
Abstract
Introduction
Posttraumatic swelling causes a delay in surgery, a prolonged hospital stay and a higher risk of complications. Thus, soft tissue conditioning following complex ankle fractures is of central importance in their perioperative management. Since the clinical benefit of VIT usage on the clinical course has been shown, it should now be investigated whether it is also cost-efficient in doing so.
Materials and methods
Included are published clinical results of the prospective, randomised, controlled, monocentric VIT study that have proven the therapeutic benefit in complex ankle fractures. Participants were allocated in a 1:1 ratio into the intervention group (VIT) and the control group (elevation). In this study, the required economic parameters of these clinical cases were collected on the data of the financial accounting and an estimation of annual cases had been performed to extrapolate the cost-efficiency of this therapy. The primary endpoint was the mean savings (in €).
Results
Thirty-nine cases were studied in the period from 2016 to 2018. There was no difference in the generated revenue. However, due to lower incurred costs in the intervention group, there were potential savings of about €2000 (pITT = 0.073) to 3000 (pAT = 0.008) per patient compared to the control group with therapy costs decreasing as the number of patients treated increases from €1400 in one case to below €200 per patient in 10 cases. There were 20% more revision surgeries in the control group or 50 min more OR time, respectively, and an increased attendance by staff and medical personnel of more than 7 h.
Conclusions
VIT therapy has been shown to be a beneficial therapeutic modality, but it is so not only in regard to soft-tissue conditioning but also cost efficiency.
Similar content being viewed by others


Introduction
Ankle fractures place an enormous socio-economic burden due to their high incidence and common complications, especially in cases with complex fractures [1,2,3,4,5]. The sole resulting incapacity to work, which according to data from a German health insurance, leads to 1 million days of work incapacity per 100,000 insured persons, resulting in an average loss of approximately €200 per day [6, 7]. In addition, however, these fractures also place a high burden on trauma departments due to the long course to soft tissue conditioning and eventual discharge [8,9,10]. Developed for thromboprophylaxis in the 1980s but increasingly used for soft-tissue conditioning are systems for intermittent pneumatic compression (IPC) as is the so-called Vascular Impulse Technology (VIT). By exerting pressure on the venous plexus of the foot it is thought to result in an improved microcirculation with decongestant and antithrombotic effects, decreasing hypoxia and pain and increasing venous return [11,12,13,14]. Numerous studies—the most recent by Schnetzke et al. [15]—have already proven their clinical benefits, for the thromboprophylactic effect as well as improved decongestion, shorter hospital stays and fewer revision surgeries [15,16,17]. In a previous study it could be shown that administration of the VIT therapy led to a significant decreased delay to surgery of 2–3 days, a significant lower pain intensity, a significantly faster oedema reduction and a significantly lower revision surgery rate [15].
What has not been investigated, though, is to what extend these clinical advantages provide an economic effect.
In 2012, Feldman et al. wrote in their systematic review on IPC that an assessment of the economic benefit of these was urgently needed given the high initial cost of the devices compared to other modalities [18]. The only figures they found were based on a single case study of lymphedema [19]. Though the work of Thordarson already refers to the cost factor in 1997, it only mentions generally that a reduction in costs of USD 2000 could be achieved per day of shorter length of stay [20]. This thesis, however, was not based on actual study data, but on the author’s opinion. More accurate yet vague data were provided by Stöckle et al. when they compared VIT therapy with various methods of cooling in 1997 [21]. Here, they spoke of either initial costs of about $4000 per device or weekly rental costs of about $170 per device and $35 per footpad. However, an actual analysis of the total costs incurred and a comparison of these with the revenues from the different groups was not made either.
Thus, this is the first study to address this question specifically, including prospectively randomised case data and a detailed analysis of revenues and costs.
The aim of this study was to investigate whether VIT therapy leads to an economic benefit due to a reduction in costs incurred, to quantify this benefit and to extrapolate it to the economic potential outside of limiting study conditions.
Materials and methods
In this study, the available data of 39 ankle fractures from the prospective randomised controlled trial performed at the BG Trauma Center Ludwigshafen during the period from 2016 to 2019 were analysed. The VIT study had been registered at the DRKS (german clinical trial registry, an approved primary registry in the WHO network; DRKS00010510) and the study protocol had been published a priori [22]. Sample size calculation for the clinical trial resulted in 34 complete datasets that would be necessary to show a reduction in delay to surgery of 2 days with a power of 80% and a significance level of 5%. These were patients with bimalleolar ankle fractures that could not be definitively treated surgically on the day of admission due to soft tissue swelling and received inpatient soft-tissue conditioning. Patients aged 18 to 80 years, without an injury to the contralateral extremity, were included. Patients with open fractures, local soft tissue problems (tension blisters, necrosis, compartment syndrome), or decompensated heart failure, thrombosis, or pulmonary artery embolism were excluded. After informed consent, they were randomised in a 1:1 ratio to the intervention and control group.
Patients in the intervention group received VIT therapy for soft-tissue conditioning and were instructed to use it 24 h per day preoperatively if possible and at least 6 to 8 h per day postoperatively. VIT therapy was performed using the VADOplex device (OPED GmbH, Oberlaindern, Germany). This air compressor inflates and deflates an air bubble, placed under the sole of the foot by a foot pad, to a pressure of 130 mmHg within one second at an interval of 20 s. The control group received exclusively elevation of the extremity. No further soft tissue conditioning measures were allowed to be applied in either group. Blinding throughout the clinical study was not possible due to the obvious difference in interventions. However, the primary outcome parameter and daily treatment were conducted by independent residents and consultant surgeons not involved in the study. The detailed description of the clinical study course, its results and limitations can be found in the paper previously published in 2021 [15].
After business accounting had been completed, it was now possible to use the case numbers of these patients to calculate the revenue, the detailed costs and thus the contribution margin generated in the individual cases. In addition, the same parameters were collected for all ankle fractures treated in 2018. Revenues were provided in form of the payment received by the health insurer per case and incurred costs included staff wages (physical therapy, surgical ward, anaesthesology and OR), pharmaceutical expenses and medical and non-medical infrastructural costs.
Statistics
As a primary outcome, it was investigated whether a statistically significant difference could be found between the VIT patients and the control group regarding the contribution margin calculated as the difference between total revenues achieved and all incurred costs in every case. This difference was compared in regard of difference in number of surgeries, total OR time and care provided by medical staff in minutes. In addition, it was examined how many ankle fractures were treated at the institution in 2018 in order to extrapolate the result to the actual annual number of cases and thus more accurately assess the economic impact. The collected data are presented using appropriate descriptive statistics (mean ± standard deviation, median with Q1 and Q3). Data were analysed, according to the intention-to-treat principle (ITT) firstly and secondly, as a sensitivity analysis, using the as-treated principle (AT), according to the therapy actually performed. Two-sided p-values were calculated for continuous characteristics using the t-test for unequal variances or the Mann–Whitney U-test, and for nominally scaled variables using the Chi2 or Fischer’s exact test. Pearson’s r was calculated to analyse correlation between allocated study group and economic impact.
Statistical analyses were performed and graphics desined using the Prism program from GraphPad Software, version 8.3.1 and statistical significance was set at p < 0.05.
Results
Complete data sets from 39 patients were available for analysis. No significant differences could be found in regard of demographic parameters, which are shown in detail in Table 1. According to the ITT principle 20 patients were analysed in the VIT group and 19 in the control group. However, in the sensitivity analysis, only 17 patients in the VIT group but 22 in the control group were analysed because of inadequate compliance in the use of the device in three cases. Patient demographics were comparable in terms of age, sex, injured side, fracture classification, and previous diseases.
No significant differences could be found analysing the total length of stay (4 days, 95% CI [− 0.8; 8.9], in favour of the VIT group; p = 0.101) and the total revenues (comparable in both groups, p = 0.921; s. Table 2). A relevant difference in incurred costs of €2200 (95% CI [850; 5200]) in favour of the VIT group could be seen, but it did not reach statistical significance (p = 0.140; s. Table 2). These reduced costs resulted mainly from less personnel (medical, nursing and administrative services) and general infrastructural expenses. Because of the longer inpatient stay (difference between medians of 4 days) and the higher rate of revision surgeries, there were mean additional costs in the control group of €540 on the trauma ward and €690 in the OR. The costs in the OR were caused by 20% more surgeries or an average of 50 min longer OR time, respectively. The raised costs in the ward were due to a need of 360 min more attendance by medical, nursing and administrative staff and 70 min more by personnel of the anaesthesiology department.
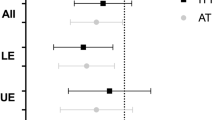
Comparing the contribution margin showed a tendency towards a larger profit in the VIT group in the ITT-analysis with a delta of €2000 (95% CI [210; 4200], pITT = 0.073) and a significant difference in the sensitivity analysis with a delta of €3000 (95% CI [870; 5000], pAT = 0.008; s. Table 2 and Fig. 1). Correlation analysis led to a Pearson’s r of − 0.42 and a p-value of 0.008. The post-hoc power analysis—that was applied since sample size calculation focused on the clinical outcome—lead to an achieved power of 0.8.

Comparison between the VIT and control group in regard of a the total length of inpatient stay depicted in Kaplan–Meier curves, b the revenues and costs per case presented in mean with standard deviation and c the incurred contribution margin according to ITT and AT compared by boxplots
In 2018 a total of 354 patients who suffered an ankle fracture were treated at the institution with a mean length of stay of 13 days (5 days less than the average study patient). Both the mean costs and the revenues were also below the study average, with a difference of approximately €660 in the former and €3200 in the latter case.
In treating one patient with the VIT therapy costs of €1200 would be incurred for the intermittent pneumatic compression device, about €100 for the foot pads (2–3 pieces, depending on usage) and €75 for maintenance fees. In total, this would amount to €1400. Since the devices can be repeatedly used and the maintenance fees are calculated annually, the more patients are treated, the lesser the cost would be in the single case, reaching a steady state below €200 per case after 10 patients treated. These expenses and the extrapolation to the estimated annual cases at this institution, are detailed in Table 3.
The relation between therapy costs and net profit as a function of patient numbers is displayed in Fig. 2.

Cost-efficiency of the VIT therapy. Costs of and profit by VIT therapy are displayed per patient. As can be seen, even in the first patient a net profit of around €600 can be achieved after all therapeutic costs have been deducted, reaching a steady state of around €1800 after 10 patients
Discussion
The purpose of this study was to investigate whether treatment with an intermittent pneumatic compression (IPC) device could provide economic benefits in addition to the proven clinical benefits. The Vascular Impulse Technology (VIT) has been introduced as a method for IPC in the 1980s, primarily as a means of thrombosis prophylaxis [11, 12]. For this purpose, the devices have also been best evaluated and already represent a standard therapeutic agent in hip and knee arthroplasty [13, 14, 23, 24]. Subsequently, studies focusing on the clinical benefit have been conducted showing a reduced delay to surgery and inpatient stay, less pain and need for analgesics, and fewer complications and revisions [11,12,13,14,15,16,17, 25, 26]. Though some papers noted high therapeutic costs of this intervention, whether it offers an economic benefit, as could be expected from shorter hospital stays and revisions, has never been assessed. Papers addressing this topic treated it merely as a minor issue in the discussion relying on vague estimated values or solely on the author’s opinion [18, 20, 21]. An actual analysis has never been performed, this study being the first to do so.
According to these findings, a potential saving in the VIT group could be found by €2000 regarding the ITT population (pITT = 0.073), being statistically significant with €3000 in the sensitivity analysis, respectively (pAT = 0.008). Upon comparison of the incurred costs of it can be concluded that with €1400 for a single patient but below €200 if more than 10 patients are treated each year, the VIT therapy resembles a cost-efficient therapeutic modality, in a single case but even more in repeated usage.
However, transferring it to the average and more benign ankle fractures is difficult and only possible to a limited extent at all. As could already be demonstrated in the shorter length of stay and the lower revenues and costs of all patients admitted with ankle fractures in general, the study patients suffered more severe fractures resulting in strained soft tissue conditions and thus being more prone to complications. Since the dislocated bimalleolar fractures, as included in the prior study, have an incidence of 15–20% among all ankle fractures it was assumed that of the 354 patients admitted in 2018 62 would have suffered from such an injury [2]. In these 62 cases a possible cost saving of €120,000 (ITT) or €185,000 (AT) could be achieved.
Another potential factor for the cost-effectiveness of VIT therapy is that this therapy reduces the median length of stay of these patients by four days (see Fig. 2). German health insurance companies pay hospitals according to diagnosis-related groups (DRG), resulting in fixed budgets depending on the injury sustained. The complexity and prolonged length of stay for complex joint fractures mean that the costs are not covered by the flat-rate payment by the health insurance funds. Resulting from this: the highest profit is made if the patient is discharged when the average length of stay (16 days for ankle fractures) is reached. As soon as the upper limit is exceeded, additional hospital days no longer lead to higher remuneration and have a negative impact on hospital accounting. In the study group, no case of exceeding the upper limit was observed—as did in the control group in 17% of their cases—and the mean length of stay corresponded to the average length of stay resulting from this DRG.
Concluding from a difference of 50 min OR time and around 7 h less personnel resources compared to incurred costs of below €200 if used frequently, the VIT therapy is a cost-efficient therapeutic modality in soft-tissue conditioning.
Limitations
The first limitation to be mentioned is that this was not a blinded study, as the intervention using the intermittent pneumatic compression device could not be simulated in placebo form for the control group. Thus, a bias because of any influence by the treating physicians cannot be ruled out completely. What was also not taken into account was the time and resources needed to ensure adequate treatment adherence, i.e. instruction of device usage, answering questions that arose or removing and reapplying the pad if dislocated. However, compared to the actual costs incurred and estimated, this would only be a small amount, assuming a time of 20–30 min per patient.
The main limitation is of course that the transfer of the potential savings from a controlled study population upon everyday treatment is only an extrapolation. If the possible savings reach the estimated number needs to be proved in further studies. However, that there is an actual possible economic benefit had been shown by the data of the RCT that had been conducted before this analysis was even planned. So there’s only a limited chance that an observer bias for example could have influenced the data in this regard. Especially figures like OR time and number of revision surgeries as objective parameters should not be susceptible to being influenced by this.
Conclusion
VIT therapy is not only an efficient adjunct to current methods for soft tissue conditioning and can improve patient care but is also cost-efficient, even if used infrequently.
Availability of data and materials
Raw data were generated at the BG Trauma Center Ludwigshafen. These and the derived data supporting the findings of this study are available from the corresponding author on request.
Code availability
Not applicable.
References
Anderson SA, et al. Ankle fractures in the elderly: initial and long-term outcomes. Foot Ankle Int. 2008;29(12):1184–8.
Daly PJ, et al. Epidemiology of ankle fractures in Rochester. Minnesota Acta Orthop Scand. 1987;58(5):539–44.
Klos K, et al. Fractures of the ankle joint in elderly patients. Unfallchirurg. 2017;120(11):979–92.
Vioreanu M, et al. Early mobilization in a removable cast compared with immobilization in a cast after operative treatment of ankle fractures: a prospective randomized study. Foot Ankle Int. 2007;28(1):13–9.
Wright DJ, Bariteau JT, Hsu AR. Advances in the surgical management of ankle fractures. Foot & Ankle Orthopaedics. 2019;4(4):2473011419888505.
Goost H, et al. Fractures of the ankle joint: investigation and treatment options. Dtsch Arztebl Int. 2014;111(21):377–88.
Health., G.F.O.f.W.S.a.O., National economic costs by work incapacity 2019. 2019: Dortmund.
Gutsfeld P, et al. Orthesen in der Unfallchirurgie. Trauma und Berufskrankheit. 2016;18(2):116–24.
Honigmann P, et al. Aftertreatment of malleolar fractures following ORIF – functional compared to protected functional in a vacuum-stabilized orthesis: a randomized controlled trial. Arch Orthop Trauma Surg. 2007;127(3):195–203.
Kimmel LA, et al. Rest easy? Is bed rest really necessary after surgical repair of an ankle fracture? Injury. 2012;43(6):766–71.
Gardner AM, et al. Reduction of post-traumatic swelling and compartment pressure by impulse compression of the foot. J Bone Joint Surg Br. 1990;72(5):810–5.
Morgan R, et al. Arterial flow enhancement by impulse compression. Vasc Surg. 1991;25(1):8–15.
O’Connell S, et al. The use of intermittent pneumatic compression in orthopedic and neurosurgical postoperative patients: a systematic review and meta-analysis. Ann Surg. 2016;263(5):888–9.
Wilson NV, et al. Thrombo-embolic prophylaxis in total knee replacement: evaluation of the A-V Impulse System. J Bone Joint Surg Br. 1992;74(1):50–2.
Schnetzke M, et al. Vascular impulse technology versus elevation for the reduction of swelling of lower extremity joint fractures: results of a prospective randomized controlled study. Bone Joint J. 2021;103-B(4):746–54.
Caschman J, Blagg S, Bishay M. The efficacy of the A-V Impulse system in the treatment of posttraumatic swelling following ankle fracture: a prospective randomized controlled study. J Orthop Trauma. 2004;18(9):596–601.
Myerson MS, Henderson MR. Clinical applications of a pneumatic intermittent impulse compression device after trauma and major surgery to the foot and ankle. Foot Ankle. 1993;14(4):198–203.
Feldman JL, et al. Intermittent pneumatic compression therapy: a systematic review. Lymphology. 2012;45(1):13–25.
Hammond, T. Reduction of complications and associated costs with flexitouch® therapy for lymphedema. Open Rehabil J. 2009;2(1).
Thordarson DB, Ghalambor N, Perlman M. Intermittent pneumatic pedal compression and edema resolution after acute ankle fracture: a prospective, randomized study. Foot Ankle Int. 1997;18(6):347–50.
Stöckle U, et al. Fastest reduction of posttraumatic edema: Continuous cryotherapy or intermittent impulse compression? Foot Ankle Int. 1997;18(7):432–8.
Schnetzke M, et al. Vascular Impulse Technology versus elevation in the treatment of posttraumatic swelling of extremity fractures: study protocol for a randomized controlled trial. Trials. 2017;18(1):73.
Ivanic GM, et al. Intermittent compression devices for swelling reduction and thrombosis prophylaxis–a pilot study after total hip replacement: Is the 2 hour daily minimum application sufficient? Unfallchirurg. 2006;109(9):786–92.
Stannard JP, et al. Prophylaxis of deep venous thrombosis after total hip arthroplasty by using intermittent compression of the plantar venous plexus. Am J Orthop (Belle Mead NJ). 1996;25(2):127–34.
Dodds MK, et al. Effectiveness of “in-cast” pneumatic intermittent pedal compression for the pre-operative management of closed ankle fractures: a clinical audit. Foot Ankle Surg. 2014;20(1):40–3.
Thordarson DB, et al. Facilitating edema resolution with a foot pump after calcaneus fracture. J Orthop Trauma. 1999;13(1):43–6.
Funding
Open Access funding enabled and organized by Projekt DEAL. We gratefully acknowledge the funding of the BG Trauma Center Ludwigshafen and the company OPED. The sponsors had no influence on the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
MS, JF and JSEB designed and directed the study. Main conduction of the study and analysis were performed by JSEB, who has also written the first draft of the manuscript. All authors commented on previous versions of the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in this study involving human participants were in accordance with the ethical standards of the Ethics Committee of the State Medical Association of the Rhineland-Palatinate and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. The study was registered in the German Clinical Trials Registry (DRKS00010510), approval was given by the Ethics Committee of the Rhineland-Palatinate State Medical Association (837.155.16/10474). Informed and signed consent was obtained from all individual participants included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article. Data collection, coding, routing and analysis were in accordance with legal data protection policy.
Consent for publication
The authors affirm that human research participants provided informed consent for publication of their anonymised data.
Competing interests
The other authors declare an institutional grant from OPED GmbH but none of the authors has received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
El Barbari, J.S., Schnetzke, M., Swartman, B. et al. Analysis of the cost-efficiency of the vascular impulse technology (VIT) in the perioperative management of complex ankle fractures: results of a prospective randomised controlled trial. J Orthop Surg Res 18, 159 (2023). https://doi.org/10.1186/s13018-023-03587-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03587-x