
Abstract
Background
Translation into practice of effective physical activity interventions in primary care is difficult, due to a complex interaction of implementation determinants. We aimed to identify implementation barriers and facilitators of four primary care interventions: physical activity assessment, counselling, prescription, and referral.
Methods
A systematic review of qualitative, quantitative and mixed-methods studies published since 2016 was conducted. The “Tailored Implementation for Chronic Diseases” (TICD) framework was adapted to extract and synthesize barriers and facilitators.
Results
Sixty-two studies met the inclusion criteria. Barriers (n = 56) and facilitators (n = 55) were identified across seven domains, related to characteristics of the intervention, individual factors of the implementers and receivers, organizational factors, and political and social determinants. The five most frequently reported determinants were: professionals’ knowledge and skills; intervention feasibility/compatibility with primary health care routine; interventions’ cost and financial incentives; tools and materials; and professionals’ cognitions and attitudes. “Social, political and legal factors” domain was the least reported. Physical activity counselling, prescription, and referral were influenced by determinants belonging to all the seven domains.
Conclusion
The implementation of physical activity interventions in primary care is influenced by a broader range of determinants. Barriers and facilitators related with health professionals, intervention characteristics, and available resources were the most frequently reported. A deep understanding of the local context, with particularly emphasis on these determinants, should be considered when preparing an intervention implementation, in order to contribute for designing tailored implementation strategies and optimize the interventions’ effectiveness.
Similar content being viewed by others


Background
The importance of maintaining regular physical activity (PA) is well established both for preventive care [1] and as a therapeutic adjuvant [2], in several chronic conditions. However, worldwide physical inactivity prevalence remains high [3,4,5].
The critical role of health systems in the promotion of PA as a way of tackling non-communicable diseases has been highlighted by the World Health Organization (WHO) during the last decade [6] with primary health care services gaining more relevance particularly since 2016 [7, 8]. More recently, the WHO Global Action Plan for PA Promotion 2018–2030 [9] has established the development of PA promotion systems within health care services – directed at patients and implemented by appropriately trained health professionals – as a priority action. A toolkit specifically designed to primary care [10] has since been created, encompassing strategies developed to support countries implementing and strengthening systems of patients’ PA assessment and counselling, as part of universal health care. Despite efforts made, only 40% of countries reported having a national protocol in this regard in 2021 [3].
Several types of primary care intervention models have been developed. They can be grouped in four major intervention types [10]: i. PA screening/assessment, which corresponds to a systematic application of an enquiry to identify patients’ levels of PA and sedentary behaviour [10, 11]; ii. PA brief counselling/advice, comprising a verbal encouragement and/or a verbal or written recommendation for PA, performed by a professional during routine care, also involving an approach to motivations, barriers, preferences, readiness, patient's health, and opportunities to perform PA [10, 12, 13]; iii. exercise prescription, comprising an initial assessment of the patients’ physical and functional fitness, body composition, past PA and clinical history, and goals/motivations, followed by a detailed selection and explanation of exercises according to the patients’ initial assessment, and also including a systematic monitoring and evaluation of effects [12]; and iv. exercise referral scheme, made by a primary care professional to a third-party service, which is responsible to prescribe a tailored PA/exercise program to the patient [10, 13,14,15]. These intervention types can be implemented individually or in combination.
Previous research evaluating these interventions has revealed clinically relevant increases in patients’ PA levels [16,17,18,19,20]. However, studies assessing interventions’ external validity, when implemented in real-world settings and integrated in primary health care assistance activities, are lacking, limiting the generalizability of such results [20]. The current research-to-practice evidence gap highlights the importance of addressing contextual determinants (barriers and facilitators) to generate evidence for implementation strategies, thus contributing for the translation of evidence-based interventions into healthcare practice [13, 21,22,23].
Key determinants of healthcare practice may be related to environmental (e.g., socio-political and legal factors) or organizational characteristics (e.g., decision-making processes, capacity for organizational change, and the existence or absence of resources and incentives), but also with characteristics of implementers, receivers, and/or the intervention itself. These determinants have been systematized through different checklists, frameworks, taxonomies, and classification systems [24,25,26,27,28,29]. Based on these, a comprehensive and integrated checklist of determinants was specifically developed for healthcare professional practice – the “Tailored Implementation for Chronic Diseases” (TICD) checklist [30], to optimize reflection and data collection on determinants of implementation. When introducing quality improvements or new interventions in healthcare, a proper investigation of implementation barriers and facilitators is critical to reveal the most relevant intervention- and context-specific ones, aiming at the development of tailored implementation strategies and more effective interventions [30].
There is a limited number of systematic reviews aimed at reporting implementation barriers and facilitators of PA interventions [31]. Some have focused in the primary health care system, but have not included PA-only interventions alone (considering weight management programs and lifestyle interventions, for instance), and were limited to analysing stakeholders’ views [32] or health professionals’ determinants and views [33,34,35], and/or considered a single PA intervention type [19, 35]. Thus, there is a need for systematic identification of whole-system implementation barriers and facilitators of the most common PA-specific promotion interventions implemented in primary care.
This systematic review aimed to identify implementation barriers and facilitators, according to the TICD framework, within the four described PA promotion interventions delivered in primary health care settings by health professionals to adult patients.
Methods
This systematic review was reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 statement [36] (see Additional file 1).
Eligibility criteria
We included peer-reviewed studies published since January 2016, the publication year of both the “Physical activity strategy for the WHO European Region 2016–2025” [7] and the guide “Integrating diet, physical activity and weight management services into primary care” [8]. Although there are studies on this topic published before this year, constant changes in health care systems, scientific knowledge, and population health pattern might make older studies not representative of today’s reality. Furthermore, 2016 marked a stronger and more focused WHO’s recommendation of PA promotion interventions in primary health care. Therefore, only studies published since 2016 were considered. We considered studies with primary care health professionals, patients (≥ 18 years), and stakeholders involved in one of the four types of PA promotion and/or sedentary time reduction interventions (i.e., PA assessment, counselling, prescription and/or referral), delivered in primary health care settings, at least in part, face-to-face. Included studies should formally assess interventions’ implementation barriers and facilitators. Several types of study design were included (i.e., qualitative, quantitative or mixed-methods).
Studies including rehabilitation patients, or patients with contraindications to perform PA autonomously, those testing interventions not specifically targeting PA promotion alone (e.g., lifestyle interventions, weight management interventions, etc.) or digital-only interventions, study protocols, literature reviews, opinion articles, conference books or papers, non-peer reviewed scientific literature (e.g., books, book chapters), and non-English or Portuguese written literature were excluded.
Information sources
A systematic literature search for titles and abstracts was conducted in five electronic databases: Web of Science, Scopus, PsycInfo, PubMed, and Medline. Databases were last searched in July 12th, 2023.
Search strategy
The search strategy comprised a combination of terms from four different categories: behaviours of interest, interventions of interest, implementation context, and review’s main outcomes (i.e., implementation determinants). The full search stem can be found in Additional file 2.
Selection and data collection processes
Two reviewers (CSS and JE) independently screened titles and abstracts and three reviewers (CSS, JE, and BR) independently analysed full text articles against eligibility criteria. A consistency check between the authors was performed in 15% of randomly selected titles and abstracts and in 20% of randomly selected full-texts to obtain inter-reviewer agreement (Cohen’s kappa and Fleiss’ kappa, respectively). Authors were blind to each other’s decisions and, given that good to excellent agreement was found in their assessments (Cohen k = 1; Fleiss’ k = 0.615), they independently screened the other 85% of titles and abstracts and 80% of full text articles. Disagreements between individual decisions were discussed to reach consensus. CADIMA® online software was used to record decisions on title and abstract screening and full text analysis. When full text articles were unavailable, authors were contacted and readily made their work available in all cases. Three reviewers (CSS, JE, and BR) independently extracted data. An excel spreadsheet was used to record extracted data. TICD framework categories [30] were used to guide data extraction.
Data items
Extracted data comprised the following outcome items of significance to the review objectives: guideline factors; individual health professional factors; patient factors; professional interactions; incentives and resources; capacity for organizational change; social, political, and legal factors; and any other factor assessed as a barrier and/or facilitator of implementation of the interventions of interest. Relevant statistical data on the outcomes of interest was also extracted, when applicable, as an indicator of its relevance. Other study information was also extracted: author; year; country of implementation; type of study; methodology; trial (if applicable); intervention; outcome; and participants’ characteristics (number of participants; health professional or stakeholder category or if the sample consisted of patients; mean age; sex distribution; patients’ chronic diseases, if applicable).
Study quality assessment
Two authors (CSS and JE) independently performed a critical appraisal of all articles included in the review. A consistency check between the two authors was performed in 15% of randomly selected studies, having obtained a good inter-reviewer agreement (Cohen’s k = 0.653). Joanna Brigs Institute (JBI) critical appraisal tools [37] were used to assess studies’ quality. For studies using a mixed-methods methodology, the Mixed-Methods Appraisal Tool (MMAT) [38] was applied, as there is no specific JBI tool for mixed-methods studies. The critical appraisal assessment is presented for each study against each checklist item, in table format [39].
Synthesis methods
As this systematic review includes very different studies and its output is qualitative, a narrative synthesis was performed. First, a preliminary synthesis was made using a thematic analysis approach [40], based on the TICD framework, and studies’ results were presented in tabular form, structured into the framework’s main themes/domains, barriers vs. facilitators, and type of PA promotion intervention. Then, a frequency table of the studies mentioning each kind of implementation barrier and facilitator was made. Last, the studies and their results were presented and relationships in the data were explored, to better interpret the facilitators and barriers of each type of PA promotion intervention. This allowed to understand the different implementation determinants in an articulated, integrated, and systematic way.
Certainty assessment of the systematic review
The Supporting the Use of Research Evidence (SURE) checklist was used, to evaluate the identification, selection and appraisal of studies (5 criteria), how findings were analysed (5 criteria), and to reflect on other considerations (one criterion) [41].
Results
Study selection
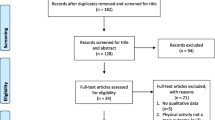
The search strategy identified a total of 4508 records (see Fig. 1). After duplicates removal and title and abstract screening, the full-text of 187 records were assessed for eligibility. After exclusion of 125 records for not meeting inclusion criteria, a total of 62 articles were included in this review [42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103].

PRISMA flowchart
Study characteristics
From the 62 articles included, 48.4% (n = 30) employed a qualitative design [43, 46, 48, 49, 54, 55, 58, 60, 62, 65, 67, 68, 71, 76,77,78,79,80, 83, 84, 87,88,89, 92,93,94,95,96,97, 99], 37.1% (n = 23) a quantitative design [42, 44, 45, 52, 53, 57, 61, 63, 64, 66, 69, 72,73,74,75, 81, 82, 85, 91, 98, 100,101,102], and 14.5% (n = 9) a mixed-methods study design [47, 50, 51, 56, 59, 70, 86, 90, 103]. The majority of the studies (87.1%) were conducted in high income countries (United Kingdom, n = 15; Canada, n = 9; USA, n = 7; other countries, n = 23), while only 12.9% were conducted in upper middle income countries (Brazil, n = 4; Thailand, n = 2; Jordan, n = 1; Turkey, n = 1), according to the categorization of the World Bank [104]. Study characteristics are outlined in Table 1.
Quality assessment of the studies is reported in Additional file 3. The main issues found in qualitative studies were the lack of a clear statement of the authors’ philosophical perspective, not addressing researcher’s cultural and theoretical location, as well as researcher-research influence. In mixed-methods studies, the main issue was the non-accomplishment of quality criteria for both study components (qualitative and quantitative). In analytical cross-sectional studies, the main issue was related to the validity and reliability of the instruments used. In prevalence studies, it was unclear whether health conditions were identified using validated methods, and there were also issues related with insufficient coverage of sample subgroups in data analysis. In quasi-experimental studies, the main issues were related to the absence of an independent control group and of a description and analysis of differences between groups at follow-up. As for the analysed randomized controlled trial, the only not fulfilled quality criteria was participants’ blinding.
Barriers and facilitators to implementation of physical activity interventions in primary care
A total of 56 barriers and 55 facilitators to implementation were identified across the seven domains/themes. A supporting codebook, based on TICD framework [30], is available in Additional file 4 and a full list of these implementation determinants is organized in Table 2. Detailed data extraction information is available in Additional file 5.
Intervention/guideline factors
“(Lack of) feasibility/compatibility” and “intervention components/characteristics/content” were the most reported determinants within this domain.
The absence of feasibility/compatibility of PA interventions’ implementation within health professionals’ usual tasks and activities was a key highlighted barrier. Extended time was emphasized as a requirement to implement interventions regularly, while simultaneously addressing the primary reason for the patient’s visit and parallel professional demands and responsibilities. PA interventions requiring a more structured local organization (e.g., a specific PA consultation) were also associated to complex logistics (e.g., specific space, more time needed), more difficult to accommodate. Some studies [46, 58, 88] reported ways by which increasing feasibility/compatibility of the intervention would be a facilitator, for instance, transferring the implementation responsibility to health care professionals who have more consultation time (as dietitians or nurse practitioners).
Some “intervention components/characteristics/content” were reported as key facilitators, namely goal setting, action planning, self-monitoring and social support components. Interventions incorporating written prescriptions and regular follow-ups were also seen as facilitators, both by health care professionals and patients. On the other hand, complex methods requiring extensive knowledge by implementers and intervention activities considered chores by the patients (e.g., PA diaries) exemplify the barriers reported in primary studies.
Other intervention/guideline factors were less studied or reported. Evidence is suggestive of the potential facilitator role of “tailored intervention/patient-centred” and “recruitment strategy” used.
Individual health professional factors
“Knowledge and skills”, “cognitions/attitudes”, and “professional behaviour” were the most highlighted determinants within this domain.
Health professional’s “knowledge and skills” to promote PA was the most frequently reported/studied determinant, both as barrier and facilitator (50 times in 62 studies). The lack of training or expertise in the area of PA and behaviour change techniques, unfamiliarity with guidelines, lack of knowledge on safety issues concerning PA practice by people with chronic conditions, and unfamiliarity with suitable PA opportunities in the community illustrate the barriers highlighted by the studies’ participants. Receiving training in medical school about PA promotion, training the health care teams working in health surgeries, especially regarding PA promotion in chronically ill patients and in behaviour change techniques, and attending local activities with information about local PA offers were examples of reported facilitators.
Health professionals’ “cognitions and attitudes” were also reported both as barriers and as facilitators. Health professionals’ belief that PA is not a relevant and/or effective prevention strategy or treatment, giving it a low priority or finding other lifestyle changes more important, was reported in several studies as barriers. Having a good attitude towards PA promotion, an increased understanding of the importance of PA promotion in healthcare, perception of no barriers to counselling, and considering PA as an important behaviour for good health were in turn emphasised by health professionals as implementation facilitators.
Although less reported than the previous, “professional behaviour” was also frequently reported, especially as a facilitator. For instance, patients appreciated trustworthy, supportive, and non-judgmental advice by genuinely interested health professionals. A previous assessment of PA levels and patients’ readiness to change facilitated the implementation of PA counselling and prescription, according to health professionals. Feeling that patients’ PA promotion is outside their professional “scope of practice/professional role”, or that it is a role shared by all healthcare professionals and not exclusively by themselves was the third most highlighted barrier.
Patient factors
“Motivation” and “health status” were the two most frequently reported patient-related determinants, being considered both as barrier and facilitator.
Health care professionals perceiving lack of “motivation” by their patients was referred as a key barrier. From the patients’ view, no interest in receiving PA counselling was reported, for instance, when they felt they were already sufficiently active or when they already had pre-existing conditions requiring regular contact with health services and did not desire further testing. On the other hand, patients’ perception of PA positive effects on health, the social recognition and feelings of enjoyment derived from PA practice, contributed to their motivation, working as a facilitator.
Patients’ “health status”, namely some comorbidities, prevent patients to fully engage in the intervention, while in other cases, the “perceived threat” (e.g., type 2 diabetes) was not sufficient to mobilize change. For health professionals, patients’ illnesses, and the implementation of treatments other than PA competed for attention. Specifically, for some diseases, such as cancer, a significantly low proportion of health professionals recommended PA. On the other hand, health professionals were more likely to recommend PA to patients with overweight or obesity, type 2 diabetes or pre-diabetes, dyslipidaemia, and hypertension.
Although less studied/reported, two other determinants gathered evidence of relevance, as they were the second most reported barriers within this theme: health professionals perceived “lack of compliance/engagement” by patients and frustration of patients’ “expectations” (e.g., health professionals felt that some patients expected drug treatment instead of exercise, whereas other patients felt that the program was missing more intense exercise training options).
Professional interactions
Professional interactions were mainly reported as facilitators. “Team processes” and “networks” were the two most relevant, playing a key facilitating role in implementation.
Highlighted positive “team processes” were mainly related with a good cooperation between PA counsellors and health care professionals, or with a good functioning dynamic of the family health teams.
Another key facilitator was “networks”. Health professionals stressed the importance of a connection between sectors, which may result in increased referral of patients, and the importance of involving all stakeholders in a shared mission.
Although less studied/reported, “team communication (constraints)” and “referral processes (constraints)” were the third most reported determinants.
Incentives and resources
“(Cost and lack of) financial incentives” and “assistance tools and materials” were the most frequently highlighted determinants, both as barriers and as facilitators.
“Cost and lack of financial incentives” was often felt as a barrier. Patients and health professionals frequently reported expensive memberships in PA facilities for patients. Health professionals also highlighted the lack of financial reimbursements to implementers. Indeed, health professionals’ reimbursements of PA prescriptions and economic subsidies for patients to reduce the cost of joining an exercise facility, or even having a trial period before membership, were often reported as a “financial incentives” facilitator.
Regarding “assistance tools and materials” constraints, health professionals often highlighted lack of instructional material and effective tools and educational information to give to patients. On the other hand, the availability of specific intervention support tools and materials (e.g., practitioner toolbox; standardized and up-to-date information about where to refer patients, as a "community mapping” including PA facilities within the geographical area; decision algorithms) were believed to facilitate the implementation process, with technological tools being especially welcomed by health professionals.
Indeed, the “information system” was mainly reported as facilitator. Health professionals welcomed procedures’ digitalization to reduce time and money, namely through the integration of PA promotion tools in the electronic health system, as referral forms, prescription pads, and modules for PA counselling, for instance. Having access to patients’ interdisciplinary health care charts was also reported by health professionals to support tailored counselling.
Providing a “continuing education system” offer for health care staff (e.g., regarding PA promotion, its pathways and modes of delivery) was also highlighted as a relevant facilitator.
Capacity for organizational change
“Capable leadership” was the most frequently reported implementation determinant. Health professionals and stakeholders identified the election of a formal coordinator/leader, regularly present in the working group and providing support and updated information/knowledge sharing to the implementation team, as an implementation facilitating factor. Managers’ championing and endorsement of the intervention was also emphasized. Cases where the primary care management was not explicitly fulfilling this role hindered the implementation.
Other determinants within this theme were less studied.
Social, political and legal factors
Determinants within this domain were the least studied/reported. “(Lack of) funder policies” and “(economic constraints on the) health care budget” were reported in five studies, both as barriers and facilitators.
Implementation determinants’ themes according to primary care physical activity intervention type
Table 3 provides a summary of the implementation determinants (main themes) reported in each intervention type.
Three interventions – PA counselling; PA prescription; PA referral schemes – and one combination – PA counselling and referral – gathered implementation barriers and facilitators from all domains, whereas those involving PA assessment seemed to be more influenced by determinants pertaining to intervention/guideline-, deliverers-, and patient-related factors. Intervention/guideline factors and individual health professional factors were reported in all intervention types and combinations, proving to be key determinants to consider when implementing PA interventions in primary healthcare. Patient factors and incentives and resources’ barriers and facilitators were also central to implementation, being reported in the four intervention types. Professional interactions, capacity for organizational change, and social, political, and legal factors did not seem to be considered pivotal in implementation processes of simpler interventions, as PA assessment alone. These groups of determinants played a more relevant role in interventions with more complexity, requiring further delivering resources, as PA counselling, PA prescription, and those involving referral processes.
Considering the reporting frequency of the main themes by each intervention type, PA counselling implementation seems to be mainly hindered by factors related to the intervention/guideline, individual health professionals and patients, and mainly facilitated by individual health professional factors. PA prescription implementation seems to be particularly influenced by barriers and facilitators pertaining incentives and resources, whereas PA referral schemes are predominantly facilitated by factors related to professional interactions.
Certainty assessment of the systematic review
The SURE tool indicated that this is a good quality systematic review with minor limitations regarding selection procedure: i. language bias, as only studies written in English were selected; and ii. status of publication, as only published studies were included (see Additional file 6). A more comprehensive search avoiding these limitations could, thus, have retrieved a higher number of studies. Even so, English is the universal language for science communication, the best available science works tend to be published, and a seven-year time interval can be considered adequate to have an updated picture of today’s health services panorama. Considering the critical appraisal of the included studies and that the output of this systematic review is qualitative, the three quality criteria that probably most negatively influence certainty of the evidence were the non-accomplishment of quality criteria for both study components (qualitative and quantitative) in mixed-methods studies, issues related with the validity and reliability of the instruments used in analytical cross-sectional studies, as well as insufficient coverage of sample subgroups in data analysis in some prevalence studies. However, it is important to stress that the vast majority of the included studies did not present any of these issues. Together, the findings of the present systematic review can be considered reliable for evidence-informed health policymaking. Results of this review should, nevertheless, be interpreted taking these minor limitations into consideration.
Discussion
This systematic review assessed implementation barriers and facilitators in real-world PA promotion and/or sedentary time reduction interventions (i.e., PA assessment, brief counselling, prescription, and referral scheme) delivered in primary healthcare settings, using the TICD framework [30]. Five determinants of implementation success stood out from our review, given their reported frequency: having health professionals with a good degree of knowledge and skills regarding PA and its promotion; the need for the intervention to be feasible/compatible with professionals’ and health services’ usual tasks; interventions’ cost and the provision of financial incentives; having adequate tools and materials to implement the intervention; and fostering positive health professionals’ cognitions and attitudes, while minimizing negative ones. These determinants belong to three domains: individual health professional factors; intervention/guideline factors, and incentives and resources. Despite being less or rarely reported, other determinants may play a particularly facilitating or hindering role regarding interventions’ implementation (e.g., networks). Apart from PA assessment, implementation of all intervention types (excluding combinations) is influenced by factors belonging to all the seven main domains, although some domains were predominantly highlighted in a certain type of intervention: PA counselling seems to be particularly hampered by intervention/guideline and individual (health professionals and patients) factors and facilitated by individual health professionals’ ones; PA prescription seems to be particularly influenced by incentives and resources’ barriers and facilitators; and PA referral schemes seem to be specially facilitated by factors related to professional interactions. PA assessment seems to be more dependent on individual factors (from patients or professionals) and available resources – whereas more complex interventions seem to rely also on organisational, political, and social determinants –, but the limited number of primary studies assessing PA assessment alone can be biasing this specific result.
Health professionals’ knowledge and skills was the most frequent reported determinant and has been previously highlighted as important for proper implementation [13, 32, 33, 35, 105]. WHO’s monitoring of the implementation of the Global Action Plan for Physical Activity also reinforced that more pre- and post-graduated training of health professionals is needed – also for professionals outside the health sector – combined with the provision of adequate tools and guidance [3]. However, training is not always sufficient to determine health professionals’ PA counselling behaviours [106, 107]. Despite this, PA promotion in medical schools’ curricula is still a hot topic, as there seems to be a recurrent gap in the pre-graduate medical training [108,109,110]. The importance of knowing PA pathways to community resources and behaviour change techniques was mentioned in several works. This reinforces the need for proper training of health professionals, not only in terms of PA content, but also in modes of delivery. Adequate and innovative information systems may be promising tools in supporting face-to-face delivery of behaviour change techniques applied to PA promotion [111]. A continuing education system that can support in-service professionals (the third most reported facilitator within incentives and resources’ theme) can also play a relevant role in this regard.
Concerning interventions’ feasibility/compatibility, a recent systematic review on the views of stakeholders also identified the congruence of the intervention with team activities as key facilitator [32]. The (lack of) compatibility of the intervention with usual tasks may be interrelated with other reported determinants (for instance, having enough human resources). Of these, a significant one is the optimization of the information system, the second most reported facilitator within the “incentives and resources” domain. Indeed, the availability of computerised solutions that help health professionals save time and efforts during interventions’ delivery may be, once more, paramount.
Interventions’ cost has long been a concern regarding PA promotion in primary care and health system sustainability. Particularly, PA counselling and referral brief interventions are very well positioned to be nationally/locally endorsed, as they are considered a “best-buy” to tackle non-communicable diseases, giving their evidence of cost-effectiveness [10, 112]. Financial incentives for patients have also gathered evidence in increasing patients’ PA in the short and long term [113], which can be an effect of an increased patients’ adherence to the intervention. The establishment of networks between healthcare and community PA programmes and resources that brings reduced costs or even free PA options for patients can offer a solution in this regard. Also, a specific budget allocated to health-enhancing physical activity promotion is considered strategic [114]. Financial incentives for healthcare professionals could, thus, be analysed in this context.
Adequate assistance tools and materials and health professionals’ cognitions and attitudes were also found to be key determinants. This result was shown in other works [32, 33], including community-based interventions [31]. Positive attitudes were linked with patients engagement and facilitated adaptation processes throughout implementation, whereas placing low value on the intervention hindered the implementation [31]. The relevance attributed to PA promotion in healthcare by medical doctors had also been identified as a significant predictor of clinical practice in this area [106].
“Social, political, and legal factors” were the least reported domain. Considering that national public health policy and legislation is recognized as crucial by international guidelines [9], this finding may reflect the scarcity of research specifically addressing health policy/legislation impact in this area. In fact, only one of the included studies [44] assessed the impact of a legislative framework on PA prescription.
Although the frequency of reporting is useful to obtain a picture of the most and least studied implementation determinants, it does not necessarily reflect the degree of importance of each barrier and facilitator. Caution is needed, as interpretation bias may be introduced if one equates the relevance of each determinant with its reporting frequency. Even so, the identified implementation determinants were under the seven domains of the TICD framework, with even distribution between barriers and facilitators in each domain, evidencing that the studies included explored an extensive set of factors influencing implementation.
This review presents suggestive evidence that other determinants may play an important role and should not be overlooked: patients’ motivation (barrier/facilitator); intervention components/characteristics/content (facilitator); positive team processes (facilitator); and the establishment of networks between sectors/stakeholders (facilitator). Having the knowledge and skills to implement an intervention evidencing compatibility/feasibility with routine care does not mean that implementation cannot be easily hindered by other determinants in place. Together, this evidence suggests that there are some more general implementation determinants and others more context-specific. A broad assessment of implementation barriers and facilitators should, thus, be made when preparing an intervention implementation to understand the local context.
The entire chain of interacting actors within and outside the health sector, influences implementation success. Each one brings unique contributions to the implementation and scaling-up phases. Planning beforehand to identify and engage all relevant stakeholders from the entire delivery chain is of outmost importance to tackle future translational challenges. Nonetheless, primary studies often overlooked the views of politicians, health coordinators or community stakeholders, suggesting an evidence gap. The need for a coordinated systems-approach to foster the implementation of PA interventions in healthcare settings, involving several key stakeholders, has been reported in multiple works in this area [13, 105, 115,116,117].
Another finding was that adequate implementation of more complex interventions implies the commitment of more structures, beyond the specific contexts of local health facilities, professionals and patients. In line with the “PA vital sign” proposal [118], it can be hypothesised that the universal implementation of PA assessment should be the first step for PA promotion in primary care, with the more complex ones being gradually introduced. Implementing PA assessment was even reported in primary studies as a facilitator of the subsequent implementation of PA counselling. However, the limited number of primary studies addressing PA assessment alone do not allow to draw firm conclusions on this issue.
Generating knowledge about key implementation barriers and facilitators of PA promotion interventions in primary healthcare contributes to define tailored implementation strategies to improve the adoption, implementation, sustainability, and scaling-up of such interventions [23]. An iterative planning process should occur to potentiate success: 1) characterizing the delivery context and anticipating barriers and facilitators; 2) designing tailored implementation strategies; 3) monitoring implementation and dealing with implementation determinants that effectively emerge during translation and scale-up; and 4) incorporating these outcomes in the implementation processes to optimize them [119,120,121].
Strengths and limitations
To our knowledge, this is the first systematic review analysing theoretically framed implementation barriers and facilitators of four PA interventions (assessment, counselling, prescription, referral) implemented in the primary health care, integrating the views of patients, health professionals and stakeholders. The framework used herein to systematize barriers and facilitators of implementation also constitutes a strength of this review, as it was specifically developed to identify determinants of practice in healthcare contexts, facilitating its identification and organisation in a parsimonious way.
Still, this review is not without limitations. Attention should be paid to the fact that more than one third of the included studies used quantitative designs. As such, some determinants may be intentionally selected and more frequently studied by researchers (e.g., in questionnaires with closed-ended questions), as opposed to implementation determinants that unintentionally emerge from qualitative data. Furthermore, only 31% of the primary studies clearly reported the use of a published framework when identifying implementation determinants, which presents a high risk of bias, as acknowledged barriers and facilitators could have been overlooked. Also, further studies including the views of stakeholders, outside the health sector, remain scarce, precluding a more comprehensive picture of implementation determinants. Most studies included in this systematic review reflect interventions implemented in high income countries, suggesting that the findings presented may not necessarily play a similar role in implementation processes occurring in countries of other income levels. Also, lack of sufficient detail in studies’ description of the PA promotion interventions was common, which may have led to an incorrect classification of the interventions. Earlier described methodological limitations of the primary studies are also concerning factors, as they could have biased the results. Lastly, the time limitation of the literature search poses a methodological limitation, as studies published before 2016 were not considered. Despite this, and together with the reasonable number of included studies obtained (n = 62), a fair picture of today’s reality of implementation determinants of PA promotion interventions in primary care was probably achieved. Caution is needed, however, when analysing the results for PA assessment, as only two primary studies addressed this type of intervention alone.
Future research
In order to bridge the gap between research and practice, future research should focus on proper implementation preparation of evidence-based interventions and enhanced dissemination, considering: a) the wide range of agents that should be involved (stakeholders from all levels); b) implementation barriers and facilitators, considering mixed-methods design studies (combining quantitative components, that estimate the degree of influence of each determinant in real-world conditions, with qualitative components that allow the identification of potential barriers and facilitators), with proper interventions’ descriptions, and investing in studies of interventions also delivered in upper middle and low income contexts; c) tailored implementation strategies and implementation plans. In implementing interventions in real-world conditions, an adaptation phase should always be expected, involving constant loops of monitoring and feedback to increase the effect, aligning with the evidence, while fully embed the intervention in a new system and carefully keeping its active ingredients – future research agenda should support these processes as well.
Conclusion
The present review identifies the most relevant implementation determinants of PA-specific promotion interventions in primary health care, from the point of view of health professionals, patients, and stakeholders. These findings address a research-to-practice gap and will support the translation process of science-based interventions.
Although implementation of PA promotion interventions in primary care is determined by a wide set of barriers and facilitators, health professionals-, intervention-, and resources-specific ones seem to be particularly relevant. As such, a careful consideration of these factors is needed when preparing interventions’ delivery. Tailored implementation strategies should be designed for successful implementation, particularly those addressing deliverers’ knowledge/skills, attitudes and cognitions; interventions’ feasibility/compatibility with routine care and cost; and the availability of adequate supporting materials and tools. Suggestive evidence also highlights some barriers and facilitators related with patients’ motivation, intervention characteristics, and professionals’ interactions as relevant. Moreover, implementation determinants are modulated by the type of PA intervention. From a practical implication perspective, there seems to be more context- and intervention-specific determinants, so a deep understanding of the local context combined with intervention’s characteristics is highly recommended when preparing an intervention implementation.
The findings of this review should be considered by primary care authorities and coordination teams aiming to optimize interventions’ implementation and effectiveness in real world conditions – from the design of tailored implementation strategies to the development of national policies, tools and systems to support regional or nationwide scale-up.
Registration and protocol
This systematic review was registered in PROSPERO (CRD42022318632). The protocol was not previously published.
Availability of data and materials
All relevant data used for the current study are within the paper and its supporting information.
Abbreviations
- JBI:
-
Joanna Brigs Institute
- MMAT:
-
Mixed-Methods Appraisal Tool
- PA:
-
Physical activity
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- SURE:
-
Supporting the Use of Research Evidence
- TICD:
-
Tailored Implementation for Chronic Diseases
- WHO:
-
World Health Organization
References
Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–29. https://doi.org/10.1016/S0140-6736(12)61031-9.
Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25(Suppl 3):1–72. https://doi.org/10.1111/sms.12581.
World Health Organization. Global status report on physical activity 2022. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018. https://doi.org/10.1016/S2214-109X(18)30357-7.
Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. 2020;4(1):23–35. https://doi.org/10.1016/S2352-4642(19)30323-2.
World Health Organization. Global action plan for the prevention and control of non-communicable diseases 2013–2020. Geneva: World Health Organization; 2013.
World Health Organization. Physical activity strategy for the WHO European Region 2016–2025. Copenhagen: World Health Organization; 2016.
World Health Organization. Integrating diet, physical activity and weight management services into primary care. Geneva: World Health Organization; 2016.
World Health Organization. Global action plan on physical activity 2018–2030: more active people for a healthier world. Geneva: World Health Organization; 2018.
World Health Organization. Promoting physical activity through primary health care: a toolkit. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
Wald NJ. The definition of screening. J Med Screen. 2001;8(1):1.
Order No. 8932/2017. Diary of the Republic No. 195/2017, Series II. 2017. Available online: https://diariodarepublica.pt/dr/detalhe/despacho/8932-2017-108275649. Accessed 27 July 2022.
Lion A, Vuillemin A, Thornton JS, Theisen D, Stranges S, Ward M. Physical activity promotion in primary care: a utopian quest? Health Promot Int. 2019;34(4):877–86. https://doi.org/10.1093/heapro/day038.
Williams NH, Hendry M, France B, Lewis R, Wilkinson C. Effectiveness of exercise-referral schemes to promote physical activity in adults: systematic review. Br J Gen Pract. 2007;57(545):979–86. https://doi.org/10.3399/096016407782604866.
Anokye NK, Trueman P, Green C, Pavey TG, Hillsdon M, Taylor RS. The cost-effectiveness of exercise referral schemes. BMC Public Health. 2011;11:954. https://doi.org/10.1186/1471-2458-11-954.
Abu-Omar K, Rütten A, Burlacu I, Schätzlein V, Messing S, Suhrcke M. The cost-effectiveness of physical activity interventions: a systematic review of reviews. Prev Med Rep. 2017;8:72–8. https://doi.org/10.1016/j.pmedr.2017.08.006.
Lamming L, Pears S, Mason D, Morton K, Bijker M, Sutton S, et al. What do we know about brief interventions for physical activity that could be delivered in primary care consultations? A systematic review of reviews. Prev Med. 2017;99:152–63. https://doi.org/10.1016/j.ypmed.2017.02.017.
Kallings LV, Leijon M, Hellénius ML, Ståhle A. Physical activity on prescription in primary health care: a follow-up of physical activity level and quality of life. Scand J Med Sci Sports. 2008;18(2):154–61. https://doi.org/10.1111/j.1600-0838.2007.00678.x.
Campbell F, Holmes M, Everson-Hock E, Davis S, Buckley Woods H, Anokye N, et al. A systematic review and economic evaluation of exercise referral schemes in primary care: a short report. Health Technol Assess. 2015;19(60):1–110. https://doi.org/10.3310/hta19600.
Sanchez A, Bully P, Martinez C, Grandes G. Effectiveness of physical activity promotion interventions in primary care: a review of reviews. Prev Med. 2015;76(Suppl):S56-67. https://doi.org/10.1016/j.ypmed.2014.09.012.
Fernandez ME, Ten Hoor GA, van Lieshout S, Rodriguez SA, Beidas RS, Parcel G, et al. Implementation mapping: using intervention mapping to develop implementation strategies. Front Public Health. 2019;7:158. https://doi.org/10.3389/fpubh.2019.00158.
Green LW, Ottoson JM, García C, Hiatt RA. Diffusion theory and knowledge dissemination, utilization, and integration in public health. Annu Rev Public Health. 2009;30:151–74. https://doi.org/10.1146/annurev.publhealth.031308.100049.
Powell BJ, Fernandez ME, Williams NJ, Aarons GA, Beidas RS, Lewis CC, et al. Enhancing the impact of implementation strategies in healthcare: a research agenda. Front Public Health. 2019;7:3. https://doi.org/10.3389/fpubh.2019.00003.
Wensing M, Bosch M, Foy R, van der Weijden T, Eccles M, Grol R. Factors in theories on behaviour change to guide implementation and quality improvement in health care. Nijmegen: Centre for Quality of Care Research (WOK); 2005.
Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282(15):1458–65. https://doi.org/10.1001/jama.282.15.1458.
Mäkelä M, Thorsen T. A framework for guidelines implementation studies. In: Thorsen T, Mäkelä M, editors. Changing professional practice: theory and practice of clinical guidelines implementation. 1st ed. Copenhagen: DSI - Danish Institute for Health Services Research; 1999. p. 23–53.
Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust. 2004;180(S6):S57-60. https://doi.org/10.5694/j.1326-5377.2004.tb05948.x.
Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33. https://doi.org/10.1136/qshc.2004.011155.
Rainbird K, Sanson-Fisher R, Buchan H. Identifying barriers to evidence uptake. Melbourne: National Institute of Clinical Studies (NICS); 2006.
Flottorp SA, Oxman AD, Krause J, Musila NR, Wensing M, Godycki-Cwirko M, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8:35. https://doi.org/10.1186/1748-5908-8-35.
Cooper J, Murphy J, Woods C, Van Nassau F, McGrath A, Callaghan D, et al. Barriers and facilitators to implementing community-based physical activity interventions: a qualitative systematic review. Int J Behav Nutr Phys Act. 2021;18(1):118. https://doi.org/10.1186/s12966-021-01177-w.
Manta SW, Sandreschi PF, dos Santos MC, Konrad LM, Tassitano RM, Benedetti TRB. Barriers and facilitators on the implementation of physical activity in Primary Health Care: a systematic review. Prev Med Rep. 2022;28:101875. https://doi.org/10.1016/j.pmedr.2022.101875.
Albert FA, Crowe MJ, Malau-Aduli AEO, Malau-Aduli BS. Physical activity promotion: a systematic review of the perceptions of healthcare professionals. Int J Environ Res Public Health. 2020;17(12). https://doi.org/10.3390/ijerph17124358.
Huijg JM, Gebhardt WA, Verheijden MW, van der Zouwe N, de Vries JD, Middelkoop BJ, et al. Factors influencing primary health care professionals’ physical activity promotion behaviors: a systematic review. Int J Behav Med. 2015;22(1):32–50. https://doi.org/10.1007/s12529-014-9398-2.
Hébert ET, Caughy MO, Shuval K. Primary care providers’ perceptions of physical activity counselling in a clinical setting: a systematic review. Br J Sports Med. 2012;46(9):625–31. https://doi.org/10.1136/bjsports-2011-090734.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.31222/osf.io/jb4dx.
Critical Appaisal Tools. Joanna Briggs Institute. Available online: https://jbi.global/critical-appraisal-tools (Accessed on 22 June 2022).
Hong Q, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT), version 2018. Registration of Copyright (#1148552), Canadian Intellectual Property Office, Industry Canada. 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf. Accessed 5 May 2022.
Tod D, Booth A, Smith B. Critical appraisal. Int Rev Sport Exerc Psychol. 2022;15(1):52–72. https://doi.org/10.1080/1750984x.2021.1952471.
Clarke V, Braun V, Hayfield N. Thematic analysis. In: Smith JA, editor. Qualitative psychology: a practical guide to research methods. London: SAGE Publications; 2015. p. 222–48.
Supporting the Use of Research Evidence (SURE) Collaboration. SURE checklist for making judgements about how much confidence to place in a systematic review. In: SURE guides for preparing and using evidence-based policy briefs: 4. Deciding on and describing policy options – Additional resources. Version 2.1 [updated November 2011]. Available online: https://epoc.cochrane.org/sites/epoc.cochrane.org/files/public/uploads/SURE-Guides-v2.1/Collectedfiles/sure_guides.html. Accessed 28 Mar 2023.
Kyei-Frimpong J, Blood-Siegfried J, Wijetilaka R, Gendler A. Exercise as medicine: providing practitioner guidance on exercise prescription. Prev Med Rep. 2021;22:101323. https://doi.org/10.1016/j.pmedr.2021.101323.
Syrjälä MB, Fharm E, Dempsey PC, Nordendahl M, Wennberg P. Reducing occupational sitting time in adults with type 2 diabetes: qualitative experiences of an office-adapted mHealth intervention. Diabet Med. 2021;38(6):e14514. https://doi.org/10.1111/dme.14514.
Charles M, Ouchchane L, Thivel D, Celine L, Duclos M. Does legislative framework favors prescription of physical activity in primary care? The French experience. Phys Sportsmed. 2022;50(1):47–53. https://doi.org/10.1080/00913847.2020.1864676.
Souza-Neto JM, Florindo AA, Costa FFD. Associated factors with physical activity counseling among Brazilian Family Health Strategy workers. Cien Saude Colet. 2021;26(1):369–78. https://doi.org/10.1590/1413-81232020261.10082019.
Huntington J, Dwyer JJM, Shama S, Brauer P. Registered dietitians’ beliefs and behaviours related to counselling patients on physical activity and sedentary behaviour from a theory of planned behaviour perspective. BMC Nutr. 2020;6(1):66. https://doi.org/10.1186/s40795-020-00392-1.
Buckley BJR, Finnie SJ, Murphy RC, Watson PM. “You’ve got to pick your battles”: a mixed-methods investigation of physical activity counselling and referral within general practice. Int J Environ Res Public Health. 2020;17(20). https://doi.org/10.3390/ijerph17207428.
Sissons A, Grant A, Kirkland A, Currie S. Using the theoretical domains framework to explore primary health care practitioner’s perspectives and experiences of preconception physical activity guidance and promotion. Psychol Health Med. 2020;25(7):844–54. https://doi.org/10.1080/13548506.2019.1679846.
Carstairs SA, Rogowsky RH, Cunningham KB, Sullivan F, Ozakinci G. Connecting primary care patients to community-based physical activity: a qualitative study of health professional and patient views. BJGP Open. 2020;4(3). https://doi.org/10.3399/bjgpopen20x101100.
Alghafri TS, Al Harthi SM, Al-Ajmi F, Al-Farsi Y, Craigie AM, Bannerman E, et al. Acceptability of the “MOVEdiabetes” physical activity intervention in diabetes primary care settings in Oman: findings from participants and practitioners. BMC Public Health. 2020;20(1):887. https://doi.org/10.1186/s12889-020-09029-1.
Parjanen S. The elements of cross-sectoral collaboration between primary care and the sports sector. Manag Sport Leis. 2021;26(3):226–44. https://doi.org/10.1080/23750472.2020.1757492.
Yonis OB, Saadeh R, Chamseddin Z, Alananzeh H. Exercise counseling by primary care physicians in Jordan - a preliminary study. J Prim Care Community Health. 2020;11:2150132720946947. https://doi.org/10.1177/2150132720946947.
Agadayı E, Karasimav Ö, Sencan İ, Agadayı S, Kasım İ, Kahveci R, et al. Knowledge and attitude relating to exercise prescription of family medicine research assistant and specialist physicians who are working in Ankara. Gulhane Med J. 2019;61(4):152. https://doi.org/10.26657/gulhane.00075.
Joelsson M, Lundqvist S, Larsson MEH. Tailored physical activity on prescription with follow-ups improved motivation and physical activity levels. A qualitative study of a 5-year Swedish primary care intervention. Scand J Prim Health Care. 2020;38(4):399–410. https://doi.org/10.1080/02813432.2020.1842965.
Christiansen M, White D, Christian J, Waugh E, Gakhal N, King L, et al. “It... Doesn’t always make it [to] the top of the list” Primary care physicians’ experiences with prescribing exercise for knee osteoarthritis. Can Fam Physician. 2020;66(1):E14-E20.
Bird EL, Biddle MSY, Powell JE. General practice referral of “at risk” populations to community leisure services: applying the RE-AIM framework to evaluate the impact of a community-based physical activity programme for inactive adults with long-term conditions. BMC Public Health. 2019;19(1):1308. https://doi.org/10.1186/s12889-019-7701-5.
Alahmed Z, Lobelo F. Correlates of physical activity counseling provided by physicians: a cross-sectional study in Eastern Province, Saudi Arabia. PLoS One. 2019;14(7):e0220396. https://doi.org/10.1371/journal.pone.0220396.
Westland H, Koop Y, Schröder CD, Schuurmans MJ, Slabbers P, Trappenburg JCA, et al. Nurses’ perceptions towards the delivery and feasibility of a behaviour change intervention to enhance physical activity in patients at risk for cardiovascular disease in primary care: a qualitative study. BMC Fam Pract. 2018;19(1):194. https://doi.org/10.1186/s12875-018-0888-1.
Harris T, Kerry S, Victor C, Iliffe S, Ussher M, Fox-Rushby J, et al. A pedometer-based walking intervention in 45- to 75-year-olds, with and without practice nurse support: the PACE-UP three-arm cluster RCT. Health Technol Assess. 2018;22(37):1–274. https://doi.org/10.3310/hta22370.
Leenaars KEF, Smit E, Wagemakers A, Molleman GRM, Koelen MA. The role of the care sport connector in the Netherlands. Health Promot Int. 2018;33(3):422–35. https://doi.org/10.1093/heapro/daw097.
Baillot A, Baillargeon JP, Paré A, Poder TG, Brown C, Langlois MF. Physical activity assessment and counseling in Quebec family medicine groups. Can Fam Physician. 2018;64(5):e234–41.
Gustavsson C, Nordqvist M, Bröms K, Jerdén L, Kallings LV, Wallin L. What is required to facilitate implementation of Swedish physical activity on prescription? - interview study with primary healthcare staff and management. BMC Health Serv Res. 2018;18(1):196. https://doi.org/10.1186/s12913-018-3021-1.
Al-Ghamdi S, Alajmi M, Al-Gonaim A, Al-Juhayyim S, Al-Qasem S, Al-Tamimi I. Perceptions and attitudes of primary healthcare providers in Riyadh City, Saudi Arabia, toward the promotion of physical activity. Int J Health Promot Educ. 2018;56(2):105–19. https://doi.org/10.1080/14635240.2018.1430601.
Fowles JR, O’Brien MW, Solmundson K, Oh PI, Shields CA. Exercise is Medicine Canada physical activity counselling and exercise prescription training improves counselling, prescription, and referral practices among physicians across Canada. Appl Physiol Nutr Metab. 2018;43(5):535–9. https://doi.org/10.1139/apnm-2017-0763.
Henderson HE, Evans AB, Allen-Collinson J, Siriwardena NA. The ‘wild and woolly’ world of exercise referral schemes: contested interpretations of an exercise as medicine programme. Qual Res Sport Exerc Health. 2018;10(4):505–23. https://doi.org/10.1080/2159676x.2017.1352018.
Johnson NA, Ewald B, Plotnikoff RC, Stacey FG, Brown WJ, Jones M, et al. Predictors of adherence to a physical activity counseling intervention delivered by exercise physiologists: secondary analysis of the NewCOACH trial data. Patient Prefer Adherence. 2018;12:2537–43. https://doi.org/10.2147/ppa.s183938.
Alghafri TS, Alharthi SM, Al-Balushi S, Al-Farsi Y, Al-Busaidi Z, Bannerman E, et al. Health professionals' perceptions about physical activity promotion in diabetes care within primary health care settings in Oman. Heliyon. 2017;3(12):e00495. https://doi.org/10.1016/j.heliyon.2017.e00495.
Bélanger M, Phillips EW, O'Rielly C, Mallet B, Aubé S, Doucet M, et al. Longitudinal qualitative study describing family physicians’ experiences with attempting to integrate physical activity prescriptions in their practice: 'it's not easy to change habits’. BMJ Open. 2017;7(7):e017265. https://doi.org/10.1136/bmjopen-2017-017265.
Cottrell E, Foster NE, Porcheret M, Rathod T, Roddy E. GPs’ attitudes, beliefs and behaviours regarding exercise for chronic knee pain: a questionnaire survey. BMJ Open. 2017;7(6):e014999. https://doi.org/10.1136/bmjopen-2016-014999.
Barrett EM, Hussey J, Darker CD. Feasibility of a physical activity pathway for Irish primary care physiotherapy services. Physiotherapy. 2017;103(1):106–12. https://doi.org/10.1016/j.physio.2016.02.001.
Matthews A, Jones N, Thomas A, van den Berg P, Foster C. An education programme influencing health professionals to recommend exercise to their type 2 diabetes patients - understanding the processes: a case study from Oxfordshire, UK. BMC Health Serv Res. 2017;17(1):130. https://doi.org/10.1186/s12913-017-2040-7.
O’Brien MW, Shields CA, Oh PI, Fowles JR. Health care provider confidence and exercise prescription practices of Exercise is Medicine Canada workshop attendees. Appl Physiol Nutr Metab. 2017;42(4):384–90. https://doi.org/10.1139/apnm-2016-0413.
Leavitt PT. Improving exercise prescribing in a rural New England free clinic. J Nurse Pract. 2017;13(1):e29–33. https://doi.org/10.1016/j.nurpra.2016.09.014.
Hidalgo KD, Mielke GI, Parra DC, Lobelo F, Simões EJ, Gomes GO, et al. Health promoting practices and personal lifestyle behaviors of Brazilian health professionals. BMC Public Health. 2016;16(1):1114. https://doi.org/10.1186/s12889-016-3778-2.
Aittasalo M, Kukkonen-Harjula K, Toropainen E, Rinne M, Tokola K, Vasankari T. Developing physical activity counselling in primary care through participatory action approach. BMC Fam Pract. 2016;17(1):141. https://doi.org/10.1186/s12875-016-0540-x.
Dutton SN, Dennis SM, Zwar N, Harris MF. An explorative qualitative study on acceptability of physical activity assessment instruments among primary care professionals in southern Sydney. BMC Fam Pract. 2016;17(1):138. https://doi.org/10.1186/s12875-016-0536-6.
Leenaars KE, Florisson AM, Smit E, Wagemakers A, Molleman GR, Koelen MA. The connection between the primary care and the physical activity sector: professionals’ perceptions. BMC Public Health. 2016;16(1):1001. https://doi.org/10.1186/s12889-016-3665-x.
Avery L, Charman SJ, Taylor L, Flynn D, Mosely K, Speight J, et al. Systematic development of a theory-informed multifaceted behavioural intervention to increase physical activity of adults with type 2 diabetes in routine primary care: Movement as Medicine for type 2 diabetes. Implement Sci. 2016;11:99. https://doi.org/10.1186/s13012-016-0459-6.
Clark RE, Milligan J, Ashe MC, Faulkner G, Canfield C, Funnell L, et al. A patient-oriented approach to the development of a primary care physical activity screen for embedding into electronic medical records. Appl Physiol Nutr Metab. 2021;46(6):589–96. https://doi.org/10.1139/apnm-2020-0356.
Attwood S, Morton KL, Mitchell J, Van Emmenis M, Sutton S, Team VP. Reasons for non-participation in a primary care-based physical activity trial: a qualitative study. BMJ Open. 2016;6(5):e011577. https://doi.org/10.1136/bmjopen-2016-011577.
Taylor AH, Taylor RS, Ingram WM, Anokye N, Dean S, Jolly K, et al. Adding web-based behavioural support to exercise referral schemes for inactive adults with chronic health conditions: the e-coachER RCT. Health Technol Assess. 2020;24(63):1–106. https://doi.org/10.3310/hta24630.
Hefnawi B, Leung L, Tomasone JR. Exploring barriers medical residents and established physicians face counselling patients on physical activity by stage of the transtheoretical model. Psychol Health Med. 2021;26(6):684–91. https://doi.org/10.1080/13548506.2020.1754437.
Hanson CL, Oliver EJ, Dodd-Reynolds CJ, Allin LJ. How do participant experiences and characteristics influence engagement in exercise referral? A qualitative longitudinal study of a scheme in Northumberland, UK. BMJ Open. 2019;9(2):e024370. https://doi.org/10.1136/bmjopen-2018-024370.
Wattanapisit A, Thanamee S, Wongsiri S. Physical activity counselling among GPs: a qualitative study from Thailand. BMC Fam Pract. 2019;20(1):72. https://doi.org/10.1186/s12875-019-0968-x.
Omura JD, Bellissimo MP, Watson KB, Loustalot F, Fulton JE, Carlson SA. Primary care providers’ physical activity counseling and referral practices and barriers for cardiovascular disease prevention. Prev Med. 2018;108:115–22. https://doi.org/10.1016/j.ypmed.2017.12.030.
Lewis ZH, Ottenbacher KJ, Fisher SR, Jennings K, Brown AF, Swartz MC, et al. The feasibility and RE-AIM evaluation of the TAME health pilot study. Int J Behav Nutr Phys Act. 2017;14(1):106. https://doi.org/10.1186/s12966-017-0560-5.
Brandborg CE, Skjerning HT, Nielsen RO. Physical activity through social prescribing: an interview-based study of Danish general practitioners’ opinions. Health Soc Care Community. 2022;30(5):1969–78. https://doi.org/10.1111/hsc.13577.
Bowen PG, William OA, Olivia A, Levi P, Wingo N. Physical activity promotion in a safety-net clinic: does the provider make a difference? A pilot study. Transl J Am Coll Sports Med. 2021;6(4). https://doi.org/10.1249/tjx.0000000000000175.
Downey J, Shearn K, Brown N, Wadey R, Breckon J. Behaviour change practices in exercise referral schemes: developing realist programme theory of implementation. BMC Health Serv Res. 2021;21(1):335. https://doi.org/10.1186/s12913-021-06349-9.
Huebschmann AG, Glasgow RE, Leavitt IM, Chapman K, Rice JD, Lockhart S, et al. Integrating a physical activity coaching intervention into diabetes care: a mixed-methods evaluation of a pilot pragmatic trial. Transl Behav Med. 2022;12(4):601–10. https://doi.org/10.1093/tbm/ibac014.
Dranebois S, Lalanne-Mistrih ML, Nacher M, Thelusme L, Deungoue S, Demar M, et al. Prescription of physical activity by general practitioners in type 2 diabetes: practice and barriers in French Guiana. Front Endocrinol (Lausanne). 2022;12:790326. https://doi.org/10.3389/fendo.2021.790326.
Morgan K, Lewis J, Hawkins J, Moore G. From a research trial to routine practice: stakeholders’ perceptions and experiences of referrals to the National Exercise Referral Scheme (NERS) in Wales. BMC Health Serv Res. 2021;21(1):1232. https://doi.org/10.1186/s12913-021-07266-7.
Albert FA, Malau-Aduli AEO, Crowe MJ, Malau-Aduli BS. The 'PRICE' of Physical Activity Referral Schemes (PARS): stakeholders' recommendations for delivering quality care to patients. Int J Environ Res Public Health. 2021;18(16). https://doi.org/10.3390/ijerph18168627.
Wattanapisit A, Amaek W, Wattanapisit S, Tuangratananon T, Wongsiri S, Pengkaew P. Challenges of implementing an mHealth application for personalized physical activity counselling in primary health care: a qualitative study. Int J Gen Med. 2021;14:3821–31. https://doi.org/10.2147/ijgm.s317241.
Calonge-Pascual S, Fuentes Jiménez F, Arnal-Selfa R, Belmonte-Cortés S, González-Gross M. Self-perception of primary health-care staff about physical activity on prescription: a qualitative semi-structured interview. Semergen. 2023;49(1):101856. https://doi.org/10.1016/j.semerg.2022.101856.
Wangler J, Jansky M. Promotion of exercise and health for older people in primary care: a qualitative study on the potential, experiences and strategies of general practitioners in Germany. J Prev. 2023. https://doi.org/10.1007/s10935-023-00730-6.
Buckley BJR, Newton J, Knox S, Noonan B, Smith M, Watson PM. Multi-stakeholder perspectives on co-production: five key recommendations following the Liverpool Co-PARS project. Qual Res Sport Exerc Health. 2023;15(2):220–34. https://doi.org/10.1080/2159676x.2022.2152085.
Alyafei M, Alchawa M, Farooq A, Selim N, Bougmiza I. Physical activity among primary health care physicians and its impact on counseling practices. Biomed Hub. 2023;8(1):31–41. https://doi.org/10.1159/000530085.
De Guzman KR, Pratt M, Hwang A, Linke SE. Patient feedback and evaluation measures of a physical activity initiative: Exercise is Medicine program. Fam Pract. 2022;39(5):813–8. https://doi.org/10.1093/fampra/cmab178.
Moraes SQ, Santos ACB, Fermino RC, Rech CR. Physical activity counseling in primary health care. Cien Saude Colet. 2022;27(9):3603–14. https://doi.org/10.1590/1413-81232022279.20192021en.
Snége A, Silva AAPD, Mielke GI, Rech CR, Siqueira FCV, Rodriguez-Añez CR, et al. Sedentary behavior counseling received from healthcare professionals: an exploratory analysis in adults at primary health care in Brazil. Int J Environ Res Public Health. 2022;19(16). https://doi.org/10.3390/ijerph19169963.
Pellerine LP, O'Brien MW, Shields CA, Crowell SJ, Strang R, Fowles JR. Health care providers' perspectives on promoting physical activity and exercise in health care. Int J Environ Res Public Health. 2022;19(15). https://doi.org/10.3390/ijerph19159466.
Albert FA, Malau-Aduli AEO, Crowe MJ, Malau-Aduli BS. Optimising care coordination strategies for physical activity referral scheme patients by Australian health professionals. PLoS One. 2022;17(7):e0270408. https://doi.org/10.1371/journal.pone.0270408.
Countries and economies. The World Bank. Available online: https://data.worldbank.org/country (Accessed 9 Sept 2022).
AuYoung M, Linke SE, Pagoto S, Buman MP, Craft LL, Richardson CR, et al. Integrating physical activity in primary care practice. Am J Med. 2016;129(10):1022–9. https://doi.org/10.1016/j.amjmed.2016.02.008.
Silva CS, Mendes R, Godinho C, Monteiro-Pereira A, Pimenta-Ribeiro J, Martins HS, et al. Predictors of physical activity promotion in clinical practice: a cross-sectional study among medical doctors. BMC Med Educ. 2022;22(1):624. https://doi.org/10.1186/s12909-022-03686-z.
Dacey ML, Kennedy MA, Polak R, Phillips EM. Physical activity counseling in medical school education: a systematic review. Med Educ Online. 2014;19:24325. https://doi.org/10.3402/meo.v19.24325.
Cardinal BJ, Park EA, Kim M, Cardinal MK. If exercise is medicine, where is exercise in medicine? Review of U.S. medical education curricula for physical activity-related content. J Phys Act Health. 2015;12(9):1336–43. https://doi.org/10.1123/jpah.2014-0316.
Strong A, Stoutenberg M, Hobson-Powell A, Hargreaves M, Beeler H, Stamatakis E. An evaluation of physical activity training in Australian medical school curricula. J Sci Med Sport. 2017;20(6):534–8. https://doi.org/10.1016/j.jsams.2016.10.011.
Osborne SA, Adams JM, Fawkner S, Kelly P, Murray AD, Oliver CW. Tomorrow’s doctors want more teaching and training on physical activity for health. Br J Sports Med. 2017;51(8):624–5. https://doi.org/10.1136/bjsports-2016-096807.
Mendes R, Silva MN, Silva CS, Marques A, Godinho C, Tomás R, et al. Physical activity promotion tools in the Portuguese primary health care: an implementation research. Int J Environ Res Public Health. 2020;17(3). https://doi.org/10.3390/ijerph17030815.
World Health Organization. Tackling NCDs: ‘Best buys’ and other recommended interventions for the prevention and control of non-communicable diseases. Geneva: World Health Organization; 2017.
Mitchell MS, Orstad SL, Biswas A, Oh PI, Jay M, Pakosh MT, et al. Financial incentives for physical activity in adults: systematic review and meta-analysis. Br J Sports Med. 2020;54(21):1259–68. https://doi.org/10.1136/bjsports-2019-100633.
World Health Organization. 2021 Physical activity factsheets for the European Union member states in the WHO european region. Copenhagen: WHO Regional Office for Europe; 2021. License: CC BY-NC-SA 3.0 IGO.
Ward M. Health-Enhancing Physical Activity (HEPA) promotion in health care settings - policy, practice & evidence. Copenhagen: WHO Regional Office for Europe; 2016.
Lobelo F, Young DR, Sallis R, Garber MD, Billinger SA, Duperly J, et al. Routine assessment and promotion of physical activity in healthcare settings: a scientific statement from the American Heart Association. Circulation. 2018;137(18):e495–522. https://doi.org/10.1161/cir.0000000000000559.
Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061. https://doi.org/10.1136/bmj.n2061.
Sallis RE, Baggish AL, Franklin BA, Whitehead JR. The call for a physical activity vital sign in clinical practice. Am J Med. 2016;129(9):903–5. https://doi.org/10.1016/j.amjmed.2016.05.005.
Koorts H, Eakin E, Estabrooks P, Timperio A, Salmon J, Bauman A. Implementation and scale up of population physical activity interventions for clinical and community settings: the PRACTIS guide. Int J Behav Nutr Phys Act. 2018;15(1):51. https://doi.org/10.1186/s12966-018-0678-0.
Koorts H, Bauman A, Edwards N, Bellew W, Brown WJ, Duncan MJ, et al. Tensions and paradoxes of scaling up: a critical reflection on physical activity promotion. Int J Environ Res Public Health. 2022;19(21). https://doi.org/10.3390/ijerph192114284.
Tabak RG, Khoong EC, Chambers DA, Brownson RC. Bridging research and practice: models for dissemination and implementation research. Am J Prev Med. 2012;43(3):337–50. https://doi.org/10.1016/j.amepre.2012.05.024.
Acknowledgements
Not applicable
Funding
This research received no external funding. C.S.S. is supported by the Portuguese Foundation for Science and Technology (SFRH/BD/139603/2018). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization, CSS, MNS, CG, and PJT; Methodology, CSS, CG, JE, BR, EVC and MNS; Data Curation and formal analysis, CSS, JE, and BR; writing—original draft preparation, CSS, CG, and MNS; writing—review and editing, CSS, CG, JE, BR, EVC, PJT, and MNS; Supervision, CG, PJT, and MNS. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA 2020 Checklist.
Additional file 2.
Search steam.
Additional file 3:
Critical appraisal of the included studies.
Additional file 4:
Codebook of the implementation determinants.
Additional file 5:
Detailed report of implementation determinants, with supporting extracted data.
Additional file 6.
Certainty assessment of the systematic review (SURE checklist).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Silva, C.S., Godinho, C., Encantado, J. et al. Implementation determinants of physical activity interventions in primary health care settings using the TICD framework: a systematic review. BMC Health Serv Res 23, 1082 (2023). https://doi.org/10.1186/s12913-023-09881-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09881-y