
Abstract
Background
During incremental exercise (Inc-Ex), the mean response time (MRT) of oxygen uptake (V̇O2) represents the time delay before changes in muscle V̇O2 reflect at the mouth level. MRT calculation by linear regression or monoexponential (τ’) fitting of V̇O2 data are known to be highly variable, and a combination of incremental and constant load exercise (CL-Ex) is more reproducible.
Methods
We evaluated MRT in older adults using linear regression and combination methods. We recruited 20 healthy adults (male: 9, 69.4 ± 6.8 years) and 10 cardiovascular risk subjects (male: 8, 73.0 ± 8.8 years). On day 1, they performed Inc-Ex using a 10W/min ramp protocol, for determination of the ventilatory anaerobic threshold (VAT) using the V-slope method. On day 2, they performed Inc-Ex to VAT exercise intensity and CL-Ex for 25min total. The MRT was calculated from the CL-Ex V̇O2 average and the time at equivalent V̇O2 in the Inc-Ex. We also assessed the amount of physical activity using the International Physical Activity Questionnaire short form (IPAQ-SF).
Results
The MRT of healthy participants and those at cardiovascular risk were 49.2 ± 36.3 vs. 83.6 ± 45.4s (p = 0.033). Total physical activity in the IPAQ-SF was inversely correlated with MRT.
Conclusion
The MRT was significantly prolonged in cardiovascular risk participants compared to healthy participants, possibly related to the amount of daily physical activity. Individual MRT may be useful for adjustment of exercise intensity, but this should also be based on daily physical activity and individual condition during exercise.
Similar content being viewed by others

Introduction
For accurate exercise prescription and cardiorespiratory health assessment, cardiopulmonary exercise testing (CPET) has become the gold standard protocol in research and clinical practice for quantifying main aerobic parameters (e.g., maximal V̇O2peak [peak oxygen uptake], ventilatory anaerobic threshold [VAT] and respiratory compensation point [RCP]) [1]. These incremental-derived parameters are then used as reference metrics to prescribe exercise intensity for individuals with cardiovascular disease and a variety of other medical conditions, including obesity and hypertension [2]. For example, exercise intensity in cardiac rehabilitation is often prescribed to be within 50–80% of VO2peak or 40–85% of VAT [3,4,5,6].
During incremental exercise, oxygen uptake (V̇O2) measured at the level of the mouth increases linearly with the power output after an initial time interval, the mean response time (MRT) [7], due to a delay in biological response. This includes both the transit delay for deoxygenated blood from exercising muscles to reach the lungs and the kinetic component of muscle V̇O2 adapting to the increased demand for adenosine triphosphate due to exercise (oxygen transfer capacity and mitochondrial function) [8,9,10,11,12].
MRT is generally calculated by monoexponential (τ’) fitting or linear regression of V̇O2 data. The time constant “τ” indicates 63.2% of the time it takes for oxygen uptake to reach a steady state during exercise at a constant load intensity [13, 14]. This time constant “τ” is prolonged in patients with heart failure [15]. The method of linear regression is defined as the time from a steady state of warm-up oxygen uptake to the beginning of incremental exercise load and the start of a gradual increase in oxygen uptake. This has been shown to be influenced by the intensity of warm-up and incremental exercise [16, 17]. Furthermore, both methods lack reproducibility [12, 18, 19]. The exercise intensity for exercise therapy in cardiac rehabilitation may also be corrected to account for this biological response delay (approximately 1min before that intensity) [20]. However, few reports have examined MRT to a given exercise intensity as a basis for exercise prescription with the 1-min pre-correction that is used as a rough approximation [13, 21].
Recently, a new method for obtaining reproducible MRT has been reported by Iannetta et al. [22]. This new method combining constant and incremental load exercise was able to reduce the effects of baseline before the incremental load and ΔVO2/Δpower output [22]. We hypothesized that this method could be used to calculate MRT in the older population and patients at cardiovascular risk and that patients at cardiovascular risk would have a prolonged MRT compared to healthy older participants. Therefore, the purpose of this study was to determine the extent of MRT, defined as the difference in response time between an incremental exercise and a constant load exercise, in older healthy participants and patients with cardiovascular risk.
Methods
The study included a total of 30 participants, and all participants were between the ages of 60 and 80 years. We recruited 10 patients on medication for cardiovascular diseases (n = 5) or cardiovascular risk factors (n = 5) (risk group, age: 73.0 ± 8.8 years). Cardiovascular disease etiologies included post-coronary artery bypass graft surgery (n = 2), myocardial infarction (n = 1), and valvular heart disease (n = 2). Cardiovascular risk factors included hypertension (n = 10), impaired glucose tolerance or diabetes mellitus (n = 1), and hyperlipidemia (n = 6). Twenty healthy individuals matched for age (healthy group, age: 69.4 ± 6.8 years) were recruited for comparison (Table1). To estimate the daily activity levels of the participants, the International Physical Activity Questionnaire (IPAQ) short form was administered [23].
Data are presented as mean ± S.D. Obesity is defined as BMI > 25kg/m2. Significant differences in clinical characteristics such as age, BMI, and physical activity (measured by the IPAQ-SF) were not observed between healthy and patient groups. CTR, cardio-thoracic ratio; BMI, body mass index; BNP, brain natriuretic peptide; LAD, left atrial diameter; LVDd, left ventricular diastolic diameter; LVDs, left ventricular systolic diameter; LVEF, left ventricular ejection fraction; E/A ratio, the peak early diastolic filling velocity/the peak atrial filling velocity ratio; IPAQ-SF, international physical activity questionnaire–short form; MET, metabolic equivalent.
Exclusion criteria included changes in medication within six months, infection within two weeks, chronic atrial fibrillation or flutter, permanent pacemaker, and presence of orthopedic conditions that rendered the individual unfit for exercise testing. In addition, we excluded participants who took warfarin, other anticoagulants, or metformin for diabetes.
Echocardiography and blood samples were measured prior to the day 1 incremental exercise testing. Left ventricular ejection fraction (LVEF) was obtained by Teichholz method. Brain natriuretic peptide (BNP) was determined by chemiluminescent enzyme immunoassay.
The cases and measurement records for this study were taken from participants in our previous article [24].
Ethical considerations
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and was approved by the ethical committee of Sapporo Ryokuai Hospital (approval number: 19–1). Informed consent was obtained from all participants for their participation in the study and for the publication of this report.
Exercise testing
CPET was performed using a stationary bicycle (Strength Ergo 8; Mitsubishi Electric Engineering, Tokyo, Japan) and a breath-by-breath gas analyzer (AE-300S; Minato Ikagaku Co., Tokyo, Japan). Exercise tests were conducted on two separate days (mean interval between the 1st- and 2nd-day tests: 4.1 ± 2.3 days). On day 1, symptomatic maximal exercise was performed using a ramp protocol of 10W/min (Inc-Ex) for VAT determination. On day 2, Inc-Ex was performed using a ramp protocol of 10W/min up to the VAT point, after which a constant load at the VAT level work rate was initiated and maintained for a total exercise duration of approximately 25min (Fig.1). Before the experiment, the total duration of the exercise (Inc-Ex + CL-Ex) on day 2 was planned to be 25min for each participant. The duration of Inc-Ex varied among participants due to different VAT levels. Consequently, the mean Inc-Ex duration was 3.2 ± 1.1min and the mean CL-Ex duration was 21.8 ± 1.1min. Thus, all graphs, tables, and text denoting 25min of CL-Ex represent approximately 22min of CL-Ex. Warm-up exercises were performed for 2min at 10W. We used 10-s average data for all analyses. This exercise testing protocol has been published previously [24].

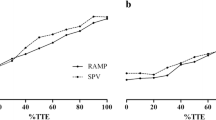
Diagram of Mean Response Time Calculation. (A) (upper panel) shows V̇O2 during incremental and constant exercise load in a sample case. Rest, warm-up, and a ramp protocol of 10W/min (Ramp10) on day 1 was followed on day 2 by constant load exercise for a total of 25min. (B) (lower panel) shows a diagram of the MRT calculation. The difference in oxygen uptake from VAT on day 1 to V̇O2 steady state (20–25min) on day 2 was defined as ΔV̇O2 ① (ΔV̇O2 after VAT). The difference in oxygen uptake from the day 1 VAT to the earlier MRT was defined as ΔV̇O2 ② (ΔV̇O2 before VAT). VAT – ventilatory anaerobic threshold; V̇O2 – oxygen uptake
Ventilatory anaerobic threshold
We determined the VAT during Inc-Ex testing on day 1 to determine the CL-Ex work rate on day 2. The VAT was visually determined using the modified V-slope method as described by Sue et al. [25], which is a modification of the method described by Beaver et al. [26]. The details of this method have been published previously [27, 28].In summary, this V-slope method involves drawing a line through the data points parallel to the respiratory exchange ratio (RER) = 1 diagonal, which is referred to as the pre-VAT baseline (S1). The point at which the data begin to deflect toward the left is selected as the VAT. The data points preceding the parallel line were disregarded. A line drawn parallel to the RER = 1 diagonal signifies a change of 1.0 in the rate of ΔV̇CO2/ΔV̇O2. Therefore, the point at which this index begins to increase above 1.0 is the VAT deflection point [27, 28]. Previous studies included actual readings of the VAT for each analyzed case. We used this approach in our study to identify the VAT.
Calculation of MRT (Fig.1)
We calculated the MRT from the oxygen uptake of the incremental and constant load exercises (Inc-Ex and CL-Ex, respectively) following the method of Iannetta et al. (MRT1) [22]. We calculated the oxygen uptake for 20–25min during CL-Ex and defined MRT1 as the difference between the time to achieve this same oxygen uptake and the time to the VAT during Inc-Ex. The difference in oxygen uptake before and after MRT1 based on VAT was also calculated during incremental exercise testing. Detailed exercise testing results such as V̇O2 and HR have been published previously [24].
In addition, we also calculated the method by linear regression (MRT2). Referring to previous studies, MRT2 was calculated from the intersection of oxygen uptake at warm-up and the linear regression equation of oxygen uptake from the start of increased oxygen uptake to VAT during incremental exercise testing [16, 17].
Statistical analysis
Data are presented as mean ± SD and 95% confidence interval. All data were assessed for normality by the Shapiro-Wilk test before analysis. Within group comparisons, such as MRT1 and MRT2, and ΔV̇O2 before and after VAT, were made using a paired t-test. Comparisons between groups in the healthy and at-risk groups were performed using the student t-test. Correlation of total metabolic equivalents (METs) in IPAQ-short form and MRT1 was performed using Pearson’s correlation. P < 0.05 was considered to indicate statistical significance.
Statistical analyses were performed with Statistics for Excel 2012 (Social Survey Research Information Co., Tokyo, Japan).
Results
The clinical characteristics of the participants are summarized in Table1. Compared to the healthy group, the cardiovascular risk group had a higher proportion of men, resulting in significantly higher height and body weight (p = 0.016, p = 0.007, respectively). The total MET minutes per week according to the IPAQ-SF was not significantly different between the healthy and risk groups (p = 0.119). This result is similar to the average of a broader healthy Japanese population in the same age range [29]. MRT1 could be calculated in all cases.
MRT - combined calculation of incremental and constant load exercise
MRT1 was 60.7 ± 42.1 sec(95% CI: 45.6–75.8) in all participants, 49.2 ± 36.3 sec(95% CI: 33.3–65.1) in the healthy group, and 83.6 ± 45.4 sec(95% CI: 55.4–111.7) in the risk group. The risk group had a significantly prolonged MRT compared with the healthy group (p = 0.033) (Fig.2).

Mean Response Time. The mean response time (MRT) for each group is shown. Green markers indicate individual mean response times for all cases. Blue markers indicate individual mean response times for the healthy group and red markers indicate individual mean response times for the cardiovascular risk group. Patients with cardiovascular risk had significantly prolonged MRT compared to healthy adults
Differences in MRT by calculation method
In the healthy group, MRT1 and MRT2 were not significantly different and not correlated (49.2 ± 36.3 vs. 46.8 ± 16.1sec, p = 0.797, r=−0.149, p = 0.681). On the other hand, in the risk group, MRT2 was significantly lower than MRT1, but no correlation was found (83.6 ± 45.4 vs. 26.4 ± 23.9sec, p = 0.010, r = 0.269, p = 0.451).
Differences in ΔV̇O2 before and after VAT
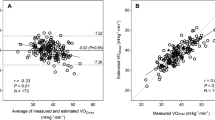
ΔV̇O2 before and after MRT with respect to VAT showed a significant correlation, but was significantly higher in the risk group (all patients: 91.3 ± 62.2 vs. 97.8 ± 70.1 ml‣min-1, p = 0.051, healthy group: 80.2 ± 53.9 vs. 82.2 ± 61.7ml‣min-1, p = 0.573, risk group. 113.5 ± 74.2 vs. 129.0 ± 78.8ml‣min-1, p = 0.028, Fig.3).

ΔV̇O2 before and after VAT. The left figure (A) shows all cases (green) and the right figure (B) shows pre- and post-VAT ΔV̇O2 for each group (healthy group: blue; risk group: red). The x-axis shows ΔV̇O2 after VAT and the y-axis shows ΔV̇O2 before VAT. Dotted lines indicate 95% confidence intervals for each group in their associated color. ΔV̇O2 showed a significant correlation in both groups. Patients with cardiovascular risk had significantly higher ΔV̇O2 compared to healthy adults. VAT – ventilatory anaerobic threshold. V̇O2 – oxygen uptake
Relationship between daily physical activity and MRT
Daily physical activity and MRT showed a negative correlation (healthy group: r=−0.522, p = 0.018, risk group: r=−0.603, p = 0.065). In both groups, the higher the daily physical activity level, the shorter the MRT tended to be (Fig.4).

Relationship between mean response time and physical activity. Physical activity (in metabolic equivalents, METs) was calculated using the responses from the International Physical Activity Questionnaire short form (IPAQ-SF). Mean response time (MRT) tended to shorten in both groups (healthy group: blue; risk group: red) as activity level increased
Discussion
Quantification of the MRT is paramount for assigning the correct load to the VAT [13, 21]. This study examined MRT, calculated using a method recently developed by Iannetta et al. [22], in a cardiovascular disease population and healthy age-matched controls. Furthermore, we compared this method against other methods that had been traditionally used in research settings (i.e., back extrapolation linear approach). The results showed that the MRT was significantly prolonged in cardiovascular disease patients when compared to controls individuals. Furthermore, there was no correlation between the MRT quantified with the novel method proposed by Iannetta et al. [22] and the back extrapolation linear approach. This means that for greater accuracy, MRT should be calculated using this novel method.
The results of this study showed that older adults with cardiovascular risk had a prolonged MRT compared to healthy older adults. Compared to previous studies, MRT was also prolonged in healthy young adults and athletes [9]. MRT may be prolonged due to multiple factors.
MRT is related to circulatory delay, pulmonary gas exchange and the oxygen uptake response of exercising muscle and increased ATP demand due to incremental exercise [22, 30]. Adequate blood flow to exercising muscles may also be relevant for MRT [8, 10]. Cardiac dysfunction such as hypertensive heart disease [31, 32], right ventricle heart failure [14, 33], left ventricular diastolic dysfunction [34,35,36], atherosclerotic diseases such as diabetes [37, 38], decreased physical activity [39], and age-related changes [39,40,41] are believed to produce a delayed or decreased cardiovascular response during exercise. Furthermore, it is reported that in pulmonary diseases, such as COPD, dynamic lung hyperinflation and pulmonary gas exchange limitation may occur [30].
In the present study, MRT was significantly prolonged in the risk group with comorbidities known to produce atherosclerosis, although there was no apparent decline in cardiac function. In addition, physical inactivity [42, 43], age-related changes [44], and comorbidities [45, 46] are believed to decrease mitochondrial function and ATP synthesis capacity. In this study, physical inactivity was shown to be associated with prolonged MRT. Although this study was not able to sufficiently investigate the possibility, it cannot be ruled out that the patients may have had coexisting pulmonary diseases, such as COPD. Altogether, these factors may have contributed to a prolonged MRT in patients at cardiovascular risk compared to healthy adults.
We used two methods to calculate MRT in this study: the method used in previous studies, which is based on a combination of incremental and constant load exercise, and a method based on a linear regression equation. In previous studies, the calculation of MRT by the linear regression equation was related to the intensity of constant load before the start of the incremental exercise (warming up intensity) and the intensity of ramp exercise [16, 17].
In this study, the ramp loading intensity was 10W/min in all cases, which was similar to the intensity of ramp exercise shown in previous studies. Conversely, although all cases of constant load exercise were standardized at 10W, the warm-up period was 2min, which may have been too short for oxygen uptake to reach a steady state. This may have affected the MRT calculated using the linear regression equation and its correlation with the MRT calculated by the combination method.
ΔV̇O2 was significantly higher in the cardiovascular risk group. The risk group had a higher initial ΔV̇O2, which may be related to the prolonged MRT. ΔV̇O2 before and after VAT was correlated very strongly in both groups and was almost the same within the groups. However, the risk group was significantly higher, albeit slightly. The degree of increase in oxygen uptake in response to incremental exercise intensity depends on the setting of the individual exercise intensity (the increase in oxygen uptake slows down with increasing exercise intensity when the incremental exercise intensity is high) [47]. Additionally, the slow component of oxygen uptake increases with exercise intensity greater than VAT [48, 49]. In the present study, MRT was prolonged and ΔV̇O2 after VAT was greater in the risk group, suggesting that the slow component may have had an effect. This may also be related to the amount of physical activity and other factors which interact with prolonged MRT [50].
Correction of exercise prescription is recommended to account for a delayed biological response and tailor to the individual [3, 51]. The results of this study showed that the average MRT in the cardiovascular risk group was actually prolonged beyond 1min, which would be easy to recommend as a simple correction. However, the range of MRT is large, so this may not be directly accurate without individual testing. As reported in our previous studies, oxygen uptake at constant load exercise in VAT intensity was around 60% V̇O2 peak, well within the range of some guidelines [6, 52, 53]. Therefore, it would not be easy to overload beyond VAT. Based on the results of this study, when setting exercise intensity for exercise therapy, it is recommended that MRT should be calculated using this novel method for greater accuracy.
Limitations
This study had some limitations. First, although it was clear that MRT was prolonged in patients with cardiovascular risk, the overall number of cases, especially in the risk group, was small, and disease specificity due to comorbidities was unclear. It is uncertain to what extent comorbidities such as hypertension and diabetes would alter MRT.
Second, the study population was not composed of patients with myocardial infarction or heart failure who were indicated for cardiac rehabilitation. MRT may be further prolonged in conditions that cause circulatory delay.
In summary, older participants with cardiovascular risk had a prolonged mean MRT compared to healthy older participants. This MRT prolongation may be linked to the impaired oxygen cascade in patients with cardiovascular disease. When setting exercise intensity for exercise therapy, we recommend that, for greater accuracy, the MRT should be calculated using this novel method.
Data Availability
The dataset used in the current study is available from the corresponding author on request.
Abbreviations
- GET:
-
gas exchange threshold.
- VAT:
-
ventilatory anaerobic threshold.
- Inc-Ex:
-
incremental exercise.
- CL-Ex:
-
constant load exercise.
- CPET:
-
Cardiopulmonary exercise testing.
- V̇O2 :
-
Oxygen uptake.
- V̇CO2 :
-
carbon dioxide production.
- RER:
-
respiratory exchange ratio.
- MRT:
-
mean response time.
- IPAQ:
-
International Physical Activity Questionnaire.
- LVEF:
-
Left ventricular ejection fraction.
- BNP:
-
Brain natriuretic peptide.
- ANOVA:
-
A repeated one-way analysis of variance.
References
Iannetta D, Keir DA, Fontana FY, Inglis EC, Mattu AT, Paterson DH, Pogliaghi S, Murias JM. Evaluating the Accuracy of Using Fixed Ranges of METs to Categorize Exertional Intensity in a Heterogeneous Group of Healthy Individuals: Implications for Cardiorespiratory Fitness and Health Outcomes. Sports Med. 2021;51:2411–21. doi:https://doi.org/10.1007/s40279-021-01476-z. Epub 2021 Apr 26. PMID: 33900580.
Deborah R, Jonathan KE, Gary L, Meir. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription Tenth edition. Philadelphia: Wolters Kluwe; 2018.
Mezzani A, Hamm LF, Jones AM, McBride PE, Moholdt T, Stone JA, et al. European Association for Cardiovascular Prevention and Rehabilitation; American Association of Cardiovascular and Pulmonary Rehabilitation; Canadian Association of Cardiac Rehabilitation. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: a joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian Association of Cardiac Rehabilitation. Eur J Prev Cardiol. 2013;20:442–67. doi: 10.1177/2047487312460484. Epub 2012 Oct 26. PMID: 23104970.
Bjarnason-Wehrens B, Nebel R, Jensen K, Hackbusch M, Grilli M, Gielen S, Schwaab B, Rauch B, German Society of Cardiovascular Prevention and Rehabilitation (DGPR). Exercise-based cardiac rehabilitation in patients with reduced left ventricular ejection fraction: The Cardiac Rehabilitation Outcome Study in Heart Failure (CROS-HF): A systematic review and meta-analysis. Eur J Prev Cardiol. 2020;27:929–52. doi: 10.1177/2047487319854140. Epub 2019 Jun 8. PMID: 31177833; PMCID: PMC7272131.
JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ J.. 2014;78:2022-93. doi: https://doi.org/10.1253/circj.cj-66-0094. PMID: 25047729.
Hansen D, Abreu A, Ambrosetti M, Cornelissen V, Gevaert A, Kemps H, Laukkanen JA, Pedretti R, Simonenko M, Wilhelm M, Davos CH, Doehner W, Iliou MC, Kränkel N, Völler H, Piepoli M. Exercise intensity assessment and prescription in cardiovascular rehabilitation and beyond: why and how: a position statement from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2022;29:230–245. doi: https://doi.org/10.1093/eurjpc/zwab007. PMID: 34077542.
Whipp BJ, Davis JA, Torres F, Wasserman K. A test to determine parameters of aerobic function during exercise. J Appl Physiol Respir Environ Exerc Physiol. 1981;50:217–221. doi: https://doi.org/10.1152/jappl.1981.50.1.217. PMID: 6782055.
Poole DC, Jones AM. Oxygen uptake kinetics. Compr Physiol. 2012;2(2):933–996. doi: https://doi.org/10.1002/cphy.c100072. PMID: 23798293.
Boone J, Bourgois J. The oxygen uptake response to incremental ramp exercise: methodogical and physiological issues. Sports Med. 2012;42:511–526. doi: https://doi.org/10.2165/11599690-000000000-00000. PMID: 22571502.
Burtscher M. Exercise limitations by the oxygen delivery and utilization systems in aging and disease: coordinated adaptation and deadaptation of the lung-heart muscle axis - a mini-review. Gerontology. 2013;59:289–96. doi: 10.1159/000343990. Epub 2012 Nov 24. PMID: 23182831.
Keir DA, Paterson DH, Kowalchuk JM, Murias JM. Using ramp-incremental V̇O2 responses for constant-intensity exercise selection. Appl Physiol Nutr Metab. 2018;43:882–892. doi: https://doi.org/10.1139/apnm-2017-0826. Epub 2018 Mar 23. PMID: 29570982.
Poole DC, Rossiter HB, Brooks GA, Gladden LB. The anaerobic threshold: 50 + years of controversy. J Physiol. 2021;599:737–767. doi: 10.1113/JP279963. Epub 2020 Nov 19. PMID: 33112439.
Koike A, Yajima T, Adachi H, Shimizu N, Kano H, Sugimoto K, Niwa A, Marumo F, Hiroe M. Evaluation of exercise capacity using submaximal exercise at a constant work rate in patients with cardiovascular disease. Circulation. 1995;91:1719–1724. doi: https://doi.org/10.1161/01.cir.91.6.1719. PMID: 7882479.
Chatterjee NA, Murphy RM, Malhotra R, Dhakal BP, Baggish AL, Pappagianopoulos PP, Hough SS, Semigran MJ, Lewis GD. Prolonged mean V̇O2 response time in systolic heart failure: an indicator of impaired right ventricular-pulmonary vascular function. Circ Heart Fail. 2013;6:499–507. doi: 10.1161/CIRCHEARTFAILURE.112.000157. Epub 2013 Apr 9. PMID: 23572493; PMCID: PMC5935663.
Hearon CM Jr, Sarma S, Dias KA, Hieda M, Levine BD. Impaired oxygen uptake kinetics in heart failure with preserved ejection fraction. Heart. 2019;105:1552–8. doi:https://doi.org/10.1136/heartjnl-2019-314797. Epub 2019 Jun 17. PMID: 31208971.
Swanson GD, Hughson RL. On the modeling and interpretation of oxygen uptake kinetics from ramp work rate tests. J Appl Physiol (1985). 1988;65:2453–2458. doi: https://doi.org/10.1152/jappl.1988.65.6.2453. PMID: 3215845.
Boone J, Koppo K, Bouckaert J. The V̇O2 response to submaximal ramp cycle exercise: Influence of ramp slope and training status. Respir Physiol Neurobiol. 2008;31:161:291–7. doi:https://doi.org/10.1016/j.resp.2008.03.008. Epub 2008 Mar 26. PMID: 18448396.
Hughson RL, Inman MD. Oxygen uptake kinetics from ramp work tests: variability of single test values. J Appl Physiol. 1986;61:373–6.
Markovitz GH, Sayre JW, Storer TW, Cooper CB. On issues of confidence in determining the time constant for oxygen uptake kinetics. Br J Sports Med. 2004;38:553–60.
The Japanese Association of Cardiac Rehabilitation, Standard Cardiac Rehabilitation Program Writing Committee. Cardiac Rehabilitation Standard Program for Acute Myocardial Infarction. (2013) from the Japanese Association of Cardiac Rehabilitation - In the Recovery Phase of Myocardial Infarction -. Retrieved April 19, 2022 from https://www.jacr.jp/web/en/standard-program/.
Koike A, Hiroe M, Adachi H, Yajima T, Yamauchi Y, Nogami A, Ito H, Miyahara Y, Korenaga M, Marumo F. Oxygen uptake kinetics are determined by cardiac function at onset of exercise rather than peak exercise in patients with prior myocardial infarction. Circulation 1994;90:2324–2332. doi: https://doi.org/10.1161/01.cir.90.5.2324. PMID: 7955190.
Iannetta D, Murias JM, Keir DA. A Simple Method to Quantify the V̇O2 Mean Response Time of Ramp-Incremental Exercise. Med Sci Sports Exerc. 2019;51:1080–1086. doi: https://doi.org/10.1249/MSS.0000000000001880. PMID: 30601794.
Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. 2011;8:115. doi:https://doi.org/10.1186/1479-5868-8-115. Pubmed PMID: 22018588. Pubmed Central PMCID: PMC3214824.
Kominami K, Nishijima H, Imahashi K, Katsuragawa T, Murakami M, Akino M. Gas exchange threshold to guide exercise training intensity of older individuals during cardiac rehabilitation. Med (Baltimore). 2021;100:e27540. doi:https://doi.org/10.1097/MD.0000000000027540. PMID: 34678888; PMCID: PMC8542148.
Sue DY, Wasserman K, Moricca RB, Casaburi R. Metabolic acidosis during exercise in patients with chronic obstructive pulmonary disease. Use of the V-slope method for anaerobic threshold determination. Chest. 1988;94:931–8. Pubmed PMID: 3180897.
Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol (1985). 1986;60:2020–7. Pubmed PMID: 3087938.
Nishijima H, Kominami K, Kondo K, Akino M, Sakurai M. New method for the mathematical derivation of the ventilatory anaerobic threshold: a retrospective study. BMC Sports Sci Med Rehabil. 2019;11:10. doi:https://doi.org/10.1186/s13102-019-0122-z. PMID: 31285827. Pubmed Central PMCID: PMC6592010.
Nishijima H, Kondo K, Yonezawa K, Hashimoto H, Sakurai M. Quantification and physiological significance of the rightward shift of the V-slope during incremental cardiopulmonary exercise testing. BMC Sports Sci Med Rehabil. 2017;9:9. doi:https://doi.org/10.1186/s13102-017-0073-1. PMID: 28435685. Pubmed Central PMCID: PMC5397810.
Tomioka K, Iwamoto J, Saeki K, Okamoto N. Reliability and validity of the International Physical Activity Questionnaire (IPAQ) in elderly adults: the Fujiwara-kyo study. J Epidemiol. 2011;21:459–65. doi:https://doi.org/10.2188/jea.je20110003. Pubmed PMID: 21946625. Pubmed Central PMCID: PMC3899462.
Rossiter HB. Exercise: Kinetic considerations for gas exchange. Compr Physiol. 2011;1:203–244. doi: https://doi.org/10.1002/cphy.c090010. PMID: 23737170.
Barmeyer A, Müllerleile K, Mortensen K, Meinertz T. Diastolic dysfunction in exercise and its role for exercise capacity. Heart Fail Rev. 2009;14:125–34. doi:https://doi.org/10.1007/s10741-008-9105-y. Epub 2008 Aug 29. PMID: 18758943.
Mitchell JH. Abnormal cardiovascular response to exercise in hypertension: contribution of neural factors. Am J Physiol Regul Integr Comp Physiol 2017;312:R851-R863. doi: https://doi.org/10.1152/ajpregu.00042.2017. Epub 2017 Apr 5. PMID: 28381455.
Hultgren HN. The effect of increased venous return on the venous pressure in patients with congestive heart failure. Am Heart J. 1950;39:592–603. doi: https://doi.org/10.1016/0002-8703(50)90256-0. PMID: 15410663.
Alonso-Gómez AM, Tojal Sierra L, Fortuny Frau E, Goicolea Güemez L, Aboitiz Uribarri A, Portillo MP, Toledo E, Schröder H, Salas-Salvadó J, Arós Borau F. Diastolic dysfunction and exercise capacity in patients with metabolic syndrome and overweight/obesity. Int J Cardiol Heart Vasc. 2018;22:67–72. doi: 10.1016/j.ijcha.2018.12.010. PMID: 30619930; PMCID: PMC6314243.
Grewal J, McCully RB, Kane GC, Lam C, Pellikka PA. Left ventricular function and exercise capacity. JAMA. 2009;301:286–94. doi:https://doi.org/10.1001/jama.2008.1022. PMID: 19155455; PMCID: PMC2862454.
Lee JF, Barrett-O’Keefe Z, Nelson AD, Garten RS, Ryan JJ, Nativi-Nicolau JN, Richardson RS, Wray DW. Impaired skeletal muscle vasodilation during exercise in heart failure with preserved ejection fraction. Int J Cardiol. 2016;211:14–21. doi:https://doi.org/10.1016/j.ijcard.2016.02.139. Epub 2016 Mar 2. PMID: 26970959; PMCID: PMC4834272.
Vinik AI, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation. 2007;115:387–397. doi: https://doi.org/10.1161/CIRCULATIONAHA.106.634949. PMID: 17242296.
Green S, Egaña M, Baldi JC, Lamberts R, Regensteiner JG. Cardiovascular control during exercise in type 2 diabetes mellitus. J Diabetes Res. 2015;2015:654204. doi: 10.1155/2015/654204. Epub 2015 Mar 30. PMID: 25918732; PMCID: PMC4396731.
Olive JL, DeVan AE, McCully KK. The effects of aging and activity on muscle blood flow. Dyn Med. 2002;1:2. doi: https://doi.org/10.1186/1476-5918-1-2. Erratum in: Dyn Med. 2003 Jul 8;2(1):3. PMID: 12605712; PMCID: PMC150384.
Hearon CM Jr, Dinenno FA. Regulation of skeletal muscle blood flow during exercise in ageing humans. J Physiol. 2016;594:2261–22273. doi: 10.1113/JP270593. Epub 2015 Nov 2. PMID: 26332887; PMCID: PMC4933119.
Behnke BJ, Ramsey MW, Stabley JN, Dominguez JM 2nd, Davis RT 3rd, McCullough DJ, Muller-Delp JM, Delp MD. Effects of aging and exercise training on skeletal muscle blood flow and resistance artery morphology. J Appl Physiol (1985). 2012;113:1699–708. doi: 10.1152/japplphysiol.01025.2012. Epub 2012 Oct 4. PMID: 23042906; PMCID: PMC3544508.
Brierley EJ, Johnson MA, James OF, Turnbull DM. Effects of physical activity and age on mitochondrial function. QJM. 1996;89:251–258. doi: https://doi.org/10.1093/qjmed/89.4.251. PMID: 8733511.
Distefano G, Standley RA, Zhang X, Carnero EA, Yi F, Cornnell HH, Coen PM. Physical activity unveils the relationship between mitochondrial energetics, muscle quality, and physical function in older adults. J Cachexia Sarcopenia Muscle. 2018;9:279–94. doi:https://doi.org/10.1002/jcsm.12272. Epub 2018 Jan 24. PMID: 29368427; PMCID: PMC5879963.
Schütt F, Aretz S, Auffarth GU, Kopitz J. Moderately reduced ATP levels promote oxidative stress and debilitate autophagic and phagocytic capacities in human RPE cells. Invest Ophthalmol Vis Sci. 2012;53:5354–5361. doi: https://doi.org/10.1167/iovs.12-9845. PMID: 22789922.
Boudina S, Sena S, O’Neill BT, Tathireddy P, Young ME, Abel ED. Reduced mitochondrial oxidative capacity and increased mitochondrial uncoupling impair myocardial energetics in obesity. Circulation. 2005;112:2686–2695. doi: 10.1161/CIRCULATIONAHA.105.554360. Erratum in: Circulation. 2021 Dec 7;144(23):e489. PMID: 16246967.
Schrauwen P, Hesselink MK. Oxidative capacity, lipotoxicity, and mitochondrial damage in type 2 diabetes. Diabetes. 2004;53:1412–1417. doi: https://doi.org/10.2337/diabetes.53.6.1412. PMID: 15161742.
Iannetta D, de Almeida Azevedo R, Keir DA, Murias JM. Establishing the V̇o2 versus constant-work-rate relationship from ramp-incremental exercise: simple strategies for an unsolved problem. J Appl Physiol (1985). 2019;127:1519–27. doi:https://doi.org/10.1152/japplphysiol.00508.2019. Epub 2019 Oct 3. PMID: 31580218; PMCID: PMC6962604.
Xu F, Rhodes EC. Oxygen uptake kinetics during exercise. Sports Med. 1999;27:313–327. doi: https://doi.org/10.2165/00007256-199927050-00003. PMID: 10368878.
Jones AM, Grassi B, Christensen PM, Krustrup P, Bangsbo J, Poole DC. Slow component of V̇O2 kinetics: mechanistic bases and practical applications. Med Sci Sports Exerc. 2011;43:2046–2062. doi: https://doi.org/10.1249/MSS.0b013e31821fcfc1. PMID: 21552162.
Russell A, Wadley G, Snow R, Giacobino JP, Muzzin P, Garnham A, Cameron-Smith D. Slow component of V̇O2 kinetics: the effect of training status, fibre type, UCP3 mRNA and citrate synthase activity. Int J Obes Relat Metab Disord. 2002;26:157–164. doi: https://doi.org/10.1038/sj.ijo.0801885. PMID: 11850746.
Iannetta D, Inglis EC, Mattu AT, Fontana FY, Pogliaghi S, Keir DA, Murias JM. A Critical Evaluation of Current Methods for Exercise Prescription in Women and Men. Med Sci Sports Exerc. 2020;52:466–473. doi: https://doi.org/10.1249/MSS.0000000000002147. PMID: 31479001.
Mann T, Lamberts RP, Lambert MI. Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med. 2013;43:613–625. doi: https://doi.org/10.1007/s40279-013-0045-x. PMID: 23620244.
Hansen D, Bonné K, Alders T, Hermans A, Copermans K, Swinnen H, Maris V, Jansegers T, Mathijs W, Haenen L, Vaes J, Govaerts E, Reenaers V, Frederix I, Dendale P. Exercise training intensity determination in cardiovascular rehabilitation: Should the guidelines be reconsidered? Eur J Prev Cardiol. 2019;26:1921–8. doi: 10.1177/2047487319859450. Epub 2019 Jun 20. PMID: 31219704.
Acknowledgements
We would like to thank Editage for assistance in English language editing. The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation, and the results of the present study do not constitute endorsement by BMC Sports Science, Medicine, and Rehabilitation.
Author information
Authors and Affiliations
Contributions
KK and MA developed the study concept and were involved in the design and implementation of the study. KK delivered the program content to participants. KK acquired the data. KK analyzed the data. KK prepared the manuscript. MA contributed to drafts of the manuscript and approved the final draft. All authors read and approved the final manuscript.
Funding
This study did not receive any funding support. This work was performed in the Cardiac Rehabilitation Center, Sapporo Ryokuai Hospital, Sapporo, Japan.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and was approved by the Ethical Committee (Institutional Review Board: IRB) of Sapporo Ryokuai Hospital (approval number: 19 − 1). Informed consent was obtained from all participants for their participation in the study and for the publication of this report. The authors confirm that there is no identifying information concerning the participants in the manuscript and that the information has been fully anonymized. Furthermore, the authors affirm that all mandatory health and safety procedures were followed in the course of conducting any experimental work reported in this paper.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Author details
1 Department of Rehabilitation, Sanseikai,6-30, 1-chome,Kitano1-jyo, Kiyota-ku,004–0861, Kitano Hospital, Sapporo, Hokkaido, Japan.
2 Department of Rehabilitation, Sapporo Kiyota Orthopedic Hospital, Sapporo, Hokkaido, Japan
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kominami, K., Akino, M. Prolonged mean response time in older adults with cardiovascular risk compared to healthy older adults. BMC Sports Sci Med Rehabil 14, 173 (2022). https://doi.org/10.1186/s13102-022-00565-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-022-00565-4