
Abstract
Background
Although some surgeons strongly advocate for one approach over the other, there are few data directly comparing the direct anterior approach with a miniposterior approach for total hip arthroplasty (THA).
Questions/purposes
Using the same advanced pain and rapid rehabilitation protocols for both groups, we compared the direct anterior and miniposterior approaches with respect to (1) return to activities of daily living at 2 days, 2 weeks, or 2 months; (2) risk of intraoperative or early postoperative complications; and (3) component position.
Methods
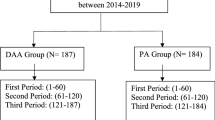
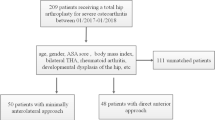
Over a 1-year period we identified all consecutive, primary direct anterior and miniposterior THAs performed by two surgeons at our institution, totaling 242 patients. Of those, 20 did not meet inclusion criteria as a result of prior trauma or surgery about the hip. A total of 222 patients, 126 direct anterior and 96 miniposterior, were retrospectively evaluated. All cases were done by one of two surgeons, one of whom performs THA exclusively through the direct anterior approach and the other who only uses the miniposterior approach. Groups did not differ demographically with mean ± SD age 64 ± 12 years, mean body mass index 30 ± 5.7 kg/m2, and 50% female. The same rapid rehabilitation protocols were used with no postoperative hip positioning precautions.
Results
No differences were seen between the two groups in mean length of stay (2.2 days; range, 1–9 days), operative or in-hospital complications, intravenous breakthrough analgesia, stairs, maximum feet walked in-hospital, or percent discharged to home (80% [177 of 222]; all p > 0.2). The direct anterior patients had longer mean operative times (114 minutes; range, 60–251 minutes) than the miniposterior patients (mean, 60 minutes; range, 41–113 minutes; p < 0.001). The direct anterior group had a higher maximum visual analog scale pain score (5.3 direct anterior; ± 2, versus 3.8 MP; ± 2; p < 0.0001). At 2 weeks, more direct anterior patients required gait aids (92% [116 of 126]) than miniposterior (68% [62 of 96]; p < 0.0001). At 8 weeks, direct anterior patients had higher mean Harris hip scores (95 versus 89) but a lower return to work and driving with no difference in their use of gait aids, narcotics, activities of daily living, or walking 0.5 mile. More wound problems occurred in the miniposterior group (p < 0.01). With the numbers available, component alignment was not different between the study groups (p > 0.05 for all comparisons).
Conclusions
There was no systematic advantage of direct anterior THA versus miniposterior THA. Contrary to conventional belief and somewhat surprising were the fewer minor wound problems in the direct anterior group and the higher proportion of patients free of gait aids at 2 weeks and back to driving and working at 8 weeks in the miniposterior group. Factors other than surgical approach, perhaps including attentive pain management, patient selection, surgical volume and experience, careful preoperative templating, and rapid rehabilitation protocols, may be more important in terms of influencing early recovery after THA.
Level of Evidence
Level III, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Similar content being viewed by others

References
Barrett WP, Turner SE, Leopold JP. Prospective randomized study of direct anterior vs postero-lateral approach for total hip arthroplasty. J Arthroplasty. 2013;28:1634–1638.
Berger RA. The technique of minimally invasive total hip arthroplasty using the two-incision approach. Instr Course Lect. 2004;53:149–155.
Berger RL, Celli BR, Meneghetti AL, Bagley PH, Wright CD, Ingenito EP, Gray A, Snider GL. Limitations of randomized clinical trials for evaluating emerging operations: the case of lung volume reduction surgery. Ann Thorac Surg. 2001;72:649–657.
Bertin KC, Rottinger H. Anterolateral mini-incision hip replacement surgery: a modified Watson-Jones approach. Clin Orthop Relat Res. 2004;429:248–255.
Browne JA, Pagnano MW. Surgical technique: a simple soft-tissue-only repair of the capsule and external rotators in posterior-approach THA. Clin Orthop Relat Res. 2012;470:511–515.
Chimento, GF, Pavone V, Sharrock N, Kahn B, Cahill J, Sculco TP. Minimally invasive total hip arthroplasty: a prospective randomized study. J Arthroplasty. 2005;20:139–144.
Dorr LD, Maheshwari AV, Long WT, Wan Z, Sirianni LE. Early pain relief and function after posterior minimally invasive and conventional total hip arthroplasty: a prospective, randomized, blinded study. J Bone Joint Surg Am. 2007;89:1153–1160.
Downing ND, Clark DI, Hutchinson JW, Colclough K, Howard PW. Hip abductor strength following total hip arthroplasty: a prospective comparison of the posterior and lateral approach in 100 patients. Acta Orthop Scand. 2001;72:215–220.
Gore DR, Murray MP, Sepic SB, Gardner GM. Anterolateral compared to posterior approach in total hip arthroplasty: differences in component positioning, hip strength, and hip motion. Clin Orthop Relat Res. 1982;165:180–187.
Howell JR, Masri BA, Duncan CP. Minimally invasive versus standard incision anterolateral hip replacement: a comparative study. Orthop Clin North Am. 2004;35:153–162.
Inaba Y, Wan Z, Sirianni L, Boutary M. Operative and patient care techniques for posterior mini incision total hip arthroplasty. Clin Orthop Relat Res. 2005;441:104–114.
Ito Y, Matsushita I, Watanabe H, Kimura T. Anatomic mapping of short external rotators shows the limit of their preservation during total hip arthroplasty. Clin Orthop Relat Res. 2012;470:1690–1695.
Jewett BA, Collis DK. High complication rate with anterior total hip arthroplasties on a fracture table. Clin Orthop Relat Res. 2011;469:503–507.
Krych AJ, Pagnano MW, Coleman Wood K, Meneghini RM, Kaufman K. No strength or gait benefit of two-incision THA: a brief followup at 1 year. Clin Orthop Relat Res. 2011;469:1110–1118.
Maheshwari AV, Blum YC, Shekhar L, Ranawat AS, Ranawat CS. Multimodal pain management after total hip and knee arthroplasty at the Ranawat Orthopaedic Center. Clin Orthop Relat Res. 2009;467:1418–1423.
Matta JM, Shahrdar C, Ferguson T. Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res. 2005;441:115–124.
Mayr E, Nogler M, Benedetti MG, Kessler O, Reinthaler A, Krismer M, Leardini A. A prospective randomized assessment of earlier functional recovery in THA patients treated by minimally invasive direct anterior approach: a gait analysis study. Clin Biomech (Bristol, Avon). 2009;24:812–818.
Meneghini RM, Pagnano MW, Trousdale RT, Hozack WJ. Muscle damage during MIS total hip arthroplasty: Smith-Peterson versus posterior approach. Clin Orthop Relat Res. 2006;453:293–298.
Meneghini RM, Smits SA. Early discharge and recovery with three minimally invasive total hip arthroplasty approaches: a preliminary study. Clin Orthop Relat Res. 2009;467:1431–1437.
Nakata K, Nishikawa M, Yamamoto K, Hirota S, Yoshikawa H. A clinical comparative study of the direct anterior with mini-posterior approach: two consecutive series. J Arthroplasty. 2009;24:698–704.
O’Brien DA, Rorabeck CH. The mini-incision direct lateral approach in primary total hip arthroplasty. Clin Orthop Relat Res. 2005;441:99–103.
Ogonda L, Wilson R, Archbold P, Lawlor M, Humphreys P, O’Brien S, Beverland D. A minimal-incision technique in total hip arthroplasty does not improve early postoperative outcomes: a prospective, randomized, controlled trial. J Bone Joint Surg Am. 2005;87:701–710.
Pagnano MW, Trousdale RT, Meneghini RM, Hanssen AD. Slower recovery after two-incision than mini-posterior-incision total hip arthroplasty: a randomized clinical trial. J Bone Joint Surg Am. 2008;90:1000–1006.
Restrepo C, Parvizi J, Pour AE, Hozack WJ. Prospective randomized study of two surgical approaches for total hip arthroplasty. J Arthroplasty. 2010;25:671–679.
Sculco TP. Minimally invasive total hip arthroplasty: in the affirmative. J Arthroplasty. 2004;19(Suppl 1):78–80.
Siguier T, Siguier M, Brumpt B. Mini-incision anterior approach does not increase dislocation rate: a study of 1037 total hip replacements. Clin Orthop Relat Res. 2004;426:164–173.
Spaans AJ, van den Hout JA, Bolder SB. High complication rate in the early experience of minimally invasive total hip arthroplasty by the direct anterior approach. Acta Orthop. 2012;83:342–346.
Tiberi JV, Pulos N, Kertzner M, Schmalzried TP. A more reliable method to assess acetabular component position. Clin Orthop Relat Res. 2012;470:471–476.
Vail TP, Callaghan JJ. Minimal incision total hip arthroplasty. J Am Acad Orthop Surg. 2007;15:707–715.
Watts CD, Pagnano MW. Minimising blood loss and transfusion in contemporary hip and knee arthroplasty. J Bone Joint Surg Br. 2012;94(Suppl A):8–10.
Woolson ST, Mow CS, Syquia JF, Lannin JV, Schurman DJ. Comparison of primary total hip replacements performed with a standard incision or a mini-incision. J Bone Joint Surg Am. 2004;86:1353–1358.
Wright JM, Crockett HC, Delgado S, Lyman S, Madsen M, Sculco TP. Mini-incision for total hip arthroplasty: a prospective, controlled investigation with 5-year follow-up evaluation. J Arthroplasty. 2004;19:538–545.
Wylde V, Maclean A, Blom AW. Post-operative radiographic factors and patient-reported outcome after total hip replacement. Hip Int. 2012;22:153–159.
Author information
Authors and Affiliations
Corresponding author
Additional information
The institution of the authors has received, during the study period, funding from DePuy Orthopaedics Inc (Warsaw, IN, USA), Stryker Orthopaedics (Mahwah, NJ, USA), Zimmer Inc (Warsaw, IN, USA), and Biomet Inc (Warsaw, IN, USA). One of the authors (MWP) certifies that he or she, or a member of his or her immediate family, has received or may receive payments or benefits, during the study period, an amount less than USD 10,000 from DePuy Orthopaedics Inc and an amount of less than USD 10,000 from Stryker Orthopaedics. One of the authors (MJT) certifies that he or she, or a member of his or her immediate family, has received or may receive payments or benefits, during the study period, an amount of less than USD 10,000 from MAKO Surgical Corp (Fort Lauderdale, FL, USA) and an amount of less than USD 10,000 from DJO, LLC (Vista, CA, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article

Cite this article
Poehling-Monaghan, K.L., Kamath, A.F., Taunton, M.J. et al. Direct Anterior versus Miniposterior THA With the Same Advanced Perioperative Protocols: Surprising Early Clinical Results. Clin Orthop Relat Res 473, 623–631 (2015). https://doi.org/10.1007/s11999-014-3827-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-3827-z