
Abstract
Background
Coronary angiography is the gold standard for the diagnosis of coronary artery disease. This intervention is nevertheless a source of anxiety for the patient both by its discomfort and by the consequences linked to the discovery of potential diseases.
Objectives
The aim of this study was to determine the effectiveness of hypnosis in reducing anxiety in patients undergoing coronary angiography.
Methods
One hundred sixty-nine patients with planned coronary angiography and no history of coronary angiography were randomized to a hypnosis or control group. Patients in the hypnosis group underwent a hypnosis session with self-hypnosis posthypnotic suggestions, while those in the control group had a conversational interview with the hypnotherapist. The primary endpoint was pre-exam anxiety level assessed by the Spielberger State-Trait Anxiety Inventory (STAI-Y A).
Results
Performing a hypnosis session did not result in a significant decrease in anxiety before the intervention. Age, high trait anxiety, high state anxiety the day before, and belief that hypnosis works in general were associated with increased anxiety before the procedure. No adverse events were reported after hypnosis. There was no statistically significant difference between the 2 groups for the occurrence of complications of the intervention.
Conclusion
In this study, performing a hypnosis session before coronary angiography did not reduce the state of anxiety measured just before the intervention. In all cases, the hypnotic experience appears to be positive for the patient, encouraging further research efforts.
Trial registration
The research protocol has been registered on the ClinicalTrials.gov registry (NCT02818101; 29/06/2016) and with the ANSM (IDRCB 2016-A00205-46; 02/02/2016).
Similar content being viewed by others


Background
Coronary angiography, a medical imaging technique used in cardiology to visualize the coronary arteries in the event of suspected coronary disease, has experienced spectacular growth over the past thirty years [1], in particular with the advent of radial puncture to replace femoral puncture. This interventional procedure is increasingly replacing gold standard surgical treatments. Percutaneous endoluminal revascularization techniques have also established themselves as a major treatment for acute and chronic coronary insufficiency [2, 3].
Coronary angiography is most often performed under local anesthesia [4]. Indeed, it is important to know during the intervention if the patient feels chest pain (which may indicate coronary injury). However, the absence of general anesthesia can be a source of anxiety for patients, which in itself can lead to adverse events [5, 6]. In addition, the procedure, which is usually painless, can become painful at different stages of the test: at the time of the puncture, during the progression of the probes along tortuous, spastic or highly calcified arteries, or during the placement of stent. In general, whether performed as an emergency or as a scheduled procedure, there is preoperative anxiety [7]. Anxiety can also affect the success of the procedure [8]. The diagnosis and its consequences can also be a source of stress for patients [9]. In the literature, preoperative anxiety is known as the most important and independent prognostic factor for mortality in patients over 70 years of age during cardiac surgery [10].
The State-Trait Anxiety Inventory (STAI) is a commonly used measure of trait and state anxiety (Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983). It can be used in clinical settings to diagnose anxiety and to distinguish it from depressive syndromes.
It has 20 items for assessing trait anxiety and 20 for state anxiety. State anxiety items include: “I am tense; I am worried” and “I feel calm; I feel secure.” Trait anxiety items include: “I worry too much over something that really doesn’t matter” and “I am content; I am a steady person.” All items are rated on a 4-point scale (e.g., from “Almost Never” to “Almost Always”). Higher scores indicate greater anxiety. The STAI is appropriate for those who have at least a sixth-grade reading level. STAI-Y A is commonly used to assess anxiety prior to cardiac catheterization combined with management techniques with the goal of reducing perioperative and pro-procedural anxiety. Music therapy is the most frequently evaluated method and it shows a significant decrease in STAI-Y A [11].
Several procedures have already been evaluated to reduce anxiety in patients before and during coronary angiography, including massage, music therapy, and aromatherapy [11,12,13,14,15,16,17,18]. Hypnosis is too one of the alternative medicines that has been evaluated. Hypnosis is a state of consciousness in which attention is focused and peripheral awareness reduced resulting in a high capacity to respond to suggestions [19]. This process can have a protective effect on pain, called hypnoanalgesia. It also reduces anxiety during therapeutic or diagnostic medical procedures [20,21,22,23,24,25]. A 2004 study of coronary angioplasty alone also compared hypnosis to drug sedation without significant results [26]. In addition, studies show that patients managed by hypnosis are more observant and the procedures are shorter by 45 min than for the control group; allowing greater operator comfort [27].
A recent review of the literature concluded that “the use of hypnosis during a surgical intervention or during a medical or interventional radiology act makes it possible to reduce the consumption of sedatives and/or analgesics during surgery [28, 29]. Thus, there is already some evidence for reducing the use of analgesics but not yet for reducing anxiety, especially before coronary angiography.
The objective of our study is to determine the effectiveness of hypnosis on anxiety before coronary angiography.
Method
Study population
The patients were recruited between March 20, 2016 and July 26, 2017 at the Metz Thionville Regional Hospital Center. Their hospitalization in cardiology was scheduled for the performance of a coronary angiography without emergency indication. The patients did not receive any systematic premedication for anxiolytic purposes. Patients who had undergone prior coronary angiography were not included, as past experiences may alter emotional state. Patients included were adults (≥ 18 years old) who underwent coronary angiography with or without stenting during the procedure. The exclusion criteria were: non-French speaking patients and/or cognitive disorders, and/or deaf or hard of hearing, and/or under legal protection, and/or psychiatric history of psychosis.
Procedures
The day before the examination, a pre-inclusion visit was carried out by a cardiologist. An information document and a non-objection form were given to the patient. The patients included were randomly divided into two arms: the hypnosis group and the control group. Only the hypnotherapist was aware of the outcome of the draw. The cardiology department and the angiography technical platform teams were blind.
On the morning of the intervention, the patients in the hypnosis group underwent a hypnosis session with post-hypnotic suggestions in self-hypnosis to be carried out during the coronary angiography. The hypnosis session was the same for all patients with a script written for the study. The session lasted 15 min. It included visual induction and catalepsy techniques with the suggestion of a safe place where the patient treated the part of the body where he felt anxiety. A post-hypnotic suggestion was introduced at the end of the session, with a brief explanation of how to do it independently during coronary angiography with authorization to enter and exit hypnosis at their convenience to answer questions from caregivers. The purpose of the post-hypnotic suggestions was to facilitate self-hypnosis in the coronary angiography room so that the patient could manage their anxiety and pain. This session took place in the patient's room, before leaving for the coronary angiography department.
The hypnotherapists participating in the study were 4 emergency physicians, a pediatric nurse and an anesthetist nurse. All were trained in an institute recognized by the Francophone Confederation of Hypnosis and Brief Therapies and had at least 2 years of experience.
Patients in the control group had a conversational interview with one of the same hypnotherapists.
State anxiety and trait anxiety were measured in both groups the day before the procedure. State anxiety was measured again immediately before performing coronary angiography. Hemodynamic parameters (blood pressure and heart rate) were monitored (1) the day before surgery, (2) the morning of surgery in the patient's room, (3) immediately before coronary angiography, (4) immediately after coronary angiography and (5) the next day. Pain was assessed using a Visual Analogue Scale (VAS) the day before surgery, on arrival in the procedure room, on leaving the procedure room and the day after the intervention. Depending on the clinical situation, the operator could prescribe an anxiolytic (midazolam) and/or analgesic (paracetamol, morphine) treatment. The treatments and the occurrence of side effects were recorded in the file. At the end of the examination, the comfort of the operator was measured by a Likert scale of 1 to 5 points (1 meaning "very uncomfortable" and 5 the most comfortable). This score was collected by the coronary angiography nurse at the end of the procedure. The cardiologist was also asked to give his opinion on whether the patient belonged to the hypnosis or control group.
Patients were contacted at 1 month post-procedure to rate their overall satisfaction using a 1–5 point Likert scale (1 worst, 5 best). How satisfied are you with your management of coronary angiography?) Their opinion on the effectiveness of hypnosis on themselves as well as on the general population was collected.
Endpoints
The primary endpoint was the patient's level of anxiety before coronary angiography using the SPIELBERGER’s inventory (STAI-Y A). The secondary endpoints were haemodynamic parameters, the use of anxiolytic or analgesic treatments and their respective dosages, pain assessment, operator comfort and patient satisfaction with their treatment.
Supervision of the study
This randomized, single-blind, single-center study was designed by the principal investigator (N.G.) and methodologist (C.G.). The research protocol has been registered on the ClinicalTrials.gov registry (NCT02818101; 29/06/2016) and with the ANSM (IDRCB 2016-A00205-46; 02/02/2016). The Metz Thionville Regional Hospital Center sponsored and funded the trial. The research protocol was approved by the East-III Personal Protection Committee. The data was processed at the hospital's Clinical Research Support Platform. The methodologist (C.G.) checked the completeness and quality of the data, and performed statistical analyses.
Statistical analysis
The sample size (85 patients per group) necessary to reach a power of 90% with an alpha risk of 5%, was calculated from the literature, which made it possible to estimate an expected score of 50 on STAI-Y A (standard deviation 10) for the control group and a clinically relevant difference of 5 points between the two groups 26,27.
The results are presented as median and ranges for qualitative data or as numbers and percentages for quantitative data. The hypnosis (experimental) and control groups were defined by intention to treat. The comparison between the two groups was carried out using Wilcoxon tests for the quantitative variables and Fisher's exact tests for the qualitative variables. A multivariate generalized linear model was used to identify factors that may influence the STAI Y A score before coronary angiography (age, sex, group, anxiety trait, anxiety state the day before, belief in the effectiveness of hypnosis in general and belief in the effectiveness of hypnosis for its own sake). The significance threshold was set at 5%. Bonferroni's corrections were applied for multiple tests where applicable. All analyzes were performed with SAS/STAT software version 9.4 (SAS Inst., Cary, NC).
Results
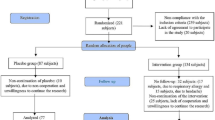
A total of 169 patients were included in the analysis: 85 patients in the hypnosis group and 84 in the control group (Fig. 1). One patient initially randomized to the control group was excluded before the end of the study because he did not fulfill the inclusion criteria. Patient characteristics were similar between sthe two groups (Table 1), except for the response to the question "Do you think hypnosis works, in general?" to which more patients in the hypnosis group answered "no."

Patient Inclusion and Follow-up Diagram
The STAI-Y A immediately before coronary angiography was 45 (range: 35–73) in the hypnosis group and 46 (36–74) in the control group (Table 2). This difference was not statistically significant. The distribution of scores in the two groups is shown in Fig. 2. Midazolam was used in 9 patients (11%) in the hypnosis group versus 14 patients (17%) in the control group, this difference was not significant (Table 2). There was no significant difference between the 2 groups regarding the occurrence of adverse events, pain, operator satisfaction, and the operator's opinion of whether the patient belonged to the hypnosis group or the control group (Table 2).

Comparison of anxiety score distributions (STAI-Y A) immediately before coronary angiography between the Hypnosis group (N = 85) and the Control group (N = 84)
In multivariate analysis (Table 3), the state of anxiety before coronary angiography was shown to decrease with age (p = 0.001) and with the belief that hypnosis works in general (p = 0.048). It has been shown to increase with trait anxiety (p = 0.03) and with state anxiety the day before (p < 0.0001). Gender and the belief that hypnosis works on himself were not significantly associated. An interaction between hypnosis group and beliefs about hypnosis was tested and was not significant (p = 0.10).
Telephone follow-up at 1 month showed no difference in patient satisfaction with their care (Table 4). In contrast, more patients in the hypnosis group responded that they thought hypnosis was effective on them compared to the control group (p = 0.003).
For hemodynamic parameters, heart rate was identical in both groups (Fig. 3A). Systolic blood pressure appeared slightly lower in the hypnosis group, but the differences were not statistically significant (Fig. 3B). Diastolic blood pressure showed no difference between the groups.

A and B Heart rate and blood pressure evolution in the hypnosis (N = 85) and control (N = 84) groups. Error bars represent 95% confidence intervals. No significant differences exist between groups at the different time points
Discussion
To our knowledge, our study is the first to date to evaluate hypnosis by STAI before coronary angiography. It shows that carrying out a hypnosis session with self-hypnosis suggestions before coronary angiography did not result in a significant drop in the state anxiety score. With a median score of 45 in the hypnosis group and 46 in the control group, the anxiety levels of the patients included could be considered “average” [30]. These values are higher than the norms reported for patients in medical stress situations such as patients hospitalized for various organic diseases, or undergoing medical examinations or surgery [30]. However, our results are in agreement with those of Lang et al., for patients hospitalized for a biopsy under hypnosis with suspicion of breast cancer or to perform a transesophageal ultrasound examination [21, 31]. The anxiety state score before the intervention, with alternative medicine, is on average comparable to that observed in our study [11, 14,15,16,17].
The lack of effectiveness of hypnosis in our study may be due to the timing of the assessment. Indeed, due to the constraints of the coronary angiography procedure, anxiety could not be measured during the procedure. It may also be due to the choice of the evaluation method. Indeed, if hypnosis is effective against anxiety, its statistical proof seems to be provided by an evaluation throughout the intervention and not in the moments preceding it [21, 23, 32, 33]. The patients were subjected to the Spielberger’s inventory on their arrival in the coronary angiography room, therefore before initiating a process of self-hypnosis. The evaluation carried out here therefore probably evaluates the effects of morning management and not the effectiveness of hypnosis during coronary angiography. This is in agreement with the results reported in several randomized clinical trials using STAI and involving interventional medicine showing a decrease in anxiety during an invasive examination but without significant difference in pre-interventional or during the first stages of the procedure. Lang et al., who also used the Spielberger inventory, found no significant difference in state anxiety scores before the procedure as well as during the first 0–15 min time interval [33]. A simple numerical rating scale is more sensitive to hypnosis-induced changes in anxiety [21, 32, 33]. Other scales, such as the Beck Anxiety Inventory or the Hamilton Anxiety Scale, also lead to the same conclusion [23]. These results therefore raise the possible interest of hypnosis during pre-coronary angiography since hypnosis showed a clear superiority compared to the groups receiving other additional measures such as "structured attention" or empathy [21, 32].
However, the main obstacle to the use of these techniques remains skepticism, maintained by the lack of scientific evidence, as it is difficult to measure the effectiveness of hypnosis or self-hypnosis, but also by the pejorative connotation disseminated, among others, by the entertainment world [34]. If self-hypnosis seems to be a promising tool for adapting to situations felt difficult (as demonstrated by Peter C. Keil in 2018 on chronic pain in hospitalized patients [35], its effectiveness must be objectively measured by standardized measures to expand its use and teaching. Our study found that patients' belief that "hypnosis works in general" prior to coronary angiography significantly influenced pre-intervention anxiety, regardless of the group to which they were assigned. This raises two important points: on the one hand, the beliefs and opinions of the patient vis-à-vis hypnosis and, on the other hand, the “hypnosis” label of the study. The general public develops ideas and expectations from different sources, including about medical care [36]. The cognitive model of hypnosis explains that variables such as participant motivation, beliefs or expectations are keys for patients' hypnotic receptivity [37, 38]. According to some authors, the reinforcement of these variables makes it possible to facilitate hypnotic reactivity [39]. On the other hand, Gandhi and Oakley highlighted the impact of the “hypnosis” label, whose title alone plays an anxiolytic role [40].
As observed by Dufresne et al., our study shows that one month after treatment, patients' opinions were influenced by the hypnotic experience [41]. This difference between the two arms of the study may suggest a use of self-hypnosis in the experimental group during the procedure. In any case, the improvement of the opinion regarding the hypnosis represents a positive reinforcement for the subsequent management. This hypothesis will require an evaluation of the effectiveness of hypnosis in patients who have previously benefited from this approach in the same procedure to confirm this hypothesis.
Study limitations
Our study has several limitations. First, it is monocentric and therefore there is a risk of bias of non-representativeness of practices and population. However, clinical activity within Mercy Hospital's cardiology department is significant, with 4,500 coronary angiograms and 2,314 percutaneous coronary angioplasties performed in 2016. In addition, the study included the intervention of 6 different cardiologists and was also carried out with the intervention of 6 health personnel qualified in hypnosis. Therefore, given the number of patients and operators, we believe that our results can be extrapolated to other centers.
Second, our study could not be double-blind because the hypnotherapist had to know whether to perform a hypnosis session or an interview with the patient. In order to avoid any follow-up bias, it would seem appropriate that the intervention in the control group not be limited to a simple interview with the hypnotherapist but also by another unconventional technique.
Third, pain assessment was only performed at peri-procedural times. It is therefore possible that such an assessment was not suitable since literature reviews highlight the positive effects of hypnosis on pain during medical or surgical procedures and often find no difference in anxiety before the procedure as in our study [21, 22, 32, 33, 42,43,44]. Therefore, it would have been more appropriate to assess pain by VAS during the procedure. It would also have been interesting to assess whether the patient had used self-hypnosis during the intervention by questioning him afterwards. These elements will have to be taken into account in another study. Finally, if none of our patients received specific premedication, the patients' usual treatment was not defined as an exclusion criterion. Under these conditions, patients on anxiolytics (benzodiazepines, antidepressants, etc.) could be included, which may induce a bias. However, these practices are usual in the coronary angiography center in which the study was conducted and we did not wish to modify them.
Conclusion
In the present study, performing a hypnosis session upstream of a coronary angiography, with posthypnotic suggestions in self-hypnosis to be performed during the procedure, failed to reduce the anxiety state measured immediately before the procedure, compared to a simple conversational interview with the hypnotherapist. Factors associated with lower state anxiety before the procedure were age, trait anxiety, and believing that hypnosis is an effective technique in general.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Bruschke AVG, Sheldon WC, Shirey EK, Proudfit WL. A half century of selective coronary arteriography. J Am Coll Cardiol. 2009;54(23):2139–44. https://doi.org/10.1016/j.jacc.2009.06.051.
Aversano T, Aversano LT, Passamani E, et al. Thrombolytic therapy vs primary percutaneous coronary intervention for myocardial infarction in patients presenting to hospitals without on-site cardiac surgery: a randomized controlled trial. JAMA. 2002;287(15):1943–51.
Trikalinos TA, Alsheikh-Ali AA, Tatsioni A, Nallamothu BK, Kent DM. Percutaneous coronary interventions for non-acute coronary artery disease: a quantitative 20-year synopsis and a network meta-analysis. Lancet Lond Engl. 2009;373(9667):911–8. https://doi.org/10.1016/S0140-6736(09)60319-6.
Meyer P, Barragan P, Blanchard D, et al. Recommendations of the French Cardiac Society concerning the education of physicians performing coronarography and angioplasty, organization and equipment of coronarography and coronary angioplasty centers. Arch Mal Coeur Vaiss. 2000;93(2):147–58.
Astin F, Jones K, Thompson DR. Prevalence and patterns of anxiety and depression in patients undergoing elective percutaneous transluminal coronary angioplasty. Heart Lung J Crit Care. 2005;34(6):393–401. https://doi.org/10.1016/j.hrtlng.2005.05.002.
Wang G, Cui J, Wang Y, et al. Anxiety and adverse coronary artery disease outcomes in Chinese patients. Psychosom Med. 2013;75(6):530–6. https://doi.org/10.1097/PSY.0b013e3182984317.
Amouroux R, Rousseau-Salvador C, Annequin D. L’anxiété préopératoire : manifestations cliniques, évaluation et prévention. Ann Méd-Psychol Rev Psychiatr. 2010;168(8):588–92. https://doi.org/10.1016/j.amp.2009.10.017.
Fuzier R, Lavidale M, Bataille B, Richez A-S, Maguès J-P. Anxiety: an independent factor of axillary brachial plexus block failure? Ann Fr Anesth Reanim. 2010;29(11):776–81. https://doi.org/10.1016/j.annfar.2010.08.010.
Sullivan MD, LaCroix AZ, Spertus JA, Hecht J. Five-year prospective study of the effects of anxiety and depression in patients with coronary artery disease. Am J Cardiol. 2000;86(10):1135–8. https://doi.org/10.1016/S0002-9149(00)01174-7.
Williams JB, Alexander KP, Morin J-F, et al. Preoperative anxiety as a predictor of mortality and major morbidity in patients aged >70 years undergoing cardiac surgery. Am J Cardiol. 2013;111(1):137–42. https://doi.org/10.1016/j.amjcard.2012.08.060.
Jayakar JP, Alter DA. Music for anxiety reduction in patients undergoing cardiac catheterization: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2017;28:122–30. https://doi.org/10.1016/j.ctcp.2017.05.011.
Peng S, Ying B, Chen Y, Sun X. Effects of massage on the anxiety of patients receiving percutaneous coronary intervention. Psychiatr Danub. 2015;27(1):44–9.
Forooghy M, Mottahedian Tabrizi E, Hajizadeh E, Pishgoo B. Effect of music therapy on patients’ anxiety and hemodynamic parameters during coronary angioplasty: a randomized controlled trial. Nurs Midwifery Stud. 2015;4(2):e25800. https://doi.org/10.17795/nmsjournal25800.
Bally K, Campbell D, Chesnick K, Tranmer JE. Effects of patient-controlled music therapy during coronary angiography on procedural pain and anxiety distress syndrome. Crit Care Nurse. 2003;23(2):50–7.
Goertz W, Dominick K, Heussen N, vom Dahl J. Music in the cath lab: who should select it? Clin Res Cardiol. 2011;100(5):395–402. https://doi.org/10.1007/s00392-010-0256-1.
Hamel WJ. The effects of music intervention on anxiety in the patient waiting for cardiac catheterization. Intensive Crit Care Nurs. 2001;17(5):279–85. https://doi.org/10.1054/iccn.2001.1594.
Taylor-Piliae RE, Chair S-Y. The effect of nursing interventions utilizing music therapy or sensory information on chinese patients’ anxiety prior to cardiac catheterization: a pilot study. Eur J Cardiovasc Nurs. 2002;1(3):203–11. https://doi.org/10.1016/S1474-5151(02)00037-3.
Cho M-Y, Min ES, Hur M-H, Lee MS. Effects of aromatherapy on the anxiety, vital signs, and sleep quality of percutaneous coronary intervention patients in intensive care units. Evid-Based Complement Altern Med ECAM. 2013;2013:381381. https://doi.org/10.1155/2013/381381.
Elkins GR, Barabasz AF, Council JR, Spiegel D. Advancing research and practice: the revised apa division 30 definition of hypnosis. Am J Clin Hypn. 2015;57(4):378–85. https://doi.org/10.1080/00029157.2015.1011465.
Corman I, Bouchema Y, Miquel B, et al. HypnosIS to faciLitate trans-Esophageal echocardiograPhy Tolerance: The I-SLEPT study. Arch Cardiovasc Dis. 2016;109(3):171–7. https://doi.org/10.1016/j.acvd.2015.09.008.
Lang EV, Berbaum KS, Faintuch S, et al. Adjunctive self-hypnotic relaxation for outpatient medical procedures: a prospective randomized trial with women undergoing large core breast biopsy. Pain. 2006;126(1–3):155–64. https://doi.org/10.1016/j.pain.2006.06.035.
Tefikow S, Barth J, Maichrowitz S, Beelmann A, Strauss B, Rosendahl J. Efficacy of hypnosis in adults undergoing surgery or medical procedures: a meta-analysis of randomized controlled trials. Clin Psychol Rev. 2013;33(5):623–36. https://doi.org/10.1016/j.cpr.2013.03.005.
Hızlı F, Özcan O, Selvi İ, et al. The effects of hypnotherapy during transrectal ultrasound-guided prostate needle biopsy for pain and anxiety. Int Urol Nephrol. 2015;47(11):1773–7. https://doi.org/10.1007/s11255-015-1111-0.
Elkins G, White J, Patel P, Marcus J, Perfect MM, Montgomery GH. Hypnosis to manage anxiety and pain associated with colonoscopy for colorectal cancer screening: case studies and possible benefits. Int J Clin Exp Hypn. 2006;54(4):416–31. https://doi.org/10.1080/00207140600856780.
Shenefelt PD. Anxiety reduction using hypnotic induction and self-guided imagery for relaxation during dermatologic procedures. Int J Clin Exp Hypn. 2013;61(3):305–18. https://doi.org/10.1080/00207144.2013.784096.
Baglini R, Sesana M, Capuano C, Gnecchi-Ruscone T, Ugo L, Danzi GB. Effect of hypnotic sedation during percutaneous transluminal coronary angioplasty on myocardial ischemia and cardiac sympathetic drive. Am J Cardiol. 2004;93(8):1035–8. https://doi.org/10.1016/j.amjcard.2003.12.058.
Lang EV, Benotsch EG, Fick LJ, Lutgendorf S, Berbaum ML, Berbaum KS, Logan H, Spiegel D. Adjunctive non-pharmacological analgesia for invasive medical procedures: a randomised trial. Lancet. 2000;355(9214):1490. https://doi.org/10.1016/s0140-6736(00)02162-0.
Gueguen J, Barry C, Hassler C, Falissard B. Evaluation de l’efficacité de la pratique de l’hypnose. Inserm U1178 Santé Mentale & Santé Publique; 2015. Available on https://www.inserm.fr/rapport/evaluation-de-lefficacite-de-la-pratique-de-lhypnose-2015/. Accessed 21 Nov 2022.
Mackey EF. Effects of hypnosis as an adjunct to intravenous sedation for third molar extraction: a randomized, blind, controlled study. Int J Clin Exp Hypn. 2010;58(1):21–38. https://doi.org/10.1080/00207140903310782 PMID: 20183736.
Spielberger CD. Stai-y inventaire d’anxiete etat-trait (Forme Y). Paris: Éditions du centre de psychologie appliquée. DL 1993, cop. 1993. 1 vol. (68 p.).
Eren G, Dogan Y, Demir G, et al. Hypnosis for sedation in transesophageal echocardiography: a comparison with midazolam. Ann Saudi Med. 2015;35(1):58–63. https://doi.org/10.5144/0256-4947.2015.58.
Lang EV, Benotsch EG, Fick LJ, et al. Adjunctive non-pharmacological analgesia for invasive medical procedures: a randomised trial. Lancet. 2000;355(9214):1486–90. https://doi.org/10.1016/S0140-6736(00)02162-0.
Lang EV, Berbaum KS, Pauker SG, et al. Beneficial effects of hypnosis and adverse effects of empathic attention during percutaneous tumor treatment: when being nice does not suffice. J Vasc Interv Radiol. 2008;19(6):897–905. https://doi.org/10.1016/j.jvir.2008.01.027.
Stewart JH. Hypnosis in contemporary medicine. Mayo Clinic Proceedings avr. 2005;80(4):511–24.
Keil PC, Lindenberg N, Lassen CL, Graf BM, Meier J, Wiese CH. „Selbsthypnosetraining“ bei chronischen stationären Schmerzpatienten: Eine retrolektive Beobachtungsstudie. Schmerz juin. 2018;32(3):181–7.
Johnson ME, Hauck C. Beliefs and Opinions about Hypnosis Held by the General Public: A Systematic Evaluation. Am J Clin Hypn. 1999;42(1):10–20. https://doi.org/10.1080/00029157.1999.10404241.
Lynn SJ, Maxwell R, Green JP. The hypnotic induction in the broad scheme of hypnosis: a sociocognitive perspective. Am J Clin Hypn. 2017;59(4):363–84. https://doi.org/10.1080/00029157.2016.1233093.
Shimizu T. Role of beliefs about hypnotic states as a moderator variable: a reexamination of the relationship between reactance and hypnotizability. Int J Clin Exp Hypn. 2016;64(2):167–86. https://doi.org/10.1080/00207144.2016.1131586.
Lynn SJ, Laurence J-R, Kirsch I. Hypnosis, suggestion, and suggestibility: an integrative model. Am J Clin Hypn. 2015;57(3):314–29. https://doi.org/10.1080/00029157.2014.976783.
Gandhi B, Oakley DA. Does ‘hypnosis’ by any other name smell as sweet? The efficacy of ‘hypnotic’ inductions depends on the label ‘hypnosis.’ Conscious Cogn. 2005;14(2):304–15. https://doi.org/10.1016/j.concog.2004.12.004.
Dufresne A, Rainville P, Dodin S, et al. Hypnotizability and Opinions About Hypnosis in a Clinical Trial for the Hypnotic Control of Pain and Anxiety During Pregnancy Termination. Int J Clin Exp Hypn. 2009;58(1):82–101. https://doi.org/10.1080/00207140903310865.
Montgomery GH, Bovbjerg DH, Schnur JB, et al. A randomized clinical trial of a brief hypnosis intervention to control side effects in breast surgery patients. JNCI J Natl Cancer Inst. 2007;99(17):1304–12. https://doi.org/10.1093/jnci/djm106.
Werner A, Uldbjerg N, Zachariae R, Nohr EA. Effect of self-hypnosis on duration of labor and maternal and neonatal outcomes: a randomized controlled trial. Acta Obstet Gynecol Scand. 2013;92(7):816–23. https://doi.org/10.1111/aogs.12141.
Marc I, Rainville P, Masse B, et al. Women’s views regarding hypnosis for the control of surgical pain in the context of a randomized clinical trial. J Womens Health. 2009;18(9):1441–7. https://doi.org/10.1089/jwh.2008.1015.
Acknowledgements
N/A.
Funding
The Metz-Thionville Regional Hospital Center sponsored and funded the trial.
Author information
Authors and Affiliations
Contributions
LAV, CG, CG, NG prepared the first draft of the manuscript. NG, CG, NO wrote the study protocol. SW, NG, MV, JB, KK were investigators. LAV reported the changes made by all authors. All authors validated the final version of the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
In accordance with the Declaration of Helsinki, all methods were carried out in accordance with relevant guidelines and regulations. The research protocol was registered on the ClinicalTrials.gov registry (NCT02818101; 29/06/2016) and with the ANSM (IDRCB 2016-A00205-46; 02/02/2016). The research protocol and ethical was approved by the East-III Protection of Persons Committee. Authors confirm that informed consent was obtained from all study participants.
Consent for publication
N/A.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abensur Vuillaume, L., Gentilhomme, C., Weber, S. et al. Effectiveness of Hypnosis for the Prevention of Anxiety During Coronary Angiography (HYPCOR study): a prospective randomized study. BMC Complement Med Ther 22, 315 (2022). https://doi.org/10.1186/s12906-022-03792-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-022-03792-x