
Abstract
Background
Total hip arthroplasty (THA) is increasingly common in younger patients, who are more likely to be working preoperatively. There is a need for an updated review of the literature regarding the rate and time to return to work (RTW), which is important when counseling patients, and also from an economic standpoint.
Methods
A systematic review and meta-analysis of the literature was performed on January 20, 2022, and studies reporting the rate and/or time to RTW after THA were included. Two authors independently selected relevant papers. RTW was extracted and analyzed using fixed-effects or random-effects models where appropriate.
Results
A total of 48 studies were included in the final analysis. We found that 70.7% of patients were working after primary THA. Among patients who were working before surgery, this rate increases to 87.9%, while 28.1% of patients who were not working preoperatively started working after surgery. Younger patients were more likely to RTW, while patients with a physically demanding job were less likely to RTW. Minimally invasive techniques were reported to yield a higher rate of RTW and an earlier time to RTW.
Conclusion
We found that the majority of patients return to work after THA, and some patients are able to start working after surgery. Compared to previous reviews, patients seem to have a higher rate and earlier RTW. The overall trend of the literature suggests that patients are returning to work earlier and at a higher rate compared to previous reviews.
Similar content being viewed by others


Introduction
As the volume of total hip arthroplasties (THA) is increasing globally, the number of younger patients is also growing. With the advent of modern surgical techniques and the increasing longevity of current designs, patients younger than 65 years are expected to constitute more than half of all arthroplasties in the USA by 2030 [1]. In addition, the number of THAs performed is projected to double during the same period. Therefore, functional outcomes of THA and the patients’ return to activities are an increasingly important metric in measuring success after hip reconstruction.
Data on return to daily activities after THA, including return to sports and return to work (RTW), are scarce in the literature. RTW after THA in patients of working age has a substantial economic impact on the patient, family, and the healthcare system, as well as the psychological and physical benefits to the individual [2]. Previous studies have been heterogeneous regarding the rate and timing of RTW, reporting a wide range from 25 to 122%, the latter indicating more patients being working at the follow-up [3]. Interestingly, more recent reports show a trend of an increasing rate of RTW, as well as a shorter duration of inability to work after surgery. The last study to systematically review the RTW data was performed in 2017, and considering the fast pace of the current joint literature and several more recent papers on this topic, there is a need for an updated review [3].
Therefore, this study was performed to systematically review the current joint literature to determine the rate of return to work after THA, time to RTW, and the potential predictors for successful RTW following THA. The results of this study would be important not only to surgeons and the healthcare system, but also to patients who will be directly affected by this outcome.
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed to perform this systematic review. The study protocol was also published on the international prospective register of systematic reviews, PROSPERO (record number CRD42022307385, available at https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022307385).
Search strategy
We performed a systematic review on January 20, 2022. We searched PubMed MEDLINE, Embase, Scopus, Web of Science, and the Cochrane library. Search queries were personalized to follow each database’s rules and regulations, with the general term of ("Total Hip Replacement" OR "Total Hip Arthroplasty" OR "Hip Prosthesis Implantation") AND ("Return to Work" OR "Back to Work" OR "Return to occupation").
PICO and inclusion/exclusion criteria
Clinical trials, retrospective, and prospective observational studies with a study population of adults were selected.
Our targeted population included the patients underwent total hip replacement (Patients and interventions), the outcomes compared between subgroups were the rate and time of returning to work and also the factors affecting return to work (comparison and outcome).
Exclusion criteria were: revision THA, those surgeries that were not primary were excluded from our studies, THA in combination with another surgical procedure was the other exclusion criteria, That is, only those studies were added that patients had undergone a total hip arthroplasty surgery and had not performed another surgery at the same time or in the same admission that would affect the results of the hip replacement surgery. Review articles, book chapters, case reports, and non-English studies were other exclusion criteria. With all these, there was no limit to the publication year of selected studies.
Quality assessment
The MINORS (Methodological Index for Non-Randomized Studies) criteria was utilized to assess study quality. MINORS is a framework for scoring non-randomized studies such as observational and descriptive studies. MINORS includes 12 items graded from 0 to 2, with maximum scores of 16 for non-comparative studies and 24 for comparative studies. Higher scores indicate a higher quality of evidence [4]. Scores of 0–8 or 0–12 were considered low quality, 9–12 or 13–18 were deemed to be moderate quality, and 13–16 or 19–24 were regarded as high quality, respectively, for non-comparative and comparative studies (Appendix 1).
Data extraction
EndNote version 20 (Clarivate, Philadelphia, PA) was used to screen the articles. Two reviewers (M.B. and M.S.) independently reviewed the titles and abstracts of each paper to select relevant papers. Discrepancies were addressed by a third author (P.M.). Data from the selected studies were collected by two reviewers (M.B. and M.S.). The course of each person's review was as follows: After extracting the articles from the databases introduced, in the screening stage the duplicated items were excluded, and then, the titles and summaries were checked. At this stage, a number of articles were selected for full-text review. In the review of the full text, the studies that did not investigate the desired outcomes were excluded. Finally, after these reviews, the remaining studies were selected for systematic review, while the studies that the reports of the results could be analyzed in terms of meta-analysis were also included in the meta-analysis cycle.
Quality of the evidence (GRADE system)
GRADE is a system for assessing the quality of the evidence of each result in a review against eight criteria (including risk of bias, inconsistency, indirectness, imprecision, and publication bias). In the GRADE system, the quality of evidence for each outcome is graded as HIGH, MODERATE, LOW or VERY LOW. Quality of evidences assessment for this study was done separately the by two authors (M.S & M.B) and the final conclusion was made by evaluating their results.
Statistical analysis
RTW data were pooled using Comprehensive Meta-Analysis (CMA) software (BioStat Inc., Englewood, NJ). Depending on the degree of statistical heterogeneity, either fixed-effects or random-effects models were used. Statistical heterogeneity was tested using the tau-squared test and I-squared test, that was completed with the I2 statistic, which quantifies the proportion of total variation across studies that is due to heterogeneity. A value of 0–25% indicates insignificant heterogeneity, while 26–50% low heterogeneity, 51–75% moderate heterogeneity and 76–100% high heterogeneity. This study calculated the pooled weighted event rates of RTW. The 95% confidence interval was used to calculate the mean prevalence. The funnel plot and Egger's regression with a 95% confidence interval were used to evaluate publication bias.
Results
Study characteristics
The initial search yielded 633 records. After multiple rounds of screening and exclusion, 48 articles were finally included in the qualitative synthesis (Fig. 1) [2, 5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52].

Flow diagram outlining the process of study selection. Adapted from the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement
In the initial screening, 633 articles were selected, which reached 453 after removing duplicates, 395 were excluded from the study in the title and abstract review, and finally 58 studies were subjected to full-text review among these 9 articles excluded for not paying to the outcomes in question and one study due to not paying attention to the primary total hip arthroplasty (dealing with revision arthroplasty) were excluded from the study. Finally, 48 studies were selected and subjected to systematic review, and 41 of them had the desired characteristics for meta-analysis.
As shown in Table 3, the included studies had an average MINORS score of 14.8 ± 4.3 (range, 7–23), indicating a moderate quality of evidence. There were 11 studies with high quality, 36 with moderate quality, and 1 with low quality. The 48 included studies were published between 1965 and 2022, comprising a combined population of 9267 patients. The mean follow-up ranged from 6 weeks to 20.1 years. Table 1 summarizes the basic characteristics of these studies, and the outcomes of interest, including the RTW rate and time to RTW, are shown in Table 2.
Preoperative working status and RTW rate
Table 2 summarizes the outcomes of included studies regarding working status before THA and RTW rates after primary THA. A total of 28 studies reported the preoperative working status, ranging from 21 to 100%. The same number of studies reported a rate of 11.1–95.7% for postoperative RTW (Fig. 2). The proportion of patients who working after THA compared to before THA ranged from 0.3 to 1.9.

Ratio of patients working after THA in the selected studies
The pooled rate of working after THA in all patients using a random-effects model was 70.7% (95% CI = 61.0–78.8%, I2 = 97.4, Fig. 2). Figure 3 illustrates the funnel plot for publication bias with the Egger’s regression (P = 0.006).

Funnel plot showing publication bias in the included studies
The pooled rate of working after THA in patients who worked before, meaning a true RTW, using a random-effects model, was 87.9% (95% CI = 79.3–93.3%, I2 = 97.1, Fig. 4). The studies showed substantial publication bias both in the funnel plot and Egger's regression (P < 0.001).

Rate of return to work after THA in patients who worked before surgery
The pooled rate of working after THA surgery in the group of patients who did not work before that means “start to work”, using a random-effects model, was 28.1% (95% CI = 17.2–42.2%, I2 = 91.6, Fig. 5). The studies did not show substantial publication bias in the funnel plot (Fig. 6) and Egger's regression (P = 0.57).

Percentage of non-working patients who started to work after THA

Funnel plot for publications bias in studies that reported “start to work” after THA
Quality of evidences
In assessing the quality of evidence based on GRADE system [53], “working after THA surgery in the group of patients who did not work” showed moderate quality of evidence, while other outcomes, “working after THA in all patients” and “working after THA in patients who worked before” showed low quality of evidence, and these results are justified by the type of included studies that were non-RCT besides the high level of heterogeneity in statistical analysis.
Time to RTW after THA
Several studies reported mean time to RTW after THA, but the data were heterogeneous. The mean shortest time to RTW was 8 days (range 1–20 days) [10], with the mean longest duration to RTW of 31 weeks in one study reporting on patients with acetabular fractures [39].
Prognostic factors
Preoperative intention to RTW Only one study assessed the “intention to return to work” and found it to be a significant predictor of RTW after THA [25].
Age Four studies found a negative correlation between age and RTW [2, 24, 43, 47], while other studies did not find an association between RTW and age [12, 20, 22, 28, 29, 40].
Time to RTW: While three studies did not find a correlation between age and time to RTW [29, 37, 40], three other studies reported shorter time to RTW in younger patients [17,18,19].
Gender Six studies found male gender to be a significant predictor of RTW [2, 12, 20, 22, 28, 45], while other studies did not find this association significant [36, 43].
Time to RTW: Six studies reported the effect of sex on time to RTW, all reporting delayed RTW in female patients [17, 18, 27, 29, 37, 45].
BMI Patients who were not obese (BMI < 30) were found to be more likely to RTW in two studies [22, 29], but other studies did not find an association between RTW and BMI [2, 12, 24, 45].
Time to RTW: Oken et al. reported earlier RTW in non-obese (BMI < 30) patients [29, 36]. Two other studies reported no effect on the time to RTW [17, 37].
Socioeconomic and education level Only two studies showed that a higher educational level is associated with RTW [24, 42], while four other studies did not find an association [2, 28, 29, 46]. Pop et al. showed that living in a rural area was predictive for patients quitting their jobs after surgery [36].
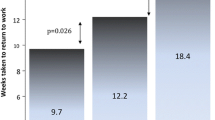
Time to RTW: Three studies reported a negative correlation between education level and time to RTW [29, 37, 51], with patients having higher educational levels returning to work earlier (9.9 vs. 12.6 weeks, P < 0.05) [29, 51]. Other studies did not find such an association [17, 29]. Additionally, Oken et al. found that single patients RTW earlier (P < 0.05) [29].
Substance use (smoking, alcohol, etc.) Two studies reported no association between RTW and smoking or alcohol use [2, 22].
Job characteristics Mental and sedentary jobs, compared to physically demanding jobs, was associated with a higher rate of return to work in several studies [12, 13, 22, 42, 47]. One study reported patients with physically demanding jobs retiring after surgery [20]. However, other studies did not find an association between RTW and physical demand [2, 28]. McGonagle et al. [25] showed a higher probability of returning to work with reduced hours and duties among those with more physically demanding jobs. Self-employment was associated with partial or no return to work in one study (OR = 7.63, 95% CI 1.5–39.8) [24], while another study revealed no such association [2]. Zaballa et al. reported fewer patients returning to jobs that required prolonged standing, kneeling, squatting, or heavy lifting [49]. One study reported higher RTW rates when preoperative job satisfaction was lower [2].
Time to RTW: Several studies reported that workers with low-to-moderate physical demands, were more likely to RTW earlier [18, 21, 37, 51]. In contrast, two other studies showed no correlation [17, 25]. RTW was reported to be delayed in jobs requiring long durations of standing [37, 49]. Self-employment [17, 37] and higher income were associated with a shorter time to RTW [37].
Indication for THA Primary osteoarthritis, compared to posttraumatic osteoarthritis or rheumatoid arthritis, was associated with a higher rate of return to work [42, 47]. A history of developmental hip dysplasia was predictive of not RTW in two studies [14, 42].
Time to RTW: One study did not find the time to RTW to be associated with indications for surgery (osteoarthritis, avascular necrosis, hip dysplasia). However, among patients with underlying hip dysplasia/dislocation, Crowe Type 1 and 2 were found to have an earlier RTW compared to Crowe types 3 and 4 [29]. The same study reported earlier RTW in patients with smaller limb length discrepancy [29].
Preoperative working status Duration of the preoperative sick leave and absence from work were associated with a lower rate of RTW in one study (OR = 8.62, 95% CI 1.9–39.0) [24].
Time to RTW: Two studies reported that patients who were not working preoperatively took a longer time to RTW [18, 27]. We also found some evidence that preoperative sick leave delayed RTW [17, 22, 51].
Preoperative functional status One study found that a negative EQ-5D score preoperatively was a negative predictor of RTW after THA, and a preoperative Oxford hip score of > 19.5 was a predictor for RTW [5]. On the other hand, Leichtenberg et al. found that a higher HOOS-ADL score weakly predicted a partial or no return to work (OR = 1.03, 95% CI 1.0–1.1) [24]. EQ-5D and other patient-reported outcome measures (PROMs) were not associated with RTW in the study by Tillbury et al. [45].
Time to RTW: Time to RTW was not significantly associated with either total physical activity level or leisure-time physical activity [11, 22]. The use of a cane, crutch, or walker before surgery was not associated with delays to RTW [37].
Postoperative functional status Postoperative walking ability was significantly correlated with RTW in one study [47]. However, improvements in PROMs following THA were not found to be associated with RTW [5, 45, 47].
Compared to similar procedures Anderson et al. found that RTW for THA was significantly higher to internal fixation or hemiarthroplasty in the treatment of displaced femoral neck fractures [6]. The rate of patients returning to work following revision THA was also found to be lower than primary THA (43.9% vs. 70.2%, P < 0.05).
Surgical approach and implants Latijnhouwers et al. reported higher rates of RTW in THAs performed with a direct anterior approach compared to a posterolateral approach within the first 3 months of surgery (31% vs. 44.6%). However, the RTW rate was similar one year postoperatively (86.2% and 84.9%) [23]. In contrast, another study found a mini-posterior approach to have a higher rate of RTW 8 weeks after surgery (97% vs. 69%) [33]. One study found a higher rate of RTW with a larger femoral head diameter [43].
Time to RTW: A minimally invasive posterior approach resulted in a significantly shorter time to return to work compared to a conventional posterior approach in one study (6.5 vs. 13.8 weeks) [37]. Comparing traditional with minimally invasive approaches, Saad et al. revealed significantly lower time to RTW in the minimally invasive group (13.8 ± 4.5 vs. 6.5 ± 0.7, P < 0.001) [50]. Tanavalee et al. reported earlier RTW in patients who underwent a successful two-incision THA compared to a mini-posterior approach [44]. However, another study did not find a difference in time to RTW between surgical approaches [31]. Hauer et al. [17] did not find the stem design to affect the time to RTW (median 10 weeks with short stem compared to 11 weeks with straight stem, P = 0.7).
Bilateral THA Early return to work rate was higher in unilateral THA compared to bilateral THA [18]. Atkinson et al. reported that the time to return to full-time employment was significantly shorter in bilateral THAs staged 1 week apart compared to delayed two-stage surgeries (22.0 vs. 35.8 weeks, P = 0.02) without an increased risk for complications [7]. In contrast, Rondon et al. did not such an association [37].
Postoperative restrictions Two studies found postoperative range of motion restrictions to be predictive for failure to RTW, with over half of patients in the unrestricted group returning to work in 6 weeks, while only 18.8% [32] and 32% [26] of the restricted group returned to work during the same period.
Time to RTW: Same studies found a significant delay in RTW in the restricted groups (6.5 vs. 9.5 weeks, p 0.001) [25, 32].
Serum markers The levels of CPK, myoglobin, C-reactive protein, interleukin-6, and tumor necrosis factor-alpha were not predictive of RTW in one study [34].
Discussion
This systematic review and meta-analysis was performed to determine the rate and time to RTW after primary THA in the current literature. The most important finding of this study was that the majority of patients return to work between 2 to 3 months after surgery. Furthermore, the rate of RTW seems to be increasing compared to previous systematic reviews. The results of this study are important in consulting patients of working age who need a THA, while also important from a healthcare economics standpoint.
In reviewing 48 studies with a combined population of 9267 patients, we found that 70.7% (95% CI = 61.0–78.8%) of patients were working after primary THA. Among patients who were working before surgery, this rate increases to 87.9% (95% CI = 79.3–93.3%). The previous systematic review, performed in 2017 by Hoorntje et al., reported 69% of patients working after THA, while 87.5% of patients working preoperatively returned to work. The increase in RTW and start-to-work rates from five years ago, while minimal, was seen in all ten newer studies published since 2017, with all ten papers reporting high rates of RTW than previously reported [9, 10, 17, 25, 31, 34, 37, 38, 41, 44]. This may be due to improved implant design, modern and minimally invasive surgical techniques, but may also be the result of increasingly younger patients, many of working age, are undergoing THA, emphasizing the importance of research on the topic. We also found that 28.1% (95%CI = 17.2–42.2%) of patients who were not working preoperatively started working after surgery, a finding not previously reported.
The studies reviewed here were not homogeneous in reporting factors predictive for RTW, but some conclusions could be made with the available data. Current suggests that younger age at surgery is associated with a higher rate of RTW [2, 24, 43, 47] and an earlier RTW [17,18,19]. Additionally, while some studies reported a delayed RTW in females compared to male patients [17, 18, 27, 29, 37, 45], the rate of RTW does not seem to be gender-related [2, 12, 20, 22, 28, 45]. Similarly, although overweight and obese patients experience delayed RTW [17, 37], the rate of RTW does not seem to be influences by BMI [2, 12, 24, 45]. Also, marital status and smoking and alcohol use were not predictive for RTW [2, 22]. However, the underlying hip pathology is important, with acetabular fractures and high-riding congenital hip dislocations having the longest RTW, exceeding 20 weeks in most reports [15, 39].
The job characteristics were also predictors of successful RTW after THA. Physically demanding jobs, and those requiring long-standing times seem to be the most important job characteristics, negatively influencing the rate of return and time RTW in several studies [12, 13, 18, 20,21,22, 37, 42, 47, 49, 51]. One study also found that providing a more flexible job schedule and reducing the physical demands of the job yield a higher rate of RTW, a luxury that is unfortunately not available for most patients [25]. Additionally, patients who missed work or had more sick leaves before surgery took a longer time to RTW, which may suggest that lower preoperative function would lead to a longer time to RTW [17, 18, 22, 27, 51].
We also found some surgical parameters influencing RTW. Minimally invasive THA and the direct anterior approach had a similar rate and speed of RTW [23, 37], superior to conventional posterior or lateral approaches [50]. Several studies showed that a minimally invasive approach resulted in faster recovery and early return to work following hip replacement surgery [50, 54,55,56]. However, implant design does not seem to be influential in RTW.
We acknowledge several limitations to this study. First, a high level of heterogenicity exists between the studies, population samples, and outcome measures involved. Second, limited by the lack of level I studies, we included retrospective and prospective cohorts as well, which makes the results more prone to bias. Third, some studies did not specify the preoperative working status of patients or the reason for not returning to work and whether it was related to surgery or not. Finally, several studies reported on a combination of THA and total knee patients, which may have different postoperative course and RTW. It was not possible to separate the data in some studies. One of the main limitations of our study is the difference in the surgical techniques considered for the patients that might be the cause of observed heterogenicity also because only limited number of studies focused minimally invasive surgeries expanding the results of this subject was not possible. Despite these limitations, we were able to provide a systematic update on the literature regarding the increasingly important topic of RTW after THA, while adding some new data to the literature. Fortunately an appropriate agreement was found between two authors searching the literature based on relevant keywords without any involving the third author for judgment.
We recommend to perform further studies with the focused on return to work considering special work condition, return to sport and physical activities and also assessing the factors influencing delayed return to work.
Conclusion
This systematic review and meta-analysis showed that 70.7% of patients were working after THA. In patients who were working before surgery, this rate increases to 87.9%, while 28.1% of patients who were not working preoperatively started working after THA. Compared to previous reviews, patients seem to have a higher rate and earlier RTW. Younger patients were more likely to RTW, while patients with a physically demanding job were less likely to RTW. Minimally invasive techniques were reported to yield a higher rate of RTW and an earlier time to RTW. The overall trend of the literature suggests that patients are returning to work earlier and at a higher rate compared to previous systematic reviews. However, THA is a major surgery specially in elderly most patients returned to their work successfully and disability after surgery seem to be low. More interestingly, the feeling to ability to physical activities postoperatively led to tending of unemployed patients to seek the job and work actively.
Availability of data and materials
Not applicable.
References
Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ. Future young patient demand for primary and revision joint replacement: national projections from 2010 to 2030. Clinical Orthopaedics and Related Research®. 2009;467(10):2606–12.
Bohm ER. The effect of total hip arthroplasty on employment. J Arthroplasty. 2010;25(1):15–8.
Hoorntje A, Janssen KY, Bolder SBT, Koenraadt KLM, Daams JG, Blankevoort L, et al. The effect of total hip arthroplasty on sports and work participation: a systematic review and meta-analysis. Sports Med. 2018;48(7):1695–726.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6.
Al-Hourani K, MacDonald DJ, Turnbull GS, Breusch SJ, Scott CEH. Return to work following total knee and hip arthroplasty: the effect of patient intent and preoperative work status. J Arthroplasty. 2021;36(2):434–41.
Anderson JT, Hudyk AR, Haas AR, Ahn NU, Rothberg DL, Gililland JM. Displaced femoral neck fractures in workers’ compensation patients aged 45–65 years: is it best to fix the fracture or replace the joint? J Arthroplasty. 2020;35(11):3195–203.
Atkinson HD, Bailey CA, Willis-Owen CA, Oakeshott RD. Bilateral hip arthroplasty: is 1-week staging the optimum strategy? J Orthop Surg Res. 2010. https://doi.org/10.1186/1749-799X-5-84.
Baldursson H, Brattstrom H, Olsson TH. Total hip replacement in ankylosing spondylitis. Acta Orthop Scand. 1977;48(5):499–507.
Batra A, Gogos S, Nizam I. When do patients drive after minimally invasive anterior hip replacements? A single surgeon experience of 212 hip arthroplasties. Sicot j. 2018;4:51.
Berger RA, Jacobs JJ, Meneghini RM, Della Valle C, Paprosky W, Rosenberg AG. Rapid rehabilitation and recovery with minimally invasive total hip arthroplasty. Clin Orthop Relat Res. 2004;429:239–47.
Boersma AR, Brouwer S, Koolhaas W, Brouwer RW, Zijlstra WP, van Beveren J, et al. No association between preoperative physical activity level and time to return to work in patients after total hip or knee arthroplasty: a prospective cohort study. PLoS ONE. 2019;14(9): e0221932.
Clyde CT, Goyal N, Matar WY, Witmer D, Restrepo C, Hozack WJ. Workers’ Compensation patients after total joint arthroplasty: do they return to work? J Arthroplasty. 2013;28(6):883–7.
Danielsson L. Arthroplasty of the hip according to Thompson and Moore. Acta Orthop Scand. 1965;35(1–4):348–57.
Drobniewski M, Borowski A, Krasińska M, Sibiński M, Synder M. Return to work after surgical treatment of coxarthrosis by total cementless hip arthroplasty. Ortop Traumatol Rehabil. 2017;19(4):349–60.
Drobniewski M, Synder M, Krasińska M, Sibiński M, Borowski A. An assessment of the return to professional activity of patients aged ≤30 years after hip replacement surgery. Int J Occup Med Environ Health. 2021;34(6):747–54.
Goeb YL, Krell EC, Nguyen JT, Carroll KM, Jerabek SA, Mayman DJ, et al. Early recovery outcomes in patients undergoing total hip arthroplasty through a posterior approach with modified postoperative precautions. J Arthroplasty. 2021;36(8):2817–22.
Hauer G, Smolle M, Zaussinger S, Friesenbichler J, Leithner A, Maurer-Ertl W. Short-stem total hip arthroplasty is not associated with an earlier return to work compared to a straight-stem design. Sci Rep. 2021;11(1):4968.
He C, He X, Tong W, Zheng W, Zhang T, Zhao J, et al. The effect of total hip replacement on employment in patients with ankylosing spondylitis. Clin Rheumatol. 2016;35(12):2975–81.
Jensen JS, Mathiesen B, Tvede N. Occupational capacity after hip replacement. Acta Orthop Scand. 1985;56(2):135–7.
Johnsson R, Persson BM. Occupation after hip replacement for arthrosis. Acta Orthop Scand. 1986;57(3):197–200.
Kamp T, Brouwer S, Hylkema TH, van Beveren J, Rijk PC, Brouwer RW, et al. Psychosocial working conditions play an important role in the return-to-work process after total knee and hip arthroplasty. J Occup Rehabil. 2021. https://doi.org/10.1007/s10926-021-10006-7.
Laasik R, Lankinen P, Kivimäki M, Aalto V, Saltychev M, Mäkelä K, et al. Return to work after primary total hip arthroplasty: a nationwide cohort study. Acta Orthop. 2019;90(3):209–13.
Latijnhouwers D, Laas N, Verdegaal S, Nelissen R, Vlieland TV, Kaptijn H, et al. Activities and participation after primary total hip arthroplasty posterolateral versus anterior approach. Osteoarthritis Cartilage. 2021;29:S249–50.
Leichtenberg CS, Tilbury C, Kuijer P, Verdegaal S, Wolterbeek R, Nelissen R, et al. Determinants of return to work 12 months after total hip and knee arthroplasty. Ann R Coll Surg Engl. 2016;98(6):387–95.
McGonagle L, Convery-Chan L, DeCruz P, Haebich S, Fick DP, Khan RJK. Factors influencing return to work after hip and knee arthroplasty. J Orthop Traumatol. 2019;20(1):9.
Mikkelsen LR, Petersen MK, Søballe K, Mikkelsen S, Mechlenburg I. Does reduced movement restrictions and use of assistive devices affect rehabilitation outcome after total hip replacement? A non-randomized, controlled study. Eur J Phys Rehabil Med. 2014;50(4):383–93.
Mobasheri R, Gidwani S, Rosson JW. The effect of total hip replacement on the employment status of patients under the age of 60 years. Ann R Coll Surg Engl. 2006;88(2):131–3.
Nevitt MC, Epstein WV, Masem M, Murray WR. Work disability before and after total hip arthroplasty. Assessment of effectiveness in reducing disability. Arthritis Rheum. 1984;27(4):410–21.
Oken FO, Yildirim OA, Asilturk M. Factors affecting the return to work of total hip arthroplasty due to of developmental hip dysplasia in in young patients. J Orthop. 2018;15(2):450–4.
Pachore JA, Shah VI, Upadhyay S, Shah K, Sheth A, Kshatriya A. Primary hip arthroplasty for the treatment of alkaptonuric hip arthritis: 3- to 24-year follow-ups. Arthroplasty. 2019;1(1):8.
Pagnano MW, Trousdale RT, Meneghini RM, Hanssen AD. Patients preferred a mini-posterior THA to a contralateral two-incision THA. Clin Orthop Relat Res. 2006;453:156–9.
Peak EL, Parvizi J, Ciminiello M, Purtill JJ, Sharkey PF, Hozack WJ, et al. The role of patient restrictions in reducing the prevalence of early dislocation following total hip arthroplasty. A randomized, prospective study. J Bone Joint Surg Am. 2005;87(2):247–53.
Poehling-Monaghan KL, Kamath AF, Taunton MJ, Pagnano MW. Direct anterior versus miniposterior THA with the same advanced perioperative protocols: surprising early clinical results. Clin Orthop Relat Res. 2015;473(2):623–31.
Poehling-Monaghan KL, Taunton MJ, Kamath AF, Trousdale RT, Sierra RJ, Pagnano MW. No correlation between serum markers and early functional outcome after contemporary THA. Clin Orthop Relat Res. 2017;475(2):452–62.
Pons M. Learning curve and short-term results with a short-stem CFP system. HIP International. 2010;20(7_suppl):52–7.
Pop T, Czenczek-Lewandowska E, Lewandowski B, Leszczak J, Podgórska-Bednarz J, Baran J. Occupational activity in patients 10 years after hip replacement surgery. Ortop Traumatol Rehabil. 2016;18(4):327–36.
Rondon AJ, Tan TL, Greenky MR, Kheir MM, Foltz C, Purtill JJ. Return to work after total joint arthroplasty: a predictive model. Orthopedics. 2020;43(5):e415–20.
Saad T, Salem K, Kadre A. Conventional versus minimally invasive total hip replacement through the posterior approach. J Arthrosc Joint Surg. 2019;7(1):26–30.
Salar N, Bilgen MS, Bilgen ÖF, Ermutlu C, Eken G, Durak K. Total hip arthroplasty for acetabular fractures: “early application.” Ulus Travma Acil Cerrahi Derg. 2017;23(4):337–42.
Sankar A, Davis AM, Palaganas MP, Beaton DE, Badley EM, Gignac MA. Return to work and workplace activity limitations following total hip or knee replacement. Osteoarthritis Cartilage. 2013;21(10):1485–93.
Stigmar K, Dahlberg LE, Zhou C, Jacobson Lidgren H, Petersson IF, Englund M. Sick leave in Sweden before and after total joint replacement in hip and knee osteoarthritis patients. Acta Orthop. 2017;88(2):152–7.
Suarez J, Arguelles J, Costales M, Arechaga C, Cabeza F, Vijande M. Factors influencing the return to work of patients after hip replacement and rehabilitation. Arch Phys Med Rehabil. 1996;77(3):269–72.
Takeuchi K, Hashimoto S, Matsumoto T, Hayashi S, Takayama K, Kuroda R. Recovery of activity level following total hip arthroplasty in patients less than 60 years of age. Hip Int. 2021;31(5):632–6.
Tanavalee A, Jaruwannapong S, Yuktanandana P, Itiravivong P. Early outcomes following minimally invasive total hip arthroplasty using a two-incision approach versus a mini-posterior approach. Hip Int. 2006;16(Suppl 4):17–22.
Tilbury C, Leichtenberg CS, Tordoir RL, Holtslag MJ, Verdegaal SH, Kroon HM, et al. Return to work after total hip and knee arthroplasty: results from a clinical study. Rheumatol Int. 2015;35(12):2059–67.
Truszczyńska A, Rąpała K, Tarnowski A, Kucharczyk W. Analysis of factors influencing return to work after total hip arthroplasty. Ortop Traumatol Rehabil. 2013;15(5):459–67.
Visuri TI, Koskenvuo MJ, Lindholm TS. Return to work and working capacity after total hip replacement. Int J Rehabil Res. 1987;10(43T):438.
White SH. The fate of cemented total hip arthroplasty in young patients. Clin Orthop Relat Res. 1988;231:29–34.
Zaballa E, Harris E, Lübbeke-Wolff A, Cooper C, Arden N, Ntani G, et al. O29 Returning to, and staying in, work after total hip arthroplasty. Rheumatology. 2021;60(Supplement_1):keab246-028.
Saad TA, Elbadry A, Salem KH, Kader KFA. Conventional versus minimally invasive total hip replacement through the posterior approach. J Arthrosc Joint Surg. 2020;7(1):26–30.
Kleim BD, Malviya A, Rushton S, Bardgett M, Deehan DJ. Understanding the patient-reported factors determining time taken to return to work after hip and knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2015;23(12):3646–52.
Mangin M, Galliot F, Houfani F, Baumann C, Mainard D. Return to work after primary total hip or knee arthroplasty. First French study. Retrospective study of 241 cases. Orthopaedics Traumatol Surg Res. 2022;108(1):103163.
Schünemann H, Hill S, Guyatt G, Akl EA, Ahmed F. The GRADE approach and Bradford Hill’s criteria for causation. J Epidemiol Community Health. 2011;65(5):392–5.
Chung WK, Liu D, Foo LSS. Mini-Incision total hip replacement—surgical technique and early results. J Orthop Surg. 2004;12(1):19–24.
Chimento GF, Pavone V, Sharrock N, Kahn B, Cahill J, Sculco TP. Minimally invasive total hip arthroplasty: a prospective randomized study. J Arthroplasty. 2005;20(2):139–44.
Fink B, Mittelstaedt A, Schulz MS, Sebena P, Singer J. Comparison of a minimally invasive posterior approach and the standard posterior approach for total hip arthroplasty. A prospective and comparative study. J Orthop Surg Res. 2010;5(1):46.
Funding
There is no funding source for authors to declare.
Author information
Authors and Affiliations
Contributions
SHS introduced the concept, supervised and designed the study, and edited the final manuscript. YF supervised the study and edited the final manuscript. MS and MB collected the data, MS analyzed the data. PM and SB wrote the initial draft and edited the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Since this study is not involving human or animal subjects, our institutional review board waived ethical review and approval. A study protocol was approved by PROSPERO with the following code: CRD42022307385.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Soleimani, M., Babagoli, M., Baghdadi, S. et al. Return to work following primary total hip arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res 18, 95 (2023). https://doi.org/10.1186/s13018-023-03578-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03578-y