
Abstract
Purpose
Mechanical power (MP) may unify variables known to be related to development of ventilator-induced lung injury. The aim of this study is to examine the association between MP and mortality in critically ill patients receiving invasive ventilation for at least 48 h.
Methods
This is an analysis of data stored in the databases of the MIMIC–III and eICU. Critically ill patients receiving invasive ventilation for at least 48 h were included. The exposure of interest was MP. The primary outcome was in-hospital mortality.
Results
Data from 8207 patients were analyzed. Median MP during the second 24 h was 21.4 (16.2–28.1) J/min in MIMIC-III and 16.0 (11.7–22.1) J/min in eICU. MP was independently associated with in-hospital mortality [odds ratio per 5 J/min increase (OR) 1.06 (95% confidence interval (CI) 1.01–1.11); p = 0.021 in MIMIC-III, and 1.10 (1.02–1.18); p = 0.010 in eICU]. MP was also associated with ICU mortality, 30-day mortality, and with ventilator-free days, ICU and hospital length of stay. Even at low tidal volume, high MP was associated with in-hospital mortality [OR 1.70 (1.32–2.18); p < 0.001] and other secondary outcomes. Finally, there is a consistent increase in the risk of death with MP higher than 17.0 J/min.
Conclusion
High MP of ventilation is independently associated with higher in-hospital mortality and several other outcomes in ICU patients receiving invasive ventilation for at least 48 h.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Mechanical power unifies variables known to be related to development of ventilator-induced lung injury. Mechanical power is independently associated with worse outcomes in patients receiving invasive ventilation. Of additional interest, even at low tidal volume and low driving pressure, high mechanical power is associated with worse patient-centered outcomes. |
Introduction
With each breath delivered by the mechanical ventilator a certain amount of energy is transferred to the patient’s respiratory system. This energy is mainly used to overcome resistance of the airways and to expand the thorax wall [1,2,3,4]. A fraction of this energy acts directly on the lung skeleton, or extracellular matrix, as such deforming the epithelial and endothelial cells anchored to it [2]. Lungs “conserve” small amounts of energy with each breath cycle as the elastic recoil of the lung returns less energy during exhalation than that absorbed during inspiration [1,2,3,4]. In fact, mechanical ventilation is associated with substantial dissipation of energy, probably resulting in “heat” or inflammation, potentially leading to injury of lung tissue.
It has been hypothesized before that the extent of so-called ventilator-induced lung injury (VILI) depends on the amount of energy transferred [1,2,3,4], and tidal volume size (VT), plateau pressure (Pplat), respiratory rate (RR), and air flow all relate to the amount of energy generated by the mechanical ventilator [2]. The amount of energy per unit of time, expressed in Joules per minute (J/min), is often referred to as the “mechanical power” (MP) [2,3,4,5,6,7,8,9]. MP can be calculated accurately through a “power equation”, increasing its applicability in clinical practice [6]. One recent study in healthy piglets with uninjured lungs elegantly showed that increases in MP during ventilation by increasing RR are associated with more VILI [2, 7]. There have been no clinical studies, however, that thoroughly examined the association between MP and outcome in ventilated patients.
It would be helpful and practical to have one single variable combining all possible factors associated with mortality that could be easily calculated and evaluated at the bedside, or maybe even displayed on the screen of a ventilator in a continuous fashion [6,7,8]. Therefore, to test the hypothesis that MP is independently associated with patient-centered outcomes in critically ill patients receiving mechanical ventilator for at least 48 h, we collected ventilation data to calculate MP using the power equation [6] in two large cohorts of intensive care unit (ICU) patients whose data were prospectively collected in two databases. Part of this work was presented as a poster in the XIII World Congress of Intensive and Critical Care Medicine in 2017 [10].
Methods
This study used data stored in the high-resolution databases of two patient cohorts, the Medical Information Mart for Intensive Care (MIMIC)-III [11, 12], and the eICU Collaborative Research Database (eICU) [13]. An extensive description of methods is reported in the online supplement.
Study design
This investigation concerns a post hoc analysis of data from critically ill patients admitted to the intensive care units (ICUs) of 59 hospitals in the USA [including the Beth Israel Deaconess Medical Center (BIDMC), Boston, MA, in MIMIC, and 58 other hospitals in eICU].
Study population
All patients in the MIMIC-III version v1.4 and eICU version v1.2 databases were eligible for inclusion in the present investigation. The following two inclusion criteria were used: (1) age 16 years or more; and (2) receiving invasive ventilation for at least 48 consecutive hours. Patients receiving ventilation through a tracheostomy cannula at any time during the first 48 h of ventilation, and patients who were extubated or died during the first 48 h were excluded. Only data of the first ICU admission of the first hospitalization were used. Patients who had incomplete datasets or datasets that did not sufficiently capture the ventilatory variables needed to calculate MP were excluded. As an additional exclusion criterion for the eICU database, hospitals that did not routinely document ventilation settings within the eICU system were deselected.
Data extraction
All ventilation variables were extracted as the highest and the lowest values per each time frame of 6 h during the first 48 h of ventilation (eFig. 1). Presence of the acute respiratory distress syndrome (ARDS) in the first 48 h of ventilation was scored according to the Berlin definition [14], using original data to reclassify patients before publication of this definition.
Mechanical power
The primary exposure of interest was MP expressed in J/min in the second 24 h of ventilation. MP was calculated as proposed previously [6, 8], using VT, peak pressure (Ppeak), RR, and driving pressure (ΔP) data:
Since the patients had several measurements available, the mean between the highest and the lowest value in the second 24 h was used. Since ventilation is a dynamic process, and to check the consistency of the findings, the time-weighted average MP over the first 48 h of ventilation was calculated as the area under the MP versus time plot (eFig. 1) [15]. Moments where data necessary to calculate MP were missing were not included in the time-weighted average calculation and the calculation was adjusted by the number of observations available.
Outcomes
The primary outcome was in-hospital mortality. Secondary outcomes included ICU, 30-day, and 1-year mortality; the number of ventilator-free days at day 28 (defined as the number of days from successfully weaning to day 28; patients who died before weaning were deemed to have no ventilator-free days), and ICU and hospital length of stay.
Statistical analysis
Continuous variables are presented as medians with their interquartile ranges and categorical variables as total number and percentage. Proportions were compared using χ2 or Fisher exact tests and continuous variables were compared using the t test or Wilcoxon rank sum test, as appropriate. Patients were categorized into groups according to the cohort analyzed, i.e., MIMIC-III or eICU.
MP in the second 24 h of ventilation was used as a continuous variable for the primary analysis. Multivariable regression was selected as the analysis technique for all outcomes to account for factors that may influence outcomes. Relevant covariates known to predict outcome were entered into the model (description in the online supplement). To evaluate consistency of findings, sensitivity analyses, including the adjustment for the covariate balancing propensity score and considering the inverse probability of treatment weighting, were performed for the primary outcome as described in the online supplement. To account for potential changes in clinical practice through the years, a sensitivity analysis including the year of admission as a random factor in mixed-effect models was carried out.
Since the exclusion of patients in the MIMIC-III database due to missing data could have led to biased analyses, we re-evaluated all analyses and models in the cohort of excluded patients, calculating MP using maximum airway pressure (Pmax) instead of Pplat. To avoid bias introduced by missing data, the analysis of the primary outcome was replicated after multiple imputation as described in the online supplement. Also, in a cohort including data from both databases, we analyzed the MP partitioned into 14 quantiles to identify the best cutoff associated with higher mortality. A receiver-operating characteristic (ROC) curve analysis was used to confirm the best cutoff. Recently, the impact of the driving pressure in obese patients was questioned [16]. Thus, an additional analysis was conducted only in obese patients, defined as patients with body mass index ≥ 30 kg/m2 [16]. To check if MP adds additional information, patients were stratified according to different levels of MP, VT size, and ∆P level (as described in the online supplement). Finally, as subgroup analyses, the association between MP and the primary outcome was assessed according to the presence of ARDS and the use of neuromuscular blocking agents (NMBA).
Statistical significance was considered to be at two-sided p < 0.05. All analyses were performed with R v.3.3.2 (http://www.R-project.org).
Results
Patients
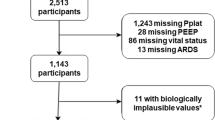
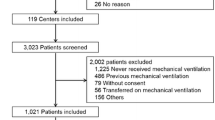
The MIMIC-III database contained 53,423 ICU admissions of 38,597 unique patients. After exclusion of patients who received invasive ventilation for less than 48 h and patients who received ventilation through a tracheostomy cannula, we had 5003 patients, of whom 3846 patients admitted from 2001 till 2012 had complete data (eFig. 2). In eICU, from the total of 99,837 unique patients, and after the exclusion of patients receiving invasive ventilation less than 48 h and with no data on ventilation variables, 4361 patients admitted from 2014 till 2015 were included (eFig. 2).
Baseline characteristics of patients are shown in Table 1; characteristics of ICUs involved are presented in eTable 1. The majority of patients in the two cohorts were male and most patients were admitted from the emergency room as a result of a clinical condition. In MIMIC-III, 11.5% of patients had ARDS in the first 48 h and in 9.8% in eICU. Vital signs and laboratory variables are presented in eTable 2 and outcomes in eTable 3. Overall in-hospital mortality was 29.9% in MIMIC–III and 31.0% in eICU. Ventilation characteristics of patients are shown in Table 2.
Mechanical power
There was a decrease in MP from the first to the second 24 h of ventilation in both cohorts (p < 0.001 by the Wilcoxon rank sign test) to 21.4 (16.2–28.1) J/min in MIMIC-III and 16.0 (11.7–22.1) J/min in eICU (Table 2).
Primary outcome
Results of the univariable analysis of the primary outcome are shown in eTable 4 and the complete multivariable analysis in eTable 5 and Fig. 1. There was no missing data for the primary outcome in both datasets. After adjustment for covariates, MP in the second 24 h of ventilation was significantly associated with higher in-hospital mortality in both cohorts, and this association remained when using adjustments for the covariate balancing propensity score (eTable 6 and Fig. 1), and after considering the inverse probability of treatment weighting (eTable 7 and Fig. 1). The amount of missing data in the variables is shown in eTable 8 and eFigs. 3 and 4. The results were consistent after multiple imputation for missing values in variables of interest (eTable 9). There is no influence of the year of admission on the effect of mechanical power (eTable 10).

Mechanical power (MP) in the second 24 h of ventilation and in-hospital mortality. Sensitivity analyses were performed to determine whether results were dependent on method of covariate adjustment. The odds ratio represents the odds of death per 5 J/min increase in MP. MP mechanical power, CBPS covariate balancing propensity score, IPTW inverse probability of treatment weight
After adjustments, there was an association between time-weighted average MP and higher in-hospital mortality in both cohorts (eTable 11). This association remained significant after adjustment for the covariate balancing propensity score and in the inverse probability of treatment weighting analysis (eTable 12).
Secondary outcomes
MP in the second 24 h of ventilation was also associated with ICU mortality, 30-day mortality (in eICU only) (Fig. 2a), the number of ventilator-free days, and ICU and hospital length of stay (Fig. 2b). Time-weighted average MP was associated with higher ICU mortality, with 30-day mortality (in eICU) but not with 1-year mortality (eTable 12). Time-weighted average MP was associated with less ventilator-free days, and longer ICU length of stay, but no association was found with hospital length of stay (eTable 12).

Mechanical power (MP) in the second day of ventilation and secondary outcomes. a Odds ratio represents the odds of death per 5 J/min increase in MP. b Effect estimates and 95% confidence interval from the multivariable linear regression for ventilator-free days, ICU length of stay, hospital length of stay. Effect estimate refers to the change in the outcome variable per 5 J/min increase in MP. MP mechanical power, ICU intensive care unit
Subgroup and sensitivity analyses
Baseline characteristics, vital signs, mechanical ventilation variables, and clinical outcomes in the cohort of patients excluded from the MIMIC-III database because of missing values are listed in eTables 13 and 14. Generally, patients excluded because of missing values were less ill than patients included in the main analysis. All the reproduced analyses confirmed the findings from the main analyses, with the exception of the absence of association between MP and ICU and hospital length of stay in the cohort of excluded patients (eTable 15).
Figure 3 shows the increase in the risk of in-hospital mortality as a function of progressive percentiles of MP in the pooled cohort. There is a consistent increase in the risk of death with MP higher than 17.0 J/min. The best cutoff found in the ROC analyses was 19.0 J/min, but this had a poor predictive power [AUC of 0.521 (0.507–0.536); sensitivity of 48% (46–50%); specificity of 56% (55–58%)] (eFig. 5). Considering only obese patients, MP remained associated with higher risk of in-hospital mortality, though this was only found in the eICU dataset (eTable 16).

Adjusted odds ratio for in-hospital mortality according to percentiles of mechanical power (MP) in the pooled cohort after multivariable adjustment. The pooled cohort was partitioned into 14 quantiles of mechanical power, and the adjusted odds ratio for each quantile was calculated in relation to the median mechanical power of the whole cohort. The odds ratio and 95% confidence intervals (error bars) for each percentile were calculated after multivariable adjustment for age, prognostic score, SOFA, pH, mean arterial pressure, PaO2/FiO2, SpO2, temperature, and PaCO2
In the analysis according to the VT size, even at low VT, high MP was associated with in-hospital mortality and other secondary outcomes (eTable 17). In the analysis according to the ∆P, even at low ∆P, high MP was associated with ICU mortality, ventilator-free days, and ICU length of stay (eTable 17).
Mechanical ventilator parameters in patients with and without ARDS in both datasets are shown in eTable 19. There was no significant interaction between the effect of MP on primary outcome and presence of ARDS at the beginning of ventilation (eFig. 6) or use of NMBA in the first 2 days of ventilation (eFig. 7) in any of the cohorts, meaning that the presence of ARDS and the use of NMBA did not affect the association between mechanical power and mortality.
Discussion
The findings of this investigation can be summarized as follows: (1) MP in the second 24 h of ventilation is independently associated with higher in-hospital mortality of critically ill patients who receive invasive ventilation for more than 48 h; (2) higher MP is independently associated with higher ICU mortality, a lower number of ventilator-free days and alive at day 28, and longer stay in ICU and hospital; (3) the impact of MP is consistent, and independent of the presence of ARDS or use of NMBA; and (4) even at low VT and low ∆P, high MP was associated with worse outcomes, suggesting that MP adds additional information beyond volume and pressure.
This is the first clinical investigation testing the hypothesis that MP generated by the mechanical ventilator is associated with patient-centered outcomes. Strengths of this post hoc analysis are that the MIMIC-III and the eICU databases contain comprehensive and high-quality data capture throughout the hospital course of a large group of well-defined and characterized ICU patients in 59 different hospitals from the USA, with different ventilatory practices and from different periods, covering from 2001 till 2015. The incidence of ARDS in the cohorts is comparable to that reported in previous studies of ventilated ICU patients [17, 18], suggesting that our cohort is similar to those studied previously. Our analysis leverages the availability of time-stamped vital signs, laboratory results, and ventilatory variables to build models that incorporate the dynamic characteristics of the invasive ventilation. The findings are consistent across several sensitivities analyses, indicating that conclusions were not dependent on the chosen statistical approach. Also, the studied cohorts were homogenous, and the 48-h time interval inclusion criterion guaranteed that all patients were exposed to invasive ventilation for a sufficient period of time. The findings were consistent in patients with and without ARDS, increasing its external validity. Finally, the confirmatory analysis using the time-weighted average helps to avoid surveillance bias.
Originally, MP was calculated according to the classical equation of motion with the addition of PEEP [2, 6, 19], and has three important components [6, 20]. The first is respiratory system elastance, which is the energy associated with the VT/ΔP. The second component is airway resistance that is related to the energy associated with gas movement. The third component equals energy needed to overcome tension in the fibers due to PEEP [6]. Recently, a so-called power equation was suggested, showing a good relationship with the original equation, but being simpler, and without the need for pressure–volume curves [6]. In the original description of MP, “measured” MP showed a good correlation with MP computed using this power equation, with a mean difference of only 0.196 J/min when computed in patients without ARDS [6]. This simplified power equation was used here.
Understanding how ventilation could harm lungs has improved over recent years [21]. The association between volumes and pressures delivered and generated by the mechanical ventilator and outcomes of critically ill patients who receive invasive ventilation has been the subject of many investigations so far [17, 22,23,24,25,26,27]. Volumes and pressures, mostly studied separately, in fact are components of the MP [6]. Other components of MP, such as RR so far received much less attention, but could play important roles in development of lung injury, even when volumes and pressures are chosen so that MP will remain low [20, 28]. The results of this analysis provide evidence that ventilation characteristics that are considered predictors of outcomes in ARDS patients may also have prognostic capacity in patients who do not fulfill the criteria for this complication of critical illness. Indeed, two important elements of the MP are tidal volume and driving pressure and, even though we did not assess the impact of the driving pressure directly, it is plausible that driving pressure is an important predictor of outcomes in a more general population.
Different mechanical ventilator variables have been shown to contribute to VILI, including VT [22, 23], Pplat [22], ∆P [9, 17, 26, 27], PEEP [24, 25], flow, and respiratory rate, all of which have been addressed separately in previous experimental or clinical studies. The MP represents the result of a combination of such variables and therefore might have a higher predictive value for patient-centered outcomes, including mortality. Since most of the evidence supporting protective ventilation supports the use of low VT, we addressed the impact of MP on in-hospital mortality in the presence of different VT sizes. In agreement with the core hypothesis, we found that even at low VT, high MP was associated with in-hospital mortality.
VILI originates from the interaction between the MP transferred to the lung parenchyma and the anatomic-pathophysiological characteristics of the latter [6]. It is suggested that if damage to lung parenchyma is a function of MP, it is possible that different combinations of its components, resulting in a MP greater than a certain threshold, may produce similar damage [2, 6]. In fact, changes in VT, ΔP, and inspiratory flow produced an identical exponential increase of MP in a previous investigation [6]. The impact of changes in RR is less pronounced, while an increase of PEEP caused only a linear increase in MP [6].
It could be an attractive concept to use MP to set a ventilator, as it combines the effects of different ventilatory variables. Changing one single variable may not always protect the lungs if it does not result in a change in the amount of energy actually delivered to lung tissue [8]. For example, a reduction in volume may not translate into benefit when it requires a higher respiratory rate to compensate for loss of minute volume [20, 28]. Likewise, PEEP increases may not be beneficial when they do not result in a decline in ΔP, e.g., when they do not lead to recruitment of atelectatic lung tissue—PEEP increases may be even harmful when they results in an increase in the ΔP, e.g., when they result in overdistension [27]. Further, excessive increases in PEEP, even if associated with reduced ∆P, in some cases may promote lung injury due to higher static strain. In fact, according to the power equation used, even if PEEP leads to a decrease in driving pressure, the MP could increase. In the future, ventilators may be able to display the MP applied to the respiratory system, helping the caregiver to titrate ventilation so that the least possible energy is being used. Smart algorithms aiming at the lowest amount of MP, built-in ventilators, may help further in preventing VILI.
The present analysis has some limitations. Its post hoc nature should be taken into account when considering the findings. Residual confounding may also mar our findings, although we attempted to account for this through several adjustments and models. Also, we tried to minimize interaction or effect modification by limiting our analysis to the first ICU stay for patients and excluding patients who had a tracheostomy or who had undergone a tracheostomy procedure during the first 72 h of their ICU admission. We considered only patients who received invasive ventilation for at least 48 h, aiming to select more severely ill patients and also those patients who had been exposed to the primary exposure of interest for a sufficient period of time. However, the present findings cannot be translated to patients who were extubated or died in the first 48 h. Around 25% of the patients receiving invasive ventilation for more than 48 h in the MIMIC-III database were excluded because of lack of Pplat measured accordingly, and this may lead to important biases if such patients are considerably different from the included cohort. This number, though, is lower than those found in two recent reports in patients with and without ARDS [17, 18], and sensitivity analyses in the cohort of excluded patients considering the Pmax instead of the Pplat for calculating MP led to similar results. We were unable to report potential complications associated with invasive ventilation and MP, including development of ARDS in patients who did not have ARDS at onset of ventilation, ventilator-associated pneumonia, atelectasis, or barotrauma, as these were not consistently captured and stored in the studied databases. It is important to emphasize that some kind of normalization, e.g., adjusted for the size of the lung, could be necessary to get an optimal cutoff that could be used to guide therapy. The amount of missing data in the variables assessed in the study is a potential limitation. However, the analyses after multiple imputation yielded similar results. Since the datasets used in this study are for clinical purposes and the present analysis is a secondary analysis of these data, we cannot guarantee that plateau pressure was collected under standard conditions, i.e., in the absence of spontaneous breathing efforts, at an adequate level of sedation, and with a sufficiently long end-inspiratory pause. Also, we present the MP applied to the respiratory system. As transpulmonary pressure data were not captured in the two databases, it is impossible to estimate the MP applied to the lung. In addition, prone positioning was not used in patients in the MIMIC-III and was not available in the eICU, and this could be a confounding factor. No sample size calculation was done, and the sample consisted of a convenience sample of patients who fulfilled the inclusion cohort in both datasets. The VT used in the patients, especially those with ARDS, is higher than expected and recommended by the guidelines; however, this represents the way that these patients were ventilated, even today. Although our findings do support an association between high MP and mortality, stronger evidence such as randomized controlled trials is necessary to establish a causal relationship.
Conclusions
In adult critically ill patients who receive invasive ventilation for at least 48 h, high mechanical power is independently associated with higher in-hospital mortality and several other important patient-centered outcomes.
References
Serpa Neto A, Amato MBP, Schultz MJ (2016) Dissipated energy is a key mediator of VILI: rationale for using low driving pressures. In: Vincent JL (ed) Annual update in intensive care and emergency medicine 2016, 1st edn. Springer, Cham, pp 311–321
Cressoni M, Gotti M, Chiurazzi C, Massari D, Algieri I, Amini M, Cammaroto A, Brioni M, Montaruli C, Nikolla K, Guanziroli M, Dondossola D, Gatti S, Valerio V, Vergani GL, Pugni P, Cadringher P, Gagliano N, Gattinoni L (2016) Mechanical power and development of ventilator-induced lung injury. Anesthesiology 124:1100–1108
Protti A, Andreis DT, Monti M, Santini A, Sparacino CC, Langer T, Votta E, Gatti S, Lombardi L, Leopardi O, Masson S, Cressoni M, Gattinoni L (2013) Lung stress and strain during mechanical ventilation: any difference between statics and dynamics? Crit Care Med 41:1046–1055
Gattinoni L, Carlesso E, Cadringher P, Valenza F, Vagginelli F, Chiumello D (2003) Physical and biological triggers of ventilator-induced lung injury and its prevention. Eur Respir J Suppl 47:15s–25s
Neto AS, Hemmes SN, Pelosi P, de Abreu MG, Schultz MJ, PROVE Network Investigators (2016) Role of shear stress in ventilator-induced lung injury—authors’ reply. Lancet Respir Med 4:e43
Gattinoni L, Tonetti T, Cressoni M, Cadringher P, Herrmann P, Moerer O, Protti A, Gotti M, Chiurazzi C, Carlesso E, Chiumello D, Quintel M (2016) Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med 42:1567–1575
Nieman GF, Satalin J, Andrews P, Habashi NM, Gatto LA (2016) Lung stress, strain, and energy load: engineering concepts to understand the mechanism of ventilator-induced lung injury (VILI). Intensive Care Med Exp 4:16–21
Gattinoni L, Tonetti T, Quintel M (2018) Intensive care medicine in 2050: ventilator-induced lung injury. Intensive Care Med 44:76–78
Maia LA, Samary CS, Oliveira MV, Santos CL, Huhle R, Capelozzi VL, Morales MM, Schultz MJ, Abreu MG, Pelosi P, Silva PL, Rocco PRM (2017) Impact of different ventilation strategies on driving pressure, mechanical power, and biological markers during open abdominal surgery in rats. Anesth Analg 125:1364–1374
Serpa Neto A, Deliberato RO, Johnson AEW, Amorim P, Pereira SM, Cazati DC, Coridoli RL, Correa TD, Coutinho E, Schettino GPP, Timenetsky KT, Pelosi P, Gama de Abreu M, Schultz MJ (2017) Mechanical power during mechanical ventilation of critically ill patients. J Crit Care 42:392
Johnson AEW, Pollard TJ, Shen L, Lehman LW, Feng M, Ghassemi M, Moody B, Szolovits P, Celi LA, Mark RG (2016) MIMIC-III, a freely accessible critical care database. Sci Data 3:160035
Johnson AE, Stone DJ, Celi LA, Pollard TJ (2018) The MIMIC code repository: enabling reproducibility in critical care research. J Am Med Inf Assoc 25:32–39
Goldberger AL, Amaral LA, Glass L, Hausdorff JM, Ivanov PC, Mark RG, Mietus JE, Moody GB, Peng CK, Stanley HE (2000) PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation 101:e215–e220
ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS (2012) Acute respiratory distress syndrome: the Berlin definition. JAMA 307:2526–2533
Matthews JN, Altman DG, Campbell MJ, Royston P (1990) Analysis of serial measurements in medical research. BMJ 300:230–235
De Jong A, Cossic J, Verzilli D, Monet C, Carr J, Conseil M, Monnin M, Cisse M, Belafia F, Molinari N, Chanques G, Jaber S (2018) Impact of the driving pressure on mortality in obese and non-obese ARDS patients: a retrospective study of 362 cases. Intensive Care Med 47:453–463
Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, LUNG SAFE Investigators, ESICM Trials Group (2016) Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 315:788–800
Neto AS, Barbas CSV, Simonis FD, Artigas-Raventós A, Canet J, Determann RM, Anstey J, Hedenstierna G, Hemmes SNT, Hermans G, Hiesmayr M, Hollmann MW, Jaber S, Martin-Loeches I, Mills GH, Pearse RM, Putensen C, Schmid W, Severgnini P, Smith R, Treschan TA, Tschernko EM, Melo MFV, Wrigge H, de Abreu MG, Pelosi P, Schultz MJ, PRoVENT, PROVE Network Investigators (2016) Epidemiological characteristics, practice of ventilation, and clinical outcome in patients at risk of acute respiratory distress syndrome in intensive care units from 16 countries (PRoVENT): an international, multicentre, prospective study. Lancet Respir Med 4:882–893
Marini JJ, Crooke PS 3rd (1993) A general mathematical model for respiratory dynamics relevant to the clinical setting. Am Rev Respir Dis 147:14–24
Marini JJ, Gattinoni L (2018) Energetics and the root mechanical cause for ventilator-induced lung injury. Anesthesiology 128:1062–1064
Slutsky AS, Ranieri VM (2013) Ventilator-induced lung injury. N Engl J Med 369:2126–2136
Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342:1301–1308
Serpa Neto A, Cardoso SO, Manetta JA, Pereira VG, Espósito DC, Pasqualucci Mde O, Damasceno MC, Schultz MJ (2012) Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA 308:1651–1659
Briel M, Meade M, Mercat A, Brower RG, Talmor D, Walter SD, Slutsky AS, Pullenayegum E, Zhou Q, Cook D, Brochard L, Richard JC, Lamontagne F, Bhatnagar N, Stewart TE, Guyatt G (2010) Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA 303:865–873
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators, Cavalcanti AB, Suzumura ÉA, Laranjeira LN, Paisani DM, Damiani LP, Guimarães HP, Romano ER, Regenga MM, Taniguchi LNT, Teixeira C, Pinheiro de Oliveira R, Machado FR, Diaz-Quijano FA, Filho MSA, Maia IS, Caser EB, Filho WO, Borges MC, Martins PA, Matsui M, Ospina-Tascón GA, Giancursi TS, Giraldo-Ramirez ND, Vieira SRR, Assef MDGPL, Hasan MS, Szczeklik W, Rios F, Amato MBP, Berwanger O, Ribeiro de Carvalho CR (2017) Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA 318:1335–1345
Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, Stewart TE, Briel M, Talmor D, Mercat A, Richard JC, Carvalho CR, Brower RG (2015) Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 372:747–755
Neto AS, Hemmes SN, Barbas CS, Beiderlinden M, Fernandez-Bustamante A, Futier E, Gajic O, El-Tahan MR, Ghamdi AA, Günay E, Jaber S, Kokulu S, Kozian A, Licker M, Lin WQ, Maslow AD, Memtsoudis SG, Reis Miranda D, Moine P, Ng T, Paparella D, Ranieri VM, Scavonetto F, Schilling T, Selmo G, Severgnini P, Sprung J, Sundar S, Talmor D, Treschan T, Unzueta C, Weingarten TN, Wolthuis EK, Wrigge H, Amato MB, Costa EL, de Abreu MG, Pelosi P, Schultz MJ, PROVE Network Investigators (2016) Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data. Lancet Respir Med 4:272–280
Santos RS, Maia LA, Oliveira MV, Santos CL, Moraes L, Pinto EF, Samary CDS, Machado JA, Carvalho AC, Fernandes MVS, Martins V, Capelozzi VL, Morales MM, Koch T, Gama de Abreu M, Pelosi P, Silva PL, Rocco PRM (2018) Biologic impact of mechanical power at high and low tidal volumes in experimental mild acute respiratory distress syndrome. Anesthesiology 128:1193–1206
Acknowledgments
To the team of the Laboratory for Computational Physiology from the Massachusetts Institute of Technology (LCP-MIT) who work to keep the MIMIC-III and eICU databases available and who organized the MIT-Datathon in São Paulo, Brazil.
Author information
Authors and Affiliations
Consortia
Contributions
ASN designed the study, conducted the data collection, data analysis, and data interpretation, and wrote the manuscript. ROC conducted the data collection, the data interpretation, and reviewed the manuscript. AEWJ conducted the data collection, the data interpretation, and reviewed the manuscript. LDB conducted the data collection, the data interpretation, and reviewed the manuscript. PA designed the study, conducted the data collection, and reviewed the manuscript. SMP designed the study, conducted the data collection, and reviewed the manuscript. DCC designed the study and reviewed the manuscript. RLC designed the study and reviewed the manuscript. TDC designed the study and reviewed the manuscript. GPPS designed the study and reviewed the manuscript. KTT designed the study and reviewed the manuscript. PP designed the study, conducted the data interpretation, and reviewed the manuscript. MGA designed the study, conducted the data interpretation, and reviewed the manuscript. MJS designed the study, conducted the data interpretation, and reviewed the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declared that they have no conflict of interest.
Additional information
The PROVE Network investigators—PROVE Network: the PROtective VEntilation Network (http://www.provenet.eu).
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Serpa Neto, A., Deliberato, R.O., Johnson, A.E.W. et al. Mechanical power of ventilation is associated with mortality in critically ill patients: an analysis of patients in two observational cohorts. Intensive Care Med 44, 1914–1922 (2018). https://doi.org/10.1007/s00134-018-5375-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-018-5375-6