
Abstract
Background
To determine the association between dynamic neutrophil-to-lymphocyte ratio (NLR) during hospitalization and mortality 1 month after ischemia reperfusion in patients undergoing endovascular treatment (EVT) with successful revascularization for acute large vessel occlusion stroke.
Methods
This retrospective study included patients who had undergone successful EVT. Information was collected regarding patients’ clinical characteristics, imaging data, and mortality at 1 month. Univariate and multivariate logistic regression models were applied to assess the association between NLR and mortality. We used a generalized additive model and a generalized additive mixed model to compare trends in NLR over time between survivors and nonsurvivors.
Results
A total of 237 patients were included. During the 1-month follow-up, 42 of these patients (17.7%) died. The multivariate analysis demonstrated that NLR obtained within 12 to 24 hours (odds ratio [OR] = 1.18; 95% confidence interval [CI]: 1.04, 1.33; P = 0.008), 24 to 48 hours (OR = 1.16; 95% CI: 1.01, 1.35; P = 0.044), and 48 to 72 hours (OR = 1.23; 95% CI: 1.03, 1.47; P = 0.021) after EVT were independently associated with mortality at 1 month. In addition, there was a trend for NLR to decrease gradually over time for both survivors and nonsurvivors; however, NLR in survivors decreased by an average of 0.29 daily than in nonsurvivors.
Conclusions
Increased NLR in the early period after EVT was associated with an increased risk of mortality, and a continued trend toward higher NLR over time was also linked with a higher mortality risk.
Similar content being viewed by others

Background
Endovascular treatment (EVT) has become the gold standard for the treatment of large vessel occlusion in patients with acute ischemic stroke [1]; however, patients undergoing this therapy are still at high risk of a poor prognosis, including mortality as high as 15.3% [2]. The inflammatory mechanism of stroke has been widely researched [3]. A systemic inflammatory response is rapidly induced shortly after ischemia reperfusion injury, and neutrophils in the blood enter ischemic or infarcted tissue through the injured blood-brain barrier and transmit inflammatory factors [4, 5]. Through a variety of mechanisms, inflammatory mediators such as oxygen free radicals and matrix metalloproteinase-9 cause damage to brain cells [6,7,8]. However, the increased concentration of neutrophils in the peripheral blood is accompanied by a continuous decrease in lymphocytes because of the engagement of T cells and platelets through P-selectin [9]. The activated platelets can prevent bleeding transformation and play a role in hemostasis [10].
Previous studies have shown that the neutrophil-to-lymphocyte ratio (NLR) in the early poststroke period may reflect the state of inflammation and which plays an important role in ischemia-reperfusion injury [11,12,13,14,15], thus NLR is served as an inexpensive and reliable biological indicator [16,17,18,19]. However, the correlation between NLR and death after ischemia reperfusion is still controversial [20, 21], and the relationship between dynamic NLR during hospitalization and death in stroke patients with successful revascularization is still unclear.
To address these uncertainties, we collected data on stroke patients undergone successful revascularization for anterior circulation large vessel occlusion stroke, and sought to assess the potential relationship between dynamic NLR during hospitalization and mortality at 1 month, in the hope that a proven correlation would help physicians make treatment decisions.
Methods
Patients and population
This case series was approved by the Ethics Committees of Changzhou Second People’s Hospital Affiliated to Nanjing Medical University (Approval No: [2021] YLJSC020). Because this study involved an observational retrospective cohort, written consent from patients was not required.
Consecutive patients aged ≥18 years who underwent EVT for large vessel occlusion stroke at Changzhou Second People’s Hospital Affiliated to Nanjing Medical University between May 2017 and December 2021 were considered for study inclusion. Eligible patients were those who had experienced an anterior circulation large vessel occlusion stroke, confirmed by head computed tomography (CT) angiography or digital subtraction angiography (DSA); those with a modified Rankin Scale score ≤ 1; those with a National Institutes of Health Stroke Scale (NIHSS) score > 5 at admission; and those in whom treatment was initiated within 12 hours after stroke onset .
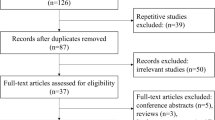
Patients were excluded from the study if > 6 hours after stroke onset and CT perfusion evaluation did not meet established criteria guidelines [1, 22]; if they had an active infection within 3 days before the onset of stroke, confirmed by clinical symptoms, elevated leukocyte levels, or elevated C-reactive protein levels; if they had a history of rheumatic immune disease; if they had incomplete clinical data (eg, missing follow-up, only 1 documented leukocyte/lymphocyte value); or if they had undergone unsuccessful EVT revascularization (ie, modified Thrombolysis in Cerebral Infarction score of 0-2a). Once these criteria were applied, 237 patients were eligible for study inclusion (Fig. 1).

Flow chart of patient selection. CTP, computed tomography perfusion; EVT, endovascular treatment; mTICI, modified Thrombolysis in Cerebral Infarction; NLR, neutrophil-to-lymphocyte ratio
Data and outcome analysis
We collected information regarding patient demographics, clinical history, past medical history and history of drug use, imaging data, laboratory results, NIHSS score, Alberta Stroke Program Early CT Score (ASPECTS), complications during hospitalization,medication during hospitalization and mortality at 1 month after EVT. DSA was used to assess collateral compensation; grades 3 and 4 were defined as favorable collateral compensation based on guidelines from the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology [23].symptomatic intracranial hemorrhage was defined as a hemorrhage volume on CT exceeding 30% of the infarct volume and an increase in the NIHSS score of 4 points within 72 hours.
All leukocyte and lymphocyte counts obtained during hospitalization were collected, and NLR for each sample were calculated by dividing the neutrophil count by the lymphocyte count. NLR were categorized into values obtained at admission, immediately after EVT, within 12 to 24 hours after EVT, within 24 to 48 hours after EVT, and within 48 to 72 hours after EVT.
Mortality at 1 month after EVT was recorded by clinicians either in the hospital or via telephone consultation after the patient had been discharged. All clinical and imaging data were assessed by 2 experienced cerebrovascular physicians who were not familiar with the clinical information and the imaging data. In case of disagreements, a third senior cerebrovascular physician was consulted.
Statistical analysis
For this analysis, we compared dynamic NLR during hospitalization in patients who were alive and those who had died at 1 month after EVT. Continuous variables were described as mean ± standard deviation or as median (interquartile range [IQR]). Categorical variables were described as rate and composition ratio. Baseline characteristics were analyzed using a t test or a Kruskal–Wallis rank-sum test for continuous variables and a chi-square test for categorical variables. Univariate and multivariate logistic regression models were applied to evaluate the association between NLR at different time points and mortality at 1 month after successful revascularization, with adjustments made for multiple confounders in multivariate models. For the multivariate analysis, the covariates were included as potential confounders in the final models if they changed the estimates of NLR on mortality at 1 month by more than 10% or were significantly associated with mortality. One such confounder was the occurrence of pneumonia during hospitalization, as poststroke infections such as pneumonia are common, and the presence of infection will affect the NLR [24,25,26,27].
The smoothing plots made by generalized additive model were used to assess NLR and mortality at different points after successful revascularization. The difference in NLR between survivors and nonsurvivors at 1 month after EVT was derived from a generalized additive mixed model. The model is used to analyze repeated measurement data, especially when some data are missing and the time interval for repeated measurements is irregular [28, 29].
All analyses were performed using the R package (http://www.R-project.org; The R Foundation) and EmpowerStats (https://www.empowerstats.com; X&Y Solutions, Inc). A P value < 0.05 (two-sided) was considered statistically significant.
Results
Baseline characteristics
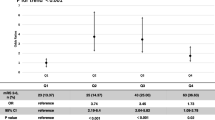
Of the 370 patients who were treated with EVT during the study period, 237 (64.1%) were included in the analysis (Fig. 1). The baseline characteristics of study patients are shown in Table 1. The study population included 147 men (62.0%), and the median age of patients was 70.0 years (IQR, 63.0–76.0). The median baseline NIHSS score was 15 points (IQR, 10.0–20.0) and the median ASPECTS was 8.0 (IQR, 7.0–9.0). Nineteen (8.0%) patients had symptomatic intracranial hemorrhage. There was not a statistically significant difference in mortality (P = 0.088) and symptomatic intracerebral hemorrhage (P = 0.400) among the categorical variable (tertile) groups of NLR.
The sample included 195 patients who were alive at 1 month after EVT (82.3%) and 42 patients who had died at 1 month after EVT (17.7%). Among nonsurvivors, the cause of death was cerebral hemorrhage in 13 patients (31.0%), malignant brain swelling in 8 patients (19.0%), respiratory failure in 12patients (28.6%), heart failure in 5 patients (11.9%), septic shock in 2 patients (4.8%), and “other cause” in 2 patient (4.8%). Among them, 21 cases (50%) died of cerebral causes and 21 cases (50%) died of extra-cerebral causes. The median NLR of the two groups was 6.69 (2.40–7.88) and 3.95 (2.62–5.48) respectively, with no significant difference between them (P = 0.489). In addition, 30 cases (71.4%) died in hospital.
Clinical outcomes
Univariate analysis demonstrated that age (P = 0.003), baseline NIHSS score (P < 0.001), history of diabetes (P = 0.001), history of chronic kidney disease (P = 0.031), glucose at admission(P = 0.017), bridging intravenous thrombolysis (P = 0.040), cardioembolism (P = 0.040), internal carotid artery occlusion (P = 0.049), Pneumonia during hospitalization (P = 0.024), anticoagulation during hospitalization (P = 0.004), use of invasive mechanical ventilation and vasopressors during hospitalization (p < 0.001), sepsis during hospitalization (P = 0.001), any intracerebral hemorrhage and symptomatic intracerebral hemorrhage during hospitalization (p < 0.001), NLR within 12 to 24 hours after EVT (p < 0.001), NLR within 24 to 48 hours after EVT (P = 0.002), and NLR within 48 to 72 hours after EVT (p < 0.001) were associated with mortality at 1 month (Table 2).
After adjustments were made for confounding factors, multivariate analysis demonstrated that NLR obtained within 12 to 24 hours after EVT (odds ratio [OR] = 1.18; 95% confidence interval [CI]: 1.04, 1.33; P = 0.008), within 24 to 48 hours after EVT (OR = 1.16; 95% CI: 1.01, 1.35; P = 0.044), and within 48 to 72 hours after EVT (OR = 1.23; 95% CI: 1.03, 1.47; P = 0.021) were independently associated with mortality at 1 month after treatment (Table 3).
There was a nearly linear relationship between NLR and mortality for 3 consecutive days after EVT (Fig. 2). We also found that there was a trend for NLR to decrease gradually over time; however, the NLR in survivors decreased significantly faster than in nonsurvivors (Fig. 3). The NLR over time differed between the 2 groups, and within 1 month after EVT, NLR in survivors had decreased by an average of 0.29 daily than in nonsurvivors (Table 4). After adjustments were made for multiple variables, this difference of 0.29 remained.

A nearly linear association between neutrophil-to-lymphocyte ratio (NLR) and mortality at 1 month after endovascular treatment (EVT) can be seen in a generalized additive model. A smooth curve fitting graph illustrates daily NLR in 237 patients (195 survivors, 42 nonsurvivors) for 3 consecutive days after EVT. The solid line and the dashed lines show the estimated value and its corresponding 95% confidence interval, respectively. Adjustments were made for sex; age; history of diabetes; history of chronic kidney disease; baseline NIHSS score; bridging intravenous thrombolysis; cardioembolic stroke; internal carotid artery occlusion; favorable collateral circulation; pneumonia during hospitalization; symptomatic intracerebral hemorrhage during hospitalization; sepsis during hospitalization; anticoagulation during hospitalization; use of invasive mechanical ventilation during hospitalization; use of vasopressors during hospitalization

A nonlinear association between change in neutrophil-to-lymphocyte ratio (NLR) and time can be seen in a generalized additive model. A smooth curve fitting graph illustrates NLR in 237 patients (195 survivors, 42 nonsurvivors) based on the number of days since endovascular treatment (EVT). The solid line represents survivors; the dashed line represents nonsurvivors. Adjustments were made for sex; age; history of diabetes; history of chronic kidney disease; baseline NIHSS score; bridging intravenous thrombolysis; cardioembolic stroke; internal carotid artery occlusion; favorable collateral circulation; pneumonia during hospitalization; symptomatic intracerebral hemorrhage during hospitalization; sepsis during hospitalization; anticoagulation during hospitalization; use of invasive mechanical ventilation during hospitalization; use of vasopressors during hospitalization
Discussion
In this study, we assessed dynamic NLR in patients who underwent EVT for ischemic stroke with acute large artery occlusion and found that increased NLR in the early stage within 3 days after treatment was associated with an increased risk of mortality at 1 month. Within 1 month after EVT, the NLR of survivors had decreased more than that of nonsurvivors, even after adjustments were made for confounders. These results suggest that increased NLR over time are associated with a higher risk of mortality. This study further expands the impact of dynamic NLR on mortality in stroke patients.
Inflammation plays an important role in the process of ischemic stroke initiation, progression, and recovery [30]. In the acute stage of stroke, blood flow stagnation at the distal end of the thrombus may cause the arterial endothelium to release adhesion molecules, cytokines, and chemokines and to recruit white blood cells, mainly neutrophils, by occluding the distal cortical pial collateral vessels [5]. These white blood cells collect in ischemic cerebral vessels. Neutrophils in the blood enter ischemic or infarcted tissue through the damaged blood-brain barrier and transmit inflammatory factors. The local release of oxygen free radicals and matrix metalloproteinase-9 and inflammatory mediators such as cytokines (eg, interleukin-1β, TNF, and interleukin-6) further increases the risk of blood-brain barrier injury and reperfusion injury, malignant edema, and/or hemorrhagic transformation [7, 8]. However, the ability of T lymphocytes to bind platelets through P-selectin may play a key role in preventing hemorrhagic transformation after acute ischemic stroke [9, 10]. In the subacute phase of acute ischemic stroke (> 48 to 72 h), cerebral ischemic tissue may release cytokines and neurotransmitters and activate immune regulation systems such as the hypothalamus-pituitary axis and sympathetic nervous system, which can lead to down-regulation of systemic immune function and stroke-induced immunosuppression) [31, 32]. This in turn leads to a decrease in lymphocytes (especially T cells and natural killer cells), systemic immunosuppression, and an increased risk of infection [30]. Acute ischemic stroke causes distal organ damage and is associated with a high risk of non-neurological complications, including respiratory failure, cardiovascular dysfunction, liver and kidney damage, and altered immune and endocrine function [33]. These complications can affect prognosis and may have serious short-term and long-term adverse consequences. Thus, assessing the state of inflammation in the early poststroke period may provide clinicians with additional information about potential outcomes.
Recent studies have shown that NLR is associated with the prognosis of hemorrhagic stroke and increased cerebral hemorrhage [34,35,36,37]. Inflammation plays an important role in the mechanism of brain injury in hemorrhagic stroke. Therefore, by releasing cytotoxic mediators, increasing capillary permeability, and promoting disruption of the blood-brain barrier, neuro-inflammation plays a pivotal part in hematoma enlargement, brain cell death, brain edema formation and intracranial hypertension [38]. In the early stage of stroke, most of the white blood cells entering the brain come from peripheral blood, with neutrophils being the first hematopoietic cells to be recruited. Hence similar action mechanisms of inflammation in ischemic stroke and hemorrhagic stroke.
Previous studies have demonstrated a relationship between mortality and NLR at admission (OR = 1.19; 95% CI 1.03, 1.36; P = 0.02) [39]. Higher NLR (6.3 (IQR 4.4–10.8) vs 4.9 (IQR 3.1–7.4); P = 0.002) and greater temporal change in NLR (2.4 (IQR 1.1–7.6) vs 1.3 (IQR 0.1–3.7); P = 0.05) within 3 to 7 days after EVT were also associated with mortality at 90 days [40]. In the present study, we found that baseline NLR were not associated with mortality at 1 month (OR = 1.00; 95% CI: 0.86, 1.16; P = 0.971), but NLR obtained within 12 to 24 hours after EVT were associated with mortality at 1 month (OR = 1.18; 95% CI: 1.04, 1.33; P = 0.008). For every unit increase in NLR in the early stage, the risk of mortality increased by approximately 18%. Differences in findings between our study and previous research may be partially explained by differences in the enrolled populations (eg, more serious condition in patients requiring thrombectomy) and the stress reaction associated with undergoing EVT.
Our previous research has shown that increased NLR immediately after EVT is associated with an unfavorable prognosis (modified Rankin Scale score of 3–6) at 3 months for anterior circulation large vessel occlusion stroke (OR = 1.19; 95% CI: 1.07, 1.32; P = 0.002) [41], but in this study we did not find that increased NLR immediately after EVT was associated with death at 1 month(OR = 1.05; 95% CI: 0.94, 1.17; P = 0.422). Additionally, we found that NLR in patients still alive at 1 month decreased by an average of 0.29 daily than in nonsurvivors. To our knowledge, this is the first study to examine the association between persistent dynamic changes in NLR during hospitalization and mortality, thus extending previous research in several ways. First, we demonstrated the trends in dynamic NLR over time during hospitalization after successful revascularization. Second, we compared these trends in survivors and nonsurvivors to assess the association between dynamic NLR and mortality at 1 month after EVT. The NLR might be a biological marker of prognosis in patients undergoing EVT and could also sensitively reflect changes in the severity of a patient’s condition [12, 42]. Additionally, we found that the change in NLR over time was more informative regarding the risk of mortality than any individual NLR. Increased NLR over time should therefore prompt closer scrutiny of a patient’s condition. Because it is easy and inexpensive to obtain routine bloodwork results, performing this testing daily may help to elucidate disease progression and may assist clinicians with formulating more effective treatment measures. NLR-like inflammatory biomarkers, such as the systemic inflammatory response index (SIRI), have been shown to predict the prognosis of stroke patients who receive endovascular treatment and are successful recanalized [43]. However, even with complete or near complete recanalization, a higher admission SIRI increased the risk of a poor outcome at 3 months. Taken together, the advantage of these inflammatory markers is that they are easily available and accessible and cost-effective since they come from widely available laboratory variables that are typically collected in routine medical practices.
Our study had some limitations. First, this study was limited to patients who had experienced an anterior circulation stroke, and so the results cannot be extrapolated to the posterior circulation stroke population. Second, in order to study the mechanism of ischemia reperfusion injury, the enrolled patients had all undergone successful recanalization after thrombectomy; patients in whom revascularization was not successful were not included in the analysis. Third, some repeated measurements of NLR were missing for study patients. However, we used a generalized additive model and a generalized additive mixed model to analyze all collected data, and these models have been found to be useful when some data are missing. Finally, although we adjusted for multiple confounding factors, other potential confounding factors may have been missed in these analyses.
Conclusion
We demonstrated the pathophysiological changes of dynamic NLR on stroke and the persistent effect of inflammation on ischemia-reperfusion injury. Because NLR can be easily obtained repeatedly, these measurements can be used to assess the changes in disease progress over time. These results suggest that physicians should be aware of the potential harm associated with persistently high NLR in patients who have undergone successful revascularization for anterior circulation large vessel occlusion stroke.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NLR:
-
Neutrophil-to-lymphocyte ratio
- EVT:
-
Endovascular treatment
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- CT:
-
Tomography
- DSA:
-
Digital subtraction angiography
- NIHSS:
-
Health Stroke Scale
- ASPECTS:
-
Alberta Stroke Program Early CT Score
- IQR:
-
Interquartile range
References
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46–e110.
Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–31.
Kim JY, Park J, Chang JY, Kim SH, Lee JE. Inflammation after ischemic stroke: the role of leukocytes and glial cells. Exp Neurobiol. 2016;25(5):241–51.
Frangogiannis NG. The inflammatory response in myocardial injury, repair, and remodelling. Nat Rev Cardiol. 2014;11(5):255–65.
Kollikowski AM, Schuhmann MK, Nieswandt B, Müllges W, Stoll G, Pham M. Local leukocyte invasion during Hyperacute human ischemic stroke. Ann Neurol. 2020;87(3):466–79.
Montaner J, Alvarez-Sabín J, Molina C, Anglés A, Abilleira S, Arenillas J, et al. Matrix metalloproteinase expression after human cardioembolic stroke: temporal profile and relation to neurological impairment. Stroke. 2001;32(8):1759–66.
Castellanos M, Leira R, Serena J, Pumar JM, Lizasoain I, Castillo J, et al. Plasma metalloproteinase-9 concentration predicts hemorrhagic transformation in acute ischemic stroke. Stroke. 2003;34(1):40–6.
Batra A, Latour LL, Ruetzler CA, Hallenbeck JM, Spatz M, Warach S, et al. Increased plasma and tissue MMP levels are associated with BCSFB and BBB disruption evident on post-contrast FLAIR after experimental stroke. J Cereb Blood Flow Metab. 2010;30(6):1188–99.
Liesz A, Suri-Payer E, Veltkamp C, Doerr H, Sommer C, Rivest S, et al. Regulatory T cells are key cerebroprotective immunomodulators in acute experimental stroke. Nat Med. 2009;15(2):192–9.
Salas-Perdomo A, Miró-Mur F, Urra X, Justicia C, Gallizioli M, Zhao Y, et al. T cells prevent hemorrhagic transformation in ischemic stroke by P-selectin binding. Arterioscler Thromb Vasc Biol. 2018;38(8):1761–71.
Brooks SD, Spears C, Cummings C, VanGilder RL, Stinehart KR, Gutmann L, et al. Admission neutrophil-lymphocyte ratio predicts 90 day outcome after endovascular stroke therapy. J Neurointerv Surg. 2014;6(8):578–83.
Goyal N, Tsivgoulis G, Chang JJ, Malhotra K, Pandhi A, Ishfaq MF, et al. Admission neutrophil-to-lymphocyte ratio as a prognostic biomarker of outcomes in large vessel occlusion strokes. Stroke. 2018;49(8):1985–7.
Fang YN, Tong MS, Sung PH, Chen YL, Chen CH, Tsai NW, et al. Higher neutrophil counts and neutrophil-to-lymphocyte ratio predict prognostic outcomes in patients after non-atrial fibrillation-caused ischemic stroke. Biom J. 2017;40(3):154–62.
Semerano A, Laredo C, Zhao Y, Rudilosso S, Renú A, Llull L, et al. Leukocytes, collateral circulation, and reperfusion in ischemic stroke patients treated with mechanical Thrombectomy. Stroke. 2019;50(12):3456–64.
Chan KL, Feng X, Ip B, Huang S, Ma SH, Fan FSY, et al. Elevated neutrophil to lymphocyte ratio associated with increased risk of recurrent vascular events in older minor stroke or TIA patients. Front Aging Neurosci. 2021;13:646961.
Chen C, Gu L, Chen L, Hu W, Feng X, Qiu F, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as potential predictors of prognosis in acute ischemic stroke. Front Neurol. 2020;11:525621.
Kotfis K, Bott-Olejnik M, Szylińska A, Rotter I. Could neutrophil-to-lymphocyte ratio (NLR) serve as a potential marker for delirium prediction in patients with acute ischemic stroke? A prospective observational study. J Clin Med. 2019;8(7):1075.
Zhang WB, Zeng YY, Wang F, Cheng L, Tang WJ, Wang XQ. A high neutrophil-to-lymphocyte ratio predicts hemorrhagic transformation of large atherosclerotic infarction in patients with acute ischemic stroke. Aging (Albany NY). 2020;12(3):2428–39.
Giede-Jeppe A, Madžar D, Sembill JA, Sprügel MI, Atay S, Hoelter P, et al. Increased neutrophil-to-lymphocyte ratio is associated with unfavorable functional outcome in acute ischemic stroke. Neurocrit Care. 2020;33(1):97–104.
Yu S, Arima H, Bertmar C, Clarke S, Herkes G, Krause M. Neutrophil to lymphocyte ratio and early clinical outcomes in patients with acute ischemic stroke. J Neurol Sci. 2018;387:115–8.
Duan Z, Wang H, Wang Z, Hao Y, Zi W, Yang D, et al. Neutrophil-lymphocyte ratio predicts functional and safety outcomes after endovascular treatment for acute ischemic stroke. Cerebrovasc Dis. 2018;45(5–6):221–7.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–418.
Zaidat OO, Yoo AJ, Khatri P, Tomsick TA, von Kummer R, Saver JL, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. 2013;44(9):2650–63.
He L, Wang J, Wang F, Zhang L, Zhang L, Zhao W. Increased neutrophil-to-lymphocyte ratio predicts the development of post-stroke infections in patients with acute ischemic stroke. BMC Neurol. 2020;20(1):328.
Wang L, Guo W, Wang C, Yang X, Hao Z, Wu S, et al. Dynamic change of neutrophil to lymphocyte ratios and infection in patients with acute ischemic stroke. Curr Neurovasc Res. 2020;17(3):294–303.
Nam KW, Kim TJ, Lee JS, Kwon HM, Lee YS, Ko SB, et al. High neutrophil-to-lymphocyte ratio predicts stroke-associated pneumonia. Stroke. 2018;49(8):1886–92.
Lan Y, Sun W, Chen Y, Miao J, Li G, Qiu X, et al. Nomogram including neutrophil-to-lymphocyte ratio for the prediction of stroke-associated infections. Front Neurol. 2020;11:574280.
Najjar SS, Scuteri A, Shetty V, Wright JG, Muller DC, Fleg JL, et al. Pulse wave velocity is an independent predictor of the longitudinal increase in systolic blood pressure and of incident hypertension in the Baltimore longitudinal study of aging. J Am Coll Cardiol. 2008;51(14):1377–83.
Gueorguieva R, Krystal JH. Move over ANOVA: progress in analyzing repeated-measures data and its reflection in papers published in the archives of general psychiatry. Arch Gen Psychiatry. 2004;61(3):310–7.
Macrez R, Ali C, Toutirais O, Le Mauff B, Defer G, Dirnagl U, et al. Stroke and the immune system: from pathophysiology to new therapeutic strategies. Lancet Neurol. 2011;10(5):471–80.
Elenkov IJ, Chrousos GP. Stress system--organization, physiology and immunoregulation. Neuroimmunomodulation. 2006;13(5–6):257–67.
Meisel C, Schwab JM, Prass K, Meisel A, Dirnagl U. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. 2005;6(10):775–86.
Robba C, Battaglini D, Samary CS, Silva PL, Ball L, Rocco PRM, et al. Ischaemic stroke-induced distal organ damage: pathophysiology and new therapeutic strategies. Intensive Care Med Exp. 2020;8(Suppl 1):23.
Lattanzi S, Cagnetti C, Provinciali L, Silvestrini M. Neutrophil-to-lymphocyte ratio and neurological deterioration following acute cerebral hemorrhage. Oncotarget. 2017;8(34):57489–94.
Lattanzi S, Cagnetti C, Rinaldi C, Angelocola S, Provinciali L, Silvestrini M. Neutrophil-to-lymphocyte ratio improves outcome prediction of acute intracerebral hemorrhage. J Neurol Sci. 2018;387:98–102.
Alimohammadi E, Bagheri SR, Mardanpour P, Moradi F, Arjmandnia F, Esmaeili N. Baseline neutrophil-lymphocyte ratio can be associated with hematoma expansion in patients with intracerebral hemorrhage: a retrospective observational study. BMC Neurosci. 2022;23(1):18.
Świtońska M, Piekuś-Słomka N, Słomka A, Sokal P, Żekanowska E, Lattanzi S. Neutrophil-to-lymphocyte ratio and symptomatic hemorrhagic transformation in ischemic stroke patients undergoing revascularization. Brain Sci. 2020;10(11):771.
Luo Y, Reis C, Chen S. NLRP3 Inflammasome in the pathophysiology of hemorrhagic stroke: a review. Curr Neuropharmacol. 2019;17(7):582–9.
Kocaturk O, Besli F, Gungoren F, Kocaturk M, Tanriverdi Z. The relationship among neutrophil to lymphocyte ratio, stroke territory, and 3-month mortality in patients with acute ischemic stroke. Neurol Sci. 2019;40(1):139–46.
Aly M, Abdalla RN, Batra A, Shaibani A, Hurley MC, Jahromi BS, et al. Follow-up neutrophil-lymphocyte ratio after stroke thrombectomy is an independent biomarker of clinical outcome. J Neurointerv Surg. 2021;13(7):609–13.
Zou F, Wang J, Han B, Bao J, Fu Y, Liu K. Early neutrophil-to-lymphocyte ratio is a prognostic marker in acute ischemic stroke after successful revascularization. World Neurosurg. 2022;157:e401–9.
Piri Cinar B, Kunt R, Yuksel B, Gulluoglu H, Sayilir I, Celiker Uslu S, et al. Assessment of the relation between the neutrophil to lymphocyte ratio and severity of ischemic stroke in a large cohort. Int J Clin Pract. 2021;75(4):e13955.
Lattanzi S, Norata D, Divani AA, Di Napoli M, Broggi S, Rocchi C, et al. Systemic inflammatory response index and futile recanalization in patients with ischemic stroke undergoing endovascular treatment. Brain Sci. 2021;11(9):1164.
Acknowledgements
Not applicable.
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Contributions
Conception and design: Song Li, Linghong Hu, Jian Wang and Kefeng Liu. Analysis and interpretation: Yougang Wang, Feihui Zou and Bin Han; Drafting the manuscript: Song Li and Linghong Hu; Statistics: Song Li and Kefeng Liu. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consents were obtained from the participants entering the stroke registry, and this analysis was approved by the Ethics Committee of Changzhou Second People’s Hospital Affiliated to Nanjing Medical University (Approval No: [2021] YLJSC020). All methods were conducted in accordance with the ethical standards of the declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, S., Hu, L., Wang, J. et al. Prolonged increased neutrophil-to-lymphocyte ratio is associated with mortality after successful revascularization for treatment of acute ischemic stroke. BMC Neurol 22, 326 (2022). https://doi.org/10.1186/s12883-022-02847-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-022-02847-3