
Abstract
Backgrounds
Stroke is a sudden disorder of cerebral blood circulation. Many studies have illustrated that dyslipidemia, hypertension, diabetes, smoking and excessive drinking are the traditional risk factors for stroke. This study aimed to observe the relationship between CYP1A1 and CYP1A2 variants and stroke risk in the Chinese population.
Methods
Agena MassARRAY Assay was used to genotype four single nucleotide polymorphisms (SNPs) in 477 cases and 480 controls. The chi-square test and logistic-regression analysis were used to explore the relationship between CYP1A1 and CYP1A2 variants and stroke risk.
Results
Individuals with CYP1A2 rs762551 C was associated with a lower risk of stroke than that of allele A. Age stratification analysis showed that rs762551 was only observed to be associated with a lower risk of stroke in ≤64ys age group. After gender stratification analysis, a significant association between rs762551 and stroke risk was found in males, but not in females. The four SNPs were found to be correlated with stroke risk in patients with hypertension, coronary heart disease, cerebral infarction and lacunar infarction.
Conclusion
In this study, the results first showed that CYP1A1 and CYP1A2 variants were associated with stroke risk. Larger and well-designed studies are needed to confirm the results.
Similar content being viewed by others


Background
Generally speaking, stroke is a sudden disorder of cerebral blood circulation in the brain that occurs when blood clot blocks arteries transmitting blood from heart to brain [1]. At present, it ranks as the second leading cause of death in the world and the main cause of adult disability and death in most developing and developed countries [2]. According to the World Health Organization report in 2019, 5.5 million people died of stroke [3]. In China, there are over 2 million stroke patients and 6–7 million stroke survivors every year [4]. About 80% of stroke patients are ischemic [5, 6]. Many studies illustrated that dyslipidemia, hypertension, diabetes, smoking and excessive drinking are the traditional risk factors for stroke [7]. Moreover, genetic factors are also involved in stroke risk assessment.
Cytochrome P450s (CYPs) is a widely distributed oxyhemoglobin superfamily, whose main function is to activate the molecular oxygen of lipophilic organic compounds, including drugs, steroids, fatty acids, bioamines, prostaglandins, plant metabolites, estradiol, estrone, etc. [8]. Some of these compounds are carcinogens, but most of them are activated by phase I enzymes encoded by the CYP superfamily and transformed into active carcinogens [9]. The active carcinogen combine with DNA to form DNA adducts causing mutation and carcinogenesis. Epidemiological and basic scientific research have shown that CYP4F2, CYP4A11 and other candidate genes played key roles in the pathogenesis of ischemic stroke [3, 10, 11]. CYP1A1 and CYP1A2 are the members of the CYP family participating in the metabolism of exogenous drugs, endogenous substrates, etc. Researchers [12, 13] reported that CYP1A1 and CYP1A2 played important roles in the bioactivation of polyunsaturated fatty acids, which can use NADPH to reduce the amount of O2, producing H2O2 and superoxide anion radicals [14]. Furthermore, induction of CYP1A1 can enhance oxidative stress response and increase the physiological production of ROS in skin [15, 16]. The above studies illustrated that CYP1A1 can induce oxidative stress induced by ROS overproduction. However, the exact mechanism of CYP1A1 and CYP1A2 in stroke remains unclear.
In this study, we used to explore the relationship between CYP1A1 and CYP1A2 genetic variants and the incidence of stroke in the Chinese population by the chi-square test and logistic-regression analysis, to provide theoretical basis for the function of CYP1A1 and CYP1A2 in stroke, and to provide more evidence for elucidating the cause of stroke.
Methods
Study design
Four hundred seventy-seven case samples and four hundred and eighty control samples were randomly collected from Traditional Chinese medicine of Baoji Hospital. All subjects were Shaanxi people of China. According to the World Health Organization’s diagnostic criteria for stroke, all cases were confirmed by professionals using computed tomography and/or magnetic resonance imaging. Cases with a history of cancer, inflammatory disease or other chronic diseases were excluded from this study. Every member of the control group had a rigorous physical examination to ensure that they were healthy without inflammatory disease and chronic diseases. Some additional information on the patients was also collected, including their history with hypertension, coronary heart disease, cerebral infarction and lumen infarction. Written informed consent was obtained from all subjects. The study period is from 2018 to 03 to 2019–12. Also, the study was approved by the Institutional Review Board of the Traditional Chinese medicine of Baoji Hospital (201802).
SNP selection, genotyping and data collection
Totally, 4 variants (rs1048943, rs4646422, rs762551 and rs2470890) were selected in the global population on the basis of the 1000 Genomes Project (https://www.internationalgenome.org/) [17]. The minor allele frequency of every SNP was greater than 5%. Primers design for amplification and extension of SNPs listed in Supplementary Table 1 were completed by the Agena Bioscience Assay Design Suite V2.0 software (https://agenacx.com/online-tools/). Genomic DNA was extracted from the participants’ blood samples using the GoldMag-Mini Whole Blood Genomic DNA Purification Kit (GoldMag. Co. Ltd., Xi’an, China) regarded as the amplification template. Target amplification of SNPs was performed according to a predetermined PCR procedure, and PCR product purification was completed by agarose gel electrophoresis. After that, SNP genotyping was performed by the Agena MassARRAY platform with iPLEX gold chemistry (Agena Bioscience, San Diego, CA, USA), and data management was completed by Agena Bioscience TYPER, Version 4.0 [18].

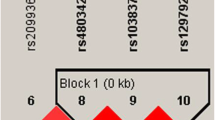
Linkage disequilibrium (LD) analysis of five SNPs in CYP1A1, and CYP1A2. The LD value is determined by r2 > 0.8 analyzed by Haploview software, version 4.2
Statistical analysis
Based on the SPSS and Excel software, the allele frequencies for each SNP were calculated. Pearson’s chi-square test was used to assess whether the genotype distribution of variants among controls were in accordance with Hardy-Weinberg equilibrium. T-test and chi-square test were utilized to estimate the differences of age and gender distribution between cases and controls, respectively. Logistic regression analysis presented by the PLINK software, version 1.07 (Harvard, Boston, MA, USA) was used to estimate the association between CYP1A1 and CYP1A2 variants and stroke risk. Linkage disequilibrium (LD) using the Haploview software, version 4.2 (Harvard, Boston, MA, USA) was detected among the SNPs of CYP1A1 and CYP1A2 with HWE (P > 0.001). All P-values were two-tailed and P<0.05 were considered significant. Regardless of the level of significance found, all of the comparisons made will be considered exploratory in nature.
Results
Basic information of participants
In this study, 316 out of 477 cases were males and 161 were females, while the number of men and women among the 480 controls was 313 and 167, respectively. Background information on the participants was listed in Table 1. The mean age of cases and controls were 64.13 ± 10.82 years old and 63.69 ± 6.69 years old, respectively, indicating that there was no significant difference in age between cases and controls. Genotype frequency of each SNP in the controls was in accordance with HWE (P > 0.05) (Supplementary Table 2).
Overall analysis of the association between CYP1A1 and CYP1A2 variants and stroke risk
As shown in Table 2, allele C of CYP1A2 rs762551 was associated with a lower risk of stroke than allele A (OR = 0.82, 95% CI: 0.68–0.99, P = 0.034). Overall analysis showed a link between the SNP and stroke risk (Table 2). Without adjustment, rs762551 was related to stroke risk in the codominant (P = 0.010), recessive (P = 0.005) and log-additive (P = 0.032) models (no shown). After adjusted for gender and age, the codominant model showed that AA carriers had a 0.60-times lower risk of stroke than CC carriers (OR = 0.60, 95% CI: 0.40–0.88, P = 0.010). The recessive model indicated that individuals with AA genotype had a lower risk of stroke compared to the C/C-A/C genotype carriers (OR = 0.60, 95% CI: 0.42–0.86, P = 0.005). The log-additive model also demonstrated that the SNP was in connection with a decreased risk of stroke (OR = 0.81, 95% CI: 0.68–0.98, P = 0.031).
Stratification analysis by age and gender
To further investigate the correlation between variants of CYP1A1, CYP1A2 and stroke risk, stratification analysis was also completed (Table 3). After age stratified by average age, the correlation between CYP1A2 rs762551 and stroke risk was analyzed. The SNP was only found to be linked with a reduced risk of stroke in ≤64ys age group (OR = 0.56, 95% CI: 0.33–0.92, P = 0.024) in the recessive model, but, the association was not significant in >64ys age group. After gender stratification, there was a significant association between rs762551 and stroke risk in males, but not in females. The codominant model showed that rs762551 AA genotype decreased stroke risk by 0.56-fold (P = 0.017). However, no significant differences were found in other models.
Analysis of the association between CYP1A1, CYP1A2 variants and stroke risk in patients with hypertension and coronary heart disease
The association between variants of CYP1A1, CYP1A2 and stroke susceptibility was evaluated in patients with hypertension and coronary heart disease shown in Table 4. By comparing with non-hypertensive cases, the correlation between CYP1A1 rs4646422, CYP1A2 (rs762551 and rs2470890) and stroke risk in hypertensive cases was first analyzed in the allele model (Table 4). Allele C of rs2470890 conferred an increased susceptibility to stroke compared to the allele T (adjusted OR = 1.68, 95% CI: 1.05–2.69, P = 0.030). In the codominant model, compared with the carriers of TT genotype, subjects with TC genotype of CYP1A1 rs4646422 had a negative effect on the risk of stroke (adjusted OR = 1.69, 95% CI: 1.04–2.74, P = 0.035). However, in the recessive model, CC genotype played a protective effect on the risk of stroke (adjusted OR = 0.28, 95% CI: 0.09–0.89, P = 0.032) compared to the T/T-T/C genotype. Additionally, there was a link between CYP1A2 rs762551 and stroke susceptibility in the codominant (adjusted OR = 1.65, 95% CI: 1.08–2.54, P = 0.022) and dominant (adjusted OR = 1.57, 95% CI: 1.04–2.36, P = 0.030) models. Moreover, CYP1A2 rs2470890 was associated with stroke risk in the codominant (adjusted OR = 1.91, 95% CI: 1.11–3.27, P = 0.019), dominant (adjusted OR = 1.85, 95% CI: 1.10–3.10, P = 0.021) and log-additive (adjusted OR = 1.67, 95% CI: 1.04–2.70, P = 0.035) models.
In patients with coronary heart disease (Table 4), individuals with rs4646422 C allele were found to be increased the likelihood of stroke by 1.54 times when compared with the T allele (P = 0.030). In addition, the variant was related to an increased risk of stroke (codominant: adjusted OR = 1.79, 95% CI: 1.11–2.90, P = 0.017; dominant: adjusted OR = 1.75, 95% CI: 1.10–2.78, P = 0.019; log-additive: adjusted OR = 1.54, 95% CI: 1.03–2.30, P = 0.036). Rs2470890 was correlated with a decreased risk of stroke in the recessive model (adjusted OR = 0.56, 95% CI: 0.31–0.99, P = 0.047).
Analysis of the association between CYP1A1, CYP1A2 variants and stroke risk in patients with cerebral infarction and lacunar infarction
In addition, we analyzed the association between CYP1A1 rs1048943 and stroke risk in cerebral infarction cases vs non-cerebral infarction cases (Supplementary Table 3). The recessive model showed that subjects with genotype TT were more likely to suffer from stroke than those with C/C-C/T genotypes before adjustment (OR = 4.48, 95% CI: 1.05–19.15, P = 0.043). Moreover, the relationship between CYP1A1 rs1048943 and stroke risk was analyzed in lacunar infarction cases vs non-lacunar infarction cases adjusted for age and gender (Supplementary Table 4). The variant was related to a decreased risk of stroke in the codominant (OR = 0.13, 95% CI: 0.02–0.96, P = 0.045) and recessive (OR = 0.13, 95% CI: 0.02–0.95, P = 0.045) models.
LD and haplotype analysis
Among the four SNPs (rs1048943, rs4646422, rs762551 and rs2470890), LD analysis was performed. A strong linkage between the SNPs was observed (Fig. 1). Table 5 listed all of the possible haplotypes of the rs762551 and rs2470890. In the overall analysis results, the frequencies of the most dominant haplotype AT was 0.876 and 0.882 in cases and controls, respectively. The CC haplotype was the disadvantaged haplotype with frequencies of 0.380 and 0.427 in cases and controls, respectively. Besides, CC haplotype was still correlated with a reduced risk of stroke (OR = 0.82, 95% CI: 0.68–0.99, P = 0.035; adjusted OR = 0.82, 95% CI: 0.68–0.99, P = 0.034). In addition, clinical characteristics analysis in patients with hypertension indicated that AT haplotype was associated with a decreased susceptibility of stroke (OR = 0.60, 95% CI: 0.37–0.96, P = 0.032; adjusted OR = 0.60, 95% CI: 0.37–0.96, P = 0.033). AC haplotype was associated with an increased susceptibility of stroke (OR = 1.56, 95% CI: 1.16–2.10, P = 0.003; adjusted OR = 1.57, 95% CI: 1.16–2.11, P = 0.003).
Discussion
This study investigated the association between CYP1A1 variants and CYP1A2 and stroke risk in the Chinese Han population. Except for rs1048943, this is the first study to show that rs4646422, rs762551 and rs2470890 were associated with stroke risk. The four SNPs were found to be correlated with stroke risk in patients with hypertension, coronary heart disease, cerebral infarction and lacunar infarction.
Recently, researches have also shown that CYP1A1 variants played a role in the development of ischemic stroke (IS) susceptibility in different populations, such as Turk [19], Indian [20] and Chinese [21]. Demirdöğen et al. [19] reported that rs1048943 and rs4646903 may play a significant role in smoking- and hypertension-induced IS risk in the Turkish population. Among the 6235C carriers or 4889G carriers, the prevalence of hypertension and IS risk associated with hypertension were lower than that of wild type carriers. Sultana et al. [20] observed that South Indian population with CYP1A1 rs4646903 CC genotype was related to an increased risk of IS, up to 5.14 times, while the other genotypes had no influence on the IS risk. Additionally, Zhang et al. [21] revealed that rs4646903 and rs1048943 of CYP1A1 were related to IS risk in eastern China. This illustrated that individuals with TC-CC genotype of rs4646903 and AG-GG genotype of rs1048943 had a lower IS risk compared to rs4646903 TT and rs1048943 AA, respectively. Whereas, rs4646922 was not found to be associated with IS risk. In this study, rs4646922 was associated with stroke risk in the Shaanxi population of China. Given the inconsistency in the above results, ethnic differences and population distribution may be an important reason.
Moreover, Mega et al. analyzed the effect of Prasugrel on CYP gene polymorphisms and found non-significant relationship between CYP1A2 SNPs and stroke risk [4]. Until now, the correlation between CYP1A2 variants and stroke risk has not been reported. In this study, the results first illustrated that rs4646422, rs762551 and rs2470890 were found to be related to stroke risk in Shaanxi population of China. In future, it needs to be tested in a larger sample to provide evidence for stroke risk prediction.
Study strengths and limitations
The study has several strengths. Firstly, the strength is the genotype distribution of variants among controls in accordance with HWE P-value, which may reduce bias to some extent. Secondly, although the number of cases and controls was not enough, it was enough for statistical analysis, and the results were adjusted by age and gender to eliminate data defects.
Moreover, this study has several limitations. First, insufficient sample size may affect the research conclusion. Then the larger sample size is needed to verify the results. Second, the sample is limited to one race, which may lead to some uncertainty in the results of the study. Later, data from different ethnic groups is needed to verify the results. Third, the study is not thorough due to a lack of information on smoking, drinking and body mass index. Finally, the results only showed that polymorphisms of CYP1A1 and CYP1A2 were related to the risk of stroke, and there was no more clear mechanism study. RegulomeDB (https://www.regulomedb.org/regulome-search/) and HaploReg v4.1 (https://pubs.broadinstitute.org/mammals/haploreg/haploreg.php) are used to predict the effect of CYP1A1 and CYP1A2 polymorphisms on their function (Supplementary Table 5). Then, molecular experiment is used to further verify the role of CYP1A1 and CYP1A2 polymorphisms in the course of stroke.
Conclusions
This was the first time that rs4646422, rs762551 and rs2470890 were observed to be related to stroke risk in the Chinese population, which is helpful for obtaining a more conclusive understanding of the function of CYP1A1 and CYP1A2 and for laying a foundation for further elucidating the pathogenesis of stroke.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Abbreviations
- SNPs:
-
Single nucleotide polymorphisms
- OR:
-
Odds ratio
- 95% CI:
-
95% confidence interval
- CYP1A:
-
Cytochrome P450, family 1, subfamily A, polypeptide 1
- LD:
-
Linkage disequilibrium
- HWE:
-
Hardy-Weinberg Equilibrium
- MAF:
-
Minor allele frequency
- IS:
-
Ischemic stroke
References
Hankey GJ. Stroke. Lancet. 2017;389:641–54.
Bonita R, Mendis S, Truelsen T, Bogousslavsky J, Toole J, Yatsu F. The global stroke initiative. Lancet Neurol. 2004;3:391–3.
Lindsay MP, Norrving B, Sacco RL, Brainin M, Hacke W, Martins S, Pandian J, Feigin V. World stroke organization (WSO): global stroke fact sheet 2019. Int J Stroke. 2019;14:806–17.
Liu M, Wu B, Wang WZ, Lee LM, Zhang SH, Kong LZ. Stroke in China: epidemiology, prevention, and management strategies. Lancet Neurol. 2007;6:456–64.
Goldstein LB, Adams R, Becker K, Furberg CD, Gorelick PB, Hademenos G, Hill M, Howard G, Howard VJ, Jacobs B. Primary prevention of ischemic stroke: a statement for healthcare professionals from the stroke Council of the American Heart Association. Circulation. 2001;103:163–82.
Warlow CP. Epidemiology of stroke. Lancet. 1998;352(Suppl 3):Siii1–4.
Guo JM, Liu AJ, Su DF. Genetics of stroke. Acta Pharmacol Sin. 2010;31:1055–64.
Yao JT, Zhao SH, Liu QP, Lv MQ, Zhou DX, Liao ZJ, Nan KJ. Over-expression of CircRNA_100876 in non-small cell lung cancer and its prognostic value. Pathol Res Pract. 2017;213:453–6.
Chen D, Ma W, Ke Z, Xie F. CircRNA hsa_circ_100395 regulates miR-1228/TCF21 pathway to inhibit lung cancer progression. Cell Cycle. 2018;17:2080–90.
Yi X, Liao D, Wang C, Cheng W, Fu X, Zhang B. Cytochrome P450 genetic variants and their metabolite levels associated with plaque stability in patients with ischemic stroke. J Atheroscler Thromb. 2016;23:330–8.
Munshi A, Sharma V, Kaul S, Al-Hazzani A, Alshatwi AA, Shafi G, Koppula R, Mallemoggala SB, Jyothy A. Association of 1347 G/a cytochrome P450 4F2 (CYP4F2) gene variant with hypertension and stroke. Mol Biol Rep. 2012;39:1677–82.
Maude F, Laurent C, Yvonne D, Emmanuelle PG, Jean-Pierre S, François B, Yolande A. Cytochromes P450 from family 4 are the main omega hydroxylating enzymes in humans: CYP4F3B is the prominent player in PUFA metabolism. J Lipid Res. 2008;49:2379–89.
Kravchenko LV, Tutel'yan VA, Trusov NV, Guseva GV, Aksenov IV. Effect of polyunsaturated fatty acids omega-3 on the induction of activity and expression of CYP1A1 and CYP1A2 genes in the liver of rats under the influence of indole-3-carbinol. Bull Exp Biol Med. 2014;156:327–31.
Luecke S, Wincent E, Backlund M, Rannug U, Rannug A. Cytochrome P450 1A1 gene regulation by UVB involves crosstalk between the aryl hydrocarbon receptor and nuclear factor kappaB. Chem Biol Interact. 2010;184:466–73.
Melchini A, Catania S, Stancanelli R, Tommasini S, Costa C. Interaction of a functionalized complex of the flavonoid hesperetin with the AhR pathway and CYP1A1 expression: involvement in its protective effects against benzo [a]pyrene-induced oxidative stress in human skin. Cell Biol Toxicol. 2011;27:371–9.
Furue M, Uchi H, Mitoma C, Hashimoto-Hachiya A, Chiba T, Ito T, Nakahara T, Tsuji G. Antioxidants for healthy skin: the emerging role of aryl hydrocarbon receptors and nuclear factor-Erythroid 2-related Factor-2. Nutrients. 2017;9:223.
Zhou F, He X, Liu H, Zhu Y, Jin T, Chen C, Qu F, Li Y, Bao G, Chen Z, Xing J. Functional polymorphisms of circadian positive feedback regulation genes and clinical outcome of Chinese patients with resected colorectal cancer. Cancer. 2012;118:937–46.
Hu QY, Jin TB, Wang L, Zhang L, Geng T, Liang G, Kang LL. Genetic variation in the TP63 gene is associated with lung cancer risk in the Han population. Tumour Biol. 2014;35:1863–6.
Demirdöğen BC, Adali A, Bek S, Demirkaya Ş, Adali O. Cytochrome P4501A1 genotypes and smoking-and hypertension-related ischemic stroke risk. Hum Exp Toxicol. 2013;32:483–91.
Sultana S, Kolla VK, Peddireddy V, Jeedigunta Y, Penagaluru PK, Joshi S, Penagaluru UR, Penagaluru PR. Association of CYP1A1 gene polymorphism with ischemic stroke in south Indian population. Transl Stroke Res. 2011;2:26–32.
Zhang M, Wu JM, Zhang QS, Yan DW, Ren LJ, Li WP. The association of CYP1A1 genetic polymorphisms and additional gene–gene interaction with ischemic stroke in the eastern Han of China. Neurol Sci. 2016;37:1679–84.
Acknowledgements
Thanks to all participants for their contributions to this manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Y M and L Y completed the experiment and the draft. JM W, YW L, HY L and JF L took part in the revising the manuscript. Q C collected the sample, ZC X was responsible for data collection and sorting. GQ L and Y S analyzed the data. Y Z designed the study and provided technical support. All authors have approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board at the Traditional Chinese medicine of Baoji Hospital (201802).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
Primers used for this study. Table S2. Basic information of candidate SNPs in CYP1A1 and CYP1A2. Table S3. The association between CYP1A1 polymorphism and stroke risk in patients with cerebral infarction. Table S4. The association between CYP1A1 polymorphism and stroke risk in patients with lacunar infarction. Fig. 1 Linkage disequilibrium (LD) analysis of five SNPs in CYP1A1, and CYP1A2. The LD value is determined by r2 > 0.8 analyzed by Haploview software, version 4.2. Table S5. In silico analysis for SNPs function annotation.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mao, Y., Yang, L., Chen, Q. et al. The influence of CYP1A1 and CYP1A2 polymorphisms on stroke risk in the Chinese population. Lipids Health Dis 19, 221 (2020). https://doi.org/10.1186/s12944-020-01370-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-020-01370-z