
Abstract
Background
Several countries in Southeast Asia are nearing malaria elimination, yet eradication remains elusive. This is largely due to the challenge of focusing elimination efforts, an area where risk prediction can play an essential supporting role. Despite its importance, there is no standard numerical method to quantify the risk of malaria infection. Thus, there is a need for a consolidated view of existing definitions of risk and factors considered in assessing risk to analyse the merits of risk prediction models. This systematic review examines studies of the risk of malaria in Southeast Asia with regard to their suitability in addressing the challenges of malaria elimination in low transmission areas.
Methods
A search of four electronic databases over 2010–2020 retrieved 1297 articles, of which 25 met the inclusion and exclusion criteria. In each study, examined factors included the definition of the risk and indicators of malaria transmission used, the environmental and climatic factors associated with the risk, the statistical models used, the spatial and temporal granularity, and how the relationship between environment, climate, and risk is quantified.
Results
This review found variation in the definition of risk used, as well as the environmental and climatic factors in the reviewed articles. GLM was widely adopted as the analysis technique relating environmental and climatic factors to malaria risk. Most of the studies were carried out in either a cross-sectional design or case–control studies, and most utilized the odds ratio to report the relationship between exposure to risk and malaria prevalence.
Conclusions
Adopting a standardized definition of malaria risk would help in comparing and sharing results, as would a clear description of the definition and method of collection of the environmental and climatic variables used. Further issues that need to be more fully addressed include detection of asymptomatic cases and considerations of human mobility. Many of the findings of this study are applicable to other low-transmission settings and could serve as a guideline for further studies of malaria in other regions.
Similar content being viewed by others


Background
Malaria remains the most serious life-threatening vector-borne disease. Approximately 240 million cases of malaria infection and 620,000 deaths were reported worldwide in 2020. Despite the high global incidence, some regions have made significant progress. Several countries in Southeast Asia, such as Thailand, Malaysia, and Indonesia, are nearing malaria elimination [1, 2]. Yet, many challenges exist in achieving the last mile of malaria elimination. In particular, it requires targeted elimination efforts, where risk prediction can play a supporting role.
Tracking progress through surveillance is essential to target elimination efforts [3], but effective surveillance faces challenges in near-elimination areas. Asymptomatic cases typically represent a small percentage of all malaria cases (less than 5%) [1], and the importance of detecting them increases in areas nearing elimination. Detection of asymptomatic cases requires active surveillance, which entails a high input of effort and costs. Furthermore, the high spatial and temporal heterogeneity of malaria cases in low-transmission settings can result in small areas of relatively high transmission. Both these factors mean that surveillance must be highly targeted. In addition, the importation of malaria cases from high-incidence areas of neighboring countries poses a further challenge. Accurate spatiotemporal risk estimates are essential in identifying transmission hotspots and potential importation routes, which are needed to inform control agencies to focus surveillance and control efforts.
Despite its importance, there is no standard numerical method to quantify the risk of malaria infection, and no acceptable risk level is advised [4]. As a result, each study of risk selects or establishes its own definition of the risk of malaria infection and designs a quantitative method to measure it, leading to incomparable results. Thus there is a need for a consolidated view of existing definitions of risk and factors/predictors considered in assessing risk to analyse the merits of risk prediction models, particularly in low transmission areas.
The risk of malaria infection in a region is typically defined in terms of prevalence (proportion of malaria cases) or entomological inoculation rate (the infective biting per time unit). Due to the labour-intensive nature of collecting such data, risk models commonly use environmental and climatic factors to infer the risk because malaria transmission is highly dependent on them [1]. This systematic review thus focuses on such models of risk, examining studies of risk in Southeast Asia with regard to their suitability in addressing the challenges of malaria elimination in low transmission areas. Factors examined include the definition of the risk of malaria infection used in each study, the spatial and temporal granularity, the environmental and climatic factors associated with the risk, the analysis techniques used to infer risk, and the generalizability of the approach. Figure 1 provides an overview of the dimensions analysed in each paper included in this review. This systematic review aims to serve as a guideline for malaria epidemiology studies in low-transmission settings.

An overview of dimensions of analysis in each paper
Methods
Inclusion criteria
-
The search terms are contained in the title, abstract, or keywords
-
Studies focus on utilizing environment and weather as predictors of risk
-
Studies are conducted in Southeast Asia region [5,6,7] (Thailand, Myanmar, Vietnam, Laos, Cambodia, Philippines, Malaysia, Indonesia, Singapore, Timor-Leste, and Brunei)
-
Studies are peer-reviewed articles or proceedings papers
-
Studies are written in English.
Exclusion criteria
-
Studies have irrelevant titles or abstracts. For example, this includes studies that mainly explore other vector-borne diseases or focus on drug experimentation or the evaluation of treatment schemes
-
Full papers are not accessible
-
Studies examine other risk factors, such as behavioural, serological, or genetic material factors, without mentioning environmental factors
-
Studies are literature reviews, systematic reviews, or protocols
Search terms
The search terms were defined to select studies involving malaria, environmental and climatic factors, risk, and the Southeast Asia region [5,6,7]. The search used was: malaria AND (“risk factors” OR “risk areas” OR “risk”) AND (“environment” OR “environmental” OR “environmental factors” OR “landcover” OR “land cover” OR “land-cover” OR “land covers” OR “land cover types” OR “land use” OR “land-use” OR “landscape”) AND (“Southeast Asia” OR Thailand OR Myanmar OR Vietnam OR Laos OR Cambodia OR Philippines OR Malaysia OR Indonesia OR Singapore OR Timor-Leste OR Brunei). The duration of publication was limited to 10 years (2010–2020). Four electronic databases were searched: PubMed, EMBASE (Medline), Web of Science, and Google Scholar.
Appraisal of the articles
The estimation of the risk of malaria based on environmental and climatic factors requires a study to select (i) a definition of risk of malaria infection, (ii) the environmental and climatic variables to use, (iii) statistical models, and (iv) quantification approach to explore the relationship between environmental and climatic factors, and risk. Each of the studies was examined according to these criteria.
Results
Search and selection strategy
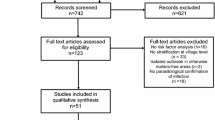
Figure 2 shows an overview of the search for articles. Use of the search terms and inclusion criteria resulted in 1297 articles being retrieved. The EndNote software (version 10) [8] was used to remove ineligible articles based on the exclusion criteria. Examination identified 200 duplicate articles, which were excluded accordingly. This left 1097 articles for further selection based on the titles and the abstracts. A total of 1014 articles were removed because they had irrelevant titles or irrelevant descriptions in the abstracts. Of the 83 articles left for further selection, 58 were excluded: four were literature reviews, systematic reviews, or research protocols, four were conducted outside Southeast Asia, 21 did not have the full manuscripts accessible, 27 were descriptive studies of other factors, such as serological factors, and two had different titles when the manuscripts were accessed. After the third screening, 25 articles were left for analysis.

Search and selection process
Definition of risk and indicators of malaria transmission
Among the 25 articles selected, nine studies were conducted in Malaysia, four in Thailand, four in China along the border with Myanmar, three in Cambodia, and two each in Indonesia, Lao PDR, and Vietnam (Table 1). All the studies examined directly used an indicator of malaria transmission in a region as their definition of risk. The studies used three indicators to measure the degree of malaria transmission: (1) the prevalence of malaria infection in the human population, (2) the prevalence of the parasite in the vector population, and (3) measures of vector abundance as proxy measures. The articles corresponding to each approach are discussed in turn. A summary of the articles is provided in Table 2.
The prevalence of infection in the human population
The prevalence of infection in the human population is typically expressed as the percentage of the sampled population infected, commonly detected through microscopy and malaria rapid diagnostic test (RDT). A variety of spatial and temporal granularities were used in measuring prevalence. In terms of spatial granularity, four articles reported the prevalence among households [9,10,11,12], seven reported the prevalence among villages [13,14,15,16,17,18,19], four reported the prevalence among districts [20,21,22,23], and one reported the prevalence among provinces [24]. Three studies [25,26,27] reported the risk in terms of the number of cases at the village (hamlet) level without baseline population adjustment. The measures of the risk of infection also varied according to temporal granularity. Thirteen studies used yearly reports [9,10,11, 13, 14, 17,18,19, 22,23,24,25, 27], and six studies used monthly reports [12, 15, 16, 20, 21, 26]. There was no particular association between the spatial and temporal granularities.
The prevalence of infection in the vector population
The entomological inoculation rate (EIR) is computed by the number of mosquitoes captured by the human landing catch approach per unit of time, such as per night and the distribution of the malaria parasite in the captured mosquitoes. Only two studies [28, 29] used human landing catch and extracted DNA from the captured mosquitoes to estimate the EIR. Both studies collected the EIR at the village level. The study by Durnez et al. [28] reported the EIR over 1 year, while the study by Van Bortel et al. [29] reported it monthly. Both studies apply enzyme-linked immunosorbent assay (ELISA) to detect Plasmodium parasites in the captured mosquitoes.
Vector abundance
Studies in this category conducted entomological surveys, such as the collection of larva near households or at the fringe of the forests or the collection of mosquitoes using standard CDC light traps, human landing catch, or cow-baited traps without detecting the parasite. There were five articles in this group, and they all reported their indicators among villages. Fornace et al. [30] used human landing catch to collect the biting rate per night over a period of 1 year. Ahmad et al. [31] presented the risk with the number of larvae near households collected over 1 year. Zhang et al. [32] and Tangena et al. [33] measured the abundance of mosquitoes using light traps and human-baited double net traps, respectively.
Environmental and climatic variables
In terms of environmental factors, 15 articles used land cover types such as types of plantations or crops [16, 17, 24, 25, 27, 33], hilly or flat areas [13, 16, 18, 25, 28], households or forest areas [28, 29, 33], distance to forest or river, and the coverage of forest [10, 12, 15, 16, 19, 32]. Eight collected the characteristics using field observations or existing data such as land cover maps and surveys [17,18,19, 24, 25, 27,28,29], while seven articles processed data from satellite images [10, 12, 13, 15, 16, 32, 33]. Three articles used other variables to characterize the environment. Yang et al. [23] used rice yield per square kilometre from field observation. Fornace et al. [30] used enhanced vegetation Index (EVI), while Okami and Kohtake [21] used normalized difference vegetation index (NDVI), normalized difference water index (NDWI), and topographic wetness index (TWI). The number of reviewed articles grouped by environmental factors is summarized in Table 3.
In terms of climatic factors, three studies investigated only the effect of the climatic factors from field observations or the reports from weather stations without using environmental factors [20, 22]. The other six studies investigated both climatic and environmental factors. The climatic factors included humidity [12, 20, 24], rainfall [12, 18, 20, 23, 24], temperature [12, 20,21,22,23,24], and seasons (wet and dry) [33]. Of all the studies that investigated the effects of climatic factors, two studies used monthly-aggregated data [12, 20], four studies used annually-aggregated data [18, 21, 23, 24], and one study used seasonally-aggregated data [22]. The summarized number of reviewed articles grouped by climatic factors is provided in Table 4.
Five studies did not use the characteristics of environmental and climatic factors discussed above. Four mentioned mosquito breeding sites near households, such as stagnant water sources or livestock near households [9, 11, 26, 31], and all of the studies collected the data using field observations. One study explored the locations of clusters of infected people along different parts of a river [14].
Statistical models
This section describes statistical analysis techniques used in the studies to analyse and quantify the relationship between environmental and climatic variables and malaria risk. The analyses can be categorized into three main groups based on the characteristics of the dependent variable (malaria risk). Some studies estimate the prevalence in the population, represented as a continuous or discrete dependent variable. Others estimate the individual risk, represented as dichotomous malaria outcome dependent variable. Thirteen articles adopted techniques to study population-level continuous dependent variables. Examples of continuous dependent variables include risk score generated by a linear combination [16] and the aggregated incidence or prevalence of malaria-infected cases [15, 17, 18, 23]. The techniques include multiple linear regression [24], generalized linear regression [21, 26, 33], generalized linear mixture models [15, 17], generalized linear mixed models with a negative binomial distribution [19], geographically weighted regression (GWR) [18, 23], regression trees (CART) [28], multi-criteria decision analysis (MCDA) [16], Bayesian hierarchical models [10], and Bayesian models with Integrated Nested Laplace Approximation [30]. Four articles applied techniques to investigate population-level discrete dependent variables, such as the integer number of malaria cases in different villages or areas. The models used were negative binomial regression [29], zero-inflated Poisson (ZIP) regression [22], Poisson regression [20], and Pearson's correlation [12]. Finally, five articles estimated the individual risk, represented as dichotomous malaria outcome dependent variable. The techniques included in the studies are logistic regression [11, 13, 27], hierarchical logistic regression [9], and matched univariate and multivariate logistic regression [25]. In addition, three studies performed only descriptive analysis of the abundance of mosquitoes [31, 32] and Plasmodium parasites [14].
Aside from the dependent variable, the reviewed articles can be categorized based on statistical methods. Seventeen articles used generalized linear models (GLMs), while eight applied other techniques. A summary of the reviewed articles grouped by the statistical models is provided in Table 5.
Quantifying the relationship between environmental and climatic factors and risk
In the previous section, the main components to quantify the relationship between the characteristics of environment and climate and malaria infection were explored. Here the focus is on the approaches that the studies used to report their results. There are three groups: odds ratio or relative risk (RR), regression/correlation, and other methods. The reviewed articles grouped by the quantification approaches are summarized in Table 6, while the summarized characteristics of the reviewed articles are provided in Table 7.
Odds ratio and relative risk
Odds ratio (OR) and relative risk (RR) are widely used (approximately 40%) in earlier studies [9, 11, 13, 15, 19, 22, 25,26,27, 33]. In an epidemiological setting, both indicators measure the association between exposure and an outcome. In this review, the exposure to malaria risk is an individual staying in presumably high-risk areas, and the outcome is that an individual develops malaria infection. The relative risk is defined as the ratio between the proportion of the population infected among those exposed to risk and the proportion of the population infected among those not exposed to risk. The odds ratio (OR) is considered an approximation of RR when the outcomes of interest are rare [34]. A RR (or OR) of 1.0 means no difference in risk (or odds) of infection between groups of exposed and non-exposed individuals. An RR (or OR) of more than 1.0 indicates an increase in risk (or odds) among exposed individuals and vice versa.
Three studies quantified the relationship between the number of identified malaria-infected people and the presence of mosquito larval habitats near households, such as stagnant ponds created by rain or running streams in forests [9, 11, 26]. Nixon et al. [9] reported a reduction in the risk of infection for households located farther than 1.6 km from larval habitat areas of Anopheles sundaicus in Indonesia, expressed as an odds ratio of 0.21 [95% confidence interval (CI): 0.14–0.32]. The presence of stagnant ponds, a larval habitat of Anopheles balabacensis, resulted in an odds ratio of identified malaria cases of 7.3 (95% CI 1.2–43.5) in a study in Malaysia [11], while the presence of cattle stalls, a larval habitat areas of Anopheles dirus, resulted in an odds ratio of 1.78 (95% CI 0.85–3.74) in a study in Lao PDR [26]. All three studies reported that larval habitats found within a distance of 1.6 km from a household increases the odds of malaria-infected individuals compared to households located outside the range.
Five studies quantified the relationship between the number of identified malaria-infected people and the observed environment surrounding households, including the elevation and the coverage of different land cover types such as agricultural vegetation, forest, and villages. Two studies conducted in Malaysia showed that the high rate of deforestation over the past 5 years resulted in an odds ratio of malaria-infected individuals in villages of 2.22 (95% CI 1.53–2.93) [19]. Consistent with the result of another study by Grigg et al. [27], the presence of long grass around households, which is considered to be evidence of deforestation, resulted in an odds ratio of malaria-infected individuals of 2.85 (95% CI 1.25–3.46) in Malaysia. Meanwhile, two studies conducted in the Philippines and along the China-Myanmar border investigated malaria transmission by An. balabacensis, An. dirus, and Anopheles minimus. These two studies did not report the effect of deforestation but emphasized the impact of forest coverage and the elevated areas around the households. In the Philippines, Fornace et al. [13] reported that households surrounded by more than 30% of forested area within 1 km resulted in an OR of 2.4 (95% CI 1.29–4.46) compared to households surrounded by less than 30% of forested area. The study along the China-Myanmar border reveals that individuals residing in foot-hill and moderate-hill households in Myanmar have an OR of malaria infection of 5.45 (95% CI 2.52–11.8) and 42.82 (95% CI 5.13–315.75) compared to people who possess households located in upper land or mountainous areas [25].
Another study conducted in Lao PDR broadly investigated the distribution of Anopheles mosquitoes. The study reported that village areas have an OR of 1.95 (95% CI 1.60–2.39) in the rainy season and 2.76 (95% CI 2.20–3.48) in the dry season of capturing Anopheles as compared to secondary forests, which contradicts the other studies. On the other hand, capturing Anopheles mosquitoes in a rubber plantation resulted in an OR of 0.46 (95% CI 0.35–0.61) in the rainy season and 0.55 (95% CI 0.40–0.76) in the dry season, as compared to the secondary forest [33]. The author discussed the possibility that the outcome could result from the low capture rate of the Anopheles mosquitoes, which is considered a common issue in low-transmission areas [35, 36].
In addition to the effect of the different land cover types, two studies investigated the role of weather in malaria transmission. Lawpoolsri et al. [15] reported an OR of malaria infections of 1.05 (95% CI 1.02–1.09) for Plasmodium vivax and 1.27 (95% CI 1.23–1.31) for Plasmodium falciparum as the mean minimum temperature increases by 1 °C at the Thai-Myanmar border. In Vietnam, Wangdi et al. [22] reported that an increment in maximum temperature by 1 °C increased the infection risk of P. falciparum by 3.9% (95% CI 3.5–4.3%) and of P. vivax by 1.6% (95% CI 0.9–2.0%) [22].
Regression and correlation
Two approaches have been mainly used to produce the quantifiers, the regression approach and others. The results are usually shown as weights or coefficients in models. There were eight studies in this category [12, 16, 18, 20, 21, 23, 24, 30].
Five studies applied a group of regression approaches: geographically weighted regression (GWR), Poisson regression, generalized linear regression, and multivariate regression. Two studies adopted the GWR quantifying the relationship between environmental/climatic factors and malaria infections. One study in Indonesia reported significant coefficients of altitude, distance from forests, and rainfall [18]. Another study on the China-Myanmar border quantified the effect of the annual average temperature, annual cumulative rainfall, and rice yield per square kilometer on malaria infections [23]. A study using the Poisson regression reported the significant effect of the maximum/minimum/mean temperature, rainfall, and humidity on malaria infections [20]. Okami and Kohtake adopted a generalized linear regression model to quantify the relationship between the normalized difference vegetation index (NDVI), normalized difference water index (NDWI), topographic wetness index (TWI), annual average temperature, and malaria reports [21]. Kaewpitoon et al. [24] applied multivariate regression to quantify the relationship and found a significant association between malaria infections and the forest areas and an average annual relative humidity.
In addition to the regression approaches, three studies applied MCDA and Pearson's correlation analysis to quantify the relationship between environment/climate and malaria infections, while the Bayesian model with Integrated Nested Laplace Approximation to quantify the relationship between environments/weather and the distribution of mosquitoes. The MDCA quantifies the effect of six environmental factors consisting of forest coverage, cropland coverage, distance to a water body, elevation, distance to urbanized areas, and distance to the road [16]. Pearson's correlation was adopted by Mercado et al. [12], who identified four significant environmental and climatic factors associated with the risk of malaria infections, including forest coverage, median temperature with a lag time of 1- and 2-month, average temperature with a lag time of 1- and 2-month, and average humidity with the lag time of 2- and 3-month. Fornace et al. [30] adopted the Bayesian model with Integrated Nested Laplace Approximation and found the significant factors consisting of EVI and distance to the forest (100 m) from a village and the distribution of captured mosquitoes (An. balabacensis).
Other methods
Seven studies included in this review used other quantifiers, including the malaria prevalence, the distribution of mosquitoes, the relative importance index, and the mean biting rate. Fornace et al. [10] reported the prevalence of malaria infections within different parts of a village. Sato et al. [17] reported the prevalence of malaria infections found in different land use types, such as palm oil plantations or rubber plantations. Similarly, Sluydts et al. [14] reported the prevalence of malaria infections in several villages without statistical analysis. Two studies quantified the number of disease-carrier mosquitoes found in nearby households. Ahmed et al. [31] reported the distribution of mosquitoes, while Zhang et al. [32] explored the diversity of the mosquitoes between villages and forest areas using the diversity indices of mosquitoes (Simpson’s diversity index and Shannon–Wiener’s index). Durnez et al. [28] adopt the relative importance index score of discriminants to rank the importance between forests and villages that affect mosquito distribution. Van Bortel et al. [29] observed the distribution of mosquitoes using the mean biting rate per night.
Discussion
Definition of risk
The World Health Organization (WHO) defines malaria risk as the malaria infection rate in a human population [37], which was used in 70% of the reviewed studies. Estimating the malaria risk based on the infection rate captures the disease burden [4, 37]. The reviewed studies obtained the malaria occurrence in humans based on the number of infections from malaria clinics in communities [15, 16, 18, 27], the regional public health offices [12, 17, 19,20,21,22,23,24,25], the door-to-door active case detection and screening [9, 11, 13, 14, 26, 30], and national disease registration systems [38,39,40]. However, the reports of malaria infection from the national disease registration systems may be incomplete or delayed, depending on the strength of the surveillance system in different countries [41].
Approximately 30% of the reviewed studies estimated the risk of malaria from the rate of malaria infection in combination with entomological determinants of malaria, such as estimates of the vector abundance and the prevalence of the Plasmodium parasite in Anopheles mosquitoes. The diversity of Anopheles mosquitoes is very high, and only a subset of the Genus transmits malaria [42, 43]. Thus, it is important to take into account the variation in main malaria vectors within the region (e.g., An. minimus and Anopheles maculatus in Thailand [35] vs. Anopheles leucosphyrus in Malaysia [19]). To provide a more accurate assessment of malaria risk, the vector abundance can be supplemented with an estimate of the distribution of Plasmodium parasites in mosquitoes [44], as represented by EIR, which measures the intensity of malaria transmission [45, 46]. Although EIR is informative, an extremely low number of mosquitos carrying malaria parasites in low-transmission areas often hinders the acquisition of EIR. Studies conducted in low transmission areas reported that only approximately 1% of captured mosquitoes had Plasmodium parasites [35, 36, 47]. Hence, it is not surprising that only 2% of the studies included in this review reported EIR as an indicator of malaria risk.
In low-transmission settings, a significant contributor to malaria transmission can be the importation of the parasite from high-transmission areas due to human mobility [15, 48, 49]. There are two basic mechanisms of importation. The importation can be caused by infected individuals living in high-transmission areas visiting low-transmission areas or by individuals living in low-transmission areas visiting and becoming infected in a high-transmission area and then bringing the infection back with them when they return home. To quantify the risk of importation, a definition of malaria risk in the high transmission area is needed, but somewhat different definitions of malaria risk are required for each of the two scenarios just enumerated. In the first case, it is sufficient to define the risk of malaria in terms of the prevalence in the high-transmission area population since the importation is occurring from that population. In the second case, a more sophisticated model is needed that quantifies the risk based on the time a traveller spends in the high-transmission area. Although none of the studies reviewed here used such a model, such models do exist in the literature. In terms of vector-borne diseases, a mathematical model proposed by Massad et al. [50] quantifies the risk of malaria for travellers to areas with stable transmission by considering the duration of exposure and season. The individual risk calculation proposed by Stoddard et al. [51] and Tatem et al. [52] illustrates the effect of the time spent in risk areas on the chance of dengue and malaria infection, respectively. Moreover, similar time-based models have also been proposed to quantify the risk of exposure to environmental hazards [53, 54].
Environmental and climatic variables
Environment and climate play an important role in malaria transmission [55,56,57]. All studies in this review included land use or land cover types that contribute to the distribution of mosquitoes. Various land cover types use used, but forests and villages were the most widely used in the studies. Forests or areas dominated by trees, including crop fields or agricultural plantations, are associated with enhanced malaria transmission because of the appropriate temperature, humidity, and breeding sites for the mosquitoes [58,59,60], whereas villages and urban areas are associated with lower malaria transmission [28]. For forest areas, detailed characteristics, such as the area of the canopy coverage and the height of the trees, are also used [61, 62].
Satellite imagery has long been used in malaria transmission studies [58, 63,64,65] and provides a variety of spatial and temporal resolutions [66, 67] without additional cost. However, utilizing the data involves several steps to extract, manipulate, and summarize data and to compute environmental indices [68], which requires expertise from epidemiology and geographic information systems [66]. Approximately 30% of the reviewed studies used satellite imagery to collect data, while the others obtained data from relevant local government agencies. Although data from both sources are acceptable, there is a need to establish a standardized taxonomy of environmental data in the studies. Consider the land-cover type forest as an example. Broadly, it is considered an area without dwellings [29]. At the same time, it can also be characterized in fine-detailed levels as a young, thick, or fallow forest [27]. The differences in the definitions of environment data limit the possibility of repeatability and reusability of the findings from studies.
In addition to land cover, other proxies commonly used to determine malaria transmission include the slope, the altitude, the distance from the breeding sites of mosquitoes (water sources such as a river, paddy field, or forest), and a group of vegetation indices. A moderate slope (less than 12 degrees) [69] is known to facilitate the formation of small running streams or ponds that are appropriate for mosquitoes to breed in [70]. Approximately 8% of studies reviewed included slope in predicting malaria risk. The distance from households or villages to high-risk land cover types such as forests was considered a risk factor for malaria infections in 16% of the reviewed studies. Likewise, evidence shows that villages or households found within a range of mosquito breeding sites or flight ranges (for example, 1.5 km for An. dirus [71, 72]) are prone to be high-transmission areas [73, 74], and the use of such distance measurement was observed in 16% of the reviewed studies. The vegetation index, which indicates the vegetation state in a study area, has long been recognized as relevant to malaria transmission [75,76,77]. Among several available vegetation indices [78], NDVI and EVI were widely used in the spatial modelling of malaria risk [79, 80] and occurred in 8% of the reviewed studies.
Nearly 26% of the reviewed studies directly included climatic factors such as precipitation, humidity, and temperature in estimating malaria risk. In addition, the effect of climatic factors is often indirectly incorporated into the estimation by means of seasonality over the data collection interval [33, 36]. The development of mosquitoes from the aquatic to the adult stage is highly correlated with rainfall and temperature [56, 81, 82]. The studies in this review employed different temporal resolutions of the rainfall and temperature ranging from hourly to annually. Because emerging from pupae to adult mosquito takes approximately 10–14 days, weekly or monthly weather reports are commonly used [81, 83,84,85]. In addition to disease risk mapping, higher temporal resolutions, such as daily or hourly, are useful in the context of mosquito behaviour, such as the time of night with the highest biting rate [35].
Human activity and population mobility
Non-environmental factors that are considered to have a pronounced effect on the risk of malaria transmission are human activity and population mobility. In the agricultural sector, both subsistence and commercial farming involve water-harvesting, storage, and irrigation activities that support the breeding of mosquitoes that carry the malaria parasite [86]. Studies that investigated the risks of malaria in rubber plantations [87, 88], paddy fields [86, 89], fruit orchards [90, 91], and palm oil plantations [27, 87] have shown a high prevalence of malaria among the labour force in the agricultural sector. Nearly 30% of the reviewed studies included factors from agricultural settings in their studies.
High population density, urbanization, and poor climatic conditions can force hired hands and workers into swidden farming and logging in forested foothills. Singhanetra-Renard [92] and Dev et al. [93] found that workers in swidden farming areas have a high risk of malaria since they are exposed to Anopheles mosquitoes that breed in small reservoirs in forested areas and shady clearings on hilly scrub terrain. The taxing physical requirements to commute to the workplace in such terrains have often led to increased logging and subsequent increase in activities such as foraging, fishing, and hunting of seasonal wild produce [94, 95]. Human mobility originating from such high-risk areas poses a continuous risk of malaria introduction into more urbanized and densely populated spaces. Besides activities in agriculture, economic activities in country border areas such as smuggling [92], livestock farming and movement [96, 97], trading of commodities [98, 99], and seeking refuge [100, 101] have been taken into account in determining the malaria risk, and the results show the association with the high rate of malaria infections in populations.
Nearly 30% of the studies included in this review were conducted in border areas, and all of them emphasized the neglected transmission of malaria caused by human mobility. Nonetheless, only one study examined the relationship between mobility and malaria transmission by looking at the relationship between human mobility and the distribution of mosquitoes [30]. Human movement contributes to the circulation of malaria parasites from high-risk areas into areas where local transmission is unsustainable. The calculated risk for non-immune hosts staying longer than 4 months in a high-risk urban setting during peak transmission is only about 0.5% per visit [50]; however, non-immunes who carried out activities in or across the high-risk forest and border areas have been the subjects of large-scale seasonal outbreaks [92, 102, 103]. Imported infections are often the reason for frequent malaria clusters along international borders of Southeast Asian countries, as most of these countries share long land borders with a typical topography consisting of mountain ranges and rivers [104].
Failure to consider population movement contributed to the failure of malaria eradication campaigns in the 1950s and 1960s [105]. Similarly, cross-border malaria hinders countries from achieving malaria elimination [106]. For the latter, consider Thailand as an example. Although most of Thailand is malaria-free, it has yet to achieve malaria elimination since the border region shared with Myanmar continues to have endemic malaria [15, 48, 49]. Due to the diversity of human mobility patterns at different spatial scales [107], acquiring mobility data is a challenging task. Quantification of human mobility has been carried out through epidemiological surveillance data [108], parasite genetic data [109], self-reported travel surveys [99], interviews [108, 110], GPS trackers [111], and anonymized mobile phone data [112]. Surveys and interviews are the principal methods for identifying imported cases, but they can be unreliable and limited due to the scope of memory bias [113]. On the other hand, tracking personalized positions to high temporal and spatial resolution with mobile GPS data is non-trivial. In fact, malaria risk may increase as a result of a combination of different forms of mobility, as well as other factors unrelated to population movements [114, 115].
Statistical models
In this review, 70% of the studies used types of generalized linear models (GLM), which are designed to generalize linear regression models to investigate non-linear relationships between dependent and independent variables [116]. GLMs also accept a variety of distributions that describe the dependent variables, including Poisson, binomial, and normal, using link functions. Dependent variables in GLMs can be of two types: continuous and discrete. GLMs are easily interpretable and considered flexible as they facilitate the addition of proxies such as socioeconomic factors [117], human mobility indicators [48], seasonality [50], and the use of prevention methods [118] to predict malaria transmission. As the predictors can be incorporated easily, GLM models are prone to include highly correlated independent variables in the models, such as NDVI and rainfall [119, 120] or NDVI and land surface temperature [121, 122]. The presence of multicollinearity between independent variables can lead to an inaccurate estimation of the relationship between the independent and dependent variables [123, 124]. Crucially, predictors must be examined for collinearity, and six studies performed such a test in the variable selection process [15, 18, 23, 26,27,28]. It is also important to note that when an independent variable that changes over time is included, GLMs are known to be sensitive to autocorrelation in errors [125, 126]. Although it is essential to explore the effect of autocorrelation, only one study in this review conducted the autocorrelation analysis [20].
A variety of spatial resolutions are used to measure the intensity of malaria transmission, including at the provincial [24, 127], regional [21, 128], and village levels [14, 17, 27]. Nearly 50% of studies that used a GLM in this review adopted the highest spatial resolution at the village level to investigate malaria transmission in low-endemic settings. Meanwhile, the rest of the studies that used a GLM utilized a low-temporal resolution for weather (annual) with a low spatial resolution (regional). These studies tended to conduct longitudinal data collection to capture the effect of seasonality on malaria transmission, which is pointed out as a limitation in previous studies [108, 110, 113].
In addition to the GLMs, 9% of the reviewed studies employed approaches that originated from Bayesian statistics. The Bayesian approach estimates the posterior distribution using priors and the observed data described by the likelihood function [129]. The prior distribution in malaria transmission is often determined based on expert opinion [130, 131] or inferred from previous work [30, 132]. Although a weakly informative prior is acceptable [129], an inappropriate prior has an effect on the goodness of fit between the prior distribution and the observed data [133]. There is no standard approach to choosing an appropriate prior, but an alternative is to use the prior predictive p-value [134] or Bayes factor [135] to measure the goodness of fit of the selected prior distribution. The posterior distribution is presented with the mean and its credible interval. The accuracy of the posterior distribution is determined by comparing the similarity between the posterior distribution and the observed data distribution [136] or posterior predictive p-value [137]. Two studies in this review did not utilize such techniques for prior and posterior distributions. One possible reason could be the scarcity of available observed data, such as the biting rate of mosquitos [30] and the prevalence of malaria [10] in low-transmission areas. Like the regression approaches, studies with the Bayesian approach need to exclude the unnecessary independent variables with proper techniques such as a collinearity test [123, 124].
Other approaches to investigate the relationship between environment, weather, and the risk of malaria infection include the use of simple correlation analysis and MCDA [138, 139]. Correlation is widely used to explore the relationship between malaria prevalence and the environment due to its simplicity and ease of interpretation [84, 140, 141]. In addition to serving as the main analysis, correlation can be utilized in data exploration and variable selection. Although MCDA requires the elicitation of expert opinion and evidence from previous work, it has the potential to serve as a guideline when field data is absent.
Issues in low-transmission areas
In low-transmission areas, asymptomatic malaria infections obstruct achieving zero local malaria transmission. Despite the typically small number of asymptomatic malaria infections, they can cause malaria outbreaks in near-elimination areas [142]. Asymptomatic infections become an issue because the standard approach to reporting malaria infection comes from passive case detection (by microscopy or rapid diagnosis test-RDT), which misses asymptomatic cases [142]. This review shows that the majority of the studies examined use reports from passive cases detection [15,16,17,18,19,20,21,22, 24, 25, 27]. In contrast, active surveillance requires utilizing sophisticated techniques such as molecular screening methods or conducting follow-up longitudinal studies with a relatively large sample of the population [143,144,145].
In low-transmission settings, two neighboring areas can have different malaria transmission rates [47, 146]. An area with high malaria transmission can be considered a source and its counterpart a sink [102]. Since hotspots can be relatively localized in low transmission areas, data collection should be carried out with high spatial and temporal granularity. This review shows that the highest granularity of data collection on malaria prevalence is at the household level [9,10,11,12]. However, most studies investigate the relationship between environmental and meteorological factors and malaria transmission collected at the village level [13,14,15,16,17,18,19, 25,26,27,28,29, 31,32,33]. The environmental and climatic factors are collected either from satellite images or weather stations because these data collection approaches require less manpower and budget than conducting observations in the actual areas of interest [66]. These approaches to data collection are the only solution in some situations where the areas of interest are distant from each other or almost impossible to reach, such as villages in dense forests or villages in neighboring countries [147,148,149].
Conclusion
There is no standard definition of the risk of malaria, but most studies in this review adopted the malaria infection rate in humans. Furthermore, malaria transmission highly depends on environmental and climatic factors in several ways, yet neither general guidelines for collecting the environmental and climate variables nor the general definition are shared among the studies. Most reviewed studies utilized GLMs to predict risk based on these factors due to the simplicity and flexibility of the models, yet did not perform the collinearity test before fitting the GLM models. Most of the studies were carried out in either a cross-sectional design or case–control studies, and most utilized OR to report the relationship between exposure to risk and malaria prevalence, which unlike relative risk is not a probability [150, 151] and thus can be difficult to interpret in terms of risk.
In near-elimination settings such as Southeast Asia, malaria proceeds to decline, but the region has encountered a number of challenges to its elimination. One challenge is the detection of asymptomatic infections, which is infeasible on a population scale due to the lack of resources. Routine monitoring of malaria infections over a long period in border areas can also be tedious due to the high level of cross-border mobility, which is difficult to monitor in Southeast Asia because of the large border areas without tight control. Accurately identifying hotspots of malaria infection is also extremely crucial. When combined with human mobility, sources of infection can be revealed. However, regular observation is challenging in border areas, for example, when a destination is deep in forests or outside a country. An important component in quantifying risk is an estimate of the population density of Anopheles mosquitoes. However, current approaches, such as larval counts and the use of light traps, are too labour-intensive to use on a routine, widespread basis. These challenges imply the necessity for new approaches to monitoring, prediction, and response to provide more rapidly actionable information to guide national malaria control programmes.
Recommendations
Following from the observations above, a number of recommendations are derived as guidelines for future studies.
-
A more standardized definition of malaria risk would help in comparing and sharing results.
-
Given the lack of standards, an explicit description of environmental and climatic variables used in a study could serve as a guideline for further studies.
-
The collinearity test should be performed before fitting the GLM models since minimizing the existence of collinearity in the models improves the results and their interpretation.
-
Unlike the Relative Risk (RR), Odds Ratio (OR) is not a probability and thus both the OR and RR should be provided in reporting results.
-
Research and development are needed into new approaches to monitoring and prediction, such has integration of human mobility in malaria prediction [52, 152], mosquito monitoring using acoustic sensors [153] or images [154], and novel prediction models [149, 155].
This review has described the definition of risk and explored the characteristics of environmental and climatic factors used for its prediction in studies in Southeast Asia. Many of the findings are applicable to other low-transmission settings and could serve as a guideline for further studies of malaria in other regions.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
References
WHO. Progress towards 0. Malaria-free in SEAR. New Delhi, World Health Organization, Regional Office for South East Asia, 2020. Available from: https://iris.who.int/bitstream/handle/10665/334208/9789290227922-eng.pdf?sequence=1&isAllowed=y
WHO. Malaria on the decline in WHO South-East Asia Region; efforts must continue as risks persist: New Delhi, World Health Organization, Regional Office for South East Asia, [cited 2022 Mar 28]. Available from: https://www.who.int/southeastasia/news/detail/04-12-2019-malaria-on-the-decline-in-who-south-east-asia-region-efforts-must-continue-as-risks-persist-who
Routledge I, Chevéz JER, Cucunubá ZM, Rodriguez MG, Guinovart C, Gustafson KB, et al. Estimating spatiotemporally varying malaria reproduction numbers in a near elimination setting. Nat Commun. 2018;9:2476.
CDC-Centers for Disease Control, Prevention. CDC - malaria - travelers - risk assessment. 2010 [cited 2022 Mar 28]. Available from: https://www.cdc.gov/malaria/travelers/risk_assessment.html
Hutchison CS, Others. Geological evolution of South-east Asia. Vol. 13. Clarendon Press Oxford; 1989.
Suwonkerd W, Ritthison W, Ngo CT, Tainchum K, Bangs MJ, Chareonviriyaphap T. Vector biology and malaria transmission in southeast Asia. In: Manguin S (ed.). Anopheles mosquitoes - New insights into malaria vectors. InTech Open. 2013.
Behrens RH, Carroll B, Hellgren U, Visser LG, Siikamäki H, Vestergaard LS, et al. The incidence of malaria in travellers to South-East Asia: is local malaria transmission a useful risk indicator? Malar J. 2010;9:266.
Edhlund B. EndNote Essentials. Lulu.com; 2015. 174 p.
Nixon CP, Nixon CE, Arsyad DS, Chand K, Yudhaputri FA, Sumarto W, et al. Distance to Anopheles sundaicus larval habitats dominant among risk factors for parasitemia in meso-endemic Southwest Sumba. Indonesia Pathog Glob Health. 2014;108:369–80.
Fornace KM, Brock PM, Abidin TR, Grignard L, Herman LS, Chua TH, et al. Environmental risk factors and exposure to the zoonotic malaria parasite Plasmodium knowlesi across northern Sabah, Malaysia: a population-based cross-sectional survey. Lancet Planet Health. 2019;3:e179–86.
Jeffree SM, Ahmed K, Safian N, Hassan R, Mihat O, Lukman KA, et al. Falciparum malaria outbreak in Sabah linked to an immigrant rubber tapper. Am J Trop Med Hyg. 2018;98:45–50.
Mercado CEG, Lawpoolsri S, Sudathip P, Kaewkungwal J, Khamsiriwatchara A, Pan-Ngum W, et al. Spatiotemporal epidemiology, environmental correlates, and demography of malaria in Tak Province, Thailand (2012–2015). Malar J. 2019;18:240.
Fornace KM, Herman LS, Abidin TR, Chua TH, Daim S, Lorenzo PJ, et al. Exposure and infection to Plasmodium knowlesi in case study communities in Northern Sabah, Malaysia and Palawan. The Philippines PLoS Negl Trop Dis. 2018;12:e0006432.
Sluydts V, Heng S, Coosemans M, Van Roey K, Gryseels C, Canier L, et al. Spatial clustering and risk factors of malaria infections in Ratanakiri Province. Cambodia Malar J. 2014;13:387.
Lawpoolsri S, Chavez IF, Yimsamran S, Puangsa-Art S, Thanyavanich N, Maneeboonyang W, et al. The impact of human reservoir of malaria at a community-level on individual malaria occurrence in a low malaria transmission setting along the Thai-Myanmar border. Malar J. 2010;9:143.
Zhao X, Thanapongtharm W, Lawawirojwong S, Wei C, Tang Y, Zhou Y, et al. Malaria risk map using spatial multi-criteria decision analysis along Yunnan border during the pre-elimination period. Am J Trop Med Hyg. 2020;103:793–809.
Sato S, Tojo B, Hoshi T, Minsong LIF, Kugan OK, Giloi N, et al. Recent incidence of human malaria caused by Plasmodium knowlesi in the villages in Kudat Peninsula, Sabah, Malaysia: mapping of the infection risk using remote sensing data. Int J Environ Res Public Health. 2019;16:2954.
Hasyim H, Nursafingi A, Haque U, Montag D, Groneberg DA, Dhimal M, et al. Spatial modelling of malaria cases associated with environmental factors in South Sumatra. Indonesia Malar J. 2018;17:87.
Fornace KM, Abidin TR, Alexander N, Brock P, Grigg MJ, Murphy A, et al. Association between landscape factors and spatial patterns of Plasmodium knowlesi infections in Sabah. Malaysia Emerg Infect Dis. 2016;22:201–8.
Ninphanomchai S, Chansang C, Hii YL, Rocklöv J, Kittayapong P. Predictiveness of disease risk in a global outreach tourist setting in Thailand using meteorological data and vector-borne disease incidences. Int J Environ Res Public Health. 2014;11:10694–709.
Okami S, Kohtake N. Fine-scale mapping by spatial risk distribution modeling for regional malaria endemicity and its implications under the low-to-moderate transmission setting in Western Cambodia. PLoS ONE. 2016;11:e0158737.
Wangdi K, Canavati SE, Ngo TD, Tran LK, Nguyen TM, Tran DT, et al. Analysis of clinical malaria disease patterns and trends in Vietnam 2009–2015. Malar J. 2018;17:332.
Yang DY, Xu CD, Wang JF, Zhao Y. Spatiotemporal epidemic characteristics and risk factor analysis of malaria in Yunnan Province. China BMC Public Health. 2017;17:66.
Kaewpitoon N, Loyd RA, Kaewpitoon SJ, Rujirakul R. Malaria risk areas in Thailand border. J Med Assoc Thai. 2015;98(Suppl 4):S17-21.
Xu JW, Liu H, Zhang Y, Guo XR, Wang JZ. Risk factors for border malaria in a malaria elimination setting: a retrospective case-control study in Yunnan. China Am J Trop Med Hyg. 2015;92:546–51.
Inthavong N, Nonaka D, Kounnavong S, Iwagami M, Phommala S, Kobayashi J, et al. Individual and household factors associated with incidences of village malaria in Xepon district, Savannakhet province. Lao PDR Trop Med Health. 2017;45:36.
Grigg MJ, Cox J, William T, Jelip J, Fornace KM, Brock PM, et al. Individual-level factors associated with the risk of acquiring human Plasmodium knowlesi malaria in Malaysia: a case-control study. Lancet Planet Health. 2017;1:e97-104.
Durnez L, Mao S, Denis L, Roelants P, Sochantha T, Coosemans M. Outdoor malaria transmission in forested villages of Cambodia. Malar J. 2013;12:329.
Van Bortel W, Trung HD, le Hoi X, Van Ham N, Van Chut N, Luu ND, et al. Malaria transmission and vector behaviour in a forested malaria focus in central Vietnam and the implications for vector control. Malar J. 2010;9:373.
Fornace KM, Alexander N, Abidin TR, Brock PM, Chua TH, Vythilingam I, et al. Local human movement patterns and land use impact exposure to zoonotic malaria in Malaysian Borneo. Elife. 2019;8: e47602.
Ahmad R, Wan Mohamad Ali WN, Mohamad Nor Z, Ismail Z, Abdul Hadi A, Ibrahim MN, et al. Mapping of mosquito breeding sites in malaria endemic areas in Pos Lenjang, Kuala Lipis, Pahang, Malaysia. Malar J. 2011;361.
Zhang SS, Zhou SS, Zhou ZB, Chen TM, Wang XZ, Shi WQ, et al. Monitoring of malaria vectors at the China-Myanmar border while approaching malaria elimination. Parasit Vectors. 2018;11:511.
Tangena JAA, Thammavong P, Malaithong N, Inthavong T, Ouanesamon P, Brey PT, et al. Diversity of mosquitoes (Diptera: Culicidae) attracted to human subjects in rubber plantations, secondary forests, and villages in Luang Prabang Province. Northern Lao PDR J Med Entomol. 2017;54:1589–604.
Connor KA. Quantifying associations: understanding relative risks and odds ratios. Pediatr Rev. 2012;33:473–4.
Sriwichai P, Samung Y, Sumruayphol S, Kiattibutr K, Kumpitak C, Payakkapol A, et al. Natural human Plasmodium infections in major Anopheles mosquitoes in western Thailand. Parasit Vectors. 2016;9:17.
Edwards HM, Sriwichai P, Kirabittir K, Prachumsri J, Chavez IF, Hii J. Transmission risk beyond the village: entomological and human factors contributing to residual malaria transmission in an area approaching malaria elimination on the Thailand-Myanmar border. Malar J. 2019;18:221.
WHO. Malaria. Geneva, World Health Organization, 2022. [cited 2019 Feb 11]. Available from: https://www.who.int/ith/diseases/malaria/en/
Bureau of Epidemiology, Department of Disease Control, Ministry of Public Health, Thailand. Malaria situation. 2022 [cited 2022 Sep 1]. Available from: http://malaria.ddc.moph.go.th/malariaR10/index_newversion.php
WHO. World malaria report 2021. Geneva, World Health Organization, 2021.
WHO. World malaria report 2020. Geneva, World Health Organization, 2020.
Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI. The global distribution of clinical episodes of Plasmodium falciparum malaria. Nature. 2005;434:214–7.
Fantini B. Anophelism without malaria: an ecological and epidemiological puzzle. Parassitologia. 1994;36:83–106.
Morgan K, Somboon P, Walton C. Understanding Anopheles diversity in Southeast Asia and its applications for malaria control. In: Manguin S (ed.). Anopheles mosquitoes - New insights into malaria vectors. InTech Open. 2013.
Rattanarithikul R, Konishi E, Linthicum KJ. Detection of Plasmodium vivax and Plasmodium falciparum circumsporozoite antigen in anopheline mosquitoes collected in southern Thailand. Am J Trop Med Hyg. 1996;54:114–21.
Shaukat AM, Breman JG, McKenzie FE. Using the entomological inoculation rate to assess the impact of vector control on malaria parasite transmission and elimination. Malar J. 2010;9:122.
Das S, Muleba M, Stevenson JC, Pringle JC, Norris DE. Beyond the entomological inoculation rate: characterizing multiple blood feeding behavior and Plasmodium falciparum multiplicity of infection in Anopheles mosquitoes in northern Zambia. Parasit Vectors. 2017;10:45.
Sturrock HJW, Bennett AF, Midekisa A, Gosling RD, Gething PW, Greenhouse B. Mapping malaria risk in low transmission settings: challenges and opportunities. Trends Parasitol. 2016;32:635–45.
Sriwichai P, Karl S, Samung Y, Kiattibutr K, Sirichaisinthop J, Mueller I, et al. Imported Plasmodium falciparum and locally transmitted Plasmodium vivax: cross-border malaria transmission scenario in northwestern Thailand. Malar J. 2017;16:258.
Parker DM, Carrara VI, Pukrittayakamee S, McGready R, Nosten FH. Malaria ecology along the Thailand-Myanmar border. Malar J. 2015;14:388.
Massad E, Behrens RH, Burattini MN, Coutinho FAB. Modeling the risk of malaria for travelers to areas with stable malaria transmission. Malar J. 2009;8:296.
Stoddard ST, Morrison AC, Vazquez-Prokopec GM, Soldan VP, Kochel TJ, Kitron U, et al. The role of human movement in the transmission of vector-borne pathogens. PLoS Negl Trop Dis. 2009;3: e481.
Tatem AJ, Qiu Y, Smith DL, Sabot O, Ali AS, Moonen B. The use of mobile phone data for the estimation of the travel patterns and imported Plasmodium falciparum rates among Zanzibar residents. Malar J. 2009;8:287.
Yu X, Ivey C, Huang Z, Gurram S, Sivaraman V, Shen H, et al. Quantifying the impact of daily mobility on errors in air pollution exposure estimation using mobile phone location data. Environ Int. 2020;141:105772.
Park YM, Kwan MP. Individual exposure estimates may be erroneous when spatiotemporal variability of air pollution and human mobility are ignored. Health Place. 2017;43:85–94.
Lindsay SW, Birley MH. Climate change and malaria transmission. Ann Trop Med Parasitol. 1996;90:573–88.
CDC. About Malaria. [cited 2019 Feb 11]. Available from: https://www.cdc.gov/malaria/about/disease.html
Segun OE, Shohaimi S, Nallapan M, Lamidi-Sarumoh AA, Salari N. Statistical modelling of the effects of weather factors on malaria occurrence in Abuja, Nigeria. Int J Environ Res Public Health. 2020;17:3474.
Stresman GH. Beyond temperature and precipitation: ecological risk factors that modify malaria transmission. Acta Trop. 2010;116:167–72.
Martens P, Kovats RS, Nijhof S, de Vries P, Livermore MTJ, Bradley DJ, et al. Climate change and future populations at risk of malaria. Glob Environ Change. 1999;9:S89-107.
Castro MC. Malaria transmission and prospects for malaria eradication: the role of the environment. Cold Spring Harb Perspect Med. 2017;7:a025601.
Guerra CA, Snow RW, Hay SI. A global assessment of closed forests, deforestation and malaria risk. Ann Trop Med Parasitol. 2006;100:189–204.
The United Nations. The definition of forest by The Food and Agriculture Organization of the United Nations. 2022.
Hay SI, Guerra CA, Tatem AJ, Atkinson PM, Snow RW. Urbanization, malaria transmission and disease burden in Africa. Nat Rev Microbiol. 2005;3:81–90.
Santos-Vega M, Bouma MJ, Kohli V, Pascual M. Population density, climate variables and poverty synergistically structure spatial risk in urban malaria in India. PLoS Negl Trop Dis. 2016;10:e0005155.
Parham PE, Michael E. Modeling the effects of weather and climate change on malaria transmission. Environ Health Perspect. 2010;118:620–6.
Wimberly MC, de Beurs KM, Loboda TV, Pan WK. Satellite observations and malaria: new opportunities for research and applications. Trends Parasitol. 2021;37:525–37.
Rogers DJ, Randolph SE, Snow RW, Hay SI. Satellite imagery in the study and forecast of malaria. Nature. 2002;415:710–5.
Liu Y, Hu J, Snell-Feikema I, VanBemmel MS, Lamsal A, Wimberly MC. Software to facilitate remote sensing data access for disease early warning systems. Environ Model Softw. 2015;74:247–57.
Sithiprasasna R, Linthicum KJ, Liu GJ, Jones JW, Singhasivanon P. Use of GIS-based spatial modeling approach to characterize the spatial patterns of malaria mosquito vector breeding habitats in northwestern Thailand. Southeast Asian J Trop Med Public Health. 2003;34:517–28.
Rattanarithikul R, Green CA, Panyim S, Noigamol C, Chanaimongkol S, Mahapibul P. Larval habitats of malaria vectors and other Anopheles mosquitoes around a transmission focus in northwestern Thailand. J Am Mosq Control Assoc. 1995;11:428–33.
Sanh NH, Van Dung N, Thanh NX, Trung TN, Van Co T, Cooper RD. Forest malaria in central Vietnam. Am J Trop Med Hyg. 2008;79:652–4.
Obsomer V, Defourny P, Coosemans M. The Anopheles dirus complex: spatial distribution and environmental drivers. Malar J. 2007;6:26.
Bøgh C, Lindsay SW, Clarke SE, Dean A, Jawara M, Pinder M, et al. High spatial resolution mapping of malaria transmission risk in the Gambia, west Africa, using LANDSAT TM satellite imagery. Am J Trop Med Hyg. 2007;76:875–81.
Hakre S, Masuoka P, Vanzie E, Roberts DR. Spatial correlations of mapped malaria rates with environmental factors in Belize. Central America Int J Health Geogr. 2004;3:6.
Fastring DR, Griffith JA. Malaria incidence in Nairobi, Kenya and dekadal trends in NDVI and climatic variables. Geocarto Int. 2009;24:207–21.
Gaudart J, Touré O, Dessay N, Dicko AL, Ranque S, Forest L, et al. Modelling malaria incidence with environmental dependency in a locality of Sudanese savannah area. Mali Malar J. 2009;8:61.
Nihei N, Hashida Y, Kobayashi M, Ishii A. Analysis of malaria endemic areas on the Indochina Peninsula using remote sensing. Jpn J Infect Dis. 2002;55:160–6.
Xue J, Su B. Significant remote sensing vegetation indices: a review of developments and applications. J Sensors. 2017;2017:1353691.
Pettorelli N, Vik JO, Mysterud A, Gaillard JM, Tucker CJ, Stenseth NC. Using the satellite-derived NDVI to assess ecological responses to environmental change. Trends Ecol Evol. 2005;20:503–10.
Defries RS, Townshend JRG. NDVI-derived land cover classifications at a global scale. Int J Remote Sens. 1994;15:3567–86.
Kristan M, Abeku TA, Beard J, Okia M, Rapuoda B, Sang J, et al. Variations in entomological indices in relation to weather patterns and malaria incidence in East African highlands: implications for epidemic prevention and control. Malar J. 2008;7:231.
Jawara M, Pinder M, Drakeley CJ, Nwakanma DC, Jallow E, Bogh C, et al. Dry season ecology of Anopheles gambiae complex mosquitoes in The Gambia. Malar J. 2008;7:156.
Bomblies A. Modeling the role of rainfall patterns in seasonal malaria transmission. Clim Change. 2012;112:673–85.
Briët OJT, Vounatsou P, Gunawardena DM, Galappaththy GNL, Amerasinghe PH. Temporal correlation between malaria and rainfall in Sri Lanka. Malar J. 2008;7:77.
Olson SH, Gangnon R, Elguero E, Durieux L, Guégan JF, Foley JA, et al. Links between climate, malaria, and wetlands in the Amazon Basin. Emerg Infect Dis. 2009;15:659–62.
Qunhua L, Xin K, Changzhi C, Shengzheng F, Yan L, Rongzhi H, et al. New irrigation methods sustain malaria control in Sichuan Province. China Acta Trop. 2004;89:241–7.
Soe HZ, Thi A, Aye NN. Socioeconomic and behavioural determinants of malaria among the migrants in gold mining, rubber and oil palm plantation areas in Myanmar. Infects Dis Poverty. 2017;6:142.
Pattanasin S, Satitvipawee P, Wongklang W, Viwatwongkasem C, Bhumiratana A, Soontornpipit P, et al. Risk factors for malaria infection among rubber tappers living in a malaria control program area in southern Thailand. Southeast Asian J Trop Med Public Health. 2012;43:1313–25.
Wangdi K, Kaewkungwal J, Singhasivanon P, Silawan T, Lawpoolsri S, White NJ. Spatio-temporal patterns of malaria infection in Bhutan: a country embarking on malaria elimination. Malar J. 2011;10:89.
Overgaard HJ, Ekbom B, Suwonkerd W, Takagi M. Effect of landscape structure on anopheline mosquito density and diversity in northern Thailand: implications for malaria transmission and control. Landscape Ecol. 2003;18:605–19.
Vythilingam I, Noorazian YM, Huat TC, Jiram AI, Yusri YM, Azahari AH, et al. Plasmodium knowlesi in humans, macaques and mosquitoes in peninsular Malaysia. Parasit Vectors. 2008;1:26.
Singhanetra-Renard A. Malaria and mobility in Thailand. Soc Sci Med. 1993;37:1147–54.
Dev V, Phookan S, Sharma VP, Anand SP. Physiographic and entomologic risk factors of malaria in Assam. India Am J Trop Med Hyg. 2004;71:451–6.
Dysoley L, Kaneko A, Eto H, Mita T, Socheat D, Börkman A, et al. Changing patterns of forest malaria among the mobile adult male population in Chumkiri District. Cambodia Acta Trop. 2008;106:207–12.
Chaveepojnkamjorn W, Pichainarong N. Malaria infection among the migrant population along the Thai-Myanmar border area. Southeast Asian J Trop Med Public Health. 2004;34:48–52.
Zeru MA, Shibru S, Massebo F. Exploring the impact of cattle on human exposure to malaria mosquitoes in the Arba Minch area district of southwest Ethiopia. Parasit Vectors. 2020;13:322.
Prothero RM. Population movements and problems of malaria eradication in Africa. Bull World Health Organ. 1961;24:405–25.
Chaves LSM, Fry J, Malik A, Geschke A, Sallum MAM, Lenzen M. Global consumption and international trade in deforestation-associated commodities could influence malaria risk. Nat Commun. 2020;11:1258.
Carrasco-Escobar G, Matta-Chuquisapon J, Manrique E, Ruiz-Cabrejos J, Barboza JL, Wong D, et al. Quantifying the effect of human population mobility on malaria risk in the Peruvian Amazon. R Soc Open Sci. 2022;9:211611.
Rowland M, Nosten F. Malaria epidemiology and control in refugee camps and complex emergencies. Ann Trop Med Parasitol. 2001;95:741–54.
Anderson J, Doocy S, Haskew C, Spiegel P, Moss WJ. The burden of malaria in post-emergency refugee sites: a retrospective study. Confl Health. 2011;5:17.
Wesolowski A, Eagle N, Tatem AJ, Smith DL, Noor AM, Snow RW, et al. Quantifying the impact of human mobility on malaria. Science. 2012;338:267–70.
Tatem AJ, Huang Z, Narib C, Kumar U, Kandula D, Pindolia DK, et al. Integrating rapid risk mapping and mobile phone call record data for strategic malaria elimination planning. Malar J. 2014;13:52.
Miettinen J, Stibig HJ, Achard F. Remote sensing of forest degradation in Southeast Asia—Aiming for a regional view through 5–30 m satellite data. Glob Ecol Conservation. 2014;2:24–36.
Bruce-Chwatt LJ. Movements of populations in relation to communicable disease in Africa. East Afr Med J. 1968;45:266–75.
Bhumiratana I. Border malaria associated with multidrug resistance on Thailand-Myanmar and Thailand-Cambodia borders: transmission dynamic, vulnerability, and surveillance. Biomed Res Int. 2013;2013:363417.
Barbosa H, Barthelemy M, Ghoshal G, James CR, Lenormand M, Louail T, et al. Human mobility: models and applications. Phys Rep. 2018;734:1–74.
Saita S, Pan-Ngum W, Phuanukoonnon S, Sriwichai P, Silawan T, White LJ, et al. Human population movement and behavioural patterns in malaria hotspots on the Thai-Myanmar border: implications for malaria elimination. Malar J. 2019;18:64.
Tessema S, Wesolowski A, Chen A, Murphy M, Wilheim J, Mupiri AR, et al. Using parasite genetic and human mobility data to infer local and cross-border malaria connectivity in Southern Africa. Elife. 2019;8: e43510.
Lowa M, Sitali L, Siame M, Musonda P. Human mobility and factors associated with malaria importation in Lusaka district, Zambia: a descriptive cross sectional study. Malar J. 2018;17:404.
Carrasco-Escobar G, Fornace K, Wong D, Padilla-Huamantinco PG, Saldaña-Lopez JA, Castillo-Meza OE, et al. Open-source 3D printable GPS tracker to characterize the role of human population movement on malaria epidemiology in river networks: a proof-of-concept study in the Peruvian Amazon. Front Public Health. 2020;8:526468.
Kim Y, Ghorpade A, Zhao F, Pereira FC, Zegras PC, Ben-Akiva M. Activity recognition for a smartphone and web-based human mobility sensing system. IEEE Intell Syst. 2018;33:5–23.
Gomes MFC, Codeço CT, Bastos LS, Lana RM. Measuring the contribution of human mobility to malaria persistence. Malar J. 2020;19:404.
Martens P, Hall L. Malaria on the move: human population movement and malaria transmission. Emerg Infect Dis. 2000;6:103–9.
Aagaard-Hansen J, Nombela N, Alvar J. Population movement: a key factor in the epidemiology of neglected tropical diseases. Trop Med Int Health. 2010;15:1281–8.
Nelder JA, Wedderburn RWM. Generalized Linear Models. J R Stat Soc Ser A. 1972;135:370.
Were V, Buff AM, Desai M, Kariuki S, Samuels A, ter Kuile FO, et al. Socioeconomic health inequality in malaria indicators in rural western Kenya: evidence from a household malaria survey on burden and care-seeking behaviour. Malar J. 2018;17:166.
Brusich M, Grieco J, Penney N, Tisgratog R, Ritthison W, Chareonviriyaphap T, et al. Targeting educational campaigns for prevention of malaria and dengue fever: an assessment in Thailand. Parasit Vectors. 2015;8:43.
Al-Bakri JT, Suleiman AS. NDVI response to rainfall in different ecological zones in Jordan. Int J Remote Sens. 2004;25:3897–912.
Richard Y, Poccard I. A statistical study of NDVI sensitivity to seasonal and interannual rainfall variations in Southern Africa. Int J Remote Sens. 1998;19:2907–20.
Anbazhagan S, Paramasivam CR. Statistical correlation between land surface temperature (LST) and vegetation index (NDVI) using multi-temporal landsat TM data. Int J Adv Earth Sci Engineer. 2016;5:333–46.
Govil H, Guha S, Diwan P, Gill N, Dey A. Analyzing Linear Relationships of LST with NDVI and MNDISI Using Various Resolution Levels of Landsat 8 OLI and TIRS Data. In: Data Management, Analytics and Innovation. Springer Singapore; 2020. p. 171–84.
Weissfeld LA, Sereika SM. A multicollinearity diagnostic for generalized linear models. Commun Stat Theory Methods. 1991;20:1183–98.
Mackinnon MJ, Puterman ML. Collinearity in generalized linear models. Commun Stat Theory Methods. 1989;18:3463–72.
Nishida T, Chen DG. Incorporating spatial autocorrelation into the general linear model with an application to the yellowfin tuna (Thunnus albacares) longline CPUE data. Fish Res. 2004;70:265–74.
Segurado P, Araujo MB, Kunin WE. Consequences of spatial autocorrelation for niche-based models. J Appl Ecol. 2006;43:433–44.
Bottieau E, Gillet P, De Weggheleire A, Scheirlinck A, Stokx J, Das Dores Mosse C, et al. Treatment practices in patients with suspected malaria in Provincial Hospital of Tete, Mozambique. Trans R Soc Trop Med Hyg. 2013;107:176–82.
Wangdi K, Gatton ML, Kelly GC, Banwell C, Dev V, Clements ACA. Malaria elimination in India and regional implications. Lancet Infect Dis. 2016;16:e214–24.
van de Schoot R, Depaoli S, King R, Kramer B, Märtens K, Tadesse MG, et al. Bayesian statistics and modelling. Nat Rev Methods Primers. 2021;1:1–26.
Speybroeck N, Praet N, Claes F, Van Hong N, Torres K, Mao S, et al. True versus apparent malaria infection prevalence: the contribution of a Bayesian approach. PLoS ONE. 2011;6: e16705.
Nkurunziza H, Gebhardt A, Pilz J. Bayesian modelling of the effect of climate on malaria in Burundi. Malar J. 2010;9:114.
Lindgren F, Rue H. Bayesian spatial modelling with R-INLA. J Stat Softw. 2015;63:1–25.
Johnson SR, Tomlinson GA, Hawker GA, Granton JT, Feldman BM. Methods to elicit beliefs for Bayesian priors: a systematic review. J Clin Epidemiol. 2010;63:355–69.
Nott DJ, Drovandi CC, Mengersen K, Evans M. Approximation of Bayesian predictive p-values with regression ABC. Bayesian Anal. 2018;13:59–83.
Kass RE, Raftery AE. Bayes factors. J Am Stat Assoc. 1995;90:773–95.
Gabry J, Simpson D, Vehtari A, Betancourt M, Gelman A. Visualization in Bayesian workflow. arXiv. 2017.
Meng XL. Posterior predictive p-values Ann Statist. 1994;22:1142–60.
Hongoh V, Hoen AG, Aenishaenslin C, Waaub JP, Bélanger D, Michel P, et al. Spatially explicit multi-criteria decision analysis for managing vector-borne diseases. Int J Health Geogr. 2011;10:70.
Malczewski J. GIS and Multicriteria Decision Analysis. John Wiley & Sons; 1999. 408 p.
Wayant NM, Maldonado D, Rojas de Arias A, Cousiño B, Goodin DG. Correlation between normalized difference vegetation index and malaria in a subtropical rain forest undergoing rapid anthropogenic alteration. Geospat Health. 2010;4:179–90.
Huang F, Zhou S, Zhang S, Wang H, Tang L. Temporal correlation analysis between malaria and meteorological factors in Motuo County. Tibet Malar J. 2011;10:54.
malERA Refresh Consultative Panel on Characterising the Reservoir and Measuring Transmission. malERA: An updated research agenda for characterising the reservoir and measuring transmission in malaria elimination and eradication. PLoS Med. 2017;14:e1002452.
Baum E, Sattabongkot J, Sirichaisinthop J, Kiattibutr K, Jain A, Taghavian O, et al. Common asymptomatic and submicroscopic malaria infections in Western Thailand revealed in longitudinal molecular and serological studies: a challenge to malaria elimination. Malar J. 2016;15:333.
Kumari P, Sinha S, Gahtori R, Yadav CP, Pradhan MM, Rahi M, et al. Prevalence of asymptomatic malaria parasitemia in Odisha, India: a challenge to malaria elimination. Am J Trop Med Hyg. 2020;103:1510–6.
Chourasia MK, Raghavendra K, Bhatt RM, Swain DK, Valecha N, Kleinschmidt I. Burden of asymptomatic malaria among a tribal population in a forested village of central India: a hidden challenge for malaria control in India. Public Health. 2017;147:92–7.
Bango ZA, Tawe L, Muthoga CW, Paganotti GM. Past and current biological factors affecting malaria in the low transmission setting of Botswana: a review. Infect Genet Evol. 2020;85:104458.
Mutuku FM, Bayoh MN, Hightower AW, Vulule JM, Gimnig JE, Mueke JM, et al. A supervised land cover classification of a western Kenya lowland endemic for human malaria: associations of land cover with larval Anopheles habitats. Int J Health Geogr. 2009;8:19.
Krefis AC, Schwarz NG, Nkrumah B, Acquah S, Loag W, Oldeland J, et al. Spatial analysis of land cover determinants of malaria incidence in the Ashanti Region. Ghana PLoS One. 2011;6: e17905.
Haddawy P, Hasan AHMI, Kasantikul R, Lawpoolsri S, Sa-angchai P, Kaewkungwal J, et al. Spatiotemporal Bayesian networks for malaria prediction. Artif Intell Med. 2018;84:127–38.
Davies HT, Crombie IK, Tavakoli M. When can odds ratios mislead? BMJ. 1998;316:989–91.
Schechtman E. Odds Ratio, Relative Risk, Absolute risk reduction, and the number needed to treat—which of these should we use? Value Health. 2002;5:431–6.
Sa-ngamuang C, Haddawy P, Lawpoolsri S, Barkowsky T, Sa-angchai P. A study of individual human mobility patterns related to malaria transmission along the Thai-Myanmar Border. In: Proceedings of the 4th International Conference on Medical and Health Informatics. New York, NY, USA: Association for Computing Machinery; 2020. p. 223–9.
Yin MS, Haddawy P, Ziemer T, Wetjen F, Supratak A, Chiamsakul K, et al. A deep learning-based pipeline for mosquito detection and classification from wingbeat sounds. Multimed Tools Appl. 2023;82:5189–205.
Okayasu K, Yoshida K, Fuchida M, Nakamura A. Vision-based classification of mosquito species: comparison of conventional and deep learning methods. NATO Adv Sci Inst Ser E Appl Sci. 2019;9:3935.
Thakur S, Dharavath R. Artificial neural network based prediction of malaria abundances using big data: a knowledge capturing approach. Clin Epidemiold Glob Health. 2019;7:121–6.
Acknowledgements
Not applicable.
Funding
This work is partially supported by a Grant from the National Research Council of Thailand (NRCT): NRCT5-RGJ63012-124, a Grant from the National Institutes of Health (U19AI089672), USA, a Grant from the Mahidol University Office of International Relations in support of the Mahidol-Bremen Medical Informatics Research Unit, a Study Group Grant from the Hanse-Wissenschaftskolleg Institute for Advanced Study, and a Grant from DAAD for the Network of Excellence in Advanced Information Technology for Tropical Medicine.
Author information
Authors and Affiliations
Contributions
CS and SL were responsible for defining the search terms. CS was responsible for implementing the search in electronic databases, and both CS and SL evaluated the searched articles to keep related articles. CS, MY, SL, and PH contributed to conceptualizing the work. All authors contributed to the writing and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sa-ngamuang, C., Lawpoolsri, S., Su Yin, M. et al. Assessment of malaria risk in Southeast Asia: a systematic review. Malar J 22, 339 (2023). https://doi.org/10.1186/s12936-023-04772-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04772-3