
Abstract
Background
Central lymph node metastasis of papillary thyroid microcarcinoma (PTMC) is common; however, prophylactic central lymph node dissection (CLND) is still controversial because of the possible increased morbidity. The purpose of this study is to determine the clinical outcome of patients with cN0 PTMC by central neck dissection.
Methods
A retrospective cohort study was conducted on patients with PTMC without preoperative evidence of lymph node disease (cN0), and the outcomes were compared between patients undergoing total thyroidectomy (TT) alone (group A) and patients undergoing TT with CLND (group B).
Results
In this study, 242 patients with cN0 PTMC were included. Group A had 108 patients and group B had 134 patients. During a follow-up of over 60 months, the long-term postoperative complications were equivalent between the two groups. In group B, the presence of involved central neck lymph nodes upstaged 16% of patients to stage III disease, which necessitated additional postoperative radioactive iodine treatment. More patients had recurrences in group A. The rate of reoperation in the central compartment was higher in group A than in group B (8.3% vs 2.2%, P < 0.01).
Conclusions
Prophylactic CLND does not increase long-term postoperative complications and reduces the risk of recurrence in the central compartment.
Similar content being viewed by others


Background
Despite the majority of papillary thyroid microcarcinoma (PTMC) patients having benign clinical courses, metastases to the lymph nodes are common. A report from Mayo Clinic showed that one third of 900 PTMC patients had metastases at the time of diagnosis [1]. The central neck compartment is the most common site of metastases. Consequently, some surgeons recommend routine prophylactic removal of the central neck lymph nodes at the time of the initial operation [2,3]. However, this was countered with some studies showing no benefit [4,5]. The purpose of this study is to evaluate the influence of prophylactic central lymph node dissection (CLND) on the oncological and functional outcomes of patients with PTMC.
Methods
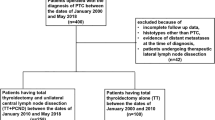
This retrospective cohort study was performed of a single institutional database of patients with histologically proven PTMC (<1 cm) at Peking Union Medical College Hospital from January 2008 to December 2009. Patients who underwent total thyroidectomy (TT) alone were designated as group A, whereas those who underwent TT with prophylactic CLND were designated as group B. Some surgeons in our institution performed routine CLND, and these surgeons contributed patients to group B. Those who did not perform CLND routinely contributed patients to group A. Patients with bilateral PTMC underwent bilateral prophylactic CLND, while patients with unilateral PTMC underwent ipsilateral CLND. CLND is defined as the removal of all level VI and VII nodes [6]. Patients with common papillary thyroid carcinoma (PTC) of >1 cm, evident preoperative abnormal lymph nodes, distant metastasis, or previous operation for PTC were excluded. Patients who underwent other operations such as lobectomy or subtotal thyroidectomy were also excluded in order to keep homogeneity in the management of patients and to avoid interference on cancer recurrence. Of the 709 patients treated surgically for PTC from January 2008 to December 2009, 242 patients satisfied the inclusion criteria. Of these, 108 patients underwent TT alone and 134 patients underwent TT and CLND. Consent statements were required from all patients.
We routinely removed badly blood-supported parathyroid during operation and cut it into 1-mm pieces to implant in the sternocleidomastoid muscle. Patients were monitored postoperatively with serum calcium determination. Temporary hypocalcemia was defined as serum calcium <8 mg/dl anytime during the initial 6-month follow-up. Permanent hypoparathyroidism was defined as a need for continued calcium beyond 6 months after surgery with persistent serum calcium <8 mg/dl. Transient recurrent laryngeal nerve (RLN) palsy was confirmed by fiber optic laryngoscopy between 0 and 6 months after operation, and permanent RLN palsy was confirmed by fiber optic laryngoscopy beyond 6 months after operation. Recurrence was defined as local or regional disease requiring reoperation or other repeat treatment, as detected by serial cervical ultrasonographies or radioactive thyroid scan [6].
Patients underwent radioactive iodine ablative therapy with iodine131 (I131) 3 to 4 weeks after operation. The indications for I131 ablation were determined by the nuclear medicine specialists based on the American Joint Committee on Cancer (AJCC) stage of disease [7]. All patients entered a scheduled clinical follow-up program on an average duration of over 60 months. Follow-up of patients involved annual examination of neck ultrasonography, I131 scintigraphy, computed tomography, and so on.
Statistical analysis was performed using SPSS13.0 software. Data were compared for statistical analysis using the chi-square test to evaluate differences between qualitative variables and using Student’s t test to compare quantitative variables. P < 0.05 was considered significant.
Results
Patient characteristics are summarized and operative results were analyzed between group A and group B based on operative and surgical pathology reports in Table 1. There were no significant differences in the age, gender distribution, and tumor pathologic characteristics. In group B, ipsilateral CLND was performed in 112 (84%) patients and 31 (16%) had bilateral CLND. The number of patients found to have involved central neck lymph nodes on final pathology was 51 of 134 (38%) in group B. The median number of lymph nodes excised was 0 in group A and 6 in group B (P < 0.01). The median number of positive lymph nodes was 0 in group A and 1 in group B (P < 0.01). A total of 22 (16%) patients over 45 years old were upstaged from stage I to stage III disease because of positive lymph node status according to the AJCC staging system for differential thyroid cancer.
The incidence of operative complications is summarized in Table 2. The incidence of postoperative infection and hematoma was similar between the groups. There were a significantly greater number of parathyroid auto-transplantations due to devascularization and a higher rate of temporary postoperative hypocalcemia in group B. Permanent hypoparathyroidism was equivalent between the groups. There was no difference in the incidence of temporary and permanent RLN injury between group A and group B. We did not list the complications of CLND in the reintervention because the number was too small to make a statistical analysis and compare it with that of the initial operation. There were 12 recurrences in both groups, and 8 of them had re-CLND, 2 of whom had nerve injury and 3 developed permanent hypocalcemia, which was much higher than that of the initial operation.
During the final follow-up, no one died in this study. A Kaplan-Meier survival analysis for central compartment reoperation was undertaken. Group B, which had prophylactic CLND, had a significantly lower failure rate (P < 0.05) compared with group A, which did not have CLND (shown in Figure 1). There was no recurrence in the thyroid bed. All 12 recurrences occurred in regional lymph nodes, 4 of whom had both central and lateral section lymph node recurrences. Recurrent disease occurred in 9 of 108 (8.3%) in group A and 3 of 134 (2.2%) in group B (P < 0.01). In 8 central compartment lymph node (levels VI and VII) recurrences, 7 (6.5%) was in group A and 1 (0.7%) was in group B (P < 0.01). In 8 lateral section lymph node (levels IV, III, and II) recurrences, 5 (4.6%) was in group A and 3 (2.2%) was in group B (NS). Eight of 12 recurrences had re-CLND (levels VI and VII), 4 of whom had both central (levels VI and VII) and lateral (levels IV, III, and II) section reoperation. The median time to reoperation in group B was longer than that in group A (27 vs 18 months, P < 0.05). The rate of reoperation in the central compartment was significantly higher in group A than in group B (6.5% vs 0.7%, P < 0.01). Although the rate of reoperation in the lateral section in group B (2.2%) was lower than that in group A (4.6%), there was no statistical significance. Data summarizing reoperation rates and regions of lymph nodes removed at secondary surgery are shown in Table 3.

Central compartment recurrence-free survival.
Discussion
The incidence of PTMC has been increasing within the recent 5 years with the extensive use of thyroid ultrasonography in routine physical examination [8]. Although it has been accepted that patients with PTMC have a good prognosis [9], cervical lymph node metastases are common, with an incidence between 30% and 60% [1,10]. Furthermore, more and more researches reported that regional lymph node metastasis was associated with increased local recurrence rates and reduced survival [11,12]. Therefore, there is renewed interest in the operative management of cervical lymph node metastases, but controversies remain. Most surgeons agree that grossly involved lymph nodes in the central neck of patients with PTMC should be managed by selective neck dissection. The debate focuses on whether the use of prophylactic CLND at the initial thyroid operation benefits PTMC patients. This retrospective cohort study examined the impact of routine CLND in addition to TT in the management of cN0 PTMC and suggests a decreased recurrence rate and a reduction in the need for reoperation in the central compartment without increasing long-term postoperative complications.
Prophylactic CLND is defined as the removal of all level VI and VII nodes when there is no evidence of lymph node metastasis on preoperative clinical examination, imaging studies, or intra-operative visual inspection [6]. It has been reported that most of central lymph node metastases are too small to be detected by sonography [13,14]. We observed that approximately 40% of the patients who underwent central neck dissection had lymph node involvement despite negative preoperative physical examination and ultrasonography in our study. The presence of lymph node metastases upgraded 16% of the patients above 45 years old with PTMC from stage I to stage III for central neck dissection, which provided improved staging accuracy rather than for the removal of subclinical disease. It is important to note that accurate staging is not only helpful for predicting the prognosis but also crucial for determining which patients would need radioiodine treatment because for PTMC patients without lymph node metastases, radioiodine therapy is not necessary.
Another advantage of prophylactic central lymph node dissection is that it provides a clear surgical field for central compartment lymph node dissection in the initial operation. In contrast, reoperation after the development of recurrence is a much more difficult and technically challenging procedure, associated with an increased morbidity.
Higher rates of complications such as temporary hypocalcemia, permanent hypoparathyroidism, and RLN palsy are often cited in arguments against prophylactic CLND in the treatment of PTMC [15,16]. Temporary hypoparathyroidism has been reported to be between 20% and 50% [17-19]. Our comparison of the two groups confirms previous reports of increased temporary hypocalcemia with CLND, which was caused by transient parathyroid dysfunction due to devascularization and could be corrected by calcium supplementation. The rate of permanent hypoparathyroidism had no difference between the two groups because of our routine use of intra-operative parathyroid auto-transplantation. The rates of temporary and permanent RLN injury did not increase with prophylactic CLND.
Despite high rates of temporary hypocalcemia, the patients in our study did get benefits from CLND. The removal of subclinical metastases improved the recurrence rate and avoided reoperation in the central compartment, which may be associated with increased risks. As expected, the rate of disease recurrence in group B is lower than that in group A (2.2% vs 8.3%, P < 0.01). Most of these recurrences were in the first 3 years after the initial operation. The median time of reoperation in group B was also longer than that in group A (27 vs 18 months, P < 0.05). There was also a reduction in the need for further surgery in the central compartment in patients who had prophylactic CLND in comparison with those who did not have (6.5% vs 0.7%, P < 0.01). Although the rate of reoperation in the lateral neck in group B is also lower than that in group A, there is no statistically significant difference. Shen et al. have shown a similar trend toward decreased recurrence in patients undergoing prophylactic CLND [20].
The limitations of this study include its nonrandomized, retrospective design, leaving the results vulnerable to selection biases. The strengths are its large population and long-time follow-up.
Conclusions
In conclusion, this study evaluates the impact of prophylactic CLND in addition to TT in the management of patients with PTMC and shows that prophylactic CLND for cN0 PTMC can be performed at the time of the initial operation without apparent increase in long-term morbidity. Prophylactic CLND should be considered because it not only allows for more accurate staging by the determination of lymph node status but also results in lower recurrence rates of PTMC and a reduction in the need for reoperation.
References
Hay ID, Hutchinason ME, Gonzalez-Losada T, McIver B, Reinalda ME, Grant CS, et al. Papillary thyroid microcarcinoma: a study of 900 cases observed in a 60-year period. Surgery. 2008;144(6):980–7.
Mazzaferri EL, Doherty GM, Steward DL. The pros and cons of prophylactic central compartment lymph node dissection for papillary thyroid carcinoma. Thyroid. 2009;19:683–9.
Son YI, Jeong HS, Baek CH, Chung MK, Ryu J, Chung JH, et al. Extent of prophylactic lymph node dissection in the central neck area of the patients with papillary thyroid carcinoma: comparison of limited versus comprehensive lymph node dissection in a 2-year safety study. Ann Surg Oncol. 2008;15(7):2020–6.
Shah MD, Hall FT, Eski SJ, Witterick IJ, Walfish PG, Freeman JL. Clinical course of thyroid carcinoma after neck dissection. Laryngoscope. 2003;113:2102–7.
Steinmuller T, Klupp J, Rayes N, Ulrich F, Jonas S, Graf KJ, et al. Prognostic factors in patients with differentiated thyroid carcinoma. Eur J Surg. 2000;166:29–337.
Ferlito A, Robbins KT, Shah JP, Medina JE, Silver CE, Al-Tamimi S, et al. Proposal for a rational classification of neck dissections. Head Neck. 2011;33:445–50.
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17:1471.
Mazzaferri EL, Sipos J. Should all patients with subcentimeter thyroid nodules undergo fine-needle aspiration biopsy and preoperative neck ultrasonography to define the extent of tumor invasion? Thyroid. 2008;18:597–602.
Lundgren CI, Hall P, Dickman PW, Zedenius J, Lundgren CI, Hall P, et al. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case–control study. Cancer. 2006;106:524–31.
He Q, Zhuang D, Zheng L, Fan Z, Zhou P, Lv Z, et al. The surgical management of papillary thyroid microcarcinoma: a 162-month single-center experience of 273 cases. Am Surg. 2012;78(11):1215–8.
White ML, Gauger PG, Doherty GM, Doherty GM. Central lymph node dissection in differentiated thyroid cancer. World J Surg. 2007;31(5):895–904.
Hughes DT, White ML, Miller BS, Gauger PG, Burney RE, Doherty GM. Influence of prophylactic central lymph node dissection on postoperative thyroglobulin levels and radioiodine treatment in papillary thyroid cancer. Surgery. 2010;148:1100–6.
Choi YJ, Yun JS, Kook SH, Jung EC, Park YL. Clinical and imaging assessment of cervical lymph node metastasis in papillary thyroid carcinomas. World J Surg. 2010;34:1494–9.
Vergez S, Sarini J, Percodani J, Serrano E, Caron P. Lymph node management in clinically node-negative patients with papillary thyroid carcinoma. Eur J Surg Oncol. 2010;36:777–82.
Rosenbaum MA, McHenry CR. Central neck dissection for papillary thyroid cancer. Arch Otolaryngology Head Neck Surg. 2009;135:1092–7.
Roh JL, Park JY, Park CY. Total thyroidectomy plus neck dissection in differentiated papillary thyroid carcinoma patients: pattern of nodal metastases, morbidity, recurrence and postoperative levels of serum parathyroid hormone. Ann Surg. 2007;245:604–10.
Moo TA, McGill J, Allendorf J, Lee J, Fahey III T, Zarnegar R. Impact of prophylactic central neck lymph node dissection on early recurrence in papillary thyroid carcinoma. World J Surg. 2010;34:1187–91.
Moo TA, Umunna B, Kato M, Butriago D, Kundel A, Lee JA, et al. Ipsilateral versus bilateral central neck lymph node dissection in papillary thyroid carcinoma. Ann Surg. 2009;250:403–8.
Lee YS, Kim SW, Kim SK, Kang HS, Lee ES, Chung KW, et al. Extent of routine central lymph node dissection with small papillary thyroid carcinoma. World J Surg. 2007;31:1954–9.
Shen WT, Ogawa L, Ruan D, Suh I, Duh QY, Clark OH. Central neck lymph node dissection for papillary thyroid cancer: the reliability of surgeon judgement in predicting which patients will benefit. Surgery. 2010;148:398–403.
Acknowledgements
The authors would like to acknowledge Dr. Jianchun Yu and Dr. Xiaoyi Li, who contributed their patients for the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Dr. LZ participated in the design of the study and drafted the manuscript. Dr. ZL participated in the collection of data and coordination. Dr. YL performed the statistical analysis. Dr. WG participated in its design. Dr. CZ contributed most patients. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Zhang, L., Liu, Z., Liu, Y. et al. The clinical prognosis of patients with cN0 papillary thyroid microcarcinoma by central neck dissection. World J Surg Onc 13, 138 (2015). https://doi.org/10.1186/s12957-015-0553-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-015-0553-2