
Abstract
Background
Smart nursing homes (SNHs) integrate advanced technologies, including IoT, digital health, big data, AI, and cloud computing to optimise remote clinical services, monitor abnormal events, enhance decision-making, and support daily activities for older residents, ensuring overall well-being in a safe and cost-effective environment. This study developed and validated a 24-item Expectation and Acceptability of Smart Nursing Homes Questionnaire (EASNH-Q), and examined the levels of expectations and acceptability of SNHs and associated factors among older adults in China.
Methods
This was an exploratory sequential mixed methods study, where the qualitative case study was conducted in Hainan and Dalian, while the survey was conducted in Xi’an, Nanjing, Shenyang, and Xiamen. The validation of EASNH-Q also included exploratory and confirmatory factor analyses. Multinomial logistic regression analysis was used to estimate the determinants of expectations and acceptability of SNHs.
Results
The newly developed EASNH-Q uses a Likert Scale ranging from 1 (strongly disagree) to 5 (strongly agree), and underwent validation and refinement from 49 items to the final 24 items. The content validity indices for relevance, comprehensibility, and comprehensiveness were all above 0.95. The expectations and acceptability of SNHs exhibited a strong correlation (r = 0.85, p < 0.01), and good test-retest reliability for expectation (0.90) and acceptability (0.81). The highest tertile of expectations (X2=28.89, p < 0.001) and acceptability (X2=25.64, p < 0.001) towards SNHs were significantly associated with the willingness to relocate to such facilities. Older adults with self-efficacy in applying smart technologies (OR: 28.0) and those expressing a willingness to move to a nursing home (OR: 3.0) were more likely to have the highest tertile of expectations compared to those in the lowest tertile. Similarly, older adults with self-efficacy in applying smart technologies were more likely to be in the highest tertile of acceptability of SNHs (OR: 13.8).
Conclusions
EASNH-Q demonstrated commendable validity, reliability, and stability. The majority of Chinese older adults have high expectations for and accept SNHs. Self-efficacy in applying smart technologies and willingness to relocate to a nursing home associated with high expectations and acceptability of SNHs.
Similar content being viewed by others


Introduction
As the world’s second-largest economy, China is also grappling with the intricate challenge of rapid ageing [1]. According to a recent national survey (2020) based on the scale assessment for activities of daily living (ADLs) and instrumental activities of daily living (IADLs) [2], three levels were categorised based on the severity of dependency and older adults’ requirements for care. The study estimated that more than 20 million Chinese older adults were in need of minimal assistance with daily living activities, such as meal preparation and basic hygiene (level 1 dependency), 36 million needed moderate assistance with daily tasks, including cooking, shopping, and medication management (level 2 dependency), and 45 million were largely dependent on others for their daily living activities, requiring continuous supervision and assistance, such as those with severe cognitive or physical impairments (level 3 dependency), respectively. The one-child policy has directly impacted the availability of family caregivers, compounding the issue of inadequate care for Chinese older adults in their later years [3]. For the majority of older adults, dependency on assistance for daily living activities and cognitive impairments has become a significant life event, and these aspects lead to an increasing demand for nursing homes [4]. However, the quality of care provided in Chinese nursing homes is primarily influenced by policies, often falling short of meeting the demands of older adults in terms of having skilled caregivers, real-time monitoring, and continuous health assessment [5].
As sustainable strategies for promoting care for the ageing population, the use of smart technologies can address the escalating unmet healthcare needs of older adults and offset the inadequacy of medical resources to effectively improve the current healthcare system [6]. In hospital settings, smart technologies are used to enhance clinical decision-making [7], while in home-based care, they help with self-management and the remote monitoring of chronic diseases [8, 9]. In nursing home settings, technologies are predominantly implemented to provide person-centred care services and integrate medical services from remote hospitals [10]. The use of smart technologies holds the potential to support a substantial number of older adults in both home-based and nursing home-based care [11]. In 2014, the Ministry of Civil Affairs of the People’s Republic of China, the supervisory department for geriatric care, initiated the ‘Smart Elderly Internet of Things (IoT) Pilot Project’ to enhance the operation of SNHs [12]. In 2015, the Chinese government introduced the ‘Internet Plus’ plan to encourage technological innovation [13], encompassing projects related to IoT or Artificial Intelligence (AI) in safety monitoring, fall prevention, and disease detection for older adults. However, the concept of a SNH and the availability of smart technologies in nursing home settings remain ambiguous. Moreover, many older adults have a negative attitude towards smart technologies, perceiving them as challenging to use and being expensive [14]. Exploring the expectations and acceptability of SNHs within a defined service scope and associated technologies [10] among stakeholders, particularly older adults, will provide a better understanding of the future development and implementation of SNH models. Expectations, in this context, generally encompass the desires of consumers regarding what they expect a SNH to provide [15], while acceptability refers to the intention to use services when they are available and meet the criteria of target users willing to adopt SNHs [16].
Previous studies have often defined a SNH as either a smart building equipped with IoT networks [17], or the isolated application of smart technology within nursing home environment [18,19,20,21]. Specifically, a precise definition of SNHs and the comprehensive implementation of functional technologies is needed. A comprehensive scoping review has defined a SNH as characterised by the incorporating of functional information technologies, encompassing the IoT, digital health, big data, AI, cloud computing technologies, and information management system (IMS) that enable the monitoring of abnormal events, provision of remote clinical services, establishment of health information databases, enhancement of decision making processes, analysis of clinical data, and facilitation of activities of daily living for older residents [10]. It may integrate medical services from remote hospitals or healthcare experts, using telemedicine, mHealth, and other electronic clinical information, to manage complex health conditions among their residents and ensure their overall well-being within a safe and cost-effective environment [10]. Previous studies have investigated the willingness and associated factors of Chinese older adults to the conventional nursing homes [22, 23]. However, there is a lack of studies that have examined the expectations and acceptability of SNHs. It is crucial to thoroughly investigate the perspective of Chinese older adults regarding SNHs. This is necessary to ensure the successful development of innovative geriatric care models that meet the healthcare demands of China’s ageing population and are widely embraced.
Research questions
Drawing upon the defined SNH model [10], the following research inquiries were devised: 1) What factors are important to assess the expectations and acceptability of SNHs, and their psychometric property as a tool? 2) To what extent are Chinese older adults inclined to embrace the evidence-based SNH model? 3) What are the levels of expectation and acceptability exhibited by Chinese older adults towards the SNH model? 4) Is there an association between the sociodemographic characteristics of Chinese older adults and their levels of expectations and acceptability concerning SNHs?
Methods
In this study, an exploratory sequential mixed method (Fig. 1) was used to answer the research questions. There were no similar instruments or pre-existing questionnaires available to measure the expectations and acceptability towards SNHs. Hence, a newly developed instrument was designed based on the results of a qualitative study to assess the levels of expectation and acceptability of SNHs among Chinese older adults. Subsequently, a survey was conducted in four Chinese cities. The sociodemographic factors associated with expectations and acceptability of SNHs were also explored and examined. Guidelines for conducting and reporting mixed research in the field of counseling and beyond guided results reporting [24] (Additional file 1). In the mixed method approach, qualitative insights were derived from a developed questionnaire assessing the expectations and acceptability. Both quantitative and qualitative data were combined in the final analysis to enhance the depth of findings. The study protocol, a scoping review and the preceding qualitative study have been previously published [10, 25, 26].

Exploratory sequential mixed methods study design
Questionnaire development and validation
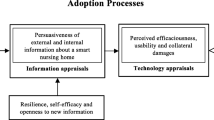
The questionnaire was developed as a measurement tool building on the conceptual framework (Fig. 2) derived from the ‘smart technology adoption behaviors of older consumers theory’ proposed by Golant [27], a scoping review [10], as well as the results of a qualitative study which has been published elsewhere [26]. According to the conceptual framework, the adoption of SNH emerges in response to unmet healthcare needs, resulting in unfulfilled expectations among older adults. The decision to embrace SNHs is underpinned by appraisals of information and technology. Older adults’ choices are influenced by their prior experiences with smart technologies and external sources of persuasiveness, including public media, friends, family members, and healthcare professionals (HCPs). The determinants shaping their technology appraisal encompass perceived efficaciousness, positive or negative usability, and the potential collateral damage associated with adopting smart technologies. Simultaneously, attributes specific to older adults, such as their resilience towards smart technologies, are linked to their acceptability of SNHs.

The coping process of Chinese older adults towards smart solutions in nursing homes
A qualitative case study was conducted using the snowball sampling method to collect data from a total of 34 participants until data saturation was achieved. Of these participants, 28 were older adults aged 60–75, residing in Hainan and Dalian, China, during the winter season. They were selected from six provinces to ensure a diverse representation of older adults. Additionally, six adult children were included in the study to explore their expectations and acceptability of SNHs. Semi-structured in-depth interviews and focus group discussions were conducted for data collection. Data were imported and managed using ATLAS.ti8 software. A framework method [28] was employed using inductive and deductive approaches to analyse the textual data. Furthermore, data were coded and categorised into themes. All items in the new questionnaire were derived from the interviews and previous scoping review through the mentioned analytical strategy. The questionnaire item design incorporated direct quotes from the qualitative data to ensure that the latter survey aligns authentically with the perspectives of the Chinese ageing population. Meanwhile, the concept of SNHs, captured from the scoping review was stated before the questionnaire to assist the respondents in sharing their perspectives on the expectation and acceptability of mart nursing homes. It included an explanation of it as a care model that provide continuous monitoring of its residents through information technologies, connect them with their remote HCPs, and integrate medical resources to satisfy the care needs of older residents. Additionally, information on sociodemographic characteristics, including age, place of residence, gender, health condition, income, type of insurance, educational attainment, number of children, and living partners, was collected from the respondents. Three items were included to measure respondents’ resilience to smart technologies, comprising familiarity with technologies, openness to new technology, and self-efficacy in applying smart technologies [27].
An expert panel, which included two statisticians, two family physicians, one public health physician, one nursing home operator, one business stakeholder, and three older adults, was invited to assess the content validity using the content validity index (CVI) for 49-item of the questionnaire [29]. This was done in line with the Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN checklist) guideline [30], which evaluates the relevance, comprehensibility, and comprehensiveness of a newly developed questionnaire. Subsequently, cognitive debriefing was conducted among ten older adults [31]. Of those, eight were selected from Dalian and two from Hainan community groups. Considering the diverse characteristics of the intended respondents, three participants with primary school education were recruited, three with junior or high school education, and remaining had university education. The research team organised an online group discussion where they introduced the purpose of the study and explained the concept of SNHs, along with the content of each item in the questionnaire. Participants were instructed to provide insights into their understanding of the questions, any ambiguous terms, and potential areas of confusion. The investigator (ZYY) recorded and clarified the responses for each question. For example, the investigator used a fixed probe to ask the participants, ‘Is this a correct choice that can reflect your response? Can you paraphrase this item in your own words based on your understanding? Can you elaborate on why you chose this answer?’. The frequency of problems encountered for each question would be gathered, such as difficulties in understanding and ambiguity of wording, and adjustments would be made accordingly. One session was carried out with a duration of approximately 2–3 h.
Structural validity was established through exploratory factor analysis (EFA), based on data collected from the survey respondents. The eigenvalue was set above 1, and items with a loading value below 0.40, as well as cross-loadings greater than 0.40 were dropped [32]. Subsequently, structural equation modelling (SEM) was utilised to evaluate model fit with the SPSS AMOS software. Internal consistency was assessed using Cronbach’s alpha. A Cronbach’s alpha exceeding 0.70 is considered indicative of good internal consistency for the questionnaire [33].
Construct validity (hypothesis-testing) was assessed by comparing responses towards the expectations and acceptability of SNHs with a single item regarding willingness to move to a nursing home (Yes or No) [22]. The expectations and acceptability scores were categorised into tertiles. The hypothesis posited that the highest tertile of expectations would exhibit an association with the willingness to move to a nursing home as evidenced by an a priori odds ratio of at least 2.0, while the highest tertile of acceptability would be linked to the willingness to move to a nursing home, reflecting a priori odds ratio of at least 3.0 [34]. It was also hypothesised that expectations and acceptability would be positively correlated, with a correlation coefficient r value of > 0.4.
A one-month intra-rater test–retest was performed among participants who answered and returned the second completed questionnaire. The participants were recruited from those who had the willingness to participate in the test–retest and provided their telephone numbers when they answered the questionnaire for the first time.
Quantitative study (survey)
Study setting
Quantitative data using surveys were collected in four major cities namely Xi’an, Nanjing, Shenyang, and Xiamen, representing the west, east, north, and south of China. In Xi’an, Nanjing, and Shenyang, the estimated older population comprises 18%, 22%, and 26%, respectively [35,36,37]. Meanwhile, the government of Xiamen has actively promoted smart healthcare initiatives to assist older adults in their activities of daily living [38].
Participants and sample size estimation
The selected older adults were within the age range of 60–75 years. Individuals residing in nursing homes, receiving palliative care, or experiencing cognitive impairment were excluded. Sample size calculation was conducted using PASS software. Based on an expected 10% level of acceptance of nursing homes among Chinese older adults [22], a 95% confidence level with a two-sided and 5% margin of error, the minimum required sample size was 139. However, for this study, a target sample size of 300 was set with inflation for non-response and incompletion rates. The data was collected from older adults who usually gather in public parks for group activities, such as morning or post-dinner exercise.
Data collection
A stratified random sampling method was used to identify participants. Eight enumerators (two in each city) recruited participants and asked them to suggest the ten most popular parks or communities where local older adults participate in physical activities. Subsequently, they recruited older adults from randomly selected public parks or community centres. In China, older adults typically visit public parks for collective activities, such as physical exercise and morning routines, or post-dinner dancing. Different age groups can be easily identified by the types of activities they engage in. For example, older adults aged 60–70 years usually join dancing groups, while older individuals prefer playing chess or engaging in conversations with others. Additionally, respondents were encouraged to provide their telephone numbers to enhance research credibility and facilitate participant recruitment for the intra-rater test-retest. During data collection, enumerators explained the concept of SNHs, which was stated on the questionnaire and checked the completeness of the questionnaires when all respondents returned them.
Data analysis
The IBM Statistical Package for Social Sciences (SPSS 26) software was used for data management and analysis. Qualitative variables were presented as frequencies and percentages. The expectations and acceptability of SNHs were categorised into tertiles.Chi-square tests were used to examine the associations among the sociodemographic factors, expectations and acceptability of SNHs, and the willingness to move to a nursing home. Multiple logistic regression models were utilised to analyse the association between the independent variables, including sociodemographic characteristics and older adults’ resilience to smart technologies, on expectations and acceptability of SNHs. Variables from the univariable regression analysis with a p-value < 0.20 in the expectation and acceptability domains were included in the multinomial logistic regression analysis. In all analyses, the significance level was set at 0.05. Statistical strategies to multicollinearity, data normality, and assumptions of the final model were checked.
Results
Questionnaire development and validation
The initial version of the questionnaire was crafted by synthesising qualitative data obtained from a scoping review and qualitative case study using both deductive and inductive analysis approaches, incorporating themes, codes, and subcodes [10, 26] (Additional file 2, A2-1). It comprised 24 items for the expectation domain, and 25 items pertaining to the acceptability domain. Among the 24 items in the expectation domain, five codes (subdomains) were identified from the qualitative phase. The subdomains are ‘quality of care supported by governments and societies’ with five items; ‘smart technology applications’ with seven items; ‘presence of a skilled HCP team’ with three items; ‘access and scope of basic medical services’ with six items; and ‘integration of medical services’ with two items. In the 25-item acceptability domain, six codes (subdomains) were identified, which encompass ‘perceived efficaciousness’ of SNHs with four items; ‘perceived positive usability’ with nine items; ‘perceived negative usability’ with two items; ‘perceived collateral damages’ with four items; ‘persuasiveness of external information’ with four items; and ‘persuasiveness of internal information’ with two items. Each item was measured on a 5-point Likert scale, where a response of 1 indicated the lowest levels of expectations or acceptability of SNHs, while a response of 5 indicated the highest levels of expectations or acceptability.
The CVI scores for relevance, comprehensibility, and comprehensiveness were 0.97, 0.96, and 0.95, respectively (Additional file 2, A2-2). These results were considered highly valuable [29]. The second version of the questionnaire had been reduced to 40 items from the initial 49 items (Additional file 2, A2-3) and named the Expectation and Acceptability of Smart Nursing Homes questionnaire (EASNH-Q). The item on willingness to move to a nursing home was moved to the sociodemographic characteristics section and all items were renumbered. All participants in the cognitive debriefing agreed with the item description and scale design for these 40 items without any problems. After undergoing the process of face and content validity, structural validity, internal consistency tests, one-month intra-rater test–retest, and construct validity were conducted using the data obtained from the latter survey among 264 respondents.
EFA identified three subdomains (three factors) for the underlying structure of expectations and these three factors were renamed as nursing care, medical services, and government and social support in relation to the service categories. EFA also identified three subdomains (three factors) for the acceptability structure and the three factors were categorised as perceived usability, perceived efficaciousness, and perceived collateral damages and negative usability (Additional file 2, A2-4). In confirmatory factor analysis (CFA), single-factor models indicated the presence of 24 remaining items. Of which, 10 items in the expectation domain and 14 items in the acceptability domain were considered adequate (Table 1; Fig. 3) (Additional file 2, A2-5). Cronbach’s alpha was 0.87 in the expectation domain, and it was 0.92 in the acceptability domain.

The assessment of model fit using the structural equation modelling (SEM)
Construct validity indicated by the strong correlation between the expectations and acceptability of SNHs Pearson’s coefficient of 0.85 (p< 0.01). Among the 264 respondents, 84 (31.8%) were unwilling to move to nursing homes, while 180 (68.2%) expressed a willingness to move (Table 2). Type of insurance, education, the degree of familiarity with technology, openness to technology, and self-efficacy in applying smart technologies were significantly associated with the willingness to move to nursing homes. The binary logistic regression analysis for expectations and acceptability in relation to the willingness to move to nursing homes presented that the odds of older adults in the higher tertiles of expectations for SNHs towards moving to nursing homes were higher compared to those with the lowest tertile scores (OR of 1.99, 95% CI 1.01–3.93 for the middle tertile and OR of 3.02, 95% CI: 1.18–7.73 for the highest tertile) (Table 3). Similarly, the odds of older adults with the higher tertiles of acceptability for SNHs towards moving to nursing homes were higher compared to those with the lowest tertile scores. (OR of 2.36, 95% CI 1.13–4.91 for the middle terile and OR of 2.43, 95% CI: 1.11–5.39 for the highest tertile).
In the test-retest reliability analysis, 52 participants (13 in each city) answered and returned the second completed EASNH-Q. More than half of them were women, the majority were aged 60–70. Five did not have a pension, two had no insurance, four had a primary school education, six had three or more children, and four lived alone without partners (Additional file 2, A2-6). The intraclass correlation coefficients (ICC) values for expectation and acceptability factors were 0.90 and 0.81, respectively (Additional file 2, A2-7).
Quantitative study (survey)
In total, 264 respondents completed the questionnaires, resulting in a response rate of 70%. The demographic characteristics of the respondents are presented in Table 4. The number of respondents in each age group (60–64 years old, 65–70 years old, and 71–75 years old) was similar. Among these respondents, over 60% reported having one or more chronic diseases. More than 90% had insurance coverage and 68.1% had a high school or university education. In addition, 56.8% had one child and only 9% lived alone. Approximately one-quarter (24.2%) of the respondents were familiar with technology, 71.2% had openness to technologies, and 63.6% had self-efficacy in applying smart technologies. The overall means (SD) for expectations and acceptability were 4.0 (0.60) (Min-Max: 2.0–5.0) and 4.0 (0.60) (Min-Max: 1.6–4.9), respectively. The associations between sociodemographic characteristics and expectations and acceptability of SNHs presented that the younger age, having insurance, a university level of education, openness to technology, and self-efficacy in applying smart technologies were significantly associated with expectations (Table 5). Older age, living with partners and children, openness to technology, and self-efficacy in applying smart technologies were significantly associated with acceptability (Table 5). Table 6 displays the comparisons between the highest tertile of the expectation group and the lowest tertile of the expectation group. Older adults with self-efficacy in applying smart technologies were 28 times more likely to have the highest tertile of expectation (OR: 28.02, 95% CI: 5.92-132.66), and those with willingness to move to a nursing home were 3 times more likely to have the highest tertile of expectation (OR: 2.98, 95% CI: 1.06–8.37). Meanwhile, older adults with self-efficacy in applying smart technologies were 14 times more likely to be in the highest tertile of acceptability compared between the highest tertile of the acceptability group and the lowest tertile group (OR: 13.80, 95% CI: 4.33–43.95). The multinomial logistic regression models revealed that 41.7% (Nagelkerke R2 = 0.417) and 32.2% (Nagelkerke R2 = 0.322) of the variances in the expectation domain and the acceptability domains, respectively.
Discussion
This is the first study in which an instrument was developed to assess the expectations and acceptability of SNHs among mainland Chinese older adults, both in general and in particular. It aims to examine their levels of expectations and acceptability towards SNHs, as well as to determine the sociodemographic factors associated with different categories of expectations and acceptability. The exploratory sequential mixed methods study design integrates various data sources offering strength to confirmatory results [39]. The study began with a qualitative phase, which explored the expectations and acceptability of a SNH model in general, and specifically among Chinese older adults and their family members. The qualitative phase mapped the knowledge bases for the development and validation of a 24-item EASNH-Q [40], and continued with a cross-sectional study in four major cities in China involving 264 respondents. Data integration was achieved through a data-building approach, in which the results from the qualitative phase and the survey were analysed and compared to understand complex phenomena, measure changes, and examine the hypothesis [24, 40]. The results from both qualitative and quantitative phases aligned with study design principles, variables exploration and analysis, and data interpretation. Many concordant findings, rather than discordant ones, were noted between the two phases. The former phase indicated the highest acceptance of moving to nursing homes as an alternative and a high level of agreeableness with external information persuasiveness for receiving healthcare benefits, such as media. A few discordant results in the later phase were related to a lower acceptance of moving to a nursing home and the family-oriented culture in healthcare decision-making as the trustworthy persuasiveness. Additionally, three items were generated from the emerging codes during the scoping review and content validity, including SNHs can provide better services to improve healthcare accessibility and availability, the preference of “human-centric” designs for the smart devices, and hospice care, were highly expected by the participants (Additional file 3).
In China, many similar questionnaires commonly focus on older adults’ willingness to move to conventional nursing homes. Two of these studies had larger samples, with 670 and 1003 Chinese older adults [22, 23], and more than half of their respondents were in aged 60–70, very similar to the main sample of this study. Additionally, more than half of the other studies’ respondents had a primary school education or lower in contrast to this study that had < 10%. In one study [22], data from an urban community showed that half of the respondents had a higher economic status which is similar to the respondents in this study (monthly pension: 1000–4000 CNY, $138–555). Regarding the proportion of willingness to move to a nursing home among Chinese older adults, this study had a higher acceptance rate (68.2%) compared to the other two previous studies (45.4–11.9%) [22, 23]. The higher acceptance rate reflects the increased demand for moving to a nursing home, particularly when older adults consider their disabilities [41]. It has been reported that older adults may choose to transition from home-based care to nursing homes with intensive supervision and more professional services due to the decline in bodily functions and the obstacles faced by family members who are unable to devote themselves to necessary or additional care [42]. As an alternative, nursing homes can provide 24-hour formal care and some medical services for older adults who require daily assistance and have complex health demands [43]. Moreover, the purpose of developing the EASNH-Q was to explore the expectations and acceptability of SNHs, making it a novel contribution. The item design of the EASNH-Q demonstrated good levels of relevance, comprehensibility, and comprehensiveness in assessing the expectations and acceptability of SNHs [44,45,46].
The expectations and acceptability of SNHs were explored among Chinese older adults who were interviewed in the qualitative phase. These expectations and acceptability were examined through a survey in the subsequent quantitative phase, providing empirical evidence of high levels. The survey sites selected from four different regions of mainland China represent the major group of the Chinese ageing population according to their family structures, health status, long-term care needs, and insurance schemes [47]. There were small variances in different cities when respondents answered the EASNH-Q (effect size: 0.34 − 0.32) (Additional file 4). The results showed that expectations were highly correlated with the acceptability of SNHs. Older adults from Nanjing, in the east of China, had the highest expectations of SNHs, and they also had the highest acceptability of SNHs. In contrast, older adults from Xiamen, in the south of China, had the lowest expectations and the lowest acceptability. These geographic differences among older adults may be attributed to their sociodemographic characteristics. For example, urban older adults living in environments more sustainable for an ageing population, with fewer children, higher income, and higher education have a better acceptability of nursing homes than those in rural areas who have more children, limited income, and lower education [48, 49].
In addition, the in-depth analysis of the response distribution for each item revealed that most of the questions had a ceiling effect (> 15%), except item for Q11, ‘persuasiveness of public media increases the acceptability of SNHs’ (3.8%). This reflects the report of Chinese older adults’ social network type to receive healthcare benefits, indicating that the media has less impact on appraising their health [50]. Meanwhile, the floor effect of each item was small (< 15%). The assessments of ceiling and floor effect indicate the ability of a questionnaire to distinguish among respondents at the extreme ends of the scale [51]. High ceiling effects, as observed in many of the items, may suggest a limited instrument range, measurement inaccuracy, or response bias [52]. However, no previous research has reported on the ceiling and floor effects on the expectations and acceptability of nursing homes in China. Nevertheless, the high ceiling and floor effects reflected and examined the results from the qualitative phase that all participants had a positive attitude towards SNHs [26].
It is believed that IoT, big data, and internet networks can provide quality services [53]. This belief was reflected in the responses to items Q1-5, particularly in real-time monitoring, disease prediction, electronic health records, and customised services. It is important to note that technology is not the primary reason for people deciding to move to nursing homes. Instead, technology acts as an assistant to the functions and care practices provided in nursing homes [54]. In China, more than half of older adults wish for nursing homes to provide medical services at a hospital level [22]. This study observed that many respondents had high expectations for collaboration between hospitals and SNHs to integrate medical services with remote hospitals. Moreover, Chinese older adults expected medical staff to be available at conventional nursing homes, as many nursing home residents are moderately dependent and at risk of fatal diseases [22, 55]. There were also high expectations of having trained caregivers, such as nurses and doctors in SNHs. Additionally, more than half of the respondents had high expectations of hospice care in SNHs because it is an essential part of all healthcare systems. This might be due to the general perception of the limited services and lack of accessibility of hospice care in the current nursing homes. For example, only 30.8% of nursing homes in Hebei province provided hospice care services [56].
Chinese older adults are influenced by the family-oriented culture when it comes to receiving and appraising information about their health [50]. The results were indicative of the same path that trustworthy health-related resources were typically found within family members, doctors, friends, and public media, as well as influenced by personal demands. Respondents showed a high acceptability of SNHs when they perceived the benefits and efficaciousness of using smart technologies. This perceived efficaciousness of technology generally involves a comparison between two options and the benefits received, such as comparing the quality of care and cost-effectiveness in SNHs versus conventional ones [27, 34]. Moreover, it has been commonly reported in previous studies that many older adults had negative attitudes towards adopting smart technologies due to the additional cost or the need to purchase expensive devices [14, 57, 58]. However, the high scores of items Q19-22 in the EASNH-Q confirmed that certain features of SNHs could increase older adults’ positive attitude and their consideration of adopting smart technologies. These features include the perceived necessity for health, ease of use, user-friendliness, convenience, and the “human-centric” design of smart solutions.
The final adjusted multivariable analysis showed that only self-efficacy among three items for testing the older adults’ resilience to smart technologies, including familiarity with technology and openness to technology [27], was more likely to influence the information and technology appraisals among Chinese older adults. The direct users of smart technologies designed and applied in nursing home settings have been revealed through the previous scoping review [10]. These users are nursing home residents (81%) and their HCPs (19%), such as nursing home staff and doctors in remote hospitals. Self-efficacy refers to an individual’s belief in their ability to successfully use smart technologies and older adults with self-efficacy in applying smart technologies may increase their willingness to adopt new solutions [59].
For other sociodemographic factors, such as age, income, and educational attainment, were not found to be significantly associated with the different categories of expectations and acceptability towards SNHs among Chinese older adults. These factors were previously reported in other studies to be directly associated with Chinese older adults’ willingness to move to a nursing home [22, 23], and the willingness to move to a nursing home was examined to be significantly associated with the highest tertile of expectations in this study.
This study employed several strategies to ensure research accuracy and credibility. Firstly, semi-structured, in-depth interviews, focus group discussions, and member checking were used for data collection in the qualitative study phase to ensure study credibility. A team of five investigators participated in data auditing, analysis, and coding discussions to authenticate the findings, ensuring the reliability of the study. In the quantitative phase, the survey sites chosen for data collection were selected to represent the west, east, north, and south of China. Eight onsite enumerators underwent training and were provided with a detailed study procedure to standardise the recruitment of participants and improve data quality. Data accuracy was cross-checked by the research team. However, this study has some potential limitations. Firstly, the concept of SNHs stated on the EASNH-Q was developed based on the informative literature, of which, most of the study population were from middle-income and high-income countries that may not be applicable to resource-challenged or low-income countries, as well as countries with limited internet access. Secondly, selection biases might have occurred, with qualitative study participants being Chinese older adults who were flown into Hainan and Dalian during the winter season, and quantitative study respondents coming from the four major cities [26]. This approach might not have captured all the essential factors necessary to measure the expectations and acceptability of SNHs among the entire Chinese ageing population, including other regions and rural areas in China, taking into consideration their multimorbidity and cultural differences. The findings should be generalised with caution to older adults residing in rural areas as they may have a lower acceptance of moving to a nursing home [22]. Moreover, the survey respondents in this study were selected among outdoors and able older adults, potentially missing specific groups of older people with limited mobility, economic disadvantages, or those who fall ill at home but still intend to move to nursing homes. In addition, the participants may find it difficult to answer the questions related to the acceptability of SNHs as a whole due to the non-existence of a SNH to refer to or a lack of experience using smart technologies for healthcare.
Conclusion
The significance of this study lies in the exploration of the expectations and acceptability of SNHs among Chinese older adults, through both qualitative and quantitative evidence leading to the 24-item EASNH-Q that demonstrated commendable validity, reliability, and stability. The rigorous development process establishes it as a reliable tool for measuring the levels of expectations and acceptability of SNHs. Self-efficacy in applying smart technologies links to the high expectations and acceptability of SNHs. The willingness to relocate to a nursing home increases the high expectations of SNHs.
A feasible SNH model presents a promising solution for addressing the challenges posed by the rapidly ageing society in China. The study results hold relevance for a wide range of stakeholders and audience with an interest in SNHs, including older adults, their family members, healthcare providers, nursing home personnel, policy-makers, and entrepreneurs in the smart device industry. Furthermore, the potential applicability of these findings extends beyond China, encompassing both developed and developing nations. Subsequent research efforts should aim to quantify the expectations and acceptability of SNHs within a larger and more diverse Chinese population considering various societal strata and potentially different countries. Gaining insights from a more extensive population base will enable a more comprehensive assessment of the determinants influencing expectations and acceptability of SNHs. This, in turn, will contribute to the development of a more effective SNH model that aligns with local settings and stakeholders’ requirements.
Availability of data and materials
The dataset supporting the results and conclusions of this article is included within the article and its additional files.
References
Tu W-J, Zeng X, Liu Q. Aging tsunami coming: the main finding from China’s seventh national population census. Aging Clin Exp Res. 2022;34(5):1159–63.
Gong J, Wang G, Wang Y, Chen X, Chen Y, Meng Q, Yang P, Yao Y, Zhao Y. Nowcasting and forecasting the care needs of the older population in China: analysis of data from the China Health and Retirement Longitudinal Study (CHARLS). Lancet Public Health. 2022;7(12):e1005-13.
Alpermann B, Zhan S. Population planning after the one-child policy: shifting modes of political steering in China. J Contemp China. 2019;28(117):348–66.
Gu D, Vlosky DA. Long-term care needs and related issues in China. Social Sci Health care Med 2008:51–84.
Xie W, Fan R. Towards ethically and medically sustainable care for the Elderly: the case of China. HEC Forum: 2020. Springer; 2020. pp. 1–12.
Ma B, Yang J, Wong FKY, Wong AKC, Ma T, Meng J, Zhao Y, Wang Y, Lu Q. Artificial intelligence in elderly healthcare: a scoping review. Ageing Res Rev. 2022;83:101808.
Mieronkoski R, Azimi I, Rahmani AM, Aantaa R, Terävä V, Liljeberg P. Salanterä SJIjons: the internet of things for basic nursing care—A scoping review. Int J Nurs Stud. 2017;69:78–90.
Marikyan D, Papagiannidis S, Alamanos E. A systematic review of the smart home literature: a user perspective. Technol Forecast Soc Chang. 2019;138:139–54.
Tun SYY, Madanian S, Mirza F. Internet of things (IoT) applications for elderly care: a reflective review. Aging Clin Exp Res 2020:1–13.
Zhao Y, Rokhani FZ, Sazlina S-G, Devaraj NK, Su J, Chew B-H. Defining the concepts of a smart nursing home and its potential technology utilities that integrate medical services and are acceptable to stakeholders: a scoping review. BMC Geriatr. 2022;22(1):1–34.
Bleda AL, Maestre R, Beteta MA, Vidal JA. AmICare: Ambient Intelligent and Assistive System for Caregivers Support. In: Proceedings – 16th International Conference on Embedded and Ubiquitous Computing, EUC 2018: 2018; 2018: 66–73.
Ministry of Civil Affairs Releases. Demonstration Project on the Application of Internet of Things for Smart Aging‘ http://news.21csp.com.cn/c3/201406/72132.html.
NationalReport. NationalReport〔2015〕No. 40, Guiding Opinions of the State Council on Actively Promoting “Internet Plus” Action. 2015.
Yusif S, Soar J, Hafeez-Baig A. Older people, assistive technologies, and the barriers to adoption: a systematic review. Int J Med Informatics. 2016;94:112–6.
Parasuraman A, Zeithaml VA, Berry LL. Servqual: a multiple-item scale for measuring consumer perc. J Retail. 1988;64(1):12.
Abbate S, Avvenuti M, Light J. Usability Study of a wireless monitoring system among Alzheimer’s disease elderly population. Int J Telemedicine Appl. 2014;2014:617495.
Roh EH, Park SC. A study on the quality of life improvement in fixed IoT environments: utilizing active aging biomarkers and big data. Qual Innov Prosperity. 2017;21(2):52–70.
Li H. Obstacles and countermeasures in the process of Smart Aging in Tianjin Nursing Homes (CN). Manage Insight. 2017;15:132–4.
Huang Z, Chen Zhuo, Liu Z. Design of Integrated Management System for Intelligent Nursing Home. Electron Sci Technol. 2015;28(11):132–4.
Lu T. Research on Intelligent Elderly problems and countermeasures (CN). Hebei Normal University; 2016.
Huang Y. Research on Key Technologies of Intelligent Nursing Home Control System Based on Deep Learning (CN). Master thesis North University of China (Shanxi); 2019.
Huang Z, Liu Q, Meng H, Liu D, Dobbs D, Hyer K. Conner KOJPo: factors associated with willingness to enter long-term care facilities among older adults in Chengdu. China. PLoS One. 2018;13(8):e0202225
Wang Z, Xing Y, Yan W, Sun X, Zhang X, Huang S, Li L. Effects of individual, family and community factors on the willingness of institutional elder care: a cross-sectional survey of the elderly in China. BMJ open. 2020;10(2):e032478.
Leech NL, Onwuegbuzie AJ. Guidelines for conducting and reporting mixed research in the field of counseling and beyond. J Couns Dev. 2010;88(1):61–9.
Zhao Y, Sazlina S-G, Rokhani FZ, Su J, Chew B-H. The expectations and acceptability of a smart nursing home model among Chinese elderly people: a mixed methods study protocol. PLoS ONE. 2021;16(8):e0255865.
Zhao Y, Sazlina S-G, Rokhani FZ, Su J, Chew B-H. The expectations and acceptability of a smart nursing home model among Chinese older adults and family members: a qualitative study. Asian Nurs Res. 2023;17(4):208–18.
Golant SM. A theoretical model to explain the smart technology adoption behaviors of elder consumers (Elderadopt). J Aging Stud. 2017;42:56–73.
Gale NK, Heath G, Cameron E, Rashid S. Redwood SJBmrm: using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117.
Yusoff MSB. ABC of content validation and content validity index calculation. Resource. 2019;11(2):49–54.
Mokkink LB, Terwee CB, Knol DL, Stratford PW, Alonso J, Patrick DL, Bouter LM, De Vet HC. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC Med Res Methodol. 2010;10(1):1–8.
Miller K, Willis G, Eason C, Moses L, Canfield B. Interpreting the results of cross-cultural cognitive interviews: a mixed-method approach. 49741. 2005;11:79–92.
Samuels P. Advice on exploratory factor analysis. 2017.
Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48(6):1273–96.
Li J, Ma Q, Chan AH, Man S. Health monitoring through wearable technologies for older adults: Smart wearables acceptance model. Appl Ergon. 2019;75:162–9.
Shaanxi’s elderly population. Over 60 years old reaches 7,023,700, accounting for 18.12% of the total population (CN) http://news.hsw.cn/system/2020/1223/1275960.shtml.
One out of every five people in. Nanjing is an elderly person (CN) https://jsnews.jschina.com.cn/nj/a/202010/t20201031_2657900.shtml.
Shenyang. free services for the elderly from special families in 100 pilot communities (CN). http://xinhuanet.com/politics/2021-03/11/c_1127199593.htm.
Fujian Xiamen. : Intelligent Elderly Care escorting the elderly in their twilight years http://m.xinhuanet.com/2019-10/06/c_1125074114.htm.
Castro FG, Kellison JG, Boyd SJ, Kopak A. A methodology for conducting integrative mixed methods research and data analyses. J Mix Methods Res. 2010;4(4):342–60.
Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134–56.
Xu X, Chen L. Projection of long-term care costs in China, 2020–2050: based on the bayesian quantile regression method. Sustainability. 2019;11(13):3530.
Zhang Y, Goza FW. Who will care for the elderly in China? A review of the problems caused by China’s one-child policy and their potential solutions. J Aging Stud. 2006;20(2):151–64.
Sanford AM, Orrell M, Tolson D, Abbatecola AM, Arai H, Bauer JM, Cruz-Jentoft AJ, Dong B, Ga H, Goel A. An international definition for nursing home. J Am Med Dir Assoc. 2015;16(3):181–4.
Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. 2018;6:149.
Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):80.
Kline R. Principles and Practice for Structural Equation Modelling (3rd Eds). 2011.
Chen S. Aging with Chinese characteristics: a public policy perspective. Ageing Int. 2009;34:172–88.
Zhang L, Zeng Y, Fang Y. The effect of health status and living arrangements on long term care models among older Chinese: a cross-sectional study. PLoS ONE. 2017;12(9):e0182219.
Wang H, Guan Y, Hu R, Bragg F, Yu M, Zhong J. Willingness for community-based and institutional eldercare among older adults: a cross-sectional study in Zhejiang, China. BMJ open. 2022;12(4):e055426.
Li T, Yang YC, Zhang Y. Culture, economic development, social-network type, and mortality: evidence from Chinese older adults. Soc Sci Med. 2018;204:23–30.
Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, Bouter LM, de Vet HC. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42.
Bernstein DN, Houck JR, Hammert WC. A comparison of PROMIS UE versus PF: correlation to PROMIS PI and depression, ceiling and floor effects, and time to completion. J Hand Surg. 2019;44(10):901. e901-901. e907.
Li S, Tang Y. A Simple Framework of Smart Geriatric Nursing considering Health Big Data and User Profile. Comput Math Methods Med. 2020;2020:5013249.
Chang F, Kuoppamäki S, Östlund B. Technology scripts in care practice: a case study of assistant nurses’ use of a social alarm system in Swedish nursing homes. Digit Health. 2022;8:20552076221089077.
Chen S, Cui Y, Ding Y, Sun C, Xing Y, Zhou R, Liu G. Prevalence and risk factors of dysphagia among nursing home residents in eastern China: a cross-sectional study. BMC Geriatr. 2020;20(1):1–10.
Yang N, Gao D, Zhang H. Status and strategies of Institutionalized Elderly Care in the context of Medical Care Integration in Baoding City (CN). Med Res Educ. 2018;35(2):45.
Pal D, Funilkul S, Charoenkitkarn N, Kanthamanon P. Internet-of-things and Smart Homes for Elderly Healthcare: an end user perspective. IEEE Access. 2018;6:10483–96.
Wong JK, Leung JK. Modelling factors influencing the adoption of smart-home technologies. Facilities. 2016;34(13/14):906–23.
Pajares F. Current directions in self-efficacy research. Adv Motivation Achievement. 1997;10(149):1–49.
Acknowledgements
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Author information
Authors and Affiliations
Contributions
ZYY formulated and assumed overall responsibility for the study’s conduct. FKR, SGS and BHC participated in the research’s design phase. SJ engaged in both qualitative data collection and statistical analysis. FZR, an expert in gerontechnology, served as one of the investigators contributing to the evaluation and appraisal of the technical aspects. KC oversaw the statistical analysis, while SGS and BHC validated the study’s qualitative and quantitative data, methodological design, and provided supervision throughout the research process. All authors have made significant intellectual contributions to the study’s development and have granted their approval for the final manuscript’s submission to the journal.
Corresponding author
Ethics declarations
Ethics approval and consent to participates
Ethical approvals for this study have been obtained from the Ethics Committee for Research Involving Human Subjects, Universiti Putra Malaysia, Malaysia (UPM/TNCPI/RMC/JKEUPM/1.4.18.2, 28/11/2020) and Hainan Medical University, China (IYLIJ-2020-021, 03/09/2020). The respondent’s Information Sheet was provided, and Informed Consent Form completed before participation in this study. All methods were performed in accordance with the Declaration of Helsinki and other relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
The Checklist of Guidelines for Conducting and Reporting Mixed Research for Counselor Researchers.
Additional file 2.
Questionnaire Development and Validation Process.
Additional file 3.
The Combination and Comparison among Qualitative and Quantitative Data.
Additional file 4.
Comparing the Variances in Cities.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, Y., Sazlina, SG., Rokhani, F.Z. et al. The expectations and acceptability of a smart nursing home model among Chinese older adults: a mixed methods study. BMC Nurs 23, 40 (2024). https://doi.org/10.1186/s12912-023-01676-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-023-01676-0