
Abstract
Background
Observational studies have reported maternal short/long sleep duration to be associated with adverse pregnancy and perinatal outcomes. However, it remains unclear whether there are nonlinear causal effects. Our aim was to use Mendelian randomization (MR) and multivariable regression to examine nonlinear effects of sleep duration on stillbirth (MR only), miscarriage (MR only), gestational diabetes, hypertensive disorders of pregnancy, perinatal depression, preterm birth and low/high offspring birthweight.
Methods
We used data from European women in UK Biobank (N=176,897), FinnGen (N=~123,579), Avon Longitudinal Study of Parents and Children (N=6826), Born in Bradford (N=2940) and Norwegian Mother, Father and Child Cohort Study (MoBa, N=14,584). We used 78 previously identified genetic variants as instruments for sleep duration and investigated its effects using two-sample, and one-sample nonlinear (UK Biobank only), MR. We compared MR findings with multivariable regression in MoBa (N=76,669), where maternal sleep duration was measured at 30 weeks.
Results
In UK Biobank, MR provided evidence of nonlinear effects of sleep duration on stillbirth, perinatal depression and low offspring birthweight. Shorter and longer duration increased stillbirth and low offspring birthweight; shorter duration increased perinatal depression. For example, longer sleep duration was related to lower risk of low offspring birthweight (odds ratio 0.79 per 1 h/day (95% confidence interval: 0.67, 0.93)) in the shortest duration group and higher risk (odds ratio 1.40 (95% confidence interval: 1.06, 1.84)) in the longest duration group, suggesting shorter and longer duration increased the risk. These were supported by the lack of evidence of a linear effect of sleep duration on any outcome using two-sample MR. In multivariable regression, risks of all outcomes were higher in the women reporting <5 and ≥10 h/day sleep compared with the reference category of 8–9 h/day, despite some wide confidence intervals. Nonlinear models fitted the data better than linear models for most outcomes (likelihood ratio P-value=0.02 to 3.2×10−52), except for gestational diabetes.
Conclusions
Our results show shorter and longer sleep duration potentially causing higher risks of stillbirth, perinatal depression and low offspring birthweight. Larger studies with more cases are needed to detect potential nonlinear effects on hypertensive disorders of pregnancy, preterm birth and high offspring birthweight.
Similar content being viewed by others

Background
Sleep occupies up to one third of the human life span. For adults, the minimum and maximum sleep durations are recommended as 7 and 9 h/day (h/d), respectively [1]. Habitual sleep duration is regulated by genetic factors [2] and can be influenced by a person’s daily routine and lifestyle factors [1]. Pregnancy is associated with alterations in sleep duration: both total and nocturnal sleep duration tend to be longer around the end of the first trimester declining by the third trimester due to pregnancy-induced changes, e.g. uterine contractions, heartburn, orthopnoea, leg cramps, pelvic girdle pain and uncomfortable sleeping position [3,4,5].
A systematic review of observational studies published up to 15 January 2018, which explored associations of prenatal sleep duration with psychological outcomes, reported a linear association of longer sleep duration with a lower risk of perinatal depression [6]. Other systematic reviews indicate that both short (<6 or <7 h/d) and/or long (>9 h/d) duration are associated with higher risks of adverse perinatal events (see Additional file 1: Table S1) [6,7,8,9,10,11,12,13]. In particular, short sleep duration is associated with higher risks of gestational diabetes [7, 8], preeclampsia [8] and preterm birth [8,9,10], while long sleep duration is associated with higher risks of stillbirth [8, 11] and gestational diabetes [8, 12]. These observational studies may be vulnerable to residual confounding, with demonstrated between-study heterogeneity likely influenced by variation in confounder control [14]. Few studies have examined several outcomes together, which is important for trying to identify a range of duration that minimizes any adverse outcomes. Studies to date have mostly examined binary variables of short and long sleep duration rather than trying to explore different patterns across sleep duration.
In the absence of large, well-conducted randomized controlled trials of interventions targeting on sleep duration during pregnancy [15], Mendelian randomization (MR) provides an alternative means of probing the effect of sleep duration on adverse pregnancy and perinatal outcomes. MR uses single nucleotide polymorphisms (SNPs) that are robustly associated with potential risk factors, e.g. sleep duration, as instrumental variables (IVs) to explore causal effects of these factors on outcomes [16, 17]. MR is less prone to confounding than observational studies, as SNPs being randomly allocated at meiosis cannot be influenced by the wide range of socio-demographic or behavioural factors conventionally confounding observational studies, nor can they be influenced by health status [16, 17]. Under key assumptions (see the “Discussion” section), MR can be used to estimate a causal effect from SNPs-risk factor and SNPs-outcome associations, and to estimate nonlinear relationships [18, 19]. SNPs robustly associated with self-report sleep duration have recently been identified in the most updated genome-wide association study (GWAS) using UK Biobank (UKB) [2]. These SNPs have been used as IVs in MR studies to investigate linear and nonlinear effects of sleep duration on cancer [20], cardiometabolic health [21, 22] and mental health [23, 24]. To the best of our knowledge, MR has not been used to explore effects of sleep duration on pregnancy and perinatal outcomes.
Our aims are to use MR to explore and compare linear and nonlinear effects of lifelong sleep duration on partum-related (stillbirth, miscarriage and preterm birth), pregnancy-related (gestational diabetes, hypertensive disorders of pregnancy and perinatal depression) and offspring-related (low birthweight, high birthweight and variation in birthweight) outcomes in up to 324,826 women. We also conducted confounder-adjusted linear and nonlinear multivariable regression (MVreg) of maternal sleep duration reported during pregnancy with outcomes, except stillbirth and miscarriage, in 76,669 women.
Methods
Participants
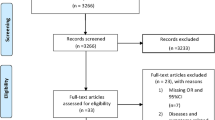
This study was undertaken using data from the MR-PREG collaboration, which aims to explore causes and consequences of different pregnancy and perinatal events [25]. We include women of European descent from (1) UKB (176,897 women recruited at age 40–60 years between 2006 and 2010 and providing retrospective reports of pregnancy and perinatal outcomes (Additional file 2: Fig S1A) [26]); (2) FinnGen (the nation-wide network of Finnish biobank with up to 123,579 women recruited at 54 years (interquartile range=25) with outcomes obtained via health record linkage), and three birth cohorts (women recruited during pregnancy with most outcomes collected prospectively); (3) Avon Longitudinal Study of Parents and Children (ALSPAC, 6826 women recruited between 1991 and 1992 (Additional file 2: Fig S1B)); (4) Born in Bradford (BiB, 2940 women recruited between 2007 and 2010 (Additional file 2: Fig S1C)); and (5) the Norwegian Mother, Father and Child Cohort Study (MoBa, 76,669 women in MVreg, of whom 14,585 women had genome wide data and were included in two-sample MR; recruited between 1999 and 2009 (Additional file 2: Fig S1D)). All studies had ethical approval from relevant national or local bodies and participants provided written informed consent. Details of their recruitment procedures, information on genetic data and measurements of baseline characteristics are described in Additional file 2: Text S1 [23, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41].
Self-report sleep duration
Information on sleep duration was obtained from UKB and MoBa. In UKB, sleep duration was measured via a self-administered question—“About how many hours sleep do you get in every 24 hours? (please include naps)” at the initial assessment centre, which recruited mostly non-pregnant participants. Women reported their sleep duration in integer values ranging from 1 to 23. Following the methods of a previous MR study [23], 1448 (0.8%) women with sleep duration shorter than 2 h or longer than 12 h were treated like those who had not responded to this question. UKB contributed to two-sample (linear) and one-sample (nonlinear) MR (Fig. 1).

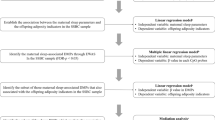
Summary of methods and data contributing to this study. aAmong 176,897 women, 99.2% of them with sleep duration ranging from 2 to 12 h were included. bIn one-sample MR, the three and five groups of different duration lengths are based on thresholds from existing literature [1, 8]. We also split UKB women into thirds (N=58,483) as a sensitivity analysis to increase instrument strength and power in the longest duration group. cTwo-sample MR methods include: inverse variance weighted, MR-Egger, weighted median and leave-one-out analysis. dMultivariable regression analysis adjusted for maternal age at time of delivery, parity, education, smoking status in pregnancy, alcohol intake in pregnancy, body mass index before pregnancy and average household income. Abbreviations: ALSPAC, Avon Longitudinal Study of Parents and Children; BiB, Born in Bradford; MoBa, Norwegian Mother, Father and Child Cohort Study; MR, Mendelian randomization; SNP, single nucleotide polymorphism; UKB, UK Biobank
In MoBa, sleep duration was assessed via a self-administered question—“How many hours a day do you usually sleep now when you are pregnant?” at 30 weeks of gestation. Women reported their sleep duration in five categories, which were “over 10 h”, “8–9 h”, “6–7 h”, “4–5 h” and “less than 4 h”. The questionnaire did not specify whether to include naps so it is unclear whether the women would have reported duration only for night sleep or across 24 h (as in UKB). Due to small numbers, we combined the last two categories into “≤5 h”. MoBa contributed to analyses of the relevance of genetic IVs in pregnancy, two-sample MR and linear/nonlinear associations in MVreg (Fig. 1).
Sleep duration data were not available in ALSPAC, BiB or FinnGen, which all contributed to two-sample MR only (Fig. 1).
Selection of genetic IVs for self-report sleep duration
Currently, nine GWAS of self-report sleep duration are available, with details in Additional file 1: Table S2 [2, 42,43,44,45,46,47,48,49,50,51]. All GWAS combined women and men (mainly of White European descent) with no sex specific analyses; the four largest GWAS (N >100,000) all included UKB. The largest and most updated GWAS identified 78 SNPs genome-wide significantly (P-value<5×10−8) associated with sleep duration in its discovery cohort—UKB men and women (N=446,118), with 55 of them being directionally consistent in the replication cohort—the Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE, N=47,180) [2]. To maximize statistical power and IV strength in our main analyses, we considered the 78 discovery SNPs from this largest GWAS. Additional file 1: Table S3 lists the characteristics of these 78 SNPs, as well as summary data for their association with sleep duration in UKB women used in this study. The 78 SNPs explained 0.69% of the variance in sleep duration in UKB [2]. We used the “clumping” function from the TwoSample MR R package [52], to check that the 78 SNPs were independent (i.e. linkage equilibrium) based on a threshold of R2≤0.01 and all European samples from the 1000 genome project as the reference population; the 78 SNPs are all independent of each other. For two-sample MR, we used these 78 SNPs as IVs with their effect alleles identified from the GWAS discovery results. For one-sample MR, we combined these 78 SNPs with the same effect alleles into an unweighted genetic risk score [53]. It was not possible to obtain external (to UKB) weights from genetic association estimates generated in the GWAS discovery analyses (due to sample overlap with our analyses sample) or replication stage (due to the trait increasing allele being inconsistent between discovery and replication stages for some SNPs).
The same GWAS has also reported results for short (defined as ≤6 h/d) and long (defined as ≥9 h/d) sleep duration, identifying 27 and 9 independent genome-wide significant SNPs, respectively [2]. We decided a priori not to use these in the one-sample MR in order to explore other possible nonlinear association or different thresholds of “healthy” sleep duration to these and for different outcomes. There were further technical considerations that are described in more detail in Additional file 2: Text S2 [2, 24, 54,55,56].
Pregnancy and perinatal outcomes
We examined associations with nine outcomes. Partum-related outcomes included stillbirth, miscarriage and preterm birth (gestational age <37 completed weeks). Pregnancy-related outcomes included gestational diabetes, hypertensive disorders of pregnancy and perinatal depression (occurring during pregnancy or within a year after delivery). Offspring-related outcomes included low birthweight (birthweight <2500 g), high birthweight (birthweight >4500 g) and birthweight (grams) as a continuous outcome. Definitions of these outcomes in UKB, ALSPAC, BiB, MoBa and FinnGen, and harmonization of their definitions across cohorts are provided in Additional file 1: Table S4. In UKB, women who reported both never experiencing a pregnancy loss and giving birth to zero child were defined as never pregnant and thus removed from the analyses. If multiple pregnancies were enrolled in the birth cohorts, we randomly selected one pregnancy per woman. In FinnGen, it was only possible to include miscarriage (N=9113 cases/89,340 controls), gestational diabetes (N=5687 cases/117,892 controls), hypertensive disorders of pregnancy (N=4255 cases/114,735 controls) and preterm birth (N=5480 cases/98,626 controls), and those outcomes were defined based on ICD codes [39].
We combined pre-eclampsia and gestational hypertension as hypertensive disorders of pregnancy since we would not have sufficient statistical power to consider pre-eclampsia separately. In UKB, gestational age was only available for a subset of women (N=7280) who were young enough to have had a child born during or after 1989, the earliest date for which linked hospital labour and perinatal data are available. As a result, numbers with data on preterm birth are smaller than for any other outcome, and we decided a priori to examine associations with low/high birthweight rather than small-/large-for-gestational age. In the three birth cohorts, stillbirth and miscarriage were retrospectively obtained (from self-report or clinical records) at the time of the index pregnancy. In ALSPAC and MoBa, women were asked if they had ever experienced a (previous) stillbirth or miscarriage, but numbers of pregnancy loss at the index pregnancy were too small for reliable results. Additionally, for miscarriage, we were concerned about misclassification or selection bias due to women who had experienced a miscarriage prior to recruitment.
Confounders in MoBa for MVreg
We considered maternal age at time of delivery, parity, education, smoking status in pregnancy, alcohol intake in pregnancy, body mass index before pregnancy and average household income as potential confounders based on their known or plausible effects on maternal sleep duration and on pregnancy and perinatal outcomes. Details of how these variables were measured are provided in Additional file 2: Text S1.
Statistical analyses
One-sample MR exploring whether data support nonlinear over linear effects
One-sample MR requires individual level data for estimation, and thus, we used data from UKB women (Fig. 1). Nonlinear MR involves generating subgroups of different sleep duration length within the study sample and undertaking (linear) MR within each of those subgroups and then comparing effects across subgroups. We could split the women into subgroups based on their reported sleep duration, but doing that could introduce a type of selection bias known as collider bias in the subsequent MR, because of the role of the genetic IV on sleep duration [19]. To avoid that, we generated “residual” sleep duration by regressing self-reported sleep duration on the genetic risk score, adjusting for genetic array, women’s age and top 40 PCs (to adjust for residual population stratification [57]). Residual sleep duration was then calculated as each woman’s observed sleep duration minus the mean centred genetic contribution to sleep duration from the IV [19, 55]. Therefore, the residual measure has a mean of 7.18 with a range from 1.77 to 12.33 h/d (Additional file 2: Fig S2) [55]. We then stratified UKB women into three and five groups based on the residual duration (details shown in Additional file 1: Table S5). We present results for three and five groups and compared effects of increasing sleep duration (measured in 1-h units) from MR analyses across the groups. Three groups would enable comparing results between analyses with greater power and IV strength, while five groups provide finer gradation for more detailed exploration of nonlinearity.
Within each subgroup of residual sleep duration, we followed the approach used in a previous MR study [55] to calculate linear MR estimates for sleep duration on pregnancy and perinatal outcomes using the Wald ratio method [56]. Technical details of this method are described in Additional file 2: Text 2. Finally, we tested differences in MR estimates across groups using Cochran’s Q-statistic, with P-value <0.05 suggesting heterogeneity [19, 55]. We performed meta-regression of MR estimates against the mean of sleep duration in each group to test nonlinearity [19, 55]. A low P-value for the regression coefficient of sleep duration mean across groups provides evidence against the null hypothesis of a linear or null association, and we used the conventional P-value <0.05 as evidence to support nonlinearity. Similar non-null effects across the group (e.g. if there was evidence of a similar magnitude positive effect in all groups) would support a linear effect. Table 1 illustrates how the pattern of a nonlinear effect is identified by comparing the magnitudes and directions of linear associations in each group and synthesizing results from one-sample and further two-sample MR.
Two-sample MR exploring linear effects
We further undertook two-sample MR to explore potential linear effects (Fig. 1). Details about obtaining SNP-sleep duration and SNP-outcome associations are described in Additional file 2: Text S1. In UKB women, we generated summary statistics from the individual participant data in a split cross-over samples design [23]. This involved randomly splitting the sample in half and generating summary data for SNP-sleep duration and SNP-outcome associations in both datasets and then conducting MR with SNP-sleep duration associations from dataset A and SNP-outcome associations from dataset B, and vice versa [23]. This was because the GWAS of sleep duration was conducted in UKB [2], and this split cross-over design enabled us to have the advantages (e.g. weak instrument bias towards the null and minimizing over-prediction or winners curse) of MR using two independent samples [30, 58]. We then meta-analysed the MR estimates from the two together for each sleep duration-outcome pair using fixed-effects (with inverse variance weights). We also conducted two-sample MR using SNP-sleep duration associations from UKB women, and SNP-outcome associations meta-analysing ALSPAC, BiB, MoBa and FinnGen using fixed effects with inverse variance weights. For each outcome, we combined MR estimates from all five cohorts using fixed effects (with inverse variance weights). The degree of between-study heterogeneity was assessed using Cochran’s Q-statistic.
We used the MR inverse variance weighted (IVW) method as the main analysis to explore the presence of linear effects of sleep duration on pregnancy and perinatal outcomes. IVW is a weighted regression of SNP-outcome associations on SNP-sleep duration associations with the intercept of the regression line forced through zero [59].
Sensitivity and additional analyses
The strength of the IVs was evaluated by the F-statistic of IV-sleep duration associations [17]. We selected the 78 SNPs robustly related to sleep duration in general population rather than pregnant women [2]. Therefore, we used linear regression to test whether our IV was also related to sleep duration during pregnancy in MoBa [16, 17]. The one-sample MR assumes the genetic IV-sleep duration association is consistent across groups [19, 55]. We explored this by using Cochran’s Q-statistic and meta-regression of these associations against the mean of observed sleep duration in each stratum [19, 55].
As with previous two-sample MR studies testing effects of sleep duration on different outcomes [20,21,22,23,24], we used the 78 genome-wide significant SNPs from the discovery sample in the original GWAS to maximize power and IV strength. To explore whether our results were sensitive to IV selection, we repeated IVW analyses with the 55 SNPs that were directionally consistent in the replication sample and the 43 SNPs of those that also reached genome-wide significance. To explore potential unbalanced horizontal pleiotropy, our sensitivity analyses for two-sample MR included (I) assessing between-SNP heterogeneity (which if present may be due to one or more SNPs having horizontal pleiotropic effects on the outcome) using Cochran’s Q-statistic and leave-one-out analysis [59] and (II) conducting weighted median [60] and MR-Egger [61], which are more likely to be more robust in the presence of horizontal pleiotropy [62]. Technical details of these MR methods were summarized in our previous study [63]. A consistent finding across multiple MR methods would strengthen causal inference. When using MR to assess maternal exposures in pregnancy on perinatal outcomes, results might be biased via a path from maternal genotype to the outcome via fetal genotype [64]. To explore this, we compared maternal SNP-outcome associations with and without adjustments for fetal SNPs in the birth cohorts.
MVreg in MoBa exploring linear/nonlinear associations and whether data supported nonlinear over linear associations
We explored observational associations of maternal sleep duration at 30 weeks of gestation with each outcome, except stillbirth and miscarriage, using logistic regression (linear regression for birthweight). To explore a possible nonlinear association, we entered the categories as indicator variables and obtained estimates comparing each of ≤5 h/d, 6–7 h/d and ≥10 h/d to our chosen reference category of 8-9 h/d. We also explored possible linear associations by recoding ≤5, 6–7, 8–9 and ≥10 h/d categories using their mid-points (i.e. 3.5, 6.5, 8.5, 11 h/d, respectively), assuming MoBa had the same minimum and maximum sleep duration as UKB. Statistical evidence for a nonlinear association across categories was obtained from a likelihood ratio test comparing the two models above.
Amongst the 76,669 MoBa women eligible for inclusion in MVreg (defined as having returned both pregnancy questionnaires [65]), there were varying amounts of missing data for sleep duration, outcomes and covariates. This was lowest for parity (0.2% missing), and highest for preterm birth (8.4% missing). Additional file 1: Table S6 provides full details of the proportion missing for each variable. Therefore, we undertook both complete records and multiple imputation analyses. Complete records analyses only included women with sleep duration, an outcome and seven confounders (N=42,001 (for stillbirth) to 62,929 (for birthweight)), assuming that missingness is not associated with the outcome. MI was conducted on all 76,669 eligible women, and assumes data are missing at random (i.e. conditional on variables included in multiple imputation, the outcome would not differ between those with missing data and those without) [66, 67].
Multiple imputation used chained equations [66] and was conducted for each outcome separately. As shown in Additional file 1: Table S6, each imputation model included one outcome, the exposure (sleep duration), the seven confounders (same as those used in complete records analyses) and three auxiliary variables (paternal education, paternal smoking status in pregnancy and maternal usage of other kinds of nicotine in pregnancy). These auxiliary variables were selected on the basis that they were likely to be important predictors of missing data. For each outcome, 100 imputed datasets were generated and results were pooled across these datasets using Robin’s Rules [68].
All multiple imputation and MVreg after imputation were conducted in Stata 16 (StataCorp LLC, College Station, TX), because we were using code provided in the STRengthening Analytical Thinking for Observational Studies (STRATOS) framework for dealing with missing data and this is only provided in Stata [66]. All other analyses (including one- and two-sample MR, and complete records MVreg analyses) were conducted in R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria), with “TwoSampleMR” package for two-sample MR [52].
Results
Table 2 summarizes the characteristics of included women for MR analyses, and the proportion of cases for pregnancy and perinatal disorders across the four cohorts, which differ substantially for some outcomes. Additional file 1: Table S6 summarizes the characteristics of MoBa women for MVreg analyses.
One sample MR in UKB exploring whether data supported nonlinear over linear effects
The F-statistic for our genetic risk score in 175,499 UKB ever pregnant women was 1219, and within each group across all three ways in which they were stratified were between 55 and 646 (Additional file 1: Table S5). For each stratification approach, we also identified statistical evidence for between-group differences in associations of genetic risk score with sleep duration (Additional file 1: Table S5).
Figures 2, 3 and 4 show the MR linear effects within five sleep duration groups; the differences in directions and magnitudes of the results between groups can be used to describe the pattern of nonlinear effects of sleep duration. There was evidence of nonlinear effects of sleep duration on stillbirth, perinatal depression and low birthweight, with a pattern suggesting that both shorter and longer sleep duration increased risks of stillbirth and low birthweight, with shorter sleep duration increasing perinatal depression (Figs. 2, 3 and 4). The nonlinear effect with mean birthweight was broadly consistent with low birthweight as expected (Fig. 4). For other outcomes, there was no strong evidence of nonlinearity, though we acknowledge that several of the within-group results are imprecise with wide, and hence overlapping confidence intervals. Patterns were generally similar for the analyses with three groups (Additional file 2: Fig S3) [1, 8].

One-sample MR estimates of effects of sleep duration on partum-related outcomes in five groups in UK Biobank women. We present MR estimates of a linear effect of increasing duration on the outcome across the length of residual duration (h/day) covered in each group. Further details about identifying the pattern of nonlinear effects are illustrated in Table 1. P-value for Cochran’s Q-statistic testing statistical evidence for between-group heterogeneity. P-value for nonlinearity testing statistical evidence whether the MR estimates are changed as the self-reported sleep duration mean increases. Abbreviation: CI, confidence interval; MR, Mendelian randomization; OR, odds ratio

One-sample MR estimates of effects of sleep duration on pregnancy-related outcomes in five groups in UK Biobank women. We present MR estimates of a linear effect of increasing duration on the outcome across the length of residual duration (h/day) covered in each group. Further details about identifying the pattern of nonlinear effects are illustrated in Table 1. P-value for Cochran’s Q-statistic testing statistical evidence for between-group heterogeneity. P-value for nonlinearity testing statistical evidence whether the MR estimates are changed as the self-reported sleep duration mean increases. Abbreviation: CI, confidence interval; HDP, hypertensive disorders of pregnancy; MR, Mendelian randomization; OR, odds ratio

One-sample MR estimates of effects of sleep duration on offspring-related outcomes in five groups in UK Biobank women. We present MR estimates of a linear effect of increasing duration on the outcome across the length of residual duration (h/day) covered in each group. Further details about identifying the pattern of nonlinear effects are illustrated in Table 1. P-value for Cochran’s Q-statistic testing statistical evidence for between-group heterogeneity. P-value for nonlinearity testing statistical evidence whether the MR estimates are changed as the self-reported sleep duration mean increases. Abbreviation: CI, confidence interval; MR, Mendelian randomization; OR, odds ratio
Two-sample MR exploring linear effects
In two-sample MR, the mean F-statistic for 78 sleep duration-IVs in 175,449 women was 15. In MoBa, 0.42% variation of sleep duration in pregnancy was explained by its IV, and one effect allele increase in the IV was associated with 0.008 h/d longer sleep duration (95% confidence interval: 0.003, 0.013, P-value = 0.0009, F-statistic = 31). Additional file 1: Tables S3 & 7 show summary results for SNP-sleep duration and SNP-outcome associations used in two-sample MR. After adjusting for fetal genotype (only possible in the birth cohorts), SNP-outcome associations with stillbirth, hypertensive disorders of pregnancy, perinatal depression, preterm birth and low birthweight were slightly attenuated; the associations with miscarriage, gestational diabetes, high birthweight and birthweight moved slightly away from the null (Additional file 2: Fig S4).
The main IVW analyses combining UKB with other cohorts find no strong evidence to support a linear effect across the whole distribution of reported sleep duration of lifetime predisposition to longer average duration on the pregnancy and perinatal outcomes (Fig. 5). However, 95% confidence intervals were wide for most outcomes (Fig. 5). Sensitivity analyses using weighted median and MR-Egger for these outcomes were largely directionally consistent (Fig. 5). Between-SNP heterogeneity for MR analyses was observed for preterm birth, gestational diabetes, hypertensive disorders of pregnancy, perinatal depression, high birthweight and birthweight (Additional file 1: Table S8), but leave-one-out analyses suggested little evidence for a single SNP driving the MR IVW results (Additional file 2: Fig S5-S7). The MR-Egger intercept P-values provided little evidence of unbalanced horizontal pleiotropy for any outcome (Additional file 1: Table S8). Across all outcomes, there was little evidence of between-study heterogeneity (all Cochran’s P-values >0.1, Fig. 5). IVW analyses using 55 SNPs and 43 SNPs (i.e. those with some evidence of replication) were broadly consistent with those from our main analyses with 78 SNPs (Additional file 2: Fig S8) [2].

Two-sample MR estimates for linear effects of sleep duration on partum-, pregnancy- and offspring-related outcomes, meta-analysing all cohorts. aP-values for Cochran’s Q-statistic testing statistical evidence for between-cohort heterogeneity, in inverse variance weighted, weighted median and MR-Egger, respectively. bResults are ORs for binary outcomes (mean difference in birthweight) per lifetime genetic tendency to 1 h longer during the 24-h duration, with numeric estimates listed in Additional file 1: Table S8. Abbreviations: CI, confidence interval; HDP, hypertensive disorders of pregnancy; MR, Mendelian randomization; OR, odds ratio
MVreg in MoBa exploring and comparing linear and nonlinear associations
Nonlinear models fitted data better than linear models across most outcomes (likelihood ratio P-values comparing the linear versus nonlinear models = 0.02 to 3.2×10−52). The one exception, based on the conventional threshold of <0.05, was gestational diabetes (0.06). Odds of gestational diabetes, hypertensive disorders of pregnancy, perinatal depression, preterm birth, low birthweight and high birthweight were higher in women reporting ≤5 h/d and ≥10 h/d sleep compared with the reference category of 8–9 h, despite some wide confidence intervals including the null (Fig. 6). Amongst them, perinatal depression showed a reverse “J-shaped” nonlinear association with considerably stronger magnitudes of associations than other outcomes (Fig. 6), which is in line with the result in one-sample nonlinear MR in UKB (Fig. 3). Differences in mean offspring birthweight were lower for those reporting ≤5 h/d, 6–7 h/d and ≥10 h/d compared to 8-9 h/d (Fig. 6). Broadly consistent results were observed for low and high birthweight when all eligible participants were included in MVreg (Additional file 2: Fig S9), and for complete records analyses (Additional file 1: Table S9).

Multivariable regression associations of self-reported sleep duration categories with partum-, pregnancy- and offspring-related outcomes in MoBa. Estimates are from multiple imputation, with numeric results listed in Additional file 1: Table S9. Abbreviations: CI, confidence interval; HDP, hypertensive disorders of pregnancy; MoBa, Norwegian Mother, Father and Child Cohort Study; OR, odds ratio
Discussion
In this study, we find MR analyses support nonlinear effects of sleep duration on stillbirth, perinatal depression and low birthweight. With the exception of gestational diabetes, we find statistical evidence for nonlinear associations with all outcomes in MVreg. We have interpreted the MR results as reflecting genetically predicted lifetime sleep duration [18]. We interpreted MVreg results as reflecting associations of sleep duration in pregnancy, though this exposure is likely to correlate strongly with sleep duration before and after pregnancy as demonstrated in a study of 1480 women showing sleep duration 2 years after pregnancy associated with sleep duration at 32 weeks of gestation and 2 months after birth, and with chronic sleep duration [69]. The association between our genetic risk score and sleep duration at 30 weeks of gestation in MoBa indicated that genetic susceptibility to lifetime longer sleep duration is correlated with sleep duration during pregnancy.
Previous observational studies have tended to assume nonlinearity and explored associations of short and long sleep duration with most pregnancy and perinatal outcomes, reporting unfavourable associations of both short and long duration with gestational diabetes, and of short duration with pre-eclampsia and preterm birth [7,8,9,10, 12]. Our MVreg analyses in one of the largest studies to date were broadly consistent with these findings. In MVreg, we found evidence of increased risks of perinatal depression with short and long duration, whereas a previous systematic review reported an association with shorter sleep duration only, which is consistent with our one-sample MR analyses [6]. MR analyses also supported increased risks of stillbirth and low birthweight with shorter and longer duration. MR evidence for other outcomes was too imprecise to make reliable conclusions. Furthermore, differences between what have been estimated (linear lifelong effects within groups of residual duration in one-sample MR versus odds of outcomes comparing for self-reported duration categories to a reference category in pregnancy in MVreg) make direct comparisons between our MR results versus our, and other published, MVreg associations difficult. As the sources of bias in two methods (MR and MVreg) differ, where we have consistency between them, this increases our confidence in those consistent results being the causal association [33, 38, 70,71,72]. The broad consistencies of nonlinear associations of sleep duration with a range of pregnancy and perinatal outcomes between our MVreg and existing literature highlight the need for further MR analyses of potential nonlinear effects in much larger sample sizes with sleep duration measured in pregnancy. The MoBa sample size of >14,000 is too small for nonlinear MR but with further GWAS in that study this might become possible in the future.
The associations of shorter and longer sleep duration with pregnancy and perinatal outcomes may be related to sleep fragmentation, circadian dysrhythmia, insulin resistance and chronic inflammatory [7, 8]. MR analyses support a causal effect of chronic inflammation on depression and anxiety outside of pregnancy [73], and therefore, this is a plausible mechanisms for perinatal depression. Multiple lines of evidence (including MR) demonstrate the positive linear effect of higher maternal glucose on higher birthweight [74, 75]. Therefore, insulin resistance is unlikely to mediate the effect we observe on low birthweight, but it is possible that inflammation has a role here [76].
Strengths and limitations
The main strengths of our study include that (1) as far as we are aware it is the first time that MR has been used to explore potential linear and nonlinear effects of lifetime sleep duration on pregnancy and perinatal outcomes; (2) we conducted confounder-adjusted MVreg of sleep duration in pregnancy in MoBa, with a larger sample size than most previous studies; and (3) we explored a range of pregnancy and perinatal outcomes.
Our MR analyses may be vulnerable to weak instrument bias, especially within some sleep duration groups in one-sample nonlinear MR which is expected to be biased towards the confounded MVreg result [58]. We used a genetic risk score to minimize the contribution of weak IVs in one-sample MR (with the lowest F-statistic=64). Weak instrument bias in our two-sample MR analysis would bias the results towards the null [58]. Our MR analyses may be biased by horizontal pleiotropy, particularly because IVs for sleep duration have also been strongly linked to other sleep traits [2], as well as lifestyle factors such as obesity and alcohol consumption [77]. We explored the potential presence of bias by horizontal pleiotropy with sensitivity analyses for two-sample MR, which are more robust to such bias than IVW [62], but one-sample MR estimates in each stratum could still be prone to horizontal pleiotropy, as methods available for exploring horizontal pleiotropy in one-sample MR would be underpowered in each stratum [63]. We were able to demonstrate that results were not biased by a path via fetal genotype to the outcome, showing similar maternal SNP-outcome associations with and without adjustment for fetal genotype. The MR monotonicity assumption requires that the proposed genetic IVs for longer sleep duration cannot increase sleep duration in some women while decreasing it in others—i.e. women are “compliers” [78]. In nonlinear MR, constant IV-duration effects across all groups is a stronger version of the monotonicity assumption [19]. As we found slightly different genetic risk score-duration associations across groups, our nonlinear MR results should be interpreted cautiously as tests for causal directions rather than as precise estimations of causal effects [78].
Both our MR and MVreg estimates could be vulnerable to selection bias as discussed in detail in other papers [79,80,81]. UKB participants are better educated and healthier than the general UK adult population [82], and perinatal depression and preterm birth may not be missing at random [28, 83]. Our target population consisted of women who have had at least one pregnancy. In UKB and birth cohorts, we were able to restrict the analyses to ever pregnant women. In FinnGen, the comparison group is all women without the outcome (i.e. including women who have never been pregnant). These are publicly available data that we cannot reanalyse. However, any potential bias resulting from this is unlikely to be substantial given we obtained near-identical results from UKB when we included never pregnant women to those presented here, and results did not substantially differ if we removed FinnGen from our analyses.
Sleep duration was measured via one self-administrated question in UKB and MoBa. Its measurement error in UKB may not bias our MR estimates, as sleep duration is a continuous variable in 1-h units [84]. However, non-differential misclassification of sleep duration categories in MoBa would be expected to bias MVreg towards the null [85]. Further studies using large, actigraphy-based sleep duration data would be required to explore optimal cut-off points for our suggestive nonlinear associations [19]. Moreover, it was ambiguous whether the variable in MoBa represented nocturnal sleep duration or included daytime naps. For our outcomes, there may be misclassification because of the absence of universal testing, assessment via self-report questionnaires, and differences between studies in definitions. Our MVreg analyses for pregnancy outcomes (including gestational diabetes, hypertensive disorders of pregnancy and perinatal depression) in MoBa could be vulnerable to reverse causality, as they were defined based on some information earlier than 30 weeks of the index pregnancy. Furthermore, our MVreg analyses in MoBa could be biased by residual and unmeasured confounding.
Conclusions
Our study shows that shorter and longer sleep duration increase risks of stillbirth, perinatal depression and low birthweight. Our MVreg analyses support nonlinear over linear effects of sleep duration on all pregnancy and perinatal outcomes, except gestational diabetes. Taken together these findings highlight the need for further MR studies based on larger numbers, particularly of cases for pregnancy and perinatal outcomes. Studies in women from non-White European ethnic background are necessary for understanding the extent to which results generalize to other groups.
Availability of data and materials
We used both individual participant cohort data and publicly available summary statistics. We present summary statistics that we generated from those individual participant cohort data in Additional file 1: Tables S3 & S7. Full information on how to access UKB data can be found at its website (https://www.ukbiobank.ac.uk/researchers/). All ALSPAC data are available to scientists on request to the ALSPAC Executive via this website (http://www.bristol.ac.uk/alspac/researchers/), which also provides full details and distributions of the ALSPAC study variables. Similarly, data from BiB are available on request to the BiB Executive (https://borninbradford.nhs.uk/research/how-to-access-data/). Data from MoBa are available from the Norwegian Institute of Public Health after application to the MoBa Scientific Management Group (see its website https://www.fhi.no/en/op/data-access-from-health-registries-health-studies-and-biobanks/data-access/applying-for-access-to-data/ for details). Summary statistics from FinnGen are publicly available on its website (https://finngen.gitbook.io/documentation/data-download). All scripts are available on GitHub (https://github.com/MRCIEU/sleep_duration_pregnancy).
Abbreviations
- ALSPAC:
-
Avon Longitudinal Study of Parents and Children
- BiB:
-
Born in Bradford
- CHARGE:
-
Cohorts for Heart and Aging Research in Genomic Epidemiology
- GWAS:
-
Genome-wide association study
- h/d:
-
Hours/day
- IVs:
-
Instrumental variables
- IVW:
-
Inverse variance weighted
- MoBa:
-
Norwegian Mother, Father and Child Cohort Study
- MR:
-
Mendelian randomization
- MVreg:
-
Multivariable regression
- SNPs:
-
Single nucleotide polymorphisms
- STRATOS:
-
STRengthening Analytical Thinking for Observational Studies
- UKB:
-
UK Biobank
References
Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1:233–43.
Dashti HS, Jones SE, Wood AR, Lane JM, van Hees VT, Wang H, et al. Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nat Commun. 2019;10:1100.
Pengo MF, Won CH, Bourjeily G. Sleep in Women Across the Life Span. Chest. 2018;154:196–206.
Lamberg L. Sleeping poorly while pregnant may not be “normal”. JAMA. 2006;295:1357–61.
Mindell JA, Cook RA, Nikolovski J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015;16:483–8.
Pauley AM, Moore GA, Mama SK, Molenaar P, Symons DD. Associations between prenatal sleep and psychological health: a systematic review. J Clin Sleep Med. 2020;16:619–30.
Yang Z, Zhu Z, Wang C, Zhang F, Zeng H. Association between adverse perinatal outcomes and sleep disturbances during pregnancy: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2022;35:166–74.
Lu Q, Zhang X, Wang Y, Li J, Xu Y, Song X, et al. Sleep disturbances during pregnancy and adverse maternal and fetal outcomes: a systematic review and meta-analysis. Sleep Med Rev. 2020;58:101436.
Warland J, Dorrian J, Morrison JL, O'Brien LM. Maternal sleep during pregnancy and poor fetal outcomes: a scoping review of the literature with meta-analysis. Sleep Med Rev. 2018;41:197–219.
Wang L, Jin F. Association between maternal sleep duration and quality, and the risk of preterm birth: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth. 2020;20:125.
Cronin RS, Wilson J, Gordon A, Li M, Culling VM, Raynes-Greenow CH, et al. Associations between symptoms of sleep-disordered breathing and maternal sleep patterns with late stillbirth: findings from an individual participant data meta-analysis. PLoS One. 2020;15:e0230861.
Zhang X, Zhang R, Cheng L, Wang Y, Ding X, Fu J, et al. The effect of sleep impairment on gestational diabetes mellitus: a systematic review and meta-analysis of cohort studies. Sleep Med. 2020;74:267–77.
Abeysena C, Jayawardana P, R DAS. Maternal sleep deprivation is a risk factor for small for gestational age: a cohort study. Aust N Z J Obstet Gynaecol. 2009;49:382–7.
Metelli S, Chaimani A. Challenges in meta-analyses with observational studies. Evid Based Ment Health. 2020;23:83–7.
Bacaro V, Benz F, Pappaccogli A, De Bartolo P, Johann AF, Palagini L, et al. Interventions for sleep problems during pregnancy: a systematic review. Sleep Med Rev. 2019;50:101234.
Davey Smith G, Ebrahim S. ‘Mendelian randomization’: can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol. 2003;32:1–22.
Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey SG. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27:1133–63.
Burgess S, Davey Smith G, Davies NM, Dudbridge F, Gill D, Glymour MM, et al. Guidelines for performing Mendelian randomization investigations. Wellcome Open Res. 2019;4:186.
Staley JR, Burgess S. Semiparametric methods for estimation of a nonlinear exposure-outcome relationship using instrumental variables with application to Mendelian randomization. Genet Epidemiol. 2017;41:341–52.
Richmond RC, Anderson EL, Dashti HS, Jones SE, Lane JM, Strand LB, et al. Investigating causal relations between sleep traits and risk of breast cancer in women: Mendelian randomisation study. BMJ. 2019;365:l2327.
Daghlas I, Dashti HS, Lane J, Aragam KG, Rutter MK, Saxena R, et al. Sleep duration and myocardial infarction. J Am Coll Cardiol. 2019;74:1304–14.
Wang J, Kwok MK, Au Yeung SL, Li AM, Lam HS, Leung JYY, et al. Sleep duration and risk of diabetes: observational and Mendelian randomization studies. Prev Med. 2019;119:24–30.
Henry A, Katsoulis M, Masi S, Fatemifar G, Denaxas S, Acosta D, et al. The relationship between sleep duration, cognition and dementia: a Mendelian randomization study. Int J Epidemiol. 2019;48:849–60.
Anderson EL, Richmond RC, Jones SE, Hemani G, Wade KH, Dashti HS, et al. Is disrupted sleep a risk factor for Alzheimer’s disease? Evidence from a two-sample Mendelian randomization analysis. Int J Epidemiol. 2020;50:817–28.
Brand JS, Gaillard R, West J, McEachan RRC, Wright J, Voerman E, et al. Associations of maternal quitting, reducing, and continuing smoking during pregnancy with longitudinal fetal growth: Findings from Mendelian randomization and parental negative control studies. PLoS Med. 2019;16:e1002972.
Mitchell R, Hemani G, Dudding T, Corbin L, Harrison S, Paternoster L. UK Biobank Genetic Data: MRC-IEU Quality Control, version 2. 2019. https://doi.org/10.5523/bris.1ovaau5sxunp2cv8rcy88688v. Accessed 22 Jan 2019.
Collins R. What makes UK Biobank special? Lancet. 2012;379:1173–4.
Davis KAS, Coleman JRI, Adams M, Allen N, Breen G, Cullen B, et al. Mental health in UK Biobank - development, implementation and results from an online questionnaire completed by 157 366 participants: a reanalysis. BJPsych Open. 2020;6:e18.
Bycroft C, Freeman C, Petkova D, Band G, Elliott LT, Sharp K, et al. The UK Biobank resource with deep phenotyping and genomic data. Nature. 2018;562:203–9.
Burgess S, Davies NM, Thompson SG. Bias due to participant overlap in two-sample Mendelian randomization. Genet Epidemiol. 2016;40:597–608.
Fraser A, Macdonald-Wallis C, Tilling K, Boyd A, Golding J, Davey Smith G, et al. Cohort profile: the Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int J Epidemiol. 2013;42:97–110.
Boyd A, Golding J, Macleod J, Lawlor DA, Fraser A, Henderson J, et al. Cohort Profile: the ‘children of the 90s’--the index offspring of the Avon Longitudinal Study of Parents and Children. Int J Epidemiol. 2013;42:111–27.
Richmond RC, Timpson NJ, Felix JF, Palmer T, Gaillard R, McMahon G, et al. Using genetic variation to explore the causal effect of maternal pregnancy adiposity on future offspring adiposity: a Mendelian randomisation study. PLoS Med. 2017;14:e1002221.
Blair PS, Drewett RF, Emmett PM, Ness A, Emond AM. Family, socioeconomic and prenatal factors associated with failure to thrive in the Avon Longitudinal Study of Parents and Children (ALSPAC). Int J Epidemiol. 2004;33:839–47.
Wright J, Small N, Raynor P, Tuffnell D, Bhopal R, Cameron N, et al. Cohort Profile: the Born in Bradford multi-ethnic family cohort study. Int J Epidemiol. 2013;42:978–91.
Magnus P, Birke C, Vejrup K, Haugan A, Alsaker E, Daltveit AK, et al. Cohort Profile Update: The Norwegian Mother and Child Cohort Study (MoBa). Int J Epidemiol. 2016;45:382–8.
Paltiel L, Anita H, Skjerden T, Harbak K, Bækken S, Kristin SN, et al. The biobank of the Norwegian Mother and Child Cohort Study – present status. Nor J Epidemiol. 2014;24:29–35.
Magnus MC, Miliku K, Bauer A, Engel SM, Felix JF, Jaddoe VWV, et al. Vitamin D and risk of pregnancy related hypertensive disorders: mendelian randomisation study. BMJ. 2018;361:k2167.
Kurki M, Karjalainen K, Palta P, Sipila T, Kristiansson K, Donner K, et al. FinnGen: Unique genetic insights from combining isolated population and national health register data. medRiv. 2022. https://doi.org/10.1101/2022.03.03.22271360.
Kiiskinen T, Mars NJ, Palviainen T, Koskela J, Rämö JT, Ripatti P, et al. Genomic prediction of alcohol-related morbidity and mortality. Transl Psychiatry. 2020;10:23.
Zhou W, Zhao Z, Nielsen JB, Fritsche LG, LeFaive J, Gagliano Taliun SA, et al. Scalable generalized linear mixed model for region-based association tests in large biobanks and cohorts. Nat Genet. 2020;52:634–9.
Garfield V. Sleep duration: a review of genome-wide association studies (GWAS) in adults from 2007 to 2020. Sleep Med Rev. 2020;56:101413.
Jansen PR, Watanabe K, Stringer S, Skene N, Bryois J, Hammerschlag AR, et al. Genome-wide analysis of insomnia in 1,331,010 individuals identifies new risk loci and functional pathways. Nat Genet. 2019;51:394–403.
Lane JM, Liang J, Vlasac I, Anderson SG, Bechtold DA, Bowden J, et al. Genome-wide association analyses of sleep disturbance traits identify new loci and highlight shared genetics with neuropsychiatric and metabolic traits. Nat Genet. 2017;49:274–81.
Jones SE, Tyrrell J, Wood AR, Beaumont RN, Ruth KS, Tuke MA, et al. Genome-wide association analyses in 128,266 individuals identifies new morningness and sleep duration loci. PLoS Genet. 2016;12:e1006125.
Scheinfeldt LB, Gharani N, Kasper RS, Schmidlen TJ, Gordon ES, Jarvis JP, et al. Using the Coriell Personalized Medicine Collaborative Data to conduct a genome-wide association study of sleep duration. Am J Med Genet B Neuropsychiatr Genet. 2015;168:697–705.
Gottlieb DJ, Hek K, Chen TH, Watson NF, Eiriksdottir G, Byrne EM, et al. Novel loci associated with usual sleep duration: the CHARGE Consortium Genome-Wide Association Study. Mol Psychiatry. 2015;20:1232–9.
Ollila HM, Kettunen J, Pietiläinen O, Aho V, Silander K, Kronholm E, et al. Genome-wide association study of sleep duration in the Finnish population. J Sleep Res. 2014;23:609–18.
Byrne EM, Gehrman PR, Medland SE, Nyholt DR, Heath AC, Madden PA, et al. A genome-wide association study of sleep habits and insomnia. Am J Med Genet B Neuropsychiatr Genet. 2013;162B:439–51.
Allebrandt KV, Amin N, Müller-Myhsok B, Esko T, Teder-Laving M, Azevedo RV, et al. A K(ATP) channel gene effect on sleep duration: from genome-wide association studies to function in Drosophila. Mol Psychiatry. 2013;18:122–32.
Gottlieb DJ, O'Connor GT, Wilk JB. Genome-wide association of sleep and circadian phenotypes. BMC Med Genet. 2007;8(Suppl 1):S9.
Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408.
Hartwig FP, Davies NM. Why internal weights should be avoided (not only) in MR-Egger regression. Int J Epidemiol. 2016;45:1676–8.
Burgess S, Small DS, Thompson SG. A review of instrumental variable estimators for Mendelian randomization. Stat Methods Med Res. 2017;26:2333–55.
Sun YQ, Burgess S, Staley JR, Wood AM, Bell S, Kaptoge SK, et al. Body mass index and all cause mortality in HUNT and UK Biobank studies: linear and non-linear mendelian randomisation analyses. BMJ. 2019;364:l1042.
Palmer TM, Sterne JA, Harbord RM, Lawlor DA, Sheehan NA, Meng S, et al. Instrumental variable estimation of causal risk ratios and causal odds ratios in Mendelian randomization analyses. Am J Epidemiol. 2011;173:1392–403.
Lawson DJ, Davies NM, Haworth S, Ashraf B, Howe L, Crawford A, et al. Is population structure in the genetic biobank era irrelevant, a challenge, or an opportunity. Hum Genet. 2020;139:23–41.
Lawlor DA. Commentary: Two-sample Mendelian randomization: opportunities and challenges. Int J Epidemiol. 2016;45:908–15.
Burgess S, Dudbridge F, Thompson SG. Combining information on multiple instrumental variables in Mendelian randomization: comparison of allele score and summarized data methods. Stat Med. 2016;35:1880–906.
Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40:304–14.
Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44:512–25.
Hemani G, Bowden J, Davey SG. Evaluating the potential role of pleiotropy in Mendelian randomization studies. Hum Mol Genet. 2018;27:R195–r208.
Yang Q, Sanderson E, Tilling K, Borges MC, Lawlor DA. Exploring and mitigating potential bias when genetic instrumental variables are associated with multiple non-exposure traits in Mendelian randomization. Eur J Epidemiol. 2022. https://doi.org/10.1007/s10654-022-00874-5.
Lawlor D, Richmond R, Warrington N, McMahon G, Davey Smith G, Bowden J, et al. Using Mendelian randomization to determine causal effects of maternal pregnancy (intrauterine) exposures on offspring outcomes: sources of bias and methods for assessing them. Wellcome Open Res. 2017;2:11.
Lupattelli A, Wood ME, Nordeng H. Analyzing missing data in perinatal pharmacoepidemiology research: methodological considerations to limit the risk of bias. Clin Ther. 2019;41:2477–87.
Lee KJ, Tilling KM, Cornish RP, Little RJA, Bell ML, Goetghebeur E, et al. Framework for the treatment and reporting of missing data in observational studies: The Treatment And Reporting of Missing data in Observational Studies framework. J Clin Epidemiol. 2021;134:79–88.
Hughes RA, Heron J, Sterne JAC, Tilling K. Accounting for missing data in statistical analyses: multiple imputation is not always the answer. Int J Epidemiol. 2019;48:1294–304.
Rubin DB. Multiple imputation for nonresponse in surveys. New York: Wiley; 2004.
Sivertsen B, Hysing M, Dørheim SK, Eberhard-Gran M. Trajectories of maternal sleep problems before and after childbirth: a longitudinal population-based study. BMC Pregnancy Childbirth. 2015;15:129.
Bond TA, Richmond RC, Karhunen V, Cuellar-Partida G, Borges MC, Zuber V, et al. Exploring the causal effect of maternal pregnancy adiposity on offspring adiposity: Mendelian randomisation using polygenic risk scores. BMC Med. 2022;20:34.
Hernáez Á, Rogne T, Skåra KH, Håberg SE, Page CM, Fraser A, et al. Body mass index and subfertility: multivariable regression and Mendelian randomization analyses in the Norwegian Mother, Father and Child Cohort Study. Hum Reprod. 2021;36:3141–51.
Lawlor DA, Tilling K, Davey SG. Triangulation in aetiological epidemiology. Int J Epidemiol. 2016;45:1866–86.
Ye Z, Kappelmann N, Moser S, Davey Smith G, Burgess S, Jones PB, et al. Role of inflammation in depression and anxiety: tests for disorder specificity, linearity and potential causality of association in the UK Biobank. EClinicalMedicine. 2021;38:100992.
Farrar D, Simmonds M, Bryant M, Sheldon TA, Tuffnell D, Golder S, et al. Hyperglycaemia and risk of adverse perinatal outcomes: systematic review and meta-analysis. Bmj. 2016;354:i4694.
Tyrrell J, Richmond RC, Palmer TM, Feenstra B, Rangarajan J, Metrustry S, et al. Genetic evidence for causal relationships between maternal obesity-related traits and birth weight. Jama. 2016;315:1129–40.
Ernst GD, de Jonge LL, Hofman A, Lindemans J, Russcher H, Steegers EA, et al. C-reactive protein levels in early pregnancy, fetal growth patterns, and the risk for neonatal complications: the Generation R Study. Am J Obstet Gynecol. 2011;205(132):e1–12.
Kamat MA, Blackshaw JA, Young R, Surendran P, Burgess S, Danesh J, et al. PhenoScanner V2: an expanded tool for searching human genotype-phenotype associations. Bioinformatics. 2019;35:4851–3.
Labrecque J, Swanson SA. Understanding the assumptions underlying instrumental variable analyses: a brief review of falsification strategies and related tools. Curr Epidemiol Rep. 2018;5:214–20.
Hughes RA, Davies NM, Davey Smith G, Tilling K. Selection bias when estimating average treatment effects using one-sample instrumental variable analysis. Epidemiology. 2019;30:350–7.
Munafò MR, Tilling K, Taylor AE, Evans DM, Davey SG. Collider scope: when selection bias can substantially influence observed associations. Int J Epidemiol. 2018;47:226–35.
Paternoster L, Tilling K, Davey SG. Genetic epidemiology and Mendelian randomization for informing disease therapeutics: conceptual and methodological challenges. PLoS Genet. 2017;13:e1006944.
Fry A, Littlejohns TJ, Sudlow C, Doherty N, Adamska L, Sprosen T, et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. Am J Epidemiol. 2017;186:1026–34.
Adams MJ, Hill WD, Howard DM, Dashti HS, Davis KAS, Campbell A, et al. Factors associated with sharing e-mail information and mental health survey participation in large population cohorts. Int J Epidemiol. 2020;49:410–21.
Pierce BL, VanderWeele TJ. The effect of non-differential measurement error on bias, precision and power in Mendelian randomization studies. Int J Epidemiol. 2012;41:1383–93.
Hutcheon JA, Chiolero A, Hanley JA. Random measurement error and regression dilution bias. BMJ. 2010;340:c2289.
Acknowledgements
This research has been conducted using the UKB Resources under application number 23938. The authors would like to thank the participants and researchers from UKB who contributed or collected data. We are extremely grateful to all the families who took part in ALSPAC, the midwives for their help in recruiting them and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. BiB is only possible because of the enthusiasm and commitment of the children and parents in BiB. We are grateful to all the participants, teachers, school staff, health professionals and researchers who have made BiB happen. This research has been conducted using MoBa data using application number 2552. MoBa is supported by the Norwegian Ministry of Health and Care services and the Ministry of Education and Research. We are grateful to all the participating families in Norway who take part in this on-going cohort study. We thank the Norwegian Institute of Public Health (NIPH) for generating high-quality genomic data. This research is part of the HARVEST collaboration, supported by the Research Council of Norway (#229624). We also thank the NORMENT Centre for providing genotype data, funded by the Research Council of Norway (#223273), South East Norway Health Authority and KG Jebsen Stiftelsen. We further thank the Center for Diabetes Research, the University of Bergen, for providing genotype data and performing quality control and imputation of the data funded by the ERC AdG project SELECTionPREDISPOSED, Stiftelsen Kristian Gerhard Jebsen, Trond Mohn Foundation, the Research Council of Norway, the Novo Nordisk Foundation, the University of Bergen and the Western Norway health Authorities (Helse Vest). The authors thank FinnGen investigators for sharing their summary-level data.
Funding
This work was supported by the University of Bristol and UK Medical Research Council (MM_UU_00011/1, MM_UU_00011/3 and MM_UU_00011/6), the US National Institute for Health (R01 DK10324), the European Research Council via Advanced Grant 669545, the British Heart Foundation (AA/18/7/34219 and CS/16/4/32482) and the National Institute of Health Research Bristol Biomedical Research Centre at University Hospitals Bristol NHS Foundation Trust and the University of Bristol. QY is funded by a China Scholarship Council PhD Scholarship (CSC201808060273). MCB was funded by a UK Medical Research Council Skills Development Fellowship (MR/P014054/1) and a University of Bristol Vice Chancellor Fellowship during her contribution to this research. MCM has received funding from the European Research Council under the European Union’s Horizon 2020 research and innovation programme (grant agreement No 947684). MCM and SEH are partly funded by the Research Council of Norway (project No 320656) through its Centres of Excellence funding scheme (project No 262700). AGS is supported by the study of Dynamic longitudinal exposome trajectories in cardiovascular and metabolic non-communicable diseases (H2020-SC1-2019-Single-Stage-RTD, project ID 874739). DAL is a British Heart Foundation Chair (CH/F/20/90003) and a National Institute of Health Research Senior Investigator (NF-0616-10102).
The UK Medical Research Council and Wellcome (Grant ref: 217065/Z/19/Z) and the University of Bristol provide core support for ALSPAC. This publication is the work of the authors and DAL will serve as guarantor for the contents of this paper. A comprehensive list of grant funding is available on the ALSPAC website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf). ALSPAC was specifically funded by Wellcome Trust (WT088806), and child’s GWAS data was generated by Sample Logistics and Genotyping Facilities at Wellcome Sanger Institute and LabCorp (Laboratory Corporation of America) using support from 23andMe. BiB is supported by a Wellcome programme grant (WT223601/Z/21/Z: Age of Wonder), an infrastructure grant (WT101597MA), a UK Medical and Economic and Social Science Research Councils programme grant (MR/N024397/1), a British Heart Foundation Clinical Study grant (CS/16/4/32482) and the National Institute of Health Research under its Applied Research Collaboration for Yorkshire and Humber (NIHR200166). Further support for genome-wide and multiple ‘omics measurements in BiB is from the UK Medical Research Council (G0600705), National Institute of Health Research (NF-SI-0611-10196), US National Institute of Health (R01DK10324) and the European Research Council under the European Union’s Seventh Framework Programme (FP7/2007–2013) / ERC grant agreement no 669545. The funders had no role in the design of the study; the collection, analysis or interpretation of the data; the writing of the manuscript; or the decision to submit the manuscript for publication. The views expressed in this paper are those of the authors and not necessarily those of any funder.
Author information
Authors and Affiliations
Contributions
DAL conceived the study idea. QY, ES, KT and MCB developed this idea. QY, ES, DAL, KT and MCB developed the analysis plan, and QY undertook all analyses with supervision from ES, DAL, KT and MCB. MCM, FK, GS, AGS, JWe, PM, JWr and SEH managed data curation for the individual participant data used in this study. QY wrote the first draft of the paper, with all other authors interpreting the results and making important critical revisions. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for UKB was obtained from the North West Multi-centre Research Ethics Committee. Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Consent for biological samples has been collected in accordance with the Human Tissue Act (2004). Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendation of the ALSPAC Ethics and Law Committee at the time. Ethical approval for BiB was obtained from the Bradford Research Ethics Committee. The establishment of MoBa and initial data collection was based on a license from the Norwegian Data Protection Agency and approval from The Regional Committees for Medical and Health Research Ethics. The MoBa cohort is now based on regulations related to the Norwegian Health Registry Act. The current study was approved by The Regional Committees for Medical and Health Research Ethics. The Coordinating Ethics Committee of the Helsinki and Uusimaa Hospital District has approved the FinnGen consortium (Nr HUS/990/2017), and this study used its summary level data.
Consent for publication
Not applicable.
Competing interests
KT has acted as a consultant for CHDI Foundation, and Expert Witness to the High Court in England, called by the UK Medicines and Healthcare products Regulatory Agency, defendants in a case on hormonal pregnancy tests and congenital anomalies 2021/22. DAL is an editorial advisor for BMC Medicine and has received support from Medtronic LTD and Roche Diagnostics for biomarker research that is not related to the study presented in this paper. The other authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
. Results extracted from recent systematic reviews. Table S2. Key characteristics of GWAS of self-report sleep duration. Table S3. SNP list and female-specific effect estimates of sleep duration SNPs identified in UK Biobank. Table S4. Definitions of outcomes. Table S5. Details of UKB women by sleep duration groups in one-sample MR. Table S6. Characteristics of the women in MoBa by sleep duration categories. Table S7. Associations of 78 SNPs with sleep duration and with outcomes in UKB, ALSPAC, BiB, and MoBa. Table S8. Two-sample MR estimates for causal effects of sleep duration on the outcomes. Table S9. MVreg associations of self-reported sleep duration categories with the outcomes in MoBa.
Additional file 2: Text S1
. Descriptions of each cohort. Text S2. Technical considerations of one-sample MR to explore potential nonlinear effects. Fig S1. Flow chart. Fig S2. Histogram of residual sleep duration in UKB women. Fig S3. One-sample MR estimates of effects of sleep duration on the outcomes in UKB women. Fig S4. Associations of 78 SNPs with the outcomes with versus without adjustments of fetal genotypes. Fig S5. Leave-one-out analyses in UKB (datasets A on B). Fig S6. Leave-one-out analyses in UKB (datasets B on A). Fig S7. Leave-one-out analyses in other cohorts. Fig S8. Two-sample MR associations of sleep duration with the outcomes using IVW. Fig S9. Comparing MVreg associations of sleep duration categories with odds of low/high birthweight using different outcome comparison groups.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, Q., Magnus, M.C., Kilpi, F. et al. Investigating causal relations between sleep duration and risks of adverse pregnancy and perinatal outcomes: linear and nonlinear Mendelian randomization analyses. BMC Med 20, 295 (2022). https://doi.org/10.1186/s12916-022-02494-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-022-02494-y