of additional exercises every day apart from the resistance training protocol (i.e., 90-min and 120-min of low-intensity rowing and cycling, respectively, on day 6 of the 7-day microcycle). Therefore, due to the possibility that the concurrent endurance training in Held et al. [28] confounded the findings, the sub-analysis comparing a velocity loss threshold of 10% to > 25% with Held et al. [28] excluded failed to reveal a small effect (MD = 1.65, p = 0.32, SMD = 0.16). As 20–25% velocity loss provided the greatest effect (SMD = 0.30), it may be suggested that 0–25% velocity loss with most training allocated at ~ 20–25% (the highest threshold compared to training at ~ 9.5 RPE—failure) is recommended to optimize 1RM strength.
Our pooled analysis revealed that velocity loss thresholds ≤ 25% resulted in significantly greater 1RM strength adaptations than velocity loss thresholds > 25% when additional exercise (beyond resistance training) was performed; however, no differences were observed when no additional exercise was performed. Therefore, it appears that the utility of velocity loss thresholds ≤ 25% for increasing 1RM strength may be most apparent when additional exercise beyond the resistance training protocol is performed (i.e., in-season) to minimize neuromuscular fatigue [28, 44]. Although relative intensity- and relative volume-equated failure training elevates muscle damage and elongates recovery time considerably compared to non-failure training [40], high volume and high velocity loss training results in greater neuromuscular fatigue and delayed recovery compared to high intensity and high RPE training [44, 86, 87]. For example, the counter-movement jump required 48-h to recover following 3 sets at 60% of 1RM with 40% velocity loss (~ 5.5 RPE) in the smith machine back squat; however, it was recovered within 6-h following 3 sets at 80% of 1RM with 20% velocity loss (~ 7 RPE) [86]. Pareja-Blanco et al. [44] also revealed that when set volume and velocity loss was equated (~ 17–23% velocity loss), the counter-movement jump was recovered at 24-h post-intervention regardless of training at a 4, 5, 6, 7, or 8 RPE at 70, 75, 80, 85, and 90% of 1RM in the smith machine back squat, respectively. Notably, Watkins and colleagues [88] investigated the counter-movement jump as an indicator of neuromuscular fatigue and readiness [89]; demonstrating that ~ 8% decrease in counter-movement jump height resulted in a ~ 28% decrease in the number of repetitions performed at 80% of 1RM in the back squat. Upon synthesis of the available evidence, it appears that training at velocity loss thresholds of 0–25% may limit undesirable neuromuscular fatigue; thereby, enabling the utilization of higher percentages of 1RM more frequently to train the high-force component of the force–velocity profile for 1RM strength adaptations.
Muscular Hypertrophy
Training with velocity loss thresholds > 25% resulted in significantly greater muscle hypertrophy than velocity loss thresholds ≤ 25%. This finding is consistent with the literature corroborating that there is a malleable inverted U-curve of optimal training volume for strength [90] and hypertrophy [91,92,93] that is individual-specific [94]. It is important to recognize that although the velocity loss threshold groups within each study were equated for set volume, velocity loss thresholds > 25% were associated with substantially greater total relative volume [30,31,32]. However, two recent systematic reviews and meta-analyses reported no difference in hypertrophy between traditional sets (higher intra-set fatigue) and alternative set structures (lower intra-set fatigue) when total relative volume was equated [26, 37]. Therefore, it appears that the significantly greater hypertrophy observed at > 25% velocity loss in our meta-analysis could be attributable to the greater total relative volume accumulated rather than due to the magnitude of intra-set fatigue (velocity loss threshold) achieved.
Although considerable intra-set fatigue and metabolic stress is unnecessary to stimulate hypertrophy [95], our meta-analysis suggests that a minimal velocity loss threshold of ~ 20–25% may be required to optimize hypertrophy as exemplified by small-to-moderate effects in favor of > 25% velocity loss arising in all sub-analyses including velocity loss thresholds at or below 20%. Despite this, future studies equated for relative volume that report intra-set fatigue with velocity loss and proximity to failure with a precise strategy are required to support or refute this finding and to establish the specific inter-dependent training status, velocity loss, and proximity to failure thresholds to optimize hypertrophy. Upon further inspection of the individual studies included in this meta-analysis, Pareja-Blanco et al. [31] demonstrated that despite no significant difference between 10 and 20% velocity loss in relative volume, number of sets, number of repetitions performed within the set, and percentage of 1RM, and despite training at nearly identical proximities to failure for the entire 8-week intervention (10% velocity loss: ~ 4–7.5 RPE; 20% velocity loss: ~ 4.5–8 RPE), 20% velocity loss elicited more than threefold greater hypertrophy compared to 10% velocity loss. Higher velocity loss thresholds result in elevated metabolite accumulation [25, 96], which has been postulated to amplify the hypertrophic response that is primarily induced from mechanical tension [97]. Consequently, it may be hypothesized that velocity loss thresholds < ~ 20% are inadequate at accumulating sufficient metabolites (i.e., lactate) to assist in augmenting optimal hypertrophic responses [97,98,99]; however, the evidence that lactate modulates anabolic signaling during resistance training in humans is conflicting [100, 101]. It is not entirely clear whether the results of this meta-analysis are due to differences between velocity loss threshold groups for relative volume, intra-set fatigue, or a combination of both.
Velocity loss thresholds of ≤ ~ 25% and > ~ 35% are associated with the preservation and reduction, respectively, of muscle fiber phenotypic characteristics that are favorable for enhancing 1RM strength adaptations [30, 102]. For example, when training at 70–85% of 1RM, 20% velocity loss at ~ 5–8 RPE preserved myosin heavy chain IIX muscle fiber percentage, whereas 40% velocity loss at ~ 9.5 RPE – failure reduced the type IIX fiber pool (i.e., with a conversion to slower fiber types) [30]. This is consistent with the electromyography literature and implies that high-threshold motor units of prime movers are activated initially within a set at ≥ ~ 70% of 1RM in trained individuals [30, 103,104,105]. However, 40% velocity loss increased vastus lateralis and vastus intermedius muscle volume to a significantly greater magnitude, suggesting that motor unit activation of synergists increases as velocity loss increases above ~ 25–35% [30]. It may be argued that hypertrophy should be related to increases in strength as muscle size accounts for ≥ 70% of the variance in strength in trained individuals [106,107,108,109,110,111]. Collectively, it may be suggested that if the primary goal is to increase strength, the majority of training should be performed at ~ 20–25% velocity loss to ensure and optimize hypertrophy while preserving type II muscle fiber phenotypic characteristics. Conversely, if the goal is to increase strength along with hypertrophy, velocity loss thresholds exceeding 25% may be employed; however, performing training at ~ 20–25% velocity loss for compound exercises with accessory exercises that target the synergist musculature may also accomplish this goal. Nonetheless, if increasing strength is of minimal importance, allocating the majority of training at a minimum of ~ 20–25% velocity loss may be recommended to optimize hypertrophy. A periodized approach integrating higher velocity loss initially within a macrocycle and decreasing towards lower velocity loss prior to competition may be employed in athletic programming settings to promote the spectrum of hypertrophy and strength velocity loss-specific adaptations in a sequential order for maximal performance.
Primary Limitations
Although velocity loss can accurately quantify acute intra-set neuromuscular and metabolic fatigue [25], it cannot precisely quantify proximity to failure [112, 113]. For example, in one of the preliminary longitudinal velocity loss studies by Pareja-Blanco et al. [31], a prescription would have been 3 sets at 70% of 1RM with a 20% velocity loss; stipulating that the FRV on each set corresponded to 70% of the individual’s 1RM. However, for example, one individual may have had an FRV of 0.60 m.s−1 at 70% of 1RM; thus, a 20% velocity loss would have terminated the set at an ACV of 0.48 m.s−1, which is associated with ~ 4 RPE [13]. Conversely, another individual may have had an FRV of 0.50 m.s−1 at 70% of 1RM; thus, a 20% velocity loss would have terminated the set at an ACV of 0.40 m.s−1, which is associated with ~ 8 RPE [13]. To further illustrate, a separate investigation by the same researchers reported that the 40% velocity loss group performed ~ 56% of the sets to failure, indicating that 40% velocity loss corresponded to differing intra- and inter-individual proximities to failure [30].
Most importantly, velocity loss is primarily influenced by the number of repetitions performed within the set rather than the proximity to failure (i.e., low velocity loss is not necessarily indicative of low RPE) [25]. For example, if an individual has an ACV corresponding to an 8 RPE of 0.30 m.s−1 and a velocity decay (change in velocity per change in RPE) of 0.04 m.s−1, the velocity loss for 3 and 7 repetitions at an 8 RPE would equate to 21 and 44%, respectively. Moreover, each velocity loss threshold is load- and lift-specific; corresponding to a different proximity to failure depending on the percentage of 1RM and exercise employed [112,113,114]. Furthermore, the inter-individual range in repetitions reported in the back squat at 10, 20, and 30% velocity loss with an FRV of 0.70 m.s−1 was 2–11, 4–19, and 4–24 repetitions, respectively [115]. Therefore, due to the extensive range in repetitions that can be performed at each percentage of 1RM [7, 8] and at each velocity loss threshold [115], as well as the FRV [116], the ACV corresponding to a specific RPE [13], and the individualized velocity decay, each individual will experience varying degrees of fatigue, terminate each set at a different proximity to failure, and perform a different number of repetitions and magnitude of relative volume. Conclusively, an autoregulatory model conceptualizing the overarching results from this meta-analysis may be required to suggest avenues for future research and potential practical applications.
Future Directions and Practical Applications
Although the results from this meta-analysis demonstrated significant differences between velocity loss thresholds ≤ 25% and > 25% for both strength and hypertrophy adaptations, several limitations require further investigation. Future studies should compare different velocity loss thresholds and equate for total relative volume and relative intensity to detect whether the specific adaptations are due to differences in the amount of volume performed, magnitude of intra-set fatigue, or a combination of both. Additionally, future research is also warranted to investigate the chronic effects of load and volume autoregulation in clinical settings when standardized resistance training strategies may be contraindicated [117]. Due to the limitations in which velocity-based load and volume autoregulation strategies have been employed and considering the conflicting findings between this meta-analysis and the sole study to date to directly compare objective to subjective load autoregulation [16], a separate autoregulatory model potentially warrants conceptualization and investigation within autoregulatory contexts. Accordingly, a model integrating individualized last repetition average concentric velocity (LRV) may be a potential autoregulatory model to conceptualize the individual- and lift-specific relationship between LRV, repetitions performed, percentage of 1RM, proximity to failure (RPE), and intra-set fatigue (velocity loss) based on emerging evidence [13, 118, 119].
In practical settings, velocity loss zones from our meta-analysis may be conceptualized contingent upon the primary goal of the individual or training phase within a theoretical model; however, LRVs may be utilized as a prescription strategy within the velocity loss zones to quantify proximity to failure and potentially help rectify the limitations of the present mutually exclusive autoregulatory prescription strategies. From a more holistic programming perspective, a periodized approach whereby higher velocity loss with higher relative volume and lower RPE change over time towards lower velocity loss with higher relative intensity and higher RPE may be recommended. An integrated approach may be a plausible advantageous strategy for optimizing total hypertrophy to potentiate neuromuscular adaptations and limit neuromuscular fatigue for peak performance at the time of primary importance [120]. Perhaps most noteworthy, the efficacy of LRVs and potential model warrants future investigation in: (1) a longitudinal volume autoregulation study comparing LRV stops to RPE stops and velocity loss thresholds; and (2) a longitudinal load autoregulation study comparing LRV-based training to RPE-based training and individualized PBT.
Conclusion
The results of this systematic review and meta-analysis provide novel evidence regarding the effect of autoregulated load and volume prescription on muscular strength and hypertrophy adaptations. Specifically, autoregulated and standardized load prescription demonstrated similar improvements in 1RM strength. Low-moderate velocity loss thresholds of 0–25% (i.e., lower intra-set fatigue) and moderate-high velocity loss thresholds of > 20–25% (i.e., higher intra-set fatigue) produce the greatest improvements in 1RM strength and muscle hypertrophy, respectively. Velocity loss thresholds of ~ 20–25% may optimize 1RM strength adaptations by maximizing favorable chronic hypertrophy adaptations (i.e., type II phenotypic characteristics), chronic neuromuscular adaptations (i.e., late rate of force development), while minimizing unnecessary acute neuromuscular fatigue. Collectively, integrating load and volume autoregulation is a plausible strategy to aid in the systematic individualization of resistance training programming prescriptions, acute responses, chronic adaptations, and performance outcomes.
Availability of Data and Materials
The datasets generated and/or analysed during the current review are available from the corresponding author on reasonable request.
Abbreviations
- ACV:
-
Average concentric velocity
- CI:
-
Confidence interval
- CSA:
-
Cross-sectional area
- ES:
-
Effect size
- FRV:
-
Individualized first repetition average concentric velocity
- LRV:
-
Individualized last repetition average concentric velocity
- MD:
-
Mean difference
- m.s−1 :
-
Metres per second
- PBT:
-
Percentage-based training
- PICOS:
-
Participants, interventions, comparisons, outcomes, and study design
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- RIR-based RPE scale:
-
Repetitions in reserve-based rating of perceived exertion scale
- RoB 2:
-
Revised Cochrane risk-of-bias tool for randomized trials
- RT:
-
Resistance training
- SD:
-
Standard deviation
- SMD:
-
Standardized mean difference
- VBT:
-
Velocity-based training
- 1RM:
-
One-repetition maximum
References
Ratamess NA, Alvar BA, Evetoch TK, Housh TJ, Kibler WB, Kraemer WJ. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687–708. https://doi.org/10.1249/MSS.0b013e3181915670.
Thompson SW, Rogerson D, Ruddock A, Barnes A. The effectiveness of two methods of prescribing load on maximal strength development: a systematic review. Sports Med. 2020;50(5):919–38. https://doi.org/10.1007/s40279-019-01241-3.
Zourdos MC, Dolan C, Quiles JM, Klemp A, Blanco R, Krahwinkel AJ, et al. Efficacy of daily one-repetition maximum squat training in well-trained lifters: three case studies. Med Sci Sports Exerc. 2015;47(5S):940. https://doi.org/10.1249/01.mss.0000479287.40858.b7.
Padulo J, Mignogna P, Mignardi S, Tonni F, D’Ottavio S. Effect of different pushing speeds on bench press. Int J Sports Med. 2012;33(5):376–80. https://doi.org/10.1055/s-0031-1299702.
Helms ER, Cronin J, Storey A, Zourdos MC. Application of the repetitions in reserve-based rating of perceived exertion scale for resistance training. Strength Cond J. 2016;38(4):42–9. https://doi.org/10.1519/ssc.0000000000000218.
Greig L, Stephens Hemingway BH, Aspe RR, Cooper K, Comfort P, Swinton PA. Autoregulation in resistance training: addressing the inconsistencies. Sports Med. 2020. https://doi.org/10.1007/s40279-020-01330-8.
Mansfield SK, Peiffer JJ, Hughes LJ, Scott BR. Estimating repetitions in reserve for resistance exercise: an analysis of factors which impact on prediction accuracy. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003779.
Cooke DM, Haischer MH, Carzoli JP, Bazyler CD, Johnson TK, Varieur R, et al. Body mass and femur length are inversely related to repetitions performed in the back squat in well-trained lifters. J Strength Cond Res. 2019;33(3):890–5. https://doi.org/10.1519/jsc.0000000000003021.
Larsen S, Kristiansen E, van den Tillaar R. Effects of subjective and objective autoregulation methods for intensity and volume on enhancing maximal strength during resistance-training interventions: a systematic review. PeerJ. 2021;9: e10663. https://doi.org/10.7717/peerj.10663.
Zourdos MC, Klemp A, Dolan C, Quiles JM, Schau KA, Jo E, et al. Novel resistance training-specific rating of perceived exertion scale measuring repetitions in reserve. J Strength Cond Res. 2016;30(1):267–75. https://doi.org/10.1519/jsc.0000000000001049.
Zourdos MC, Goldsmith JA, Helms ER, Trepeck C, Halle JL, Mendez KM, et al. Proximity to failure and total repetitions performed in a set influences accuracy of intraset repetitions in reserve-based rating of perceived exertion. J Strength Cond Res. 2019. https://doi.org/10.1519/jsc.0000000000002995.
González-Badillo JJ, Sánchez-Medina L. Movement velocity as a measure of loading intensity in resistance training. Int J Sports Med. 2010;31(5):347–52. https://doi.org/10.1055/s-0030-1248333.
Morán-Navarro R, Martínez-Cava A, Sánchez-Medina L, Mora-Rodríguez R, González-Badillo JJ, Pallarés JG. Movement velocity as a measure of level of effort during resistance exercise. J Strength Cond Res. 2019;33(6):1496–504. https://doi.org/10.1519/jsc.0000000000002017.
Jovanovic M, Flanagan EP. Researched applications of velocity based strength training. J Aust Strength Cond. 2014;22:58–69.
Dorrell HF, Smith MF, Gee TI. Comparison of velocity-based and traditional percentage-based loading methods on maximal strength and power adaptations. J Strength Cond Res. 2020;34(1):46–53. https://doi.org/10.1519/jsc.0000000000003089.
Shattock K, Tee JC. Autoregulation in resistance training: a comparison of subjective versus objective methods. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003530.
Banyard HG, Tufano JJ, Delgado J, Thompson SW, Nosaka K. Comparison of the effects of velocity-based training methods and traditional 1RM-percent-based training prescription on acute kinetic and kinematic variables. Int J Sports Physiol Perform. 2019;14(2):246–55. https://doi.org/10.1123/ijspp.2018-0147.
Dorrell HF, Moore JM, Gee TI. Comparison of individual and group-based load-velocity profiling as a means to dictate training load over a 6-week strength and power intervention. J Sports Sci. 2020;38:1–8. https://doi.org/10.1080/02640414.2020.1767338.
Orange ST, Metcalfe JW, Robinson A, Applegarth MJ, Liefeith A. Effects of in-season velocity- versus percentage-based training in academy rugby league players. Int J Sports Physiol Perform. 2019;15:1–8. https://doi.org/10.1123/ijspp.2019-0058.
Graham T, Cleather DJ. Autoregulation by “repetitions in reserve" leads to greater improvements in strength over a 12-week training program than fixed loading. J Strength Cond Res. 2019. https://doi.org/10.1519/jsc.0000000000003164.
Helms ER, Byrnes RK, Cooke DM, Haischer MH, Carzoli JP, Johnson TK, et al. RPE vs. percentage 1RM loading in periodized programs matched for sets and repetitions. Front Physiol. 2018;9:247. https://doi.org/10.3389/fphys.2018.00247.
Banyard HG, Tufano JJ, Weakley JJS, Wu S, Jukic I, Nosaka K. Superior changes in jump, sprint, and change-of-direction performance but not maximal strength following 6 weeks of velocity-based training compared with 1-repetition-maximum percentage-based training. Int J Sports Physiol Perform. 2020;16:1–11. https://doi.org/10.1123/ijspp.2019-0999.
Arede J, Vaz R, Gonzalo-Skok O, Balsalobre-Fernandéz C, Varela-Olalla D, Madruga-Parera M, et al. Repetitions in reserve vs maximum effort resistance training programs in youth female athletes. J Sports Med Phys Fit. 2020;60(9):1231–9. https://doi.org/10.23736/s0022-4707.20.10907-1.
Helms ER, Cross MR, Brown SR, Storey A, Cronin J, Zourdos MC. Rating of perceived exertion as a method of volume autoregulation within a periodized program. J Strength Cond Res. 2018;32(6):1627–36. https://doi.org/10.1519/jsc.0000000000002032.
Sánchez-Medina L, González-Badillo JJ. Velocity loss as an indicator of neuromuscular fatigue during resistance training. Med Sci Sports Exerc. 2011;43(9):1725–34. https://doi.org/10.1249/MSS.0b013e318213f880.
Jukic I, Van Hooren B, Ramos AG, Helms ER, McGuigan MR, Tufano JJ. The effects of set structure manipulation on chronic adaptations to resistance training: a systematic review and meta-analysis. Sports Med. 2021. https://doi.org/10.1007/s40279-020-01423-4.
Galiano C, Pareja-Blanco F, Hidalgo de Mora J, Sáez de Villarreal E. Low-velocity loss induces similar strength gains to moderate-velocity loss during resistance training. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003487.
Held S, Hecksteden A, Meyer T, Donath L. Improved strength and recovery after velocity-based training: a randomized controlled trial. Int J Sports Physiol Perform. 2021;16:1–9. https://doi.org/10.1123/ijspp.2020-0451.
Pareja-Blanco F, Sánchez-Medina L, Suárez-Arrones L, González-Badillo JJ. Effects of velocity loss during resistance training on performance in professional soccer players. Int J Sports Physiol Perform. 2017;12(4):512–9. https://doi.org/10.1123/ijspp.2016-0170.
Pareja-Blanco F, Rodríguez-Rosell D, Sánchez-Medina L, Sanchis-Moysi J, Dorado C, Mora-Custodio R, et al. Effects of velocity loss during resistance training on athletic performance, strength gains and muscle adaptations. Scand J Med Sci Sports. 2017;27(7):724–35. https://doi.org/10.1111/sms.12678.
Pareja-Blanco F, Alcazar J, Sánchez-Valdepeñas J, Cornejo-Daza PJ, Piqueras-Sanchiz F, Mora-Vela R, et al. Velocity loss as a critical variable determining the adaptations to strength training. Med Sci Sports Exerc. 2020;52(8):1752–62. https://doi.org/10.1249/mss.0000000000002295.
Pareja-Blanco F, Alcazar J, Cornejo-Daza PJ, Sánchez-Valdepeñas J, Rodriguez-Lopez C, Hidalgo-de Mora J, et al. Effects of velocity loss in the bench press exercise on strength gains, neuromuscular adaptations and muscle hypertrophy. Scand J Med Sci Sports. 2020. https://doi.org/10.1111/sms.13775.
Rodiles-Guerrero L, Pareja-Blanco F, León-Prados JA. Effect of velocity loss on strength performance in bench press using a weight stack machine. Int J Sports Med. 2020. https://doi.org/10.1055/a-1179-5849.
Rodríguez-Rosell D, Yáñez-García JM, Mora-Custodio R, Pareja-Blanco F, Ravelo-García AG, Ribas-Serna J, et al. Velocity-based resistance training: impact of velocity loss in the set on neuromuscular performance and hormonal response. Appl Physiol Nutr Metab. 2020;45(8):817–28. https://doi.org/10.1139/apnm-2019-0829.
Rodríguez-Rosell D, Yáñez-García JM, Mora-Custodio R, Sánchez-Medina L, Ribas-Serna J, González-Badillo JJ. Effect of velocity loss during squat training on neuromuscular performance. Scand J Med Sci Sports. 2021. https://doi.org/10.1111/sms.13967.
Sánchez-Moreno M, Cornejo-Daza PJ, González-Badillo JJ, Pareja-Blanco F. Effects of velocity loss during body mass prone-grip pull-up training on strength and endurance performance. J Strength Cond Res. 2020;34(4):911–7. https://doi.org/10.1519/jsc.0000000000003500.
Davies TB, Tran DL, Hogan CM, Haff GG, Latella C. Chronic effects of altering resistance training set configurations using cluster sets: a systematic review and meta-analysis. Sports Med. 2021. https://doi.org/10.1007/s40279-020-01408-3.
Davies T, Orr R, Halaki M, Hackett D. Effect of training leading to repetition failure on muscular strength: a systematic review and meta-analysis. Sports Med. 2016;46(4):487–502. https://doi.org/10.1007/s40279-015-0451-3.
Davies T, Orr R, Halaki M, Hackett D. Erratum to: effect of training leading to repetition failure on muscular strength: a systematic review and meta-analysis. Sports Med. 2016;46(4):605–10. https://doi.org/10.1007/s40279-016-0509-x.
Morán-Navarro R, Pérez CE, Mora-Rodríguez R, de la Cruz-Sánchez E, González-Badillo JJ, Sánchez-Medina L, et al. Time course of recovery following resistance training leading or not to failure. Eur J Appl Physiol. 2017;117(12):2387–99. https://doi.org/10.1007/s00421-017-3725-7.
Vieira AF, Umpierre D, Teodoro JL, Lisboa SC, Baroni BM, Izquierdo M, et al. Effects of resistance training performed to failure or not to failure on muscle strength, hypertrophy, and power output: a systematic review with meta-analysis. J Strength Cond Res. 2021. https://doi.org/10.1519/jsc.0000000000003936.
Grgic J, Schoenfeld B, Orazem J, Sabol F. Effects of resistance training performed to repetition failure or non-failure on muscular strength and hypertrophy: a systematic review and meta-analysis. J Sport Health Sci. 2021. https://doi.org/10.1016/j.jshs.2021.01.007.
Jukic I, Ramos AG, Helms ER, McGuigan MR, Tufano JJ. Acute effects of cluster and rest redistribution set structures on mechanical, metabolic, and perceptual fatigue during and after resistance training: a systematic review and meta-analysis. Sports Med. 2020. https://doi.org/10.1007/s40279-020-01344-2.
Pareja-Blanco F, Rodríguez-Rosell D, Aagaard P, Sánchez-Medina L, Ribas-Serna J, Mora-Custodio R, et al. Time course of recovery from resistance exercise with different set configurations. J Strength Cond Res. 2018. https://doi.org/10.1519/jsc.0000000000002756.
Leite CMF, Profeta V, Chaves SFN, Benine RPC, Bottaro M, Ferreira-Júnior JB. Does exercise-induced muscle damage impair subsequent motor skill learning? Hum Mov Sci. 2019;67: 102504. https://doi.org/10.1016/j.humov.2019.102504.
Grgic J, Schoenfeld BJ, Davies TB, Lazinica B, Krieger JW, Pedisic Z. Effect of resistance training frequency on gains in muscular strength: a systematic review and meta-analysis. Sports Med. 2018;48(5):1207–20. https://doi.org/10.1007/s40279-018-0872-x.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339: b2535. https://doi.org/10.1136/bmj.b2535.
Abe T, DeHoyos DV, Pollock ML, Garzarella L. Time course for strength and muscle thickness changes following upper and lower body resistance training in men and women. Eur J Appl Physiol. 2000;81(3):174–80. https://doi.org/10.1007/s004210050027.
Brzycki M. Strength testing—predicting a one-rep max from reps-to-fatigue. J Phys Educ Recreat Dance. 1993;64(1):88–90. https://doi.org/10.1080/07303084.1993.10606684.
Campos GE, Luecke TJ, Wendeln HK, Toma K, Hagerman FC, Murray TF, et al. Muscular adaptations in response to three different resistance-training regimens: specificity of repetition maximum training zones. Eur J Appl Physiol. 2002;88(1–2):50–60. https://doi.org/10.1007/s00421-002-0681-6.
Schoenfeld BJ, Grgic J, Ogborn D, Krieger JW. Strength and hypertrophy adaptations between low- vs. high-load resistance training: a systematic review and meta-analysis. J Strength Cond Res. 2017;31(12):3508–23. https://doi.org/10.1519/jsc.0000000000002200.
Bottinelli R, Schiaffino S, Reggiani C. Force-velocity relations and myosin heavy chain isoform compositions of skinned fibres from rat skeletal muscle. J Physiol. 1991;437:655–72. https://doi.org/10.1113/jphysiol.1991.sp018617.
Andersen LL, Andersen JL, Magnusson SP, Suetta C, Madsen JL, Christensen LR, et al. Changes in the human muscle force-velocity relationship in response to resistance training and subsequent detraining. J Appl Physiol. 2005;99(1):87–94. https://doi.org/10.1152/japplphysiol.00091.2005.
Weakley JJS, Wilson KM, Till K, Read DB, Darrall-Jones J, Roe GAB, et al. Visual feedback attenuates mean concentric barbell velocity loss and improves motivation, competitiveness, and perceived workload in male adolescent athletes. J Strength Cond Res. 2019;33(9):2420–5. https://doi.org/10.1519/jsc.0000000000002133.
González-Badillo JJ, Rodríguez-Rosell D, Sánchez-Medina L, Gorostiaga EM, Pareja-Blanco F. Maximal intended velocity training induces greater gains in bench press performance than deliberately slower half-velocity training. Eur J Sport Sci. 2014;14(8):772–81. https://doi.org/10.1080/17461391.2014.905987.
Banyard HG, Nosaka K, Vernon AD, Haff GG. The reliability of individualized load-velocity profiles. Int J Sports Physiol Perform. 2018;13(6):763–9. https://doi.org/10.1123/ijspp.2017-0610.
McBurnie AJ, Allen KP, Garry M, Martin M, Thomas DS, Jones PA, et al. The benefits and limitations of predicting one repetition maximum using the load-velocity relationship. Strength Cond J. 2019;41(6):28–40. https://doi.org/10.1519/ssc.0000000000000496.
Nevin J. Autoregulated resistance training: does velocity-based training represent the future? Strength Cond J. 2019;41(4):34–9. https://doi.org/10.1519/ssc.0000000000000471.
Weakley J, Mann B, Banyard H, McLaren S, Scott T, Garcia-Ramos A. Velocity-based training: from theory to application. Strength Cond J. 2020. https://doi.org/10.1519/ssc.0000000000000560.
Banyard HG, Nosaka K, Haff GG. Reliability and validity of the load-velocity relationship to predict the 1RM back squat. J Strength Cond Res. 2017;31(7):1897–904. https://doi.org/10.1519/jsc.0000000000001657.
Hughes LJ, Banyard HG, Dempsey AR, Scott BR. Using a load-velocity relationship to predict one repetition maximum in free-weight exercise: a comparison of the different methods. J Strength Cond Res. 2019;33(9):2409–19. https://doi.org/10.1519/jsc.0000000000002550.
Ruf L, Chéry C, Taylor KL. Validity and reliability of the load-velocity relationship to predict the one-repetition maximum in deadlift. J Strength Cond Res. 2018;32(3):681–9. https://doi.org/10.1519/jsc.0000000000002369.
Benavides-Ubric A, Dìez-Fernandez DM, Rodriguez-Perez M, Ortega-Becerra M, Pareja-Blanco F. Analysis of the load-velocity relationship in deadlift exercise. J Sport Sci Med. 2020;9:452–9.
Jukic I, García-Ramos A, Malecek J, Omcirk D, Tufano JJ. Validity of load-velocity relationship to predict 1 repetition maximum during deadlifts performed with and without lifting straps: the accuracy of six prediction models. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003596.
Williams TD, Esco MR, Fedewa MV, Bishop PA. Bench press load-velocity profiles and strength after overload and taper microcyles in male powerlifters. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003835.
Jiménez-Alonso A, García-Ramos A, Cepero M, Miras-Moreno S, Rojas FJ, Pérez-Castilla A. Velocity performance feedback during the free-weight bench press testing procedure: an effective strategy to increase the reliability and one repetition maximum accuracy prediction. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003609.
García-Ramos A, Haff GG, Pestaña-Melero FL, Pérez-Castilla A, Rojas FJ, Balsalobre-Fernández C, et al. Feasibility of the 2-point method for determining the 1-repetition maximum in the bench press exercise. Int J Sports Physiol Perform. 2018;13(4):474–81. https://doi.org/10.1123/ijspp.2017-0374.
Pérez-Castilla A, Suzovic D, Domanovic A, Fernandes JFT, García-Ramos A. Validity of different velocity-based methods and repetitions-to-failure equations for predicting the 1 repetition maximum during 2 upper-body pulling exercises. J Strength Cond Res. 2019. https://doi.org/10.1519/jsc.0000000000003076.
Turner A, Comfort P, McMahon J, Bishop C, Chavda S, Read P, et al. Developing powerful athletes, part 1: mechanical underpinnings. Strength Cond J. 2020;42:1. https://doi.org/10.1519/SSC.0000000000000543.
Turner AN, Comfort P, McMahon J, Bishop C, Chavda S, Read P, et al. Developing powerful athletes part 2: practical applications. Strength Cond J. 2021;43(1):23–31. https://doi.org/10.1519/ssc.0000000000000544.
Behm DG, Sale DG. Velocity specificity of resistance training. Sports Med. 1993;15(6):374–88. https://doi.org/10.2165/00007256-199315060-00003.
Coyle EF, Feiring DC, Rotkis TC, Cote RW, Roby FB, Lee W, et al. Specificity of power improvements through slow and fast isokinetic training. J Appl Physiol Respir Environ Exerc Physiol. 1981;51(6):1437–42. https://doi.org/10.1152/jappl.1981.51.6.1437.
Macgregor LJ, Hunter AM, Orizio C, Fairweather MM, Ditroilo M. Assessment of skeletal muscle contractile properties by radial displacement: the case for tensiomyography. Sports Med. 2018;48(7):1607–20. https://doi.org/10.1007/s40279-018-0912-6.
Pisot R, Narici MV, Simunic B, De Boer M, Seynnes O, Jurdana M, et al. Whole muscle contractile parameters and thickness loss during 35-day bed rest. Eur J Appl Physiol. 2008;104(2):409–14. https://doi.org/10.1007/s00421-008-0698-6.
Wilson GJ, Murphy AJ, Pryor JF. Musculotendinous stiffness: its relationship to eccentric, isometric, and concentric performance. J Appl Physiol. 1994;76(6):2714–9. https://doi.org/10.1152/jappl.1994.76.6.2714.
Simunič B, Degens H, Rittweger J, Narici M, Mekjavić IB, Pišot R. Noninvasive estimation of myosin heavy chain composition in human skeletal muscle. Med Sci Sports Exerc. 2011;43(9):1619–25. https://doi.org/10.1249/MSS.0b013e31821522d0.
Kompf J, Arandjelović O. The sticking point in the bench press, the squat, and the deadlift: similarities and differences, and their significance for research and practice. Sports Med. 2017;47(4):631–40. https://doi.org/10.1007/s40279-016-0615-9.
Andersen LL, Andersen JL, Zebis MK, Aagaard P. Early and late rate of force development: differential adaptive responses to resistance training? Scand J Med Sci Sports. 2010;20(1):e162–9. https://doi.org/10.1111/j.1600-0838.2009.00933.x.
Hvid L, Aagaard P, Justesen L, Bayer ML, Andersen JL, Ørtenblad N, et al. Effects of aging on muscle mechanical function and muscle fiber morphology during short-term immobilization and subsequent retraining. J Appl Physiol. 2010;109(6):1628–34. https://doi.org/10.1152/japplphysiol.00637.2010.
Bottinelli R, Canepari M, Pellegrino MA, Reggiani C. Force-velocity properties of human skeletal muscle fibres: myosin heavy chain isoform and temperature dependence. J Physiol. 1996;495(Pt 2):573–86. https://doi.org/10.1113/jphysiol.1996.sp021617.
Methenitis S, Karandreas N, Spengos K, Zaras N, Stasinaki AN, Terzis G. Muscle fiber conduction velocity, muscle fiber composition, and power performance. Med Sci Sports Exerc. 2016;48(9):1761–71. https://doi.org/10.1249/mss.0000000000000954.
Gabriel DA, Kamen G, Frost G. Neural adaptations to resistive exercise: mechanisms and recommendations for training practices. Sports Med. 2006;36(2):133–49. https://doi.org/10.2165/00007256-200636020-00004.
Folland JP, Williams AG. The adaptations to strength training: morphological and neurological contributions to increased strength. Sports Med. 2007;37(2):145–68. https://doi.org/10.2165/00007256-200737020-00004.
Semmler JG. Motor unit synchronization and neuromuscular performance. Exerc Sport Sci Rev. 2002;30(1):8–14. https://doi.org/10.1097/00003677-200201000-00003.
Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol. 2002;93(4):1318–26. https://doi.org/10.1152/japplphysiol.00283.2002.
Pareja-Blanco F, Villalba-Fernández A, Cornejo-Daza PJ, Sánchez-Valdepeñas J, González-Badillo JJ. Time course of recovery following resistance exercise with different loading magnitudes and velocity loss in the set. Sports (Basel). 2019;7(3):59. https://doi.org/10.3390/sports7030059.
Bartolomei S, Sadres E, Church DD, Arroyo E, Gordon JAI, Varanoske AN, et al. Comparison of the recovery response from high-intensity and high-volume resistance exercise in trained men. Eur J Appl Physiol. 2017;117(7):1287–98. https://doi.org/10.1007/s00421-017-3598-9.
Watkins CM, Barillas SR, Wong MA, Archer DC, Dobbs IJ, Lockie RG, et al. Determination of vertical jump as a measure of neuromuscular readiness and fatigue. J Strength Cond Res. 2017;31(12):3305–10. https://doi.org/10.1519/jsc.0000000000002231.
Claudino JG, Cronin J, Mezêncio B, McMaster DT, McGuigan M, Tricoli V, et al. The countermovement jump to monitor neuromuscular status: a meta-analysis. J Sci Med Sport. 2017;20(4):397–402. https://doi.org/10.1016/j.jsams.2016.08.011.
Krieger JW. Single versus multiple sets of resistance exercise: a meta-regression. J Strength Cond Res. 2009;23(6):1890–901. https://doi.org/10.1519/JSC.0b013e3181b370be.
Schoenfeld BJ, Ogborn D, Krieger JW. Dose-response relationship between weekly resistance training volume and increases in muscle mass: a systematic review and meta-analysis. J Sports Sci. 2017;35(11):1073–82. https://doi.org/10.1080/02640414.2016.1210197.
Krieger JW. Single vs. multiple sets of resistance exercise for muscle hypertrophy: a meta-analysis. J Strength Cond Res. 2010;24(4):1150–9. https://doi.org/10.1519/JSC.0b013e3181d4d436.
Figueiredo VC, de Salles BF, Trajano GS. Volume for muscle hypertrophy and health outcomes: the most effective variable in resistance training. Sports Med. 2018;48(3):499–505. https://doi.org/10.1007/s40279-017-0793-0.
Scarpelli MC, Nóbrega SR, Santanielo N, Alvarez IF, Otoboni GB, Ugrinowitsch C, et al. Muscle hypertrophy response is affected by previous resistance training volume in trained individuals. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003558.
Dankel SJ, Mattocks KT, Jessee MB, Buckner SL, Mouser JG, Loenneke JP. Do metabolites that are produced during resistance exercise enhance muscle hypertrophy? Eur J Appl Physiol. 2017;117(11):2125–35. https://doi.org/10.1007/s00421-017-3690-1.
Weakley J, McLaren S, Ramirez-Lopez C, García-Ramos A, Dalton-Barron N, Banyard H, et al. Application of velocity loss thresholds during free-weight resistance training: responses and reproducibility of perceptual, metabolic, and neuromuscular outcomes. J Sports Sci. 2019;38:1–9. https://doi.org/10.1080/02640414.2019.1706831.
Schoenfeld BJ. The mechanisms of muscle hypertrophy and their application to resistance training. J Strength Cond Res. 2010;24(10):2857–72. https://doi.org/10.1519/JSC.0b013e3181e840f3.
Wackerhage H, Schoenfeld BJ, Hamilton DL, Lehti M, Hulmi JJ. Stimuli and sensors that initiate skeletal muscle hypertrophy following resistance exercise. J Appl Physiol. 2019;126(1):30–43. https://doi.org/10.1152/japplphysiol.00685.2018.
Morton RW, Oikawa SY, Wavell CG, Mazara N, McGlory C, Quadrilatero J, et al. Neither load nor systemic hormones determine resistance training-mediated hypertrophy or strength gains in resistance-trained young men. J Appl Physiol. 2016;121(1):129–38. https://doi.org/10.1152/japplphysiol.00154.2016.
Liegnell R, Apró W, Danielsson S, Ekblom B, van Hall G, Holmberg HC, et al. Elevated plasma lactate levels via exogenous lactate infusion do not alter resistance exercise-induced signaling or protein synthesis in human skeletal muscle. Am J Physiol Endocrinol Metab. 2020;319(4):E792-e804. https://doi.org/10.1152/ajpendo.00291.2020.
Cerda-Kohler H, Henríquez-Olguín C, Casas M, Jensen TE, Llanos P, Jaimovich E. Lactate administration activates the ERK1/2, mTORC1, and AMPK pathways differentially according to skeletal muscle type in mouse. Physiol Rep. 2018;6(18): e13800. https://doi.org/10.14814/phy2.13800.
Martinez-Canton M, Gallego-Selles A, Gelabert-Rebato M, Martin-Rincon M, Pareja-Blanco F, Rodriguez-Rosell D, et al. Role of CaMKII and sarcolipin in muscle adaptations to strength training with different levels of fatigue in the set. Scand J Med Sci Sports. 2021;31(1):91–103. https://doi.org/10.1111/sms.13828.
van den Tillaar R, Andersen V, Saeterbakken AH. Comparison of muscle activation and kinematics during free-weight back squats with different loads. PLoS ONE. 2019;14(5): e0217044. https://doi.org/10.1371/journal.pone.0217044.
McBride JM, Larkin TR, Dayne AM, Haines TL, Kirby TJ. Effect of absolute and relative loading on muscle activity during stable and unstable squatting. Int J Sports Physiol Perform. 2010;5(2):177–83. https://doi.org/10.1123/ijspp.5.2.177.
Król H, Gołaś A. Effect of barbell weight on the structure of the flat bench press. J Strength Cond Res. 2017;31(5):1321–37. https://doi.org/10.1519/jsc.0000000000001816.
Taber CB, Vigotsky A, Nuckols G, Haun CT. Exercise-induced myofibrillar hypertrophy is a contributory cause of gains in muscle strength. Sports Med. 2019;49(7):993–7. https://doi.org/10.1007/s40279-019-01107-8.
Siahkouhian M, Hedayatneja M. Correlations of anthropometric and body composition variables with the performance of young elite weightlifters. J Hum Kinet. 2010. https://doi.org/10.2478/v10078-010-0040-3.
Blazevich AJ, Coleman DR, Horne S, Cannavan D. Anatomical predictors of maximum isometric and concentric knee extensor moment. Eur J Appl Physiol. 2009;105(6):869–78. https://doi.org/10.1007/s00421-008-0972-7.
Trezise J, Collier N, Blazevich AJ. Anatomical and neuromuscular variables strongly predict maximum knee extension torque in healthy men. Eur J Appl Physiol. 2016;116(6):1159–77. https://doi.org/10.1007/s00421-016-3352-8.
Lietzke MH. Relation between weightlifting totals and body weight. Science. 1956;124(3220):486–7. https://doi.org/10.1126/science.124.3220.486.
Brechue WF, Abe T. The role of FFM accumulation and skeletal muscle architecture in powerlifting performance. Eur J Appl Physiol. 2002;86(4):327–36. https://doi.org/10.1007/s00421-001-0543-7.
Rodríguez-Rosell D, Yáñez-García JM, Sánchez-Medina L, Mora-Custodio R, González-Badillo JJ. Relationship between velocity loss and repetitions in reserve in the bench press and back squat exercises. J Strength Cond Res. 2019. https://doi.org/10.1519/jsc.0000000000002881.
Beck M, Varner W, LeVault L, Boring J, Fahs CA. Decline in unintentional lifting velocity is both load and exercise specific. J Strength Cond Res. 2020. https://doi.org/10.1519/jsc.0000000000003786.
Izquierdo M, González-Badillo JJ, Häkkinen K, Ibáñez J, Kraemer WJ, Altadill A, et al. Effect of loading on unintentional lifting velocity declines during single sets of repetitions to failure during upper and lower extremity muscle actions. Int J Sports Med. 2006;27(9):718–24. https://doi.org/10.1055/s-2005-872825.
Weakley J, Ramirez-Lopez C, McLaren S, Dalton-Barron N, Weaving D, Jones B, et al. The effects of 10%, 20%, and 30% velocity loss thresholds on kinetic, kinematic, and repetition characteristics during the barbell back squat. Int J Sports Physiol Perform. 2019;15:1–9. https://doi.org/10.1123/ijspp.2018-1008.
Fahs CA, Blumkaitis JC, Rossow LM. Factors related to average concentric velocity of four barbell exercises at various loads. J Strength Cond Res. 2019;33(3):597–605. https://doi.org/10.1519/jsc.0000000000003043.
Fairman CM, Zourdos MC, Helms ER, Focht BC. A scientific rationale to improve resistance training prescription in exercise oncology. Sports Med. 2017;47(8):1457–65. https://doi.org/10.1007/s40279-017-0673-7.
Odgers JB, Zourdos MC, Helms ER, Candow DG, Dahlstrom B, Bruno P, et al. Rating of perceived exertion and velocity relationships among trained males and females in the front squat and hexagonal bar deadlift. J Strength Cond Res. 2021;35(Suppl 1):S23-s30. https://doi.org/10.1519/jsc.0000000000003905.
Helms ER, Storey A, Cross MR, Brown SR, Lenetsky S, Ramsay H, et al. RPE and velocity relationships for the back squat, bench press, and deadlift in powerlifters. J Strength Cond Res. 2017;31(2):292–7. https://doi.org/10.1519/jsc.0000000000001517.
Williams TD, Tolusso DV, Fedewa MV, Esco MR. Comparison of periodized and non-periodized resistance training on maximal strength: a meta-analysis. Sports Med. 2017;47(10):2083–100. https://doi.org/10.1007/s40279-017-0734-y.
Acknowledgements
Not applicable.
Funding
No sources of funding were used to assist in the preparation of this article.
Author information
Authors and Affiliations
Contributions
LMH conceptualized the manuscript, performed the systematic review and meta-analysis, and wrote the first and final version of the manuscript. PDC, KAS, and SJB assisted with the systematic review and meta-analysis. All authors edited and revised the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing Interests
Landyn M. Hickmott, Philip D. Chilibeck, Keely A. Shaw, and Scotty J. Butcher declare that they have no potential competing interests relevant to the content of this review.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Methodological quality of included studies on load autoregulation.
Additional file 2: Table S2.
Methodological quality of included studies on volume autoregulation.
Additional file 3: Fig. S1.
Funnel plot for fixed effects meta-analysis of the mean differences in one-repetition maximum strength adaptations comparing autoregulated to standardized load prescription with subgroup analysis comparing subjective to objective autoregulation. MD mean difference, SE standard error.
Additional file 4: Fig. S2.
Funnel plot for fixed effects meta-analysis of the mean differences in one-repetition maximum strength adaptations comparing ≤ 25% to > 25% velocity loss with subgroup analysis comparing additional to no additional exercise apart from the main comparator resistance training protocol. MD mean difference, SE standard error.
Additional file 5: Fig. S3.
Funnel plot for fixed effects meta-analysis of the mean differences in cross-sectional area hypertrophy adaptations comparing > 25% to ≤ 25% velocity loss. MD mean difference, SE standard error.
Additional file 6: Table S3.
Results from sub-analyses for 1RM strength between autoregulated and standardized load prescription.
Additional file 7: Table S4.
Results from sub-analyses for 1RM strength between ≤ 25% velocity loss and > 25% velocity loss.
Additional file 8: Table S5.
Results from sub-analyses for 1RM strength between respective velocity loss and > 25% velocity loss.
Additional file 9: Table S6.
Results from sub-analyses for CSA hypertrophy between > 25% velocity loss and respective velocity loss.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hickmott, L.M., Chilibeck, P.D., Shaw, K.A. et al. The Effect of Load and Volume Autoregulation on Muscular Strength and Hypertrophy: A Systematic Review and Meta-Analysis. Sports Med - Open 8, 9 (2022). https://doi.org/10.1186/s40798-021-00404-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-021-00404-9