
Abstract
This review discusses the effects of short-chain fatty acids (SCFAs) and trimethylamine-N-oxide (TMAO) on metabolic diseases, focusing on non-alcoholic fatty liver disease (NAFLD) and cardiovascular disease, and suggests dietary modification as a promising therapeutic strategy. SCFAs, a product of fiber fermentation by microbiota, foster intestinal cell populations, upregulate mucin production, and secure the gut barrier. In contrast, TMAO, a microbiota-produced metabolite from choline, phosphatidylcholine, and l-carnitine, induces atherosclerosis by decreasing cholesterol clearance. An unmanageable abundance of TMAO is potentially harmful to patients with NAFLD owing to its ability to regulate the synthesis and transport of bile acids. The production of SCFAs and TMAO is strongly dependent on the microbial community; therefore, dietary modifications, such as reduction in meat intake, and prebiotic and probiotic consumption that can shape the gut microbiome are considered as promissing therapeutic approaches. This review focuses on well-known prebiotics, such as inulin, fructooligosaccharides, and β-glucan, and probiotics, such as VSL#3 mixture, Lactobacillus rhamnosus GG, Bifidobacterium, and Lactobacillus spp. These additives facilitate microbiota modification, gut homeostasis, intestinal barrier maintenance, and promotion of cholesterol excretion, which may protect the liver from steatosis, inflammation, and fibrosis. Controversial results from previous studies suggest that personalized approaches should be used for dietary modifications.
Similar content being viewed by others


Non-alcoholic fatty liver disease and non-alcoholic steatohepatitis
Over the past century, excessive growth of the fast-food industry and predominance of automatic devices have resulted in sedentary lifestyles and unbalanced energy consumption, which are the crucial causes of metabolic disorders, such as obesity and diabetes. In addition, non-alcoholic fatty liver disease (NAFLD) and its progressive stage, non-alcoholic steatohepatitis (NASH) are the most important consequences of such disorders, as 30% and 3–6% of US citizens suffer from NAFLD and NASH, respectively, and 20% of total cases of NASH progress to cirrhosis, which increases the mortality rate or leads to liver transplantation [1]. Although there are some available non-invasive tests, including blood and urine analysis for liver damage markers, such as aspartate aminotransferase (AST) and alanine aminotransferase (ALP), only liver biopsy is accepted as reliable diagnosis to differentiate NASH from simple steatosis [1]. NAFLD is confirmed by the presence of more than 5% hepatic steatosis, and NASH is diagnosed by the simultaneous occurrence of hepatocyte ballooning degeneration and lobular inflammation (neutrophil invasion) with steatosis [2]. Notably, 4% of simple steatosis and 20% of NASH cases finally develop cirrhosis with fibrosis-including NASH as the intermediary stage [3]. No therapy has been officially approved by the US Food and Drug Administration, and controlled lifestyle, including dietary management and exercise, is recommended for patients with a low-grade condition [1]. The imbalance of energy intake, together with the disruption in energy and nutrition metabolism, are the main causes of NAFLD. Excessive and continuous consumption of saturated fatty acids (SFAs) induces liver fat accumulation with NAFLD as the ultimate consequence, while moderate unsaturated fat consumptions shows protective effects [4]. A recent study suggests that SFAs can be associated with liver steatosis by changing the structure and function of mitochondria, which ultimately disrupts the respiratory transport, produces reactive oxygen species, and damages the neighboring structures, causing apoptosis, inflammation, and scarring in the liver [4]. Besides unhealthy intake of SFAs, steatosis can be observed as a hepatic manifestation during inflammatory bowel disease (IBD), suggesting an intimate relationship between the gastrointestinal tract and liver condition [5, 6]. During IBD, the intestinal barrier is disrupted, leading to increased gut permeability and uncontrolled transport of lipopolysaccharide (LPS) to the liver via the portal vein [5, 6]. As a result of aforementioned endotoxin transport, hepatocytes are damaged and macrophages infiltrate into the liver and can lead to liver inflammation [5].
Short-Chain fatty acids
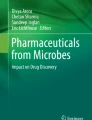
Gut microbiota plays an important role in maintaining gut homeostasis and is essential for regulating the gut and liver axes [6]. A healthy population of microbiota consolidates the intestinal barrier and helps to maintain gut homeostasis by interacting with intestinal cells and the immune system [5, 7]. Short-chain fatty acids (SCFAs) are important products of fiber fermentation by microbiota that are known to have diverse benefits on gut-liver axes (Fig. 1). SCFAs help to secure the intestinal barrier by increasing the expression levels of tight junction proteins, such as zonula occludens-1, claudin, occludin, and E-cadherin that limits intestinal permeability and reduces the transportation of endotoxin to the liver in IBD [5]. In addition, butyrate, one of the SCFAs, is mainly utilized by intestinal epithelial cells such as enterocytes and goblet cells to proliferate and secrete lubricating mucin [5, 8]. Besides that, SCFAs increase the protein expression levels of glucagon-like peptide-1 (GLP-1) in enteroendocrine cells, improving glucose tolerance in both cell and animal models [9]. Consistent with this, Weitkunat et al. [10] demonstrated that acetate and propionate ameliorate high-fat diet (HFD)-induced insulin insensitivity and hepatic triglyceride (TG) accumulation [10]. In addition, propionate is known to specifically enhances GLP-1 levels and decreases fat accumulation in the liver by hindering triglyceride synthesis [11]. Moreover, propionate could also regulate cellular lipid metabolism via the its effect in the modulation of fasting-induced adipose factor, protein-coupled receptor 43, and histone deacetylases [12]. In a co-culture system with epithelial cells, hepatocyte-like cells show an increase in glycogen synthesis and storage following propionate treatment [13]. GLP-1 receptor expression levels are downregulated in patients with NAFLD and animal models, but treatment with butyrate can reverse this effect and induce phosphorylation of hepatic AMP-activated protein kinase (AMPK) and insulin receptor [14]. Besides butyrate, propionate is also known about its capacity in increasing the phosphorylation of AMPK and limiting a number of transcriptional factors which control the expression of gluconeogenesis enzymes like glucose-6-phosphatase and phosphoenolpyruvate carboxykinase [15]. SCFAs are also known about their capacity in immunoregulation and immunity enhancement. It is stated that the immunity is enhanced by SCFAs to extracellular bacteria (C. rodentium and C. difficile), viruses (influenza and respiratory viruses), and intracellular pathogens (Listeria monocytogenes and Salmonella typhimurium) [16,17,18,19]. Moreover, SCFAs also ameliorated chronic colitis and the development of inflammation-associated colon cancer [20, 21]. SCFAs can also be carried to the liver, where they exert beneficial effects by regulating steatosis and inflammation, as proven in both in vitro and in vivo experiments [22]. Butyrate also decreases the expression levels of tumor necrosis factor-α and increases the levels of prostaglandin E2 in a myeloid subset consisting of hepatic and Kupffer cells, suggesting the immunoregulatory and anti-inflammatory capacity of butyrate [23, 24]. Finally, there are various cell types consisting of tissue cells (epithelial cells and myeloid cells) and immune cells (T cells, B cells, and innate lymphoid cells) that take part in inducing the protective effect of SCFAs [25].

Beneficial effect of SCFAs on Gut–liver axis. There is a close relationship between the liver and the gut. Humans consume food that is digested and metabolized by microbiota in the gut to produce essential metabolites, such as trimethylamine (TMA), amino acids, and fatty acids, which are transported to the liver via portal veins. Since different microbiota results in distinct products of digestion that will be transported to the liver, healthy gut microbiota is essential for a healthy liver. Diet modification and additives (prebiotics and probiotics) consumption are promising approaches to have a healthy microbiota community. SCFAs are products of the beneficial bacterial community which have various benefits toward the host consisting of improving overall metabolism, strengthening intestinal epithelium, and regulating immune response
Effects of trimethylamine N-oxide on cardiovascular disease and NAFLD
According to mentioned results, it is clear that the gut has a substantial impact on the liver. On the other hand, the liver can regulate the microbiota population via secretion of bile acids (BA), potent antimicrobials [26]. Since the late 1940, BAs have been known about their impact on susceptible bacteria such genera as Staphylococcus, Balantidium, Pneumococcus, Enterococcus, and members of the phylum Spirochaetes in both bacteriostatic and bactericidal fashion [26]. Primary BAs could dose dependently disrupt bacterial membranes and non-conjugated BAs could induce a more vigorous reduction in viability than their conjugated counterparts against Staphylococcus aureus, several Lactobacillus and Bifidobacterium species [26]. Later on, the secondary BA is transported back to the liver, together with other substrates, such as amino acids, glucose, free fatty acids (FFAs), and trimethylamine (TMA), with the production of TMA is strongly depend on gut microbiota. FFAs and TMA are accumulated and metabolized in the liver into trimethylamine N-oxide (TMAO) by flavin-containing monooxygenases, and high levels of urinary and plasma TMAO are strongly associated with insulin resistance, NAFLD, and cardiovascular disease (CVD) [27, 28]. For decades, TMA was known as a microbiota-dependent metabolite of choline and phosphatidylcholine, until Koeth et al. [29] demonstrated that TMA is also a product of gut flora-metabolized l-carnitine in red meat [28, 29]. Importantly, the authors pointed out that the gut microbes from omnivorous participants may support a higher production of TMAO than that from participants who consume a vegan diet, emphasizing the norm that dietary habits shape the microbiome [29]. Moreover, oral administration of broad-spectrum antibiotics decreased plasma TMAO levels (lower than 100 nM) by 100-fold compared to the control, indicating the essential role of gut microbiota in TMAO synthesis [28].
Past studies have shown that the administration of l-carnitine to Apoe-/- mice leads to double atherosclerosis burden due to increased TMAO levels compared with control counterparts, while suppression of gut microbiota by antibiotics successfully prevents this risk [29]. TMAO and its precursors, such as choline, phosphatidylcholine, and l-carnitine, can decrease reverse cholesterol transport (RCT) by 35%, which is crucial for the accumulation of cholesterol in peripheral tissues, ultimately resulting in cholesterol-related CVDs [29]. In literature, RCT is the process in which excess cholesterol from cells in peripheral tissues and macrophages in vessel walls is transported to the liver in order to be removed from the body via excretion of neutral sterols and bile acids in feces [30]. The suppression of RCT by TMAO is explained by the downregulation of BA transport and synthesis in the liver of TMAO-treated mice, while BA is the major product of cholesterol, its synthesis pathway is the main elimination mechanism of cholesterol from the blood circulation [29]. In addition, NPC1-like intracellular cholesterol transporter and ATP binding cassette subfamily G (ABCG)-5–8, which are cholesterol transporters in and out of enterocytes, respectively, were suppressed by TMAO consumption, resulting in a 26% loss of cholesterol absorption by the gut [29]. In addition, Zhao’s study using rats fed a high-fat high-cholesterol (HFHC) diet demonstrated that oral treatment with TMAO lowered HFHC-induced steatohepatitis by reducing cholesterol accumulation in the liver [31]. Tan et al. (2019) revealed that the serum level of BA is significantly higher in patients with NAFLD, and that there is a positive correlation between the serum levels of TMAO and BA and the mRNA levels of cholesterol 7 alpha-hydroxylase (CYP7A1), an enzyme for cholesterol-origin BA synthesis [32]. The authors also showed that 18 weeks of treatment with TMAO led to liver dysfunction, lipogenesis, and TG accumulation in HFD-fed mice [32]. In-depth experiments showed that TMAO increases BA synthesis and shifts the proportion of liver BA toward farnesoid X receptor (FXR)-antagonistic activity [32]. Knockdown of CYP7A1 or activation of FXR by GW4064 inhibits TMAO-induced lipogenesis in palmitic acid-treated HEPG2 cells [32]. FXR is an important nuclear receptor that maintains the synthesis and transport of hepatic BA, and downregulation of FXR activation can lead to liver diseases, such as cholestasis, NAFLD, and hepatocellular carcinoma [33]. TMAO plays a crucial role in the modulation of BA metabolism and FXR activation, while BA is a key regulator of glucose and lipid metabolism, suggesting that TMAO can exert an impact on hepatic fat accumulation, cholesterol regulation, glucose, and energy homeostasis [28]. The pathogenic impact of TMAO on CVD has been confirmed; however, the roles of TMAO and BA in liver diseases, such as NAFLD and NASH, remain ambiguous. Koeth, Zhao, Wang, and Tan's studies revealed controversial results regarding the effects of TMAO in the liver (Table 1). Tan’s results disagree with those of the early three groups, concluding that TMAO reduces BA synthesis and steatohepatitis, while inducing CVD. These differences in results can be explained by the high cholesterol level models used to investigate CVD in Koeth, Zhao, and Wang's studies, unlike the use of a normal HFD-fed model by Tan. These data suggest that the effect of TMAO could vary and strongly depend on the plasma levels of other substrates, such as cholesterol. However, based on Tan’s results, high plasma TMAO levels were observed in patients with NAFLD together with liver dysfunction and TG accumulation in TMAO-treated HFA-fed mice, suggesting the pathogenic potential of TMAO in NAFLD. The conclusion is also supported by a cohort study conducted by Jose L. Flores-Guerrero et al. (2021) which investigated the association between TMAO level and mortality rate in people with NAFLD [34]. The result of the study demonstrated that a high level of TMAO was associated with an increase in the risk of all-cause mortality in patients with NAFLD while the relationship was not observed in patients without NAFLD [34]. Jose's and Tan's studies suggest that TMAO could be the key factor that can exacerbate the severity of NAFLD which finally ends up increasing the rate of mortality.
Bile acid and the activation of FXR
BA is synthesized from cholesterol in the liver via various pathways, with CYP7A1 is the rate-limiting enzyme in the main pathway [33]. After being formed by CYP7A1, 7α-hydroxycholesterol is converted to cholic acid (CA) or chenodeoxycholic acid (CDCA), and the proportion of CA and CDCA differs between species, such as humans and mice [33]. In humans, primary BA consists CA and CDCA, which finally forms a BA pool comprise 40% CA, 40% CDCA (potent FXR agonist), and 20% deoxycholic acid (DCA), whereas in mice, primary BAs are CA and muricholic acid (MCA; FXR antagonist) which is the product of 6-hydroxylation of CDCA [33]. Moreover, the DCA level is higher in humans owing to the presence of CYP2A12 in mice, the enzyme catalyzes the 7α-rehydroxylation of deoxycholic acid (DCA) and lithocholic acid (LCA) back to CA. Finally, primary BA was subjected to final conjugation using BA-CoA: amino acid N-acyltransferase with glycine and taurine, with mainly glycine in humans and taurine in rodents [33]. Conjugated BA is transported to the gut, where it is deconjugated by bacterial bile salt hydrolases. Furthermore, the microbiota enzyme, 7α-dehydroxylase, in the large intestine converts CA to DCA, and CDCA to LCA. Subsequently, LCA is excreted together with feces, while DCA can be reabsorbed via passive diffusion. In the mouse liver, DCA can be rehydroxylated back to CA using CYP2A12, suggesting that differences in species should be considered when choosing the model for the investigation of human BA signaling. The effects of BA on the intestinal tract include lipid and lipid-soluble nutrient absorption, cholesterol removal, microbiota modification, and regulation of energy homeostasis. FXR plays the most important role in maintaining BA homeostasis, and its operating mechanism and structure have been well described in a previous study [33]. FXR is mainly expressed in the liver, ileum, kidneys, and adrenal glands, and either free or conjugated BAs, mostly CDCA, can activate FXR, however, the responses induced by the activation of FXR are different in a tissue-dependent manner [33]. While activation of FXR in both the intestine and liver suppresses the expression of classical BA synthesis enzymes such as CYP7A1 and CYP8B1, and regulates the enterohepatic circulation of BAs, the response with lower degree is observed in hepatic FXR activation [33]. FXR knockout mice suffer from fatty liver, increased levels of circulating FFAs, serum glucose, and insulin resistance [35], while overexpression of FXR exerts the opposite effects [36] suggesting that FXR activation is required for the recovery of metabolic homeostasis. Importantly, FXR activation is beneficial in liver inflammation and fibrosis, since the activation leads to a decrease in inflammatory cell infiltration by suppressing the monocyte chemoattractant protein-1, and FXR knockout results in strong hepatic inflammation via liver necrosis and upregulation of inducible nitric oxide synthase, cyclooxygenase-2, and interferon-γ [37]. Moreover, FXR suppresses hepatic inflammation by regulating cholestasis and the production and transportation of toxic BA [33]. Activation of the mammalian target of rapamycin by secondary BA in the liver is suggested to be responsible for hepatic carcinogenesis during NASH [38, 39]. The FXR agonist, GW4064, markedly reduces liver injury in cholestatic models via a decrease in alanine transaminase (ALT) and aspartate transaminase (AST) serum levels, necrosis, inflammation, and bile duct proliferation [40, 41]. However, another study demonstrated that FXR knockout confers protection against obstructive cholestasis by reducing mortality and liver injury [42]. Because of the powerful impact of FXR, some FXR-targeting drugs, such as obeticholic acid (OCA; steroidal FXR agonist) and tropifexor (non-steroidal agonist), are being developed to treat NASH [43,44,45]. A trial in which patients with cirrhotic NASH received 25 mg OCA daily for 72 weeks showed improved biochemical and histological features [43]. Another study using 2,065 patients with NASH divided into three groups treated with 10 mg OCA, 25 mg OCA, and placebo for 18 months showed improvement in fibrosis and NASH stage without worsening fibrosis [44]. In an animal study using a mouse model, reduction in oxidative stress, steatosis, inflammation, and fibrosis was observed following treatment with tropifexor [45].
Dietary modification approaches
Since dietary modification is the most advocated approach for NAFLD, it is necessary to determine which kind of dietary treatment can improve the gut and liver health (Fig. 2). Because of the important role of gut microbiota in regulating the gut and liver axes, three types of additives known to modulate the gut microbiota have received vast attention: prebiotics, probiotics, and synbiotics.

Dietary modification affects gut and liver health. Dietary modifications and supplementation of additives can improve the gut health by shaping the gut toward a healthy population that produces beneficial metabolites, such as short-chain fatty acids (SCFAs). SCFAs can then be utilized by intestinal cells to produce essential substances, such as lubricating mucus and tight-junction proteins, which are required to maintain the intestinal barrier and proper bowel movement. Meanwhile, excessive intake of red meat containing a high amount of choline and L-carnitine can increase the trimethylamine-N-oxide (TMAO) levels, leading to cardiovascular disease (CVD), non-alcoholic fatty liver disease (NAFLD), non-alcoholic steatohepatitis (NASH), and cirrhosis
Prebiotics
Dietary fiber is comprised of non-digestible forms of carbohydrates which are usually in the form of polysaccharides (≥ 10 monomers) and could be easily found in plant-based food [46]. Although human is unable to digest and absorb polysaccharides, the microbiota in our gut could handle the task effectively. As the result of the fiber fermentation by gut microbiome, dietary fibers are broken down in the form of SCFAs consisting of acetate, propionate, and butyrate [5]. Those metabolites could be utilized by human cells and have a vast impact on our body by securing intestinal epithelium, regulating overall metabolism, and taking part in immunoregulation [5]. Owing to the benefits of SCFAs, the sources of SCFAs as fibers are recommended for metabolic conditions, such as obesity, diabetes, and IBD (Table 2) [5, 47]. For instance, universal prebiotic fibers, including fructooligosaccharides (FOS), galacto-oligosaccharides, and inulin, have been recently used in many investigations in order to ameliorate IBD [48]. Prebiotic fiber, such as FOS, galactooligosaccharides, and inulin, exert beneficial effects against obesity, IBD, and NAFLD [47, 49]. A study in which C57BL/6 mice were fed a chow diet, choline-deficient high-fat diet (CDHFD), or high-fat high-cholesterol diet (HFHCD) for 16 weeks compared the effects of soluble fibers (inulin) and insoluble fibers (cellulose) on NASH development [50]. Both CDHFD and HFHCD induced NASH in mice via hepatic steatosis and necrosis inflammation, whereas treatment with inulin significantly ameliorated the development of NASH [50]. In comparison with the cellulose-treated group, inulin markedly enriched Bacteroides uniformis, Bacteroides acidifaciens, and Parabacteroides distasonis, which are beneficial in reducing CDHFD-induced NASH. In stool and serum of inulin-treated mice, the authors found a marked increase in pentadecanoic acid, an inulin metabolite produced by P. distasonis, which has protective effects against fat accumulation, inflammation, and oxidative stress in the liver [50]. Another group used C57BL/6 mice fed a normal diet and HFD, with or without inulin, for 14 weeks [51]. Inulin successfully ameliorated HFD-induced outcomes, such as body and liver weight gain, increased AST, ALT, TG, and total Cho levels, and reduced plasma interleukin (IL)-10 levels [51]. In addition, pro-inflammatory markers were decreased concomitant with reduced macrophages and Toll-like receptor (TLR)-4+ macrophages in the liver owing to inulin consumption [51]. In addition, treatment with inulin resulted in the enrichment of Akkermansia and Bifidobacterium, while decreasing the ratio of Firmicutes/Bacteroidetes, together with increased SCFA production [51]. Aoki et al. [52] have proven that inulin alleviates the phenotypes of NAFLD/NASH, such as hepatic steatosis and fibrosis, which are attributed to enrichment in Bacteroides and Blautia, and increased production of SCFAs, especially acetate [52]. Administration of acetate producing substrate; resistant starch and acetate producing Bacteroides acidifaciens and Blautia producta suppressed NAFLD development in germ-free mice [52]. Moreover, the deficiency of FFA receptor 2, an acetate receptor, completely inhibits inulin-induced benefits via hepatic hypertrophy, inflammation, and hypercholesterolemia [52]. However, a clinical trial with two groups, either receiving 20 g/day of inulin or inulin-propionate ester, demonstrated that inulin-fermented acetate could increase the accumulation of intra hepatocellular lipids, while an increase in colonic propionate could ameliorate this effect [53]. An anomaly in accumulation of BA, despite the downregulation of BA signaling pathways, was observed in patients with NAFLD, while it is known that the key function of BA synthesis is to maintain the healthy cholesterol level by induce the excretion of superfluous cholesterol [54]. The above evidence suggests that the excessive amount of BA could be the reason for the downregulation of BA synthesis and ultimately leads to high level of cholesterol in NAFLD cases [54]. Wang et al. [54] demonstrated that inulin ameliorated HFD-induced NAFLD in mice by improving BA excretion via activation of FXR–fibroblast growth factor 15 signaling and recovery of BA de novo synthesis [54]. In addition to inulin, FOS have been widely investigated as a prebiotic treatment for NAFLD and other metabolic disorders. Takai et al. [55] induced NAFLD in C57BL/6 J mice via subcutaneous injection of monosodium glutamate (MSG) and treatment with 5% FOS in drinking water for 18 weeks [55]. The induction of MSG leads to hepatic steatosis, hepatocyte hypertrophy, inflammation, and macrophage infiltration, and upregulated mRNAs are involved in fatty acid synthesis [55]. Mice in the FOS-treated group showed reduced MSG-induced NAFLD via blunted mRNA levels of lipid metabolism enzymes, reduced hepatocyte ballooning, crown-like formation, and M1 macrophages in epididymal fat [55]. The beneficial effect of FOS is attributed to the increased concentration of SCFAs, containing n-butyric, propionic, and acetic acids, in fecal samples and propionic acid in serum [55]. Another study demonstrated that treatment with choline (3 g/100 g diet) and FOS (10 g/100 g diet) reduced the total mean fat in the liver and heart tissues of NAFLD mice by 0.2 and 1.7 g, respectively [56]. FOS administration suppressed both plasma levels of cholesterol and triacylglycerides compared to the standard diet-treated mice and mice before treatment [56]. Matsumoto et al. [57] conducted a study with three groups of mice fed different diets, including a control diet, methionine–choline-deficient (MCD) diet, and an MCD diet plus 5% FOS. The MCD diet fostered Clostridium cluster XI and subcluster XIVa populations and suppressed Lactobacillales spp., whereas the supplementation of FOS in the MCD diet helped maintain a healthy population of microbiota [57]. In comparison to MCD-fed mice, mice fed the FOS-supplemented MCD diet showed reduced hepatic steatosis, inflammation, CD14 + Kupffer cells, and TLR4 expression, while increasing the fecal SCFAs and intestinal immunoglobulin A (IgA) levels [57]. The authors suggested that MCD-induced microbiota dysbiosis, which results in decreased production of SCFAs, interrupts tight junction protein expression and increases the gut permeability, followed by the translocation of pathogen-associated molecular patterns (PAMPs) to the liver. Subsequently, PAMPs recognized by TLR4 in Kupffer cells activate the cells to secrete inflammatory cytokines together with hepatocyte steatosis, which causes NAFLD/NASH [57]. FOS is known to foster populations of Bifidobacterium and Lactobacillales, which are SCFA-producing strains, thereby increasing SCFAs production and securing the intestinal barrier [57]. β-glucan, another source of fiber, which is compatible with FOS, has beneficial effects on microbiota modification, intestinal barrier maintenance, and liver condition improvement [5]. A study demonstrated that Schizophyllum commune (a species of fungus in the genus Schizophyllum)-derived β-glucan successfully secures the intestinal barrier in dextran sodium sulfate (DSS) -induced ulcerative colitis (UC) mice by fostering SCFA-producing bacteria and increasing SCFA production [5]. Hence, β-glucan significantly ameliorates DSS-induced colitis and colitis-associated NAFLD by reducing hepatic steatosis, hepatitis, and inflammatory cell infiltration [5]. LPS is a bacterial toxin, whose translocation to the liver leads to hepatic steatosis and inflammation. A study induced NASH in mice using intraperitoneal injections of LPS at a dose of 1.5 mg/kg to investigate the protective effects of oat-derived β-glucan at different doses up to 10% in a specific pathogen-free diet [58]. The results showed that β-glucan dose independently reduced the serum endotoxin and glucose levels, and insulin resistance caused by LPS [58]. Plasma AST and ALT levels also decreased due to β-glucan consumption concomitant with reduced hepatic inflammation and fibrosis observed in hematoxylin and eosin-stained hepatic sections [58]. In addition, the effect of Aureobasidium pullulans (yeast-like fungus)-derived β-glucan has been investigated [59]. Oral administration of fungal β-glucan for 16 weeks significantly inhibited HFD-induced hepatic steatosis and elevated cholesterol, TG, and ALT serum levels [59]. Treatment with β-glucan leads to an increase in CYP7A1 expression and plays an important role in cholesterol excretion via BA synthesis [59]. Moreover, other sources of β-glucan, such as A. pullulans and baker’s yeast, demonstrated beneficial effects in NAFLD [60, 61]. Compared with conventional drugs, prebiotics are easily accessible and have minimal side effects. Furthermore, abundant sources of prebiotics with distinct benefits confer a wide range of choices for personalized therapy.
Probiotics
Besides prebiotics, probiotics that produce SCFAs, such as Lactobacillus, Firmicutes members, F. prausnitzii, Bifidobacterium, and Streptococcus salivarius, have also been suggested as a promising therapeutic (Table 3) [5, 62,63,64]. A meta-analysis of 25 studies demonstrated a reduced body mass index (BMI) of 0.54, 0.51, and 0.13 kg/m2 as the result of prebiotic, probiotic, and synbiotic treatments, respectively [49]. Amelioration of liver injury was also observed via treatment with additives observed via reduced ALT and AST serum levels [49]. Importantly, a subgroup analysis demonstrated that microbial therapies reduced BMI by 0.55 kg/m2, ALT by 11.74 U/L, and AST by 8.56 U/L in patients with NAFLD, but not those without NAFLD [49]. The different effects of additives in patients with and without NAFLD suggest the need for a disease background to observe the efficiency; however, a study suggests that despite the lack of change at the basal state, prebiotics exert protective effects against common metabolic diseases [8]. Previous trials have clearly shown the beneficial effects of VSL#3, the most widely known probiotic mixture containing four strains of Lactobacillus (L. acidophilus, L. plantarum, L. casei, and L. delbrueckii subsp. Bulgaricus), Bifidobacterium (B. breve, B. infantis, and B. longum), and Streptococcus salivarius subsp. Thermophilus, on NAFLD via a reduction in BMI and liver injury markers [65]. A clinical study investigated the effect of a VSL#3 mixture on obese children with NASH and found that treatment with VSL#3 for 4 months led to a reduced BMI and NAFLD [65]. Moreover, treatment with the mixture resulted in the upregulation of GLP-1 and activated GLP-1 levels in the serum [65]. By applying VSL#3 to MCD diet-induced NASH mice, Velayudham et al. [66] indicated that VSL#3 mixture shows a lack of effect on reducing MCD-induced hepatic steatosis and inflammation [66]. In contrast, liver fibrosis caused by MCD was ameliorated by VSL#3, due to the downregulation of hepatic collagen and alpha-smooth muscle actin levels, together with an increase in the expression levels of BMP and activin membrane bound inhibitor, a transforming growth factor-beta pseudoreceptor [66]. The insufficient effect of VSL#3 was also observed in patients with NAFLD, showing insignificant improvement in the serum levels of biomarkers of cardiovascular risk and liver injury [67]. In contrast, Chong et al. [67] demonstrated that treatment with VSL#3 significantly reduced the levels of TGs, high-sensitivity C-reactive protein, transaminases, and gamma-glutamyltransferases, which are biomarkers for the occurrence of hepatic injury and inflammation [68]. Despite the amelioration of hepatic steatosis and inflammation, BMI, circumference, and plasma glucose, total Cho, LDL-C, HDL-C, and adiponectin levels remained unchanged after treatment with VSL#3 [68]. Besides VSL#3, Lactobacillus rhamnosus GG (LGG) is one of the most well-studied probiotics. A screening study indicated that LGG is one of the seven strains isolated from traditional Chinese fermented food and healthy human feces that exhibits a cholesterol-suppressing effect [69]. Moreover, LGG is the strain that survives in 0.3% bile salt and has the best cell adhesion abilities [69]. Treatment with LGG and Lactobacillus plantarum resulted in decreased serum lipid levels by increasing hepatic CYP7A1 and LDL receptor mRNA levels and peroxisome proliferator-activated receptor (PPAR)-α protein levels, while decreasing PPAR-γ and sterol regulatory element binding transcription factor 1 isoform c (SREBP-1C) protein levels [69]. Moreover, administration of 5 × 107 CFU/g body weight of LGG to high-fructose diet-induced NAFLD in C57BL/J6 mice restored the intestinal tight junction protein expression [70]. Therefore, treatment with LGG leads to reduced LPS, hepatic inflammatory marker, and ALT serum levels, and fat accumulation [70]. A clinical trial investigated the effect of LGG on obese children with persistent hypertransaminasemia and bright ultrasonographic (US) liver image [71]. The results showed a decrease in ALT and antipeptidoglycan-polysaccharide antibodies in treated individuals despite a constant BMI, z-score, and US liver parameters [71]. Bifidobacterium spp. and Lactobacillu spp. were also investigated to determine if they affected liver conditions, such as NAFLD and NASH. A clinical trial investigated the relationship between NAFLD/NASH-related metabolic parameters and fecal bacteria, focusing on Bifidobacteria and Lactobacilli [72]. The trial indicated that three Bifidobacterium spp. (B. longum, B. bifidum, and B. adolescentis) and five Lactobacillus spp. (L. zeae, L. vaginalis, L. brevis, L. ruminis, and L. mucosae) are usually detected in metagenomic analyses [72]. The metagenomic results indicated that a higher proportion of Lactobacillus spp. was observed in fecal samples of NAFLD, NASH, and obese children, especially L. mucosae, whereas an abundant population of Bifidobacterium spp. was observed in healthy individuals [72]. These results suggest that the uplifting population of Bifidobacterium members can be promising targets for gut microbiota modification [72]. A study in 2020 demonstrated that Bifidobacterium animalis subsp. Lactis V9 (V9) treatment ameliorated hepatic steatosis and inflammation in HFD-fed male Wistar rats [73]. The reduction in hepatic steatosis is attributed to the effect on de novo lipid synthesis regulation by reducing the transcription of SREBP-1c and fatty acid synthase (FAS), whereas hepatic phosphorylated-AMPK and PPAR-α expression levels were upregulated by V9 [73]. V9 anti-inflammatory effect was observed via decreased expression levels of inflammatory cytokines and receptors, together with the suppression of AMPK and TLR-NF-κB pathways, compared to HFD-fed rats [73]. Besides Bifidobacterium, Lactobacillus has also received adequate attention as a therapeutic probiotic [74, 75]. Lee et al. [75] demonstrated that treatments with four Lactobacillus strains, L. acidophilus, L. fermentum, L. paracasei, and L. plantarum, have beneficial effects on NAFLD [74]. Administration of L. acidophilus led to a decreased liver/body weight ratio, while reduced cholesterol levels were observed in mice treated with L. acidophilus, L. fermentum, and L. plantarum [74]. Furthermore, L. acidophilus-, L. plantarum-, and L. paracasei-supplemented diets induced the amelioration of hepatic steatosis [74]. Before this study, the aforementioned group had already revealed the benefits of L. bulgaricus, L. casei, L. helveticus, and Pediococcus pentosaceus KID7, including reduced liver/body ratio and improvement in hepatic steatosis and inflammation, in western diet-induced conditions [75].
Synbiotics
Notably, prebiotics and probiotics can be administered together to have a synergistic effect, and supplementation with prebiotics can prevent nutrient competition between fiber-ingesting indigenous and administered beneficial strains (Table 4) [5]. As one of the most well-investigated prebiotics, the benefits of combining inulin with other probiotics have been widely studied. A clinical study conducted in 2018 by Bakhshimoghaddam et al. consolidated the protective effects of inulin and Bifidobacterium spp. against NAFLD [76]. Patients consuming synbiotic yogurt daily for 24 weeks had lower risk of NAFLD and serum levels of ALT, AST, ALP, and γ-glutamyl-transferase in comparison with the conventional yogurt and control groups [76]. Both separate and combined treatments of inulin with B. longum and L. acidophilus in patients with NAFLD showed decreased BMI and AST serum levels, and increased total antioxidant capacity [77, 78]. In the co-treatment group, patients showed a significant decrease in high-sensitivity C-reactive protein levels compared to the placebo and single-treatment groups [77]. In addition to inulin, the combination of FOS and probiotics also has beneficial effects on NAFLD [79]. A clinical trial was conducted with 80 patients with NAFLD who were daily administered synbiotic capsules containing seven species of probiotic bacteria and FOS for 8 weeks [79]. The ultrasound grade of NAFLD was decreased in synbiotic-treated patients despite unchanged ALT and AST serum levels [79]. Mofidi et al. [80] conducted a clinical trial to investigate the combined effects of FOS and probiotics in patients with NAFLD with normal or low BMI [80]. After 28 weeks of intervention, reduction in hepatic steatosis and fibrosis, along with low serum levels of fasting blood sugar, TG, and inflammatory mediators were observed in the synbiotic-treated group [80]. In another study, 104 patients with NAFLD participated in a double-blind and placebo-controlled phase 2 trial for 12 months and were administered a synbiotic or a placebo [81]. Patients treated with FOS and probiotics showed insignificant changes in hepatic fat and liver fibrosis markers despite the modification of gut microbiota by fostering Bifidobacterium and Faecalibacterium, while suppressing Oscillibacter and Alistipes [81]. Besides inulin and FOS, the co-administration of β-glucan with other probiotics is worth investigating. In 2021, a study using HFD-induced obese mice with UC induction using 3% DSS revealed the close relationship between UC and NAFLD, in which colitis-associated gut permeability led to the transport of endotoxins and caused hepatic steatosis and inflammation [5]. The study demonstrated that treatment with β-glucan together with probiotics (VSL#3 and LGG) outperformed the separate treatment groups (β-glucan or probiotics) in protecting the liver from UC-induced NAFLD via hepatic steatosis and inflammation using hematoxylin and eosin-stained liver sections [5]. Several clinical trials using a combination of prebiotics, such as inulin and FOS, and probiotics, such as Bifidobacterium, Lactobacillus, and Streptococcus, showed decreased BMI and serum levels of AST and ALT [82,83,84]. However, many trials have indicated that the treatment with additives is inefficient and has variable benefits, suggesting that individual genetic traits also affect the treatment [79, 85, 86].
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S (2020) Nonalcoholic steatohepatitis: a review. JAMA 323:1175–1183. https://doi.org/10.1001/jama.2020.2298
Abd El-Kader SM, El-Den Ashmawy EM (2015) Non-alcoholic fatty liver disease: the diagnosis and management. World J Hepatol 7:846–858. https://doi.org/10.4254/wjh.v7.i6.846
Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, McCullough AJ (1999) Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 116:1413–1419. https://doi.org/10.1016/s0016-5085(99)70506-8
Meex RCR, Blaak EE (2021) Mitochondrial dysfunction is a key pathway that links saturated fat intake to the development and progression of NAFLD. Mol Nutr Food Res 65:e1900942. https://doi.org/10.1002/mnfr.201900942
Vu V, Muthuramalingam K, Singh V, Hyun C, Kim YM, Unno T, Cho M (2021) Effects of β-glucan, probiotics, and synbiotics on obesity-associated colitis and hepatic manifestations in C57BL/6J mice. Eur J Nutr 61:793–807. https://doi.org/10.1007/s00394-021-02668-z
Albillos A, de Gottardi A, Rescigno M (2020) The gut-liver axis in liver disease: pathophysiological basis for therapy. J Hepatol 72:558–577. https://doi.org/10.1016/j.jhep.2019.10.003
Maloy KJ, Powrie F (2011) Intestinal homeostasis and its breakdown in inflammatory bowel disease. Nature 474:298–306. https://doi.org/10.1038/nature10208
Vu V, Muthuramalingam K, Singh V, Choi C, Kim YM, Unno T, Cho M (2022) Schizophyllum commune-derived β-glucan improves intestinal health demonstrating protective effects against constipation and common metabolic disorders. Appl Biol Chem 65:9. https://doi.org/10.1186/s13765-022-00680-3
Tolhurst G, Heffron H, Lam YS, Parker HE, Habib AM, Diakogiannaki E, Cameron J, Grosse J, Reimann F, Gribble FM (2012) Short-chain fatty acids stimulate glucagon-like peptide-1 secretion via the G-protein-coupled receptor FFAR2. Diabetes 61:364–371. https://doi.org/10.2337/db11-1019
Weitkunat K, Schumann S, Nickel D, Kappo KA, Petzke KJ, Kipp AP, Blaut M, Klaus S (2016) Importance of propionate for the repression of hepatic lipogenesis and improvement of insulin sensitivity in high-fat diet-induced obesity. Mol Nutr Food Res 60:2611–2621. https://doi.org/10.1002/mnfr.201600305
Singh V, Park Y-J, Lee G, Unno T, Shin J-H (2022) Dietary regulations for microbiota dysbiosis among post-menopausal women with type 2 diabetes. Crit Rev Food Sci Nutr. https://doi.org/10.1080/10408398.2022.2076651
Lukovac S, Belzer C, Pellis L, Keijser BJ, de Vos WM, Montijn RC, Roeselers G (2014) Differential modulation by Akkermansia muciniphila and Faecalibacterium prausnitzii of host peripheral lipid metabolism and histone acetylation in mouse gut organoids. mBio 5:e01438-01414. https://doi.org/10.1128/mBio.01438-14
Visekruna A, Luu M (2021) The role of short-chain fatty acids and bile acids in intestinal and liver function, inflammation, and carcinogenesis. Front Cell Dev Biol 9:703218. https://doi.org/10.3389/fcell.2021.703218
Zhou D, Chen YW, Zhao ZH, Yang RX, Xin FZ, Liu XL, Pan Q, Zhou H, Fan JG (2018) Sodium butyrate reduces high-fat diet-induced non-alcoholic steatohepatitis through upregulation of hepatic GLP-1R expression. Exp Mol Med 50:1–12. https://doi.org/10.1038/s12276-018-0183-1
Jeon SM (2016) Regulation and function of AMPK in physiology and diseases. Exp Mol Med 48:e245. https://doi.org/10.1038/emm.2016.81
Antunes KH, Fachi JL, de Paula R, da Silva EF, Pral LP (2019) Microbiota-derived acetate protects against respiratory syncytial virus infection through a GPR43-type 1 interferon response. Nat Commun 10:3273. https://doi.org/10.1038/s41467-019-11152-6
Trompette A, Gollwitzer ES, Pattaroni C, Lopez-Mejia IC, Riva E, Pernot J, Ubags N, Fajas L, Nicod LP, Marsland BJ (2018) Dietary fiber confers protection against flu by shaping Ly6c(-) patrolling monocyte hematopoiesis and CD8(+) T cell metabolism. Immunity 48:992-1005.e1008. https://doi.org/10.1016/j.immuni.2018.04.022
Sencio V, Barthelemy A, Tavares LP, Machado MG, Soulard D, Cuinat C, Queiroz-Junior CM, Noordine ML, Salomé-Desnoulez S, Deryuter L, Foligné B, Wahl C, Frisch B, Vieira AT, Paget C, Milligan G, Ulven T, Wolowczuk I, Faveeuw C, Le Goffic R, Thomas M, Ferreira S, Teixeira MM, Trottein F (2020) Gut dysbiosis during influenza contributes to pulmonary pneumococcal superinfection through altered short-chain fatty acid production. Cell Rep 30:2934-2947.e2936. https://doi.org/10.1016/j.celrep.2020.02.013
Kim MH, Kang SG, Park JH, Yanagisawa M, Kim CH (2013) Short-chain fatty acids activate GPR41 and GPR43 on intestinal epithelial cells to promote inflammatory responses in mice. Gastroenterology 145:396-406 e391 310. https://doi.org/10.1053/j.gastro.2013.04.056
Kim M, Friesen L, Park J, Kim HM, Kim CH (2018) Microbial metabolites, short-chain fatty acids, restrain tissue bacterial load, chronic inflammation, and associated cancer in the colon of mice. Eur J Immunol 48:1235–1247. https://doi.org/10.1002/eji.201747122
Hu Y, Le Leu RK, Christophersen CT, Somashekar R, Conlon MA, Meng XQ, Winter JM, Woodman RJ, McKinnon R, Young GP (2016) Manipulation of the gut microbiota using resistant starch is associated with protection against colitis-associated colorectal cancer in rats. Carcinogenesis 37:366–375. https://doi.org/10.1093/carcin/bgw019
Deng M, Qu F, Chen L, Liu C, Zhang M, Ren F, Guo H, Zhang H, Ge S, Wu C, Zhao L (2020) SCFAs alleviated steatosis and inflammation in mice with NASH induced by MCD. J Endocrinol 245:425–437. https://doi.org/10.1530/JOE-20-0018
Perez R, Stevenson F, Johnson J, Morgan M, Erickson K, Hubbard NE, Morand L, Rudich S, Katznelson S, German JB (1998) Sodium butyrate upregulates Kupffer cell PGE2 production and modulates immune function. J Surg Res 78:1–6. https://doi.org/10.1006/jsre.1998.5316
Perez RV, Johnson J, Hubbard NE, Erickson K, Morgan M, Kim S, Rudich SM, Katznelson S, German JB (1998) Selective targeting of Kupffer cells with liposomal butyrate augments portal venous transfusion-induced immunosuppression. Transplantation 65:1294–1298. https://doi.org/10.1097/00007890-199805270-00002
Kim CH (2021) Control of lymphocyte functions by gut microbiota-derived short-chain fatty acids. Cell Mol Immunol 18:1161–1171. https://doi.org/10.1038/s41423-020-00625-0
Guzior DV, Quinn RA (2021) Review: microbial transformations of human bile acids. Microbiome 9:140. https://doi.org/10.1186/s40168-021-01101-1
Chen YM, Liu Y, Zhou RF, Chen XL, Wang C, Tan XY, Wang LJ, Zheng RD, Zhang HW, Ling WH, Zhu HL (2016) Associations of gut-flora-dependent metabolite trimethylamine-N-oxide, betaine and choline with non-alcoholic fatty liver disease in adults. Sci Rep 6:19076. https://doi.org/10.1038/srep19076
Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, Dugar B, Feldstein AE, Britt EB, Fu X, Chung YM, Wu Y, Schauer P, Smith JD, Allayee H, Tang WH, DiDonato JA, Lusis AJ, Hazen SL (2011) Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 472:57–63. https://doi.org/10.1038/nature09922
Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, Britt EB, Fu X, Wu Y, Li L, Smith JD, DiDonato JA, Chen J, Li H, Wu GD, Lewis JD, Warrier M, Brown JM, Krauss RM, Tang WHW, Bushman FD, Lusis AJ, Hazen SL (2013) Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med 19:576–585. https://doi.org/10.1038/nm.3145
Brufau G, Groen AK, Kuipers F (2011) Reverse cholesterol transport revisited: contribution of biliary versus intestinal cholesterol excretion. Arterioscler Thromb Vasc Biol 31:1726–1733. https://doi.org/10.1161/atvbaha.108.181206
Zhao ZH, Xin FZ, Zhou D, Xue YQ, Liu XL, Yang RX, Pan Q, Fan JG (2019) Trimethylamine N-oxide attenuates high-fat high-cholesterol diet-induced steatohepatitis by reducing hepatic cholesterol overload in rats. World J Gastroenterol 25:2450–2462. https://doi.org/10.3748/wjg.v25.i20.2450
Tan X, Liu Y, Long J, Chen S, Liao G, Wu S, Li C, Wang L, Ling W, Zhu H (2019) Trimethylamine N-oxide aggravates liver steatosis through modulation of bile acid metabolism and inhibition of farnesoid X receptor signaling in nonalcoholic fatty liver disease. Mol Nutr Food Res 63:1900257. https://doi.org/10.1002/mnfr.201900257
Stofan M, Guo GL (2020) Bile acids and FXR: novel targets for liver diseases. Front Med 7:544. https://doi.org/10.3389/fmed.2020.00544
Flores-Guerrero JL, Post A, van Dijk PR, Connelly MA, Garcia E, Navis G, Bakker SJL, Dullaart RPF (2021) Circulating trimethylamine-N-oxide is associated with all-cause mortality in subjects with nonalcoholic fatty liver disease. Liver Int 41:2371–2382. https://doi.org/10.1111/liv.14963
Ma K, Saha PK, Chan L, Moore DD (2006) Farnesoid X receptor is essential for normal glucose homeostasis. J Clin Invest 116:1102–1109. https://doi.org/10.1172/jci25604
Zhang Y, Lee FY, Barrera G, Lee H, Vales C, Gonzalez FJ, Willson TM, Edwards PA (2006) Activation of the nuclear receptor FXR improves hyperglycemia and hyperlipidemia in diabetic mice. Proc Natl Acad Sci U S A 103:1006–1011. https://doi.org/10.1073/pnas.0506982103
Wang YD, Chen WD, Wang M, Yu D, Forman BM, Huang W (2008) Farnesoid X receptor antagonizes nuclear factor kappaB in hepatic inflammatory response. Hepatology 48:1632–1643. https://doi.org/10.1002/hep.22519
Yamada S, Takashina Y, Watanabe M, Nagamine R, Saito Y, Kamada N, Saito H (2018) Bile acid metabolism regulated by the gut microbiota promotes non-alcoholic steatohepatitis-associated hepatocellular carcinoma in mice. Oncotarget 9:9925–9939. https://doi.org/10.18632/oncotarget.24066
Zhai H, Li Z, Peng M, Huang Z, Qin T, Chen L, Li H, Zhang H, Zhang W, Xu G (2018) Takeda G protein-coupled receptor 5-mechanistic target of rapamycin complex 1 signaling contributes to the increment of glucagon-like peptide-1 production after Roux-en-Y gastric bypass. EBioMedicine 32:201–214. https://doi.org/10.1016/j.ebiom.2018.05.026
Liu Y, Binz J, Numerick MJ, Dennis S, Luo G, Desai B, MacKenzie KI, Mansfield TA, Kliewer SA, Goodwin B, Jones SA (2003) Hepatoprotection by the farnesoid X receptor agonist GW4064 in rat models of intra- and extrahepatic cholestasis. J Clin Invest 112:1678–1687. https://doi.org/10.1172/jci18945
Cui YJ, Aleksunes LM, Tanaka Y, Goedken MJ, Klaassen CD (2009) Compensatory induction of liver efflux transporters in response to ANIT-induced liver injury is impaired in FXR-null mice. Toxicol Sci 110:47–60. https://doi.org/10.1093/toxsci/kfp094
Stedman C, Liddle C, Coulter S, Sonoda J, Alvarez JG, Evans RM, Downes M (2006) Benefit of farnesoid X receptor inhibition in obstructive cholestasis. Proc Natl Acad Sci U S A 103:11323–11328. https://doi.org/10.1073/pnas.0604772103
Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, Chalasani N, Dasarathy S, Diehl AM, Hameed B, Kowdley KV, McCullough A, Terrault N, Clark JM, Tonascia J, Brunt EM, Kleiner DE, Doo E (2015) Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet 385:956–965. https://doi.org/10.1016/s0140-6736(14)61933-4
Ratziu V, Sanyal AJ, MacConell L, Shringarpure R, Marmon T, Shapiro D, Younossi ZM (2016) THU-488—regenerate: a phase 3, double-blind, randomized, placebo-controlled multicenter study of obeticholic acid therapy for nonalcoholic steatohepatitis. J Hepatol 64:S294–S295. https://doi.org/10.1016/S0168-8278(16)00372-X
Hernandez ED, Zheng L, Kim Y, Fang B, Liu B, Valdez RA, Dietrich WF, Rucker PV, Chianelli D, Schmeits J, Bao D, Zoll J, Dubois C, Federe GC, Chen L, Joseph SB, Klickstein LB, Walker J, Molteni V, McNamara P, Meeusen S, Tully DC, Badman MK, Xu J, Laffitte B (2019) Tropifexor-mediated abrogation of steatohepatitis and fibrosis is associated with the antioxidative gene expression profile in rodents. Hepatol Commun 3:1085–1097. https://doi.org/10.1002/hep4.1368
Hijová E, Bertková I, Štofilová J (2019) Dietary fibre as prebiotics in nutrition. Cent Eur J Public Health 27:251–255. https://doi.org/10.21101/cejph.a5313
Davani-Davari D, Negahdaripour M, Karimzadeh I, Seifan M, Mohkam M, Masoumi SJ, Berenjian A, Ghasemi Y (2019) Prebiotics: definition, types, sources, mechanisms, and clinical applications. Foods (Basel, Switzerland) 8:92. https://doi.org/10.3390/foods8030092
Davani-Davari D, Negahdaripour M, Karimzadeh I, Seifan M, Mohkam M, Masoumi SJ, Berenjian A, Ghasemi Y (2019) Prebiotics: definition, types, sources, mechanisms, and clinical applications. Foods 8:92. https://doi.org/10.3390/foods8030092
Loman BR, Hernández-Saavedra D, An R, Rector RS (2018) Prebiotic and probiotic treatment of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Nutr Rev 76:822–839. https://doi.org/10.1093/nutrit/nuy031
Wei W (2021) Dietary inulin ameliorates non-alcoholic steatohepatitis through direct modulating gut microbiota and metabolites. Ph.D., The Chinese University of Hong Kong (Hong Kong) https://www.proquest.com/openview/30fbabfd237e3075226263a6e0239165/1?pqorigsite=gscholar&cbl=2026366&diss=y
Bao T, He F, Zhang X, Zhu L, Wang Z, Lu H, Wang T, Li Y, Yang S, Wang H (2020) Inulin exerts beneficial effects on non-alcoholic fatty liver disease via modulating gut microbiome and suppressing the lipopolysaccharide-toll-like receptor 4-Mψ-nuclear factor-κB-nod-like receptor protein 3 pathway via gut-liver axis in mice. Front Pharmacol 11:558525. https://doi.org/10.3389/fphar.2020.558525
Aoki R, Onuki M, Hattori K, Ito M, Yamada T, Kamikado K, Kim Y-G, Nakamoto N, Kimura I, Clarke JM, Kanai T, Hase K (2021) Commensal microbe-derived acetate suppresses NAFLD/NASH development via hepatic FFAR2 signalling in mice. Microbiome 9:188. https://doi.org/10.1186/s40168-021-01125-7
Chambers ES, Byrne CS, Rugyendo A, Morrison DJ, Preston T, Tedford C, Bell JD, Thomas L, Akbar AN, Riddell NE, Sharma R, Thursz MR, Manousou P, Frost G (2019) The effects of dietary supplementation with inulin and inulin-propionate ester on hepatic steatosis in adults with non-alcoholic fatty liver disease. Diabetes Obes Metab 21:372–376. https://doi.org/10.1111/dom.13500
Wang R, Ren Y, Bao T, Wang T, Li Y, Liu Y, Zhang X, Yang S, Wang H (2022) Inulin activates FXR-FGF15 signaling and further increases bile acids excretion in non-alcoholic fatty liver disease mice. Biochem Biophys Res Commun 600:156–162. https://doi.org/10.1016/j.bbrc.2022.02.033
Takai A, Kikuchi K, Ichimura M, Tsuneyama K, Moritoki Y, Matsumoto K, Tsunashima H, Onda T, Kuniyoshi N, Nariyama T, Ohyatsu S, Kubota J, Nagumo K, Sato S, Hara M, Miyakawa H (2020) Fructo-oligosaccharides ameliorate steatohepatitis, visceral adiposity, and associated chronic inflammation via increased production of short-chain fatty acids in a mouse model of non-alcoholic steatohepatitis. BMC Gastroenterol 20:46. https://doi.org/10.1186/s12876-020-01194-2
Borges Haubert NJ, Marchini JS, Carvalho Cunha SF, Suen VM, Padovan GJ, Jordao AAJ, Marchini Alves CM, Marchini JF, Vannucchi H (2015) Choline and fructooligosaccharide: non-alcoholic fatty liver disease, cardiac fat deposition, and oxidative stress markers. Nutr Metab Insights 8:1–6. https://doi.org/10.4137/nmi.s24385
Matsumoto K, Ichimura M, Tsuneyama K, Moritoki Y, Tsunashima H, Omagari K, Hara M, Yasuda I, Miyakawa H, Kikuchi K (2017) Fructo-oligosaccharides and intestinal barrier function in a methionine-choline-deficient mouse model of nonalcoholic steatohepatitis. PLoS ONE 12:e0175406. https://doi.org/10.1371/journal.pone.0175406
You S, Hu X, Zhao Q, Chen X, Xu C (2013) Oat β-glucan inhibits lipopolysaccharide-induced nonalcoholic steatohepatitis in mice. Food Funct 4:1360–1368. https://doi.org/10.1039/c3fo60081e
Aoki S, Iwai A, Kawata K, Muramatsu D, Uchiyama H, Okabe M, Ikesue M, Maeda N, Uede T (2015) Oral administration of the Aureobasidium pullulans-derived β-glucan effectively prevents the development of high fat diet-induced fatty liver in mice. Sci Rep 5:10457. https://doi.org/10.1038/srep10457
Ikewaki N, Levy GA, Kurosawa G, Iwasaki M, Dedeepiya VD, Vaddi S, Senthilkumar R, Preethy S, Abraham SJK (2022) Hepatoprotective effects of Aureobasidium pullulans derived β 1,3–1,6 glucans in a murine model of non-alcoholic steatohepatitis. J Clin Exp Hepatol 12:1428–1437. https://doi.org/10.1016/j.jceh.2022.06.008
Huang T, Liu Y, Li H, Zhang Y, Kong D, Cui G (2020) β-Glucan ameliorates nonalcoholic steatohepatitis induced by methionine and choline-deficient diet in mice. J Food Biochem 44:e13408. https://doi.org/10.1111/jfbc.13408
Liu X-j, Yu R, Zou K-f (2019) Probiotic mixture VSL#3 alleviates dextran sulfate sodium-induced colitis in mice by downregulating T follicular helper cells. Curr Med Sci 39:371–378. https://doi.org/10.1007/s11596-019-2045-z
Segers ME, Lebeer S (2014) Towards a better understanding of Lactobacillus rhamnosus GG–host interactions. Microb Cell Fact 13(Suppl 1):S7–S7. https://doi.org/10.1186/1475-2859-13-S1-S7
Parada Venegas D, De la Fuente MK, Landskron G, González MJ, Quera R, Dijkstra G, Harmsen HJM, Faber KN, Hermoso MA (2019) Short Chain Fatty Acids (SCFAs)-mediated gut epithelial and immune regulation and its relevance for inflammatory bowel diseases. Front Immunol 10:277. https://doi.org/10.3389/fimmu.2019.00277
Alisi A, Bedogni G, Baviera G, Giorgio V, Porro E, Paris C, Giammaria P, Reali L, Anania F, Nobili V (2014) Randomised clinical trial: the beneficial effects of VSL#3 in obese children with non-alcoholic steatohepatitis. Aliment Pharmacol Ther 39:1276–1285. https://doi.org/10.1111/apt.12758
Velayudham A, Dolganiuc A, Ellis M, Petrasek J, Kodys K, Mandrekar P, Szabo G (2009) VSL#3 probiotic treatment attenuates fibrosis without changes in steatohepatitis in a diet-induced nonalcoholic steatohepatitis model in mice. Hepatology 49:989–997. https://doi.org/10.1002/hep.22711
Chong PL, Laight D, Aspinall RJ, Higginson A, Cummings MH (2021) A randomised placebo controlled trial of VSL#3® probiotic on biomarkers of cardiovascular risk and liver injury in non-alcoholic fatty liver disease. BMC Gastroenterol 21:144. https://doi.org/10.1186/s12876-021-01660-5
Derosa G, Guasti L, D’Angelo A, Martinotti C, Valentino MC, Di Matteo S, Bruno GM, Maresca AM, Gaudio GV, Maffioli P (2022) Probiotic therapy with VSL#3® in patients with NAFLD: a randomized clinical trial. Front Nutr 9:846873. https://doi.org/10.3389/fnut.2022.846873
Mei L, Tang Y, Li M, Yang P, Liu Z, Yuan J, Zheng P (2015) Co-administration of cholesterol-lowering probiotics and anthraquinone from Cassia obtusifolia L ameliorate non-alcoholic fatty liver. PLOS ONE 10:e0138078. https://doi.org/10.1371/journal.pone.0138078
Ritze Y, Bárdos G, Claus A, Ehrmann V, Bergheim I, Schwiertz A, Bischoff SC (2014) Lactobacillus rhamnosus GG protects against non-alcoholic fatty liver disease in mice. PLoS ONE 9:e80169. https://doi.org/10.1371/journal.pone.0080169
Vajro P, Mandato C, Licenziati MR, Franzese A, Vitale DF, Lenta S, Caropreso M, Vallone G, Meli R (2011) Effects of Lactobacillus rhamnosus strain GG in pediatric obesity-related liver disease. J Pediatr Gastroenterol Nutr 52:740–743. https://doi.org/10.1097/MPG.0b013e31821f9b85
Nobili V, Putignani L, Mosca A, Del Chierico F, Vernocchi P, Alisi A, Stronati L, Cucchiara S, Toscano M, Drago L (2018) Bifidobacteria and lactobacilli in the gut microbiome of children with non-alcoholic fatty liver disease: which strains act as health players? Arch Med Sci 14:81–87. https://doi.org/10.5114/aoms.2016.62150
Yan Y, Liu C, Zhao S, Wang X, Wang J, Zhang H, Wang Y, Zhao G (2020) Probiotic Bifidobacterium lactis V9 attenuates hepatic steatosis and inflammation in rats with non-alcoholic fatty liver disease. AMB Express 10:101. https://doi.org/10.1186/s13568-020-01038-y
Lee NY, Shin MJ, Youn GS, Yoon SJ, Choi YR, Kim HS, Gupta H, Han SH, Kim BK, Lee DY, Park TS, Sung H, Kim BY, Suk KT (2021) Lactobacillus attenuates progression of nonalcoholic fatty liver disease by lowering cholesterol and steatosis. Clin Mol Hepatol 27:110–124. https://doi.org/10.3350/cmh.2020.0125
Lee NY, Yoon SJ, Han DH, Gupta H, Youn GS (2020) Lactobacillus and Pediococcus ameliorate progression of non-alcoholic fatty liver disease through modulation of the gut microbiome. Gut Microbes 11:882–899. https://doi.org/10.1080/19490976.2020.1712984
Bakhshimoghaddam F, Shateri K, Sina M, Hashemian M, Alizadeh M (2018) Daily consumption of synbiotic yogurt decreases liver steatosis in patients with nonalcoholic fatty liver disease: a randomized controlled clinical trial. J Nutr 148:1276–1284. https://doi.org/10.1093/jn/nxy088
Javadi L, Khoshbaten M, Safaiyan A, Ghavami M, Abbasi MM, Gargari BP (2018) Pro- and prebiotic effects on oxidative stress and inflammatory markers in non-alcoholic fatty liver disease. Asia Pac J Clin Nutr 27:1031–1039. https://doi.org/10.6133/apjcn.042018.05
Javadi L, Ghavami M, Khoshbaten M, Safaiyan A, Barzegari A, Pourghassem Gargari B (2017) The effect of probiotic and/or prebiotic on liver function tests in patients with nonalcoholic fatty liver disease: a double blind randomized clinical trial. Iran Red Crescent Med J 19:e46017. https://doi.org/10.5812/ircmj.46017
Asgharian A, Askari G, Esmailzade A, Feizi A, Mohammadi V (2016) The effect of symbiotic supplementation on liver enzymes, C-reactive protein and ultrasound findings in patients with non-alcoholic fatty liver disease: a clinical trial. Int J Prev Med 7:59. https://doi.org/10.4103/2008-7802.178533
Mofidi F, Poustchi H, Yari Z, Nourinayyer B, Merat S, Sharafkhah M, Malekzadeh R, Hekmatdoost A (2017) Synbiotic supplementation in lean patients with non-alcoholic fatty liver disease: a pilot, randomised, double-blind, placebo-controlled, clinical trial. Br J Nutr 117:662–668. https://doi.org/10.1017/S0007114517000204
Scorletti E, Afolabi PR, Miles EA, Smith DE, Almehmadi A, Alshathry A, Childs CE, Del Fabbro S, Bilson J, Moyses HE, Clough GF, Sethi JK, Patel J, Wright M, Breen DJ, Peebles C, Darekar A, Aspinall R, Fowell AJ, Dowman JK, Nobili V, Targher G, Delzenne NM, Bindels LB, Calder PC, Byrne CD (2020) Synbiotics alter fecal microbiomes, but not liver fat or fibrosis, in a randomized trial of patients with nonalcoholic fatty liver disease. Gastroenterology 158:1597-1610.e1597. https://doi.org/10.1053/j.gastro.2020.01.031
Javadi L, Ghavami M, Khoshbaten M, Safaiyan A, Barzegari A, Gargari BP (2017) The effect of probiotic and/or prebiotic on liver function tests in patients with nonalcoholic fatty liver disease: a double blind randomized clinical trial. Iran Red Crescent Med J 19:e46017. https://doi.org/10.5812/ircmj.46017
Malaguarnera M, Vacante M, Antic T, Giordano M, Chisari G, Acquaviva R, Mastrojeni S, Malaguarnera G, Mistretta A, Li Volti G, Galvano F (2012) Bifidobacterium longum with fructo-oligosaccharides in patients with non alcoholic steatohepatitis. Dig Dis Sci 57:545–553. https://doi.org/10.1007/s10620-011-1887-4
Eslamparast T, Poustchi H, Zamani F, Sharafkhah M, Malekzadeh R, Hekmatdoost A (2014) Synbiotic supplementation in nonalcoholic fatty liver disease: a randomized, double-blind, placebo-controlled pilot study. Am J Clin Nutr 99:535–542. https://doi.org/10.3945/ajcn.113.068890
Daubioul C, Horsmans Y, Lambert P, Danse E, Delzenne NM (2005) Effects of oligofructose on glucose and lipid metabolism in patients with nonalcoholic steatohepatitis: results of a pilot study. Eur J Clin Nutr 59:723–726. https://doi.org/10.1038/sj.ejcn.1602127
Farhangi MA, Javid AZ, Dehghan P (2016) The effect of enriched chicory inulin on liver enzymes, calcium homeostasis and hematological parameters in patients with type 2 diabetes mellitus: a randomized placebo-controlled trial. Prim Care Diabetes 10:265–271. https://doi.org/10.1016/j.pcd.2015.10.009
Acknowledgements
We would like to thank Editage (www.editage.co.kr) for English language editing.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (NRF-2020R1I1A3072840).
Author information
Authors and Affiliations
Contributions
VV and YMK collected information and wrote the review article. MJC conceptualized and reviewed the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vu, V., Kim, Y. & Cho, M. Effects of SCFAs and TMAO on non-alcoholic fatty liver disease indicating the therapeutic benefits of plant-based diet, and supplemental prebiotics, probiotics and synbiotics. Appl Biol Chem 66, 11 (2023). https://doi.org/10.1186/s13765-022-00755-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13765-022-00755-1