
Abstract
Objective
Few studies evaluated the association between neutrophil to lymphocyte ratio (NLR) and clinical outcomes in ischemic stroke or transient ischemia attack (TIA) in young adults. We aimed to investigate the relationship of NLR with 90-day functional independence in ischemic stroke or TIA in young adults.
Methods
We retrospectively included patients aged 18–45 and diagnosed with ischemic stroke or TIA. Information including demographics, clinical and imaging characteristics, and the 90-day clinical outcome was collected. The primary outcome was excellent clinical outcome at 90 days, defined as mRS 0–1. Logistic regression analyses and a receiver operator characteristic (ROC) curve were used to investigate the association between NLR and 90-day clinical outcome.
Results
A total of 691 young patients with ischemic stroke or TIA were included in the final study. A higher level of NLR indicated poorer clinical outcome at 90 days (p for trend <0.001). The multivariable logistics regression suggested that NLR was an independent predictor of mRS 0–1 at 90 days (crude OR: 0.88, 95% CI 0.83–0.94, p < 0.001; adjusted OR of model 2: 0.87, 95% CI 0.84–0.94, p < 0.001; adjusted OR of model 3: 0.92, 95% CI 0.84–0.99, p = 0.04).
Conclusion
In our study, a higher level of NLR was correlated with poorer functional outcomes at 90 days in ischemic stroke or TIA in young adults.
Similar content being viewed by others


Introduction
Ischemic stroke in young adults caused a great global burden of disease in the world with incidences from 5 to 40 per 100,000 person-years across different regions in the world [1]. Given the differences in clinical features, etiology, and risk factors of juvenile ischemic stroke compared to ischemic stroke in the elderly population [2], young ischemic stroke deserves more investigations to further reveal the mechanism and interventions.
The inflammatory process initiated after the onset of ischemic stroke was related to the progression and prognosis of ischemic stroke [3,4,5]. Plus, preceding and post-stroke infections in young adults might also be associated with clinical outcomes in young ischemic stroke [6]. Some laboratory parameters including leukocyte rate, which were associated with inflammation and infection, were found to be related to clinical outcomes in young ischemic stroke [7]. Neutrophil to lymphocyte ratio (NLR), an inflammatory marker, was also reported to be correlated with clinical outcomes in patients irrespective of age with ischemic stroke [8, 9]. NLR is also a quite convenient biomarker in the clinical practice for neutrophil and lymphocyte count could be obtained through a routine laboratory examination. However, it remained unknown whether the role of NLR in young ischemic stroke was the same as that in the elderly patients with ischemic stroke. Hence, it is necessary to investigate the clinical significance of NLR and other inflammatory parameters in young ischemic stroke, considering different rate or role of pre- or post- stroke infection.
The aim of our study was to investigate the relationship between NLR and 90-day functional outcomes in ischemic stroke and TIA in young adults.
Methods
Study design
Patients admitted to the neurology department of Beijing Tiantan Hospital were screened for eligibility in our retrospective study. The study was approved by the ethics committee of Beijing Tiantan Hospital.
Participants
Young patients with ischemic stroke or TIA were recruited consecutively from January 2019 to December 2021 and would be assessed for eligibility if they met the inclusion criteria:
1) aged 18–45 years;
2) ischemic stroke or TIA;
3) admitted within 3 days from ischemia onset.
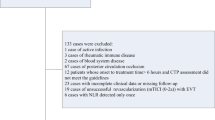
Patients were excluded if they were 1) diagnosed with cerebral venous thrombosis, iatrogenic stroke; 2) without laboratory test results on neutrophils or lymphocytes; 3) disability before the index event of stroke or TIA (mRS ≥2); 4) without information on 90-d mRS.
Data collection and outcome
A neurological resident physician (L.G.) collected clinical data blinded to the results of blood tests and imaging information. The clinical data collected included demographic information (age, sex), medical history (hypertension, diabetes, hyperlipidemia, prior stroke, etc.), and alcohol intake / smoking status. Neurological impairment severity was evaluated by the National Institute of Health Stroke Scale (NIHSS) score [10]. Stroke etiology was classified based on the Trial of Org 10,172 in Acute Stroke Treatment (TOAST) classification [11].
Another neurologist (J.J.) conducted the data collection of imaging and laboratory examination. NLR was calculated by neutrophil count divided by lymphocyte count. Peripheral blood samples were collected within 24 hours from admission. Excellent functional outcome was defined as modified Rankin Scale (mRS) 0–1 at 90 days.
Statistical analysis
The included patients were categorized into four groups according to the NLR level (Q1-Q4 based on median and interquartile ranges). For continuous variables, normally distributed data were shown as mean ± SD and compared using the student t test while non-normally distributed data were shown as median (interquartile range) and compared using Mann–Whitney U test. The normality was tested by the Shapiro test. Classified variables were shown as number (percentage) and compared using the χ2 or Fisher’s exact tests. Adjusted confounders in multivariable logistics analyses were variables with a P value < 0.05 in baseline comparisons. All statistical analyses were performed with the SPSS 25.0. P value< 0.05 was defined as statistically significant.
Results
From January 2019 to December 2021, 691 young patients were included in our study. The included patients had an average age was 37 [33–42] and 83.94% (580/691) of them were male. Among the included patients, 4.49% (31/691) patients were treated with intravenous thrombolysis (IV tPA). The median admission NIHSS score was 2 (0–5) and 14.62% (101/691) patients had hemorrhagic transformation during hospitalization. The proportion of 77.71% (537/691) patients had excellent functional outcome (mRS 0–1) at 90 days.
Baseline comparison between the Q1-Q4 groups of NLR
Compared with the Q1-Q3 groups (Table 1), the Q4 group had a larger proportion of IV tPA (8.72%, p = 0.008), higher level of systolic blood pressure (148 [132.75–170] mmHg, p < 0.001) as well as a higher level of diastolic blood pressure (94.5 [82–110] mmHg, p < 0.001), more severe neurological impairment (median NIHSS score, 3.5 [1–7], p < 0.001) and a higher proportion of pulmonary infection (11.05%, p < 0.001). The Q4 group also had a higher proportion of disability at 90 days (mRS 2–6, 36.63%, p < 0.001). As Fig. 1 showed, proportions of disability increased among the Q1-Q4 groups (P for trend < 0.001).

Relationship between different level of NLR and 90d disability (mRS 2–6)
Relationship between NLR and functional outcome at 90 days
Table 2 summarized the comparison of baseline characteristics between mRS 2–6 and mRS 0–1 group. Compared to mRS 2–6 group, mRS 0–1 group was younger (37 [32–42] vs. 38 [35–42], p = 0.03), had a lower proportion of hemorrhagic transformation (12.48% vs. 22.08%, P = 0.004), higher level of random glucose (5.46 [4.62–6.71] vs. 5.92 [5.00–7.68], p = 0.002), lower level of systolic blood pressure (140 [129–159] vs. 149 [129.25–170], p = 0.006) as well as lower level of diastolic blood pressure (90 [81–103] vs. 96 [82, 109.50], p = 0.008), higher proportion of dyslipidemia (85.29% vs. 92.21%, p = 0.035), lower proportion of atrial fibrillation (0.93% vs. 3.9%, p = 0.026), lower proportion of current smoker (50.28% vs. 62.99%, p = 0.017), lower admission NIHSS score (1 [0–3] vs. 8 [6–10], p < 0.001), lower proportion of pulmonary infection (2.79% vs. 11.04%, p < 0.001), lower level of low-density lipoprotein (2.13 [1.60–2.87] vs. 2.36 [1.81–3.00], p = 0.035), lower level of CRP (1.01 [0.43–2.93] vs. 2.17 [0.90–7.14], p < 0.001) and lower level of NLR (2.39 [1.84–3.54] vs. 3.38 [2.48–5.24], p < 0.001). As shown in Fig. 2, multivariable logistics regression analyses found that NLR indicated to be an independent predictor of mRS 0–1 at 90 days (crude OR: 0.88, 95% CI 0.83–0.94, p < 0.001; adjusted OR of model 2: 0.87, 95% CI 0.84–0.94, p < 0.001; adjusted OR of model 3: 0.92, 95% CI 0.84–0.99, p = 0.04).

Multivariable logistics regression analyses: #) adjusted for age and sex; *) adjusted for age, random glucose, hemorrhagic transformation, systolic blood pressure, diastolic blood pressure, smoke status, alcoholic status, history of dyslipidemia, history of atrial fibrillation, pulmonary infection, low-density lipoprotein, CRP and NIHSS score
ROC curves and ordinal analyses
The ROC curve (Fig. 3) showed that the area under curve (AUC) of NLR was 0.66 (95% CI 0.62–0.71, p < 0.001) and the optimal cut-off was 2.40 (sensitivity 0.77, specificity 0.50).

Receiver operating characteristic curves
Based on the optimal cut-off value, the shift analyses of mRS distribution between the high-level group and low-level group of NLR was shown in Fig. 4. For NLR, a high level of NLR represented a poor functional outcome at 90 days (P < 0.001). We also used restricted cubic splines (4 knots: 5th, 35th, 65th and 95th centiles) to flexibly model the association of NLR. (Fig. 5).

Distribution of mRS score at discharge between different level of NLR. For NLR, high level of NLR represented poor functional outcome at 90 days

restricted cubic splines
Discussion
In our study, NLR was independently correlated to the functional outcome at 90 days in young patients with TIA / ischemic stroke. As far as we know, our study was the first to report the relationship between NLR and functional outcome at 90 days in young patients with TIA / ischemic stroke.
Studies based on animal models and in vitro experiments delineated the association between neuroinflammation and outcomes in ischemic stroke. Astrocytes and microglial were the initiators of neuroinflammation cascade triggered by cerebral ischemia or hypoprefusion [12, 13]. Inflammatory cytokines including interleukin-1 and tumor necrosis factor-α (TNF-α) secreted from microglia participated in recruiting immune cells including neutrophils, lymphocytes and monocytes [14, 15]. In these recruited immune cells, reactive oxygen species (ROS) build-up and activation of matrix metalloproteinases (MMP) were occurred and disrupted the integrity of the blood-brain barrier (BBB) [16]. Disrupted BBB recruited neutrophils into the brain tissue within 1 hour after ischemic stroke onset and last for about 14 days with a peak at 2–3 days [15]. The neutrophils recruited into the parenchyma generated damage to the parenchyma and worsened neurological deficits [15]. Lymphocyte were recruited into the parenchyma within days after stroke onset and both protective and harmful function was found of lymphocyte [16,17,18]. Lymphocytes could mend the inflammatory damage but also excrete cytotoxic chemicals at the same time [19,20,21]. This paradoxical function of lymphocytes may be attributed to different subtypes [22, 23]. Apart from neuroinflammation, pre- and post-stroke infections might also be associated with poor clinical outcome [6].
Our study indicated that a higher level of NLR was related to poor functional outcome at 90 days [24, 25]. However, most previous studies investigated the relationship between NLR and excellent outcome in elderly adults. Wang et al. conducted an analysis using the data of 808 patients from the Chengdu stroke registry, another registry in China, and found NLR ≥ 5 was associated with 3-month disability or death [9]. Another observational study in Germany enrolled 807 ischemic stroke patients and showed higher admission NLR level was associated with poorer functional outcome [8]. This observational study [8] also identified a similar AUC (0.69 vs. 0.66) and a higher NLR cut off value compared with our study (3.3 vs. 2.4). The higher NLR cut-off relative to that in our study was probably due to the higher admission median NLR in the Germany observational registry (3.4 vs. 2.6) [8]. Admission NLR higher than 5.9 was associated with 90-day functional outcome in patients treated with endovascular thrombectomy [26]. For patients treated with IV tPA, the cut-off value of NLR after tPA therapy was 4.8 [27].
Our study has some potential limitations. First, the retrospective study design of our observational study in a single stroke center might result in additional bias. However, blind assessment was conducted to reduce the potential bias. Secondly, the sample size of our study was limited. This study was initiated to conduct a pilot analysis to test whether the association between NLR and clinical outcome was statistical significance based on our single-center database. A future prospective registry was planned to include more participants. Third, we failed to collect the details on the ‘unknown etiology’ in TOAST of the patients enrolled in our study. Considering the retrospective design of our study, some additional examination on the rare causes of ischemic stroke was hard to perform and it was difficult to provide complete data on these rare reasons. We planned to collect more information on the rare reasons for ischemic stroke in young adults in the future prospective cohort.
Conclusion
NLR may be served as promising biomarkers for functional outcomes at 90-day among ischemic stroke or TIA in young adults.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Boot E, Ekker MS, Putaala J, Kittner S, De Leeuw FE, Tuladhar AM. Ischaemic stroke in young adults: a global perspective. J Neurol Neurosurg Psychiatry. 2020;91:411–7.
McKinney JS, Kostis WJ. Statin therapy and the risk of intracerebral hemorrhage: A meta-analysis of 31 randomized controlled trials. Stroke. 2012;43:2149–56.
Schuhmann MK, Stoll G, Bieber M, Vogtle T, Hofmann S, Klaus V, et al. Cd84 links t cell and platelet activity in cerebral thrombo-inflammation in acute stroke. Circ Res. 2020;127:1023–35.
Parikh NS, Merkler AE, Iadecola C. Inflammation, autoimmunity, infection, and stroke: epidemiology and lessons from therapeutic intervention. Stroke. 2020;51:711–8.
Stoll G, Nieswandt B. Thrombo-inflammation in acute ischaemic stroke - implications for treatment. Nat Rev Neurol. 2019;15:473–81.
Heikinheimo T, Broman J, Haapaniemi E, Kaste M, Tatlisumak T, Putaala J. Preceding and poststroke infections in young adults with first-ever ischemic stroke: effect on short-term and long-term outcomes. Stroke. 2013;44:3331–7.
Heikinheimo T, Putaala J, Haapaniemi E, Kaste M, Tatlisumak T. Leucocyte count in young adults with first-ever ischaemic stroke: associated factors and association on prognosis. Int J Stroke. 2015;10:245–50.
Giede-Jeppe A, Madzar D, Sembill JA, Sprugel MI, Atay S, Hoelter P, et al. Increased neutrophil-to-lymphocyte ratio is associated with unfavorable functional outcome in acute ischemic stroke. Neurocrit Care. 2020;33:97–104.
Wang L, Song Q, Wang C, Wu S, Deng L, Li Y, et al. Neutrophil to lymphocyte ratio predicts poor outcomes after acute ischemic stroke: a cohort study and systematic review. J Neurol Sci. 2019;406:116445.
Lyden PBT, Tilley B, Welch KM, Mascha EJ, Levine S, Haley EC, et al. Improved reliability of the nih stroke scale using video training. Ninds tpa stroke study group. Stroke. 1994;25:2220–6.
Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. Toast. Trial of org 10172 in acute stroke treatment. Stroke. 1993;24:35–41.
Berchtold D, Priller J, Meisel C, Meisel A. Interaction of microglia with infiltrating immune cells in the different phases of stroke. Brain Pathol. 2020;30:1208–18.
Xu S, Lu J, Shao A, Zhang JH, Zhang J. Glial cells: role of the immune response in ischemic stroke. Front Immunol. 2020;11:294.
Khoshnam SE, Winlow W, Farzaneh M, Farbood Y, Moghaddam HF. Pathogenic mechanisms following ischemic stroke. Neurol Sci. 2017;38:1167–86.
Ao LY, Yan YY, Zhou L, Li CY, Li WT, Fang WR, et al. Immune cells after ischemic stroke onset: roles, migration, and target intervention. J Mol Neurosci. 2018;66:342–55.
Jian Z, Liu R, Zhu X, Smerin D, Zhong Y, Gu L, et al. The involvement and therapy target of immune cells after ischemic stroke. Front Immunol. 2019;10:2167.
Planas AM. Role of immune cells migrating to the ischemic brain. Stroke. 2018;49:2261–7.
Rayasam A, Hsu M, Kijak JA, Kissel L, Hernandez G, Sandor M, et al. Immune responses in stroke: how the immune system contributes to damage and healing after stroke and how this knowledge could be translated to better cures? Immunology. 2018;154:363–76.
Xue J, Huang W, Chen X, Li Q, Cai Z, Yu T, et al. Neutrophil-to-lymphocyte ratio is a prognostic marker in acute ischemic stroke. J Stroke Cerebrovasc Dis. 2017;26:650–7.
Kim JYKM, Yenari MA. Innate inflammatory responses in stroke: mechanisms and potential therapeutic targets. Curr Med Chem. 2014;21:2076–97.
Zhang J, Ren Q, Song Y, He M, Zeng Y, Liu Z, et al. Prognostic role of neutrophil-lymphocyte ratio in patients with acute ischemic stroke. Medicine (Baltimore). 2017;96:e8624.
Liesz A, Suri-Payer E, Veltkamp C, Doerr H, Sommer C, Rivest S, et al. Regulatory t cells are key cerebroprotective immunomodulators in acute experimental stroke. Nat Med. 2009;15:192–9.
Ren X, Akiyoshi K, Dziennis S, Vandenbark AA, Herson PS, Hurn PD, et al. Regulatory b cells limit cns inflammation and neurologic deficits in murine experimental stroke. J Neurosci. 2011;31:8556–63.
Wang H, Zhang M, Hao Y, Zi W, Yang D, Zhou Z, et al. Early prediction of poor outcome despite successful recanalization after endovascular treatment for anterior large vessel occlusion stroke. World Neurosurg. 2018;115:e312–21.
Zhang R, Wu X, Hu W, Zhao L, Zhao S, Zhang J, et al. Neutrophil-to-lymphocyte ratio predicts hemorrhagic transformation in ischemic stroke: a meta-analysis. Brain Behav. 2019;9(9):e01382. https://doi.org/10.1002/brb3.1382.
Brooks SD, Spears C, Cummings C, VanGilder RL, Stinehart KR, Gutmann L, et al. Admission neutrophil-lymphocyte ratio predicts 90 day outcome after endovascular stroke therapy. J Neurointerv Surg. 2014;6:578–83.
Chen CT, Li LH, Su PY, Chang YC, Lee IH, Yen DH, et al. Neutrophil-to-lymphocyte ratio in predicting neurologic outcome of patients with acute ischemic stroke treated with intravenous thrombolytics. J Chin Med Assoc. 2022;85:102–8.
Acknowledgements
We wish to acknowledge the staff and participants of our study for their contribution.
Funding
This work was supported by the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences [grant numbers 2019-I2M-5-029]; Beijing Municipal Committee of Science and Technology [grant numbers Z201100005620010]; and Beijing Natural Science Foundation [grant numbers Z200016], Ministry of Finance of the People’s Republic of China [issued by Finance and Social Security [2015] Document No. 82; [2016] Document No. 50; [2017] Document No. 72; [2018] Document No. 48; [2019] Document No. 77; [2020] Document No. 75; [2021] Document No. 84, Ministry of Finance], Beijing Hospitals Authority Innovation Studio of Young Staff Funding Support, code: 202112.
Author information
Authors and Affiliations
Contributions
G.L., Y.L. and X.Z. contributed to the conception and design of the study; Y.L., J.J., X.L. and J.G. contributed to the acquisition and analysis of data; Y.L., G.L. and X.Z. contributed to drafting the text and preparing the figures. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of Beijing Tiantan Hospital (No.: KY2019–019- 05). Due to the fully dei-dentified data on the patients enrolled in the current study and its retrospective study design this study received a waiver of informed consent by the local institutional review board of Beijing Tiantan Hospital. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable. No information or images that could lead to identification of a study participant was mentioned in our study.
Competing interests
None to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, Y., Li, G., Jia, J. et al. Clinical significance of neutrophil to lymphocyte ratio in ischemic stroke and transient ischemic attack in young adults. BMC Neurol 22, 481 (2022). https://doi.org/10.1186/s12883-022-03011-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-022-03011-7