
Abstract
Introduction
Lung protective ventilation (LPV) comprising low tidal volume (VT) and high positive end-expiratory pressure (PEEP) may compromise cerebral perfusion in acute brain injury (ABI). In patients with ABI, we investigated whether LPV is associated with increased intracranial pressure (ICP) and/or deranged cerebral autoregulation (CA), brain compensatory reserve and oxygenation.
Methods
In a prospective, crossover study, 30 intubated ABI patients with normal ICP and no lung injury were randomly assigned to receive low VT [6 ml/kg/predicted (pbw)]/at either low (5 cmH2O) or high PEEP (12 cmH2O). Between each intervention, baseline ventilation (VT 9 ml/kg/pbw and PEEP 5 cmH2O) were resumed. The safety limit for interruption of the intervention was ICP above 22 mmHg for more than 5 min. Airway and transpulmonary pressures were continuously monitored to assess respiratory mechanics. We recorded ICP by using external ventricular drainage or a parenchymal probe. CA and brain compensatory reserve were derived from ICP waveform analysis.
Results
We included 27 patients (intracerebral haemorrhage, traumatic brain injury, subarachnoid haemorrhage), of whom 6 reached the safety limit, which required interruption of at least one intervention. For those without intervention interruption, the ICP change from baseline to “low VT/low PEEP” and “low VT/high PEEP” were 2.2 mmHg and 2.3 mmHg, respectively, and considered clinically non-relevant. None of the interventions affected CA or oxygenation significantly. Interrupted events were associated with high baseline ICP (p < 0.001), low brain compensatory reserve (p < 0.01) and mechanical power (p < 0.05).
The transpulmonary driving pressure was 5 ± 2 cmH2O in both interventions. Partial arterial pressure of carbon dioxide was kept in the range 34–36 mmHg by adjusting the respiratory rate, hence, changes in carbon dioxide were not associated with the increase in ICP.
Conclusions
The present study found that most patients did not experience any adverse effects of LPV, neither on ICP nor CA. However, in almost a quarter of patients, the ICP rose above the safety limit for interrupting the interventions. Baseline ICP, brain compensatory reserve, and mechanical power can predict a potentially deleterious effect of LPV and can be used to personalize ventilator settings.
Trial registration NCT03278769. Registered September 12, 2017.
Graphical Abstract

Similar content being viewed by others


Introduction
The optimal ventilator settings are still debated in patients with severe acute brain injury (ABI) admitted to the intensive care unit (ICU) [1,2,3,4]. Lung protective ventilation (LPV) with low tidal volume (VT) and sufficiently high positive end-expiratory pressure (PEEP) to avoid airway collapse is recommended in patients with acute respiratory distress syndrome (ARDS) [5], and may be guided by transpulmonary pressure (TPP) and mechanical power (MP) [6, 7]. Nevertheless, in two recent studies of ICU patients without ARDS, neither the use of different levels of VT nor PEEP, changed patients’ outcome or ventilator-free days [8, 9].
In patients with ABI, lower tidal volumes may improve outcomes [10,11,12]. A recent expert recommendation on mechanical ventilation (MV) in patients with ABI, suggests using LPV in all patients with ABI and normal ICP, including those without ARDS, but has acknowledged the lack of evidence to support this recommendation [4]. The main concern with application of LPV is the increased intrathoracic pressure, reduced venous return and increased ICP through hypoventilation-induced hypercapnia [13]. The latter changes also have the potential to modify cerebral autoregulation (CA).
It is generally accepted that in patients with ABI, monitoring and treatment of the ICP as the only single cerebral parameter is of limited value [14]. By combining monitoring of cerebral oxygenation, ICP and arterial blood pressure (ABP), the application of waveform analysis, can be used to shed light on the brain pathophysiology in critically ill patient [15]. Two indices are of particular interest from the clinical perspective: the cerebrovascular reactivity index (PRx), and the compensatory reserve index (RAP) [16, 17]. PRx represents a surrogate measure of CA, with a positive index indicating loss of vascular reactivity, consistent with impaired autoregulation [18]. RAP can be described as a surrogate index of global cerebral compliance, with the higher the RAP, the lower the intracranial compliance. Moreover, near-infrared spectroscopy (NIRS) might be used to assess regional cerebral oxygen saturation (rSO2) [19].
As a first step, recognizing the need to enrich the evidence behind the recommendations for ventilator management in ABI patients without lung injury, we hypothesized that LPV would not induce significant changes in neuromonitoring-derived variables in this setting, provided that the baseline ICP was less than 22 mmHg. Therefore, the aim was to conduct the brain vent study to investigate the effects of LPV on brain pathophysiology, determined by simultaneous monitoring of TPP, brain oxygenation and indices derived from ICP waveform analysis.
Materials and methods
Study design
Brain vent is as a single centre, randomised, crossover interventional clinical trial, which was approved by the Regional Committee for Medical Research Ethics Northern Norway (2017/1941/REK North). The study was conducted between May 2019 and August 2021 in the ICU of a tertiary trauma and neurosurgery centre, affiliated with the University Hospital of North Norway, Tromsø, Norway. The trial is reported according to the Consort guidelines [20].
An overview of the study procedures and interventions is presented in Fig. 1. The randomisation was performed through the web-based software program Research Electronic Data Capture (RedCap) [21]. Age (≥ 70, < 70) and type of ABI were used to stratify the two groups. To minimise changes in arterial partial pressure of carbon dioxide (PaCO2), minute ventilation was kept as close to the baseline as possible by adjusting the respiratory rate (RR) when VT was changed. Blood gases were sampled after a stabilization period of approximately 30 min after each change in ventilator settings. For safety reasons, the interventions were interrupted if ICP increased above the predefined limit of 22 mmHg for more than 5 min. A healthcare worker blinded to the intervention arm monitored the safety endpoint for the interruption.

Study design: crossover design and intervention settings. Panel A shows the ventilator settings in the different study periods. Panel B shows the randomisation scheme and the study periods. During the baselines, patients were ventilated with VT 9 ml/kg/pbw and PEEP 5 cmH20. Group A was first exposed to “low VT/low PEEP” followed by “low VT/high PEEP”. Group B was subjected to the same interventions in reverse order. The length of the periods was chosen to allow PRx to stabilize and thus display less variance. A washout period with baseline ventilator settings was used to reduce the risk for carry-over effect of the intervention. VT, tidal volume; PEEP, positive end expiratory pressure; h, hours; ml/pbw, milliliter per kg predicted body weight
Participants
All consecutive intubated patients on controlled MV with ABI requiring continuous monitoring of intracranial pressure (ICP) were screened for inclusion at the ICU admission. Exclusion criteria were ICP > 22 mmHg, preceding decompressive craniectomy, presence of open external ventricular drainage (EVD), acute hypoxaemic respiratory failure (defined as PaO2/FiO2 < 300 mmHg and presence of infiltrates on the chest X-ray), a history of severe lung disease, body mass index (BMI) > 35 kg/m2, or known cardiac failure. We treated hypovolemia with fluid resuscitation prior to inclusion. All patients were managed according to the local protocols (Additional file 1: Methods 1). The patients were deeply sedated with continuous infusions of propofol and fentanyl to reach a Richmond Agitation Sedation Scale of minus 5 without the use of muscle relaxants. In addition, infusion of midazolam was administrated, if necessary, to reach the sedation target.
Measurements and data collection
Airway pressure and flow (pneumotachograph) were measured proximal to the endotracheal tube. Oesophageal pressure was measured by using an oesophageal balloon catheter (BA-A-008, MBMed, Argentina). Airway and oesophageal pressures and airflow signals were recorded with FluxView software on a computer connected to a respiratory monitor (FluxMed GrT®, MBMed, Argentina). TPP was calculated as the difference between airway and oesophageal pressures, as described by others [22, 23]. Respiratory mechanics were assessed by using end-inspiratory and end-expiratory holds on the ventilator.
Intensive care monitoring software (ICM + ®, Cambridge Enterprise Ltd, Cambridge UK) [24] was used for continuous recording of high-resolution ICP, ABP, central venous pressure, end-tidal carbon dioxide (EtCO2), RR, PEEP, minute ventilation and near-infrared spectroscopy (NIRS)-derived percentage of regional cerebral oxygen saturation (rSO2) from both hemispheres (Invos™, Medtronic, USA) [19]. A screenshot of the respiratory monitor and the intensive care monitoring during the data collection is presented in Additional file 1: Fig. S1.
Additionally, the following demographic and clinical data were retrieved from the medical records of the patients: age, sex, BMI, predicted body weight (PBW), Glasgow Coma Scale (GCS), type of brain injury, severity of traumatic brain injury (TBI) by Marshall classification [25], severity of subarachnoid haemorrhage (SAH) by modified Fisher scale [26] and severity of intracerebral haemorrhage (ICH) by intracerebral haemorrhage scale [27], type of ICP device, length of MV, length of ICU stay, ICU mortality, PaCO2, pH, arterial partial pressure of oxygen (PaO2). The data were collected and managed using RedCap electronic data capture tools [21].
Outcome measures
The primary outcome was the effect of LPV on ICP and PRx. We identified three endpoints:
-
1
Number and percentage (%) of patients in whom the ICP response to interventions was below the safety limit of 22 mmHg and therefore could complete the whole protocol.
-
2
‘Noninferiority’ of mean ICP, to be understood as an intervention ICP mean value not exceeding the preceding baseline values by more than 3 mmHg. Hence, an increase in ICP ≥ 3 mmHg was considered clinically significant.
-
3
No worsening in PRx between the intervention value and the preceding baseline value.
The secondary outcome was the effect of LPV on RAP and brain oxygenation, rSO2.
Data analysis
The full set of variables considered in the analysis in addition to outcome variables are presented in the Additional file 1 (Methods 2), together with a detailed data analysis method, including data processing, formulas for calculations of respiratory mechanics and statistical methods. Below, we provide a summary.
Data processing
ICM + software was used for data preprocessing of the high-resolution recordings prior to statistical analysis. The secondary indices, PRx and RAP were calculated as 5 min window moving Pearson correlation coefficients between 30 consecutive 10-s averages between ABP and ICP, and between intracranial pulse pressure amplitude and ICP, respectively, and updated every minute [28]. Fisher transformation was applied to PRx and RAP prior to further analysis.
Each variable was considered as one average value (for data collected with ICM +) or one single value (for data collected with FluxMed) per each study period and patient.
Sample size and statistical analysis
The sample size calculation was based on the primary outcome and the crossover study design. Assuming a difference of zero, a standard deviation of 4 mmHg [29] and a noninferiority margin of 3 mmHg, an alpha risk of 0.05, and a beta risk of 0.20 and, a total number of 28 patients were required. We aimed to include 30 patients to count for dropouts.
Continuous variables were tested for normality and are presented as the mean and standard deviation or median and interquartile range, and categorical variables are presented as counts and percentage. Carry-over and group effects were ruled out. The analysis was performed to investigate the treatment effect, assessed as a comparison between the intervention and preceding baseline (paired t-test (two-tailed) or Wilcoxon signed-rank test). We assessed the effect of the increase in PEEP by comparing mean values between the two interventions. Noninferiority of mean ICP was tested with paired t-test (one-tailed) on mean values (baseline vs intervention).
Further exploratory analysis. If the intervention(s) were interrupted, we set out to explore reasons for such outcomes with between-group comparisons. The groups were defined as follows: in the “interrupted group”, the patients had at least one interrupted intervention due to safety reasons; the “completed group” completed the interventions successfully. For between-group comparisons, we used the Mann–Whitney U test and presented the results as boxplots or violin plots. Lastly, we investigated the relationships between the changes induced by the interventions and neurological, haemodynamic, and respiratory variables, using scatterplots and Pearson correlations.
A p value < 0.05 was considered statistically significant. Bonferroni corrections for multiple comparisons were performed for the exploratory analysis (between-group comparisons and relationships with changes in ICP). The statistical analysis was performed with R software version 4.0 [30].
Results
Baseline characteristics of the patients
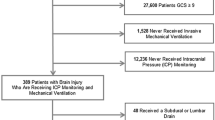
Fifty-eight patients were assessed for eligibility, of whom 27 were included in the analysis (Fig. 2). In one patient, the “low VT/high PEEP” intervention was not performed because pneumothorax had developed.

CONSORT flow diagram for crossover study. VT, tidal volume; PEEP, positive end expiratory pressure; ICP, intracranial pressure
Twenty-three of 27 patients had correct measurements from the oesophageal balloon catheter whereas four installations failed for technical reasons. Patient demographics and clinical characteristics are described in Table 1. Only 4 SAH patients were included, as these patients were commonly treated with open EVD. Therefore, they met more often the exclusion criteria for the study.
Baseline respiratory data are displayed in Table 2.
Effects of LPV on ICP and PRx
In 21 of 27 patients, the interventions with low tidal volume, neither with low PEEP nor with high PEEP caused clinically important increases in ICP (Table 3, Fig. 3). However, eight of 53 (15%) attempted interventions on 6 patients, were interrupted because they reached the prespecified safety limit of ICP > 22 mmHg for more than 5 min (Fig. 2 and 3).

Mean ICP and PRx induced changes. The interrupted interventions were presented in red. The value displayed is the mean value before interruption of the intervention, hence not entirely representative or comparable with not interrupted interventions. Panel (A). Mean ICP did not have a clinically important rise as compared with baseline, neither following the “Low VT/low PEEP” intervention nor during “Low VT/high PEEP” (one tailed paired t-test for noninferiority, both interventions p = 0.99). Similar results were achieved when including patients in whom the interventions were interrupted. In six of 27 (22%) patients, “Low VT/high PEEP” alone or both interventions were interrupted because the safety limit of ICP > 22 mmHg was reached. In one patient only the “low VT/low PEEP” intervention was interrupted. This patient had an increase in ICP over time, which might explain why the first attempted intervention “low VT/high PEEP” could be tolerated. Panel (B). None of the interventions produced significant changes from baseline in mean PRx, neither during intervention “Low VT/low PEEP” (paired t-test, p = 0.56) nor during intervention “Low VT/high PEEP” (p = 0.50). Similar results were achieved when including patients in whom the interventions were interrupted. VT, tidal volume; PEEP, positive end expiratory pressure; ICP, intracranial pressure; PRx, pressure reactivity index
The interventions did not produce significant changes in mean PRx in comparison with the baseline values (Table 3, Fig. 3).
Overall, there were no significant differences, neither in mean ICP nor in PRx between the two interventions.
Effects of LPV on rSO2 and RAP
We found no significant differences in the mean rSO2 between interventions or in comparison with the preceding baseline (Table 3). Left-sided rSO2 displayed a small (2%) difference between the two interventions, which was statistically significant, albeit not considered clinically relevant. RAP tended to increase during the interventions as compared with the preceding baselines but was not different between interventions. Only the increase during the intervention “low VT/low PEEP” was statistically significant (p < 0.05).
Further exploratory analysis
Additional file 1 (Table S1 and S2) present all the neuromonitoring, haemodynamic and respiratory variables, comparing the study periods, considered in the exploratory analysis.
Below we report the most relevant findings. Additional exploratory analyses on variables associated with the increase in ICP are presented in the Additional file 1 (Fig. S2 and Fig. S3).
Effect of LPV on respiratory mechanics and gas exchange. PaCO2 was 35 ± 3 mmHg at baseline and 36 ± 3 mmHg in both interventions. Although there was a statistically significant increase in PaCO2 between baseline and intervention, the increase was small (< 2 mmHg). TPPee was higher in the “low VT/high PEEP” intervention. Of note, TPPee was negative with PEEP 5 cmH2O. MP was significantly different both between preceding baselines and interventions and between interventions. The highest MP was in the “low VT/high PEEP” intervention, 13 [11,12,13,14] J/min.
Variables associated with increased ICP that warranted the interruption. Figure 4 presents differences in physiological variables between the completed and the interrupted group. Baseline ICP, RAP, EtCO2 and MP were all significantly different between the completed and the interrupted groups. TPP and compliance of the respiratory system (Crs) or lung were not different between completed and interrupted interventions.

Differences in ICP (A), RAP (B), EtCO2 (C), MP (D), TPPei (E) and TPPee (F) at baseline preceding interrupted and completed interventions. The data are presented with violin plots and boxplots. A. ICP (n = 8, median ICP = 17.1 (15.9 -19.7) mmHg) at the baseline in the interrupted interventions vs. completed interventions (n = 43, median ICP = 10.0 (4.6–13.3) mmHg). B. RAP at the baseline in the interrupted (n = 8, median RAP = 0.97 (0.86–1.18) vs. the completed (n = 41, median RAP = 0.42 (0.24–0.80) interventions. C. EtCO2 at baseline in interrupted (n = 8, median EtCO2 = 29.2 (25.5–30.9) mmHg) versus completed (n = 43, median EtCO2 = 31.1 (29.5–32.8) mmHg) interventions. D. MP at the baseline in interrupted (n = 7, median MP = 12.1 (10.1–13.0) J/min) vs. completed (n = 33, median MP = 8 (6.4—9.3) J/min) interventions. E and F. Neither TPPei and TPPee were significantly different between completed and interrupted events. ICP, intracranial pressure; RAP, compensatory reserve index; EtCO2, end-tidal partial pressure of CO2; MP, mechanical power; TPPei, transpulmonary pressure end inspiration, absolute; TPPee, transpulmonary pressure end expiration, absolute
Baseline PaCO2 was determined to 33.6 ± 1.4 mmHg and 34.9 ± 2.7 mmHg in completed and interrupted interventions, respectively (p = 0.81). The alveolar dead space during the intervention was not significantly different between completed (12 ± 8%) and interrupted (18 ± 9%) interventions (p = 0.19).
Discussion
In the present clinical, prospective study, the main finding was that most of the patients with ABI had no adverse effects of LPV, neither on ICP nor on PRx, independent of PEEP levels applied in this study. However, nearly one-quarter of the patients exhibited a transient rise in ICP during the intervention, requiring it to be interrupted. The high PEEP strategy was as expected associated with higher TPPee and MP. To our knowledge, this is the first clinical study attempting to elucidate the effects of lung protective ventilation on brain physiology in ABI patients without lung injury, as assessed by simultaneous monitoring of respiratory mechanics and neurophysiological variables.
Studies dealing with the influence on ICP of various types of MV and associated PEEP levels remain inconclusive [29, 31, 32]. Retrospective post hoc analysis of observational data from patients with ABI without lung injury did not show any significant association between PEEP and ICP [29, 33]. However, such analysis has some limitations; notably, ICP exceeding the predefined target value is treated and therefore cannot become part of a retrospective analysis. In a subgroup of patients with severe lung injury presented in one of the latter studies, the investigators found that there was a 0.3 mmHg increase in ICP for every cmH2O rise in PEEP above 5 cmH2O [29]. This is consistent with the minor increments in ICP we noticed in patients in whom the interventions were completed.
To date, no prospective phase III clinical trials showing a better outcome with multimodal neuromonitoring have been published [34]. Nevertheless, in recent years there have been attempts to incorporate multimodal monitoring of CA and oxygenation into treatment protocols for ABI [35]. Continuous monitoring of PRx allows for identifying individualised autoregulation-based cerebral perfusion pressure targets in TBI patients. A recent phase II clinical trial has proven the safety and feasibility of this approach, paving the path for outcome trials [36]. However, if different levels of VT and PEEP were to affect CA, independently of PaCO2 or CPP, then PRx-based CPP targets would be difficult to implement in clinical practice. In our study, LPV did not affect PRx. Consequently, PRx-based CPP management protocols can most likely be applied regardless of the ventilator settings, provided that PaCO2 levels are kept stable.
The modest increase in RAP observed during the intervention periods, suggesting a slightly decrease in cerebral compliance, was consistent with a small and clinically unimportant increment of ICP. rSO2 can be considered as an indirect, surrogate measure of cerebral blood flow. The fact that rSO2 did not decrease with the application of LPV supports the hypothesis that LPV can be safe in ABI patients. In patients with the combination of ABI and ARDS, Nemer et al. have reported an increase in brain tissue oxygenation during a short trial of high PEEP [37].
The interaction between neurological and respiratory variables and ICP
In the present study, we specifically targeted tight EtCO2 control to minimize the confounding effects of a rise in EtCO2 on ICP and PRx. Patients also had stable haemodynamics and hypovolemia was treated prior to the start of the study. This allowed us to look for other mechanisms of intracranial hypertension that made interruption of interventions necessary. Notably, the latter patients experienced a higher ICP level at baseline, and the subsequent rise in ICP might well have emerged in a state of low brain compliance, as determined with the RAP index at the preceding baseline. Our result is supported by an early report that examined the potential role of brain compliance in the ICP response to PEEP, employing cerebral pressure–volume measurements[38]. Contrary to our findings, McGuire and co-workers noticed that patients with increased baseline ICP did not respond with a further rise when exposed to higher PEEP levels [39]. However, brain compliance was not assessed in that study. If ICP waveform analysis is available, we suggest paying special attention to those patients with high RAP.
We observed a tendency towards a wider PaCO2–EtCO2 gap at the baseline in patients in whom we interrupted the intervention. The present study was not designed to elucidate the interaction between ICP and CO2. Therefore, we cannot draw any conclusions from this observation. Monitoring the PaCO2–EtCO2 gap is easily feasible, and we hope future studies will consider this observation.
MP is described as energy delivered to the respiratory system over time. In neurocritical care patients, increased MP may be related to higher ICU mortality [40]. The present study is the first one to analyse the relationship between MP and cerebral variables in patients with ABI. As expected, MP was highest in the high PEEP intervention. It was also highest at baseline, in patients in whom we interrupted the interventions. Nevertheless, MP was lower than the potential safety limit of MP 17 J/min, indicating that the use of a lower TV and higher RR is acceptable in relation to MP [41]. The pathophysiological mechanisms and the clinical significance of these associations need to be further elucidated and analysed.
In this investigation on non-ARDS patients, we found no relationship between increased TPP and interrupted events. Of note, TPPee was negative with PEEP 5 cmH2O. We cannot exclude the possibility that the patients might be at risk of developing atelectasis by applying PEEP of 5 cmH2O or below [42]. Considering the risk for ARDS that the ABI patients are exposed to, further data on TPP from randomised, multi-centre studies are warranted to explore optimal PEEP in patients with ABI, both with and without ARDS.
Our study did not demonstrate significant associations between respiratory compliance and the responses of ICP to LPV. Previous studies of lung compliance and ICP have given contradictory results [31, 43, 44]. Regarding patients with SAH, Chen et al. revealed that chest wall compliance, in contrast to lung or airway compliance, correlated inversely with ICP under exposure to increasing PEEP from 5 cmH2O to 15 cmH2O [43]. In the latter study, the differences in mean ICP at the two PEEP levels were consistent with those observed in the present study, but with no interrupted events. We admit that their study population was not entirely comparable with ours since both the baseline ICP and the P/F ratios were lower in their study. Investigators of an observational study employing computed tomography, reported a significant increase in ICP following a rise in PEEP from 5 to 15 cmH2O [31]. The authors observed that, when applying high PEEP, the increase in ICP correlated inversely with Crs. Notably, PaCO2 was higher than in our study, and the patient´s head level was positioned flat for computer tomography. These variations can partly explain the different results. Moreover, Mascia et al. reported a significant correlation between ICP, PaCO2 and Crs in response to changes in PEEP in patients with moderate to severe lung injury [44]. The cohort consisted of patients on both spontaneous and controlled ventilation.
Limitations
The present study has some limitations. A major one is that it is a single-centre study with a small sample size. Notably, the interrupted group is too small, to draw any firm conclusions from. The power analysis was based on local retrospective ICP data in parallel with clinical judgement, in combination with a previous observational study [29]. We considered an ICP change of 3 mmHg was considered as clinically significant, in accordance with previous studies [43, 45]. We also thought that the results of this pilot study could inspire a future multicentre trial encompassing more rigid power analysis. Although the numbers used for power analysis should be interpreted with caution, we believe that our study provided solid data, particularly because the patients were thoroughly monitored and treated by a few dedicated physicians and intensive care nurses. All relevant events were documented in real-time during the whole study period. All these precautions most likely contributed to reducing the number and impact of confounding variables.
It is possible, albeit not proven, that another study design with slowly increasing PEEP would have given other changes in ICP. We did not test the response to high tidal volume and high PEEP, because of the risk of overdistention. However, the study design allowed us to explore the effect of low tidal volume and high PEEP separately, which had not been done before. A limitation is also the fact that we did neither have recordings of brain tissue oxygen tension, nor cardiac output measurement, since this type of devices are used sparingly in our ICU in this patient group.
Conclusion
LPV seems to be safe and feasible for most but not all patients with ABI. In patients with suspected low brain compliance, LPV should be performed under careful monitoring, with an emphasis on respiratory mechanics and ICP waveform-derived variables when available. Baseline ICP, RAP, etCO2 and MP were significant predictors of an ICP increase, suggesting that they can be used to individualize ventilator settings in this context. Our findings provide a basis for further clinical investigations of the interaction between ventilator settings and ABI complicated with ARDS, using TPP and multimodal neuromonitoring tools.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request. Full details of the trial protocol can be found at clinicaltrials.gov/NCT03278769.
Abbreviations
- ABI:
-
Acute brain injury
- ABP:
-
Arterial blood pressure
- ARDS:
-
Acute respiratory distress syndrome
- BMI:
-
Body mass index
- Crs :
-
Compliance of the respiratory system
- CA:
-
Cerebral blood flow autoregulation
- CPP:
-
Cerebral perfusion pressure
- EVD:
-
External ventricular drainage
- EtCO2 :
-
End-tidal partial pressure of CO2
- FiO2 :
-
Fraction of inspired oxygen
- ICH:
-
Intracranial haemorrhage
- ICM + :
-
Intensive care monitor +
- ICP:
-
Intracranial pressure
- ICU:
-
Intensive care unit
- LPV:
-
Lung protective ventilation
- MP:
-
Mechanical power
- MV:
-
Mechanical ventilation
- NIRS:
-
Near-infrared spectroscopy
- PaCO2 :
-
Arterial carbon dioxide partial pressure
- PaO2 :
-
Arterial oxygen partial pressure
- Pbw:
-
Predicted body weight
- PEEP:
-
Positive end-expiratory pressure
- PRx:
-
Pressure reactivity index
- RAP:
-
Compensatory reserve index
- RR:
-
Respiratory rate
- RedCap:
-
Research electronic data capture
- rSO2 :
-
Regional cerebral oxygen saturation
- SAH:
-
Subarachnoid haemorrhage
- TBI:
-
Traumatic brain injury
- TPP:
-
Transpulmonary pressure
- TPPei :
-
End-inspiratory transpulmonary pressure, absolute
- TPPee :
-
End-expiratory transpulmonary pressure
- VT:
-
Tidal volume
References
Ziaka M, Exadaktylos A. Brain–lung interactions and mechanical ventilation in patients with isolated brain injury. Crit Care. 2021;25(1):1–10.
Taran S, Cho SM, Stevens RD. Mechanical Ventilation in patients with traumatic brain injury: Is it so Different? Neurocrit Care. 2022;7:1–4.
Frisvold SK, Robba C, Guérin C. What respiratory targets should be recommended in patients with brain injury and respiratory failure? Intensive Care Med. 2019;45(5):683–6.
Robba C, Poole D, McNett M, Asehnoune K, Bösel J, Bruder N, et al. Mechanical ventilation in patients with acute brain injury: recommendations of the European Society of Intensive Care Medicine consensus. Intensive Care Med. 2020;46(12):2397–410.
Fan E, del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–63.
Gattinoni L, Tonetti T, Cressoni M, Cadringher P, Herrmann P, Moerer O, et al. Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med. 2016;42(10):1567–75.
Mauri T, Yoshida T, Bellani G, Goligher EC, Carteaux G, Rittayamai N, et al. Esophageal and transpulmonary pressure in the clinical setting: meaning, usefulness and perspectives. Intensive Care Med. 2016;42:1360–73.
Simonis FD, Serpa Neto A, Binnekade JM, Braber A, Bruin KCM, Determann RM, et al. Effect of a low vs intermediate tidal volume strategy on ventilator-free days in intensive care unit patients without ARDS. JAMA. 2018;320(18):1872.
Algera AG, Pisani L, Serpa Neto A, den Boer SS, Bosch FFH, Bruin K, et al. Effect of a lower vs higher positive end-expiratory pressure strategy on ventilator-free days in ICU patients without ARDS: a randomized clinical trial. JAMA J Am Med Assoc. 2020;324(24):2509–20.
Mascia L, Zavala E, Bosma K, Pasero D, Decaroli D, Andrews P, et al. High tidal volume is associated with the development of acute lung injury after severe brain injury: an international observational study. Crit Care Med. 2007;35(8):1815–20.
Beitler JR, Ghafouri TB, Jinadasa SP, Mueller A, Hsu L, Anderson RJ, et al. Favorable neurocognitive outcome with low tidal volume ventilation after cardiac arrest. Am J Respir Crit Care Med. 2017;195(9):1198–206.
Asehnoune K, Mrozek S, Perrigault PF, Seguin P, Dahyot-Fizelier C, Lasocki S, et al. A multi-faceted strategy to reduce ventilation-associated mortality in brain-injured patients. The BI-VILI project: a nationwide quality improvement project. Intensive Care Med. 2017;43(7):957–70.
Nyquist P, Stevens RD, Mirski MA. Neurologic injury and mechanical ventilation. Neurocrit Care. 2008;9(3):400–8.
Meyfroidt G, Bouzat P, Casaer MP, Chesnut R, Hamada SR, Helbok R, et al. Management of moderate to severe traumatic brain injury: an update for the intensivist. Intensive Care Med. 2022;48(6):649–66.
Donnelly J, Budohoski KP, Smielewski P, Czosnyka M. Regulation of the cerebral circulation: bedside assessment and clinical implications. Crit Care. 2016;20(1):129.
Zeiler FA, Ercole A, Beqiri E, Cabeleira M, Thelin EP, Stocchetti N, et al. Association between cerebrovascular reactivity monitoring and mortality is preserved when adjusting for baseline admission characteristics in adult traumatic brain injury: a CENTER-TBI study. J Neurotrauma. 2020;37(10):1233–41.
Zeiler FA, Ercole A, Cabeleira M, Beqiri E, Zoerle T, Carbonara M, et al. Compensatory-reserve-weighted intracranial pressure versus intracranial pressure for outcome association in adult traumatic brain injury: a CENTER-TBI validation study. Acta Neurochir (Wien). 2019;161(7):1275–84.
Czosnyka M, Smielewski P, Kirkpatrick P, Laing R, Menon D, Pickard JD. Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery. 1997;41(1):11–9.
Barud M, Dabrowski W, Siwicka-Gieroba D, Robba C, Bielacz M, Badenes R. Usefulness of cerebral oximetry in tbi by nirs. J Clin Med. 2021;10(13):1–9.
Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010. https://doi.org/10.1016/j.ijsu.2011.10.001.
Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95(April): 103208.
Yoshida T, Brochard L. Esophageal pressure monitoring: Why, when and how? Curr Opin Crit Care. 2018;24(3):216–22.
Baydur A, Behrakis PK, Zin WA, Jaeger M, Milic-Emili J. A simple method for assessing the validity of the esophageal balloon technique. Am Rev Respir Dis. 1982;126(5):788–91.
Smielewski P, Czosnyka M, Steiner L, Belestri M, Piechnik SPJ. ICM+: software for on-line analysis of bedside monitoring data after severe head trauma. Acta Neurochir Suppl. 2005;95:43–9.
Marshall LF, Marshall SB, Klauber MR, van Berkum Clark M, Eisenberg HM, Jane JA, et al. A new classification of head injury based on computerized tomography. J Neurosurg. 1991;75(SUPPL.):S14-20.
Frontera JA, Claassen J, Schmidt JM, Wartenberg KE, Temes R, Connolly ES, et al. Prediction of symptomatic vasospasm after subarachnoid hemorrhage. Neurosurgery. 2006;59(1):21–7.
Hemphill JC, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32(4):891–6.
Czosnyka M, Smielewski P, Timofeev I, Lavinio A, Guazzo E, Hutchinson P, Pickard JD. Intracranial pressure: more than a number. Neurosurg Focus. 2007;22(5):1–7.
Boone MD, Jinadasa SP, Mueller A, Shaefi S, Kasper EM, Hanafy KA, et al. The effect of positive end-expiratory pressure on intracranial pressure and cerebral hemodynamics. Neurocrit Care. 2016;1–8.
R2021. R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2021.
Robba C, Ball L, Nogas S, Battaglini D, Messina A, Brunetti I, et al. Effects of positive end-expiratory pressure on lung recruitment, respiratory mechanics, and intracranial pressure in mechanically ventilated brain-injured patients. Front Physiol. 2021;12:1684.
Shapiro H, Marshall LF. Intracranial pressure responses to PEEP in head-injured patients. J Trauma Inj Infect Crit Care. 1978;18(4):254–6.
Tejerina E, Pelosi P, Muriel A, Peñuelas O, Sutherasan Y, Frutos-Vivar F, et al. Association between ventilatory settings and development of acute respiratory distress syndrome in mechanically ventilated patients due to brain injury. J Crit Care. 2017;38:341–5.
Bernard F, Barsan W, Diaz-Arrastia R, Merck LH, Yeatts S, Shutter LA. Brain Oxygen Optimization in Severe Traumatic Brain Injury (BOOST-3): a multicentre, randomised, blinded-endpoint, comparative effectiveness study of brain tissue oxygen and intracranial pressure monitoring versus intracranial pressure alone. BMJ Open. 2022;12(3):1–9.
Chesnut R, Aguilera S, Buki A, Bulger E, Citerio G, Cooper DJ, et al. A management algorithm for adult patients with both brain oxygen and intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2020;46(5):919–29.
Tas J, Beqiri E, van Kaam RC, Czosnyka M, Donnelly J, Haeren RH, et al. Targeting autoregulation-guided cerebral perfusion pressure after traumatic brain injury (COGiTATE): a feasibility randomized controlled clinical trial. J Neurotrauma. 2021;38(20):2790–800.
Nogueira Nemer S, Caldeira JB, Santos RG, Guimarães BL, Márcio Garcia J, Prado D, et al. Effects of positive end-expiratory pressure on brain tissue oxygen pressure of severe traumatic brain injury patients with acute respiratory distress syndrome: a pilot study. J Crit Care. 2015;30(6):1263–6.
Apuzzo JL, Wiess MH, Petersons V, Small RB, Kurze THJ. Effect of positive end expiratory pressure ventilation on intracranial pressure in man. J Neurosurg. 1977;46(2):227–32.
McGuire G, Crossley D, Richards J, Wong D. Effects of varying levels of positive end-expiratory pressure on intracranial pressure and cerebral perfusion pressure. Crit Care Med. 1997;25(6):1059–62.
Jiang X, Zhu Y, Zhen S, Wang L. Mechanical power of ventilation is associated with mortality in neurocritical patients: a cohort study. J Clin Monit Comput. 2022;36(6):1621–8.
Serpa Neto A, Deliberato RO, Johnson AEW, Bos LD, Amorim P, Pereira SM, et al. Mechanical power of ventilation is associated with mortality in critically ill patients: an analysis of patients in two observational cohorts. Intensive Care Med. 2018;44(11):1914–22.
Cortes GA, Marini JJ. Two steps forward in bedside monitoring of lung mechanics: transpulmonary pressure and lung volume. Crit Care. 2013;17(2):219.
Chen H, Chen K, Xu JQ, Zhang YR, Yu RG, Zhou JX. Intracranial pressure responsiveness to positive end-expiratory pressure is influenced by chest wall elastance: a physiological study in patients with aneurysmal subarachnoid hemorrhage. BMC Neurol. 2018;18(1):124.
Mascia L, Grasso S, Fiore T, Bruno F, Berardino M, Ducati A, et al. Cerebro-pulmonary interactions during the application of low levels of positive end-expiratory pressure. Intensive Care Med. 2005;31:373–9.
Schirmer-Mikalsen K, Vik A, Skogvoll E, Moen KG, Solheim O, Klepstad P. Intracranial pressure during pressure control and pressure-regulated volume control ventilation in patients with traumatic brain injury: a randomized crossover trial. Neurocrit Care. 2016;24(3):332–41.
Acknowledgements
We acknowledge the medical doctors Christian Holgersen and Krister Ekeroth and the medical student Lisa Jakobsen who participated in part of the data collection. We acknowledge statistician, Professor of Medical epidemiology at UiT the Arctic University of Norway, Dr. Tom Wilsgaard for assistance with sample size calculation.
Funding
Open access funding provided by UiT The Arctic University of Norway (incl University Hospital of North Norway). This research was funded in whole by the Northern Norway Regional Health Authority (181021) and ESICM clinical award 2018. Erta Beqiri is supported by the Medical Research Council (Grant No.: MR N013433-1) and by the Gates Cambridge Scholarship.
Author information
Authors and Affiliations
Contributions
SKF, CG and PS conceived and designed the study. SKF administered the study. EB, SKF and PS performed the data analysis. CG contributed to data analysis. EB, PS, CG and SKF wrote the first draft and revised the manuscript for resubmissions. All authors contributed to the study protocol and manuscript editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Norwegian Regional Committee for Medical and Health Research Ethics (REC), and informed consent was obtained from the next of kin and later by the patient whenever appropriate, according to local regulations (2017/1941/REK North).
Consent for publication
“Not applicable”.
Competing interests
Peter Smielewski and Marek Czosnyka receive part of the licensing fees for ICM + software, licensed by Cambridge Enterprise Ltd, University of Cambridge, Cambridge. The authors declare that they have no other competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Detailed methods, supplemental tables and figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Beqiri, E., Smielewski, P., Guérin, C. et al. Neurological and respiratory effects of lung protective ventilation in acute brain injury patients without lung injury: brain vent, a single centre randomized interventional study. Crit Care 27, 115 (2023). https://doi.org/10.1186/s13054-023-04383-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04383-z